Contents
What is laryngeal cancer
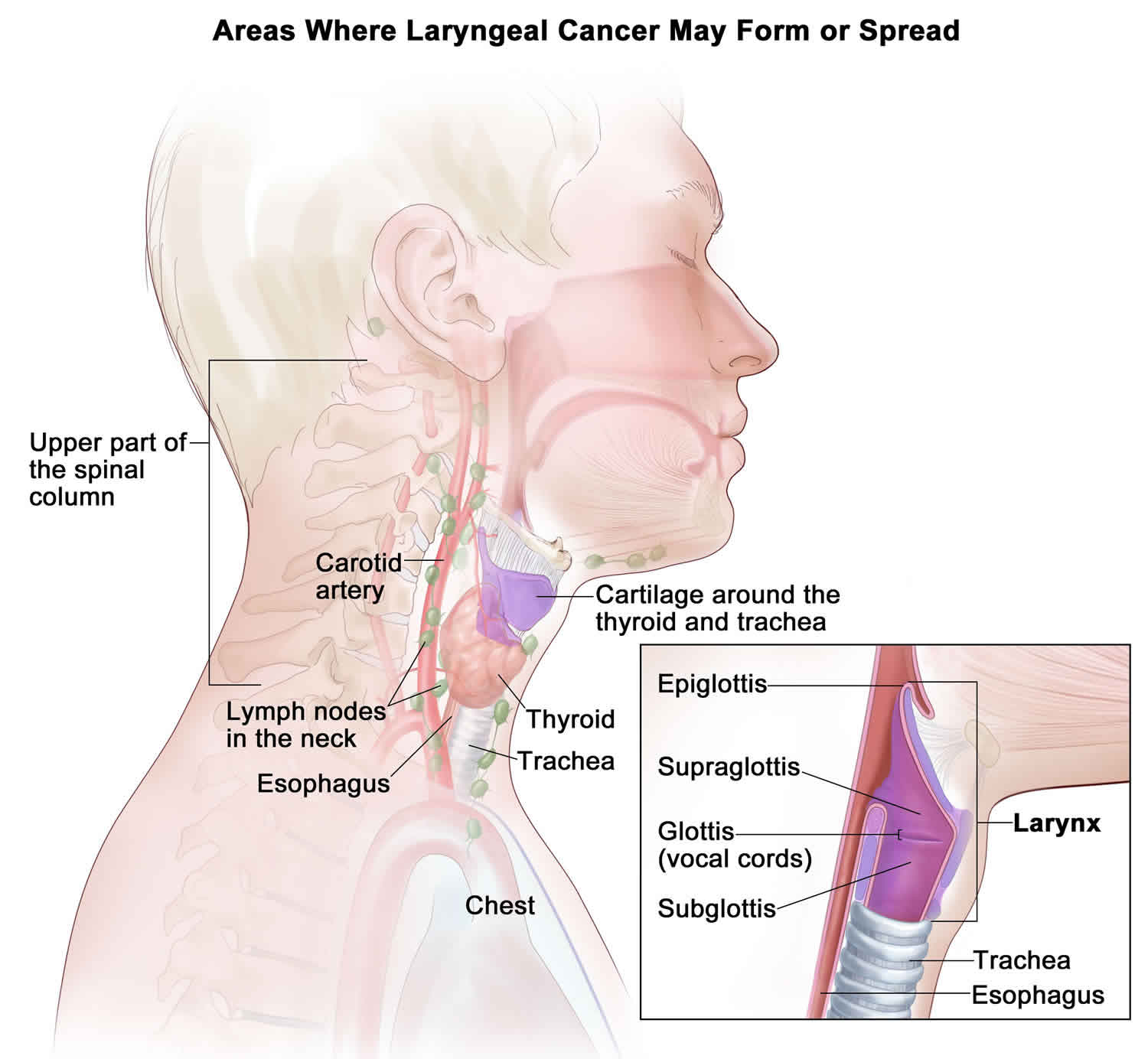
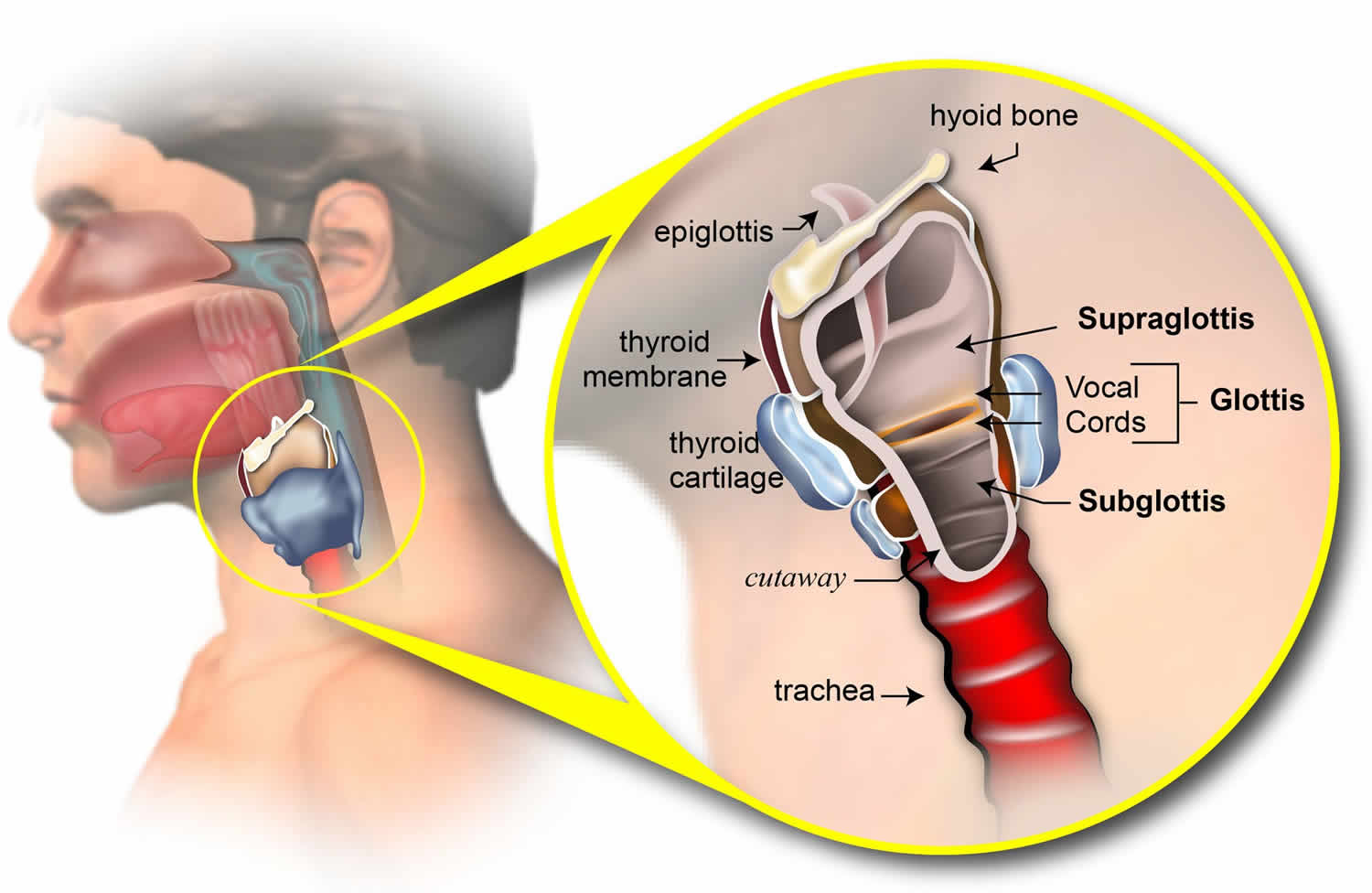
Laryngeal cancer is malignant (cancerous) cells that form in the larynx (voice box). The larynx, or voice box, is located in your throat. The larynx helps you breathe, speak, and swallow. The vocal cords, which help you speak, are part of the larynx. Most laryngeal cancers occur in the squamous cells, which line the inside of the larynx.
The larynx is made up mostly of cartilage, a flexible tissue that forms a framework of support.
There are three parts to the larynx:
- The supraglottis, or upper part.
- The glottis, the middle part. This is where the vocal cords are located. The vocal cords open and close, and allow you to breathe and speak.
- The subglottis, the lower part.
The larynx plays a role in several functions:
- When you breathe, the vocal cords open to allow air to pass through.
- When you speak, the vocal cords close. The air that passes through the vocal cords makes them vibrate, which helps create the sound of speech.
- When you swallow, the epiglottis (which is part of the supraglottis) drops down over the larynx and the vocal cords close tight to keep food out of the lungs. (Food goes down the esophagus to the stomach.)
About 60% of laryngeal cancers start in the glottis, 35% in the supraglottis, and the rest in the subglottis.
Laryngeal cancer is one of a group of head and neck cancers. In the United States, approximately 13,000 people a year are diagnosed with laryngeal cancer, and about 3,700 die from the disease every year.
The main symptoms of laryngeal cancer include:
- a change in your voice, such as sounding hoarse
- pain when swallowing or difficulty swallowing
- a lump or swelling in your neck
- a long-lasting cough
- a persistent sore throat or earache
- in severe cases, difficulty breathing
Some people may also experience bad breath, breathlessness, a high-pitched wheezing noise when breathing, unexplained weight loss, or fatigue (extreme tiredness).
Treatment options for laryngeal cancer depend on the following:
- The stage of the laryngeal cancer.
- The location and size of the tumor.
- Keeping the patient’s ability to talk, eat, and breathe as normal as possible.
- Whether the cancer has come back (recurred).
- Smoking tobacco and drinking alcohol decrease the effectiveness of treatment for laryngeal cancer. Patients with laryngeal cancer who continue to smoke and drink are less likely to be cured and more likely to develop a second tumor. After treatment for laryngeal cancer, frequent and careful follow-up is important.
Figure 1. Larynx
Laryngeal cancer causes
It’s not clear exactly what causes laryngeal cancer, but your risk of getting laryngeal cancer is increased by:
- smoking tobacco
- regularly drinking large amounts of alcohol
- having a family history of head and neck cancer
- having an unhealthy diet
- exposure to certain chemicals and substances, such as asbestos and coal dust
By adopting a healthy lifestyle, including avoiding alcohol and tobacco, you can significantly reduce your chances of developing laryngeal cancer.
Scientists believe that some risk factors, such as tobacco or heavy alcohol use, cause these cancers by damaging the DNA of the cells that line the inside of the larynx and hypopharynx.
DNA is the chemical in each of our cells that makes up our genes – the instructions for how our cells function. We usually look like our parents because they are the source of our DNA. But DNA affects more than how we look. Some genes have instructions for controlling when cells grow and divide into new cells. Genes that help cells grow and divide are called oncogenes. Genes that slow down cell division or cause cells to die at the right time are called tumor suppressor genes. Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes.
Some people inherit DNA mutations (changes) from their parents that greatly increase their risk for developing certain cancers. But inherited gene mutations are not believed to cause very many cancers of the larynx or hypopharynx.
Gene changes related to these cancers usually happen during life, rather than being inherited. These acquired mutations often result from exposure to cancer-causing chemicals, like those found in tobacco smoke. An acquired change in the p16 tumor suppressor gene seems to be important in laryngeal and hypopharyngeal cancers, although not all these cancers have this change. Several different gene changes are probably needed for cancer to develop, and not all of these changes are understood at this time.
Inherited mutations of oncogenes or tumor suppressor genes rarely cause these cancers, but some people seem to inherit a reduced ability to detoxify (break down) certain types of cancer-causing chemicals. These people are more sensitive to the cancer-causing effects of tobacco smoke, alcohol, and certain industrial chemicals. Researchers are developing tests that may help identify such people, but these tests are not yet reliable enough for routine use.
Some forms of human papillomavirus (HPV) are important causes of some throat cancers (including cancers of the hypopharynx). The outlook for people with these cancers appears to be better than for people whose cancers are the result of tobacco or alcohol use.
Risk factors for developing laryngeal cancer
A person has a much greater risk of developing laryngeal cancer if he or she smokes or uses other tobacco products. Drinking alcohol, especially in large amounts, also can increase the risk of developing laryngeal cancer. In fact, using tobacco and alcohol together increases the risk of cancer even more.
Other risk factors for laryngeal cancer include:
- Age: Laryngeal cancer occurs most often in people over the age of 55.
- Gender: Men are more likely to develop cancer of the larynx.
- A personal history of head and neck cancer: Nearly one in four people who have had head and neck cancer will get it again.
- Occupation: Workers who are exposed to sulfuric acid mist, wood dust, nickel, or the manufacturing of mustard gas have a greater risk of laryngeal cancer. In addition, machinists and people who work with asbestos are at greater risk.
Tobacco and alcohol use
Tobacco use is the most important risk factor for head and neck cancers (including cancers of the larynx and hypopharynx). The risk for these cancers is much higher in smokers than in nonsmokers. Most people with these cancers have a history of smoking or other tobacco exposure. The more you smoke, the greater your risk. Smoke from cigarettes, pipes, and cigars all increase your risk of getting these cancers.
Some studies have also found that long-term exposure to secondhand smoke might increase the risk of these cancers, but more research is needed to confirm this.
Moderate or heavy alcohol use (more than 1 drink a day) also increases the risk of these cancers, although not as much as smoking.
People who use both tobacco and alcohol have the highest risk of all. Combining these 2 habits doesn’t just add both risks together, it actually multiplies them. People who smoke and drink are many times more likely to get head and neck cancer than are people with neither habit.
Poor nutrition
Poor nutrition may increase the risk of getting head and neck cancer. The exact reason for this isn’t clear. Heavy drinkers often have vitamin deficiencies, which may help explain the role of alcohol in increasing risk of these cancers.
Researchers have been comparing eating habits and risk. It’s been suggested that eating fewer fried foods and processed foods and eating more plant-based foods might help reduce laryngeal cancer risk.
Human papillomavirus infection
Human papillomavirus (HPV) is a group of over 150 related viruses. They are called papilloma viruses because some of them cause a type of growth called a papilloma, more commonly known as a wart.
Infection with certain types of HPV can also cause some forms of cancer, including cancers of the penis, cervix, vulva, vagina, anus, and throat. Other types of HPV cause warts in different parts of the body.
HPV infection of the throat seems to be a factor in some throat cancers, such as some cancers of the tonsils and some cancers of the hypopharynx. HPV infection is very rarely a factor in laryngeal cancer.
Genetic syndromes
People with syndromes caused by inherited gene defects (mutations) have a very high risk of throat cancer, including cancer of the hypopharynx.
- Fanconi anemia: People with this syndrome often have blood problems at an early age, which may lead to leukemia or aplastic anemia. They also have a very high risk of cancer of the mouth and throat.
- Dyskeratosis congenita: This genetic syndrome can cause aplastic anemia, skin rashes, and abnormal fingernails and toenails. People with this syndrome have a very high risk of developing cancer of the mouth and throat when they are young.
Workplace exposures
Long and intense exposures to wood dust, paint fumes, and certain chemicals used in the metalworking, petroleum, plastics, and textile industries can increase the risk of laryngeal and hypopharyngeal cancers.
Asbestos is a mineral fiber that was often used as an insulating material in many products in the past. Exposure to asbestos is an important risk factor for lung cancer and mesothelioma (cancer that starts in the lining of the chest or abdomen). Some studies have suggested a link between asbestos exposure and laryngeal cancer, but not all studies agree.
Gender
Cancers of the larynx and hypopharynx are about 4 times more common in men than women. This is likely because the main risk factors − smoking and heavy alcohol use − are more common in men. But in recent years, as these habits have become more common among women, their risks for these cancers have increased as well.
Age
Cancers of the larynx and hypopharynx usually develop over many years, so they are not common in young people. Over half of patients with these cancers are 65 or older when the cancers are first found.
Race
Cancers of the larynx and hypopharynx are more common among African Americans and whites than among Asians and Latinos.
Gastroesophageal reflux disease
When acid from the stomach backs up into the esophagus it’s called gastroesophageal reflux disease (GERD). GERD can cause heartburn and increase the chance of cancer of the esophagus. Studies are being done to see if it increases the risk of laryngeal and hypopharyngeal cancers, too.
Laryngeal cancer prevention
It’s thought that most laryngeal cancers can be prevented by adopting a healthy lifestyle.
Avoiding tobacco products, cutting down on how much alcohol you drink and having a healthy diet are particularly important in reducing your chances of developing laryngeal cancer. Tobacco use is the most important cause of these cancers. Avoiding exposure to tobacco (by not smoking and avoiding secondhand smoke) lowers the risk of laryngeal cancers. Heavy alcohol use is a risk factor on its own. It also greatly increases the cancer-causing effect of tobacco smoke, so it’s especially important to avoid the combination of drinking and smoking.
Avoiding tobacco products
Using tobacco products increases your chances of developing several different types of cancer, including laryngeal cancer.
Tobacco comes in many forms, including:
- cigarettes
- pipe tobacco
- cigars
- cigarillos
- snuff (powdered tobacco snorted through the nose)
- chewing tobacco
If you smoke or use other tobacco products, stopping will have both short- and long-term health benefits, including significantly reducing your risk of developing laryngeal cancer.
Cutting down on alcohol
Staying within the recommended guidelines for alcohol consumption will also reduce your risk of developing laryngeal and liver cancers.
- men and women are advised not to regularly drink more than 14 units a week
- spread your drinking over 3 days or more if you drink as much as 14 units a week
A unit of alcohol is equal to about half a pint of normal-strength lager or a pub measure (25ml) or spirits. Read more about alcohol units.
Studies have found that your risk of developing laryngeal cancer reduces significantly within 5 to 10 years of not drinking, and after 20 to 30 years your risk is about the same as someone who has never drunk alcohol.
Contact your doctor if you’re finding it difficult to reduce the amount of alcohol you drink. You may need additional treatment, which could include counselling, group work or medication.
Healthy diet
Research shows a diet that contains plenty of fresh fruits and vegetables, particularly tomatoes, citrus fruit (such as oranges, grapefruits and lemons), olive oil and fish oil, may reduce your risk of getting laryngeal cancer. This type of diet is sometimes known as a “Mediterranean diet”.
Eating plenty of fruit and vegetables each day may help to reduce your chances of developing many types of cancer, including laryngeal cancer.
Avoid HPV infection
The risk of human papillomavirus (HPV) infection of the throat is increased in those who have oral sex and multiple sex partners. Smokers are more likely to get HPV infections, probably because the smoke damages their immune system or the cells that line the throat. These infections are common and rarely cause symptoms. While HPV infection is linked to some cases of cancer of the larynx or hypopharynx, most people with HPV infections of the throat do not go on to develop this cancer. And most cancers of the larynx and hypopharynx are not related to HPV infection.
Vaccines that reduce the risk of infection with certain types of HPV are available. At first, these vaccines were meant to lower the risk of cervical cancer, but they’ve been shown to lower the risk of other cancers linked to HPV as well, such as cancers of the anus, vulva, vagina, and mouth and throat cancers.
Since HPV vaccines are only effective if given before someone is infected with HPV, they are given at an early age.
Laryngeal cancer signs and symptoms
Some of the following may be symptoms of laryngeal cancer, or they could be symptoms of other conditions:
- A sore throat or cough that does not go away
- A change in your voice, such as hoarseness, that does not get better after two weeks
- Any pain or other trouble when you swallow
- Ear pain
- A lump in the neck or throat
- Dysphonia (problems producing voice sounds)
If you have any of the following symptoms, see your doctor right away:
- Dyspnea (trouble breathing)
- Stridor (breathing that is high-pitched and noisy)
- Globus sensation (a feeling like there is something in the throat)
- Hemoptysis (coughing up blood)
Early signs of laryngeal cancer
In most cases, laryngeal and hypopharyngeal cancers are found because of the symptoms they cause. Possible signs of laryngeal cancer include a sore throat and ear pain.
Hoarseness or voice changes
Laryngeal cancers that form on the vocal cords (glottis) often cause hoarseness or a change in the voice. This can lead to them being found at a very early stage. People who have voice changes (like hoarseness) that do not improve within 2 weeks should see their health care provider right away.
For cancers that don’t start on the vocal cords, hoarseness occurs only after these cancers reach a later stage or have spread to the vocal cords. These cancers are sometimes not found until they have spread to the lymph nodes and the person notices a growing mass in the neck.
Other symptoms
Cancers that start in the area of the larynx above the vocal cords (supraglottis), the area below the vocal cords (subglottis), or the hypopharynx do not usually cause voice changes, and are therefore more often found at later stages.
Symptoms of these cancers may include:
- A sore throat that does not go away
- Constant coughing
- Pain when swallowing
- Trouble swallowing
- Ear pain
- Trouble breathing
- Weight loss
- A lump or mass in the neck (due to spread of the cancer to nearby lymph nodes)
Many of these symptoms are more likely to be caused by conditions other than laryngeal or hypopharyngeal cancer. Still, if you have any of these symptoms, it is very important to have them checked by a doctor so that the cause can be found and treated, if needed.
Laryngeal cancer diagnosis
Laryngeal and hypopharyngeal cancers are usually found because of signs or symptoms a person is having. If cancer is suspected, tests will be needed to confirm the diagnosis. Getting a diagnosis of laryngeal or hyopharyngeal cancer when you haven’t had symptoms is rare. When it does happen, the cancer is usually found because of tests done to check other medical problems.
If you have signs or symptoms that suggest you might have a cancer of the larynx or hypopharynx, your doctor will need to do exams or tests to be sure.
These tests and procedures may be used to help diagnose laryngeal cancer:
- Physical exam: A physician will examine the throat and neck.
- Laryngoscopy: The doctor examines the larynx with a mirror or a thin, lighted tube called a flexible endoscope.
- Biopsy: The doctor removes a small piece of the larynx so that it can be examined under a microscope.
- CT or CAT scan (also called computed tomography, computerized tomography, or computerized axial tomography): Computed tomography uses X-rays and computers to produce images of a cross-section of the body.
- MRI (also called magnetic resonance imaging): Magnetic resonance imaging uses a large magnet, radio waves, and a computer to produce clear pictures, or images, of the human body.
- PET scan: A very small dose of a radioactive chemical, called a radiotracer, is injected into a vein in the arm. The tracer travels through the body and is absorbed by the organs and tissues being studied. A machine called a PET scanner creates three- dimensional pictures from the energy given off by the tracer substance.
If your doctor suspects a cancer of the larynx or hypopharynx, you will be referred to an ear, nose, and throat (ENT) doctor, also called an otolaryngologist. This doctor will do a more complete exam of your head and neck. This will include an inside look at the larynx and hypopharynx, known as laryngoscopy, which can be done in 2 ways:
- Direct (flexible) laryngoscopy: To do this, the doctor puts a fiber-optic laryngoscope (a thin, flexible, lighted tube) in through your mouth or nose to look at your larynx and nearby areas. Biopsies can be done through the scope (covered below).
- Indirect laryngoscopy: The doctor uses special small mirrors that are put into your mouth to look at your larynx and nearby areas.
Both types of exams can be done in the doctor’s office. For either type of exam, the doctor may spray the back of your throat with numbing medicine to help make the exam easier.
People with laryngeal or hypopharyngeal cancer also have a higher risk for other cancers in the head and neck region, so the nasopharynx (part of the throat behind the nose), mouth, tongue, and the neck are also carefully looked at and checked for any signs of cancer.
Panendoscopy
Panendoscopy is a procedure that combines laryngoscopy, esophagoscopy, and (at times) bronchoscopy. This lets the doctor thoroughly examine the entire area around the larynx and hypopharynx, including the esophagus (swallowing tube) and trachea (windpipe).
This exam is usually done in an operating room while you are under general anesthesia. (This means drugs are used to put you into a deep sleep.) The doctor uses a rigid laryngoscope to look for tumors in the larynx and hypopharynx. Other parts of the mouth, nose, and throat are examined as well. The doctor may also use an endoscope to look into the esophagus or a bronchoscope to look into the trachea (windpipe).
Your doctor will look at these areas through the scope(s) to find any tumors, see how large they are, and see how far they have spread to nearby areas. The doctor might also take out (biopsy) small tissue samples from any tumors or other changed areas using special tools put in through the scopes.
Biopsies to diagnose laryngeal and hypopharyngeal cancers
In a biopsy, the doctor removes a sample of tissue to be looked at under a microscope. It’s the only way to be sure of a diagnosis of laryngeal or hypopharyngeal cancer. There are many different types of biopsies.
Endoscopic biopsy
The larynx and hypopharynx are deep inside the neck, so taking out samples for biopsy can be complex. Biopsies of these areas are done in the operating room while you are under general anesthesia (asleep). The surgeon uses special instruments through an endoscope to remove small pieces of tissue.
Fine needle aspiration (FNA) biopsy
This type of biopsy isn’t used to remove samples in the larynx or hypopharynx, but it may be done to find the cause of an swollen lymph node in the neck. A thin, hollow needle is put through the skin into the mass (or tumor) to get cells for a biopsy. The cells are then looked at under a microscope. If the FNA finds cancer, the pathologist (the doctor examining the samples) can often tell what type of cancer it is. If the cancer cells look like they might have come from the larynx or hypopharynx, an endoscopic exam and biopsy of these areas will be needed.
If the FNA doesn’t find cancer, it only means that cancer was not found in that lymph node. There could still be cancer in other places. If you’re having symptoms that might be from a laryngeal or hypopharyngeal cancer, you could still need other tests to find the cause of the symptoms.
FNA biopsies may also be useful in some patients already known to have laryngeal or hypopharyngeal cancer. If the person has a lump in the neck, an FNA can show if the mass is due to spread of the cancer. FNA may also be used in patients whose cancer has been treated by surgery and/or radiation therapy, to help find out if a neck mass in the treated area is scar tissue or if it’s a return (recurrence) of the cancer.
Imaging tests
Imaging tests use x-rays, magnetic fields, or radioactive substances to create pictures of the inside of your body. Imaging tests are not used to diagnose laryngeal or hypopharyngeal cancers, but they’re done for a number of reasons after a cancer diagnosis, such as:
- To help look for a tumor if one is suspected
- To learn how far cancer may have spread
- To help determine if treatment is working
- To look for signs that the cancer has come back after treatment
Computed tomography (CT) scan
The CT scan (also known as a CAT scan) uses x-rays to make detailed cross-sectional images of your body. Instead of taking one picture like a standard x-ray, a CT scanner takes many pictures as it rotates around you. A computer then combines these pictures into an image of a slice of your body. Unlike a regular x-ray, a CT scan creates detailed images of the soft tissues and organs in the body.
This test can help your doctor determine the size of the tumor, see if it’s growing into nearby tissues, and find out if it has spread to lymph nodes in your neck. It may also be done to look for the spread of cancer to your lungs.
Magnetic resonance imaging (MRI) scan
MRI scans use radio waves and strong magnets instead of x-rays. The energy from the radio waves is absorbed and then released in a pattern formed by the type of tissue and by certain diseases. A computer translates the pattern into a very detailed image of parts of your body.
Because it provides a very detailed picture, an MRI scan may be done to look for spread of the cancer in the neck. These scans can be very useful in looking at other areas of the body, too.
Barium swallow
This is often the first test done if someone is having a problem with swallowing. For this test, you drink a chalky liquid called barium to coat the walls of the throat and esophagus (swallowing tube). A series of x-rays of the throat and esophagus is taken as you swallow. The barium can help show problems in the throat.
Chest x-ray
A chest x-ray may be done to see if the cancer has spread to the lungs. If any suspicious spots are seen on the chest x-ray, a CT scan of the chest may be needed to get a more detailed picture.
Positron emission tomography (PET) scan
For a PET scan, a form of radioactive sugar (known as fluorodeoxyglucose or FDG) is injected into the blood. The amount of radioactivity used is very low. Cancer cells grow quickly, so they absorb large amounts of the radioactive sugar. After about an hour, you will be moved onto a table in the PET scanner. A special camera creates a picture of areas of radioactivity in your body. The picture is not finely detailed like a CT or MRI scan, but it provides helpful information about your whole body. Some machines can do both a PET and CT scan at the same time (PET/CT scan). This lets the doctor compare areas of higher radioactivity on the PET with the more detailed pictures of that area on the CT.
A PET scan may be used to look for possible areas of cancer spread, especially if there is a good chance that the cancer is more advanced. This test can also be used to help tell if a suspicious area seen on another imaging test is cancer or not.
Other tests
Other tests may be done as part of a workup in people diagnosed with laryngeal or hypopharyngeal cancer. These tests are not used to diagnose the cancer, but they may be done to see if a person is healthy enough for certain treatments, like surgery or chemotherapy.
Blood tests are often done to see how well your liver and kidneys are working, and to help evaluate your overall health before treatment. Blood tests are also needed if you are getting chemo because it can affect the levels of blood cells in your body.
If surgery is planned, you might also get an electrocardiogram (EKG) to make sure your heart is working well. Some people having surgery also may need tests of their lung function. These are known as pulmonary function tests (PFTs).
Laryngeal cancer staging
After someone is diagnosed with laryngeal cancer, doctors will try to figure out if it has spread, and if so, how far. This process is called staging. The stage of a cancer describes how much cancer is in the body. It helps determine how serious the cancer is and how best to treat it. Doctors also use a cancer’s stage when talking about survival statistics.
The earliest stage of laryngeal cancer is stage 0, also known as carcinoma in situ (CIS). The other main stages range from I (1) through IV (4). Some stages are split further, using capital letters (A, B, etc.). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means cancer has spread more. And within a stage, an earlier letter means a lower stage. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
The staging system most often used for laryngeal cancer is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
- The extent of the main tumor (T): Where is the tumor? How far has it grown into the larynx and nearby structures? Has it affected vocal cord movement?
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes in the neck? If so, how many are affected, and how large are they?
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant parts of the body? (The most common sites of spread are the lungs, liver, or bones.)
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced.
Once the T, N, and M categories of the cancer have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The system described below is the most recent American Joint Committee on Cancer (AJCC) system, effective January 2018.
Laryngeal cancer is typically given a clinical stage based on the results of any exams, biopsies, and imaging tests that might have been done. If surgery has been done, the pathologic stage (also called the surgical stage) can be determined.
The stages of laryngeal cancer are slightly different, based on which part of the larynx the cancer starts in:
- The supraglottis (the area above the vocal cords)
- The glottis (the area that includes the vocal cords)
- The subglottis (the area below the vocal cords)
Laryngeal cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Stages of supraglottic laryngeal cancer
| AJCC stage | Stage grouping | Stage description* |
| 0 | Tis N0 M0 | The tumor is only in the top layer of cells lining the inside of the larynx and has not grown any deeper (Tis). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| I | T1 N0 M0 | The tumor has grown deeper, but it is only in one part of the supraglottis, and the vocal cords move normally (T1). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| II | T2 N0 M0 | The tumor has grown deeper, and it has grown into more than one part of the supraglottis (or glottis), and the vocal cords move normally (T2). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| III | T3 N0 M0 | The tumor is still only in the larynx, but it has caused a vocal cord to stop moving, OR the tumor is growing into nearby areas such as the postcricoid area, paraglottic space, pre-epiglottic (in front of the epiglottis) tissues, or the inner part of the thyroid cartilage (firm tissue that separates the thyroid gland from the front of the larynx) (T3). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| OR | ||
| T1 to T3 N1 M0 | The tumor might or might not have grown into structures just outside the larynx, and it might or might not have affected a vocal cord (T1 to T3). The cancer has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). | |
| IVA | T4a N0 or N1 M0 | The tumor has grown through the thyroid cartilage and/or is growing into tissues beyond the larynx (such as the thyroid gland, trachea, esophagus, tongue muscles, or neck muscles). This is also known as moderately advanced local disease (T4a). The cancer has not spread to nearby lymph nodes (N0), or it has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T1-T4a N2 M0 | The tumor might or might not have grown into structures outside the larynx (as far as moderately advanced disease), and it might or might not have affected a vocal cord (T1 to T4a). The cancer is N2:
The cancer has not spread to distant parts of the body (M0). | |
| IVB | T4b Any N M0 | The tumor is growing into the area in front of the spine in the neck (the prevertebral space), surrounds a carotid artery, or is growing down into the space between the lungs. This is also known as very advanced local disease (T4b). The cancer might or might not have spread to nearby lymph nodes (any N). It has not spread to distant parts of the body (M0). |
| OR | ||
| Any T N3 M0 | The tumor might or might not have grown into structures outside the larynx, and it might or might not have affected a vocal cord (any T). The cancer has spread to at least one lymph node that is larger than 6 cm across, OR it has spread to a lymph node and then grown outside of the lymph node (N3). It has not spread to distant parts of the body (M0). | |
| IVC | Any T Any N M1 | The tumor might or might not have grown into structures outside the larynx, and it might or might not have affected a vocal cord (any T). The cancer might or might not have spread to nearby lymph nodes (any N). The cancer has spread to distant parts of the body (M1). |
Footnote:
* The following additional categories are not listed on the table above:
- TX: Main tumor cannot be assessed due to lack of information.
- NX: Regional lymph nodes cannot be assessed due to lack of information.
Table 2. Stages of glottic laryngeal cancer
| AJCC stage | Stage grouping | Stage description* |
| 0 | Tis N0 M0 | The tumor is only in the top layer of cells lining the inside of the larynx and has not grown any deeper (Tis). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| I | T1 N0 M0 | The tumor has grown deeper, but it is only in the vocal cords, and they move normally (T1). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| II | T2 N0 M0 | The tumor has grown into the supraglottis or subglottis, and/or the vocal cords do not move normally (T2). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| III | T3 N0 M0 | The tumor is still only in the larynx, but it has caused a vocal cord to stop moving, OR the tumor is growing into the paraglottic space, OR the tumor is growing into the inner part of the thyroid cartilage (firm tissue that separates the thyroid gland from the front of the larynx) (T3). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| OR | ||
| T1 to T3 N1 M0 | The tumor might or might not have grown into structures just outside the larynx, and it might or might not have affected a vocal cord (T1 to T3). The cancer has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). | |
| IVA | T4a N0 or N1 M0 | The tumor has grown through the thyroid cartilage and/or is growing into tissues beyond the larynx (such as the thyroid gland, trachea, cricoid cartilage, esophagus, tongue muscles, or neck muscles). This is also known as moderately advanced local disease (T4a). The cancer has not spread to nearby lymph nodes (N0), or it has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T1-T4a N2 M0 | The tumor might or might not have grown into structures outside the larynx (as far as moderately advanced disease), and it might or might not have affected a vocal cord (T1 to T4a). The cancer is N2:
The cancer has not spread to distant parts of the body (M0). | |
| IVB | T4b Any N M0 | The tumor is growing into the area in front of the spine in the neck (the prevertebral space), surrounds a carotid artery, or is growing down into the space between the lungs. This is also known as very advanced local disease (T4b). The cancer might or might not have spread to nearby lymph nodes (any N). It has not spread to distant parts of the body (M0). |
| OR | ||
| Any T N3 M0 | The tumor might or might not have grown into structures outside the larynx, and it might or might not have affected a vocal cord (any T). The cancer has spread to at least one lymph node that is larger than 6 cm across, OR it has spread to a lymph node and then grown outside of the lymph node (N3). It has not spread to distant parts of the body (M0). | |
| IVC | Any T Any N M1 | The tumor might or might not have grown into structures outside the larynx, and it might or might not have affected a vocal cord (any T). The cancer might or might not have spread to nearby lymph nodes (any N). The cancer has spread to distant parts of the body (M1). |
Footnote:
* The following additional categories are not listed on the table above:
- TX: Main tumor cannot be assessed due to lack of information.
- NX: Regional lymph nodes cannot be assessed due to lack of information.
Table 3. Stages of subglottic laryngeal cancer
| AJCC stage | Stage grouping | Stage description* |
| 0 | Tis N0 M0 | The tumor is only in the top layer of cells lining the inside of the larynx and has not grown any deeper (Tis). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| I | T1 N0 M0 | The tumor has grown deeper, but it is only in the subglottis (T1). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| II | T2 N0 M0 | The tumor has grown into the vocal cords, which might or might not move normally (T2). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| III | T3 N0 M0 | The tumor is still only in the larynx, but it has caused a vocal cord to stop moving, OR the tumor is growing into the paraglottic space, OR the tumor is growing into the inner part of the thyroid cartilage (firm tissue that separates the thyroid gland from the front of the larynx) (T3). The cancer has not spread to nearby lymph nodes (N0) or to distant parts of the body (M0). |
| OR | ||
| T1 to T3 N1 M0 | The tumor might or might not have grown into structures just outside the larynx, and it might or might not have affected a vocal cord (T1 to T3). The cancer has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). | |
| IVA | T4a N0 or N1 M0 | The tumor is growing through the cricoid or thyroid cartilage and/or is growing into structures beyond the larynx (such as the thyroid gland, trachea, esophagus, tongue muscles, or neck muscles). This is also known as moderately advanced local disease (T4a). The cancer has not spread to nearby lymph nodes (N0), or it has spread to a single lymph node on the same side of the neck as the tumor, which is no larger than 3 centimeters (cm) across (N1). The cancer has not spread to distant parts of the body (M0). |
| OR | ||
| T1-T4a N2 M0 | The tumor might or might not have grown into structures outside the larynx (as far as moderately advanced disease), and it might or might not have affected a vocal cord (T1 to T4a). The cancer is N2:
The cancer has not spread to distant parts of the body (M0). | |
| IVB | T4b Any N M0 | The tumor is growing into the area in front of the spine in the neck (the prevertebral space), surrounds a carotid artery, or is growing down into the space between the lungs. This is also known as very advanced local disease (T4b). The cancer might or might not have spread to nearby lymph nodes (any N). It has not spread to distant parts of the body (M0). |
| OR | ||
| Any T N3 M0 | The tumor might or might not have grown into structures outside the larynx, and it might or might not have affected a vocal cord (any T). The cancer has spread to at least one lymph node that is larger than 6 cm across, OR it has spread to a lymph node and then grown outside of the lymph node (N3). It has not spread to distant parts of the body (M0). | |
| IVC | Any T Any N M1 | The tumor might or might not have grown into structures outside the larynx, and it might or might not have affected a vocal cord (any T). The cancer might or might not have spread to nearby lymph nodes (any N). The cancer has spread to distant parts of the body (M1). |
Footnote:
* The following additional categories are not listed on the table above:
- TX: Main tumor cannot be assessed due to lack of information.
- NX: Regional lymph nodes cannot be assessed due to lack of information.
Laryngeal cancer treatment
The treatment for laryngeal cancer largely depends on the size of the cancer. The main treatments for laryngeal cancer are radiotherapy, surgery and chemotherapy.
Radiotherapy or surgery to remove the cancerous cells from the larynx can often cure laryngeal cancer if it’s diagnosed early.
If the laryngeal cancer is advanced, a combination of surgery to remove part or all of the larynx, radiotherapy and chemotherapy can be used.
If you have surgery to remove your larynx, you’ll no longer be able to speak or breathe in the usual way. Instead, you will breathe through a permanent hole in your neck (stoma) and you will need additional treatment to help restore your voice.
This may include an implant in your throat, or an electrical device you hold against your throat to produce sound.
Most hospitals use multidisciplinary teams of specialists that work together to decide the best way to proceed with your treatment.
Members of your multidisciplinary team will probably include a surgeon, a clinical oncologist (a specialist in non-surgical treatment of cancer), and a specialist cancer nurse who will be responsible for co-ordinating your care.
Your cancer team will recommend what they think is the best treatment option, but the final decision will be yours.
Before visiting hospital to discuss your treatment options, you may find it useful to write a list of questions you’d like to ask your care team. For example, you may want to find out the advantages and disadvantages of particular treatments.
Your treatment plan
Your recommended treatment plan will depend on the stage of the cancer (see diagnosing laryngeal cancer for more information on staging).
If you have early-stage laryngeal cancer, it may be possible to remove the cancer using surgery (endoscopic resection) or radiotherapy alone. This may also be the case with slightly larger cancers, although a combination of surgery and radiotherapy is sometimes required.
In later-stage laryngeal cancer, more extensive surgery may be needed. Radiotherapy and chemotherapy will probably be used in combination. In some cases, the entire larynx may have to be removed.
A medication called cetuximab may be used in cases where chemotherapy is not suitable.
These treatments are described below.
Radiotherapy
Radiotherapy uses controlled doses of high-energy radiation to destroy cancerous cells. It can be used as a treatment on its own for early-stage laryngeal cancer, or it can be used after surgery to stop cancerous cells returning. It’s sometimes combined with chemotherapy.
The energy beams used during radiotherapy have to be precisely targeted to your larynx. To ensure the beams are directed at the exact area, a special plastic mask will be made to hold your head in the right position. A mould of your face will be taken, so that the mask can be made before treatment starts.
Radiotherapy is usually given in short daily sessions from Monday to Friday, with a break from treatment at the weekend. The course of treatment usually lasts for 3 to 7 weeks.
As well as killing cancerous cells, radiotherapy can affect healthy tissue and has a number of side effects, including:
- sore, red skin (similar to sunburn)
- mouth ulcers
- dry mouth
- loss of taste
- loss of appetite
- tiredness
- feeling sick
Your multidisciplinary team will monitor any side effects and treat them when possible. For example, protective gels can be used to treat mouth ulcers, and medicines are available for a dry mouth.
Radiotherapy can sometimes cause your throat tissue to become inflamed. Severe inflammation can cause breathing difficulties. Contact your key worker or visit your local accident and emergency (A&E) department as soon as possible if you have difficulty breathing.
Most side effects should pass within a few weeks of treatment finishing.
Surgery
There are 3 types of surgery that can be used to treat laryngeal cancer. They are:
- endoscopic resection
- partial laryngectomy
- total laryngectomy
These are described below.
Endoscopic resection
Endoscopic resection can be used in early-stage laryngeal cancer.
During the procedure, a surgeon uses a special microscope to get a magnified view of the larynx. This allows them to remove the cancer either with a laser or small surgical instruments.
An endoscopic resection is carried out under general anesthetic, so you will be unconscious during the procedure and won’t feel any pain.
Your mouth and throat may feel sore for a few weeks after the operation and there’s a risk of your voice changing as a result of the procedure, which can be permanent.
Partial laryngectomy
A partial laryngectomy can be used to treat some laryngeal cancers. The operation involves surgically removing the affected part of your larynx. Some of your vocal cords will be left in place, so you will still be able to talk, but your voice may be quite hoarse or weak.
While your larynx is healing, you may find breathing difficult. Your surgeon may need to create a temporary hole in your neck, which will be attached to a tube you can breathe through. This is known as a temporary tracheostomy.
Once your larynx has healed, the tube can be removed and the hole will heal, leaving a small scar.
This operation is uncommon nowadays, as endoscopic resection is preferred whenever possible.
Total laryngectomy
A total laryngectomy is usually used to treat advanced laryngeal cancer. The operation involves removing your entire larynx. Nearby lymph nodes (small glands that form part of the immune system) may also need to be removed if the cancer has spread to them.
As your vocal cords will be removed, you won’t be able to speak in the usual way after the operation. However, there are several ways to help restore your speech.
If you have a total laryngectomy, your surgeon will also need to create a permanent hole in your neck (called a stoma) to help you breath after the operation.
You will be given training on how to keep your stoma clean. Having a stoma can seem daunting and frightening at first, but most people get used to it after a few months.
Chemotherapy
Chemotherapy uses powerful cancer-killing medicines to damage the DNA of the cancerous cells and stop them reproducing. It may be used to shrink a tumour before surgery or radiotherapy, or in combination with radiotherapy to make the radiotherapy more effective.
It can also be used to treat laryngeal cancer that’s advanced or has come back after treatment. In this situation, it can relieve symptoms and may slow the cancer’s growth.
Chemotherapy medication is usually given as an injection into a vein (intravenously) once every 3 or 4 weeks, for up to 6 months. You may need to stay in hospital for a few days during each treatment or you may just come in for a short visit each time.
Chemotherapy can sometimes damage healthy tissue as well as the cancerous tissue. This, unfortunately, means side effects are common, such as:
- feeling and being sick
- hair loss
- loss of appetite
- diarrhea
- sore mouth and mouth ulcers
- tiredness
Chemotherapy can also weaken your immune system, making you more vulnerable to infection and illness.
It’s therefore important to report any symptoms of a potential infection to your multidisciplinary team, such as a high temperature, chills or a persistent cough. You should also avoid close contact with people known to have an infection.
The side effects of chemotherapy should improve after your treatment has finished.
Cetuximab
Cetuximab is a type of medication called a biological therapy. These medications target and disrupt the processes that cancerous cells use to grow and reproduce.
Cetuximab can be used in combination with radiotherapy to treat more advanced laryngeal cancer, when it’s not possible to use chemotherapy. For example, people with kidney or heart disease, or people with an ongoing infection, may not be able to have chemotherapy, because it could make them very ill.
Cetuximab is given slowly through a drip into your vein (intravenously) for up to an hour or more. It’s usually given weekly for up to 7 weeks.
Side effects of cetuximab are usually mild and include:
- rashes
- feeling sick
- diarrhoea
- breathlessness
Cetuximab can also trigger allergic reactions in some people, which can cause problems such as a swollen tongue or throat. In a few cases, the reaction can be severe and potentially life-threatening.
Most serious reactions occur within a day of treatment starting, so you’ll be closely monitored once your treatment begins. If you have symptoms of a severe reaction, such as a rapid heartbeat or breathing problems, medication can be used to relieve them (such as corticosteroids).
Laryngeal cancer prognosis
Laryngeal cancer prognosis depends on the following:
- The stage of the laryngeal cancer.
- The location and size of the tumor.
- The grade of the tumor.
- The patient’s age, gender, and general health, including whether the patient is anemic.
The prognosis for laryngeal cancer depends on the extent of the cancer when it’s diagnosed and treated.
Fortunately, most laryngeal cancers are diagnosed at an early stage, which means the outlook is generally better than some other types of cancer.
Overall, about 70 out of every 100 people will live for at least 5 years after diagnosis and about 60 out of every 100 people will live for at least 10 years.
If you smoke, stopping smoking after being diagnosed with laryngeal cancer may improve your outlook.
Laryngeal cancer survival rate
Survival rates can give you an idea of what percentage of people with the same type and stage of cancer are still alive a certain amount of time (usually 5 years) after they were diagnosed. They can’t tell you how long you will live, but they may help give you a better understanding of how likely it is that your treatment will be successful.
Keep in mind that survival rates are estimates and are often based on previous outcomes of large numbers of people who had a specific cancer, but they can’t predict what will happen in any particular person’s case. These statistics can be confusing and may lead you to have more questions. Talk with your doctor about how these numbers may apply to you, as he or she is familiar with your situation.
A relative survival rate compares people with the same type and stage of cancer to people in the overall population. For example, if the 5-year relative survival rate for a specific stage of laryngeal cancer is 60.3%, it means that people who have that cancer are, on average, about 60.3% as likely as people who don’t have that cancer to live for at least 5 years after being diagnosed.
The Surveillance, Epidemiology, and End Results (SEER) database tracks 5-year relative survival rates for laryngeal and hypopharyngeal cancer in the United States, based on how far the cancer has spread. The SEER database, however, does not group cancers using AJCC TNM stages (stage 1, stage 2, stage 3, etc.) for laryngeal or hypopharyngeal cancer. Instead, it groups cancers into localized, regional, and distant stages:
- Localized: There is no sign that the cancer has spread outside of the larynx (or hypopharynx). The 5-year survival for localized laryngeal cancer is 77.4% 2.
- Regional: The cancer has spread outside the larynx (or hypopharynx) to nearby structures or lymph nodes. The 5-year survival for localized laryngeal cancer is 44.7% 2.
- Distant: The cancer has spread to distant parts of the body, such as the lungs. The 5-year survival for localized laryngeal cancer is 33.3% 2.
- Unknown: Unstaged. The 5-year survival for localized laryngeal cancer is 51.2% 2.
In general, if the laryngeal cancer is found only in the part of the body where it started it is localized (sometimes referred to as stage 1). If it has spread to a different part of the body, the stage is regional or distant. The earlier laryngeal cancer is caught, the better chance a person has of surviving five years after being diagnosed. For laryngeal cancer, 54.0% are diagnosed at the local stage. The 5-year survival for localized laryngeal cancer is 77.4% 2.
These numbers are based on people diagnosed with cancers of the larynx or hypopharynx between 2008 and 2015. For laryngeal cancers, survival rates differ based on which part of the larynx the cancer started in (supraglottis, glottis, or subglottis).
Table 4. Supraglottis laryngeal cancer (part of the larynx above the vocal cords) 5-year relative survival rates
| SEER stage | 5-year relative survival rate |
| Localized | 60% |
| Regional | 47% |
| Distant | 30% |
| All SEER stages combined | 46% |
Table 5. Glottis laryngeal cancer (part of the larynx including the vocal cords) 5-year relative survival rates
| SEER stage | 5-year relative survival rate |
| Localized | 83% |
| Regional | 50% |
| Distant | 42% |
| All SEER stages combined | 77% |
Table 6. Subglottis laryngeal cancer (part of the larynx below the vocal cords) 5-year relative survival rates
| SEER stage | 5-year relative survival rate |
| Localized | 61% |
| Regional | (not available) |
| Distant | 47% |
| All SEER stages combined | 53% |
Understanding the numbers
- These numbers apply only to the stage of the cancer when it is first diagnosed. They do not apply later on if the cancer grows, spreads, or comes back after treatment.
- These numbers don’t take everything into account. Survival rates are grouped based on how far the cancer has spread. But other factors, such as your age and overall health, and how well the cancer responds to treatment, can also affect your outlook.
- People now being diagnosed with laryngeal or hypopharyngeal cancer may have a better outlook than these numbers show. Treatments improve over time, and these numbers are based on people who were diagnosed and treated at least five years earlier.





{kind=link}