Contents
Liver abscess
Liver abscess also called hepatic abscess is a pus-filled cavity within your liver, typically caused by bacterial, parasitic, or fungal infections 1, 2, 3, 4, 5. There are 3 major types of liver abscess classified by causes (etiology) 6:
- Pyogenic liver abscess, which is most often caused by several different types of microorganisms (polymicrobial), accounting for 80% of liver abscess cases in the United States.
- Amebic liver abscess caused by the protozoan Entamoeba histolytica, a parasite transmitted via the fecal–oral route that enters the portal venous system from the colon, accounting for 10% of liver abscess cases in the United States 7, 8. Amebic liver abscess is the most frequent extraintestinal manifestation of Entamoeba histolytica infection. Globally, amebic liver abscesses are the most common 9, 10. Amebic liver abscess is an important cause of space-occupying lesions of the liver, mainly in developing countries 11. For poorly understood reasons, amebic liver abscesses are 10 times more common in men than women, often presenting between the ages of 20 and 40 years 12, 13, 14. Onset can be acute, subacute, or subtle. Hepatic amebiasis has been reported over 20 years after the last visit to an endemic area, so any travel history may be important in this diagnosis. The majority will present with fever and right upper quadrant pain, typically without concurrent dysentery or gastrointestinal symptoms 15. Prompt recognition and appropriate treatment of amebic liver abscess lead to improved morbidity and mortality.
- Fungal liver abscess, most often due to fungal infection caused by the yeast Candida species, accounting for fewer than 10% of liver abscess cases in the United States, especially in individuals with weakened immune systems.
Most liver abscesses in the United States are caused by Streptococcus (52.5%) (subgroup: milleri [97%] and group D [3%]), Klebsiella pneumoniae (24.6%), and Escherichia coli (16.4%) bacteria (pyogenic liver abscess) and sometimes the protozoan parasite Entamoeba histolytica (amebic liver abscess). Very rarely, liver abscess can be caused by the Candida species fungi (fungal liver abscess), mycobacteria, and other atypical organisms 16, 17, 18, 19, 5. Amoebic liver abscess caused by Entamoeba histolytica is the predominant cause of liver abscess in India, seen in more than 60% of cases 20, 8. Appendicitis was traditionally the major cause of liver abscess. As diagnosis and treatment of appendicitis has advanced, its frequency as a cause for liver abscess has decreased to 10%.
Liver abscesses can occur via different routes such as 21:
- Blood spread of infection via the portal vein or hepatic arteries e.g., hepatic artery bacteremia 1
- Biliary spread of infection from ascending cholangitis or cholecystitis 22
- Direct inoculation in the setting of penetrating trauma or iatrogenic following a procedure e.g. endoscopic retrograde cholangiopancreatography (ERCP) 23
- Cirrhosis 24
- Inflammatory bowel disease (IBD) 22
- Pancreatic disease 22
- Perforated duodenal ulcer 25.
The usual pattern of hepatic abscess formation is that there is leakage of bowel in the abdomen that will travel to the liver through the portal vein. Many cases have an infected biliary tract that will cause an abscess via direct contact. The usual pathophysiology for pyogenic liver abscesses is bowel content leakage and peritonitis. Bacteria travel to the liver via the portal vein and resides there. Infection can also originate in the biliary system. Hematogenous spreading is also possible 26. Liver abscesses are most commonly due to pyogenic, amebic or mixed infections 27. The pyogenic abscesses are usually polymicrobial, but some organisms are seen more commonly in them; such as E.coli, Klebsiella, Streptococcus, Staphylococcus, and anaerobes 26. Less commonly hepatic abscess may be fungal in origin. The majority of liver abscesses in the Western world are infected with bacteria 28. In developing countries, parasitic liver abscesses are the most common 29. Most amoebic infections are caused by Entamoeba histolytica 26.
The annual incidence rate is about 2.3 cases per 100,000 people. Males are more frequently affected than females 30. Age plays a factor in the type of abscess one develops. People aged 40-60 years are more vulnerable to developing liver abscess that does not result from trauma.
The typical symptoms of liver abscess are right upper quadrant abdominal pain, fever, chills and jaundice. Anorexia, malaise and weight loss are also frequently seen. Depending on the immune status of the patient, and the organism involved, the presentation may be dramatic (acute) or gradual (insidious).
The most frequent symptoms of liver abscess include the following:
- Fever (either continuous or spiking). Afebrile presentations have also been documented.
- Chills
- Right upper quadrant abdominal pain
- Right shoulder pain
- Nausea and vomiting
- Anorexia
- Malaise
- Weight loss
- Night sweats
- Diarrhea
- Shortness of breath (dyspnea)
- Cough or hiccoughs due to diaphragmatic irritation may be reported.
- Pleurisy
Signs of liver abscess include:
- Right upper quadrant abdominal pain
- Hepatomegaly
- Jaundice
- Pleural effusion
- Elevated hemidiaphragm
- Right basilar rales
- Hepatic friction rub
Liver abscess is diagnosed by imaging scans like ultrasound or CT scans and microbiologic culture of abscess fluid. Blood cultures are positive in roughly 50% of cases. Laboratory tests include a complete blood count (CBC) with differential to identify anemia of chronic disease or neutrophilic leukocytosis, tests for liver function (liver enzymes are usually elevated in half the cases with hypoalbuminemia and elevation of alkaline phosphatase are the most common abnormalities; elevations of transaminase and bilirubin levels are variable), liver synthetic function tests (Prealbumin and INR), alkaline phosphatase (elevated in around 90% of patients), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and blood cultures to rule out bacteremia 31.
Percutaneous or surgical drainage of the liver abscess and antibiotic treatment are the cornerstones of liver abscess treatment 17. Liver abscess drainage is needed and can be done under ultrasonography or CT guidance 32, 33, 34. Percutaneous needle aspiration (at times repeatedly) might be all that is required for liver abscesses less than 5 cm, but a catheter placement might be warranted if the liver abscess diameter is more than 5 cm 35, 36. Percutaneous drainage with catheter placement is probably the most successful procedure for larger than 5 cm liver abscesses 37. Laparoscopic drainage is also used at times. Surgery should be done for peritonitis, thick wall abscesses, ruptured abscess, multiple large abscesses, and previously failed drainage procedures 1. An operation is performed either by a transperitoneal approach or by the posterior transpleural approach 1. The former approach drains the abscess and allows for the exploration of undetected ulcers, while the latter is better for posterior abscesses 1. Size, location, and stage help determine a successful treatment plan. When previous biliary procedures have been done, endoscopic retrograde cholangiopancreatography (ERCP) drainage might be used 38. Undrained liver abscesses may cause sepsis, peritonitis, and empyema.
Empiric antibiotic coverage is essential when the organism is unknown. The antibiotics should cover Enterobacteriaceae, anaerobes, streptococci, enterococci, and Entamoeba histolytica 1. Such antibiotic regimens include cephalosporins plus metronidazole, Beta-lactam Beta-Lactamase inhibitor plus metronidazole, or synthetic penicillins plus aminoglycosides and metronidazole 1. Alternatively, fluoroquinolones or carbapenems can be substituted for cephalosporins or penicillins in case of allergy or unavailability. Metronidazole should cover Entamoeba histolytica 1. The duration of treatment varies but is usually from two to six weeks 1. After initial intravenous treatment, the oral route can be used safely in most cases to complete the course 1. Culture results help narrow down the organism, so empiric treatment is no longer needed, as it can lead to antibiotic resistance. Anaerobes are hard to culture, so sometimes they should be treated for the entire course empirically. For stable patients, antibiotics can be given post-drainage to increase culture yield for proper treatment. Empiric antifungal treatment is crucial in immunosuppressed patients with a risk for chronic disseminated fungemia 1.
Antibiotic therapy as a sole treatment for liver abscess is not routinely advocated, though it has been successful in a few reported cases. Antibiotic therapy alone may be the only alternative in patients too ill to undergo invasive procedures or in those with multiple abscesses not amenable to percutaneous or surgical drainage 1, 39. In these instances, patients are likely to require many months of antimicrobial therapy with serial imaging and close monitoring for associated complications.
If the source is Echinococcus tapeworms (Echinococcus granulosus, Echinococcus multilocularis, Echinococcus oligarthrus or Echinococcus vogeli), treatment includes a benzimidazole, such as albendazole 1. This therapy may last for several years 1. Although most cases are uncomplicated and can be treated with an antiparasitic drug, complicated cases must be treated delicately. In most complicated cases, drainage is necessary. Surgeons must take caution to inject the hydatid cysts before draining them, as sometimes the rupture can cause the patient to go into shock rapidly 1.
In a study by Abbas 40, the mean duration of hospital stay for those with pyogenic liver abscesses was 13.6 days. Antibiotic therapy used for them was approximately 34.7 days. One patient expired. On the other hand, patients with amebic liver abscesses had a mean hospital stay of approximately 7.7 days, with a mean duration of treatment of 11.8 days, where all patients were cured 40.
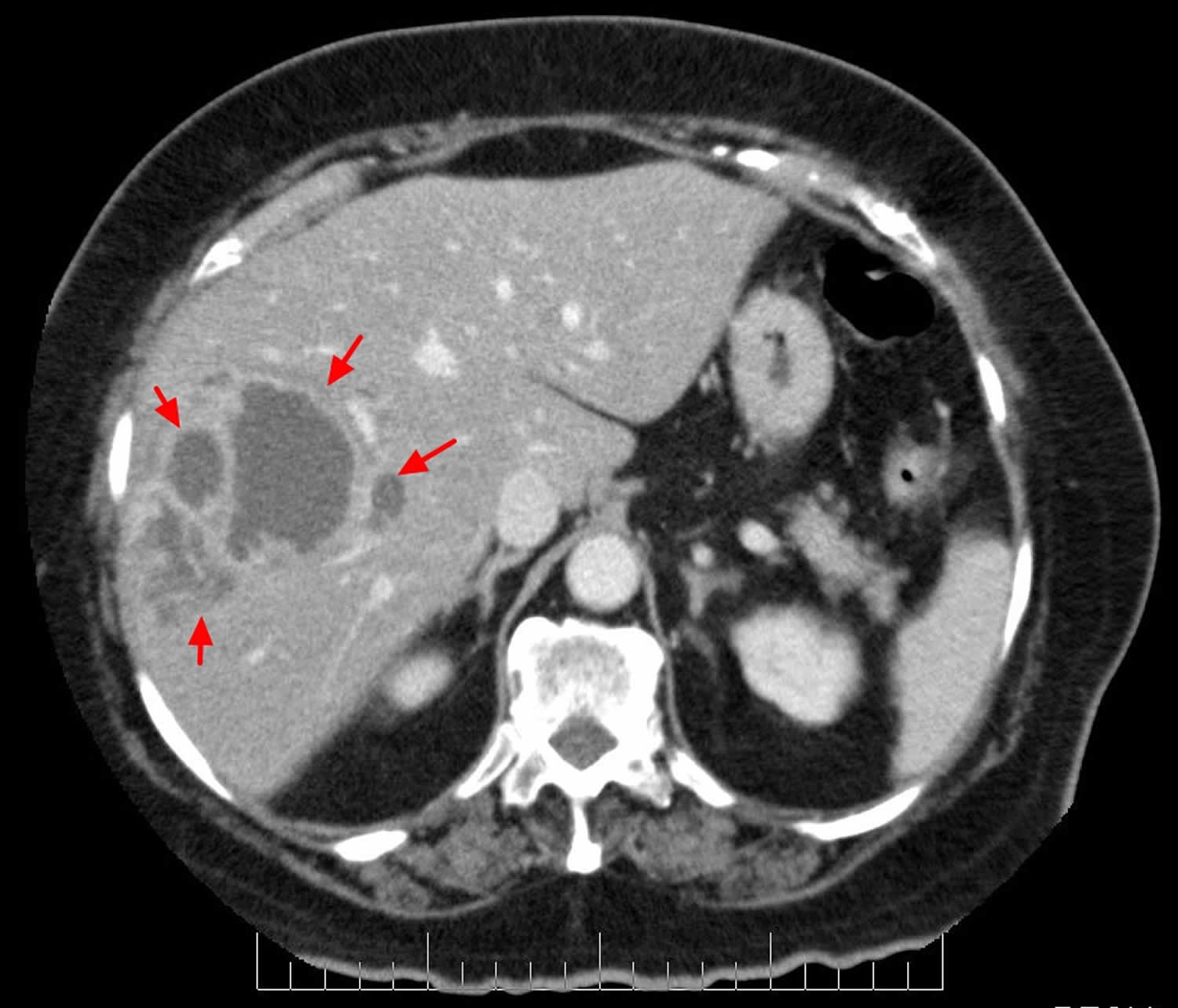
Figure 1. Liver abscess

Footnotes: Abdominal computed tomography (CT) scan showing a multiloculated liver abscess measuring 10 cm x 7.8 cm with multiple small abscesses on the left liver lobe. A 55-year-old woman who presented with 6 months of intermittent high fever, chronic non-bloody watery diarrhea and weight loss. There were no other complaints. She went to another hospital two years ago for chronic diarrhea and abdominal pain, for which she had an incomplete sigmoidoscopy which was normal according to the patient. There was no history of extra-intestinal and hepatobiliary manifestations when she was seen for the first time two years ago. Besides hypertension, she had no significant past medical or surgical history. She denied any travel history, intravenous (IV) drug abuse or a history of chronic intake of immunosuppressants or antibiotics. Her family history was non-contributory. Her vital signs were: temperature 102.2 °F, heart rate 105 beats per minute, respiratory rate 18/minute and blood pressure 150/103 mmHg. Physical examination was only significant for mild tenderness in the epigastric/periumbilical area with intact bowel sounds. There was no guarding/rebound tenderness or organomegaly. Laboratory workup revealed elevated white blood cell (WBC) count at 25.91 x 109 cells per liter with a left shift, hemoglobin at 10.1 g/dL and platelets at 462 x 109/L. The basic metabolic panel did not reveal significant electrolytes disturbances. Kidney and liver functions were within normal limits except mild coagulopathy with international normalised ratio (INR) at 1.58 and hypoalbuminemia at 2.9 g/dL. Inflammatory markers erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were remarkably elevated. Infectious workup including human immunodeficiency virus (HIV), hepatitis, clostridium difficile, ova/parasites, Entamoeba, Giardia and feces culture with toxin were not suggestive. Stool osmolar gap was indeterminate and celiac workup was negative.
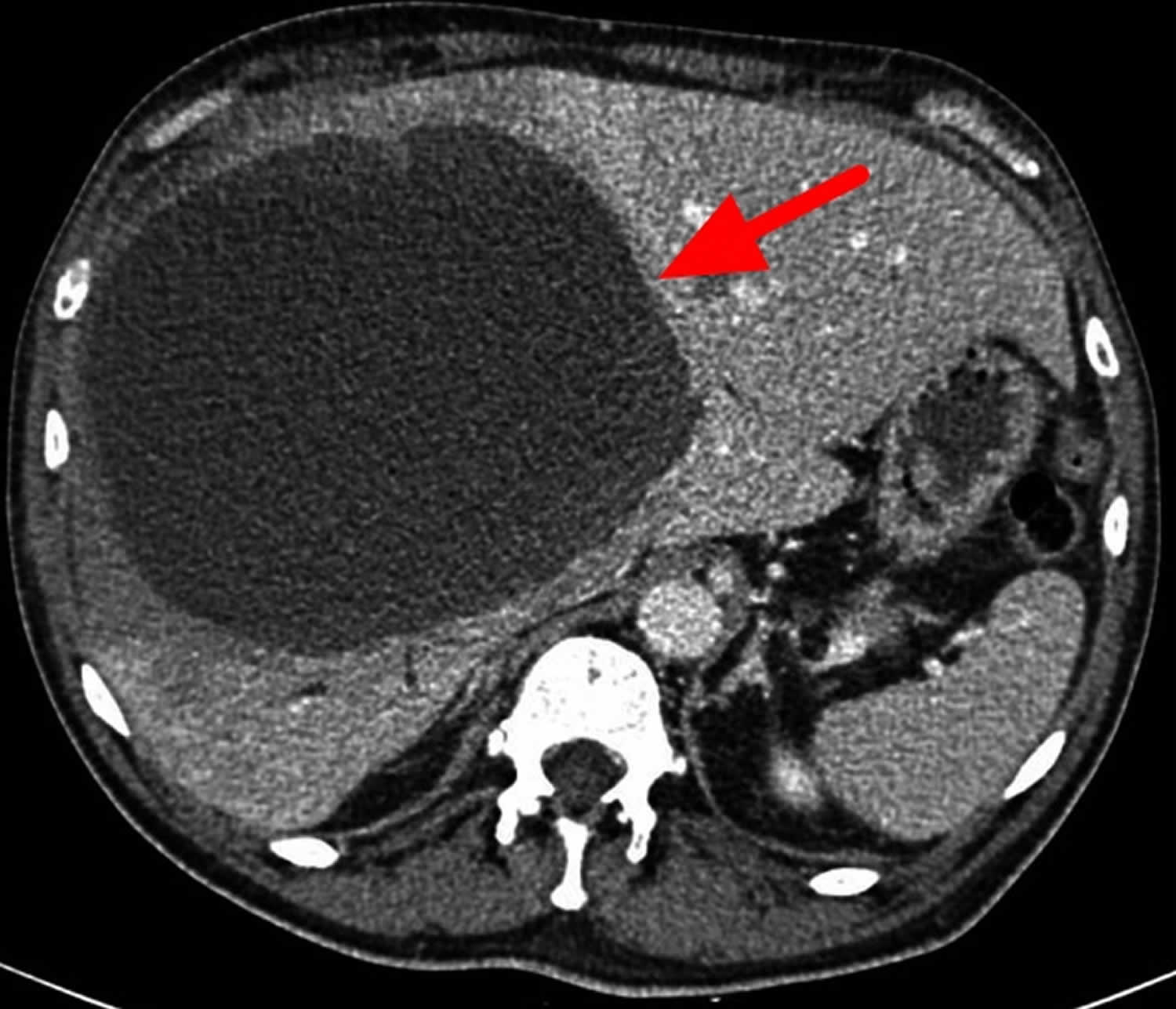
[Source 19 ]Figure 2. Pyogenic liver abscess CT scan
Footnotes: Pyogenic liver abscess in a 75 year old woman who presented with right upper quadrant abdominal pain and fever. CT demonstrates a large irregular fluid-density lesion within the right lobe of the liver with rim enhancement (inner rim) and a thin outer ring of hypoattenuation (“double target sign”). There are multiple smaller peripheral lesions with similar characteristics. Some of these appear coalescent forming “cluster sign”. This is the typical appearance of a pyogenic liver abscess. Percutaneous CT-guided drainage was performed. Heavy growth of Streptococcus milleri was grown. The most common organisms found in pyogenic liver abscesses are Staphylococcus aureus in children and Escherichia coli in adults. Differential diagnoses include: amoebic abscess, hydatid cyst, cystic metastasis, and biliary cystadenocarcinoma.
[Source 41 ]Figure 3. Amoebic liver abscess CT scan
Footnotes: A 63-year-old Italian man with unremarkable medical history required medical attention because of abdominal pain and fever. He was initially hospitalized in another hospital, where a CT scan of the abdomen was performed showing the presence of a large liver abscess of 11 cm involving the S6 and S7 segments. A drainage was positioned into the abscess but culture of the fluid was negative. Therefore, an empirically broad-spectrum antimicrobial therapy with piperacillin/tazobactam was started with benefit on symptoms, and size reduction of liver lesion at a follow-up CT scan. The patient was finally discharged after hepatic drainage removal. One month after discharge, he experienced new onset of daily fever up to 100.4°F (38°C) and abdominal pain, so he presented to medical attention (day 0). New abdominal CT scan was performed with evidence of a dimensional increase of the known liver lesion (14 × 16 cm) involving the S4, S5, S7, and S8 segments with compression of the intrahepatic tract of the inferior vena cava, portal system, and suprahepatic veins, and leading to dilatation of the intrahepatic biliary tract. Among the microbiological investigations performed, serology for Entamoeba histolytica test was positive, using an ELISA method performed with an Entamoeba histolytica IgG DRG kit (DRG Instruments GmbH, Germany), whereas detection of amoebic antigen in stools and blood was negative using an immunochromatographic method performed with an ImmunoCardSTAT CGE kit (Meridian Bioscence, Milan, Italy). On day 3, a percutaneous liver drainage was positioned, with evacuation of purulent, brown-colored material (with the presence of 92,000/mm³ leukocytes and 88,000/mm³ lymphocytes on cytometry). From drainage culture a contaminant coagulase-negative Staphylococcus spp. was isolated, and the amoebic antigen test was negative. On day 12 after admission, the patient needed laparotomy, with resection of a voluminous septate liver lesion. Intraoperative drainage fluid presented as brown purulent material, resembling the classic amoebic “anchovy paste” appearance. At this point, Biofire FilmArray gastrointestinal multiplex PCR panel (BioMérieux, France) was performed on the sterile intraoperative drainage fluid, with rapid molecular detection of the Entamoeba histolytica gene, despite the same test performed on stool being negative. Targeted antimicrobial therapy with metronidazole 750 mg every 8 hour was started on the same day (day 12). Since the majority of Gram-negative pathogens responsible for bacterial liver abscess are not detected by the FilmArray panel, empirical antibiotic therapy previously started was discontinued only when superinfection of the lesion was excluded by negative traditional culture on drainage fluid (day 17). A 7-day course of intraluminal therapy with paromomycin was also performed after completion of a well-tolerated 10-day course of metronidazole therapy, to promote intestinal decolonization of the parasite.
[Source 8 ]Figure 4. Liver abscess treatment algorithm
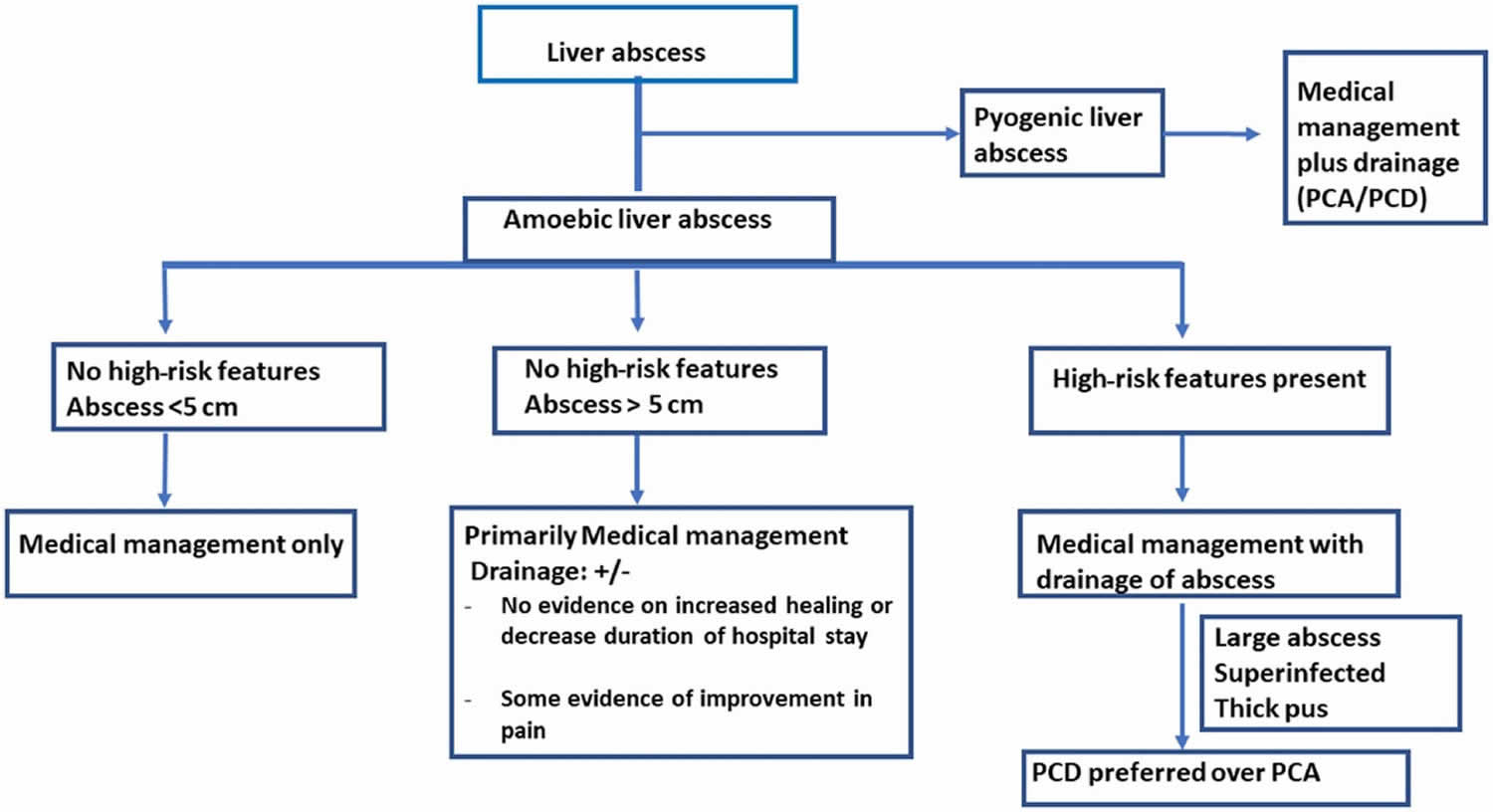
Footnotes: Suggested algorithm for the management of liver abscess.
Abbreviations: PCD = percutaneous catheter drainage; PCA = percutaneous needle aspiration
[Source 4 ]Liver abscess causes
Most liver abscesses in the United States are caused by Streptococcus (52.5%) (subgroup: milleri [97%] and group D [3%]), Klebsiella pneumoniae (24.6%), and Escherichia coli (16.4%) bacteria (pyogenic liver abscess) and sometimes the protozoan parasite Entamoeba histolytica (amebic liver abscess). Very rarely, liver abscess can be caused by the Candida species fungi (fungal liver abscess), mycobacteria, and other atypical organisms 16, 17, 18, 19, 5. Amoebic liver abscess caused by Entamoeba histolytica is the predominant cause of liver abscess in India, seen in more than 60% of cases 20, 8.
Pyogenic liver abscess may be caused by a variety of organism, including Klebsiella pneumoniae, Escherichia coli and Burkholderia pseudomallei 42. The microbiology differs according to the presumed route of hepatic invasion. Infections may arise from the biliary tree usually from an impacted gallstone, circulation (portal vein, hepatic artery), a contiguous focus of infection and penetrating trauma 2. Reports suggest that Klebsiella pneumoniae is an increasingly prominent cause 16. Abscesses involving Klebsiella pneumoniae have been associated with multiple cases of endophthalmitis. Enterobacteriaceae are especially prominent when the infection is of biliary origin. In the South–East Asian region, patients working with soil and water with comorbidities such as diabetes, liver and kidney failure and hazardous consumption of alcohol are also at risk of infection with Burkholderia pseudomallei (Melioidosis) 43.
Melioidosis is an important cause of liver abscess in Southeast Asia 43. Melioidosis also called Whitmore’s disease, is an infectious disease caused by the aerobic, Gram-negative soil-dwelling bacillus bacteria Burkholderia pseudomallei that are commonly found in the soil and water, that can infect humans or animals through direct contact with soil, water, or air contaminated by the bacteria 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55. Because the Burkholderia pseudomallei bacteria reside in soil and water, weather events such as hurricanes, heavy rain, flooding and typhoons have been implicated in outbreaks of melioidosis. Burkholderia pseudomallei is mostly found in tropical climates, especially in Southeast Asia and northern Australia, where it causes widespread melioidosis. In the United States, Burkholderia pseudomallei is found in Puerto Rico, the U.S. Virgin Islands, and the Gulf Coast area of the state of Mississippi. Melioidosis is a rare disease in the United States with most melioidosis illnesses in the United States occur in people who have traveled to areas where the disease is more common. Some cases have also occurred in people who have had contact with contaminated products from overseas 55.
People can get melioidosis by 55:
- Breathing in contaminated dust or water droplets
- Eating or drinking contaminated food or water
- Having contact with contaminated soil or water, especially through skin breaks (cuts, scrapes, etc.) or getting it in their mouths
It’s very rare for people to get melioidosis from another person.
Appendicitis was traditionally the major cause of liver abscess 56. As diagnosis and treatment of appendicitis has advanced, its frequency as a cause for liver abscess has decreased to 10% 56.
Biliary tract disease is now the most common source of pyogenic liver abscess 56. Obstruction of bile flow allows for bacterial proliferation. Biliary stone disease, obstructive cancer affecting the biliary tree, stricture, and congenital diseases are common inciting conditions. With a biliary source, liver abscesses usually are multiple, unless they are associated with surgical interventions or indwelling biliary stents. In these instances, solitary lesions can be seen.
Infections in organs in the portal bed can result in a localized septic thrombophlebitis, which can lead to liver abscess 56. Septic emboli are released into the portal circulation, trapped by the hepatic sinusoids, and become the nidus for microabscess formation. These microabscesses initially are multiple but usually coalesce into a solitary lesion.
Microabscess formation can also be due to hematogenous dissemination of organisms in association with systemic bacteremia, such as endocarditis and pyelonephritis 56. Cases also are reported in children with underlying defects in immunity, such as chronic granulomatous disease and leukemia 56.
Approximately 4% of liver abscesses result from fistula formation between local intra-abdominal infections 56.
Despite advances in diagnostic imaging, cryptogenic causes account for a significant proportion of liver abscess cases; surgical exploration has impacted this minimally 56. These lesions usually are solitary in nature.
Pyogenic liver abscess has been reported as a secondary infection of amebic abscess, hydatid cystic cavities, and metastatic and primary liver tumors 56. A small case series in Taiwan investigated pyogenic liver abscess as the initial manifestation of underlying hepatocellular carcinoma (liver cancer). In regions with a high prevalence of both pyogenic liver abscess and hepatocellular carcinoma, clinicians should be aware of the possibility of underlying hepatocellular carcinoma in patients with risk factors for the disease 57.
Pyogenic liver abscess is also a known complication of liver transplantation, hepatic artery embolization in the treatment of hepatocellular carcinoma, and the ingestion of foreign bodies, which penetrate the liver parenchyma 56. Trauma and secondarily infected liver pathology account for a small percentage of liver abscess cases 56. Penetrating trauma to the liver can inoculate organisms directly into the liver parenchyma, resulting in pyogenic liver abscess 56. Nonpenetrating trauma can also be the precursor to pyogenic liver abscess by causing localized hepatic necrosis, intrahepatic hemorrhage, and bile leakage. The resulting tissue environment permits bacterial growth, which may lead to pyogenic liver abscess 56. These lesions are typically solitary.
The pathogenic role of anaerobes was underappreciated until the isolation of anaerobes from 45% of cases of pyogenic liver abscess in 1974 58. Since that time, increasing rates of anaerobic involvement have been reported, likely because of increased awareness and improved culturing techniques. The most frequently encountered anaerobes are Bacteroides species, Fusobacterium species, and microaerophilic and anaerobic streptococci 58. A colonic source is usually the initial source of infection 58.
Staphylococcus aureus liver abscesses usually result from blood spread of organisms involved with distant infections, such as endocarditis 58. Streptococcus milleri is neither anaerobic nor microaerophilic. Streptococcus milleri has been associated with both monomicrobial and polymicrobial abscesses in patients with Crohn disease, as well as with other patients with pyogenic liver abscess 58.
Amebic liver abscess is most often caused by the protozoan parasite Entamoeba histolytica. Liver abscess is the most common extraintestinal manifestation of amebiasis.
Fungal abscesses primarily are due to Candida albicans and occur in individuals with prolonged exposure to antimicrobials, hematologic cancers, solid-organ transplants, and congenital and acquired immunodeficiency. Cases involving Aspergillus species have been reported.
Other organisms reported in the literature include Actinomyces species, Eikenella corrodens, Yersinia enterocolitica, Salmonella typhi, and Brucella melitensis.
The right hepatic lobe is affected more often than the left hepatic lobe by a factor of 2:1 56. Bilateral involvement is seen in 5% of cases. The predilection for the right hepatic lobe can be attributed to anatomic considerations. The right hepatic lobe receives blood from both the superior mesenteric and portal veins, whereas the left hepatic lobe receives inferior mesenteric and splenic drainage 56. It also contains a denser network of biliary canaliculi and, overall, accounts for more hepatic mass. Studies have suggested that a streaming effect in the portal circulation is causative 56.
Risk factors for getting liver abscess
The following risk factors are associated with liver abscess:
In developed countries, bacterial abscesses are most common, usually in the setting of comorbidities such as:
- infection elsewhere (most common)
- abdominal sepsis most common 59
- necrotizing enterocolitis (portal venous drainage)
- immunocompromised
- intravenous drug use
- trauma
- Endoscopic Retrograde Cholangiopancreatography (ERCP) 23
- cirrhosis 24
- hepatic artery bacteremia 1
- biliary disease 22
- inflammatory bowel disease (IBD) 22
- pancreatic disease 22
- perforated duodenal ulcer 25
Liver abscess signs and symptoms
The typical symptoms of liver abscess are right upper quadrant abdominal pain, fever, chills and jaundice. Anorexia, malaise and weight loss are also frequently seen. Depending on the immune status of the patient, and the organism involved, the presentation may be dramatic (acute) or gradual (insidious).
The most frequent symptoms of liver abscess include the following:
- Fever (either continuous or spiking). Afebrile presentations have also been documented.
- Chills
- Right upper quadrant abdominal pain
- Right shoulder pain
- Nausea and vomiting
- Anorexia
- Malaise
- Weight loss
- Night sweats
- Diarrhea
- Shortness of breath (dyspnea)
- Cough or hiccoughs due to diaphragmatic irritation may be reported.
- Pleurisy
Signs of liver abscess include:
- Right upper quadrant abdominal pain
- Enlarged liver (hepatomegaly)
- Jaundice
- Pleural effusion
- Elevated hemidiaphragm
- Right basilar rales
- Hepatic friction rub
Fever and tender hepatomegaly are the most common signs 61. A palpable mass need not be present. Midepigastric tenderness, with or without a palpable mass, is suggestive of left hepatic lobe involvement 61.
Decreased breath sounds in the right basilar lung zones, with signs of atelectasis and effusion on examination or radiologically, may be present 61. A pleural or hepatic friction rub can be associated with diaphragmatic irritation or Glisson capsule inflammation.
Jaundice may be present in as many as 25% of cases and usually is associated with biliary tract disease or the presence of multiple abscesses 61.
Fever of unknown origin (FUO) frequently can be an initial diagnosis in indolent cases. Multiple abscesses usually result in more acute presentations, with symptoms and signs of systemic toxicity.
Afebrile presentations have been documented.
Liver abscess complication
Liver abscess complications include:
- Hepatic vein thrombosis: ~22% 62
- Portal vein thrombosis: ~24% 62
- Abscess rupture into:
- right subphrenic space
- abdominal cavity
- pericardium
- gastrointestinal tract 63
- Empyema resulting from contiguous spread or intrapleural rupture of abscess
- Peritonitis or abdominal collection
- Pyopericardium – a severe and often fatal condition where pus accumulates in the pericardial sac.
- Sepsis
- Thrombosis of the inferior vena cava 63
- Compression of inferior vena cava: ascites and pedal edema
- Compression of biliary tree: jaundice
- Septic pulmonary embolism may occur in patients with a liver abscess caused by Klebsiella pneumoniae; a study by Wang et al reported an incidence of 6% in a group of these patients 64
- Endophthalmitis when an abscess is associated with Klebsiella pneumoniae bacteremia
- Systemic inflammatory response syndrome (SIRS)
- Shock
- Encephalopathy
- Acute kidney injury
- Acute respiratory distress syndrome (ARDS)
If untreated, liver abscesses can rupture, cause peritonitis and shock 1. At times the area will get walled off, and chronic pain and discomfort in the right upper quadrant with occasional nighttime fever can follow 1. Complications are also possible after drainage and include liver or kidney failure, intraabdominal lesions, infections, or recurring liver abscesses 65. Other complications include subphrenic abscess, fistula to organs nearby such as pleuropulmonary and hypobranchial fistula, acute pancreatitis, abdominal or hepatic venous thrombosis, and liver pseudoaneurysm 1. Infectious metastatic complications include endophthalmitis or central nervous system septic emboli 1.
It is vitally important to follow up with patients after treatment to prevent and recognize some of these complications 1. Immediate treatment for intraabdominal infection is the best preventive measure for liver abscesses. Four to six weeks of antibiotic therapy post-drainage can prevent almost any complications 1. Antibiotic prophylaxis during chemoembolization or endoscopic retrograde cholangiography help in the prevention of future abscess formation.
Radiographic abnormalities will take longer than clinical or lab abnormalities to go away, as is with many other medical problems. So enough time should elapse before the graphs go back to normal.
Liver abscess diagnosis
It is vital to perform a thorough history and physical examination before choosing any diagnostic measures. This includes but not limited to gathering the patient’s personal history, occupation, travel, place of origin, recent infections, or treatments. Certain risk factors promote the development of liver abscess; such as diabetes, cirrhosis, male gender, elderly, immunocompromised states, and people with proton pump inhibitor usage.
On physical exam, a patient can have hepatomegaly with an enlarged mass and jaundice. Although Charcot’s triad (right upper quadrant pain, jaundice, and fever) is a sign of cholangitis, the physician will need to consider liver abscess as a differential 66. A small number of patients with hepatic abscesses may present in distress or even overt shock (septic shock or anaphylactic shock in case of the hydatiform mole rupture).
In case of Klebsiella liver abscesses (happen mostly in southeast Asia), in addition to the symptoms mentioned above, it also sends septic emboli to eye, meninges, and brain. Therefore symptoms of these organ systems can be present, and it can last after the liver abscess is drained.
In the case of Echinococcus infection, there is an initial asymptomatic infection in a child. Years later some of these people will show clinical symptoms from reactivation of the infection 67. The clinical manifestations depend on the type, size, and site of the cysts present. Small cysts in non-vital organs can go undetected, but large ones in critical locations can cause compressive signs or rupture 68. Usual rate of cyst progression is 1 to 5 centimeters in a year. The liver is affected in two-thirds of cases of Echinococcus infection. Symptoms of compression usually start when the diameter is 10 cm and include biliary colic, cholangitis, obstructive jaundice, portal and venous obstruction, Budd-Chiari syndrome, bronchial fistula, If it ruptures, overt peritonitis or anaphylaxis will be present.
After obtaining medical history and doing physical examination, the next step is to obtain laboratory and diagnostic evidence to determine the cause of the patient’s chief complaint and confirm or rule out a liver abscess. Laboratory tests include a complete blood count (CBC) with differential to identify anemia of chronic disease or neutrophilic leukocytosis, tests for liver function (liver enzymes are usually elevated in half the cases with hypoalbuminemia and elevation of alkaline phosphatase are the most common abnormalities; elevations of transaminase and bilirubin levels are variable), liver synthetic function tests (Prealbumin and INR), alkaline phosphatase (elevated in around 90% of patients), C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and blood cultures to rule out bacteremia 31.
Blood cultures are positive in roughly 50% of cases. Culture of abscess fluid should be the goal in establishing microbiologic diagnosis.
Enzyme immunoassay should be performed to detect Entamoeba histolytica in patients either from endemic areas or who have traveled to endemic areas
If an amebic abscess is suspected (such as in residents or travelers from Southeast Asia, Africa, etc.), stool test or serology for Entamoeba histolytica should be performed. For the hydatid cyst, serology for Echinococcus is needed. Enzyme-linked immunosorbent assay (ELISA) seems to be the most sensitive and specific for Echinococcus. After initial screening with ELISA, confirmatory tests with immunoelectrophoresis and immunoblotting are needed. Serology positivity is dependant on the size and site of the cysts. Liver and bone cysts produce positive serology, whereas lung, brain, eye, splenic, or calcified cysts do not. Calcification is usually a sign of non-viable material.
Many radiographical tests can be performed, and certain tests should take precedence. It is important to limit a patient’s exposure to unnecessary radiation and tests. There can be findings in the chest x-ray, pointing to this diagnosis, such as basilar atelectasis, right hemidiaphragm elevation, right pleural effusion over the liver and amorphous gas accumulation in the liver. However, the initial test of choice is an abdominal ultrasound (sensitivity of 80% to 90%), which shows hyper or hypoechoic lesions with occasional debris or septation 69. Computed tomography (CT) with contrast is the next step, and slightly more sensitive (sensitivity of 95% to 100%). Computed tomography (CT) is superior in its ability to detect lesions less than 1 cm. Computed tomography (CT) with contrast also enables evaluation for an underlying concurrent pathology throughout the abdomen and pelvis. Indium-labeled white blood cell (WBC) scans are somewhat more sensitive in this regard. Lesions on CT evaluation are well-demarcated areas hypodense to the surrounding hepatic parenchyma. Peripheral enhancement is seen when intravenous (IV) contrast is administered. Gas can be seen in as many as 20% of lesions. Rim enhancement and edema are not typical but very specific for infection.
The ultrasound or CT is then followed by needle aspiration under guidance to identify the exact causative organism, which is essential for diagnostic as well as therapeutic purposes (small cysts) 70. Technetium scan is another test with an 80% sensitivity (less than CT), which is 50-80% for gallium and 90% for indium 71, 72. If inner cyst walls are in-folded (separation of hydatid membrane from the wall of the cyst) during the ultrasound, hydatid disease is more likely.
Stains and cultures should be obtained from the direct aspirate. Drains that are in place will get contaminated with skin flora and are not accurate for cultural purposes. Stains and cultures should be done for aerobes and anaerobes (special handling might be needed), but occasionally more specific cultures need to be done, such as fungi, Mycobacterium, Entamoeba histolytica, and parasites.
Diagnosis is confirmed when there are cystic or solid areas in the liver that, upon aspiration, will yield fluid with positive cultures. It is important to obtain these tests quickly and start treatment because of the high complication rate if left untreated.
Percutaneous needle aspiration
Under CT or ultrasonographic guidance, needle aspiration of cavity material can be performed. Needle aspiration enables rapid recovery of material for microbiologic and pathologic evaluation. It can be performed with the initial diagnostic procedure.
Percutaneous catheter drainage
Percutaneous drainage has become the standard of care and should be the first intervention considered for small cysts. Advantages include reduced costs, recovery time, and postprocedure recovery rate; it eliminates the need for general anesthesia. This also allows for gradual, controlled drainage. For cysts larger than 5 cm, ruptured cysts, and multiloculated cysts, surgical drainage is generally recommended over percutaneous intervention.
A catheter is placed under ultrasonographic or CT guidance via the Seldinger or trocar techniques. The catheter is flushed daily until output is less than 10 mL/day or cavity collapse is documented by serial CT.
Multiple abscesses have been drained successfully by this method. Failure to respond to catheter drainage is the main reported complication and is also an indication for surgical intervention. Other complications reported (rarely) are bleeding at the catheter site, perforation of hollow viscus, and peritonitis from intraperitoneal spillage of cavity fluid.
Contraindications include coagulopathy; a difficult access path to the cavity; peritonitis; and/or a complicated, multiloculated, thick-walled abscess with viscous pus.
Laboratory studies
Laboratory tests include a complete blood count (CBC) with differential, tests for hepatocellular injury (AST, ALT usually elevated in half the cases), liver synthetic function tests (Prealbumin and INR), alkaline phosphatase (elevated around 90%), C-reactive protein, sedimentation rate, and blood cultures to rule out bacteremia 73.
If an amebic abscess is suspected (residents or travelers from Southeast Asia or Africa), stool test or serology for Entamoeba histolytica should be performed. For hydatid cyst, serology for Echinococcus is needed. Enzyme-linked immunosorbent assay (ELISA) seems to be the most sensitive and specific for Echinococcus. After initial screening with ELISA, confirmatory tests with immunoelectrophoresis and immunoblotting is needed. Serology positivity is dependant on size and site of the cysts. Liver and bone cysts produce positive serology whereas lung, brain, eye, splenic or calcified cysts do not. Calcification is usually a sign of non-viable material.
Many radiographical tests can be performed, and certain tests should take precedence. It is important to limit a patient’s exposure to unnecessary radiation and tests. There can be findings in the chest x-ray pointing to this diagnosis such as elevated hemidiaphragm on the right and pleural effusion over the liver. However, the initial test of choice is an abdominal ultrasound (US) which shows hyper or hypoechoic lesions with occasional debris or septation. Computed tomography (CT) with contrast is the next step, and slightly more sensitive. Rim enhancement and edema are not typical but very specific for infection. The ultrasound or CT is followed by needle aspiration under guidance to identify the exact causative organism which is essential for diagnostic as well as therapeutic purposes (small cysts) 74. Technetium scan is another test with an 80% sensitivity (less than CT); 50-80% for gallium and 90% for indium 75. If inner cyst walls are in-folded (separation of hydatid membrane from the wall of the cyst) during the ultrasound, hydatid disease is more likely.
Stains and cultures should be obtained from direct aspirate. Drains that are in place will get contaminated with skin flora and are not accurate for culture purposes. Stains and cultures should be done for aerobes and anaerobes (special handling might be needed), but occasionally more specific cultures need to be done such as fungi, Mycobacterium, Entamoeba histolytica, and parasites.
Diagnosis is confirmed when there are cystic or solid areas in the liver that upon aspiration will yield fluid with positive cultures. It is important to obtain these tests quickly and start treatment because of the high complication rate if left untreated.
Liver abscess differential diagnosis
Liver abscess manifests with right upper quadrant pain, fever, and hepatitis. Many liver and non-liver ailments are in its differential diagnoses, such as:
- Viral hepatitis
- Cholecystitis
- Cholangitis
- Right lower lobe pneumonia
- Appendicitis
- Necrotic liver masses
- Acute gastritis
- Biliary disease
- Hepatocellular Carcinoma (HCC)
- Hydatid Cysts
- Parapneumonic Pleural Effusions and Empyema Thoracis.
Other causes of hepatitis such as autoimmune, drug-induced and acetaminophen (paracetamol) toxicity can be mistaken although they are usually not painful.
Liver abscess treatment
The management of liver abscesses varies on the basis of the organism involved. In general, liver abscesses require medical management with antibiotics or amebicides, often in addition to percutaneous aspiration or percutaneous catheter drainage 4. Pyogenic liver abscesses almost always require both antibiotics and source control through aspiration or drainage. Antibiotic of choice should be tailored to the specific bacteria isolated, although infections are often polymicrobial 14. The most commonly implicated aerobic bacteria include E. coli, Klebsiella species, Streptococcus species, and Staphylococcus aureus 76. The appropriate empirical antibiotic regimen includes a third-generation cephalosporin with oral metronidazole, with the latter providing anerobic coverage, or a beta-lactam/beta-lactam inhibitor combination of antibiotics such as piperacillin/tazobactam 76. A fluoroquinolone with metronidazole or carbapenem can be used in those with a penicillin allergy 76. Antibiotics should be given for 2 to 6 weeks and should always be narrowed once cultures provide further information on specific organisms involved 4, 17. Only pyogenic liver abscesses less than 3 cm should be managed with antibiotics alone 76. Those liver abscesses measuring 3 to 5 cm can be aspirated, whereas those more than 5 cm require catheter drainage 76. Multiple aspirations are often needed, whereas definitive management is typically achieved with percutaneous catheter drainage. If liver abscesses are not responsive to antibiotic therapy and are not amenable to drainage, or are multiple in nature or there is evidence of rupture, liver resection should be considered 4, 17.
Amebic liver abscess treatment
Management of amebic liver abscess comprises medical management, radiological drainage, and surgical management. Most uncomplicated amebic liver abscesses can be treated successfully with conservative management, such as with amebicidal drug therapy alone 77. Use tissue amebicides to eradicate the invasive trophozoite forms in the liver. Tissue amebicides such as nitroimidazoles form the mainstay of management of all patients with amebic liver abscess 4. In general, metronidazole, tinidazole, emetine, and dehydroemetine are active in invaded tissues; chloroquine is active only in the liver; tetracycline acts on the bowel wall; and diloxanide furoate, paromomycin, and iodoquinol are luminal agents only. Oral or intravenous (IV) administration (in patients unable to take orally [PO]) of metronidazole results in resolution of fever, toxemia, and pain in 80% of 90% of patients with uncomplicated amebic liver abscess within 48 to 72 hours of treatment 4. Tinidazole is better tolerated and has the advantage of shorter duration of treatment. Other options include nitazoxanide, which has an advantage of being both tissue and luminal amebicide.
The treatment with tissue amebicides should be followed with luminal amoebicidal agents to eradicate the luminal amebae and to prevent subsequent tissue invasion and spread of the infection through cyst 78. Failure to use luminal amebicides agents can lead to relapse of infection in approximately 10% of patients.
Table 1. Drugs used in the management of amebic liver abscess
| Drugs | Dose and Duration | Adverse Events |
|---|---|---|
| Tissue amoebicidal drugs | ||
| Metronidazole | 800 mg three times a day PO or 500 mg IV three times a day for 7‐10 days | Gastrointestinal: anorexia, nausea, vomiting, metallic taste |
| Neurological: dizziness, peripheral neuropathy, seizures | ||
| Tinidazole | 1.2 g PO per day for 7 days | Gastrointestinal‐like metronidazole |
| Luminal amoebicidal drugs | ||
| Diloxanide furoate | 500 mg three times a day for 20 days | Gastrointestinal: nausea, vomiting |
| Paromomycin | 30 mg/kg for 10 days (in 3 divided doses) | Gastrointestinal: diarrhea, nausea |
| Tissue plus luminal amoebicidal drug | ||
| Nitazoxanide | 500 mg twice a day for 10 days | Gastrointestinal: nausea, vomiting |
Metronidazole
Metronidazole remains the drug of choice for amebic liver abscess 79. Metronidazole enters the protozoa by passive diffusion and is converted to reactive cytotoxic nitroradicals by reduced ferredoxin or flavodoxin. Tinidazole, another nitroimidazole closely related to metronidazole, was approved for the treatment of amebic liver abscess and invasive amebiasis 79. Tinidazole is well tolerated by patients. Tinidazole may be administered once daily and appears to be at least as effective as metronidazole, with a clinical cure rate of more than 90% 79.
Metronidazole, 750 mg 3 times a day orally for 10 days, was reported to be curative in 90% of patients with amebic liver abscess 79. Metronidazole is also available for intravenous administration for those patients who are unable to take the medication by the oral route.
Resolution of symptoms is fairly rapid and is observed within 3 days in most patients in the United States. In endemic areas outside the United States, it takes relatively longer to resolve the symptoms because the abscesses are quite large or multiple by the time patients seek medical attention 79.
In vivo Entamoeba histolytica resistance to metronidazole has not been reported. Nevertheless, in vitro studies have shown an association between metronidazole resistance and decreased expression of ferredoxin 1 and flavodoxin and increased expression of iron-containing superoxide dismutase and peroxiredoxin in Entamoeba histolytica.
Usual adverse effects of metronidazole include nausea, headache, and metallic taste. Abdominal cramps, vomiting, diarrhea, and dizziness also may occur. Dark urine caused by a metabolite of the drug may be observed.
Other considerations
Other considerations include the following:
- No randomized controlled trials exist that demonstrate the benefits of combination therapy over monotherapy.
- Outside the United States, other closely related amebicidal agents, such as secnidazole or ornidazole, can be substituted in appropriate dosages. These drugs are not available in the United States.
- Chloroquine phosphate may be substituted or added in the event of failure of resolution of clinical symptoms with metronidazole or another nitroimidazole within 5 days, or intolerance to metronidazole or a nitroimidazole. Chloroquine has the disadvantage of being associated with higher relapse rates than nitroimidazoles. Adverse effects include gastrointestinal upset, headache, dizziness, and blurred vision. Retinopathy does not occur at the dose used for amebic liver abscess.
- Emetine or dehydroemetine has a direct lethal action on the trophozoites of Entamoeba histolytica. These agents are very toxic and, therefore, should be used only as a second-line therapy. Their toxicity includes cardiac arrhythmias, precordial pain, muscle weakness, vomiting, and diarrhea. Dehydroemetine is less toxic than emetine.
Administer a luminal amebicidal agent to eradicate the intestinal carriage after the amebic liver abscess has been treated with one of the tissue amebicides noted above. Failure to use luminal agents can lead to relapse of infection in approximately 10% of patients. Luminal agents with proven efficacy include diloxanide furoate, iodoquinol, and paromomycin. Note the following:
- Diloxanide furoate is free of major adverse effects. The most common adverse effect is flatulence and occasional gastrointestinal upset.
- Iodoquinol (diiodohydroxyquin) rarely causes abdominal pain, diarrhea, or rash. A structurally related diiodohydroxyquin caused subacute myelopticoneuropathy and is obsolete now.
- Although paromomycin may occasionally cause nausea, abdominal cramps, or diarrhea, it is the preferred luminal amebicidal.
Drainage of amebic liver abscess
The indications for drainage of liver abscess together with medical management are 4:
- Left lobe liver abscess,
- Liver abscess with thin rim of hepatic parenchyma (<10 mm) around it,
- Multiple liver abscesses,
- Impending rupture recognized on imaging, and
- Nonresponse to medical therapy after 3 to 5 days.
In the absence of these high‐risk features, the evidence for upfront drainage is controversial 4. Faster resolution of clinical and biochemical features is seen in some but not in other randomized trials comparing the strategy of combination of drainage and medical management with that of medical management alone 4. A recent systematic review found a combination strategy to be effective in reducing the abdominal pain and local tenderness, but not in resolution of fever, healing of abscess, and length of hospital stay, with benefits limited to abscesses of more than 5 cm 80. Hence routine drainage of liver abscess is not recommended in patients with amebic liver abscess but may be used in selected patients with liver abscess size greater than 5 cm 4. Percutaneous catheter drainage (PCD) is preferred over percutaneous needle aspiration, particularly in larger abscess (>10 cm), subcapsular location, high risk for rupture, and if superinfected. Even for complications such as rupture into peritoneum, there is evidence that conservative management with percutaneous catheter drainage results in better outcomes than surgery 81. Catheter removal is usually recommended when the drainage output is less than 10 mL/day 82. Duration of catheter removal may vary; however, earlier removal is not associated with a higher healing rate 83. The higher mortality associated with surgery combined with the widespread availability of image‐guided drainage has limited the role of surgery in the management of amebic liver abscess. Surgery can be considered in those with no response to appropriate antibiotics and percutaneous catheter drainage. Clinical and biochemical resolution occurs rapidly in patients with amebic liver abscess with optimal management. Radiological resolution is often delayed and does not warrant additional therapy. Relapses are uncommon in amebic liver abscess 84.
Pyogenic liver abscess treatment
Patients with pyogenic liver abscess usually have more pronounced systemic features with multiple liver abscess on imaging compared with those with amebic liver abscess. Unlike amebic liver abscess, the principles of treatment of pyogenic liver abscess involve drainage of abscess, use of appropriate antibiotics, and control of primary source of infection 17. An untreated liver abscess is nearly uniformly fatal as a result of complications that include sepsis, empyema, or peritonitis from rupture into the pleural or peritoneal spaces, and retroperitoneal extension.
Percutaneous or surgical drainage of the liver abscess and antibiotic treatment are the cornerstones of pyogenic liver abscess treatment. Liver abscess drainage is needed and can be done under ultrasonography or CT guidance 32, 33, 34. Percutaneous needle aspiration (at times repeatedly) might be all that is required for liver abscesses less than 5 cm, but a catheter placement might be warranted if the liver abscess diameter is more than 5 cm 35, 36. Percutaneous drainage with catheter placement is probably the most successful procedure for larger than 5 cm liver abscesses 37. Laparoscopic drainage is also used at times. Surgery should be done for peritonitis, thick wall abscesses, ruptured abscess, multiple large abscesses, and previously failed drainage procedures 1. An operation is performed either by a transperitoneal approach or by the posterior transpleural approach 1. The former approach drains the abscess and allows for the exploration of undetected ulcers, while the latter is better for posterior abscesses 1. Size, location, and stage help determine a successful treatment plan. When previous biliary procedures have been done, endoscopic retrograde cholangiopancreatography (ERCP) drainage might be used 38. Undrained liver abscesses may cause sepsis, peritonitis, and empyema.
Empiric antibiotic coverage is essential when the organism is unknown. The antibiotics should cover Enterobacteriaceae, anaerobes, streptococci, enterococci, and Entamoeba histolytica 1. Such antibiotic regimens include cephalosporins plus metronidazole, Beta-lactam Beta-Lactamase inhibitor plus metronidazole, or synthetic penicillins plus aminoglycosides and metronidazole 1. Alternatively, fluoroquinolones or carbapenems can be substituted for cephalosporins or penicillins in case of allergy or unavailability. Metronidazole should cover Entamoeba histolytica 1. The duration of treatment varies but is usually from two to six weeks 1. After initial intravenous treatment, the oral route can be used safely in most cases to complete the course 1. Culture results help narrow down the organism, so empiric treatment is no longer needed, as it can lead to antibiotic resistance. Anaerobes are hard to culture, so sometimes they should be treated for the entire course empirically. For stable patients, antibiotics can be given post-drainage to increase culture yield for proper treatment. Empiric antifungal treatment is crucial in immunosuppressed patients with a risk for chronic disseminated fungemia 1.
Antibiotic therapy as a sole treatment for liver abscess is not routinely advocated, though it has been successful in a few reported cases. In pyogenic liver abscess management, antibiotic therapy without drainage has a high mortality rate 85. In a 35-Year Olmsted County Study 5, of the 14 patients (20%) who did not undergo aspiration, 5 (36%) died within 3 months of pyogenic liver abscess diagnosis. Better outcome after percutaneous aspiration of the abscess may be related to better source control as well as to more accurate identification of the causative organism and determination of antibiotic susceptibility 5.
Antibiotic therapy alone may be the only alternative in patients too ill to undergo invasive procedures or in those with multiple abscesses not amenable to percutaneous or surgical drainage 1, 39. In these instances, patients are likely to require many months of antimicrobial therapy with serial imaging and close monitoring for associated complications.
If the source is Echinococcus tapeworms (Echinococcus granulosus, Echinococcus multilocularis, Echinococcus oligarthrus or Echinococcus vogeli), treatment includes a benzimidazole, such as albendazole 1. This therapy may last for several years 1. Although most cases are uncomplicated and can be treated with an antiparasitic drug, complicated cases must be treated delicately. In most complicated cases, drainage is necessary. Surgeons must take caution to inject the hydatid cysts before draining them, as sometimes the rupture can cause the patient to go into shock rapidly 1.
In a study by Abbas 40, the mean duration of hospital stay for those with pyogenic liver abscesses was 13.6 days. Antibiotic therapy used for them was approximately 34.7 days. One patient expired. On the other hand, patients with amebic liver abscesses had a mean hospital stay of approximately 7.7 days, with a mean duration of treatment of 11.8 days, where all patients were cured 40.
Surgical care
Surgical drainage was the standard of care until the introduction of percutaneous drainage techniques in the mid-1970s. With the refinement of image-guided techniques, percutaneous drainage and aspiration have become the standard of care for pyogenic liver abscesses 86.
Current indications for the surgical treatment of pyogenic liver abscess are for the treatment of underlying intra-abdominal processes, including signs of peritonitis; existence of a known abdominal surgical pathology (eg, diverticular abscess); failure of previous drainage attempts; and the presence of a complicated, multiloculated, thick-walled abscess with viscous pus 86.
Shock with multisystem organ failure is a contraindication for surgery 86.
Open surgery can be performed by either of the following two approaches 86:
- A transperitoneal approach allows for abscess drainage and abdominal exploration to identify previously undetected abscesses and the location of an etiologic source
- For high posterior lesions, a posterior transpleural approach can be used; although this affords easier access to the abscess, the identification of multiple lesions or a concurrent intra-abdominal pathology is lost
A laparoscopic approach is also commonly used in select cases. This minimally invasive approach affords the opportunity to explore the entire abdomen and to significantly reduce patient morbidity. A growing literature is defining the optimal population for this mode of intervention.
A retrospective chart review compared surgery versus percutaneous drainage for liver abscesses greater than 5 cm. Morbidity was comparable for the two procedures, but those treated with surgery had fewer secondary procedures and fewer treatment failures.
Postoperative complications are not uncommon and include recurrent pyogenic liver abscess, intra-abdominal abscess, hepatic or renal failure, and wound infection.
Liver abscess prognosis
Liver abscess prognosis is highly variable, depending not only on the organism involved and size of the abscess but also on the comorbidities present. Despite the more aggressive approach to liver abscess treatment, the mortality (dying) from liver abscess remained at 60% to 80% 23, 87. Traditionally liver abscess has been regarded as a high-morbidity disease, routinely managed by open drainage, with mortality rates between 9% and 80% 88, 89, 90, 91, 92, 93, 94. The mortality rate is higher in elderly, ICU admissions, shock, cancer, fungal infections, cirrhosis, chronic renal failure, acute respiratory failure, severe disease, and biliary origin of an abscess. Escherichia coli liver abscesses carry a significant mortality rate, as high as 26.4% in 1 study 95. However, the development of new radiologic techniques, the improvement in microbiologic identification, and the advancement of drainage techniques, as well as improved supportive care, have reduced mortality (dying) from liver abscess to 5 to 30%; yet, the prevalence of liver abscess has remained relatively unchanged 6. Untreated, pyogenic liver abscess, the most common liver abscess in United States caused by several different types of microorganisms, remains fatal as a result of complications that include sepsis, empyema, or peritonitis from rupture into the pleural or peritoneal spaces, and retroperitoneal extension 6. With timely administration of antibiotics and drainage procedures, mortality currently occurs in 5% to 30% of cases. The most common causes of death include sepsis, multi-organ failure, and liver failure 96. Liver abscess recurrence is frequent in patients who present with a biliary tract disease 97.
Indicators of a poor prognosis have been described since 1938 and include multiple liver abscesses, underlying cancer, severity of underlying medical conditions, presence of complications, and delay in diagnosis 96.
Indicators of a poor prognosis in amebic liver abscess include:
- Encephalopathy
- Jaundice
- Serum bilirubin greater than 3.5 mg/dL
- Serum albumin less than 2 g/dL (hypoalbuminemia)
- Ultrasound findings
- Large volume liver abscess
- Multiple liver abscesses
- Underlying chronic liver disease
An underlying malignant etiology and an Acute Physiology and Chronic Health Evaluation (APACHE II) score greater than 9 increases the relative mortality by 6.3-fold and 6.8-fold, respectively.
Chen et al 98 examined prognostic factors for elderly patients with pyogenic liver abscess. Results from the study, which included 118 patients aged 65 years or older and 221 patients below age 65 years, indicated that age and an Acute Physiology and Chronic Health Evaluation (APACHE II) score of 15 or greater at hospital admission were risk factors for mortality. The evidence ultimately suggested that outcomes for older patients with pyogenic liver abscess are on a par with those for younger patients. The investigators also found that in the younger patient group, there was greater frequency of males suffering from alcoholism, a cryptogenic abscess, and Klebsiella pneumoniae infection 98.
- Akhondi H, Sabih DE. Liver Abscess. [Updated 2023 Jul 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538230[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Khim G, Em S, Mo S, Townell N. Liver abscess: diagnostic and management issues found in the low resource setting. Br Med Bull. 2019 Dec 11;132(1):45-52. doi: 10.1093/bmb/ldz032[↩][↩]
- Hepatic abscess. https://radiopaedia.org/articles/hepatic-abscess-1?lang=us[↩]
- Sharma S, Ahuja V. Liver Abscess: Complications and Treatment. Clin Liver Dis (Hoboken). 2021 Jul 16;18(3):122-126. doi: 10.1002/cld.1128[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Sharma A, Mukewar S, Mara KC, Dierkhising RA, Kamath PS, Cummins N: Epidemiologic factors, clinical presentation, causes, and outcomes of liver abscess: a 35-Year olmsted county study. Mayo Clin Proc. 2018, 2:16-25. 10.1016/j.mayocpiqo.2018.01.002[↩][↩][↩][↩][↩]
- Liver Abscess. https://emedicine.medscape.com/article/188802-overview[↩][↩][↩]
- Othman N, Mohamed Z, Yahya MM, Leow VM, Lim BH, Noordin R. Entamoeba histolytica antigenic protein detected in pus aspirates from patients with amoebic liver abscess. Exp Parasitol. 2013 Aug;134(4):504-10. doi: 10.1016/j.exppara.2013.05.001[↩]
- Portunato F, Bartalucci C, Vena A, Giacobbe DR, Porcile E, Montanelli P, Piol N, Centanaro M, Andorno E, Bassetti M. Amoebic Liver Abscess: Potential Application of New Diagnostic Techniques for an Old Pathogen. Infect Dis Ther. 2024 Mar;13(3):625-632. doi: 10.1007/s40121-024-00934-1[↩][↩][↩][↩]
- Kantor M, et al. Entamoeba histolytica : updates in clinical manifestation, pathogenesis, and vaccine development. Can J Gastroenterol Hepatol. 2018;2018:1–6. doi: 10.1155/2018/4601420[↩]
- Shirley DT, Farr L, Watanabe K, Moonah S. A Review of the Global Burden, New Diagnostics, and Current Therapeutics for Amebiasis. Open Forum Infect Dis. 2018 Jul 5;5(7):ofy161. doi: 10.1093/ofid/ofy161[↩]
- Carrero JC, Reyes-López M, Serrano-Luna J, Shibayama M, Unzueta J, León-Sicairos N, de la Garza M. Intestinal amoebiasis: 160 years of its first detection and still remains as a health problem in developing countries. Int J Med Microbiol. 2020 Jan;310(1):151358. doi: 10.1016/j.ijmm.2019.151358[↩]
- Fu B, Wang J, Fu X. A rare case of extraintestinal amebiasis. BMC Infect Dis. 2022 Apr 11;22(1):364. doi: 10.1186/s12879-022-07348-9[↩]
- Nespola B, Betz V, Brunet J, Gagnard JC, Krummel Y, Hansmann Y, Hannedouche T, Christmann D, Pfaff AW, Filisetti D, Pesson B, Abou-Bacar A, Candolfi E. First case of amebic liver abscess 22 years after the first occurrence. Parasite. 2015;22:20. doi: 10.1051/parasite/2015020[↩]
- Roediger R, Lisker-Melman M. Pyogenic and Amebic Infections of the Liver. Gastroenterol Clin North Am. 2020 Jun;49(2):361-377. doi: 10.1016/j.gtc.2020.01.013[↩][↩]
- Cordel H, Prendki V, Madec Y, Houze S, Paris L, Bourée P, Caumes E, Matheron S, Bouchaud O; ALA Study Group. Imported amoebic liver abscess in France. PLoS Negl Trop Dis. 2013 Aug 8;7(8):e2333. doi: 10.1371/journal.pntd.0002333[↩]
- Brisse S, Fevre C, Passet V, Issenhuth-Jeanjean S, Tournebize R, Diancourt L, Grimont P. Virulent clones of Klebsiella pneumoniae: identification and evolutionary scenario based on genomic and phenotypic characterization. PLoS One. 2009;4(3):e4982. doi: 10.1371/journal.pone.0004982[↩][↩][↩]
- Lardière-Deguelte S, Ragot E, Amroun K, Piardi T, Dokmak S, Bruno O, Appere F, Sibert A, Hoeffel C, Sommacale D, Kianmanesh R. Hepatic abscess: Diagnosis and management. J Visc Surg. 2015 Sep;152(4):231-43. doi: 10.1016/j.jviscsurg.2015.01.013[↩][↩][↩][↩][↩][↩]
- Alshammary, Shadi Abdullah; Boumarah, Dhuha Nahar. Hepatic Abscess in Inflammatory Bowel Disease: A Systematic Scoping Review of an Overlooked Entity. Saudi Journal of Medicine & Medical Sciences 11(4):p 267-274, Oct–Dec 2023. DOI: 10.4103/sjmms.sjmms_545_22 [↩][↩]
- Jain AG, FaisalUddin M, Gllava I, Gordon D, Guan J. A Rare Case of Crohn’s Disease Manifesting as a Large Liver Abscess. Cureus. 2018 Dec;10(12):e3758. DOI: 10.7759/cureus.3758 https://www.cureus.com/articles/16580-a-rare-case-of-crohns-disease-manifesting-as-a-large-liver-abscess#![↩][↩][↩]
- Jindal A, Pandey A, Sharma MK, Mukund A, Vijayaraghavan R, Arora V, Shasthry SM, Choudhary A, Sarin SK. Management Practices and Predictors of Outcome of Liver Abscess in Adults: A Series of 1630 Patients from a Liver Unit. J Clin Exp Hepatol. 2021 May-Jun;11(3):312-320. doi: 10.1016/j.jceh.2020.10.002[↩][↩]
- Joshi G, Crawford KA, Hanna TN, Herr KD, Dahiya N, Menias CO. US of Right Upper Quadrant Pain in the Emergency Department: Diagnosing beyond Gallbladder and Biliary Disease. Radiographics. 2018 May-Jun;38(3):766-793. doi: 10.1148/rg.2018170149[↩]
- Chadwick M, Shamban L, Neumann M. Pyogenic Liver Abscess with No Predisposing Risk Factors. Case Rep Gastrointest Med. 2018 Sep 4;2018:9509356. doi: 10.1155/2018/9509356[↩][↩][↩][↩][↩][↩]
- Pearce NW, Knight R, Irving H, Menon K, Prasad KR, Pollard SG, Lodge JP, Toogood GJ. Non-operative management of pyogenic liver abscess. HPB (Oxford). 2003;5(2):91-5. doi: 10.1080/13651820310001126[↩][↩][↩]
- Mølle I, Thulstrup AM, Jepsen P, Sørensen HT, Vilstrup H. Liver cirrhosis is risk factor for pyogenic liver abscesses. BMJ. 2001 Jul 7;323(7303):52-3. https://pmc.ncbi.nlm.nih.gov/articles/PMC1120686[↩][↩]
- Park HJ, Kim SH, Jang KM, Lee SJ, Park MJ, Choi D. Differentiating hepatic abscess from malignant mimickers: value of diffusion-weighted imaging with an emphasis on the periphery of the lesion. J Magn Reson Imaging. 2013 Dec;38(6):1333-41. doi: 10.1002/jmri.24112[↩][↩]
- Akhondi H, Sabih DE. Liver Abscess. [Updated 2019 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538230[↩][↩][↩]
- Singh S, Chaudhary P, Saxena N, Khandelwal S, Poddar DD, Biswal UC. Treatment of liver abscess: prospective randomized comparison of catheter drainage and needle aspiration. Ann Gastroenterol. 2013;26(4):332–339. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3959473[↩]
- Lardière-Deguelte S, Ragot E, Armoun K, Piardi T, Dokmak S, Bruno O, et al. Hepatic abscess: diagnosis and management. J Visc Surg. 2015;152:231–243. doi: 10.1016/j.jviscsurg.2015.01.013[↩]
- Kumar V, Abbas AK, Fausto N et-al. Robbins and Cotran pathologic basis of disease. W B Saunders Co. (2005) ISBN:0721601871[↩]
- Kaplan GG, Gregson DB, Laupland KB. Population-based study of the epidemiology of and the risk factors for pyogenic liver abscess. Clin. Gastroenterol. Hepatol. 2004 Nov;2(11):1032-8.[↩]
- Rahimian J, Wilson T, Oram V, Holzman RS. Pyogenic liver abscess: recent trends in etiology and mortality. Clin Infect Dis. 2004 Dec 1;39(11):1654-9. doi: 10.1086/425616[↩][↩]
- vanSonnenberg E, Wittich GR, Goodacre BW, Casola G, D’Agostino HB. Percutaneous abscess drainage: update. World J Surg. 2001 Mar;25(3):362-9; discussion 370-2. doi: 10.1007/s002680020386[↩][↩]
- Giorgio A, de Stefano G, Di Sarno A, Liorre G, Ferraioli G. Percutaneous needle aspiration of multiple pyogenic abscesses of the liver: 13-year single-center experience. AJR Am J Roentgenol. 2006 Dec;187(6):1585-90. doi: 10.2214/AJR.05.1104[↩][↩]
- Ferraioli G, Garlaschelli A, Zanaboni D, Gulizia R, Brunetti E, Tinozzi FP, Cammà C, Filice C. Percutaneous and surgical treatment of pyogenic liver abscesses: observation over a 21-year period in 148 patients. Dig Liver Dis. 2008 Aug;40(8):690-6. doi: 10.1016/j.dld.2008.01.016[↩][↩]
- Zerem E, Hadzic A. Sonographically guided percutaneous catheter drainage versus needle aspiration in the management of pyogenic liver abscess. AJR Am J Roentgenol. 2007 Sep;189(3):W138-42. doi: 10.2214/AJR.07.2173[↩][↩]
- Ch Yu S, Hg Lo R, Kan PS, Metreweli C. Pyogenic liver abscess: treatment with needle aspiration. Clin Radiol. 1997 Dec;52(12):912-6. doi: 10.1016/s0009-9260(97)80223-1[↩][↩]
- Cai YL, Xiong XZ, Lu J, Cheng Y, Yang C, Lin YX, Zhang J, Cheng NS. Percutaneous needle aspiration versus catheter drainage in the management of liver abscess: a systematic review and meta-analysis. HPB (Oxford). 2015 Mar;17(3):195-201. doi: 10.1111/hpb.12332[↩][↩]
- Sersté T, Bourgeois N, Vanden Eynden F, Coppens E, Devière J, Le Moine O. Endoscopic drainage of pyogenic liver abscesses with suspected biliary origin. Am J Gastroenterol. 2007 Jun;102(6):1209-15. doi: 10.1111/j.1572-0241.2007.01140.x[↩][↩]
- Liver Abscess Treatment & Management. https://emedicine.medscape.com/article/188802-treatment[↩][↩]
- Abbas MT, Khan FY, Muhsin SA, Al-Dehwe B, Abukamar M, Elzouki AN. Epidemiology, Clinical Features and Outcome of Liver Abscess: A single Reference Center Experience in Qatar. Oman Med J. 2014 Jul;29(4):260-3. doi: 10.5001/omj.2014.69[↩][↩][↩][↩]
- Pyogenic liver abscess. https://radiopaedia.org/cases/pyogenic-liver-abscess-2[↩]
- Bory S, Daily F, Khim G, Letchford J, Sok S, Kol H, Seang Lak M, Tuseo L, Vibol C, Oeng S, Turner P. A Report from the Cambodia Training Event for Awareness of Melioidosis (C-TEAM), October 2017. Trop Med Infect Dis. 2018 Feb 23;3(1):23. doi: 10.3390/tropicalmed3010023[↩]
- Maude RR, Vatcharapreechasakul T, Ariyaprasert P, Maude RJ, Hongsuwan M, Yuentrakul P, Limmathurotsakul D, Koh GC, Chaowagul W, Day NP, Peacock SJ. Prospective observational study of the frequency and features of intra-abdominal abscesses in patients with melioidosis in northeast Thailand. Trans R Soc Trop Med Hyg. 2012 Oct;106(10):629-31. doi: 10.1016/j.trstmh.2012.05.007[↩][↩]
- Nguyen HVN, Smith ME, Hayoun MA. Glanders and Melioidosis. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448110[↩]
- Meumann, E.M., Limmathurotsakul, D., Dunachie, S.J. et al. Burkholderia pseudomallei and melioidosis. Nat Rev Microbiol 22, 155–169 (2024). https://doi.org/10.1038/s41579-023-00972-5[↩]
- Ganeshalingam V, Kaestli M, Norton RE, Gassiep I. The effect of climate on melioidosis incidence in Townsville, Australia: a dry tropical region. Environ Health Prev Med. 2023;28:33. doi: 10.1265/ehpm.22-00177[↩]
- Shukla T, Smith S, Johnstone K, Donald P, Hanson J. The characteristics and clinical course of patients with melioidosis and cancer. PLoS Negl Trop Dis. 2024 Oct 25;18(10):e0012631. doi: 10.1371/journal.pntd.0012631[↩]
- Weerasinghe NP, Herath HMM, Liyanage TMU. Isolated septic arthritis of hip joint: a rare presentation of melioidosis. A case report. BMC Res Notes. 2018 Jan 19;11(1):50. doi: 10.1186/s13104-018-3171-6[↩]
- Wiersinga, W., van der Poll, T., White, N. et al. Melioidosis: insights into the pathogenicity of Burkholderia pseudomallei. Nat Rev Microbiol 4, 272–282 (2006). https://doi.org/10.1038/nrmicro1385[↩]
- This Germ Can Live Decades In Distilled Water, Kill Humans In 48 Hours. https://www.npr.org/sections/goatsandsoda/2016/01/11/462416728/this-germ-can-live-decades-in-distilled-water-kill-humans-in-48-hours[↩]
- Cheng AC, Currie BJ. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005 Apr;18(2):383-416. doi: 10.1128/CMR.18.2.383-416.2005. Erratum in: Clin Microbiol Rev. 2007 Jul;20(3):533. Dosage error in article text.[↩]
- White NJ. Melioidosis. Lancet. 2003 May 17;361(9370):1715-22. doi: 10.1016/s0140-6736(03)13374-0[↩]
- Rammaert B, Beauté J, Borand L, Hem S, Buchy P, Goyet S, Overtoom R, Angebault C, Te V, Try PL, Mayaud C, Vong S, Guillard B. Pulmonary melioidosis in Cambodia: a prospective study. BMC Infect Dis. 2011 May 14;11:126. doi: 10.1186/1471-2334-11-126[↩]
- Suputtamongkol Y, Chaowagul W, Chetchotisakd P, Lertpatanasuwun N, Intaranongpai S, Ruchutrakool T, Budhsarawong D, Mootsikapun P, Wuthiekanun V, Teerawatasook N, Lulitanond A. Risk factors for melioidosis and bacteremic melioidosis. Clin Infect Dis. 1999 Aug;29(2):408-13. doi: 10.1086/520223[↩]
- Melioidosis. https://www.cdc.gov/melioidosis/about[↩][↩][↩]
- Liver Abscess Pathophysiology. https://emedicine.medscape.com/article/188802-overview#a5[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Lin YT, Liu CJ, Chen TJ, Chen TL, Yeh YC, Wu HS, Tseng CP, Wang FD, Tzeng CH, Fung CP. Pyogenic liver abscess as the initial manifestation of underlying hepatocellular carcinoma. Am J Med. 2011 Dec;124(12):1158-64. doi: 10.1016/j.amjmed.2011.08.012[↩]
- Liver Abscess Etiology. https://emedicine.medscape.com/article/188802-overview#a7[↩][↩][↩][↩][↩]
- Krige JE, Beckingham IJ. ABC of diseases of liver, pancreas, and biliary system. BMJ. 2001 Mar 3;322(7285):537-40. doi: 10.1136/bmj.322.7285.537[↩][↩]
- Yang YF, Wang HJ, Kan WC, Kuo HL, Huang CC. Pyogenic liver abscess in ESRD patients undergoing maintenance dialysis therapy. Am J Kidney Dis. 2006 May;47(5):856-61. doi: 10.1053/j.ajkd.2006.01.032[↩]
- Liver Abscess Clinical Presentation. https://emedicine.medscape.com/article/188802-clinical#b2[↩][↩][↩][↩]
- Syed MA, Kim TK, Jang HJ. Portal and hepatic vein thrombosis in liver abscess: CT findings. Eur J Radiol. 2007 Mar;61(3):513-9. doi: 10.1016/j.ejrad.2006.11.022[↩][↩]
- Yang DM, Kim HN, Kang JH, Seo TS, Park CH, Kim HS. Complications of pyogenic hepatic abscess: computed tomography and clinical features. J Comput Assist Tomogr. 2004 May-Jun;28(3):311-7. doi: 10.1097/00004728-200405000-00002[↩][↩]
- Wang Y, Wang H, Liu Z, Chang Z. The Incidence of Septic Pulmonary Embolism in Patients with Klebsiella pneumoniae Liver Abscess: A Systematic Review and Meta-analysis. Gastroenterol Res Pract. 2022 Apr 15;2022:3777122. doi: 10.1155/2022/3777122[↩]
- Dietrick RB. Experience with liver abscess. Am J Surg. 1984 Feb;147(2):288-91. doi: 10.1016/0002-9610(84)90109-0[↩]
- Boĭko VV, Tishchenko AM, Gusak IV, Maloshtan AA, Skoryĭ DI, Smachilo RM. [Surgical treatment of a solitary hepatic abscess]. Klin Khir. 2013 Jun;(6):22-5.[↩]
- Moro PL, Gilman RH, Verastegui M, Bern C, Silva B, Bonilla JJ. Human hydatidosis in the central Andes of Peru: evolution of the disease over 3 years. Clin. Infect. Dis. 1999 Oct;29(4):807-12.[↩]
- Frider B, Larrieu E, Odriozola M. Long-term outcome of asymptomatic liver hydatidosis. J. Hepatol. 1999 Feb;30(2):228-31.[↩]
- Fontanilla T, Noblejas A, Cortes C, Minaya J, Mendez S, Van den Brule E, Hernando CG, Alfageme M, Baños I, Aguirre E. Contrast-enhanced ultrasound of liver lesions related to arterial thrombosis in adult liver transplantation. J Clin Ultrasound. 2013 Oct;41(8):493-500. doi: 10.1002/jcu.22069[↩]
- Ahn SJ, Kim JH, Lee SM, Park SJ, Han JK. CT reconstruction algorithms affect histogram and texture analysis: evidence for liver parenchyma, focal solid liver lesions, and renal cysts. Eur Radiol. 2019 Aug;29(8):4008-4015. doi: 10.1007/s00330-018-5829-9[↩]
- Rassam F, Cieslak KP, Beuers UHW, van Gulik TM, Bennink RJ. Stress test of liver function using technetium-99m-mebrofenin hepatobiliary scintigraphy. Nucl Med Commun. 2019 Apr;40(4):388-392. doi: 10.1097/MNM.0000000000000979[↩]
- van der Velden S, Dietze MMA, Viergever MA, de Jong HWAM. Fast technetium-99m liver SPECT for evaluation of the pretreatment procedure for radioembolization dosimetry. Med Phys. 2019 Jan;46(1):345-355. doi: 10.1002/mp.13253[↩]
- Rahimian J, Wilson T, Oram V, Holzman RS. Pyogenic liver abscess: recent trends in etiology and mortality. Clin. Infect. Dis. 2004 Dec 01;39(11):1654-9.[↩]
- Ahn SJ, Kim JH, Lee SM, Park SJ, Han JK. CT reconstruction algorithms affect histogram and texture analysis: evidence for liver parenchyma, focal solid liver lesions, and renal cysts. Eur Radiol. 2018 Nov 19[↩]
- Rassam F, Cieslak KP, Beuers UHW, van Gulik TM, Bennink RJ. Stress test of liver function using technetium-99m-mebrofenin hepatobiliary scintigraphy. Nucl Med Commun. 2019 Apr;40(4):388-392.[↩]
- Angeli A, Blazek A, Stephenson C. 64-Year-Old Woman With Fevers and Abdominal Pain. Mayo Clin Proc. 2024 Aug;99(8):1312-1316. https://www.mayoclinicproceedings.org/article/S0025-6196(23)00467-6/fulltext[↩][↩][↩][↩][↩]
- Kale S, Nanavati AJ, Borle N, Nagral S. Outcomes of a conservative approach to management in amoebic liver abscess. J Postgrad Med. 2017 Jan-Mar;63(1):16-20. doi: 10.4103/0022-3859.191004[↩]
- Sharma MP, Ahuja V. Management of amebic and pyogenic liver abscess. Indian J Gastroenterol. 2001 Mar;20 Suppl 1:C33-6.[↩]
- Amebic Liver/Hepatic Abscesses Treatment & Management. https://emedicine.medscape.com/article/183920-treatment[↩][↩][↩][↩][↩]
- Kumar R, Ranjan A, Narayan R, Priyadarshi RN, Anand U, Shalimar. Evidence-based therapeutic dilemma in the management of uncomplicated amebic liver abscess: A systematic review and meta-analysis. Indian J Gastroenterol. 2019 Dec;38(6):498-508. doi: 10.1007/s12664-019-01004-y[↩]
- Kumar R, Anand U, Priyadarshi RN, Mohan S, Parasar K. Management of amoebic peritonitis due to ruptured amoebic liver abscess: It’s time for a paradigm shift. JGH Open. 2019 Feb 8;3(3):268-269. doi: 10.1002/jgh3.12144[↩]
- Ahmed S, Chia CL, Junnarkar SP, Woon W, Shelat VG. Percutaneous drainage for giant pyogenic liver abscess–is it safe and sufficient? Am J Surg. 2016 Jan;211(1):95-101. doi: 10.1016/j.amjsurg.2015.03.002[↩]
- Haider SJ, Tarulli M, McNulty NJ, Hoffer EK. Liver Abscesses: Factors That Influence Outcome of Percutaneous Drainage. AJR Am J Roentgenol. 2017 Jul;209(1):205-213. doi: 10.2214/AJR.16.17713[↩]
- Sharma MP, Dasarathy S, Sushma S, Verma N. Long term follow-up of amebic liver abscess: clinical and ultrasound patterns of resolution. Trop Gastroenterol. 1995 Jul-Sep;16(3):24-8.[↩]
- Branum GD, Tyson GS, Branum MA, Meyers WC. Hepatic abscess. Changes in etiology, diagnosis, and management. Ann Surg. 1990 Dec;212(6):655-62. doi: 10.1097/00000658-199012000-00002[↩]
- Liver Abscess Treatment & Management. https://emedicine.medscape.com/article/188802-treatment#d8[↩][↩][↩][↩]
- Chen SC, Lee YT, Yen CH, Lai KC, Jeng LB, Lin DB, Wang PH, Chen CC, Lee MC, Bell WR. Pyogenic liver abscess in the elderly: clinical features, outcomes and prognostic factors. Age Ageing. 2009 May;38(3):271-6; discussion. doi: 10.1093/ageing/afp002[↩]
- Oschner A, DeBakey M, Murray S. Pyogenic abscess of the liver. Am J Surg. 1938;40:292–353.[↩]
- Branum GD, Tyson GS, Branum MA, Meyers WC. Hepatic abscess. Ann Surg. 1990;212:655–62. doi: 10.1097/00000658-199012000-00002[↩]
- Barbour GL, Juniper K., Jr A clinical comparison of amoebic and pyogenic hepatic abscess of the liver in sixty six patients. Arm Intern Med. 1972;77:629. doi: 10.1016/0002-9343(72)90175-1[↩]
- Farges O, Leese T, Bismuth H. Pyogenic liver abscess: an improvement in prognosis. Br J Surg. 1988;75:862–5. doi: 10.1002/bjs.1800750910[↩]
- Rubin RH, Swartz MN, Malt R. Hepatic abscess: changes in clinical, bacteriologic and therapeutic aspects. Am J Surg. 1974;57:601–10. doi: 10.1016/0002-9343(74)90012-6[↩]
- Miedema BW, Dineen P. The diagnosis and treatment of pyogenic liver abscesses. Ann Surg. 1984;200:328–35. doi: 10.1097/00000658-198409000-00010[↩]
- Pitt HA, Zuidema GD. Factors influencing mortality in the treatment of pyogenic hepatic abscess. Surg Gynecol Obstet. 1975 Feb;140(2):228-34.[↩]
- Chen SC, Yen CH, Lai KC, Tsao SM, Cheng KS, Chen CC, Lee MC, Chou MC. Pyogenic liver abscesses with Escherichia coli: etiology, clinical course, outcome, and prognostic factors. Wien Klin Wochenschr. 2005 Dec;117(23-24):809-15. doi: 10.1007/s00508-005-0481-1[↩]
- Chen SC, Huang CC, Tsai SJ, Yen CH, Lin DB, Wang PH, Chen CC, Lee MC. Severity of disease as main predictor for mortality in patients with pyogenic liver abscess. Am J Surg. 2009 Aug;198(2):164-72. doi: 10.1016/j.amjsurg.2008.08.022[↩][↩]
- You MS, Lee SH, Kang J, Choi YH, Choi JH, Shin BS, Huh G, Paik WH, Ryu JK, Kim YT, Jang DK, Lee JK. Natural Course and Risk of Cholangiocarcinoma in Patients with Recurrent Pyogenic Cholangitis: A Retrospective Cohort Study. Gut Liver. 2019 May 15;13(3):373-379. doi: 10.5009/gnl18339[↩]
- Shiuan-Chih Chen, Yuan-Ti Lee, Chi-Hua Yen, et al. Pyogenic liver abscess in the elderly: clinical features, outcomes and prognostic factors, Age and Ageing, Volume 38, Issue 3, May 2009, Pages 271–276, https://doi.org/10.1093/ageing/afp002[↩][↩]
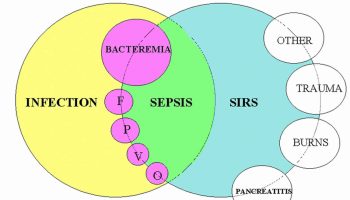



{kind=link}