Contents
Loiasis
Loiasis also known as African eye worm is an filarial infection caused by a parasitic roundworm (nematode) called Loa loa that is endemic in the forested areas of Central and western Africa and is transmitted by the bite of an infected Chrysops deer fly (Chrysops silacea or Chrysops dimidiata) 1, 2, 3, 4, 5, 6, 7, 8. Loiasis spreads to people through the repeated bites of deerflies that breed in rain forests in West and Central Africa which include the coastal plains of northern Angola, southeastern Benin, Cameroon, Central African Republic, Chad, Equatorial Guinea, Gabon, Nigeria, Sudan, the Democratic Republic of Congo, and Uganda. The highest prevalence of Loiasis was described for rural regions of Gabon, Equatorial Guinea and parts of Cameroon, the Central African Republic, the Democratic Republic of the Congo, and Republic of the Congo 9. It is estimated that between 3 and 13 million people are infected with Loa loa 10. Infection occurs most commonly among residents of endemic areas. It is unclear whether naturally acquired immunity develops after prolonged periods of exposure. Infection is asymptomatic in a large proportion of patients; therefore, in many areas, the epidemiology of loiasis has not been clearly defined. In endemic regions, the probability of Loa loa infection increases with age and forest exposure 11; the proportion of infected individuals varies depending on Chrysops vector abundance, which in turn is dependent on local ecology 3.
Most people infected with Loa loa parasitic roundworms do not develop symptoms (asymptomatic). But in those who do, symptoms can include 12:
- Itchy, non-painful body swelling that comes and goes, known as Calabar swelling. Calabar swelling can show up anywhere, although it’s more likely to happen near joints.
- Migration of the adult worm through the sclera or subconjunctival palpebral (under the eyelid) or bulbar tissue of the eye (the white part of the eyeball).
- Loa loa worms visibly crawling under your skin.
Less common symptoms include 12:
- Itching all over your body
- Muscle pain and joint pain
- Feeling weak and tired (fatigue)
In rare cases, people with loiasis may experience 12:
- Painful swellings of lymph glands
- Swollen scrotum, in men
- Inflammation of parts of the lungs
- Fluid collection around the lung
- Scarring of heart muscle
- Kidney damage, if infection continues for many years
If you traveled to or live in affected areas of Africa and you have Loiasis symptoms, your doctor may order a blood test. This test can show whether you have the Loa loa microfilariae in your blood. Your doctor may also perform a physical exam and look for signs of loiasis, such as itchy, swollen areas on your body.
Loa loa is usually diagnosed by the finding of microfilaria in peripheral blood smears or adults in the subconjunctiva. The blood films may be thick or thin and stained with Giemsa or hematoxylin-and-eosin (H&E). For increased sensitivity, concentration techniques can be used. These include centrifugation of the blood sample lysed in 2% formalin (Knott’s technique), or filtration through a Nucleopore® membrane. Microfilariae of Loa loa exhibit diurnal periodicity and a diagnosis is best made from blood collected during the midday (10 AM to 2 PM). The presence of Calabar swellings can aid in the diagnosis.
The treatment of loiasis is complex and is best undertaken after consultation with experts who have experience in the treatment of the disease and prevention of complications of treatment. Additionally, there may be times when it is best not to treat the infection.
Antiparasitic medications, like ivermectin and diethylcarbamazine (DEC), treat loiasis. Diethylcarbamazine is the treatment of choice and is known to be effective at eradicating both microfilariae and adult worms but must be used with caution 13. But people with high levels of Loa loa microfilariae in their blood (>8,000 microfilariae per ml) can have life-threatening reactions to these medications. Microfilarial loads are determined by calculating the number of microfilariae per milliliter using a measured quantity of blood 14. Your doctor may order a test to measure the number of microfilariae in your blood before giving you ivermectin or diethylcarbamazine (DEC).
If you have more than 8,000 microfilariae per milliliter of blood, ivermectin and diethylcarbamazine (DEC) may not be safe for you. Your doctor may recommend a medication called albendazole or a blood filtering procedure (apheresis) first. Albendazole and blood filtering (apheresis) lower the number of microfilariae in your blood. Then, ivermectin or diethylcarbamazine (DEC) may be safe for you to take.
Available data demonstrate that the risk of fatal encephalopathy in patients treated with diethylcarbamazine (DEC) with microfilarial loads <8,000 microfilariae per mL approaches zero. In those patients with microfilarial loads more than 8,000 microfilariae per mL (>8,000 microfilariae per ml) , apheresis can be used in specialized centers to reduce the load below the 8,000 threshold prior to beginning treatment. Some authors suggest a more conservative threshold of 2,500 microfilariae per mL for the initiation of treatment of loaisis. This lower threshold would need to be balanced with the risk associated with apheresis. There are some data available that suggest treating the patient with albendazole, 200mg twice daily for 21 days, may reduce the microfilarial load to acceptable levels. Re-measurement of levels after albendazole treatment would be required prior to treatment with diethylcarbamazine (DEC).
Note that Diethylcarbamazine (DEC) is contraindicated in persons with onchocerciasis co-infection because of the risk of blindness and/or severe exacerbation of skin disease.
Diethylcarbamazine (DEC) has been used worldwide for more than 50 years. Because Loiasis is rare in the United States, diethylcarbamazine (DEC) is no longer approved by the U.S. Food and Drug Administration (FDA) and cannot be sold in the United States. Physicians can obtain the medication from CDC after confirmed positive lab results.
Because loiasis is rare in the U.S., your doctor may consult with an expert in tropical medicine to treat the infection. If you have a severe infection, you’ll need to see an experienced tropical medicine specialist.
Surgical removal of adult worms from the conjunctiva of the eye is indicated whenever the adult worm presents in the subconjunctival space, and is followed up with systemic medications, which prevent recurrence by reducing systemic micro- and macrofilarial loads.
Table 1. Loiasis medications
| Medication | Indication | Adult Dose | Children Dose |
|---|---|---|---|
| Diethylcarbamazine (DEC) | Symptomatic loiasis with <8,000 microfilariae/mL | 8–10 mg/kg/day orally in 3 divided doses daily for 21 days | 8–10 mg/kg/day orally in 3 divided doses daily for 21 days |
| Albendazole | Symptomatic loiasis, with <8,000 microfilariae/mL and failed 2 rounds diethylcarbamazine (DEC) OR Symptomatic loiasis, with ≥8,000 microfilariae/ml to reduce level to <8,000 microfilariae/ml prior to treatment with diethylcarbamazine (DEC) | 200 mg orally twice daily for 21 days | 200 mg orally twice daily for 21 days |
| Apheresis* followed by diethylcarbamazine (DEC) | Symptomatic loiasis, with ≥8,000 microfilariae/mL | N/A | N/A |
Footnotes: * Apheresis should be performed at an institution with experience in using this therapeutic modality for loiasis. Oral albendazole is available for human use in the United States.
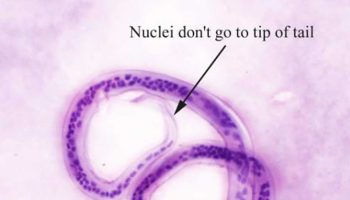
[Source 15 ]Figure 1. Loa loa worm
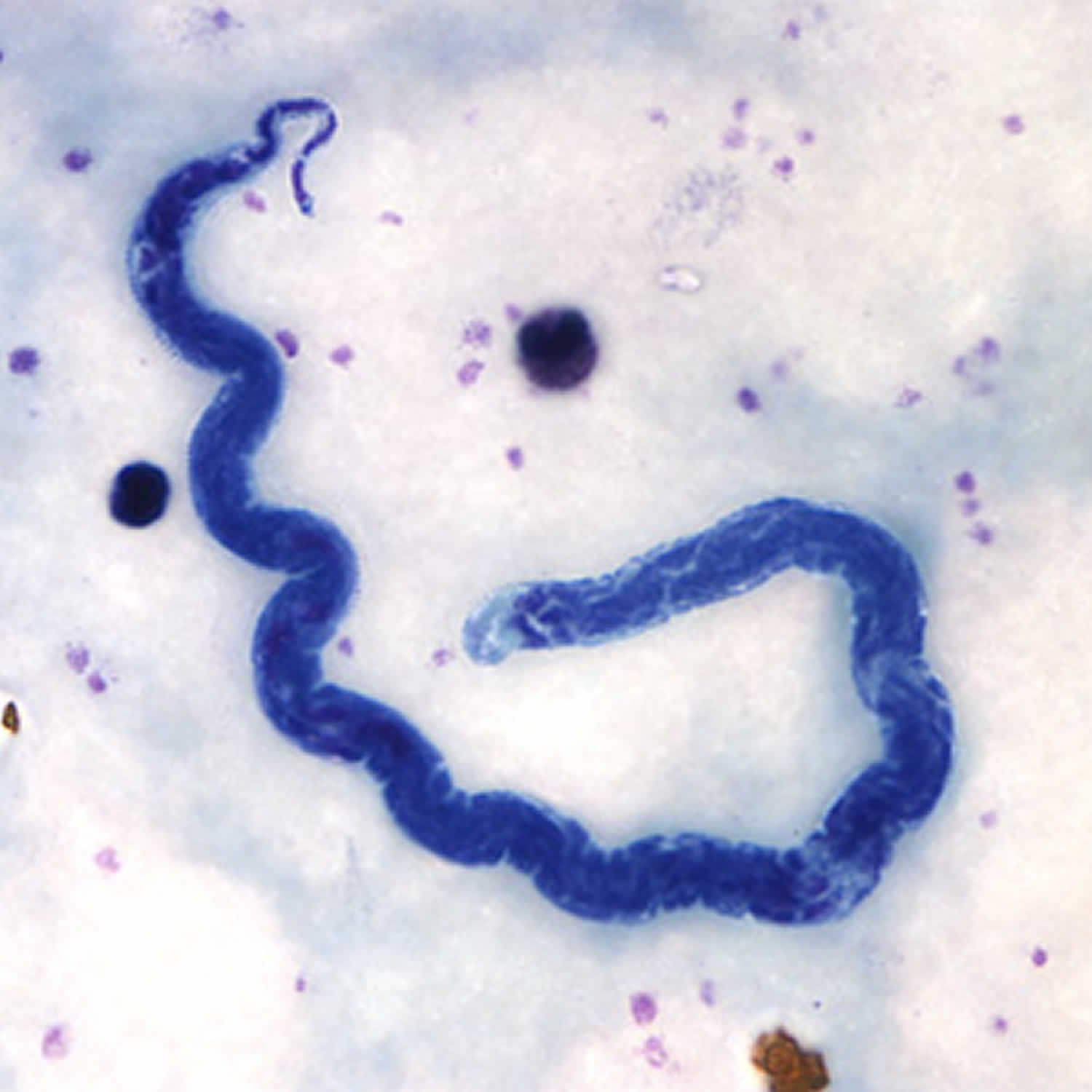
Footnotes: Microfilaria of Loa loa in a thick blood smear, stained with Giemsa. Loa loa microfilariae (immature worms) are large (231 to 250 μm in length) on stained blood films with a short headspace and nuclei that extend irregularly to the tip of the tail. The microfilariae have a sheath that is not always visible, because it does not usually stain bright pink with Giemsa but can be visualized with hematoxylin stains. Of note is that sheaths may be shed if there is a delay in processing the blood specimen.
[Source 16 ]Figure 2. Loa loa microfilariae (Loa loa immature worms)
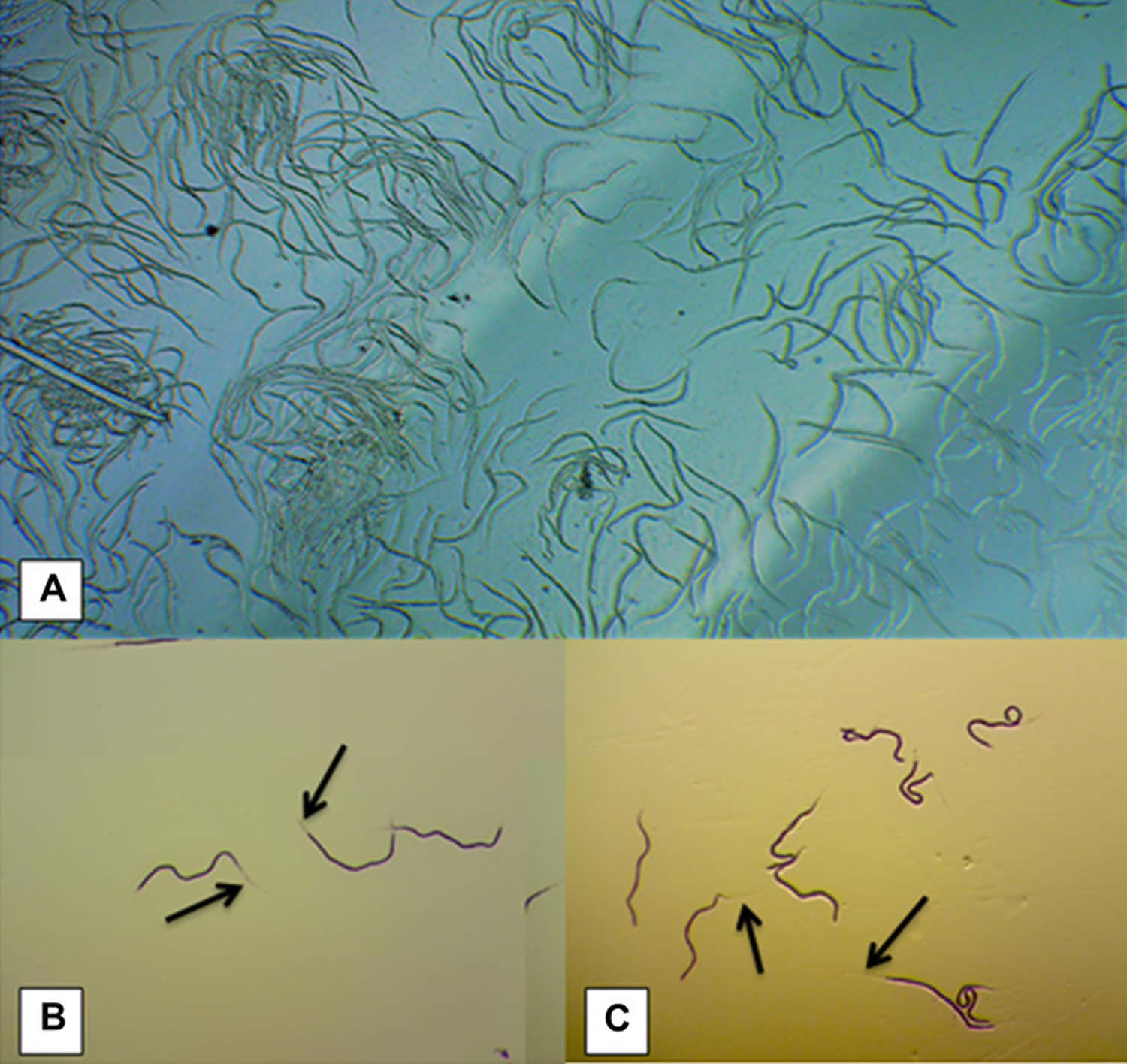
Footnotes: Loa loa microfilariae (immature worms) purified after Percoll gradient cell separation (A) and May–Grünwald Giemsa staining (B and C). The sheath can be seen as an extended translucid structure along the end tail (arrows).
[Source 1 ]Figure 3. Loiasis signs and symptoms
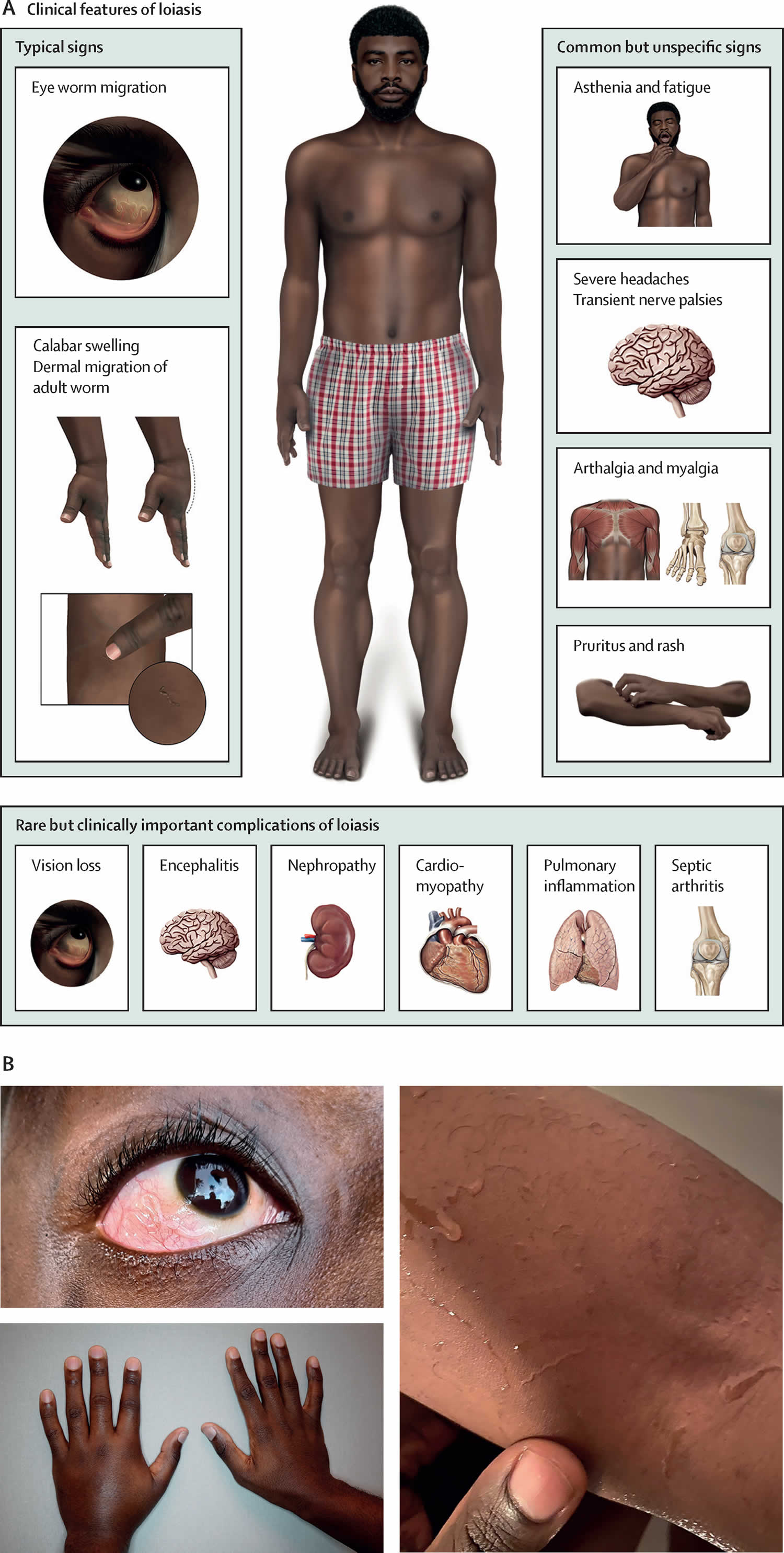
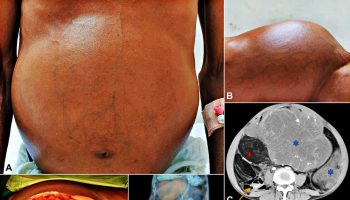
Footnotes: (A) Illustration of typical signs, common but unspecific signs, and rare but clinically important complications of Loiasis. (B) Eye worm migration, Calabar swelling of the left hand, and dermal migration of adult worm.
[Source 17 ]Figure 4. Loiasis
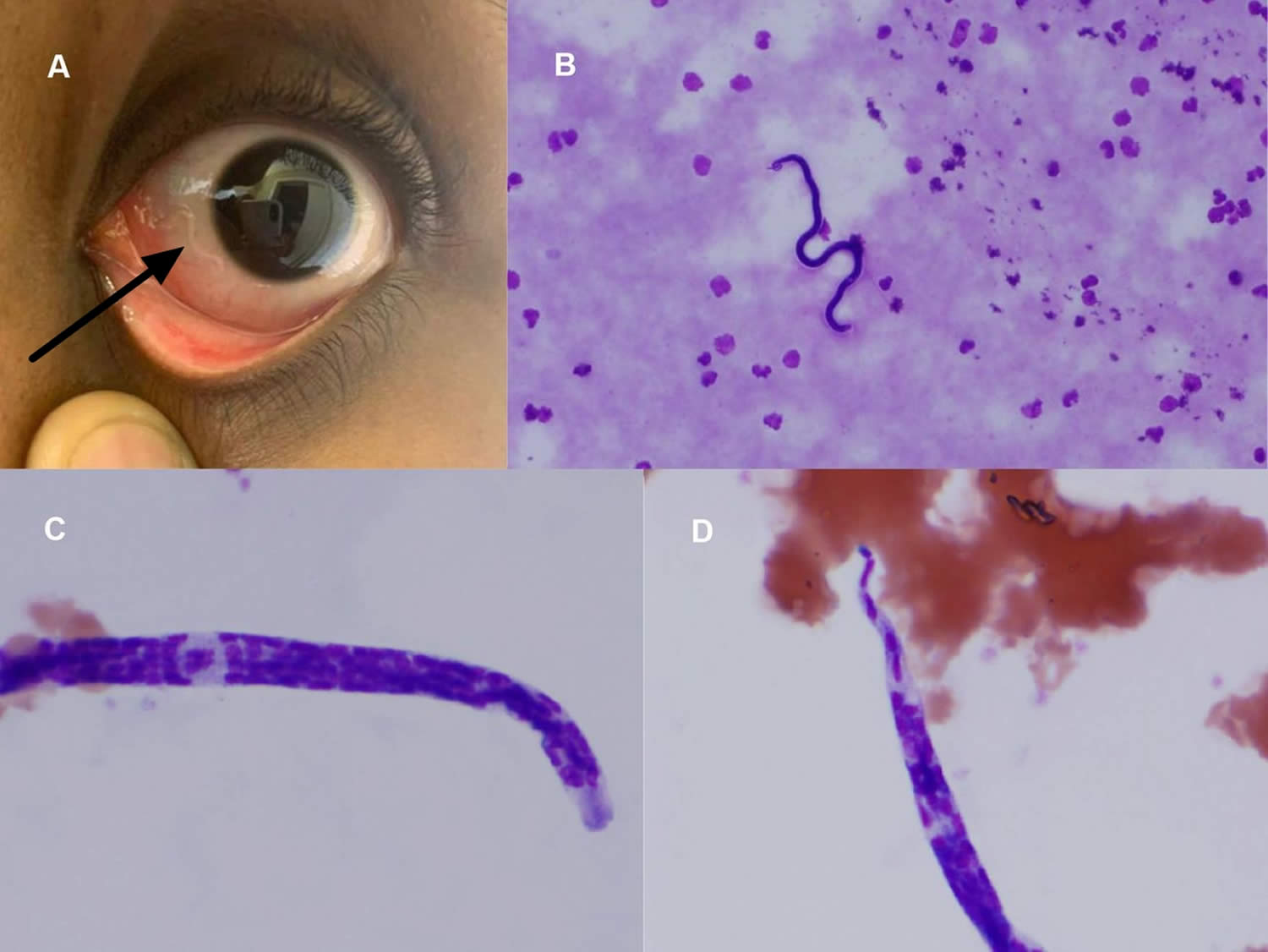
Footnotes: (A) Adult Loa loa subconjunctival worm in patient’s right eye. (B) Loa loa microfilaria (immature worm) in Giemsa-stained thick blood smear (original magnification, ×10). (C) Anterior end of microfilaria showing short headspace and nuclei that are coarse and densely packed throughout the length of the worm. A sheath is not present (original magnification, ×40). (D) Tapered tail with nuclei extending to the tip (original magnification, ×40).
[Source 18 ]Figure 5. Chrysops silacea (deer fly)
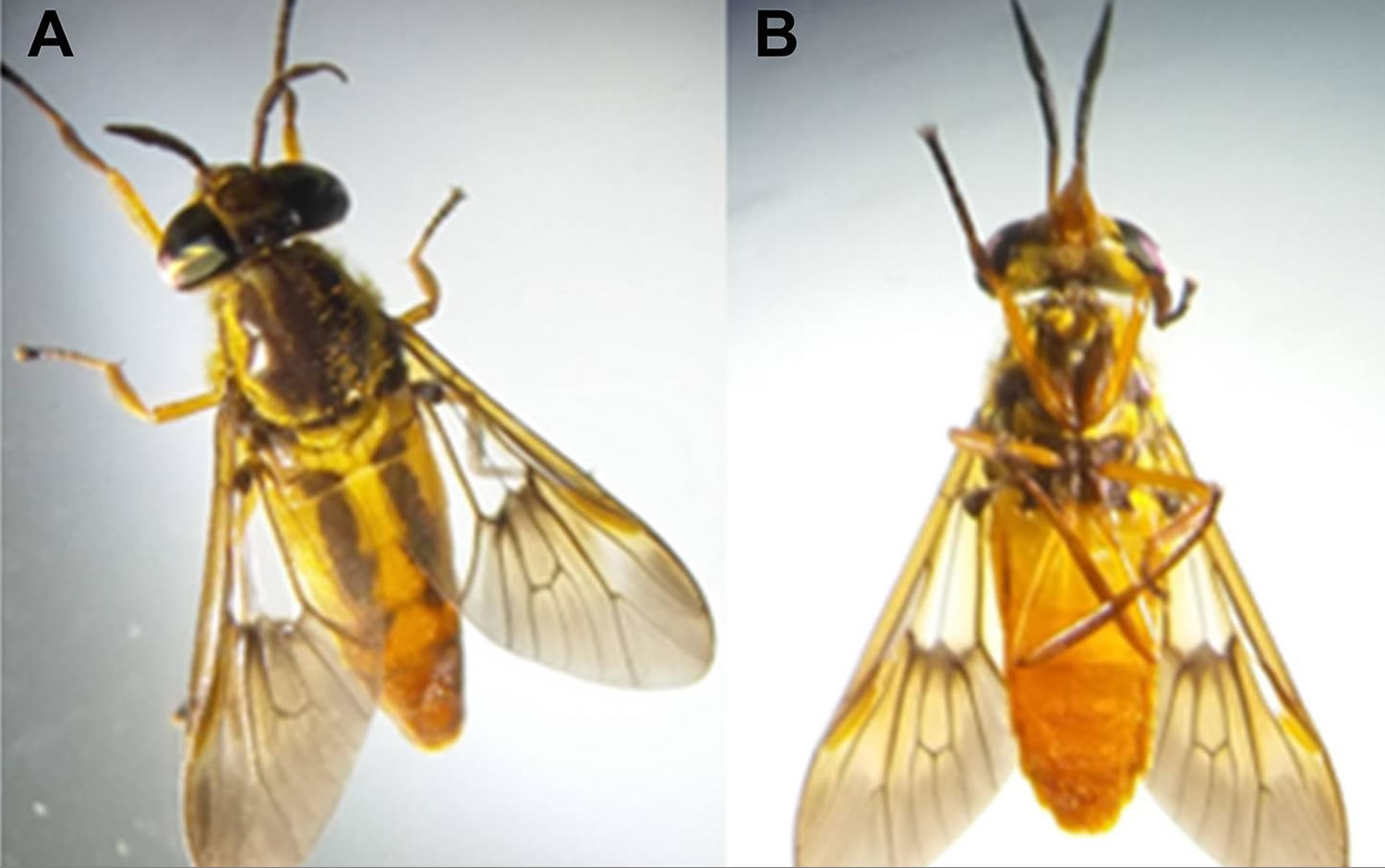
Footnotes: View of Chrysops silacea deer fly with the typical two longitudinal stripes on the back that never extend beyond the third abdominal segment and may be so attenuated or interrupted as to be almost absent (A) and ventral side of the fly (B). The wing markings of the two species of Chrysops are similar. Chrysops silacea deer flies can carry more infective L3 Loa loa larvae along their proboscis and thorax. These serve as a source of natural infective-stage larvae of Loa loa. Only females take a blood meal, and, with rare exception, they feed during the daytime 19. Unlike numerous other groups of blood sucking flies, female deer flies do not enter structures and thus do not feed on humans indoors 19. Female deer flies typically feed on moving hosts and usually bite on the shoulders and head 19. They have a wide host range, attacking mammals of all sizes, including humans, and some species feed on birds and reptiles. Female deer flies are aggressive, persistent feeders that quickly return to bite again if they are interrupted before they take a complete blood meal 19.
[Source 1 ]Figure 6. Chrysops dimidiata (deer fly)

Footnotes: View of Chrysops dimidiata deer fly the abdominal stripes are broader and reach the fourth segment, where they usually become merged into the darker brown color of the terminal segments (A) and ventral side of the fly (B). The wing markings of the two species of Chrysops are similar. Chrysops dimidiata deer flies can carry more infective L3 Loa loa larvae along their proboscis and thorax. These serve as a source of natural infective-stage larvae of Loa loa. Only females take a blood meal, and, with rare exception, they feed during the daytime 19. Unlike numerous other groups of blood sucking flies, female deer flies do not enter structures and thus do not feed on humans indoors 19. Female deer flies typically feed on moving hosts and usually bite on the shoulders and head 19. They have a wide host range, attacking mammals of all sizes, including humans, and some species feed on birds and reptiles. Female deer flies are aggressive, persistent feeders that quickly return to bite again if they are interrupted before they take a complete blood meal 19.
[Source 1 ]Figure 7. Loiasis geographic distribution
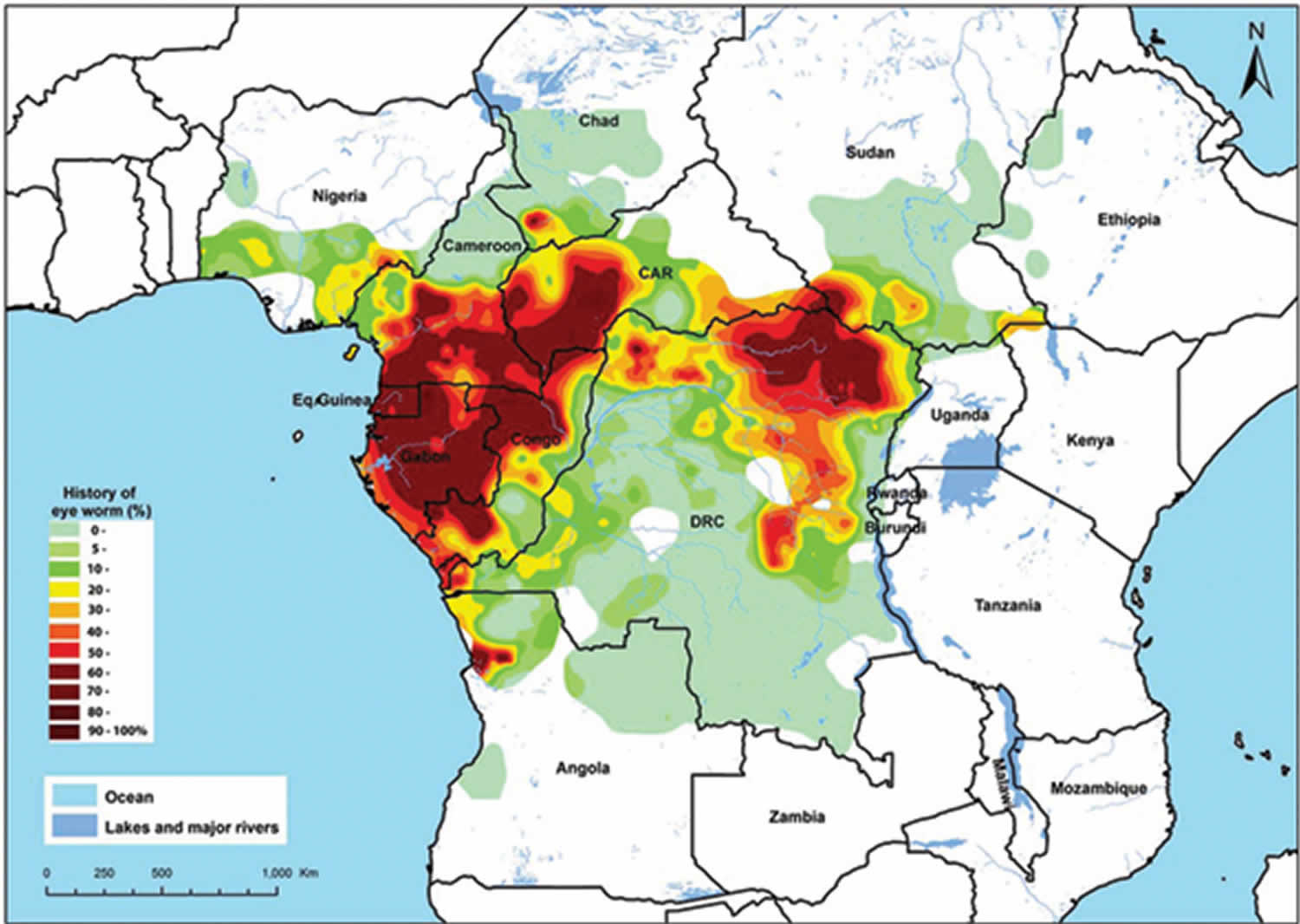
Footnotes: Zouré et al. 9 provided a comprehensive distribution of loiasis in Africa, which nearly corresponds to the distribution of Chrysops fly vectors 20, 21 because the transmission of loiasis is correlated to the distribution of its vectors. According to these authors, two main zones of highly endemic loiasis can be distinguished: a western zone that comprises part of the Equatorial Guinea, Gabon, Cameroon, Republic of Congo, Central African Republic and Chad, Democratic Republic of Congo (DRC) and Angola; the second hyper‐endemic zone is mainly made up of the North‐Eastern part of the Democratic Republic of Congo (DRC) 9. Areas of low endemicity include most parts of Democratic Republic of Congo (DRC), north Cameroon and large sections of Angola, Nigeria, Chad and Sudan. Because some Chrysops flies are essentially zoophilic, the geographic distribution likely expands beyond the previously described area. For instance, Chrysops species have been described in Egypt 22 and in Rwanda 21, countries not mentioned in the previously described area of distribution.
[Source 9 ]Can loiasis cause blindness?
Seeing a worm in your eye can be unsettling and uncomfortable. But Loa loa worms, which are 1 to 3 inches long, don’t cause blindness and usually don’t damage your eyes 23, 24, 25. The worm usually moves across your eye and back into your body. Your eye doctor can safely remove a visible worm with a minor procedure, but this will not cure the infection. You’ll need a followed up treatment with systemic medications, which prevent recurrence by reducing systemic micro- and macrofilarial loads.
Intraocular filariasis due to Loa loa is an uncommon occurrence, which presents with pain and foreign body sensation 26. Unlike subconjunctival filariasis, intraocular filariasis is associated with significant risk of visual acuity loss with some patients ending up with complete blindness 27). Your pre-operative presentation is strongly correlated with your postoperative outcome 28, 29, 30, 31, 32. In general, patients with more advanced eye disease at presentation with more pronounced intraocular inflammation are more likely to suffer significant long-term vision loss, while patients whose intraocular filariae are removed prior to development of intraocular membranes may be able to return to their normal visual acuity 30.
What causes Loiasis
Loiasis also known as African eye worm is an filarial infection caused by a parasitic roundworm (nematode) called Loa loa that is endemic in the rain forests of Central and western Africa and is transmitted by the bite of an infected Chrysops deer fly (Chrysops silacea or Chrysops dimidiata) 1, 2, 3, 4, 5, 6, 7, 8. Loiasis spreads to people through the repeated bites of deerflies that breed in rain forests in West and Central Africa which include the coastal plains of northern Angola, southeastern Benin, Cameroon, Central African Republic, Chad, Equatorial Guinea, Gabon, Nigeria, Sudan, the Democratic Republic of Congo, and Uganda. The highest prevalence of Loiasis was described for rural regions of Gabon, Equatorial Guinea and parts of Cameroon, the Central African Republic, the Democratic Republic of the Congo, and Republic of the Congo 9. Only female Chrysops deer fly (Chrysops silacea or Chrysops dimidiata) take a blood meal, and, with rare exception, they feed during the daytime 19. Unlike numerous other groups of blood sucking flies, female deer flies do not enter structures and thus do not feed on humans indoors 19. Female deer flies typically feed on moving hosts and usually bite on the shoulders and head 19. They have a wide host range, attacking mammals of all sizes, including humans, and some species feed on birds and reptiles. Female deer flies are aggressive, persistent feeders that quickly return to bite again if they are interrupted before they take a complete blood meal 19.
It is estimated that between 3 and 13 million people are infected with Loa loa 10. Infection occurs most commonly among residents of endemic areas. It is unclear whether naturally acquired immunity develops after prolonged periods of exposure. Infection is asymptomatic in a large proportion of patients; therefore, in many areas, the epidemiology of loiasis has not been clearly defined. In endemic regions, the probability of Loa loa infection increases with age and forest exposure 11; the proportion of infected individuals varies depending on Chrysops vector abundance, which in turn is dependent on local ecology 3.
When the Chrysops silacea or Chrysops dimidiata deer fly bite people with Loa loa infection, they pick up immature worms, or microfilariae, in that person’s blood 33. The microfilairiae (immature worms) develop into infectious larvae (L3 larvae) in the fly and can then infect people 33. When the deerfly bites a person’s skin to feed (take a bloodmeal), the infectious larvae (L3 larvae) enter the wound and begin moving through the person’s body (see Loa loa Life Cycle below).
It takes about five months for the third-stage infective L3 larvae to develop into adult worms. Larvae can only become adults inside the human body 33. The adult worms live between layers of connective tissue (e.g., ligaments, tendons) under the skin and between the thin layers of tissue that cover muscles (fascia). Their microfilariae will spread into the lymph nodes and eventually the lungs 33.
People who develop symptoms typically start seeing them about five months after they are infected. This is also when the microfilariae begin to enter the bloodstream. Adult worms can live in the body up to 17 years, reproducing most of this time 33.
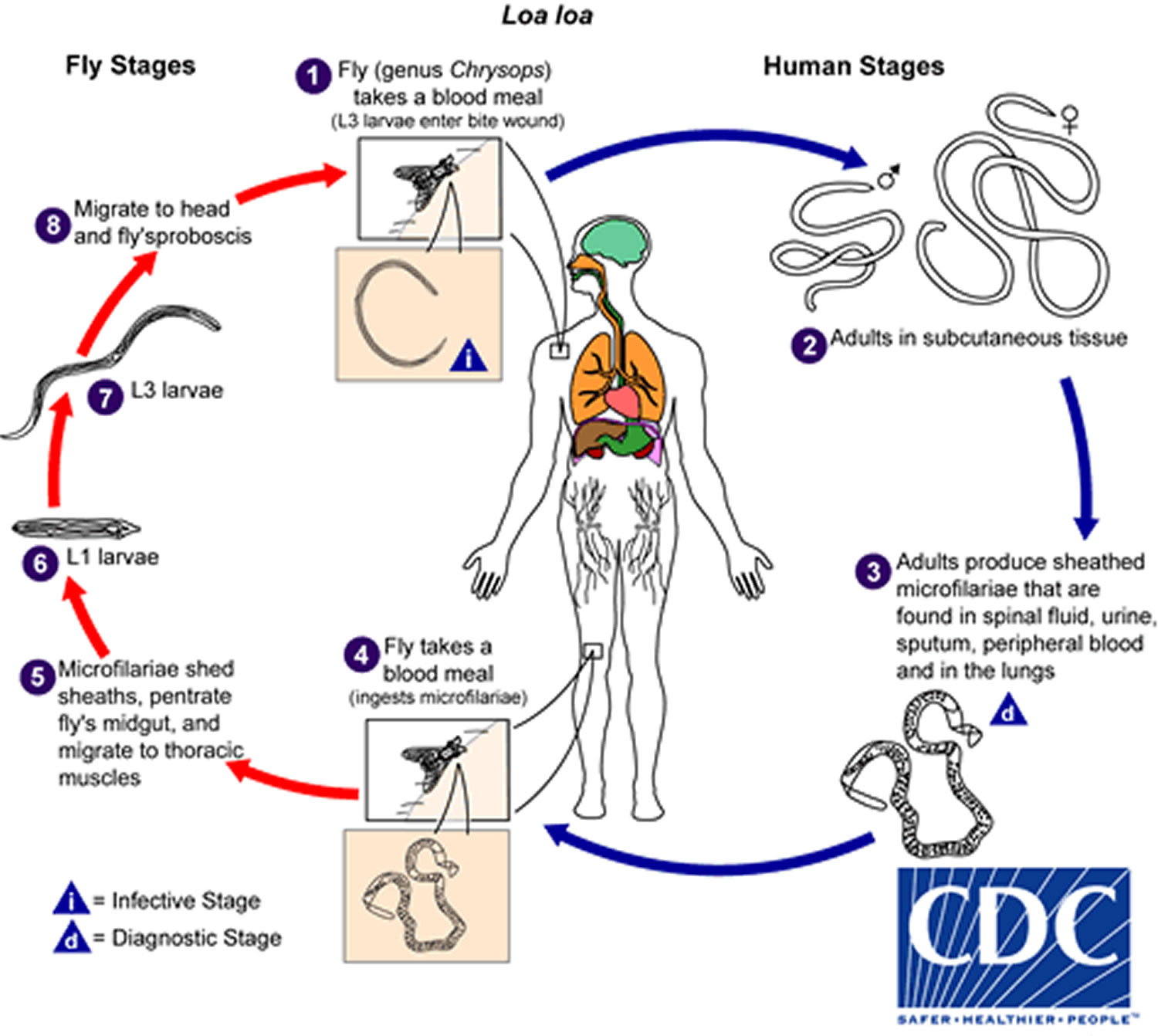
Loa loa Life Cycle
The vector for Loa loa filariasis are deer flies from two species of the genus Chrysops, Chrysops silacea and Chrysops dimidiata. During a blood meal, an infected Chrysops fly (day-biting flies) introduces third-stage infective L3 larvae onto the skin of the human host, where they penetrate into the bite wound (number 1). The larvae develop into adults that commonly reside in subcutaneous tissue (number 2). The female Loa loa worms measure 40 to 70 mm in length and 0.5 mm in diameter, while the males measure 30 to 34 mm in length and 0.35 to 0.43 mm in diameter. Adult Loa loa worms produce microfilariae measuring 250 to 300 µm by 6 to 8 μm, which are sheathed and have diurnal periodicity. Microfilariae have been recovered from spinal fluids, urine, and sputum. During the day they are found in peripheral blood, but during the noncirculation phase, they are found in the lungs (number 3). The Chrysops fly ingests microfilariae during a blood meal (number 4). After ingestion, the microfilariae lose their sheaths and migrate from the fly’s midgut through the hemocoel to the thoracic muscles of the arthropod (number 5). There the microfilariae develop into first-stage larvae (number 6) and subsequently into third-stage infective L3 larvae (number 7). The third-stage infective L3 larvae migrate to the fly’s proboscis (number 8) and can infect another human when the fly takes a blood meal (number 1).
Figure 8. Loa loa life cycle
Loiasis prevention
The best way to prevent Loiasis is to avoid Chrysops silacea or Chrysops dimidiata deer fly bites by limiting outdoor exposure during daytime and use of protective clothing are currently the only effective ways to prevent individuals from infectious bites 17. It is unclear whether classic insect repellents, including diethyltoluamide (DEET) and icaridin, confer protection against bites from Chrysops silacea or Chrysops dimidiata deer flies and consequent infection with Loa loa for travellers to or residents in endemic regions 17. Controlling deer flies (and horse flies) is nearly impossible 19. The use of insecticides to kill the fly larvae is not an option because the vast majority of species develop in natural habitats in which
insecticides cannot be applied due to environmental concerns 19. Even if they could be used, insecticides would be ineffective in controlling larvae because they are widely dispersed in a developmental site. The use of insecticides against adult
horse and deer flies is not a realistic option because they are relatively large to very large and unaffected by the rate of insecticide that can be applied according to product label 19. At best, an insecticide application aimed at adult flies might produce a minor and temporary reduction in biting. A number of trapping devices have been used to capture adults, but their value is limited to sampling. At best, trapping devices produce temporary, minor relief from female flies.
If you’re traveling to West or Central Africa and planning to stay for a long period of time, you can reduce your risk of loiasis infection by:
- Taking 300 milligrams (mg) of diethylcarbamazine (DEC) once a week.
- Wearing insect repellants with DEET (N,N-Diethyl-meta-toluamide or diethyltoluamide).
- Wearing long pants and long-sleeved shirts to keep flies off your skin.
- Applying an insecticide called permethrin to your clothes.
Historically, 60% dimethyl phthalate (DMP) solution conferred good protection against Chrysops bites 19, 4. However, due to the substantial potential for irritation of the eyes and the respiratory tract and its unclear carcinogenic potential, this hardly constitutes a practical control tool 35, 36.
Animal studies had indicated that diethylcarbamazine (DEC) might be used as a prophylactic (preventive) drug in the prevention of Loa loa infection 37. A randomised controlled clinical trial evaluated weekly doses of 300 mg diethylcarbamazine (DEC) as a chemoprophylactic regimen for long-term travellers to Gabon, Cameroon, and Central African Republic 38. In this study, weekly diethylcarbamazine (DEC) prophylaxis led to a complete protection from loiasis compared with a 30% attack rate in participants travelling to Gabon who had not taken the prophylaxis 38. The safety profile of diethylcarbamazine (DEC) was good, although the tolerability analysis indicated increased frequency of nausea. Although diethylcarbamazine (DEC) prophylaxis might be used exceptionally on a case-by-case basis for people from non-endemic countries travelling for long-term visits to regions of highest transmission (eg, Peace-Corps volunteers, soldiers, or missionaries), this strategy is unsuitable for a group of people who are indigenous and native to a specific place, having originated from that location for a very long time with established Loa loa infections due to longterm safety concerns with the use of diethylcarbamazine (DEC) 39.
Mass treatment of populations using mass drug administration (MDA) in endemic regions has proven extremely successful in controlling several neglected tropical diseases 40. Ivermectin-based onchocerciasis control programmes simultaneously led to substantial reduction of Loa loa microfilaremia, indicating the usefulness of mass drug administration (MDA) for the future control of loiasis 41. However, to date no treatment regimen is safe and efficacious enough to be used routinely for loiasis control 17. Therefore, the clinical development of new drug regimens suitable for population-based mass drug administration (MDA) programmes is an important research priority 17. The roll-out of mass drug administration (MDA) programmes will allow the effective reduction of the infectious reservoir in the local population and will therefore reduce the number of newly infected individuals 17. The availability of such mass drug administration control programmes and the roll-out of effective diagnostic and treatment services for individual patient care will prove vital to reduce the intolerable morbidity and mortality that loiasis exerts today on affected communities 17.
Loiasis signs and symptoms
As with other diseases caused by parasitic worms, many people who are infected with Loa loa never develop symptoms (asymptomatic). But in those who do, the main symptoms are 12:
- Itchy, non-painful body swelling that comes and goes, known as Calabar swelling. Calabar swelling can show up anywhere, although it’s more likely to happen near joints.
- Migration of the adult worm through the sclera or subconjunctival palpebral (under the eyelid) or bulbar tissue of the eye (the white part of the eyeball).
- Loa loa worms visibly crawling under your skin.
Most patients with loiasis are asymptomatic. The classic clinical sign and symptom of loiasis is the formation of Calabar swellings, which are transient subcutaneous nodules created by migrating adult worms. Calabar swellings can occur anywhere on your body but are most common on the trunk and arms. Occasionally, adult worms will migrate to the eye and can be observed grossly in the conjunctiva 42.
Loa loa is referred to as “African Eye Worm” because the Loa loa worm can be observed migrating across the periorbital tissues and into the subconjunctiva. This observation is not associated with lasting damage to tissues. However, discomfort and foreign body sensation are commonly reported symptoms 6, 43, 23, 24.
In rare cases, Loa loa has been noted to enter the anterior chamber of the eye, and live Loa loa worms have been reported in the vitreous. Such patients present with a grossly visible intraocular filarial worm on physical exam, usually with pain and photophobia. Associated vision loss at presentation has ranged from 6/24 to light perception. Slit lamp exam often reveals fibrinous membrane formation, cell/flare, and keratic precipitates. More prolonged cases may develop retinal detachments 28, 29, 30, 31, 32.
Less common symptoms include 12:
- Itching all over your body
- Muscle pain and joint pain
- Feeling weak and tired (fatigue)
In rare cases, people with loiasis may experience 12:
- Painful swellings of lymph glands
- Swollen scrotum, in men
- Inflammation of parts of the lungs
- Fluid collection around the lung
- Scarring of heart muscle
- Kidney damage, if infection continues for many years
Loiasis diagnosis
If you traveled to or live in affected areas of Africa and you have Loiasis symptoms, your doctor may order a blood test. This test can show whether you have the Loa loa microfilariae in your blood. Your doctor may also perform a physical exam and look for signs of loiasis, such as itchy, swollen areas on your body.
Traditionally, the diagnosis of Loiasis requires demonstrating microfilariae in the peripheral blood or skin under microscopy. Loa loa is primarily diagnosed by the finding of microfilariae in thick and thin blood films stained with Giemsa, Wright, Wright-Giemsa, or hematoxylin stains. It is best performed using capillary or venous peripheral blood taken between 10AM and 4PM because peripheral microfilaremia peaks during the hot hours of the day 44, 45. Serpent-like moving microfilariae might be directly visualised in fresh blood or a more detailed morphological assessment is performed in stained blood smears 46. The microfilariae measure 231 to 250 μm long on stained blood films and possess a sheath that usually does not stain with Giemsa. Also, the sheath may be shed and not visible if there is a delay in processing the blood. Loa loa microfilariae have a dense nuclear column with a short headspace and tail extending irregularly to the tip 47. Loa loa may also be diagnosed by the gross examination of adult worms removed from the eye or in histopathologic examination of skin biopsy specimens. In both instances, the adults need to be differentiated from zoonotic filarids in the genus Dirofilaria 47, 48. The adults of both Loa loa and Dirofilaria worms are similar in size and macroscopic appearance. A distinguishing difference is that the adult Loa loa has small irregularly spaced bumps (bosses) on the surface of the cuticle, while the adult Dirofilaria has a thick cuticle with multiple longitudinal ridges 48. Dirofilaria microfilariae are rarely seen in human blood and are unsheathed, and nuclei do not extend to the tip of the tail.
Staining is most commonly done with Giemsa stain, although the pathognomonic features including the presence of a sheath are better visualized by hematoxylin-based stains 49. Rapid stains have been shown to be similarly accurate while substantially shortening the processing time 50, 51. The sensitivity of microscopic assays relies most importantly on the total amount of blood being investigated. Concentration techniques with lysing solutions or filtration techniques improve sensitivity in individuals with low levels of microfilaremia 52, 53, 54. Over the past 5 years, an innovative approach for the time-efficient testing of large numbers of blood samples was established by a smartphone-based automated reader (the LoaScope) 55. This diagnostic technique has been useful for ruling out Loa loa hypermicrofilaremia in onchocerciasis control programmes 56, 57, 58. However, its diagnostic accuracy for individual case management has not yet been established and the device has an only limited availability.
Numerous approaches to improve Loa loa diagnostics have been initiated using biomarkers, such as immunoglobulin 4 (IgG4), polymerase chain reaction (PCR), reverse transcriptase PCR (RT-PCR), loop-mediated isothermal amplification, and lateral flow assays (LFAs) 59, 60, 61, 62. Absolute eosinophil counts and immunoglobulin E (IgE) levels, both are typically increased in patients with acute and chronic loiasis 63. Although serology has high sensitivity, it often lacks specificity, particularly in co-infected residents of endemic regions. A rapid diagnostic test detecting Loa loa-specific antibodies seems particularly useful for large-scale mapping of Loa loa transmission in communities targeted for ivermectin mass drug administration (MDA) 56, 64, 65. The test for Loa loa-specific antibodies has also shown reasonable diagnostic accuracy when used for patients of an Italian travel clinic 62. Whether the test has sufficiently high diagnostic accuracy for case management of permanent residents in high transmission regions is currently under investigation.
Direct detection of adult worms is desirable to prove infection in occult loiasis. The observation and potential extraction of an adult worm migrating through the eye, often documented by patients themselves via smartphone photography, has so far been the only certain detection method 66, 67. Several polymerase chain reaction (PCR) protocols have been advocated to detect occult loiasis. However, it remains unclear whether these assays truly detect migrating adult worms or rather submicroscopic microfilaremia. Independent validation in different settings is still absent, so no final conclusion can be drawn for their diagnostic accuracy in detecting occult loiasis 68, 69.
Loiasis treatment
There are several drugs with known activity against the adult or larval developmental stages of Loa loa, which are of varying clinical usefulness. Antiparasitic medications, like ivermectin and diethylcarbamazine (DEC), treat loiasis. But people with high levels of Loa loa microfilariae in their blood (> 8,000 microfilaria/mL) can have life-threatening reactions to these medications 70. Your doctor may order a test to measure the number of microfilariae in your blood before giving you ivermectin or diethylcarbamazine (DEC). Diethylcarbamazine (DEC) is contraindicated in persons with onchocerciasis co-infection because of the risk of blindness and/or severe exacerbation of skin disease.
The drug of choice for the treatment of loiasis is diethylcarbamazine (DEC). Most patients will achieve cure, defined as resolution of symptoms, resolution of eosinophilia, and decreasing antifilarial antibody titers, with one or two courses of diethylcarbamazine (DEC). Some will require additional courses of diethylcarbamazine (DEC) or a trial of albendazole. Diethylcarbamazine (DEC) is the treatment of choice because there is solid evidence that it kills both the microfilariae and the adult worms, resulting in quicker resolution of the infection. The risk of fatal encephalopathy or other severe adverse neurologic events is related to the microfilarial load. Quantitative blood smears are required before initiating treatment (see notes below). Prophylactic diethylcarbamazine (DEC) (300 mg once a week) can be used to prevent infection in long-term travelers to endemic areas.
Diethylcarbamazine (DEC) has been used worldwide for more than 50 years. Because Loiasis is rare in the United States, diethylcarbamazine (DEC) is no longer approved by the U.S. Food and Drug Administration (FDA) and cannot be sold in the United States. Physicians can obtain the medication from CDC after confirmed positive lab results.
There is some evidence that albendazole given twice daily for 21 days may be an effective treatment for loiasis that is refractory to diethylcarbamazine (DEC) treatment. It also may be used to reduce microfilarial load prior to initiation of diethylcarbamazine (DEC) treatment. The response to albendazole is slow so close, frequent monitoring would be needed to determine when it is safe to treat with diethylcarbamazine (DEC). Albendazole does not appear to be prone to cause encephalopathy, though published data are limited.
Treatment of loiasis with antiparasitic agents may result in a brief increase of symptoms, such as Calabar swelling or pruritus. Some authors suggest that these symptoms might be reduced with the concomitant use of antihistamines or corticosteroids during the first seven days of treatment. There is also the risk of fatal encephalopathy with diethylcarbamazine (DEC) treatment; this risk has not been shown to be eliminated by corticosteroid treatment.
If you have more than 8,000 microfilariae per milliliter of blood, ivermectin and diethylcarbamazine (DEC) may not be safe for you. Your doctor may recommend a medication called albendazole or a blood filtering procedure first. Albendazole is a broad-spectrum antihelmintic and antiprotozoal agent of the benzimidazole type that is FDA-approved for the treatment of a variety of parasitic worm infections 71, 72. Albendazole is thought not to directly kill Loa loa microfilariae but rather to suppress embryogenesis and release of microfilariae. This leads to a relatively slow and gradual but also safe reduction of microfilaremia over a period of about 3 weeks 43. It has been postulated that longer treatment courses of albendazole alone or in combination with ivermectin also exert adulticidal activity, although further evidence is needed 73. Due to these pharmacodynamic features, albendazole therapy is advocated for the safe and gradual reduction of microfilaremia before administration of diethylcarbamazine (DEC) for curative therapy.
Albendazole and blood filtering lower the number of microfilariae in your blood or reduce the parasitic load before introducing a curative treatment such as ivermectin or diethylcarbamazine (DEC). Then, ivermectin or diethylcarbamazine (DEC) may be safe for you to take.
The main limitation of albendazole-based regimens is the necessity for prolonged treatment courses leading to problems in treatment adherence, the requirement for biological follow-up to rule out liver toxicity, and possible intolerance due to allergic reactions 74. Development of encephalitis on initiation of albendazole therapy has been reported occasionally but is considered rare 75, 76. Albendazole may induce worm migration from the blood to other compartments such as the central nervous system (brain and spinal cord). The encephalopathy may result from the death of the microfilaria in the central nervous system (brain and spinal cord) and the ensuing inflammation 70. The rapid release of antigens can also lead to severe immune-mediated reactions 76.
Diethylcarbamazine (DEC) is the gold standard for curative treatment of loiasis and is the oldest of the commonly used antifilarial drugs and the only drug that has specifically been developed to treat filarial infections. The mode of action of diethylcarbamazine (DEC) is incompletely understood but its action is thought to be mediated indirectly by rendering the filarial pathogens susceptible to the host’s immune system 77. Diethylcarbamazine (DEC) induces a paralysis and rapid destruction of microfilariae in the liver and a fast clearance of microfilariae from peripheral blood 78, 79. Diethylcarbamazine (DEC) also exerts substantial adulticidal activity against Loa loa, leading to complete cure in around 40% to 80% of patients per 3-week treatment cycle 80, 81. Due to diethylcarbamazine (DEC) rapid onset of action, a large proportion of patients with high microfilarial loads have moderate to severe adverse drug reactions, particularly at the onset of treatment. Severe and life-threatening reactions, including encephalopathy, are often associated with retinal hemorrhages and have been ascribed to embolisms of microfilariae rapidly killed by diethylcarbamazine (DEC) 82, 83, 84, 85. Other complications, such as kidney insufficiency, pleural effusion, or laryngeal edema have been reported 82, 86.
Diethylcarbamazine (DEC) is also contraindicated in patients with co-infection with Onchocerca volvulus due to the risk for highly inflammatory skin and eye reactions leading to non-reversible complications 87, 88, 89. Therefore, diethylcarbamazine (DEC) should be used with great caution and experts recommend its use only in individuals with microfilaremia below 2000 microfilariae per mL (<2000 microfilariae/mL). Slow titration of diethylcarbamazine (DEC) doses over the first days of treatment and concomitant use of corticosteroids and antihistamines are advocated to dampen a potential over-reactive immunological response 84, 90. Often, more than one cycle of diethylcarbamazine (DEC) therapy is necessary for complete cure. Due to the potential safety issues associated with diethylcarbamazine treatment, it is most commonly used in non-endemic settings and is rarely employed in endemic regions for the treatment of loiasis.
Single-dose ivermectin therapy at 150–200 mcg/kg has a profound and rapid microfilaricidal effect, leading to an approximately 80% reduction of Loa loa microfilaremia. Ivermectin acts on the glutamate-gated chlorine channels of filarial pathogens but might also inhibit the worm’s immunomodulatory activity 91. Ivermectin leads to sustained suppression of microfilaremia, which is exerted over a period that by far exceeds the interval of pharmacokinetically relevant drug concentrations 92, 93, 94. This long-term sterilizing effect would be uniquely well suited for use in mass drug administration (MDA) programmes as a single-dose treatment regimen targeting the infectious stages of Loa loa. However, ivermectin used in mass drug administration (MDA) programmes to control onchocerciasis has been shown to be associated with treatment-emergent encephalopathy, a risk that is closely linked to the peripheral microfilarial load of Loa loa 95, 96, 97, 98, 99. Conjunctival hemorrhages, delirium, and movement disorders are typical clinical signs for ivermectin-associated encephalopathy, which, in the absence of an established specific therapy, might result in death or long-term complications. Similar to the assumed pathophysiology of encephalopathy, kidney changes linked to capillary embolisms of decaying microfilariae were reported after ivermectin treatment of loiasis 100. On the basis of ivermectin’s stage-specific action, preferentially targeting microfilariae while not being active against the adult developmental stages, it might be hypothesized that ivermectin exerts no direct effect on the signs and symptoms of loiasis caused by the migrating adult worms. However, it remains unclear whether ivermectin truly lacks any adulticidal activity and limited evidence suggests some benefit on subjective signs and symptoms 101.
On the basis of the current understanding of ivermectin’s safety in the treatment of loiasis, most experts would discourage its use in patients with microfilaraemia above 8000 microfilariae per mL (8000 microfilariae/mL) without previous medical or mechanical reduction of microfilaremia below this threshold. Given its unclear usefulness in alleviating clinical signs and symptoms caused by adult stages of Loa loa, ivermectin’s indication for individual treatment approaches is limited. Ivermectin might be of therapeutic value as a sequential drug following albendazole therapy, as this combination was highly efficacious in patients treated in a non-endemic region 102, 73. However, this high cure rate was not confirmed when ivermectin was used in a region of high transmission and therefore requires further evidence 103.
Table 2. Loiasis medications
| Antiparasitic medications | Dosage and instruction |
|---|---|
| Occult loiasis | |
| Diethylcarbamazine (first-line treatment) | 9 mg/kg in three divided doses daily for 21 days; more than one treatment cycle of 21 days might be necessary as cure rate is between 40% and 80% per cycle; contraindication in patients co-infected with onchocerciasis |
| Albendazole (alternative treatment option) | 400 mg* twice daily for 4-week treatment cycle; cure rate is unclear |
| Albendazole–ivermectin (alternative treatment option) | Albendazole (as described above) followed sequentially by single-dose 150–200 μg (microgram)/kg ivermectin; conflicting reports on overall cure rate |
| Microfilaremia, 1 to 2000 microfilariae per mL | |
| Diethylcarbamazine (first-line treatment) | Slow titration starting with 50 mg single dose on day 1, 50 mg three times on day 2, 100 mg three times on day 3, and subsequent 9 mg/kg divided in three daily doses until day 21; each 21-day treatment cycle leads to a 40–80% cure rate; more than one cycle might be needed; contraindication in patients co-infected with onchocerciasis |
| Albendazole (alternative treatment option) | 400 mg* twice daily for 4-week treatment cycle leads to relatively safe reduction of microfilaraemia; cure rate is unclear |
| Albendazole–ivermectin† (alternative treatment option) | Albendazole (as described above) followed sequentially by single-dose 150–200 μg/kg ivermectin leads to relatively safe reduction of microfilaraemia; conflicting reports on overall cure rate |
| Microfilaremia, 2000 to 8000 microfilariae per mL | |
| Albendazole (first-line treatment) | 400 mg* twice daily for 4-week treatment cycle as stand-alone treatment or as preparatory treatment to lower microfilaria load to less than 2000 microfilariae per mL for sequential treatment with diethylcarbamazine (see above) |
| Ivermectin (first-line treatment) | 150–200 μg (microgram)/kg single dose as preparatory treatment to lower microfilaria load to less than 2000 microfilariae per mL for sequential treatment with diethylcarbamazine (see above) |
| Albendazole–ivermectin† (alternative treatment option) | Albendazole (as described above) followed sequentially by single dose 150–200 μg (microgram)/kg ivermectin as stand-alone treatment or as preparatory treatment to lower microfilaria load to less than 2000 microfilariae per mL for sequential treatment with diethylcarbamazine (see above) |
| Microfilaremia, 8,000 to 30,000 microfilariae per mL | |
| Albendazole (first-line treatment) | 400 mg* twice daily for 4-week treatment cycle as stand-alone treatment or as preparatory treatment to lower microfilaria load to less than 8000 microfilariae per mL for sequential treatment with ivermectin† as stand-alone treatment or as preparatory treatment to lower microfilaria to less than 2000 microfilariae per mL for sequential treatment with diethylcarbamazine (see above) |
| Microfilaremia, more than 30,000 microfilariae per mL | |
| Apheresis (first-line treatment) | Mechanical reduction of microfilaria load by several cycles of apheresis safely reduces microfilaria load before treatments as indicated above |
| Albendazole (alternative treatment option) | Rare reports on encephalopathy associated with albendazole therapy indicates that this treatment approach is not without risk; gradual reduction of microfilariae is the treatment objective before treatment as indicated above for loiasis with microfilaria less than 30,000 microfilariae per mL |
| Adjunct treatments | Antihistamines and corticosteroids might be used for the first few days of treatment to reduce the severity of adverse drug reactions; however, adjunct treatments have no influence on the occurrence or severity of potentially life-threatening serious adverse events including encephalopathy |
Footnotes: Proposed treatment algorithm for individual case management of occult and microfilaraemic loiasis.
* 200 mg administered twice daily has also been shown to exert a substantial effect on microfilarial load. Given albendazole’s overall limited bioavailability with important interindividual and intraindividual variability and the good safety profile of albendazole at a daily dose of 800 mg, a dose regimen of 400 mg twice daily is suggested in this proposed treatment algorithm.
† Ivermectin is administered after 28 days of albendazole therapy and confirmation of microfilaraemia below 8000 microfilariae per mL.
[Source 17 ]Apheresis and host-directed therapies
Apheresis is a medical procedure that involves separating one or more components from a patient’s blood and returning the remaining blood to the body. A non-drug intervention successfully used for patients with hypermicrofilaraemic loiasis is apheresis. Here, mechanical reduction of microfilaraemia in several cycles safely reduces microfilarial loads and thus prepares the patient for safe follow-on treatment with antifilarial drugs for complete cure 104, 105, 106, 107, 108, 109.
Another therapeutic approach for excessive hypermicrofilaraemia is the use of host-directed therapies. These include corticosteroid therapy to dampen potential hyper-reaction of the immune system on the release of decaying microfilariae as well as novel therapeutic approaches using monoclonal antibodies targeting the eosinophilic immune reaction 90, 110, 111, 112, 113. Although the use of corticosteroids is included in several treatment recommendations, there is no clear evidence for its usefulness to avoid serious adverse drug reactions. This knowledge gap and the evaluation of host-directed therapies remain research priorities.
Surgery
The mechanical extraction of adult worms is technically relatively straightforward when the migration path becomes visible in the subconjunctival tissue, as well as during its infrequent and transient intradermal passage 114. Although the physical extraction of an adult worm constitutes a causative treatment approach, it might arguably only be of value in individuals with infection with a single or few worms, which is almost exclusively the case in temporary travellers after return from transmission regions. This procedure is of only limited therapeutic value for permanent residents in transmission zones due to the multiplicity of infections and high risk for re-infection 17.
Subconjunctival filariasis
Procedure: Given that a worm in the subconjunctival space may quickly migrate out of sight, the worm should first be grasped externally with forceps to prevent migration. Subsequent subconjunctival injection of 2% lidocaine with epinephrine 1:100,000 can then be used to simultaneously numb the region and paralyze the worm. A peritomy generally ≤ 5 mm allows access to the paralyzed worm, which can then be removed with a second set of forceps 24.
Postoperative Care: Systemic diethylcarbamazine or albendazole with topical steroids and antibiotics
Intraocular filariasis
Intraocular filariasis due to Loa loa is an uncommon occurrence, which presents with pain and foreign body sensation 26. Unlike subconjunctival filariasis, intraocular filariasis is associated with significant risk of visual acuity loss and blindness.
Anterior chamber filariasis
Procedure: Intracameral filarial worms may be removed with an anterior chamber washout, followed by a subconjuctival injection of steroids and antibiotics 30. In patients with more prolonged disease and more intense intraocular inflammation, excision of intracameral fibrinous membranes may be indicated 29.
Postoperative Care: Case reports suggest that patients often require high doses and prolonged courses of topical steroids, as well as topical antibiotics and sometimes mydriatics.
Vitreous chamber filariasis
One case report of Loa loa in the vitreous was effectively treated with vitrectomy with steroid cover 115.
Loiasis prognosis
Many people who have loiasis don’t know they have it (asymptomatic), and may not have serious health problems from it. If you have symptoms or suspect you have loiasis, see an experienced tropical medicine specialist. Medications can treat the infection and prevent possible complications.
- Dieki R, Nsi-Emvo E, Akue JP. The Human Filaria Loa loa: Update on Diagnostics and Immune Response. Res Rep Trop Med. 2022 Aug 1;13:41-54. doi: 10.2147/RRTM.S355104[↩][↩][↩][↩][↩]
- Kamgno, J., Nana-Djeunga, H.C., Kouam-Kenmogne, M. (2016). Loiasis. In: Gyapong, J., Boatin, B. (eds) Neglected Tropical Diseases – Sub-Saharan Africa. Neglected Tropical Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-25471-5_7[↩][↩]
- Kelly-Hope LA, Bockarie MJ, Molyneux DH. Loa loa ecology in central Africa: role of the Congo River system. PLoS Negl Trop Dis. 2012;6(6):e1605. doi: 10.1371/journal.pntd.0001605[↩][↩][↩][↩]
- Kelly-Hope L, Paulo R, Thomas B, Brito M, Unnasch TR, Molyneux D. Loa loa vectors Chrysops spp.: perspectives on research, distribution, bionomics, and implications for elimination of lymphatic filariasis and onchocerciasis. Parasit Vectors. 2017 Apr 5;10(1):172. doi: 10.1186/s13071-017-2103-y[↩][↩][↩]
- Metzger WG, Mordmüller B. Loa loa-does it deserve to be neglected? Lancet Infect Dis. 2014 Apr;14(4):353-7. doi: 10.1016/S1473-3099(13)70263-9[↩][↩]
- Padgett JJ, Jacobsen KH. Loiasis: African eye worm. Trans R Soc Trop Med Hyg. 2008 Oct;102(10):983-9. doi: 10.1016/j.trstmh.2008.03.022[↩][↩][↩]
- Antinori S., Schifanella L., Million M., Galimberti L., Ferraris L., Mandia L., Trabucchi G., Cacioppo V., Monaco G., Tosoni A., et al. Imported Loa Loa Filariasis: Three Cases and a Review of Cases Reported in Non-Endemic Countries in the Past 25 Years. Int. J. Infect. Dis. 2012;16:e649–e662. doi: 10.1016/j.ijid.2012.05.1023[↩][↩]
- Dieki R., Nsi-Emvo E., Akue J.P. The Human Filaria Loa Loa: Update on Diagnostics and Immune Response. Res. Rep. Trop. Med. 2022;13:41–54. doi: 10.2147/RRTM.S355104[↩][↩]
- Zouré HG, Wanji S, Noma M, Amazigo UV, Diggle PJ, Tekle AH, Remme JH. The geographic distribution of Loa loa in Africa: results of large-scale implementation of the Rapid Assessment Procedure for Loiasis (RAPLOA). PLoS Negl Trop Dis. 2011 Jun;5(6):e1210. doi: 10.1371/journal.pntd.0001210[↩][↩][↩][↩][↩]
- Klion A, Nutman TB. Loiasis and Mansonella Infections. In: Tropical Infectious Diseases: Principles, Pathogens and Practice, 3rd ed, Guerrant R, Walker DH, Weller PF (Eds), Saunders Elsevier, Philadelphia 2011. p.735.[↩][↩]
- Mischlinger J, Veletzky L, Tazemda-Kuitsouc GB, Pitzinger P, Matsegui PB, Gmeiner M, Lagler H, Gebru T, Held J, Mordmüller B, Ramharter M. Behavioural and clinical predictors for Loiasis. J Glob Health. 2018 Jun;8(1):010413. doi: 10.7189/jogh.08.010413[↩][↩]
- Symptoms of Loiasis. https://www.cdc.gov/filarial-worms/signs-symptoms/loiasis.html[↩][↩][↩][↩][↩][↩]
- Metzger WG, Mordmüller B. 2014. Loa loa—does it deserve to be neglected? Lancet Infect Dis 14:353–357. doi: 10.1016/S1473-3099(13)70263-9[↩]
- World Health Organization. 1997. Bench aids for the diagnosis of filarial infections. World Health Organization, Geneva, Switzerland.[↩]
- Clinical Treatment of Loiasis. https://www.cdc.gov/filarial-worms/hcp/clinical-care/loiasis.html[↩]
- https://www.cdc.gov/dpdx/loiasis/images/1/Loa2_1000.jpg[↩]
- Ramharter M, Butler J, Mombo-Ngoma G, Nordmann T, Davi SD, Zoleko Manego R. The African eye worm: current understanding of the epidemiology, clinical disease, and treatment of loiasis. Lancet Infect Dis. 2024 Mar;24(3):e165-e178. https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(23)00438-3/fulltext[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Burd EM, Babiker A, Fairley JK, Bhamidipati D, Woc-Colburn LE, Mathison BA. The Brief Case: Loa loa in a Patient from Nigeria. J Clin Microbiol. 2020 Dec 17;59(1):e01587-20. doi: 10.1128/JCM.01587-20. Erratum in: J Clin Microbiol. 2021 Aug 18;59(9):e0133821. doi: 10.1128/JCM.01338-21[↩]
- Hill, C ∙ MacDonald, J. Horse and deer flies: biology and public health risk. https://extension.entm.purdue.edu/publications/E-246.pdf[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Fain, A. 1978. Loaiasis: The present situation. Bull. O.M.S. 56, 155–167.[↩]
- Fain, A. 1969. Notes on the geographical distribution of the filarial worm Loa loa and of the horse flies of the genus Chrysops in Congo and Rwanda. Ann. Soc. Belge Med. Trop 49, 499–530.[↩][↩]
- Müller GC, Revay EE, Hogsette JA, Zeegers T, Kline D, Kravchenko VD, Schlein Y. An annotated checklist of the horse flies (Diptera: Tabanidae) of the Sinai Peninsula Egypt with remarks on ecology and zoogeography. Acta Trop. 2012 May;122(2):205-11. doi: 10.1016/j.actatropica.2012.01.013[↩]
- Okonkwo ON, Hassan AO, Alarape T, Akanbi T, Oderinlo O, Akinye A, Oyekunle I. Removal of adult subconjunctival Loa loa amongst urban dwellers in Nigeria. PLoS Negl Trop Dis. 2018 Nov 14;12(11):e0006920. doi: 10.1371/journal.pntd.0006920[↩][↩]
- Nam JN, Reddy S, Charles NC. Surgical management of conjunctival loiasis. Ophthalmic Plast Reconstr Surg. 2008 Jul-Aug;24(4):316-7. doi: 10.1097/IOP.0b013e31817d8a0b[↩][↩][↩]
- Rautaraya B, Tiwari S, Mahapatra A, Nanda A. Ocular filariasis. Trop Parasitol. 2011 Jul;1(2):116-8. doi: 10.4103/2229-5070.86957[↩]
- Aiello F, Palma S, Varesi C, Cerulli A, Valente R, Aiello L. A rare case report of Loa loa ocular filariasis. Eur J Ophthalmol. 2010 Jan-Feb;20(1):237-9. doi: 10.1177/112067211002000137[↩][↩]
- Loa Loa Filariasis (African Eye Worm). https://eyewiki.org/Loa_Loa_Filariasis_(African_Eye_Worm[↩]
- Hassan S, Isyaku M, Yayo A, Sarkin Fada F, Ihesiulor GU, Iliyasu G. Adult Loa loa Filarial Worm in the Anterior Chamber of the Eye: A First Report from Savanna Belt of Northern Nigeria. PLoS Negl Trop Dis. 2016 Apr 7;10(4):e0004436. doi: 10.1371/journal.pntd.0004436[↩][↩]
- Osuntokun O, Olurin O. Filarial worm (Loa loa) in the anterior chamber. Report of two cases. Br J Ophthalmol. 1975 Mar;59(3):166-7. doi: 10.1136/bjo.59.3.166[↩][↩][↩]
- Kagmeni G, Cheuteu R, Bilong Y, Wiedemann P. Anterior Chamber Live Loa loa: Case Report. Clin Med Insights Case Rep. 2016 Jul 14;9:55-6. doi: 10.4137/CCRep.S40012[↩][↩][↩][↩]
- Kumari V, Ahmad S, Singh A, Banerjee T. Presence of adult Loa loa in the anterior chamber of the eye along with microfilaremia from nonendemic region: A rare presentation from India. Tzu Chi Med J. 2019 Sep 16;31(4):283-285. doi: 10.4103/tcmj.tcmj_227_18[↩][↩]
- Barua P, Barua N, Hazarika NK, Das S. Loa loa in the anterior chamber of the eye: a case report. Indian J Med Microbiol. 2005 Jan;23(1):59-60. doi: 10.4103/0255-0857.13877[↩][↩]
- What Causes Loiasis. https://www.cdc.gov/filarial-worms/causes/loiasis.html[↩][↩][↩][↩][↩]
- Loiasis. https://www.cdc.gov/dpdx/loiasis/index.html[↩]
- Gray LE Jr, Ostby J, Furr J, Price M, Veeramachaneni DN, Parks L. Perinatal exposure to the phthalates DEHP, BBP, and DINP, but not DEP, DMP, or DOTP, alters sexual differentiation of the male rat. Toxicol Sci. 2000 Dec;58(2):350-65. doi: 10.1093/toxsci/58.2.350[↩]
- Fonger GC, Hakkinen P, Jordan S, Publicker S. The National Library of Medicine’s (NLM) Hazardous Substances Data Bank (HSDB): background, recent enhancements and future plans. Toxicology. 2014 Nov 5;325:209-16. doi: 10.1016/j.tox.2014.09.003[↩]
- DUKE BO. Studies on the chemoprophylaxis of loiasis. I. Experiments on monkeys, with special reference to diethylcarbamazine (Banocide). Ann Trop Med Parasitol. 1961 Dec;55:447-51. doi: 10.1080/00034983.1961.11686073[↩]
- Nutman TB, Miller KD, Mulligan M, Reinhardt GN, Currie BJ, Steel C, Ottesen EA. Diethylcarbamazine prophylaxis for human loiasis. Results of a double-blind study. N Engl J Med. 1988 Sep 22;319(12):752-6. doi: 10.1056/NEJM198809223191204[↩][↩]
- Albanus, C ∙ Ewers, N ∙ Probst-Kepper, M ∙ et al. Vier deutsche Patienten mit Loa-loa-Filariasis bei Missionstätigkeit im Osten Kameruns Flugmedizin Tropenmedizin Reisemedizin. 2023; 30:11-14[↩]
- Ackley C, Elsheikh M, Zaman S. Scoping review of Neglected Tropical Disease Interventions and Health Promotion: A framework for successful NTD interventions as evidenced by the literature. PLoS Negl Trop Dis. 2021 Jul 6;15(7):e0009278. doi: 10.1371/journal.pntd.0009278[↩]
- Chippaux JP, Bouchité B, Boussinesq M, Ranque S, Baldet T, Demanou M. Impact of repeated large scale ivermectin treatments on the transmission of Loa loa. Trans R Soc Trop Med Hyg. 1998 Jul-Aug;92(4):454-8. doi: 10.1016/s0035-9203(98)91091-4[↩]
- Cho H-Y, Lee Y-J, Shin S-Y, Song H-O, Ahn M-H, Ryu J-S. 2008. Subconjunctival Loa loa with Calabar swelling. J Korean Med Sci 23:731–733. doi: 10.3346/jkms.2008.23.4.731[↩]
- Boussinesq M. Loiasis. Ann Trop Med Parasitol. 2006 Dec;100(8):715-31. doi: 10.1179/136485906X112194[↩][↩]
- Harder, HI & Watson, D. Human filariasis. Identification of species on the basis of staining and other morphologic characteristics of microfilariae. Am J Clin Pathol. 1964; 42:333-339. doi: 10.1093/ajcp/42.4.333[↩]
- Fülleborn, F. Beiträge zur Morphologie und Differentialdiagnose der Mikrofilarien. Archiv Schiffs-u Tropenhyg. 1913; 17:7-72[↩]
- Mischlinger J, Manego RZ, Mombo-Ngoma G, et al. Diagnostic performance of capillary and venous blood samples in the detection of Loa loa and Mansonella perstans microfilaraemia using light microscopy. PLoS Negl Trop Dis. 2021 Aug 16;15(8):e0009623. doi: 10.1371/journal.pntd.0009623[↩]
- Mathison BA, Couturier MRC, Pritt BS. 2019. Diagnostic identification and differentiation of microfilariae. J Clin Microbiol 57:e00706-19. doi: 10.1128/JCM.00706-19[↩][↩]
- Mathison BA, Pritt BS. 2018. Parasitic diseases, p 193–208. In Pritt BS. (ed), Atlas of fundamental infectious diseases histopathology: a guide for daily practice. College of American Pathologists, Northfield, IL.[↩][↩]
- Bench Aids for the diagnosis of filarial infections. https://iris.who.int/bitstream/handle/10665/37156/9241544899_eng.pdf[↩]
- Ekoka Mbassi FA, Mombo-Ngoma G, Ndoumba WN, Yovo EK, Eberhardt KA, Ekoka Mbassi D, Adegnika AA, Agnandji ST, Bouyou-Akotet MK, Ramharter M, Zoleko-Manego R. Performance of Field’s Stain Compared with Conventional Giemsa Stain for the Rapid Detection of Blood Microfilariae in Gabon. Am J Trop Med Hyg. 2022 Jul 5;107(2):383-387. doi: 10.4269/ajtmh.22-0061[↩]
- Datry A, Lecso G, Richard-Lenoble D, Kombila M. Coloration rapide des plasmodies et des microfilaires par les colorants solubles dans l’eau [Rapid staining of Plasmodia and microfilaria with dyes soluble in water]. Med Trop (Mars). 1982 Nov-Dec;42(6):673-6. French.[↩]
- Goussard B, Garin Y, Ivanoff B. Loa loa: a simple method for isolation of microfilariae from blood with production of antigen in extraction medium. Trans R Soc Trop Med Hyg. 1985;79(6):788-91. doi: 10.1016/0035-9203(85)90118-x[↩]
- Petithory JC, Ardoin F, Ash LR, Vandemeulebroucke E, Galeazzi G, Dufour M, Paugam A. Microscopic diagnosis of blood parasites following a cytoconcentration technique. Am J Trop Med Hyg. 1997 Dec;57(6):637-42. doi: 10.4269/ajtmh.1997.57.637[↩]
- Melrose WD, Turner PF, Pisters P, Turner B. An improved Knott’s concentration test for the detection of microfilariae. Trans R Soc Trop Med Hyg. 2000 Mar-Apr;94(2):176. doi: 10.1016/s0035-9203(00)90266-9[↩]
- Kamgno J, Pion SD, Chesnais CB, et al. A Test-and-Not-Treat Strategy for Onchocerciasis in Loa loa-Endemic Areas. N Engl J Med. 2017 Nov 23;377(21):2044-2052. doi: 10.1056/NEJMoa1705026[↩]
- Johnson O, Giorgi E, Fronterrè C, Amoah B, Atsame J, Ella SN, Biamonte M, Ogoussan K, Hundley L, Gass K, Diggle PJ. Geostatistical modelling enables efficient safety assessment for mass drug administration with ivermectin in Loa loa endemic areas through a combined antibody and LoaScope testing strategy for elimination of onchocerciasis. PLoS Negl Trop Dis. 2022 Feb 9;16(2):e0010189. doi: 10.1371/journal.pntd.0010189[↩][↩]
- Pion SD, Nana-Djeunga H, Niamsi-Emalio Y, Chesnais CB, Deléglise H, Mackenzie C, Stolk W, Fletcher DA, Klion AD, Nutman TB, Boussinesq M, Kamgno J. Implications for annual retesting after a test-and-not-treat strategy for onchocerciasis elimination in areas co-endemic with Loa loa infection: an observational cohort study. Lancet Infect Dis. 2020 Jan;20(1):102-109. doi: 10.1016/S1473-3099(19)30554-7[↩]
- Emukah E, Rakers LJ, Kahansim B, et al. In Southern Nigeria Loa loa Blood Microfilaria Density is Very Low Even in Areas with High Prevalence of Loiasis: Results of a Survey Using the New LoaScope Technology. Am J Trop Med Hyg. 2018 Jul;99(1):116-123. doi: 10.4269/ajtmh.18-0163[↩]
- Touré FS, Mavoungou E, Deloron P, Egwang TG. Analyse comparative de deux méthodes diagnostiques de la loase humaine: sérologie IgG4 et PCR nichée [Comparative analysis of 2 diagnostic methods of human loiasis: IgG4 serology and nested PCR]. Bull Soc Pathol Exot. 1999 Jul;92(3):167-70. French.[↩]
- Touré FS, Egwang TG, Millet P, Bain O, Georges AJ, Wahl G. IgG4 serology of loiasis in three villages in an endemic area of south-eastern Gabon. Trop Med Int Health. 1998 Apr;3(4):313-7. doi: 10.1046/j.1365-3156.1998.00224.x[↩]
- Akue JP, Hommel M, Devaney E. IgG subclass recognition of Loa loa antigens and their correlation with clinical status in individuals from Gabon. Parasite Immunol. 1998 Aug;20(8):387-93. doi: 10.1046/j.1365-3024.1998.00172.x[↩]
- Gobbi F, Buonfrate D, Boussinesq M, Chesnais CB, Pion SD, Silva R, Moro L, Rodari P, Tamarozzi F, Biamonte M, Bisoffi Z. Performance of two serodiagnostic tests for loiasis in a Non-Endemic area. PLoS Negl Trop Dis. 2020 May 26;14(5):e0008187. doi: 10.1371/journal.pntd.0008187[↩][↩]
- Veletzky L, Eberhardt KA, Hergeth J, et al. Distinct loiasis infection states and associated clinical and hematological manifestations in patients from Gabon. PLoS Negl Trop Dis. 2022 Sep 19;16(9):e0010793. doi: 10.1371/journal.pntd.0010793[↩]
- Pedram B, Pasquetto V, Drame PM, Ji Y, Gonzalez-Moa MJ, Baldwin RK, Nutman TB, Biamonte MA. A novel rapid test for detecting antibody responses to Loa loa infections. PLoS Negl Trop Dis. 2017 Jul 27;11(7):e0005741. doi: 10.1371/journal.pntd.0005741[↩]
- Ella SN, Ogoussan K, Gass K, Hundley L, Diggle PJ, Johnson O, Biamonte M, Atsame J. An Integrated District Mapping Strategy for Loiasis to Enable Safe Mass Treatment for Onchocerciasis in Gabon. Am J Trop Med Hyg. 2021 Nov 15;106(2):732-739. doi: 10.4269/ajtmh.21-0799[↩]
- Davi, SD ∙ Ramharter, M ∙ Nordmann, T. Loiasis—Eine extrem vernachlässigte Tropenerkrankung Flugmedizin Tropenmedizin Reisemedizin. 2023; 30:15-19[↩]
- WERNER H. Demonstration einer mit Schmalfilm festgehaltenen subconjunctivalen Filaria Loa [Demonstration of subconjunctival Filaria loa with an 8 mm. film recording]. Ophthalmologica. 1959 Mar;137(3):160-2. German. doi: 10.1159/000303506[↩]
- Touré FS, Bain O, Nerrienet E, Millet P, Wahl G, Toure Y, Doumbo O, Nicolas L, Georges AJ, McReynolds LA, Egwang TG. Detection of Loa loa-specific DNA in blood from occult-infected individuals. Exp Parasitol. 1997 Jul;86(3):163-70. doi: 10.1006/expr.1997.4168[↩]
- Gerber V, Greigert V, Pfaff A, Jaennel J, Marteau A, Argy N, Candolfi E, Abou-Bacar A, Brunet J. Imported occult loiasis: diagnostic algorithm proposal for a difficult diagnosis. J Travel Med. 2022 Nov 4;29(7):taab178. doi: 10.1093/jtm/taab178[↩]
- Mackenzie C.D., Geary T.G., Gerlach J.A. Possible pathogenic pathways in the adverse clinical events seen following ivermectin administration to onchocerciasis patients. Filaria J. 2003;2(Suppl. 1):S5. doi: 10.1186/1475-2883-2-S1-S5[↩][↩]
- Klion AD, Massougbodji A, Horton J, Ekoué S, Lanmasso T, Ahouissou NL, Nutman TB. Albendazole in human loiasis: results of a double-blind, placebo-controlled trial. J Infect Dis. 1993 Jul;168(1):202-6. doi: 10.1093/infdis/168.1.202[↩]
- Klion AD, Horton J, Nutman TB. Albendazole therapy for loiasis refractory to diethylcarbamazine treatment. Clin Infect Dis. 1999 Sep;29(3):680-2. doi: 10.1086/598654[↩]
- Gobbi F, Buonfrate D, Tamarozzi F, Degani M, Angheben A, Bisoffi Z. Efficacy of High-Dose Albendazole with Ivermectin for Treating Imported Loiasis, Italy. Emerg Infect Dis. 2019 Aug;25(8):1574-1576. doi: 10.3201/eid2508.190011[↩][↩]
- Tamarozzi F, Horton J, Muhtarov M, Ramharter M, Siles-Lucas M, Gruener B, Vuitton DA, Bresson-Hadni S, Manciulli T, Brunetti E. A case for adoption of continuous albendazole treatment regimen for human echinococcal infections. PLoS Negl Trop Dis. 2020 Sep 17;14(9):e0008566. doi: 10.1371/journal.pntd.0008566[↩]
- Volpicelli L, De Angelis M, Morano A, Biliotti E, Franchi C, Gabrielli S, Mattiucci S, Di Bonaventura C, Taliani G. Encephalopathy in a patient with loiasis treated with albendazole: A case report. Parasitol Int. 2020 Apr;75:102006. doi: 10.1016/j.parint.2019.102006[↩]
- Métais A, Michalak S, Rousseau A. Albendazole-related Loa Loa encephalopathy. IDCases. 2021 Jan 6;23:e01033. doi: 10.1016/j.idcr.2020.e01033[↩][↩]
- Maizels RM, Denham DA. Diethylcarbamazine (DEC): immunopharmacological interactions of an anti-filarial drug. Parasitology. 1992;105 Suppl:S49-60. doi: 10.1017/s0031182000075351[↩]
- WOODRUFF AW. Destruction of microfilariae of Loa loa in the liver in loiasis treated with banocide (hetrazan). Trans R Soc Trop Med Hyg. 1951 Feb;44(4):470-80. doi: 10.1016/s0035-9203(51)80025-7[↩]
- Verma S, Kashyap SS, Robertson AP, Martin RJ. Diethylcarbamazine activates TRP channels including TRP-2 in filaria, Brugia malayi. Commun Biol. 2020 Jul 28;3(1):398. doi: 10.1038/s42003-020-01128-4. Erratum in: Commun Biol. 2020 Aug 12;3(1):449. doi: 10.1038/s42003-020-01194-8[↩]
- Klion AD, Ottesen EA, Nutman TB. Effectiveness of diethylcarbamazine in treating loiasis acquired by expatriate visitors to endemic regions: long-term follow-up. J Infect Dis. 1994 Mar;169(3):604-10. doi: 10.1093/infdis/169.3.604[↩]
- Jaccard A, Lortholary O, Visser H. Diethylcarbamazine and human loiasis. N Engl J Med. 1989 Feb 2;320(5):320. doi: 10.1056/NEJM198902023200519[↩]
- Boulesteix, J ∙ Carme, B. Encephalite au cours du traitement de la filariose a Loa loa par la diethylcarbamazine. Bull Soc Pathol Exot. 1986; 43:279-282[↩][↩]
- Stanley SL Jr, Kell O. Ascending paralysis associated with diethylcarbamazine treatment of M. loa loa infection. Trop Doct. 1982 Jan;12(1):16-9. doi: 10.1177/004947558201200107[↩]
- Carme B, Boulesteix J, Boutes H, Puruehnce MF. Five cases of encephalitis during treatment of loiasis with diethylcarbamazine. Am J Trop Med Hyg. 1991 Jun;44(6):684-90. doi: 10.4269/ajtmh.1991.44.684[↩][↩]
- Herrick JA, Legrand F, Gounoue R, Nchinda G, Montavon C, Bopda J, Tchana SM, Ondigui BE, Nguluwe K, Fay MP, Makiya M, Metenou S, Nutman TB, Kamgno J, Klion AD. Posttreatment Reactions After Single-Dose Diethylcarbamazine or Ivermectin in Subjects With Loa loa Infection. Clin Infect Dis. 2017 Apr 15;64(8):1017-1025. doi: 10.1093/cid/cix016[↩]
- Gentilini M, Carme B. Traitement des filarioses en pratique hospitalière. Complications – résultats [Treatment of filariases in a hospital setting. Complications – results]. Ann Soc Belg Med Trop. 1981 Jun;61(2):319-26. French.[↩]
- Duke BO, Thylefors B. Need for caution in use of DEC for treatment of onchocerciasis. Trop Doct. 1986 Apr;16(2):69-70.[↩]
- Bird AC, el-Sheikh H, Anderson J, Fuglsang H. Changes in visual function and in the posterior segment of the eye during treatment of onchocerciasis with diethylcarbamazine citrate. Br J Ophthalmol. 1980 Mar;64(3):191-200. doi: 10.1136/bjo.64.3.191[↩]
- Taylor HR, Greene BM. Ocular changes with oral and transepidermal diethylcarbamazine therapy of onchocerciasis. Br J Ophthalmol. 1981 Jul;65(7):494-502. doi: 10.1136/bjo.65.7.494[↩]
- Boussinesq M. Loiasis: new epidemiologic insights and proposed treatment strategy. J Travel Med. 2012 May-Jun;19(3):140-3. doi: 10.1111/j.1708-8305.2012.00605.x[↩][↩]
- Geary TG, Moreno Y. Macrocyclic lactone anthelmintics: spectrum of activity and mechanism of action. Curr Pharm Biotechnol. 2012 May;13(6):866-72. doi: 10.2174/138920112800399077[↩]
- Richard-Lenoble D, Kombila M, Rupp EA, Pappayliou ES, Gaxotte P, Nguiri C, Aziz MA. Ivermectin in loiasis and concomitant O. volvulus and M. perstans infections. Am J Trop Med Hyg. 1988 Nov;39(5):480-3. doi: 10.4269/ajtmh.1988.39.480[↩]
- Kamgno J, Pion SD, Tejiokem MC, Twum-Danso NA, Thylefors B, Boussinesq M. Randomized, controlled, double-blind trial with ivermectin on Loa loa microfilaraemia: efficacy of a low dose (approximately 25 microg/kg) versus current standard dose (150 microg/kg). Trans R Soc Trop Med Hyg. 2007 Aug;101(8):777-85. doi: 10.1016/j.trstmh.2007.03.018[↩]
- Kombila M, Duong TH, Ferrer A, Perret JL, Marion MC, Nguiri C, Gaxotte P, Manfoumbi M, Richard-Lenoble D. Short- and long-term action of multiple doses of ivermectin on loiasis microfilaremia. Am J Trop Med Hyg. 1998 Apr;58(4):458-60. doi: 10.4269/ajtmh.1998.58.458[↩]
- Boussinesq M, Gardon J, Gardon-Wendel N, Kamgno J, Ngoumou P, Chippaux JP. Three probable cases of Loa loa encephalopathy following ivermectin treatment for onchocerciasis. Am J Trop Med Hyg. 1998 Apr;58(4):461-9. doi: 10.4269/ajtmh.1998.58.461[↩]
- Boussinesq M, Kamgno J, Pion SD, Gardon J. What are the mechanisms associated with post-ivermectin serious adverse events? Trends Parasitol. 2006 Jun;22(6):244-6. doi: 10.1016/j.pt.2006.04.006[↩]
- Boullé C, Chesnais CB, Kamgno J, Gardon J, Chippaux JP, Ranque S, Garcia A, Pion SD, Boussinesq M. Evaluating post-treatment Loa loa microfilarial densities to classify serious adverse events caused by ivermectin: a retrospective analysis. Lancet Microbe. 2023 Feb;4(2):e93-e101. doi: 10.1016/S2666-5247(22)00331-7[↩]
- Campillo JT, Boussinesq M, Bertout S, Faillie JL, Chesnais CB. Serious adverse reactions associated with ivermectin: A systematic pharmacovigilance study in sub-Saharan Africa and in the rest of the World. PLoS Negl Trop Dis. 2021 Apr 20;15(4):e0009354. doi: 10.1371/journal.pntd.0009354[↩]
- Chesnais CB, Pion SD, Boullé C, Gardon J, Gardon-Wendel N, Fokom-Domgue J, Kamgno J, Boussinesq M. Individual risk of post-ivermectin serious adverse events in subjects infected with Loa loa. EClinicalMedicine. 2020 Oct 10;28:100582. doi: 10.1016/j.eclinm.2020.100582[↩]
- Akue JP, Nkoghe D, Padilla C, Moussavou G, Moukana H, Mbou RA, Ollomo B, Leroy EM. Epidemiology of concomitant infection due to Loa loa and Mansonella perstans in Gabon. PLoS Negl Trop Dis. 2011 Oct;5(10):e1329. doi: 10.1371/journal.pntd.0001329[↩]
- Hovette P, Debonne JM, Touze JE, Gaxotte P, Imbert P, Fourcade L, Laroche R. Efficacy of ivermectin treatment of Loa loa filariasis patients without microfilaraemias. Ann Trop Med Parasitol. 1994 Feb;88(1):93-4. doi: 10.1080/00034983.1994.11812842[↩]
- Gobbi F, Bottieau E, Bouchaud O, Buonfrate D, Salvador F, Rojo-Marcos G, Rodari P, Clerinx J, Treviño B, Herrera-Ávila JP, Neumayr A, Calleri G, Angheben A, Rothe C, Zammarchi L, Guerriero M, Bisoffi Z. Comparison of different drug regimens for the treatment of loiasis-A TropNet retrospective study. PLoS Negl Trop Dis. 2018 Nov 1;12(11):e0006917. doi: 10.1371/journal.pntd.0006917[↩]
- Zoleko-Manego R, Kreuzmair R, Veletzky L, et al. Efficacy, safety, and tolerability of albendazole and ivermectin based regimens for the treatment of microfilaraemic loiasis in adult patients in Gabon: A randomized controlled assessor blinded clinical trial. PLoS Negl Trop Dis. 2023 Aug 28;17(8):e0011584. doi: 10.1371/journal.pntd.0011584[↩]
- Chandenier, J ∙ Pillier-Loriette, C ∙ Datry, A ∙ et al. Value of cytapheresis in the treatment of loaiasis with high blood microfilaria levels. Results in 7 cases. Bull Soc Pathol Exot. 1987; 80:624-633 (in French).[↩]
- Muylle L, Taelman H, Moldenhauer R, Van Brabant R, Peetermans ME. Usefulness of apheresis to extract microfilarias in management of loiasis. Br Med J (Clin Res Ed). 1983 Aug 20;287(6391):519-20. doi: 10.1136/bmj.287.6391.519[↩]
- Abel L, Ioly V, Jeni P, Carbon C, Bussel A. Apheresis in the management of loiasis with high microfilariaemia and renal disease. Br Med J (Clin Res Ed). 1986 Jan 4;292(6512):24. doi: 10.1136/bmj.292.6512.24[↩]
- Zhao Y, Alexander B, Bailey JA, Welch L, Greene M, Vauthrin M, Mitchell M, Weinstein R. Therapeutic apheresis using a mononuclear cell program to lower the microfilaria burden of a 23-year-old African woman with loiasis. J Clin Apher. 2017 Jun;32(3):200-202. doi: 10.1002/jca.21479[↩]
- Norgan AP, Juskewitch JE, Pritt BS, Winters JL. The use of cytapheresis in the treatment of infectious diseases. J Clin Apher. 2018 Aug;33(4):529-537. doi: 10.1002/jca.21620. Epub 2018 Feb 28. Erratum in: J Clin Apher. 2018 Dec;33(6):685-686. doi: 10.1002/jca.21668[↩]
- Odedra A, Lalloo DG, Kennedy G, Llewellyn S, McCarthy JS. Safety and effectiveness of apheresis in the treatment of infectious diseases: A systematic review. J Infect. 2019 Dec;79(6):513-520. doi: 10.1016/j.jinf.2019.09.014[↩]
- Legrand F, Herrick J, Makiya M, Ramanathan R, Thompson R, Rampertaap S, Stoddard J, Ware J, Fay MP, Holland-Thomas N, Nutman TB, Klion AD. A Randomized, Placebo-controlled, Double-blind Pilot Study of Single-dose Humanized Anti-IL5 Antibody (Reslizumab) for the Reduction of Eosinophilia Following Diethylcarbamazine Treatment of Loa loa Infection. Clin Infect Dis. 2021 Oct 5;73(7):e1624-e1631. doi: 10.1093/cid/ciaa1365[↩]
- THOMPSON JH. ACTH as an adjunct to the treatment of loaiasis. Am J Trop Med Hyg. 1956 Nov;5(6):1103-5. doi: 10.4269/ajtmh.1956.5.1103[↩]
- GALLIARD H, LARIVIERE M. Recherches sur l’eosinophilie au cours de la filariose a Loa loa et de son traitement; éffets de l’A.C.T.H. et resultats des tests d’insuffisance surrénale [Eosinophilia in Loa filariasis and its treatment; effects of ACTH and results of adrenal insufficiency tests]. Ann Parasitol Hum Comp. 1953;28(4):312-20. French.[↩]
- Herrick JA, Makiya MA, Holland-Thomas N, Klion AD, Nutman TB. Infection-associated Immune Perturbations Resolve 1 Year Following Treatment for Loa loa. Clin Infect Dis. 2021 Mar 1;72(5):789-796. doi: 10.1093/cid/ciaa137[↩]
- Sachs HG, Heep M, Gabel VP. Chirurgische Wurmentfernung bei Loa-Loa-Ophthalmie [Surgical worm extraction in loa loa ophthalmia]. Klin Monbl Augenheilkd. 1998 Dec;213(6):367-9. German. doi: 10.1055/s-2008-1035005[↩]
- Nayak B, Sinha S, Nayak L. Loa loa in the vitreous cavity of the eye. BMJ Case Rep. 2016 Jan 8;2016:bcr2015213879. doi: 10.1136/bcr-2015-213879[↩]



{kind=link}