
Contents
What is malignant hypertension
Malignant hypertension also called hypertensive emergency or hypertensive crisis, is very high blood pressure that comes on suddenly and quickly. Malignant hypertension is a medical emergency. Malignant hypertension can be further classified as a hypertensive emergency when severe elevation in blood pressure is associated with end-organ damage, or hypertensive urgency when severe hypertension occurs without it. Most patients have persistently-high blood pressure for years before presenting with hypertensive emergency.
Malignant hypertension is a term that has been used to describe patients with elevated blood pressure and multiple complications with a poor prognosis. Today, the term hypertensive crisis is used to describe patients who present with severe blood pressure elevations as follow 1:
- Systolic blood pressure (SBP) greater than 180 mm Hg
- Diastolic blood pressure (DBP) greater than 120 mm Hg)
Hypertensive emergencies occur when a relatively rapid elevation of blood pressure develops in a short period. Increase in systemic vascular resistance by an increase in vasoconstriction mechanisms through renin-angiotensin activation, pressure natriuresis, hypoperfusion, and ischemia are the most common culprits of end-organ damage 1.
Malignant hypertension affects a small number of people with high blood pressure, including children and adults. Malignant hypertension is more common in younger adults, especially African American men.
Hypertensive emergencies are unusual, with a projected incidence of 1 to 2 cases per million per year 1. A recent investigation showed that the estimated number of visits due to malignant hypertension and the rate per million per adult, emergency department (ED) visits have more than doubled from 2006 to 2013.
Prompt treatment of blood pressure can prevent a hypertensive emergency and consequently, serious life-threatening complications 2. Few examples include eclampsia (2%), cerebral infarction (39%), and acute pulmonary edema (25%) 1.
You will need to stay in the hospital until your severe high blood pressure is under control. You will receive medicines through a vein (IV) to reduce your blood pressure.
If there is fluid in your lungs, you will be given medicines called diuretics, which help the body remove fluid. Your doctor may give you medicines to protect your heart if you have signs of heart damage.
It is generally not recommended to decrease the blood pressure too quickly or too much as ischemic damage can occur in vascular territories that have become habituated with the elevated level of blood pressure. For most hypertensive emergencies, the mean arterial pressure (MAP) should be reduced gradually by approximately 10 to 20% within the first hour, and by a further 5% to 15% over the next 24 hours, with a final goal of approximately 25% reduction compared with baseline 1.
After your severe high blood pressure is under control, blood pressure medicines taken by mouth can control blood pressure. Your medicine may need to be changed sometimes. High blood pressure can be difficult to control.
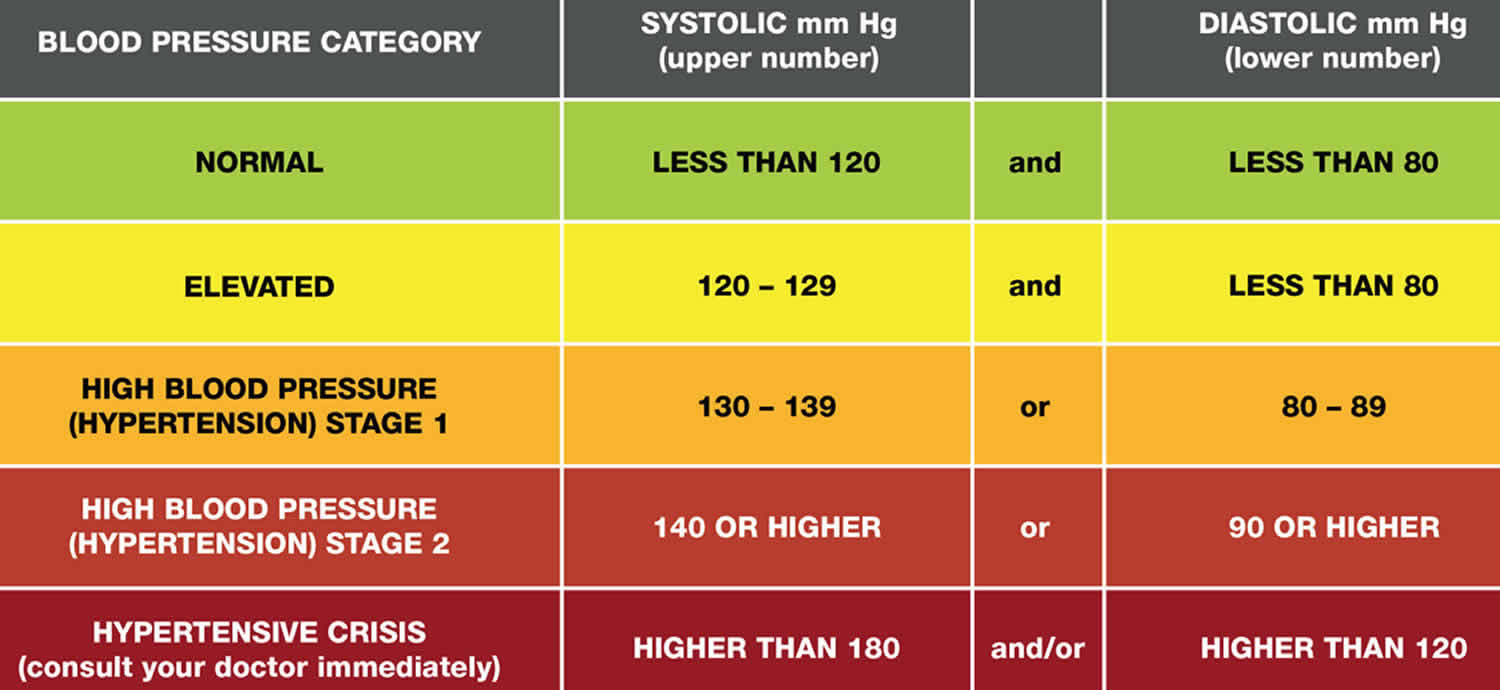
Figure 1. Blood pressure categories
Malignant hypertension vs Hypertensive emergency
Malignant hypertension is a medical emergency. Go to the emergency room or call your local emergency number if you have symptoms of malignant hypertension. Malignant hypertension is an emergency condition that can be life threatening.
Call your health care provider if you know you have poorly controlled high blood pressure.
Benign vs malignant hypertension
‘Benign hypertension’ is more commonly called ‘primary hypertension’ or ‘essential hypertension’, which means there’s no identifiable cause of high blood pressure. Benign hypertension tends to develop gradually over many years. On the other hand, malignant hypertension can be caused by benign hypertension (primary hypertension) or caused by an underlying condition, called secondary hypertension, that tends to appear suddenly and cause higher blood pressure than does benign hypertension (primary hypertension).
Hypertension or high blood pressure, rarely has noticeable symptoms. But if untreated, it increases your risk of serious problems such as heart attacks and strokes. The only way to find out if your blood pressure is high is to have your blood pressure checked.
If your blood pressure is too high, it puts extra strain on your blood vessels, heart and other organs, such as the brain, kidneys and eyes.
Persistent high blood pressure can increase your risk of a number of serious and potentially life-threatening conditions, such as:
- heart disease
- heart attacks
- strokes
- heart failure
- peripheral arterial disease
- aortic aneurysms
- kidney disease
- vascular dementia
If you have high blood pressure, reducing it even a small amount can help lower your risk of these conditions.
Causes of malignant hypertension
There are multiple causes of malignant hypertension (hypertensive crisis) including the following 1:
- Medication noncompliance
- Renovascular diseases, such as renal artery stenosis, polyarteritis nodosa, and Takayasu arteritis
- Renal parenchymal disease including glomerulonephritis, tubulointerstitial nephritis, systemic sclerosis, hemolytic-uremic syndrome, systemic lupus erythematosus
- Endocrine dysfunction, such as pheochromocytoma, Cushing disease, primary hyperaldosteronism, renin-secreting tumor
- Coarctation of aorta; drugs or other exposures, including cocaine, phencyclidine, sympathomimetics, erythropoietin, cyclosporine
- Antihypertensive medication withdrawal
- Amphetamines
- Central nervous system disorders, such as head injury, cerebral infarction, and cerebral hemorrhage.
Malignant hypertension also occurs in people with:
- Collagen vascular disorders (such as systemic lupus erythematosus, systemic sclerosis, and periarteritis nodosa)
- Kidney problems
- Pregnancy-induced high blood pressure (toxemia)
You are at high risk for malignant hypertension if you smoke and if you have had:
- Kidney failure
- Renal hypertension caused by renal artery stenosis
Malignant hypertension prevention
If you have high blood pressure, carefully monitor your blood pressure and take your medicines properly to help reduce your risk. Eat a healthy diet that is low in salt and fat.
Malignant hypertension symptoms
Symptoms of malignant hypertension include:
- Blurred vision
- Change in mental status, such as anxiety, confusion, decreased alertness, decreased ability to concentrate, fatigue, restlessness, sleepiness, or stupor
- Chest pain (feeling of crushing or pressure)
- Cough
- Headache
- Nausea or vomiting
- Numbness of the arms, legs, face, or other areas
- Reduced urine output
- Seizure
- Shortness of breath
- Weakness of the arms, legs, face, or other areas
Malignant hypertension possible complications
Multiple complications can arise when target organs are affected, including encephalopathy, intracerebral hemorrhage, acute myocardial infarction, acute heart failure, pulmonary edema, unstable angina, dissecting aortic aneurysm, acute kidney injury, and vision loss.
These complications may occur:
- Brain damage (stroke, seizures)
- Heart damage, including: heart attack, angina (chest pain due to narrowed blood vessels or weakened heart muscle), heart rhythm disturbances
- Kidney failure
- Permanent blindness
- Fluid in the lungs
Malignant hypertension diagnosis
Initial questioning should focus on finding indicators related to end-organ damage including a headache, nausea or vomiting, visual disturbances, chest or back pain, dyspnea, orthopnea, or visual disturbances. Review all prescription and nonprescription medications, adherence, and time from the last dose. Ask about recreational drug use, such as amphetamines, cocaine, phencyclidine.
On physical exam, confirm blood pressure on both arms using appropriately-sized blood pressure cuff. Funduscopic exam findings may include hemorrhages, exudates or papilledema. Assess for murmurs and gallops or other signs of heart failure. Look for evidence of pulmonary edema, abdominal bruits. Neurological findings can include stupor, seizures, delirium, agitation 3.
A physical exam commonly shows:
- Extremely high blood pressure (blood pressure greater than 180/120 mm Hg)
- Swelling in the lower legs and feet
- Abnormal heart sounds and fluid in the lungs
- Changes in thinking, sensation, and reflexes
An eye exam will reveal changes that indicate high blood pressure, including:
- Bleeding of the retina (back part of the eye)
- Narrowing of the blood vessels in the retina
- Swelling of the optic nerve
- Other problems with the retina
Tests to determine damage to the kidneys may include:
- Arterial blood gas analysis
- BUN (blood urea nitrogen)
- Creatinine
- Urinalysis
- Kidney ultrasound
A chest x-ray may show congestion in the lungs and an enlarged heart.
Malignant hypertension may also affect the results of these tests:
- Level of aldosterone (a hormone from the adrenal gland)
- Cardiac enzymes (markers of heart damage)
- Chest x-Ray
- CT/MRI of the brain, when head injury, neurologic symptoms, hypertensive retinopathy, nausea, or vomiting are present
- Contrast CT/MRI of the chest or TEE, if aortic dissection is suspected
- Electrocardiogram (EKG)
- Renin level
- Urinary sediment
It is often easiest to categorize malignant hypertension by the organ that is being damaged. The evaluation above can usually identify the at-risk target organ and can direct both, the target blood pressure and the promptness with which the target is achieved.
Malignant hypertension treatment
Adequate therapy, including the choice of the medication and the blood pressure target, changes depending on the specific hypertensive emergency and the affected organ 4.
It is not recommended to decrease the blood pressure too fast or too much, as ischemic damage can occur in vascular territories that have become habituated with the elevated level of blood pressure. For the majority of hypertensive emergencies, mean arterial pressure (MAP) should be reduced by approximately 10 to 20% within the first hour and by another 5% to 15% over the next 24 hours 1. This often results in a target blood pressure of less than 180/120 mm Hg for the first hour and less than 160/110 mm Hg for the next 24 hours, but rarely less than 130/80 mm Hg during that time frame 1.
Common intravenous (IV) medications and doses used to treat hypertensive emergencies include 1:
- Nicardipine, initial infusion rate 5 mg per hour, increasing by 2.5 mg per hour every 5 minutes to a maximum of 15 mg per hour
- Sodium nitroprusside, 0.3 to 0.5 mcg/kg/minute, increase by 0.5 mcg/kg per minute every few minutes as needed to a maximum dose of 10 mcg/kg per minute
- Labetalol 10 to 20 mg IV followed by bolus doses of 20 to 80 mg at 10-minute intervals until a target blood pressure is reached to a maximum 300-mg cumulative dose
- Esmolol, initial loading dose 500 mcg/kg/minute over 1 minute, then 50 to 100 mcg/kg/minute to a maximum dose of 300 mcg/kg per minute.
If there is any possibility of over or underestimation of blood pressure using frequent noninvasive cuff measurements or if the end-organ damage is life-threatening, consider arterial catheterization for precise, second-to-second measurements allowing for more careful medication titration.
The major exceptions to gradual blood pressure lowering over the first day are 1:
- Acute Phase of an Ischemic Stroke: The blood pressure is usually not treated unless it is greater than 185/110 mmHg in patients who reperfusion therapy could be an option or greater than 220/120 mm Hg in patients who might not qualify for it. Consider labetalol or nicardipine infusion.
- Acute Aortic Dissection: The Sblood pressure should be lowered to 120 mm Hg within 20 minutes, and a target heart rate around 60 beats per minute, to reduce aortic shearing forces. Treatment usually requires a beta blocker and a vasodilator. Options include esmolol, nicardipine, or nitroprusside.
- An Intracerebral Hemorrhage: The goals of therapy are different and depend on the location and surgical approach.
- Acute Myocardial Ischemia: Nitroglycerin is the drug of choice; do not use if the patient has taken phosphodiesterase inhibitors, including sildenafil or tadalafil, within the past 48 hours.
After a suitable period, often 8 to 24 hours, of blood pressure control at a target, oral medications are usually given, and the initial intravenous therapy is tapered and discontinued.
Malignant hypertension prognosis
Many body systems are at serious risk from the extreme rise in blood pressure. Organs including the brain, eyes, blood vessels, heart, and kidneys may be damaged.
The blood vessels of the kidney are very likely to be damaged by high blood pressure. Kidney failure may develop, which may be permanent. If this happens, you may need dialysis (machine that removes waste products from blood).
If treated right away, malignant hypertension can often be controlled without causing permanent problems. If it is not treated right away, it can be fatal. However, most patients with severely elevated blood pressure have no acute end-organ damage (hypertensive urgency). Nevertheless, some patients have signs and symptoms of acute, ongoing injury, which is recognized as malignant hypertension or hypertensive emergency.
The outcome for most patients with malignant hypertension in the short term is good but in the long term exacerbations are common. Strokes, vision loss, kidney damage and adverse cardiac events are known to occur in a number of patients who are not compliant with therapy 5.
- Naranjo M, Paul M. Malignant Hypertension. [Updated 2019 Feb 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507701[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Yong B, Power DA. Malignant Hypertension Causing a Pulmonary-Renal Syndrome. Case Rep Nephrol. 2018;2018:3273695[↩]
- Kimura N, Takekoshi K, Naruse M. Risk Stratification on Pheochromocytoma and Paraganglioma from Laboratory and Clinical Medicine. J Clin Med. 2018 Aug 27;7, 9[↩]
- Smith M. Refractory Intracranial Hypertension: The Role of Decompressive Craniectomy. Anesth. Analg. 2017 Dec;125(6):1999-2008[↩]
- Liu S, Song A, Zhou X, Kong X, Li WA, Wang Y, Liu Y. Malignant pheochromocytoma with multiple vertebral metastases causing acute incomplete paralysis during pregnancy: Literature review with one case report. Medicine (Baltimore). 2017 Nov;96(44):e8535.[↩]





{kind=link}