Contents
What is meatal stenosis
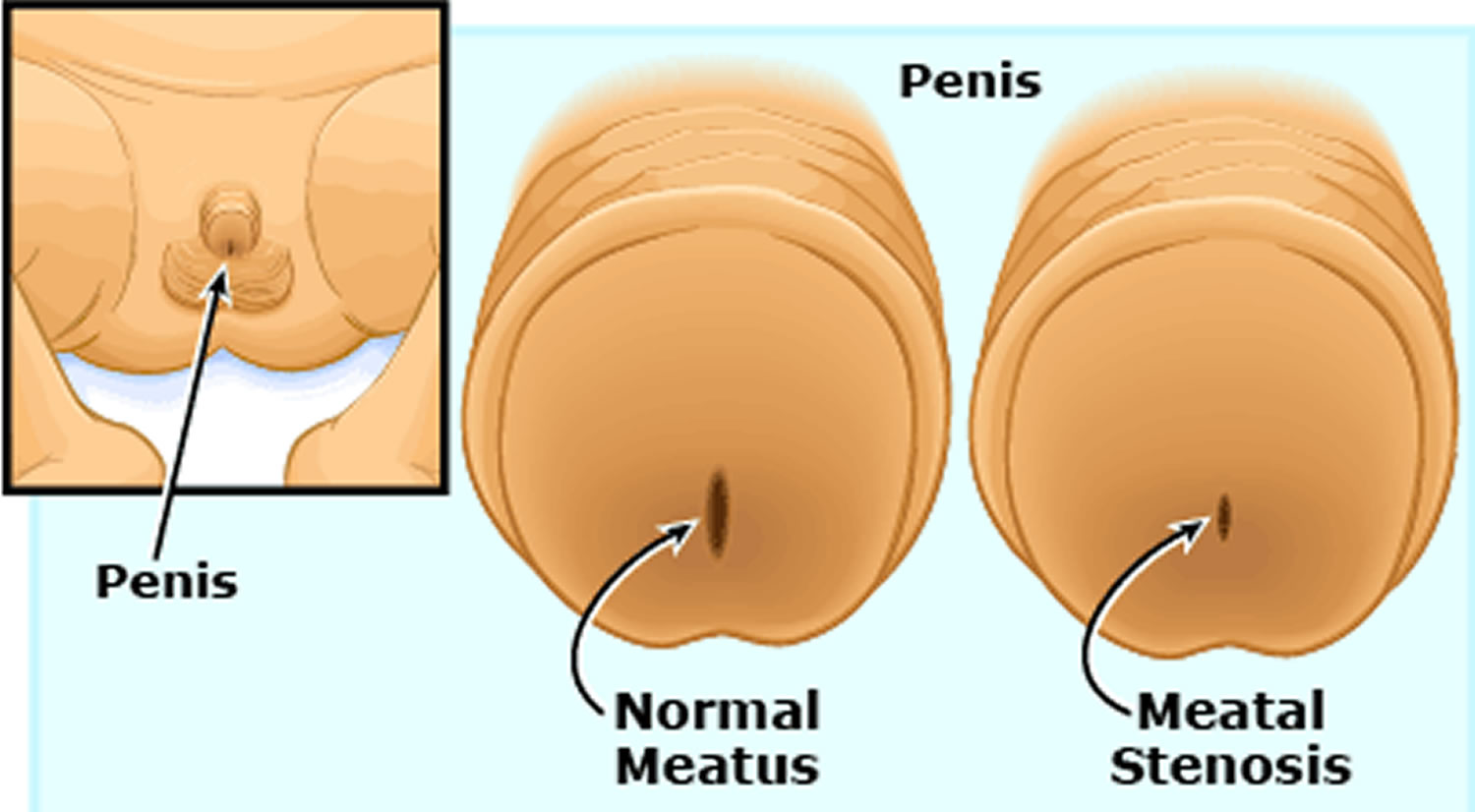
Meatal stenosis is a narrowing of the opening of the urethra, the tube through which urine leaves the body. Urinary meatal stenosis can affect both males and females. It is more common in males.
In males, it is often caused by swelling and irritation (inflammation) after a newborn is circumcised. This leads to abnormal tissue growth and scarring across the opening of the urethra. In most cases, the problem is not found until the child is toilet trained. If your baby boy has recently been circumcised, try to keep the diaper clean and dry. Avoid exposing the newly circumcised penis to any irritants. They may cause inflammation and narrowing of the opening. A systematic review and meta-analysis by Morris et al. 1 found that application of petroleum jelly to the glans after circumcision was associated with a reduction in the risk of meatal stenosis (relative risk, 0.024).
Meatal stenosis affects 9-20% of males who are circumcised 2. Children who are not toilet-trained are more prone to develop meatal stenosis after circumcision because of exposure of the meatus to urine in diapers. Most children who are toilet-trained can verbalize their difficulties during micturition to their caregivers. Meatal stenosis has no racial predilection. The condition can occur in circumcised males independent of ethnicity.
Surgery on the urethra, chronic catheterization, or other medical instruments in the urethra may also lead to meatal stenosis.
In females, meatal stenosis is present at birth (congenital). Less commonly, meatal stenosis may also affect adult women.
Meatal stenosis risks in female include:
- Having many endoscopic procedures (cystoscopy)
- Severe, long-term atrophic vaginitis
Meatal stenosis causes
In a child who is circumcised, persistent exposure of the meatus to urine and mechanical trauma from rubbing against a wet diaper results in ammoniac dermatitis, loss of meatal epithelium, and fusion of its ventral edges. This results in a pinpoint orifice at the tip of the head of the penis (glans penis) 2.
Other causes of meatal stenosis include the following:
- Previous hypospadias repair
- Trauma
- Prolonged catheterization
- Balanitisxerotica obliterans (BXO), an unusual condition that causes a whitish discoloration and dry appearance of the head of the penis 3
A 10-year retrospective series of boys with balanitis xerotica obliterans at Boston Children’s Hospital included 41 patients with a median age of 10.6 years, of whom 85% were aged 8-13 years 4. The disease process was found to involve the prepuce, the glans, and sometimes the urethra. The most common referral diagnoses included phimosis (52%), balanitis (13%), and buried penis (10%). In 46% of the patients, circumcision was curative; 27% (11 patients) had meatal involvement that was treated by meatotomy and meatoplasty, and 22% required extensive plastic procedures of the penis, including buccal mucosal grafts.
Meatal stenosis occurs in as many as 20% of pediatric patients with balanitis xerotica obliterans. Although balanitis xerotica obliterans is difficult to treat, meatotomy typically produces a durable treatment of the meatal stenosis.
Meatal stenosis symptoms
Urethral meatal stenosis symptoms include:
- Abnormal strength and direction of urine stream
- Bed wetting
- Bleeding (hematuria) at end of urination
- Discomfort with urination or straining with urination
- Incontinence (day or night)
- Visible narrow opening in boys
Meatal stenosis complications
Urinary meatal stenosis complications may include:
- Difficult-to-aim (upward-deflected), high-velocity (long-distance) stream of urine; the misdirection of the urine stream is the most important feature of the history, in that this is what is most likely related to meatal stenosis and is most reliably corrected by meatotomy or meatoplasty
- Abnormal urine stream
- Blood in the urine
- Frequent urination
- Painful urination or pain upon initiation of urination
- Urinary incontinence
- Urinary tract infections
- Damage to bladder or kidney function in severe cases
It is important to note that symptoms other than misdirection of the urinary stream (eg, pain, urinary hesitancy, and frequency) may be signs of underlying voiding dysfunction rather than results of meatal stenosis. Consequently, these symptoms may not improve after correction of the meatal stenosis.
Meatal stenosis diagnosis
In boys, a history and physical exam are enough to make the diagnosis of urinary meatal stenosis.
In girls, a voiding cystourethrogram may be done. The narrowing may also be found during a physical exam, or when a health care provider tries to place a Foley catheter. Litvak et al. 5 report that the meatus in children younger than 1 year will accept a lubricated 5-French feeding tube; they also report that in children aged 1-6 years, an 8-French feeding tube should pass without difficulty.
Other tests may include:
- Complete blood count (CBC)
- Kidney and bladder ultrasound
- Urine analysis
- Urine culture
Meatal stenosis treatment
In females, meatal stenosis is most often treated in the provider’s office. This is done using local anesthesia to numb the area. Then the opening of the urethra is widened (dilated) with special instruments.
In boys, a minor outpatient surgery called meatoplasty or meatotomy is the treatment of choice. Meatoplasty is a simple procedure in which the ventrum of the meatus is crushed (for hemostasis) for 60 seconds with a straight clamp (the authors have found the striations of a small nontoothed bowel clamp to be ideal for this application) and then divided with fine-tipped scissors.
Dilation of the meatus may also be appropriate in some cases.
Meatal stenosis surgery
Brown et al. 6 reported excellent results following 130 office meatotomies, with only two recurrences of meatal stenosis and one patient with bleeding requiring stitches. They also cited the cost-effectiveness of this treatment and noted good patient tolerance when a caring approach is used to reassure the child before and during the procedure. In this series, parents were encouraged to remain with the children during the operation; their presence seemed to have a calming effect.
In a retrospective study of 55 boys who underwent clinic meatotomy under topical lidocaine and prilocaine (EMLA) anesthesia, Fronczak et al. 7 found that although their success rate was lower than that reported in earlier studies and the incidence of pain higher, it was nonetheless possible to complete all of the clinic meatotomies, and more than 90% of patients experienced resolution or improvement of their symptoms. The cost of clinic meatotomy was approximately one tenth that of meatotomy performed under general anesthesia, with no evidence of inferiority evident in the literature.
If the caregivers and the patient are cooperative, meatotomy can be performed in the office of the physician with a topical eutectic mixture of local anesthetics (EMLA cream) applied liberally over the entire glans and secured in place for at least 30 minutes with an occlusive dressing. After being in place for 30 minutes, the dressing is removed, and the penis is prepared and draped into a sterile field.
Throughout the procedure, it is important to reassure the child and tell him what is being done.
One blade of a straight clamp is introduced into the meatus, and the ventrum of the meatus is crushed (~3 mm) by closing the clamp. This provides adequate hemostasis in most cases. The crushed area is divided with a straight fine-tipped scissors, and an antibiotic ointment is applied.
After the operation, it is critical that the caregivers separate the edges of the meatus and apply ointment twice a day for 2 weeks and then once a day for another 2 weeks to prevent one side of the meatotomy from adhering to the other side. Some medical professionals recommend dilation with a lubricated feeding tube or the tip of an ointment tube (antibiotic, steroid, or combination) for a period of up to 8 weeks.
In a survey of office pediatric urologic procedures, which included meatotomy, lysis of labial adhesions, and newborn circumcision, Smith and Smith 8 found that 95 of 99 parents stated that they were satisfied with their decision to have these procedures performed in the office, and 95% reported good outcomes (only one patient had recurrent meatal stenosis).
Mild dysuria may be present for 1-2 days after meatotomy. If dysuria results in urinary retention, placing the child in a tub of warm water may stimulate urination.
It is also important to note that spraying of the urine stream may occur for a while after surgical correction as a consequence of edema.
Depending on the age and temperament of the child, it may be preferable to perform meatotomy with the patient under sedation or general anesthesia in the operating room.
Some surgeons prefer meatoplasty, in which stitches are placed to help keep the meatus open, to meatotomy, citing research that suggests a lower recurrence rate after meatoplasty 9. Meatoplasty typically requires sedation or general anesthesia.
Others have reported excellent results with meatotomy. Ultimately, the choice of approach (meatotomy, meatoplasty, or no surgery) is based on a thorough discussion among the provider, the family members, and the patient (if applicable).
Postoperative Care
After meatotomy, caregivers will typically be instructed to separate the edges of the meatus and apply antibiotic, steroid, or combination ointment twice a day for 2 weeks and then once a day for 2 more weeks. The physician may have other specific instructions, based on their usual care.
Activity
After meatotomy, instruct caregivers to dress the child in loose underwear for 24 hours. Restrict activities, such as contact sports, bicycle rides, and playground activities, for 3-4 days.
Complications
Complications include bleeding during or after meatotomy, infection, and recurrence. All of these complications are rare and typically respond readily to appropriate management.
Mild painful urination may persist for 1-2 days. Placing the child in a tub of warm water may provide relief.
Meatal stenosis prognosis
Meatal stenosis prognosis is excellent after surgery: Meatotomy or meatoplasty is typically curative of the misdirection of the urinary stream. Morbidity is limited to the clinical symptoms and complications of surgical repair, including bleeding, infection, and recurrence. If there are also voiding symptoms (e.g, pain with urination or hesitancy), these may be related to underlying voiding dysfunction, and surgical correction of meatal stenosis may not alleviate them.
- Morris BJ, Krieger JN. Does Circumcision Increase Meatal Stenosis Risk?-A Systematic Review and Meta-analysis. Urology. 2017 Dec. 110:16-26.[↩]
- Meatal stenosis. https://emedicine.medscape.com/article/1016016-overview[↩][↩]
- Stewart L, McCammon K, Metro M, Virasoro R. SIU/ICUD Consultation on Urethral Strictures: Anterior urethra-lichen sclerosus. Urology. 2014 Mar. 83 (3 Suppl):S27-30[↩]
- Gargollo PC, Kozakewich HP, Bauer SB, Borer JG, Peters CA, Retik AB, et al. Balanitis xerotica obliterans in boys. J Urol. 2005 Oct. 174 (4 Pt 1):1409-12.[↩]
- Litvak AS, Morris JA Jr, McRoberts JW. Normal size of the urethral meatus in boys. J Urol. 1976 Jun. 115 (6):736-7.[↩]
- Brown MR, Cartwright PC, Snow BW. Common office problems in pediatric urology and gynecology. Pediatr Clin North Am. 1997 Oct. 44 (5):1091-115[↩]
- Fronczak CM, Villanueva CA. Clinic meatotomy under topical anesthesia. J Pediatr Urol. 2017 Oct. 13 (5):499.e1-499.e3[↩]
- Smith C, Smith DP. Office pediatric urologic procedures from a parental perspective. Urology. 2000 Feb. 55 (2):272-6.[↩]
- Godley SP, Sturm RM, Durbin-Johnson B, Kurzrock EA. Meatal stenosis: a retrospective analysis of over 4000 patients. J Pediatr Urol. 2015 Feb. 11 (1):38.e1-6[↩]





{kind=link}