Contents
What is melioidosis
Melioidosis also called Whitmore’s disease, is an infectious disease caused by the aerobic, Gram-negative soil-dwelling bacillus bacteria Burkholderia pseudomallei that are commonly found in the soil and water, that can infect humans or animals through direct contact with soil, water, or air contaminated by the bacteria 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12. Because the Burkholderia pseudomallei bacteria reside in soil and water, weather events such as hurricanes, heavy rain, flooding and typhoons have been implicated in outbreaks of melioidosis. Burkholderia pseudomallei is mostly found in tropical climates, especially in Southeast Asia and northern Australia, where it causes widespread melioidosis. In the United States, Burkholderia pseudomallei is found in Puerto Rico, the U.S. Virgin Islands, and the Gulf Coast area of the state of Mississippi. Melioidosis is a rare disease in the United States with most melioidosis illnesses in the United States occur in people who have traveled to areas where the disease is more common. Some cases have also occurred in people who have had contact with contaminated products from overseas 12.
People can get melioidosis by 12:
- Breathing in contaminated dust or water droplets
- Eating or drinking contaminated food or water
- Having contact with contaminated soil or water, especially through skin breaks (cuts, scrapes, etc.) or getting it in their mouths
It’s very rare for people to get melioidosis from another person.
Burkholderia pseudomallei infection was first recognized in Rangoon a city located in southern Myanmar (formerly Burma) by Whitmore and Krishnaswami in 1911 13. In 2016, a statistical model estimated that there would be 165,000 new cases of melioidosis worldwide and 89,000 deaths, suggesting that melioidosis is significantly underreported 14. Community-acquired pneumonia is the most frequent clinical presentation of melioidosis and bacteremia the most common microbiological diagnosis 15, 16 In Ubon Ratchathani, Thailand, Burkholderia pseudomallei accounts for up to approximately 20% of community-acquired bacteremias 17. At the Royal Darwin Hospital, Australia, Burkholderia pseudomallei has been the most common cause of fatal community-acquired bacteremic pneumonia 18, 19.
Melioidosis usually occurs in individuals with specific comorbidities that include diabetes mellitus, hazardous alcohol consumption, chronic lung disease, chronic kidney disease, and immunosuppression 2. Patients with cancer are also more likely to develop melioidosis, a result of the immunosuppressive anti-cancer therapy that they frequently receive, although other factors including medical comorbidities and poor nutritional status also contribute to their greater risk 20. Despite the higher incidence of melioidosis in patients with cancer, the characteristics and clinical course of melioidosis in these patients have rarely been described in detail 21, 22.
Many kinds of animals can get melioidosis, including:
- Sheep
- Goats
- Pigs, hogs, boar
- Horses
- Cats
- Dogs
- Cows
In the United States, confirmed cases reported in previous years have ranged from zero to five and have occurred among travelers and immigrants coming from places where melioidosis is widespread. Moreover, it has been found among troops of all nationalities that have served in areas with widespread disease.
The greatest numbers of melioidosis cases are reported in:
- Thailand
- Malaysia
- Singapore
- Northern Australia
Though rarely reported, cases are thought to frequently occur in:
- Papua New Guinea
- Most of the Indian subcontinent
- Southern China
- Hong Kong
- Taiwan
- Vietnam
- Indonesia
- Cambodia
- Laos
- Myanmar (Burma)
Outside of Southeast Asia and Australia, cases have been reported in:
- The South Pacific (New Caledonia)
- Sri Lanka
- Mexico
- El Salvador
- Panama
- Ecuador
- Peru
- Guyana
- Puerto Rico
- Martinique
- Guadeloupe
- Brazil
- Parts of Africa and the Middle East
Melioidosis is spread to humans and animals through direct contact with soil, water, or air contaminated by the Burkholderia pseudomallei bacteria. Humans and animals are believed to acquire melioidosis by inhalation of contaminated dust or water droplets, ingestion of contaminated water, and contact with contaminated soil, especially through skin abrasions (e.g., by means of a penetrating injury or open wound), inhalation (e.g., during severe weather or as a result of deliberate release), or ingestion (e.g., through contaminated food or water) (see Figure 2 above) 23, 15, 24, 25. Melioidosis is predominantly seasonal; 75 to 81% of cases occur during the rainy season 8, 26. Incidence peaks between 40 and 60 years of age, but melioidosis is also well recognized in children 27. Melioidosis has been transmitted to infants through breast milk from mothers with mastitis 8.
Melioidosis signs and symptoms can vary greatly and may mimic those of tuberculosis (TB) or common forms of pneumonia 28. Signs and symptoms may include pain or swelling, fever, abscess, cough, high fever, headache, trouble breathing, and more. Although healthy people can also experience signs and symptoms of the disease, people with certain conditions like diabetes, liver disease, kidney disease, lung disease, thalassemia, cancer, or certain autoimmune diseases are more severely affected.
Symptoms of melioidosis or Burkholderia pseudomallei infection include:
- Fever
- Headache
- Trouble breathing
- Stomach or chest pain
- Muscle pain
- Confusion
- Seizure.
A delay in diagnosis can be fatal, since empirical antibiotic regimens used for suspected bacterial sepsis often do not provide adequate coverage for Burkholderia pseudomallei.
Melioidosis diagnosis is made by collecting blood, sputum, urine, or pus samples and growing the bacteria 29. Current treatment is divided into two stages: an intravenous (IV) antibiotic stage and oral antibiotic maintenance stage to prevent recurrence 29.
Antimicrobial agents that have been effective against melioidosis include:
Intravenous therapy antibiotics for 2 to 8 weeks that consists of:
- Ceftazidime administered every 6-8 hours
- OR
- Meropenem administered every 8 hours
Followed by oral antimicrobial therapy for 3 to 6 months that consists of:
- Trimethoprim-sulfamethoxazole taken every 12 hours
- OR
- Amoxicillin/clavulanic acid (co-amoxiclav) taken every 8 hours.
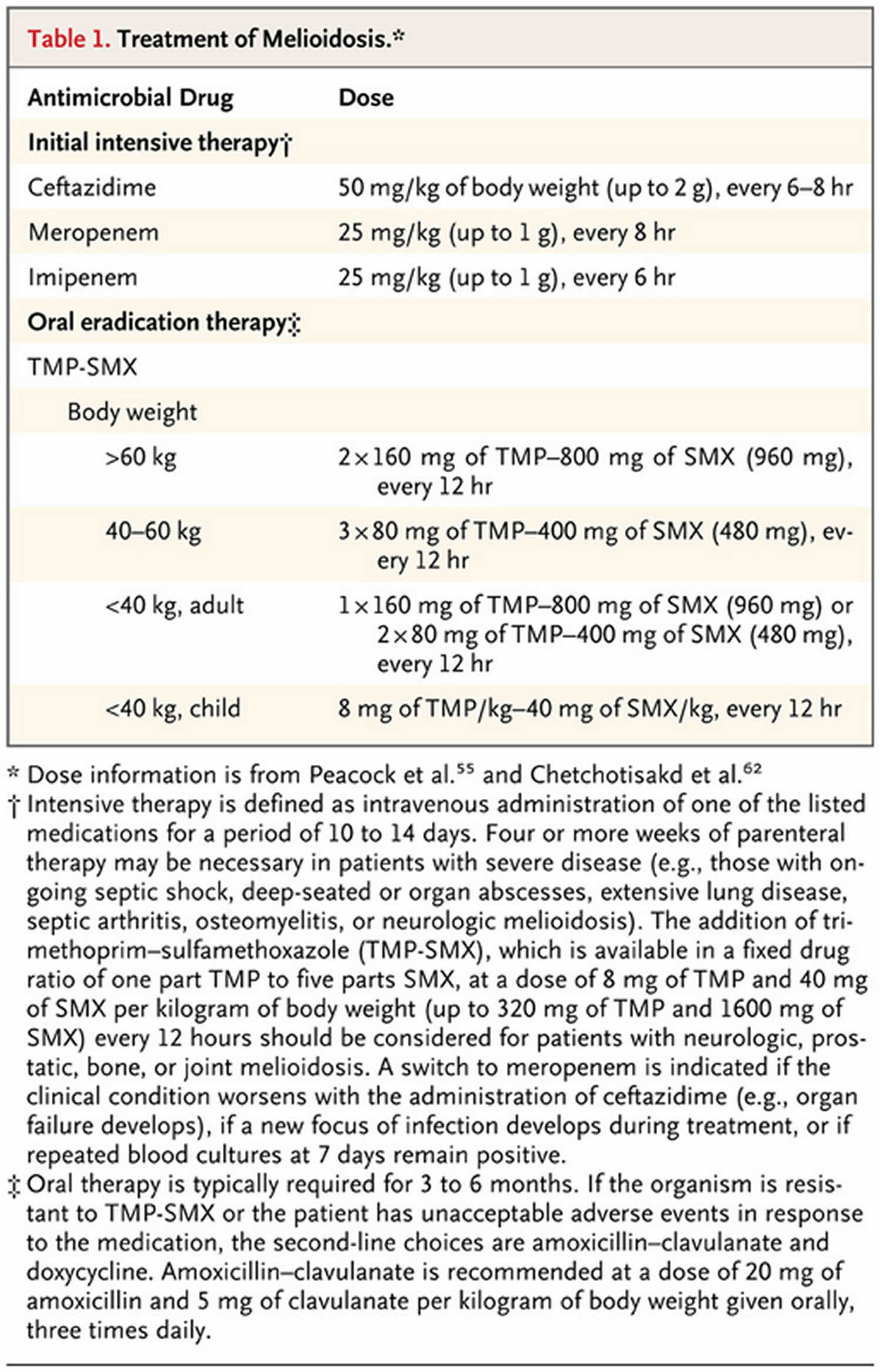
Patients with penicillin allergies should notify their doctor, who can prescribe an alternative treatment course. Current melioidosis therapy guidelines recommend an initial intensive phase of at least 10 to 14 days of ceftazidime, meropenem, or imipenem administered intravenously (IV) followed by oral eradication therapy, usually with trimethoprim–sulfamethoxazole (TMP-SMX) for 3 to 6 months (Table 3) 30, 31, 32, 33. Carbapenems, such as meropenem and imipenem, have lower minimum inhibitory concentrations (MIC) and superior results in in vitro time-kill studies than ceftazidime, but a randomized comparative study in Thailand did not show a survival advantage of imipenem over ceftazidime 34. The current recommendation for the oral phase of therapy is trimethoprim–sulfamethoxazole (TMP-SMX), which replaces the previous recommendation to give this medication in conjunction with doxycycline 32.
The 2014 Revised Royal Darwin Hospital guideline recommends an intravenous intensive phase including therapy with either ceftazidime at 50 mg/kg of body weight (up to 2 g) every 6 to 8 hour if the patient is in the general medical ward (a hospital room designed for multiple patients, typically with two or more beds, that provides general medical care for a wide range of conditions) or meropenem at 25 mg/kg (up to 1 g) every 8 hour if in the intensive care unit (ICU) 31. The duration of this phase is 10 to 14 days for uncomplicated infection or 4 to 6 weeks for persistent septic shock, deep-seated or organ abscesses, extensive lung disease, septic arthritis, osteomyelitis, or neurological melioidosis. The oral eradication phase includes therapy with trimethoprim–sulfamethoxazole (TMP-SMX), dose depending on weight and age, for a period of 3 to 6 months. For a child of <40 kg, a dosage of 8/40 mg every 12 h is recommended. Dosage recommendations for adults include the following: <40 kg, 160/800 mg every 12 hours; 40 to 60 kg, 240/1,200 mg every 12 hours; and >60 kg, 320/1,600 mg every 12 hours 30, 31, 35.
A careful search for internal-organ abscesses is recommended, such as with the use of computed tomography (CT scan) or ultrasonography of the abdomen and pelvis. Adjunctive therapy for abscesses includes drainage of collections and aspiration and washout of septic joints.
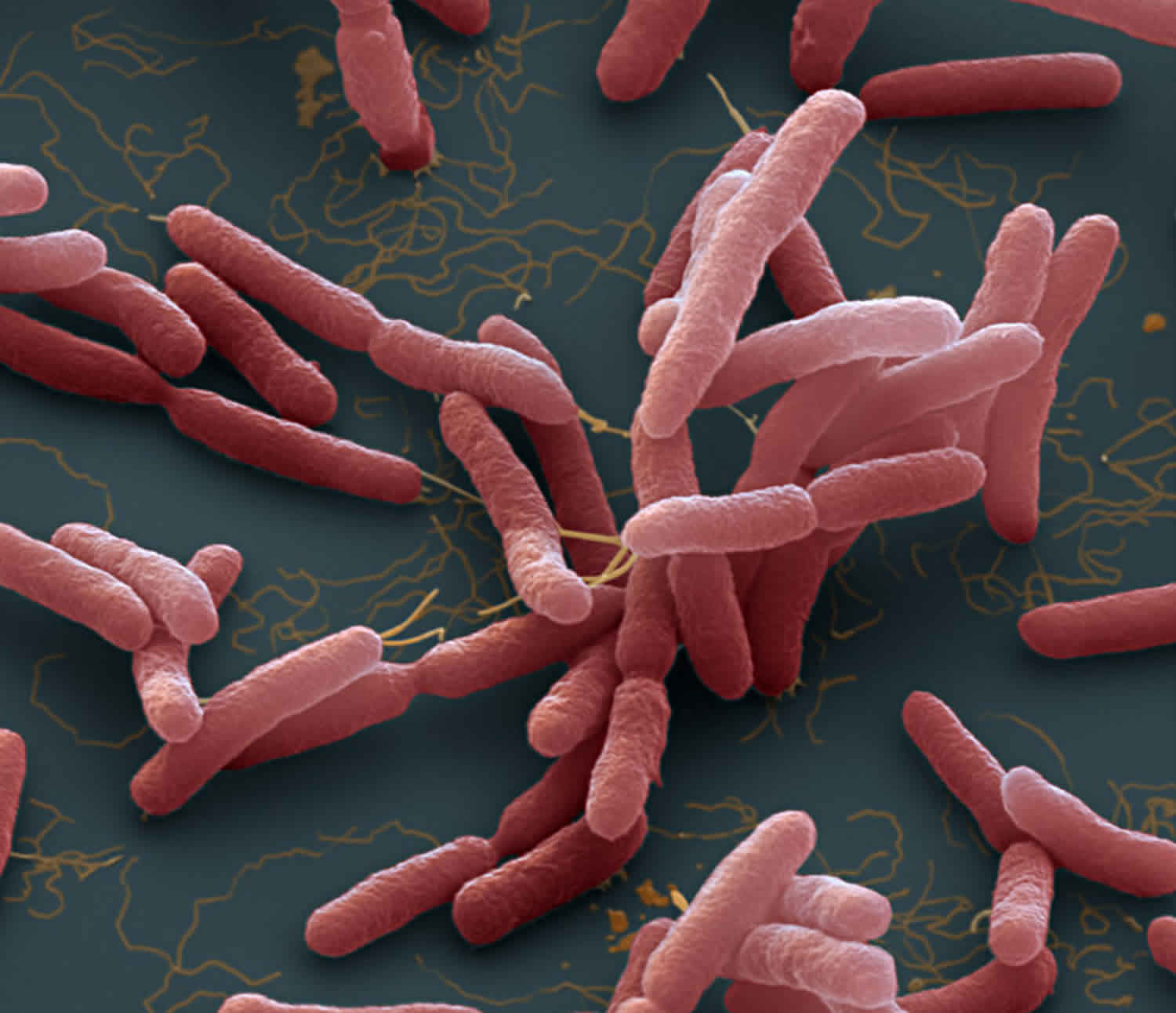
Figure 1. Burkholderia pseudomallei
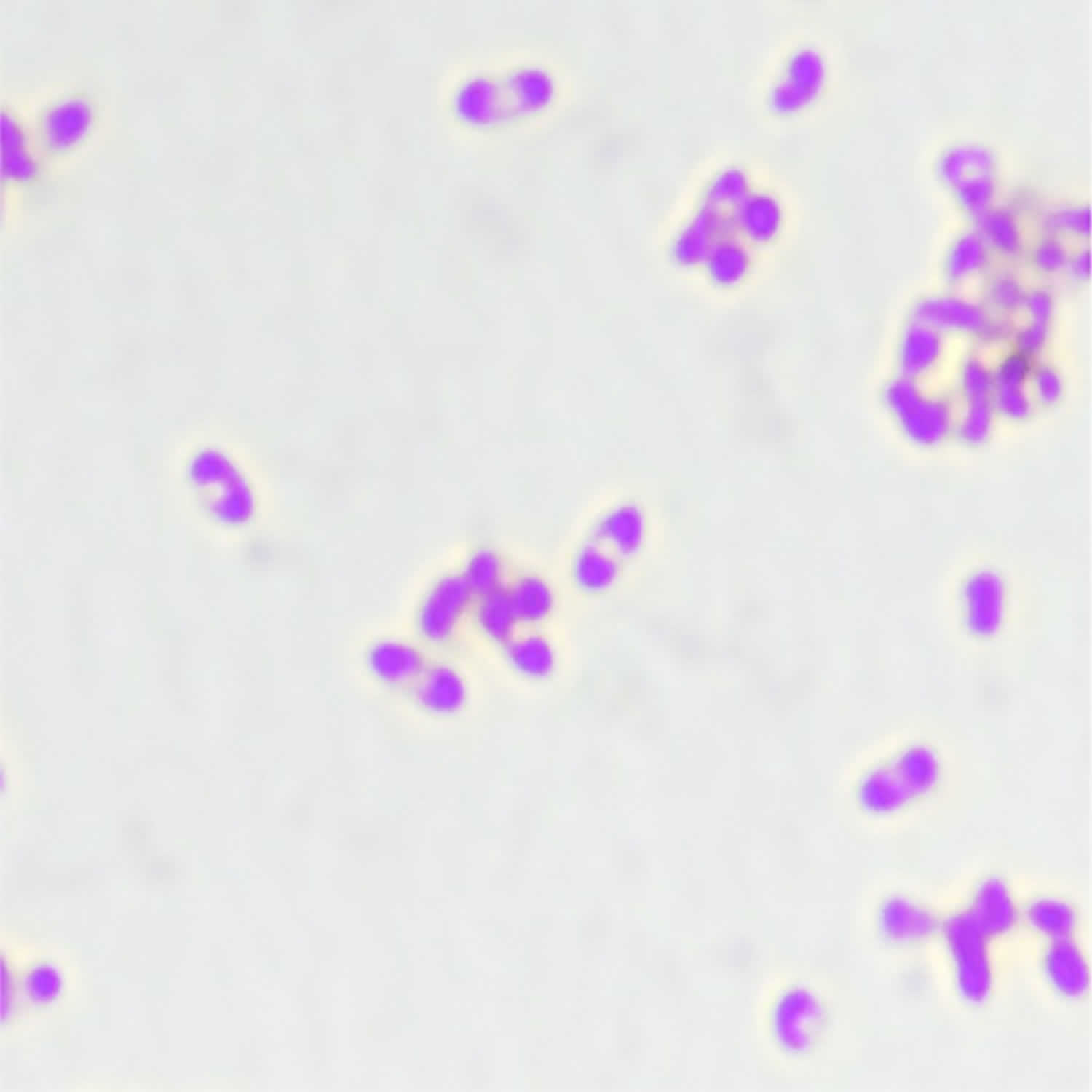
Footnotes: Burkholderia pseudomallei organisms are small Gram-negative bacilli with bipolar staining giving them a “safety pin” appearance due to central accumulation of polyhydroxybutyrate (PHB) granules, which do not retain the staining reagents 36. (Magnification ×100). However, the “safety pin” appearance is not specific to Burkholderia pseudomallei. The Gram stain appearance alone is not sufficient to make a presumptive diagnosis.
[Source 21 ]Figure 2. Burkholderia pseudomallei transmission
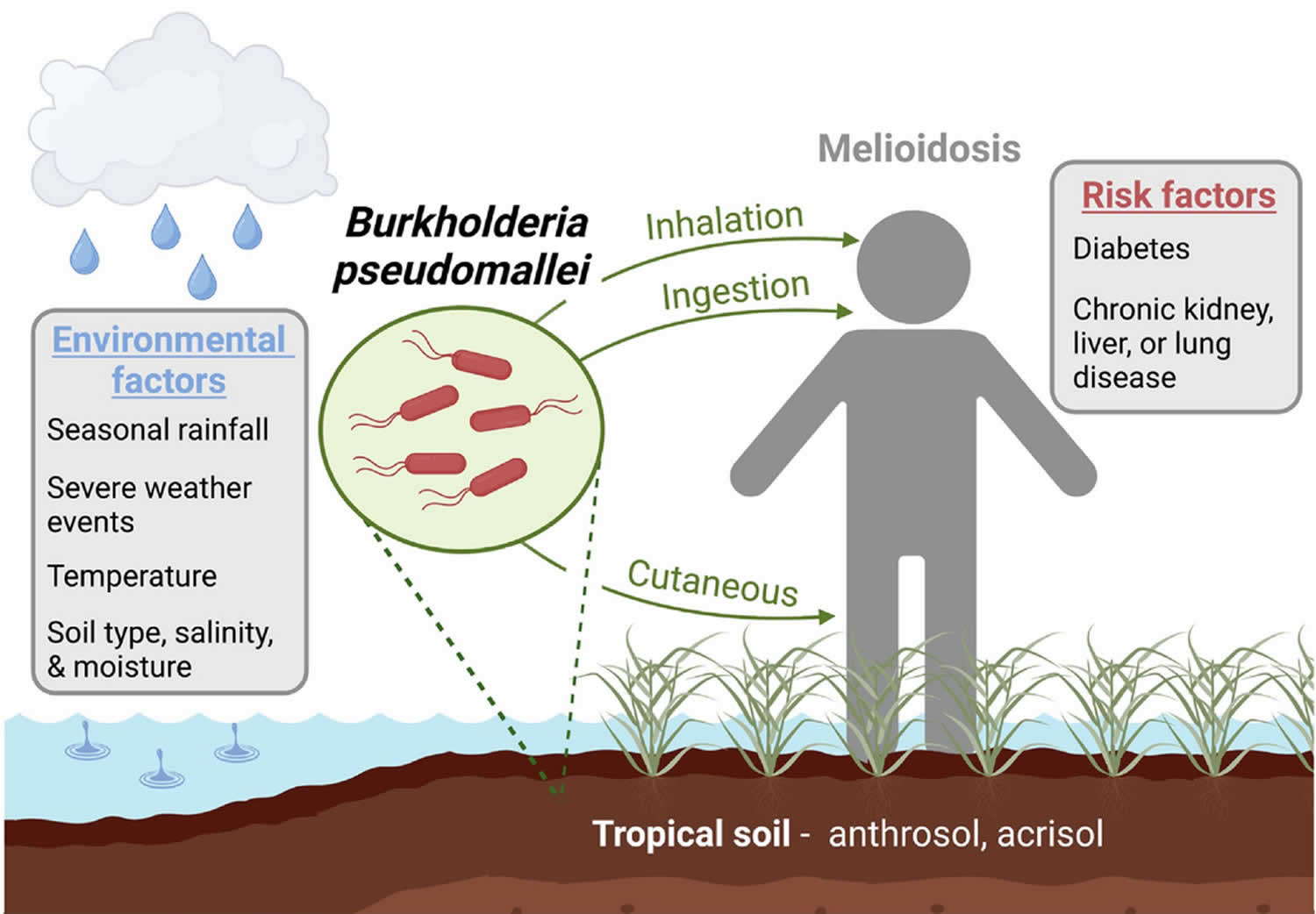
Footnotes: Burkholderia pseudomallei is a aerobic, Gram-negative soil-dwelling facultative intracellular bacterium that resides in the rhizosphere of tropical soils. Burkholderia pseudomallei causes melioidosis, which is transmitted by cutaneous entry, ingestion, or inhalation of contaminated soil or water. Infection with Burkholderia pseudomallei can cause a wide array of clinical symptoms such as pneumonia, bone, joint, skin, genitourinary, and central nervous system infections, as well as parotid abscesses in children. Mammalian virulence is linked to the Burkholderia pseudomallei intracellular life cycle, which begins with attachment and internalization by host cells. Burkholderia pseudomallei can infect a wide range of eukaryotic cells, including macrophages, monocytes, and neutrophils, as well as nonphagocytic cells. Once internalized, a type 3 secretion system (T3SSBsa) facilitates Burkholderia pseudomallei escape from the phagosome, and the bacteria replicate in the cytoplasm. Autotransporter protein BimA mediates actin polymerization, enabling Burkholderia pseudomallei to spread, cell to cell, using actin-based motility. This process, coupled with the activity of a type 6 secretion system (T6SS-5), results in host membrane fusion and the formation of multinucleated giant cells. Capsule polysaccharides also contribute to virulence and evasion of host innate immunity. Treatment of Burkholderia pseudomallei infections is complicated by the organism’s intrinsic resistance to multiple classes of antimicrobials, largely due to an abundance of efflux pumps and reduced outer membrane permeability. While Burkholderia pseudomallei is commonly associated with endemic ‘hotspots’ in southeast Asia and northern Australia, there is increasing evidence that it is likely endemic in a large range of tropical and subtropical areas, including regions in Africa, South America, the Middle East, Central America, and the Caribbean. Soil and climate conditions favorable for Burkholderia pseudomallei survival are also found in additional areas worldwide. Consequently, it is important for clinical and public health laboratories located outside of high-endemicity areas to be aware of Burkholderia pseudomallei, as well as for improved diagnostic and reporting methods.
[Source 37 ]Figure 3. Melioidosis geographic distribution
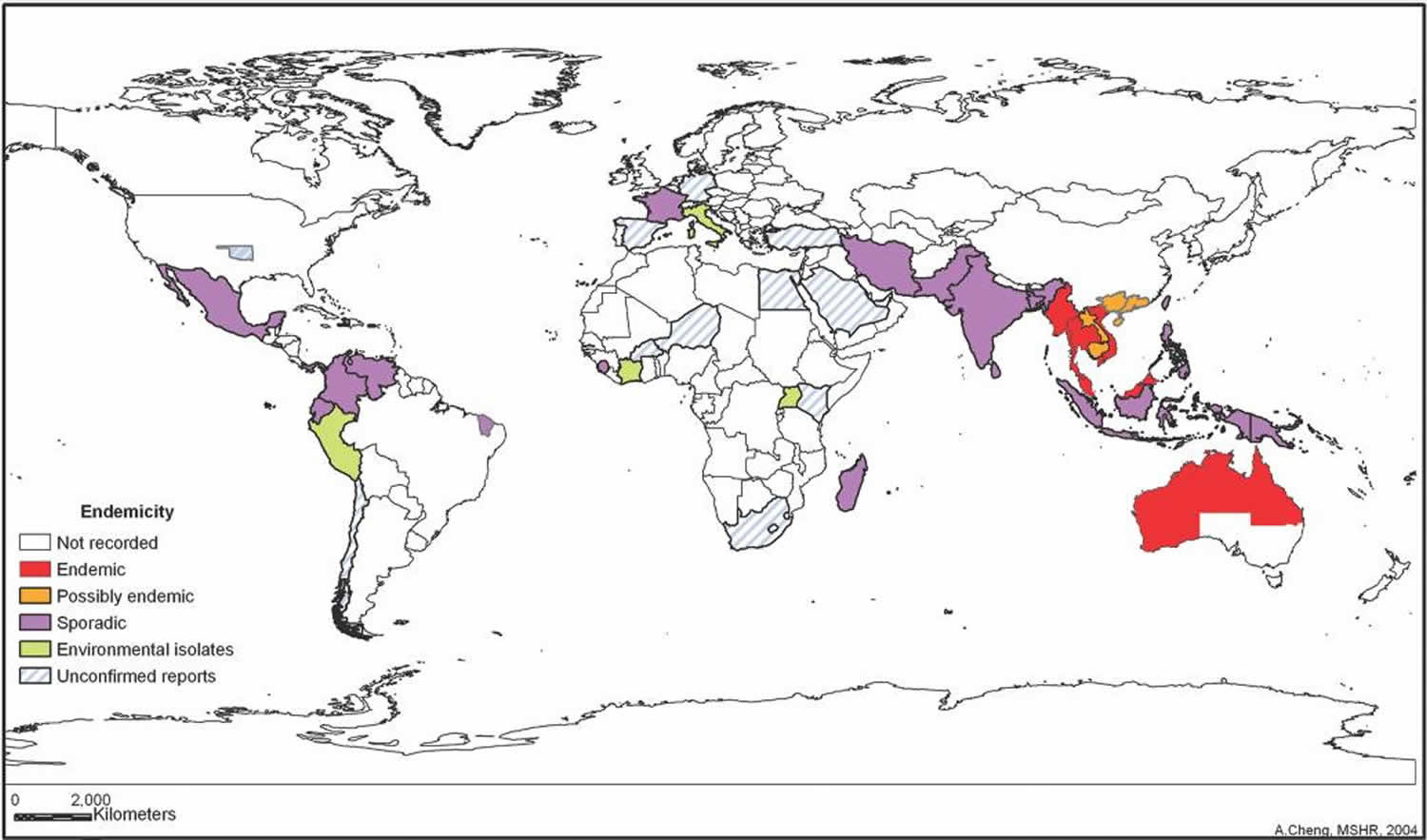
Footnotes: Areas where melioidosis is highly endemic, endemic, or sporadic and possibly endemic are indicated. This reflects current knowledge that is based on limited evidence and is likely to change over time.
[Source 8 ]Figure 4. Melioidosis signs and symptoms
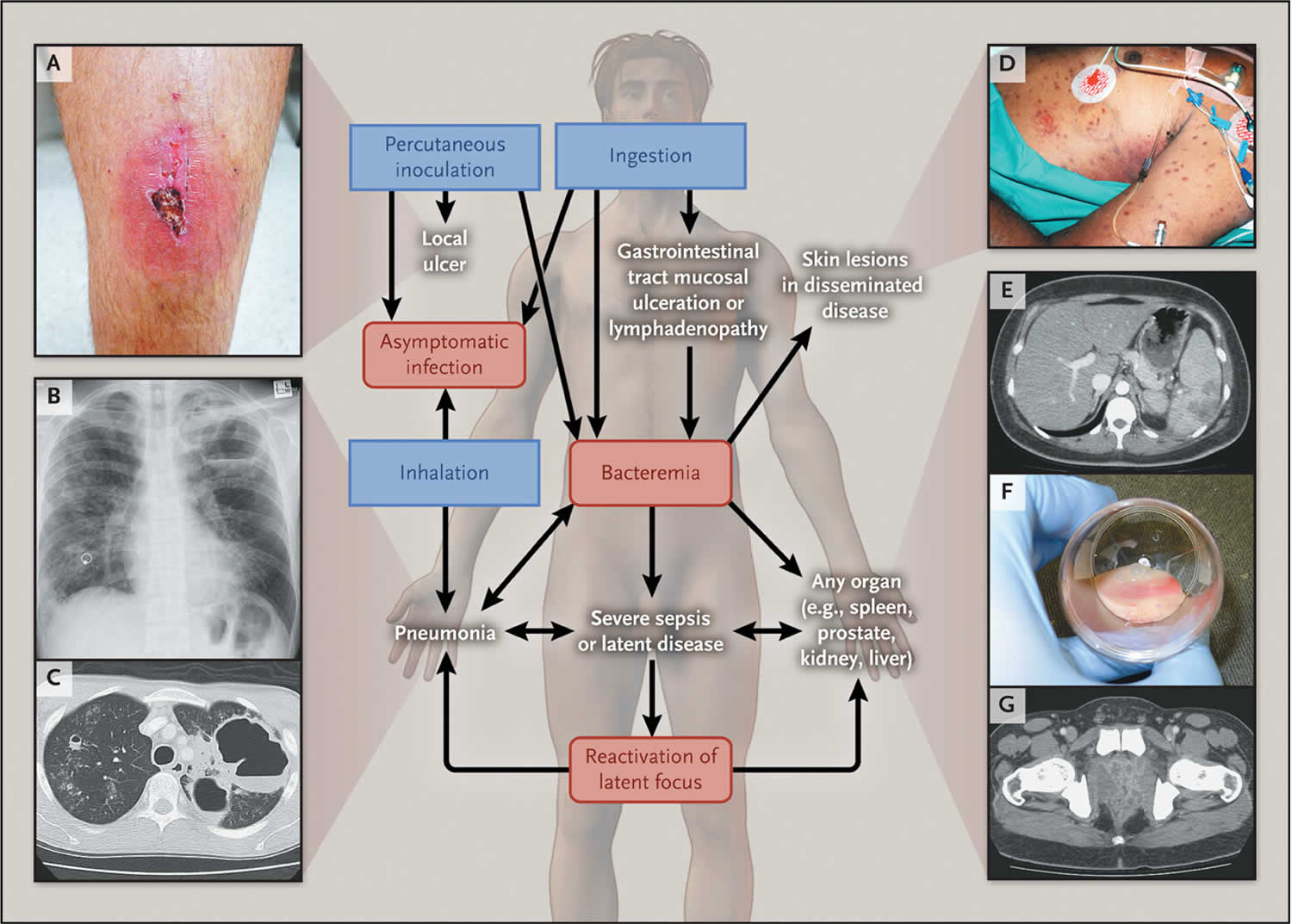
Footnotes: Melioidosis have a wide range of clinical signs and symptoms, and severity varies from an acute fulminant septic illness to a chronic infection. Shown are the routes of infection (blue boxes: percutaneous inoculation, inhalation, and ingestion), the natural history of infection (red boxes: asymptomatic infection, bacteremia, or reactivation of latent focus), and the diverse disease manifestations (white text). Panel A shows cutaneous melioidosis in a healthy host. Panel B shows lung abscesses on the chest radiograph of a patient with acute melioidosis pneumonia, and Panel C shows the corresponding computed tomographic (CT) scan. Panel D shows the skin manifestations in a fatal case of disseminated melioidosis. Panel E shows splenic abscesses on an abdominal CT scan. Panel F shows aspirated pus in a patient with prostatic and periprostatic abscesses, and Panel G shows the abscesses on a CT scan from the patient.
[Source 35 ]Table 1. Melioidosis treatment
Melioidosis transmission
Melioidosis is an infectious disease caused by the aerobic, Gram-negative soil-dwelling facultative intracellular bacteria Burkholderia pseudomallei that are commonly found in the soil and water, that can infect humans or animals through direct contact with soil, water, or air contaminated by the bacteria. While melioidosis infection has taken place all over the world, Southeast Asia and northern Australia are the areas in which it is primarily found. People can get Melioidosis through direct contact with contaminated soil and surface waters.
Humans and animals are believed to acquire melioidosis by inhalation of contaminated dust or water droplets, ingestion of contaminated water, and contact with contaminated soil, especially through skin abrasions (e.g., by means of a penetrating injury or open wound), inhalation (e.g., during severe weather or as a result of deliberate release), or ingestion (e.g., through contaminated food or water) (see Figure 2 above) 23, 15, 24, 25. Melioidosis is predominantly seasonal; 75 to 81% of cases occur during the rainy season 8, 26. Incidence peaks between 40 and 60 years of age, but melioidosis is also well recognized in children 27. Melioidosis has been transmitted to infants through breast milk from mothers with mastitis 8.
It is very rare for people to get melioidosis from another person. While a few cases have been documented, contaminated soil and surface water remain the primary way in which people become infected.
The incubation period for melioidosis has been evaluated in a single published study, in which 25% of patients who recalled a specific event such as an injury had clinical signs and symptoms 1 to 21 days (mean, 9 days) later 38. The inoculating dose, strain virulence, mode of infection, and risk factors in the host are all likely contributors to the incubation period, clinical presentation, and outcome 35. An incubation period of a day or less was documented after aspiration of Burkholderia pseudomallei in a near-drowning event 39, whereas the longest recorded apparent incubation period was 62 years 40.
Besides humans, many animal species are susceptible to melioidosis, including:
- Sheep
- Goats
- Swine
- Horses
- Cats
- Dogs
- Cattle.
Burkholderia pseudomallei
Burkholderia pseudomallei belongs to the Burkholderia genus, which contains over 80 species 41. Only Burkholderia pseudomallei, Burkholderia mallei, Burkholderia cepacia complex, and Burkholderia gladioli are generally recognized as human pathogens 42. These organisms are aerobic, non-spore-forming, nonfermenting Gram-negative bacilli. All are environmental organisms, with the exception of the host-adapted pathogen Burkholderia mallei 42.
Burkholderia mallei causes glanders in horses and other solipeds and is highly virulent in humans. Burkholderia cenocepacia is an important cause of opportunistic infection in patients with cystic fibrosis. Burkholderia thailandensis coexists with Burkholderia pseudomallei in the soil in Thailand and Australia. Burkholderia oklahomensis is sporadically found in the midwestern United States. Burkholderia thailandensis and Burkholderia oklahomensis rarely, if ever, cause disease and are much less virulent (by a factor of >100,000) than Burkholderia pseudomallei in hamsters and mice 43, 44.
Risk factor for melioidosis
Although healthy people may get melioidosis, having the following medical conditions may increase your risk 2, 21:
- Diabetes
- Liver disease
- Heavy alcohol use
- Kidney disease
- Thalassemia (a group of inherited genetic blood disorders where the body produces insufficient amounts of healthy hemoglobin, a protein in red blood cells essential for carrying oxygen)
- Cancer, or another condition that weakens the immune system
- Chronic heart disease
- HIV
- Kava
- Smoking
- Chronic lung disease, like cystic fibrosis, chronic obstructive pulmonary disease (COPD), or bronchiectasis.
- Australian Aboriginal and/or Torres Strait Islander race.
Certain activities also may increase your risk of being exposed to the Burkholderia pseudomallei bacteria that causes melioidosis, including:
- Travel to areas where the disease is common.
- Breathing in contaminated water droplets or soil dust that get into the air after severe weather like hurricanes or heavy rainfall.
- Hobbies or jobs that could put you in contact with contaminated soil or water.
- Drinking unchlorinated or untreated drinking water.
Since up to 80% of patients with melioidosis have one or more risk factors for the infection, it has been suggested that melioidosis should be considered an opportunistic infection that is unlikely to have a fatal outcome in a previously healthy person, provided that the infection is diagnosed early and appropriate antibiotic agents and intensive care resources are available 45. Risk factors for melioidosis include diabetes (present in 23 to 60% of patients), heavy alcohol use (in 12 to 39%), chronic lung disease (in 12 to 27%), chronic kidney disease (in 10 to 27%), thalassemia (in 7%), glucocorticoid therapy (in <5%), and cancer (in <5%) 45, 46.
Melioidosis prevention
In areas where the melioidosis disease is widespread, contact with contaminated soil or water can put people at risk for melioidosis.
However, in these areas, there are things that certain groups of people can do to help minimize the risk of exposure:
- If you have open skin wounds, or if you have chronic conditions like diabetes or kidney disease, avoid contact with soil and standing water.
- If you perform agricultural work or have hobbies or jobs that raise your risk of exposure, wear boots, which can prevent infection through your feet and lower legs.
- Healthcare workers can use standard precautions when treating patients with melioidosis to help prevent infection. They should also label samples appropriately if they suspect melioidosis to protect lab personnel.
- Laboratory personnel should follow good laboratory practices, including using appropriate personal protective equipment (PPE) and respiratory protection.
No vaccines are currently available for glanders or melioidosis 1.
Currently there is limited evidence to demonstrate effective prevention of infection in humans 47, 48. Amoxicillin-clavulanic acid, doxycycline, and trimethoprim–sulfamethoxazole (TMP-SMX) have been assessed in a 10-day postexposure prophylaxis mouse model. Trimethoprim–sulfamethoxazole (TMP-SMX) was the only agent to achieve 100% survival at 21 days in this study; however, additional murine research demonstrated 44% and 83% survival following a 14- or 21-day course 49, 50. Current international consensus guidelines recommend a 21-day course of trimethoprim–sulfamethoxazole (TMP-SMX). Alternative prophylactic therapy includes doxycycline or amoxicillin-clavulanic acid 47, 30. Prophylaxis for specific at-risk populations may be considered. One study reported that trimethoprim–sulfamethoxazole (TMP-SMX) prophylaxis for hemodialysis patients during the wet season in a region of endemicity is likely to be effective in reducing incidence of infection and that an oral dose of 160/800 mg daily appears to be well tolerated and safe in this patient cohort 51. Notably, compared to that in a neighboring region, the study appears to have included a higher proportion of indigenous hemodialysis patients in rural dialysis centers. This region had a lower incidence of melioidosis among their hemodialysis cohort, and therefore, rates of adverse effects, and cost-effectiveness modelling, would not support universal prophylaxis of their population 52.
Melioidosis symptoms
There are several types of melioidosis infection, each with their own set of signs and symptoms. However, it is important to note that melioidosis has a wide range of signs and symptoms and severity varies from an acute fulminant septic illness to a chronic infection (the presence of symptoms for >2 months, accounting for 11% of all cases) that can be mistaken for other diseases such as tuberculosis (TB) or more common forms of pneumonia or cancer 9, 26.
You usually develop symptoms of melioidosis within 1 to 3 weeks after you’ve been infected with the Burkholderia pseudomallei bacteria. Some cases have developed symptoms months or years after exposure. Melioidosis can affect one body system or affect the entire body. Because of these factors, melioidosis is hard to diagnose and may be mistaken for other diseases.
Sometimes melioidosis is just in one area (localized), and it may look like an ulcer or skin sore. You might have a fever, swelling, and muscle aches.
Most often, melioidosis shows up as a lung infection. You might have a cough, chest pain, high fever, headache, and you might not feel like eating.
Whether you’ve just come down with melioidosis or you’ve had it for a long time, it can affect different organ systems throughout the body (disseminated infection). It can cause problems with the liver, spleen, prostate, joints, bones, lymph nodes, skin, or brain. Melioidosis can lead to a dangerous bloodstream infection (sepsis).
Localized Infection:
- Localized pain or swelling
- Fever
- Ulceration
- Abscess
Pulmonary Infection:
- Cough
- Chest pain
- High fever
- Headache
- Anorexia
Bloodstream Infection:
- Fever
- Headache
- Respiratory distress
- Abdominal discomfort
- Joint pain
- Disorientation
Disseminated Infection:
- Fever
- Weight loss
- Stomach or chest pain
- Muscle or joint pain
- Headache
- Seizures
The time between an exposure to the Burkholderia pseudomallei bacteria that causes melioidosis disease and the emergence of symptoms is not clearly defined, but may range from one day to many years; generally symptoms appear two to four weeks after exposure.
In a descriptive study involving 540 patients in tropical Australia over a 20-year period, the primary presenting feature was pneumonia (in 51% of patients), followed by genitourinary infection (in 14%), skin infection (in 13%), bacteremia without evident focus (in 11%), septic arthritis or osteomyelitis (in 4%), and neurologic involvement (in 3%) 45. The remaining 4% of patients had no evident focus of infection. Over half of patients have bacteremia on presentation, and septic shock develops in approximately one fifth 45. Internal-organ abscesses and secondary foci in the lungs, joints, or both are common.
A notable difference in presentation between patients in tropical Australia and those in Southeast Asia is suppurative parotitis, which accounts for up to 40% of cases of melioidosis in children in Thailand and Cambodia but is extremely rare in Australia 27. In Australia, prostatic melioidosis is present in approximately 20% of male patients, and neurologic melioidosis is manifested as brain-stem encephalitis, often with cranial-nerve palsies (especially cranial nerve VII [7th cranial nerve or facial nerve]), or as myelitis with peripheral motor weakness 45. Recurrent melioidosis occurs in approximately 1 in 16 patients, often in the first year after the initial presentation 45, 53. Roughly a quarter of recurrences are due to reinfection, with the remainder due to relapse from a persistent focus of infection 53. Mortality rates for melioidosis are approximately 40% in northeast Thailand (35% in children) 46 and 14% in Australia 45.
Table 2. Melioidosis clinical presentation by region
| Clinical presentation | No./total (%) | ||||
|---|---|---|---|---|---|
| Australia | Malaysia | Singapore | India | Thailand | |
| Fever | a — | 119/128 (93) | 293/372 (79) | 21/32 (66) | 95/134 (71) |
| Pulmonary infection | 412/763 (54) | 225/537 (42) | 203/614 (33) | 53/226 (23) | 121/247 (49) |
| Skin/soft tissue infection | 123/761 (16) | 99/402 (25) | 65/372 (17) | 23/180 (13) | 35/247 (14) |
| Bone and joint infection | 22/597 (4) | 35/402 (9) | 2/372 (1) | 36/226 (16) | 35/247 (14) |
| Genitourinary infection b | — | 10/360 (3) | — | 5/180 (3) | 8/134 (6) |
| Neurological infection | 22/751 (3) | 21/370 (6) | 2/372 (1) | 19/180 (11) | 2/30 (7) |
| Liver abscess | 17/597 (3) | 46/537 (9) | — | 20/180 (11) | 93/247 (38) |
| Splenic abscess | 30/597 (5) | 45/537 (8) | — | 20/226 (9) | 68/247 (28) |
| Prostate abscess | 83/408 (20) | 5/225 (2) | — | 8/226 (4) | 13/155 (8) |
| Parotid abscess | 2/794 (0) | — | 77/226 (3) | 5/134 (4) | |
| Mycotic pseudoaneurysm | 3/597 (1) | 4/67 (6) | — | — | — |
| Pericardial effusion/pericarditis | 4/540 (1) | 1/67 (1) | 1/372 (0) | 3/180 (2) | — |
| No clinical focus | 66/597 (11) | 69/392 (18) | — | 9/95 (9) | — |
| Septic shock | 174/715 (24) | 93/225 (41) | — | 32/180 (18) | 26/134 (19) |
| Bacteremia | 477/794 (60) | 391/537 (73) | 592/986 (60) | 87/226 (38) | 491/874 (56) |
| Mortality | 118/794 (15) | 212/527 (40) | 260/614 (42) | 32/180 (18) | 1,205/2,913 (41) |
Footnotes:
a —, no data reported.
b Excluding prostate.
Melioidosis diagnosis
Microbiological culture of Burkholderia pseudomallei from any specimen in a patient with suspected melioidosis remains the diagnostic “gold standard” 21. But culture of Burkholderia pseudomallei is not optimal because the sensitivity may be as low as 60% 54. Culture specimens include blood, throat, urine, respiratory secretions, and, when available, cerebrospinal fluid (CSF), pus, and swabs from wounds or surface lesions as appropriate, for all patients with suspected Burkholderia pseudomallei cases. Burkholderia pseudomallei grows well on most routine laboratory media 21. Improved isolation of the organism from nonsterile sites can be achieved by the use of selective media such as Ashdown’s media and selective enrichment broth 55. Any positive culture is considered diagnostic for melioidosis because Burkholderia pseudomallei is not considered to be a member of the colonizing microbiota.
Bacteremia has been found to occur in 38 to 73% of cases 21. In one study isolating Burkholderia pseudomallei from blood using the BacT/Alert (bioMérieux, Marcy l’Etoile, France) automated blood culture system, 62.5% of isolates were detected in 24 hour and 93% were detected within 48 hour of incubation. The time for the system to signal positive (mean ± standard error) was 23.9 ± 14.9 hour 56. When comparing the BacT/Alert system with conventional culture, which utilized in-house brain heart infusion media and visual detection, the automated system was found to have a sensitivity of 73.5%, compared to 90.3% for conventional culture 57. The major benefit of the automated system was a shorter time to positivity, approximately 1 day 57. Additionally, a study evaluating the sensitivity of the BacT/Alert FA aerobic bottle and BacT/Alert MB bottle with those of Middlebrook 7H9 broth, glycerol, and sodium polyanethol sulfonate demonstrated improved organism recovery with the MB bottle for patients with prior antimicrobial exposure 58. The Bactec (Becton Dickinson, Sparks, MD) automated blood culture system has also been used in laboratories for the isolation of Burkholderia pseudomallei from blood and sterile fluid. There are, however, limited data regarding the comparative sensitivity and time to positivity 59, 60. The urine culture of patients with melioidosis is estimated to be positive for 28% of cases in Thailand 61. Centrifugation of the sample and culture of the pellet improve sensitivity. Additionally, a quantitative urine culture revealed a comparatively higher mortality rate with increasing counts, with in-hospital mortality of 39% in culture-negative patients, 58% with a quantification of <10³ CFU/ml, and up to 71% with a quantification of >105 CFU/ml 61. Throat swabs are an effective method of organism recovery, and routine screening of suspected melioidosis patients is performed in certain centers 62, 63.
Laboratory procedures for maximizing the culture and identification of Burkholderia pseudomallei have been developed, but a delay in the identification of Burkholderia pseudomallei or a misidentification as another species is not uncommon in laboratories that are unfamiliar with this organism 33. A direct polymerase-chain-reaction assay of a clinical sample to detect Burkholderia pseudomallei and Burkholderia mallei may provide a more rapid test result than culture, but the assay is less sensitive than culture , especially when performed on blood 64, 65, 66. Serologic testing alone is inadequate for confirming the diagnosis, especially in endemic regions where the background seropositivity rate can be more than 50% 67. If empirical therapy for melioidosis is begun and Burkholderia pseudomallei is not subsequently detected in adequate cultures of specimens obtained before therapy, completion of a full course of antimicrobial therapy is generally not recommended.
Gram staining and examination under light microscopy of clinical specimens or bacterial colonies can identify gram-negative bacilli with a granular or safety pin appearance, but this appearance is not specific for Burkholderia pseudomallei. Gram-negative organisms that are oxidase positive, gentamicin- and colistin-resistant, and susceptible to amoxicillin/clavulanic acid, also known as co-amoxiclav, should be strongly suspected to be Burkholderia pseudomallei. During a public health emergency, or where Burkholderia pseudomallei may be of high prevalence in the community, a selective medium such as Ashdown agar 68 that will suppress overgrowth of normal microbiota in nonsterile specimens (e.g., throat swabs) should be used for suspected cases. However, rare gentamicin-susceptible Burkholderia pseudomallei isolates exist (1 in 1,000), which will not grow on Ashdown agar 69.
Commercial Burkholderia cepacia agar is a good alternative if Ashdown agar is not available 70. Bacterial colonies are usually visible after 24 hour. Colonies grown on Ashdown agar might have a violet or purple rugose, cornflower-like appearance. Colonies on nonselective media can vary in appearance and can be rugose or smooth. After positive identification is established, isolates should be collected for strain characterization and epidemiologic information as well as to aid forensic data investigations.
Biochemical tests such as the API 20NE (bioMérieux Inc., Durham, NC, USA) and Vitek II (bioMérieux Inc.) might help with confirmation, but misidentifications by both systems have been reported 71. Bacterial identification methods that use assays with polyclonal or monoclonal antibodies against B. pseudomallei and B. mallei have been described, e.g., a direct immunofluorescence assay that can be applied directly to clinical specimens and has been reported to have a sensitivity of 66% 72 and a latex agglutination assay that can be used to identify colonies. Both of these assays use in-house reagents developed in Thailand that are not commercially available but would be useful during a public health emergency for which there is a need to quickly distinguish between melioidosis and other illnesses that produce similar signs and symptoms.
Time to positive culture result (which is correlated with the level of bacteremia) is a prognostic indicator of death. Melioidosis results in a mortality rate of 74% if blood cultures show positive results within 24 h, compared with 41% mortality rate if >24 h pass before blood cultures become positive 73.
Melioidosis treatment
When a melioidosis infection is diagnosed, the disease can be treated with the use of appropriate medication.
The type of infection and the course of treatment will impact long-term outcome. Treatment generally starts with intravenous (within a vein) antimicrobial therapy for 10-14 days, followed by 3-6 months of oral antimicrobial therapy.
Antimicrobial agents that have been effective against melioidosis include:
Intravenous therapy antibiotics for 2 to 8 weeks that consists of:
- Ceftazidime administered every 6-8 hours
- OR
- Meropenem administered every 8 hours
Followed by oral antimicrobial therapy for 3 to 6 months that consists of:
- Trimethoprim–sulfamethoxazole (TMP-SMX) taken every 12 hours
- OR
- Amoxicillin/clavulanic acid (co-amoxiclav) taken every 8 hours.
Patients with penicillin allergies should notify their doctor, who can prescribe an alternative treatment course.
Current melioidosis therapy guidelines recommend an initial intensive phase of at least 10 to 14 days of ceftazidime, meropenem, or imipenem administered intravenously (IV) followed by oral eradication therapy, usually with trimethoprim–sulfamethoxazole (TMP-SMX) for 3 to 6 months (Table 3) 30, 31, 32, 33. Carbapenems, such as meropenem and imipenem, have lower minimum inhibitory concentrations (MIC) and superior results in in vitro time-kill studies than ceftazidime, but a randomized comparative study in Thailand did not show a survival advantage of imipenem over ceftazidime 34. The current recommendation for the oral phase of therapy is trimethoprim–sulfamethoxazole (TMP-SMX), which replaces the previous recommendation to give this medication in conjunction with doxycycline 32.
The 2014 Revised Royal Darwin Hospital guideline recommends an intravenous intensive phase including therapy with either ceftazidime at 50 mg/kg of body weight (up to 2 g) every 6 to 8 hour if the patient is in the general medical ward (a hospital room designed for multiple patients, typically with two or more beds, that provides general medical care for a wide range of conditions) or meropenem at 25 mg/kg (up to 1 g) every 8 hour if in the intensive care unit (ICU) 31. The duration of this phase is 10 to 14 days for uncomplicated infection or 4 to 6 weeks for persistent septic shock, deep-seated or organ abscesses, extensive lung disease, septic arthritis, osteomyelitis, or neurological melioidosis. The oral eradication phase includes therapy with trimethoprim–sulfamethoxazole (TMP-SMX), dose depending on weight and age, for a period of 3 to 6 months. For a child of <40 kg, a dosage of 8/40 mg every 12 h is recommended. Dosage recommendations for adults include the following: <40 kg, 160/800 mg every 12 hours; 40 to 60 kg, 240/1,200 mg every 12 hours; and >60 kg, 320/1,600 mg every 12 hours 30, 31, 35.
Although trimethoprim–sulfamethoxazole (TMP-SMX) is thought to be a bacteriostatic antimicrobial with time-dependent action, a time-kill study demonstrated that achievable in vivo drug concentrations appear to have a concentration-dependent bactericidal effect 74. Second-line oral antimicrobial agents include doxycycline and amoxicillin-clavulanic acid. The recommended amoxicillin-clavulanic acid dosage is 20/5 mg per kilogram of body weight three times per day 75, 8, 35. Previous Thai recommendations for oral therapy included a four-drug regimen consisting of trimethoprim–sulfamethoxazole (TMP-SMX), chloramphenicol, and doxycycline 76. However, one open-label randomized trial demonstrated no difference in efficacy of this regimen and poorer tolerability than with the combination of trimethoprim–sulfamethoxazole (TMP-SMX) and doxycycline. Furthermore, this trial revealed that duration of therapy was critical, with patients receiving less than 12 weeks of therapy incurring a 5.7-fold-increased risk of relapse or death 77. More recent evidence has shown noninferiority and improved tolerability when comparing trimethoprim–sulfamethoxazole (TMP-SMX) alone and trimethoprim–sulfamethoxazole (TMP-SMX) with doxycycline 78. Therefore, the current Thai recommendation for duration of oral therapy is 12 to 20 weeks, compared to the Australian recommendation of 3 to 6 months 8, 53.
Research in the Northern Territory of Australia has revealed decreased rates of relapse or recrudescence depending on duration of intensive-phase therapy 79. With a median intensive phase of 26 days, the relapse or recrudescence rate decreased from 5.2% to 0.5% irrespective of compliance to eradication/oral phase 79. Current Darwin Northern Territory of Australia guidelines recommend a minimum intensive phase of 2 weeks for skin abscess, bacteremia without focus, and pneumonia without lymphadenopathy or ICU admission 79. Four weeks is required for pneumonia with lymphadenopathy or ICU admission or deep-seated collection (abscess anywhere other than skin), 6 weeks for osteomyelitis, and 8 weeks for CNS or arterial infection 79. This study alters traditional thinking that choice and duration of eradication therapy are the most important predictors of relapse 79. Further analysis of septic arthritis and osteomyelitis management suggests that 5 weeks of intravenous therapy or 4 weeks for an isolated single joint without osteomyelitis will suffice. Three months of oral eradication-phase therapy appears to demonstrate a similar rate of relapse or complications. However, there is insufficient evidence to recommend a shorter course of therapy for osteomyelitis 80. A relapse rate of approximately 9.7% between 1986 and 2004 was reported from Thailand 81. This has improved to approximately 6% with an unspecified intravenous phase of at least 10 days 81, 82. There is a role for 3 months of oral-only therapy for uncomplicated soft tissue infection, provided that investigations for deep-seated collections are negative 83, 84.
Adjunctive therapy may include the addition of granulocyte colony-stimulating factor (G-CSF), which has been studied in multiple locations with various results 85, 86, 87. Initial observational data suggested that decreased in-hospital mortality from 95 to 10% was attributable to the use of granulocyte colony-stimulating factor (G-CSF) 87. However, it was subsequently argued that concomitant improvement in other management factors confounded these results 88. A randomized controlled trial of G-CSF use in severe melioidosis sepsis demonstrated a longer duration of survival when measured in hours, but no overall mortality benefit 86. The current Darwin in the Northern Territory of Australia guidelines recommend 300 μg of intravenous G-CSF daily for patients with septic shock, initiated as soon as a probable microbiological diagnosis of melioidosis is made and continuing for either 10 days or the duration of intensive care unit stay contingent on clinical progress. Contraindications to commencement or continuation include an acute coronary event or total blood white cell count of >50,000 ×106/liter 31.
Source control is an important feature in overall management 48. Abscesses in most organ systems of patients with melioidosis often resolve after antibiotic therapy; however, prostatic abscesses greater than 1 cm usually require surgical debridement and drainage 89, 90, 91, 92, 93, 94, 95.
Fever clearance may be slow, with a median of 9 days in one study, and therefore, this may not necessarily stand as an indication for surgical intervention 96. While ideal, source control may not be achieved in every circumstance, particularly in resource-limited settings. It is important to note that treatment success has been achieved with prolonged therapy in the setting of undrained abscesses 23, 94.
Table 3. Melioidosis treatment and prophylaxis
| Phase or adjustment | Drug and dose | Clinical manifestation(s) (duration of treatment) |
|---|---|---|
| Intensive |
|
|
| Renal dose adjustment | ||
| Ceftazidime | ||
| Creatinine clearance of (ml/min): | ||
| 31–50 ml/min | ≤60 kg, 1 g q8h; >60 kg, 2 g q8h | |
| 15–30 ml/min | ≤60 kg, 1 g q12h; >60 kg, 2 g q12h | |
| <15 ml/min | ≤60 kg, 1 g q24h | |
| Dialysis | ||
| Hemodialysis | As for creatinine clearance of <15 ml/min, dose post-hemodialysis | |
| Continuous ambulatory peritoneal dialysis | As for creatinine clearance of <15 ml/min, dose post-hemodialysis, may administer intraperitoneally with dwell time of >6 h and 25% extra dose for convenience | |
| Continuous renal replacement therapy | 2 g q12h | |
| Meropenem | ||
| Creatinine clearance of (ml/min): | ||
| 31–50 ml/min | 1 g q12h | |
| 15–30 ml/min | 1 g q12h | |
| <15 ml/min | 1 g q24h | |
| Dialysis | ||
| Hemodialysis | As for creatinine clearance of <15 ml/min, dose post-hemodialysis | |
| Continuous ambulatory peritoneal dialysis | As for creatinine clearance of <15 ml/min | |
| Continuous renal replacement therapy | 1 g q12h | |
| Trimethoprim-sulfamethoxazole (TMP-SMX) | ||
| Creatinine clearance of (ml/min): | ||
| 31–50 ml/min | ≤60 kg, 240/1,200 mg every 12 hours; >60 kg, 320/1,600 mg every 12 hours | |
| 15–30 ml/min | ≤60 kg, 240/1,200 mg every 24 hours; >60 kg, 320/1,600 mg every 24 hours | |
| <15 ml/min | ≤60 kg, 240/1,200 mg every 24 hours; >60 kg, 320/1,600 mg every 24 hours | |
| Dialysis | ||
| Hemodialysis | As for creatiine clearance of <15 ml/min, dose post-hemodialysis | |
| Continuous ambulatory peritoneal dialysis | As for creatiine clearance of <15 ml/min | |
| Continuous renal replacement therapy | As for creatiine clearance of 15–30 ml/min | |
| Eradication | Trimethoprim-sulfamethoxazole (child, 6/30 mg/kg up to 240/1,200 mg; adult 40–60 kg, 240/1,200 mg; >60 kg, 320/1,600 mg orally, every 12 hours) and folic acid, 5 mg (child, 0.1 mg/kg up to 5 mg) orally, daily | Pneumonia (3 mo); bacteremia, no focus (3 mo); skin and soft tissue (3 mo); abscess, deep tissue (3 mo); septic arthritis, single joint (3 mo); osteomyelitis (6 mo); neurological (6 mo); endovascular (6 mo) |
| Prophylaxis |
| High probability postexposure (3 wks) |
| Trimethoprim-sulfamethoxazole (160/800 mg orally, daily) and folic acid (5 mg orally, daily) | Hemodialysis patients, wet season, high-incidence region (26 wks) |
Melioidosis prognosis
Melioidosis overall survival is affected by multiple factors, including premorbid host determinants. Diabetes, Australian Aboriginal and/or Torres Strait Islander race, chronic renal disease, and older age negatively impact mortality 23, 16, 97, 98. In southern Thailand, septic shock on admission has a reported in-hospital mortality odds ratio of 29.14 to 68.20 99. An odds ratio (OR) is a measure of association between an exposure and an outcome. The odds ratio (OR) represents the odds that an outcome will occur given a particular exposure, compared to the odds of the outcome occurring in the absence of that exposure 100.
- Odds ratio (OR) =1 Exposure does not affect odds of outcome
- Odds ratio (OR) >1 Exposure associated with higher odds of outcome
- Odds ratio (OR) <1 Exposure associated with lower odds of outcome
It has been shown that 73.7% of patients with a positive blood culture occurring within 24 hour of incubation died during their admission. This compared with a 40.9% in-hospital mortality rate for patients whose blood cultures signaled positive more than 24 hour from incubation 56. A bacteremia quantification of ≤1 CFU/ml has been associated with a 42% mortality rate, while a positive blood culture with >100 CFU/ml resulted in a fatal outcome in 96% of patients 101.
Although mortality remains high in developing nations such as Thailand, two centers in Australia have demonstrated a remarkable decrease in overall mortality over the preceding two decades 23, 16, 102. The initial peak mortality of 30% in one facility has decreased to 9% in all patients monitored throughout treatment 23. When comparing presentation with septic shock and death over time, the improvement has been found to be dramatic, improving from 100% mortality to 27% 23. Patients over 50 years of age have an increased mortality, with an odds ratio of 2.0, compared with the rate for those under 50. The presence of any risk factor has a reported mortality odds ratio of 9.4 23. With regard to bacteremia, repeated positive blood culture after the first or second week of therapy is a strong predictor of mortality, with an odds ratio of 4.2 after adjustment for age, sex, diabetes, blood pressure, pneumonia, and duration of intravenous antibiotics. Importantly, repeated culture of Burkholderia pseudomallei from nonsterile sites did not confer increased risk of death 103. The mortality of chronic melioidosis is low and is estimated at 2% in Australia 23.
In children, the mortality rates range from 7% overall in a prospective Australian study to 16.8% in-hospital mortality from a retrospective Cambodian study 104, 83. This Cambodian study revealed a 71.8% in-hospital mortality rate in bacteremic children, and another study revealed a similarly high in-hospital mortality rate (73%) in a Thai neonatal population who presented with either neonatal meningitis or bacteremia 104, 105. Additional prospective data from Cambodia reveal an overall mortality rate of 62% 106. Specifically in Cambodia, potential reasons for a high mortality rate may be a combination of inadequate microbiology diagnostic services coupled with empirical therapy without adequate Burkholderia pseudomallei activity 107. Combined Malaysian data report an overall in-hospital mortality rate of 33 to 54% 108, 109, 97, 110, 111, 112, 113. Bacteremic patients have a mortality rate of of 48 to 65%, and nonbacteremic patients had a substantially lower case-fatality rate, 19%. Additionally, the mortality rate was 100% among those patients, while patients without septic shock had a mortality rate of 30% 108, 113.
Genetic risk factors for melioidosis-associated mortality have recently been described 114. In a study of melioidosis patients in northeast Thailand, HLA-B*46 and HLA-C*01 were associated with an increased risk of death 114. A recent evaluation of the TLR1 variants common in East Asian populations demonstrated an association with a severe bacteremic phenotype and potentially worse outcome (580). Conversely, genetic polymorphisms for two flagellin-sensing receptors, TLR5 and NLRC4, have demonstrated survival benefit in patients with melioidosis 115, 116, 117. A review of 600 Thai patients with melioidosis infection reported a protective effect with regard to in-hospital death and organ failure in patients with a TLR5 genetic variant resulting in decreased function 115. A specific NLRC4 region polymorphism was also associated with survival in patients with pulmonary involvement. Furthermore, coinheritance of both TLR5 and NLRC4 polymorphisms has a cumulative effect on survival 116. It is interesting that while these receptors are required for functional immunity, in the setting of Burkholderia pseudomallei infection they appear to have a potentially detrimental immunomodulatory effect resulting in inflammation-associated organ failure 115.
- Nguyen HVN, Smith ME, Hayoun MA. Glanders and Melioidosis. [Updated 2023 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448110[↩][↩]
- Meumann, E.M., Limmathurotsakul, D., Dunachie, S.J. et al. Burkholderia pseudomallei and melioidosis. Nat Rev Microbiol 22, 155–169 (2024). https://doi.org/10.1038/s41579-023-00972-5[↩][↩][↩]
- Ganeshalingam V, Kaestli M, Norton RE, Gassiep I. The effect of climate on melioidosis incidence in Townsville, Australia: a dry tropical region. Environ Health Prev Med. 2023;28:33. doi: 10.1265/ehpm.22-00177[↩]
- Shukla T, Smith S, Johnstone K, Donald P, Hanson J. The characteristics and clinical course of patients with melioidosis and cancer. PLoS Negl Trop Dis. 2024 Oct 25;18(10):e0012631. doi: 10.1371/journal.pntd.0012631[↩]
- Weerasinghe NP, Herath HMM, Liyanage TMU. Isolated septic arthritis of hip joint: a rare presentation of melioidosis. A case report. BMC Res Notes. 2018 Jan 19;11(1):50. doi: 10.1186/s13104-018-3171-6[↩]
- Wiersinga, W., van der Poll, T., White, N. et al. Melioidosis: insights into the pathogenicity of Burkholderia pseudomallei. Nat Rev Microbiol 4, 272–282 (2006). https://doi.org/10.1038/nrmicro1385[↩]
- This Germ Can Live Decades In Distilled Water, Kill Humans In 48 Hours. https://www.npr.org/sections/goatsandsoda/2016/01/11/462416728/this-germ-can-live-decades-in-distilled-water-kill-humans-in-48-hours[↩]
- Cheng AC, Currie BJ. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev. 2005 Apr;18(2):383-416. doi: 10.1128/CMR.18.2.383-416.2005. Erratum in: Clin Microbiol Rev. 2007 Jul;20(3):533. Dosage error in article text.[↩][↩][↩][↩][↩][↩][↩][↩]
- White NJ. Melioidosis. Lancet. 2003 May 17;361(9370):1715-22. doi: 10.1016/s0140-6736(03)13374-0[↩][↩]
- Rammaert B, Beauté J, Borand L, Hem S, Buchy P, Goyet S, Overtoom R, Angebault C, Te V, Try PL, Mayaud C, Vong S, Guillard B. Pulmonary melioidosis in Cambodia: a prospective study. BMC Infect Dis. 2011 May 14;11:126. doi: 10.1186/1471-2334-11-126[↩]
- Suputtamongkol Y, Chaowagul W, Chetchotisakd P, Lertpatanasuwun N, Intaranongpai S, Ruchutrakool T, Budhsarawong D, Mootsikapun P, Wuthiekanun V, Teerawatasook N, Lulitanond A. Risk factors for melioidosis and bacteremic melioidosis. Clin Infect Dis. 1999 Aug;29(2):408-13. doi: 10.1086/520223[↩]
- Melioidosis. https://www.cdc.gov/melioidosis/about[↩][↩][↩]
- Whitmore A, Krishnaswami CS. A Hitherto Undescribed Infective Disease in Rangoon. Ind Med Gaz. 1912 Jul;47(7):262-267. https://pmc.ncbi.nlm.nih.gov/articles/instance/5168169/pdf/indmedgaz71624-0010.pdf [↩]
- Limmathurotsakul D, Golding N, Dance DA, Messina JP, Pigott DM, Moyes CL, et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nat Microbiol. 2016;1(1). doi: 10.1038/nmicrobiol.2015.8[↩]
- Cheng AC, Currie BJ. 2005. Melioidosis: epidemiology, pathophysiology, and management. Clin Microbiol Rev 18:383–416. doi: 10.1128/CMR.18.2.383-416.2005[↩][↩][↩]
- Stewart JD, Smith S, Binotto E, McBride WJ, Currie BJ, Hanson J. 2017. The epidemiology and clinical features of melioidosis in Far North Queensland: implications for patient management. PLoS Negl Trop Dis 11:e0005411. doi: 10.1371/journal.pntd.0005411[↩][↩][↩]
- Chaowagul W, White NJ, Dance DA, Wattanagoon Y, Naigowit P, Davis TM, Looareesuwan S, Pitakwatchara N. Melioidosis: a major cause of community-acquired septicemia in northeastern Thailand. J Infect Dis. 1989 May;159(5):890-9. doi: 10.1093/infdis/159.5.890[↩]
- Currie BJ, Fisher DA, Howard DM, Burrow JN, Selvanayagam S, Snelling PL, Anstey NM, Mayo MJ. The epidemiology of melioidosis in Australia and Papua New Guinea. Acta Trop. 2000 Feb 5;74(2-3):121-7. doi: 10.1016/s0001-706x(99)00060-1[↩]
- Douglas MW, Lum G, Roy J, Fisher DA, Anstey NM, Currie BJ. Epidemiology of community-acquired and nosocomial bloodstream infections in tropical Australia: a 12-month prospective study. Trop Med Int Health. 2004 Jul;9(7):795-804. doi: 10.1111/j.1365-3156.2004.01269.x[↩]
- Zembower TR. Epidemiology of infections in cancer patients. Cancer Treat Res. 2014;161:43-89. doi: 10.1007/978-3-319-04220-6_2[↩]
- Gassiep I, Armstrong M, Norton R. Human Melioidosis. Clin Microbiol Rev. 2020 Mar 11;33(2):e00006-19. doi: 10.1128/CMR.00006-19[↩][↩][↩][↩][↩][↩][↩][↩]
- Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med. 2012 Sep 13;367(11):1035-44. doi: 10.1056/NEJMra1204699[↩]
- Currie BJ, Ward L, Cheng AC. 2010. The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS Negl Trop Dis 4:e900. doi: 10.1371/journal.pntd.0000900[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Currie BJ, Price EP, Mayo M, Kaestli M, Theobald V, Harrington I, Harrington G, Sarovich DS. 2015. Use of whole-genome sequencing to link Burkholderia pseudomallei from air sampling to mediastinal melioidosis, Australia. Emerg Infect Dis 21:2052–2054. doi: 10.3201/eid2111.141802[↩][↩]
- Chen P-S, Chen Y-S, Lin H-H, Liu P-J, Ni W-F, Hsueh P-T, Liang S-H, Chen C, Chen Y-L. 2015. Airborne transmission of melioidosis to humans from environmental aerosols contaminated with B. pseudomallei. PLoS Negl Trop Dis 9:e0003834. doi: 10.1371/journal.pntd.0003834[↩][↩]
- Meumann EM, Cheng AC, Ward L, Currie BJ. Clinical features and epidemiology of melioidosis pneumonia: results from a 21-year study and review of the literature. Clin Infect Dis. 2012 Feb 1;54(3):362-9. doi: 10.1093/cid/cir808[↩][↩][↩]
- Pagnarith Y, Kumar V, Thaipadungpanit J, Wuthiekanun V, Amornchai P, Sin L, Day NP, Peacock SJ. Emergence of pediatric melioidosis in Siem Reap, Cambodia. Am J Trop Med Hyg. 2010 Jun;82(6):1106-12. doi: 10.4269/ajtmh.2010.10-0030[↩][↩][↩]
- Melioidosis Signs and Symptoms. https://www.cdc.gov/melioidosis/symptoms/index.html[↩]
- Melioidosis. http://www.checkorphan.org/diseases/meliodosis[↩][↩]
- Lipsitz R, Garges S, Aurigemma R, Baccam P, Blaney DD, Cheng AC, Currie BJ, Dance D, Gee JE, Larsen J, Limmathurotsakul D, Morrow MG, Norton R, O’Mara E, Peacock SJ, Pesik N, Rogers LP, Schweizer HP, Steinmetz I, Tan G, Tan P, Wiersinga WJ, Wuthiekanun V, Smith TL. 2012. Workshop on treatment of and postexposure prophylaxis for Burkholderia pseudomallei and B. mallei infection, 2010. Emerg Infect Dis 18:e2. doi: 10.3201/eid1812.120638[↩][↩][↩][↩][↩]
- Currie BJ. 2014. Melioidosis: the 2014 revised RDH guideline. Northern Territ Dis Control Bull 21:4–8.[↩][↩][↩][↩][↩][↩][↩]
- Chetchotisakd P, Chierakul W, Chowagul V, et al. Trimethoprim-sulfamethoxazole alone or with doxycycline for eradication phase treatment of melioidosis (MERTH-study group). Presented at the VI World Melioidosis Congress, Townsville, QL, Australia, December 3, 2010.[↩][↩][↩][↩]
- Peacock SJ, Schweizer HP, Dance DA, Smith TL, Gee JE, Wuthiekanun V, DeShazer D, Steinmetz I, Tan P, Currie BJ. Management of accidental laboratory exposure to Burkholderia pseudomallei and B. mallei. Emerg Infect Dis. 2008 Jul;14(7):e2. doi: 10.3201/eid1407.071501[↩][↩][↩]
- Simpson AJ, Suputtamongkol Y, Smith MD, Angus BJ, Rajanuwong A, Wuthiekanun V, Howe PA, Walsh AL, Chaowagul W, White NJ. Comparison of imipenem and ceftazidime as therapy for severe melioidosis. Clin Infect Dis. 1999 Aug;29(2):381-7. doi: 10.1086/520219[↩][↩]
- Wiersinga WJ, Currie BJ, Peacock SJ. Melioidosis. N Engl J Med. 2012 Sep 13;367(11):1035-44. https://www.nejm.org/doi/full/10.1056/NEJMra1204699[↩][↩][↩][↩][↩][↩]
- Inglis TJ, Sagripanti J-L. 2006. Environmental factors that affect the survival and persistence of Burkholderia pseudomallei. Appl Environ Microbiol 72:6865–6875. doi: 10.1128/AEM.01036-06[↩]
- Phillips ED, Garcia EC. Burkholderia pseudomallei. Trends Microbiol. 2024 Jan;32(1):105-106. doi: 10.1016/j.tim.2023.07.008[↩]
- Currie BJ, Fisher DA, Anstey NM, Jacups SP. Melioidosis: acute and chronic disease, relapse and re-activation. Trans R Soc Trop Med Hyg. 2000 May-Jun;94(3):301-4. doi: 10.1016/s0035-9203(00)90333-x[↩]
- Chierakul W, Winothai W, Wattanawaitunechai C, Wuthiekanun V, Rugtaengan T, Rattanalertnavee J, Jitpratoom P, Chaowagul W, Singhasivanon P, White NJ, Day NP, Peacock SJ. Melioidosis in 6 tsunami survivors in southern Thailand. Clin Infect Dis. 2005 Oct 1;41(7):982-90. doi: 10.1086/432942[↩]
- Ngauy V, Lemeshev Y, Sadkowski L, Crawford G. Cutaneous melioidosis in a man who was taken as a prisoner of war by the Japanese during World War II. J Clin Microbiol. 2005 Feb;43(2):970-2. doi: 10.1128/JCM.43.2.970-972.2005[↩]
- Depoorter E, Bull MJ, Peeters C, Coenye T, Vandamme P, Mahenthiralingam E. 2016. Burkholderia: an update on taxonomy and biotechnological potential as antibiotic producers. Appl Microbiol Biotechnol 100:5215–5229. doi: 10.1007/s00253-016-7520-x[↩]
- LiPuma JJ, Currie BJ, Peacock SJ, Vandamme PWE. 2015. Burkholderia, Stenotrophomonas, Ralstonia, Cupriavidus, Pandoraea, Brevundimonas, Comamonas, Delftia, and Acidovorax, p 791–812. In Jorgensen JH, Pfaller MA, Carroll KC, Funke G, Landry ML, Richter SS, Warnock DW (ed), Manual of clinical microbiology, 11th ed ASM Press, Washington, DC.[↩][↩]
- Stewart T, Engelthaler DM, Blaney DD, Tuanyok A, Wangsness E, Smith TL, Pearson T, Komatsu KK, Keim P, Currie BJ, Levy C, Sunenshine R. Epidemiology and investigation of melioidosis, Southern Arizona. Emerg Infect Dis. 2011 Jul;17(7):1286-8. doi: 10.3201/eid1707.100661[↩]
- Deshazer D. Virulence of clinical and environmental isolates of Burkholderia oklahomensis and Burkholderia thailandensis in hamsters and mice. FEMS Microbiol Lett. 2007 Dec;277(1):64-9. doi: 10.1111/j.1574-6968.2007.00946.x[↩]
- Currie BJ, Ward L, Cheng AC. The epidemiology and clinical spectrum of melioidosis: 540 cases from the 20 year Darwin prospective study. PLoS Negl Trop Dis. 2010 Nov 30;4(11):e900. doi: 10.1371/journal.pntd.0000900[↩][↩][↩][↩][↩][↩][↩]
- Limmathurotsakul D, Wongratanacheewin S, Teerawattanasook N, Wongsuvan G, Chaisuksant S, Chetchotisakd P, Chaowagul W, Day NP, Peacock SJ. Increasing incidence of human melioidosis in Northeast Thailand. Am J Trop Med Hyg. 2010 Jun;82(6):1113-7. doi: 10.4269/ajtmh.2010.10-0038[↩][↩]
- Peacock SJ, Schweizer HP, Dance DAB, Smith TL, Gee JE, Wuthiekanun V, DeShazer D, Steinmetz I, Tan P, Currie BJ. 2008. Management of accidental laboratory exposure to Burkholderia pseudomallei and B. mallei. Emerg Infect Dis 14:e2. doi: 10.3201/eid1407.071501[↩][↩]
- Dance D. 2014. Treatment and prophylaxis of melioidosis. Int J Antimicrob Agents 43:310–318. doi: 10.1016/j.ijantimicag.2014.01.005[↩][↩]
- Sivalingam SP, Sim SH, Jasper LCW, Wang D, Liu Y, Ooi EE. 2008. Pre- and post-exposure prophylaxis of experimental Burkholderia pseudomallei infection with doxycycline, amoxicillin/clavulanic acid and co-trimoxazole. J Antimicrob Chemother 61:674–678. doi: 10.1093/jac/dkm527[↩]
- Barnes KB, Steward J, Thwaite JE, Lever MS, Davies CH, Armstrong SJ, Laws TR, Roughley N, Harding SV, Atkins TP, Simpson AJH, Atkins HS. 2013. Trimethoprim/sulfamethoxazole (co-trimoxazole) prophylaxis is effective against acute murine inhalational melioidosis and glanders. Int J Antimicrob Agents 41:552–557. doi: 10.1016/j.ijantimicag.2013.02.007[↩]
- Majoni SW, Hughes JT, Heron B, Currie BJ. 2018. Trimethoprim+sulfamethoxazole reduces rates of melioidosis in high-risk hemodialysis patients. Kidney Int Rep 3:160–167. doi: 10.1016/j.ekir.2017.09.005[↩]
- Chau KWT, Smith S, Kang K, Dheda S, Hanson J. 2018. Antibiotic prophylaxis for melioidosis in patients receiving hemodialysis in the tropics? One size does not fit all. Am J Trop Med Hyg 99:597–600. doi: 10.4269/ajtmh.18-0421[↩]
- Limmathurotsakul D, Chaowagul W, Chierakul W, Stepniewska K, Maharjan B, Wuthiekanun V, White NJ, Day NP, Peacock SJ. Risk factors for recurrent melioidosis in northeast Thailand. Clin Infect Dis. 2006 Oct 15;43(8):979-86. doi: 10.1086/507632[↩][↩][↩]
- Limmathurotsakul D, Jamsen K, Arayawichanont A, Simpson JA, White LJ, Lee SJ, Defining the true sensitivity of culture for the diagnosis of melioidosis using Bayesian latent class models. PLoS ONE. 2010;5:e12485[↩]
- Wuthiekanun V, Dance DAB, Wattanagoon Y, Supputtamongkol Y, Chaowagul W, White NJ. 1990. The use of selective media for the isolation of Pseudomonas pseudomallei in clinical practice. J Med Microbiol 33:121–126. doi: 10.1099/00222615-33-2-121[↩]
- Tiangpitayakorn C, Songsivilai S, Piyasangthong N, Dharakul T. 1997. Speed of detection of Burkholderia pseudomallei in blood cultures and its correlation with the clinical outcome. Am J Trop Med Hyg 57:96–99. doi: 10.4269/ajtmh.1997.57.96[↩][↩]
- Teerawattanasook N, Limmathurotsakul D, Day NPJ, Wuthiekanun V. 2014. Failure of Burkholderia pseudomallei to grow in an automated blood culture system. Am J Trop Med Hyg 91:1173–1175. doi: 10.4269/ajtmh.14-0018[↩][↩]
- Jorakate P, Higdon M, Kaewpan A, Makprasert S, Yuenprakhon S, Tawisaid K, Dejsirilert S, Whistler T, Baggett HC. 2015. Contribution of the BacT/Alert MB Mycobacterium bottle to bloodstream infection surveillance in Thailand: added yield for Burkholderia pseudomallei. J Clin Microbiol 53:910–914. doi: 10.1128/JCM.02008-14[↩]
- Udayan U, Dias M. 2014. Evaluation of BACTEC™ blood culture system for culture of normally sterile body fluids. Indian J Crit Care Med 18:829–830. doi: 10.4103/0972-5229.146331[↩]
- Chantratita N, Tandhavanant S, Wongsuvan G, Wuthiekanun V, Teerawattanasook N, Day NPJ, Limmathurotsakul D, Peacock SJ. 2013. Rapid detection of Burkholderia pseudomallei in blood cultures using a monoclonal antibody-based immunofluorescent assay. Am J Trop Med Hyg 89:971–972. doi: 10.4269/ajtmh.13-0212[↩]
- Limmathurotsakul D, Wuthiekanun V, Chierakul W, Cheng AC, Maharjan B, Chaowagul W, White NJ, Day NP, Peacock SJ. 2005. Role and significance of quantitative urine cultures in diagnosis of melioidosis. J Clin Microbiol 43:2274–2276. doi: 10.1128/JCM.43.5.2274-2276.2005[↩][↩]
- Cheng AC, Wuthiekanun V, Limmathurosakul D, Wongsuvan G, Day NP, Peacock SJ. 2006. Role of selective and nonselective media for isolation of Burkholderia pseudomallei from throat swabs of patients with melioidosis. J Clin Microbiol 44:2316. doi: 10.1128/JCM.00231-06[↩]
- Hoffmaster AR, AuCoin D, Baccam P, Baggett HC, Baird R, Bhengsri S, Blaney DD, Brett PJ, Brooks TJ, Brown KA, Chantratita N, Cheng AC, Dance DA, Decuypere S, Defenbaugh D, Gee JE, Houghton R, Jorakate P, Lertmemongkolchai G, Limmathurotsakul D, Merlin TL, Mukhopadhyay C, Norton R, Peacock SJ, Rolim DB, Simpson AJ, Steinmetz I, Stoddard RA, Stokes MM, Sue D, Tuanyok A, Whistler T, Wuthiekanun V, Walke HT. 2015. Melioidosis diagnostic workshop, 2013. Emerg Infect Dis doi: 10.3201/eid2102.141045[↩]
- Bowers JR, Engelthaler DM, Ginther JL, Pearson T, Peacock SJ, Tuanyok A, BurkDiff: a real-time PCR allelic discrimination assay for Burkholderia pseudomallei and B. mallei. PLoS ONE. 2010;5:e15413[↩]
- Richardson LJ, Kaestli M, Mayo M, Bowers JR, Tuanyok A, Schupp J, Engelthaler D, Wagner DM, Keim PS, Currie BJ. Towards a rapid molecular diagnostic for melioidosis: Comparison of DNA extraction methods from clinical specimens. J Microbiol Methods. 2012 Jan;88(1):179-81. doi: 10.1016/j.mimet.2011.10.023[↩]
- Chantratita N, Wuthiekanun V, Limmathurotsakul D, Thanwisai A, Chantratita W, Day NP, Peacock SJ. Prospective clinical evaluation of the accuracy of 16S rRNA real-time PCR assay for the diagnosis of melioidosis. Am J Trop Med Hyg. 2007 Nov;77(5):814-7.[↩]
- Wuthiekanun V, Chierakul W, Langa S, Chaowagul W, Panpitpat C, Saipan P, Thoujaikong T, Day NP, Peacock SJ. Development of antibodies to Burkholderia pseudomallei during childhood in melioidosis-endemic northeast Thailand. Am J Trop Med Hyg. 2006 Jun;74(6):1074-5.[↩]
- Ashdown LR. An improved screening technique for isolation of Pseudomonas pseudomallei from clinical specimens. Pathology. 1979;11:293–7[↩]
- Trunck LA, Propst KL, Wuthiekanun V, Tuanyok A, Beckstrom-Sternberg SM, Beckstrom-Sternberg JS, Molecular basis of rare aminoglycoside susceptibility and pathogenesis of Burkholderia pseudomallei clinical isolates from Thailand. PLoS Negl Trop Dis. 2009;3:e519[↩]
- Peacock SJ, Chieng G, Cheng AC, Dance DA, Amornchai P, Wongsuvan G, Comparison of Ashdown’s medium, Burkholderia cepacia medium, and Burkholderia pseudomallei selective agar for clinical isolation of Burkholderia pseudomallei. J Clin Microbiol. 2005;43:5359–61[↩]
- Amornchai P, Chierakul W, Wuthiekanun V, Mahakhunkijcharoen Y, Phetsouvanh R, Currie BJ, Accuracy of Burkholderia pseudomallei identification using the API 20NE system and a latex agglutination test. J Clin Microbiol. 2007;45:3774–6[↩]
- Wuthiekanun V, Desakorn V, Wongsuvan G, Amornchai P, Cheng AC, Maharjan B, Rapid immunofluorescence microscopy for diagnosis of melioidosis. Clin Diagn Lab Immunol. 2005;12:555–6[↩]
- Tiangpitayakorn C, Songsivilai S, Piyasangthong N, Dharakul T. Speed of detection of Burkholderia pseudomallei in blood cultures and its correlation with the clinical outcome. Am J Trop Med Hyg. 1997;57:96–9[↩]
- Cheng AC, McBryde ES, Wuthiekanun V, Chierakul W, Amornchai P, Day NP, White NJ, Peacock SJ. 2009. Dosing regimens of cotrimoxazole (trimethoprim-sulfamethoxazole) for melioidosis. Antimicrob Agents Chemother 53:4193–4199. doi: 10.1128/AAC.01301-08[↩]
- Cheng AC, Chierakul W, Chaowagul W, Chetchotisakd P, Limmathurotsakul D, Dance DA, Peacock SJ, Currie BJ. 2008. Consensus guidelines for dosing of amoxicillin-clavulanate in melioidosis. Am J Trop Med Hyg 78:208–209. doi: 10.4269/ajtmh.2008.78.208[↩]
- Chaowagul W, Simpson AJ, Suputtamongkol Y, Smith MD, Angus BJ, White NJ. 1999. A comparison of chloramphenicol, trimethoprim-sulfamethoxazole, and doxycycline with doxycycline alone as maintenance therapy for melioidosis. Clin Infect Dis 29:375–380. doi: 10.1086/520218[↩]
- Chaowagul W, Chierakul W, Simpson AJ, Short JM, Stepniewska K, Maharjan B, Rajchanuvong A, Busarawong D, Limmathurotsakul D, Cheng AC, Wuthiekanun V, Newton PN, White NJ, Day NP, Peacock SJ. 2005. Open-label randomized trial of oral trimethoprim-sulfamethoxazole, doxycycline, and chloramphenicol compared with trimethoprim-sulfamethoxazole and doxycycline for maintenance therapy of melioidosis. Antimicrob Agents Chemother 49:4020–4025. doi: 10.1128/AAC.49.10.4020-4025.2005[↩]
- Chetchotisakd P, Chierakul W, Chaowagul W, Anunnatsiri S, Phimda K, Mootsikapun P, Chaisuksant S, Pilaikul J, Thinkhamrop B, Phiphitaporn S, Susaengrat W, Toondee C, Wongrattanacheewin S, Wuthiekanun V, Chantratita N, Thaipadungpanit J, Day NP, Limmathurotsakul D, Peacock SJ. 2014. Trimethoprim-sulfamethoxazole versus trimethoprim-sulfamethoxazole plus doxycycline as oral eradicative treatment for melioidosis (MERTH): a multicentre, double-blind, non-inferiority, randomised controlled trial. Lancet 383:807–814. doi: 10.1016/S0140-6736(13)61951-0[↩]
- Pitman MC, Luck T, Marshall CS, Anstey NM, Ward L, Currie BJ. 2015. Intravenous therapy duration and outcomes in melioidosis: a new treatment paradigm. PLoS Negl Trop Dis 9:e0003586. doi: 10.1371/journal.pntd.0003586[↩][↩][↩][↩][↩]
- Shetty RP, Mathew M, Smith J, Morse LP, Mehta JA, Currie BJ. 2015. Management of melioidosis osteomyelitis and septic arthritis. Bone Joint J 97-b:277–282. doi: 10.1302/0301-620X.97B2.34799[↩]
- Limmathurotsakul D, Chaowagul W, Chierakul W, Stepniewska K, Maharjan B, Wuthiekanun V, White NJ, Day NP, Peacock SJ. 2006. Risk factors for recurrent melioidosis in northeast Thailand. Clin Infect Dis 43:979–986. doi: 10.1086/507632[↩][↩]
- Chetchotisakd P, Chierakul W, Chaowagul W, et al. 2014. Trimethoprim-sulfamethoxazole versus trimethoprim-sulfamethoxazole plus doxycycline as oral eradicative treatment for melioidosis (MERTH): a multicentre, double-blind, non-inferiority, randomised controlled trial. Lancet 383:807–814. doi: 10.1016/S0140-6736(13)61951-0[↩]
- McLeod C, Morris PS, Bauert PA, Kilburn CJ, Ward LM, Baird RW, Currie BJ. 2015. Clinical presentation and medical management of melioidosis in children: a 24-year prospective study in the Northern Territory of Australia and review of the literature. Clin Infect Dis 60:21–26. doi: 10.1093/cid/ciu733[↩][↩]
- Gibney KB, Cheng AC, Currie BJ. 2008. Cutaneous melioidosis in the tropical top end of Australia: a prospective study and review of the literature. Clin Infect Dis 47:603–609. doi: 10.1086/590931[↩]
- Cheng AC, Dasari P, Currie BJ. 2004. Granulocyte colony-stimulating factor and an in vitro whole blood model of melioidosis. Eur J Clin Microbiol Infect Dis 23:205–207. doi: 10.1007/s10096-003-1088-y[↩]
- Cheng AC, Limmathurotsakul D, Chierakul W, Getchalarat N, Wuthiekanun V, Stephens DP, Day NP, White NJ, Chaowagul W, Currie BJ, Peacock SJ. 2007. A randomized controlled trial of granulocyte colony-stimulating factor for the treatment of severe sepsis due to melioidosis in Thailand. Clin Infect Dis 45:308–314. doi: 10.1086/519261[↩][↩]
- Cheng AC, Stephens DP, Anstey NM, Currie BJ. 2004. Adjunctive granulocyte colony-stimulating factor for treatment of septic shock due to melioidosis. Clin Infect Dis 38:32–37. doi: 10.1086/380456[↩][↩]
- Currie BJ. 2015. Melioidosis: evolving concepts in epidemiology, pathogenesis, and treatment. Semin Respir Crit Care Med 36:111–125. doi: 10.1055/s-0034-1398389[↩]
- Georgiades C, Fishman EK. Clinical image. Glanders disease of the liver and spleen: CT evaluation. J Comput Assist Tomogr. 2001 Jan-Feb;25(1):91-3. doi: 10.1097/00004728-200101000-00016[↩]
- Limmathurotsakul D, Funnell SG, Torres AG, Morici LA, Brett PJ, Dunachie S, Atkins T, Altmann DM, Bancroft G, Peacock SJ; Steering Group on Melioidosis Vaccine Development. Consensus on the development of vaccines against naturally acquired melioidosis. Emerg Infect Dis. 2015 Jun;21(6):e141480. doi: 10.3201/eid2106.141480[↩]
- Hatcher CL, Muruato LA, Torres AG. Recent Advances in Burkholderia mallei and B. pseudomallei Research. Curr Trop Med Rep. 2015 Jun;2(2):62-69. doi: 10.1007/s40475-015-0042-2[↩]
- Podnecky NL, Rhodes KA, Schweizer HP. Efflux pump-mediated drug resistance in Burkholderia. Front Microbiol. 2015 Apr 14;6:305. doi: 10.3389/fmicb.2015.00305[↩]
- Cheng AC, Currie BJ, Dance DAB, Funnell SGP, Limmathurotsakul D, Simpson AJH, Peacock SJ. Clinical definitions of melioidosis. Am J Trop Med Hyg. 2013 Mar;88(3):411-413. doi: 10.4269/ajtmh.12-0555[↩]
- Morse LP, Morse LP, Moller C-CB, Harvey E, Ward L. 2009. Prostatic abscess due to Burkholderia pseudomallei: 81 cases from a 19-year prospective melioidosis study. J Urol 182:542–547. doi: 10.1016/j.juro.2009.04.010[↩][↩]
- Currie BJ, Fisher DA, Howard DM, Burrow JN, Lo D, Selva-Nayagam S, Anstey NM, Huffam SE, Snelling PL, Marks PJ, Stephens DP, Lum GD, Jacups SP, Krause VL. 2000. Endemic melioidosis in tropical northern Australia: a 10-year prospective study and review of the literature. Clin Infect Dis 31:981–986. doi: 10.1086/318116[↩]
- Simpson AJ, Suputtamongkol Y, Smith MD, Angus BJ, Rajanuwong A, Wuthiekanun V, Howe PA, Walsh AL, Chaowagul W, White NJ. 1999. Comparison of imipenem and ceftazidime as therapy for severe melioidosis. Clin Infect Dis 29:381–387. doi: 10.1086/520219[↩]
- Hassan MRA, Pani SP, Peng NP, Voralu K, Vijayalakshmi N, Mehanderkar R, Aziz NA, Michael E. 2010. Incidence, risk factors and clinical epidemiology of melioidosis: a complex socio-ecological emerging infectious disease in the Alor Setar region of Kedah, Malaysia. BMC Infect Dis 10:302. doi: 10.1186/1471-2334-10-302[↩][↩]
- Vlieghe E, Kruy L, Smet B, Kham C, Veng CH, Phe T, Koole O, Thai S, Lynen L, Jacobs J. 2011. Melioidosis, Phnom Penh, Cambodia. Emerg Infect Dis 17:1289–1292. doi: 10.3201/eid1707.101069[↩]
- Churuangsuk C, Chusri S, Hortiwakul T, Charernmak B, Silpapojakul K. 2016. Characteristics, clinical outcomes and factors influencing mortality of patients with melioidosis in southern Thailand: a 10-year retrospective study. Asian Pac J Trop Med 9:256–260. doi: 10.1016/j.apjtm.2016.01.034[↩]
- Szumilas M. Explaining odds ratios. J Can Acad Child Adolesc Psychiatry. 2010 Aug;19(3):227-9. Erratum in: J Can Acad Child Adolesc Psychiatry. 2015 Winter;24(1):58. https://pmc.ncbi.nlm.nih.gov/articles/PMC2938757[↩]
- Walsh AL, Smith MD, Wuthiekanun V, Suputtamongkol Y, Chaowagul W, Dance DA, Angus B, White NJ. 1995. Prognostic significance of quantitative bacteremia in septicemic melioidosis. Clin Infect Dis 21:1498–1500. doi: 10.1093/clinids/21.6.1498[↩]
- Limmathurotsakul D, Wongratanacheewin S, Teerawattanasook N, Wongsuvan G, Chaisuksant S, Chetchotisakd P, Chaowagul W, Day NPJ, Peacock SJ. 2010. Increasing incidence of human melioidosis in northeast Thailand. Am J Trop Med Hyg 82:1113–1117. doi: 10.4269/ajtmh.2010.10-0038[↩]
- Limmathurotsakul D, Wuthiekanun V, Wongsuvan G, Pangmee S, Amornchai P, Teparrakkul P, Teerawattanasook N, Day NPJ, Peacock SJ. 2011. Repeat blood culture positive for B. pseudomallei indicates an increased risk of death from melioidosis. Am J Trop Med Hyg 84:858–861. doi: 10.4269/ajtmh.2011.10-0618[↩]
- Turner P, Kloprogge S, Miliya T, Soeng S, Tan P, Sar P, Yos P, Moore CE, Wuthiekanun V, Limmathurotsakul D, Turner C, Day NPJ, Dance DAB. 2016. A retrospective analysis of melioidosis in Cambodian children, 2009–2013. BMC Infect Dis 16:688. doi: 10.1186/s12879-016-2034-9[↩][↩]
- Thatrimontrichai A, Maneenil G. 2012. Neonatal melioidosis: systematic review of the literature. Pediatr Infect Dis J 31:1195–1197. doi: 10.1097/INF.0b013e318265ac62[↩]
- Rammaert B, Beaute J, Borand L, Hem S, Buchy P, Goyet S, Overtoom R, Angebault C, Te V, Try PL, Mayaud C, Vong S, Guillard B. 2011. Pulmonary melioidosis in Cambodia: a prospective study. BMC Infect Dis 11:126. doi: 10.1186/1471-2334-11-126[↩]
- Om C, Daily F, Vlieghe E, McLaughlin JC, McLaws M-L. 2016. “If it’s a broad spectrum, it can shoot better”: inappropriate antibiotic prescribing in Cambodia. Antimicrob Resist Infect Control 5:58. doi: 10.1186/s13756-016-0159-7[↩]
- Zueter AR, Yean CY, Abumarzouq M, Rahman ZA, Deris ZZ, Harun A. 2016. The epidemiology and clinical spectrum of melioidosis in a teaching hospital in a North-Eastern state of Malaysia: a fifteen-year review. BMC Infect Dis 16:333. doi: 10.1186/s12879-016-1583-2[↩][↩]
- Nathan S, Chieng S, Kingsley P, Mohan A, Podin Y, Ooi M-H, Mariappan V, Vellasamy K, Vadivelu J, Daim S, How S-H. 2018. Melioidosis in Malaysia: incidence, clinical challenges, and advances in understanding pathogenesis. Trop Med Infect Dis 3:25. doi: 10.3390/tropicalmed3010025[↩]
- Puthucheary SD, Parasakthi N, Lee MK. 1992. Septicaemic melioidosis: a review of 50 cases from Malaysia. Trans R Soc Trop Med Hyg 86:683–685. doi: 10.1016/0035-9203(92)90191-e[↩]
- How SH, Ng KH, Jamalludin AR, Shah A, Rathor Y. Melioidosis in Pahang, Malaysia. Med J Malaysia. 2005 Dec;60(5):606-13. https://www.e-mjm.org/2005/v60n5/Melioidosis_Pahang.pdf[↩]
- Pagalavan L. Melioidosis: the Johor Bahru experience. Med J Malaysia. 2005 Dec;60(5):599-605. https://www.e-mjm.org/2005/v60n5/Melioidosis_Johor_Bahru.pdf[↩]
- Kingsley PV, Leader M, Nagodawithana NS, Tipre M, Sathiakumar N. 2016. Melioidosis in Malaysia: a review of case reports. PLoS Negl Trop Dis 10:e0005182. doi: 10.1371/journal.pntd.0005182[↩][↩]
- Dunachie SJ, Jenjaroen K, Reynolds CJ, Quigley KJ, Sergeant R, Sumonwiriya M, Chaichana P, Chumseng S, Ariyaprasert P, Lassaux P, Gourlay L, Promwong C, Teparrukkul P, Limmathurotsakul D, Day NPJ, Altmann DM, Boyton RJ. 2017. Infection with Burkholderia pseudomallei—immune correlates of survival in acute melioidosis. Sci Rep 7:12143. doi: 10.1038/s41598-017-12331-5[↩][↩]
- West TE, Chantratita N, Chierakul W, Limmathurotsakul D, Wuthiekanun V, Myers ND, Emond MJ, Wurfel MM, Hawn TR, Peacock SJ, Skerrett SJ. 2013. Impaired TLR5 functionality is associated with survival in melioidosis. J Immunol 190:3373–3379. doi: 10.4049/jimmunol.1202974[↩][↩][↩]
- West TE, Myers ND, Chantratita N, Chierakul W, Limmathurotsakul D, Wuthiekanun V, Miao EA, Hajjar AM, Peacock SJ, Liggitt HD, Skerrett SJ. 2014. NLRC4 and TLR5 each contribute to host defense in respiratory melioidosis. PLoS Negl Trop Dis 8:e3178. doi: 10.1371/journal.pntd.0003178[↩][↩]
- Chantratita N, Tandhavanant S, Myers ND, Chierakul W, Robertson JD, Mahavanakul W, Singhasivanon P, Emond MJ, Peacock SJ, West TE. 2014. Screen of whole blood responses to flagellin identifies TLR5 variation associated with outcome in melioidosis. Genes Immun 15:63–71. doi: 10.1038/gene.2013.60[↩]




{kind=link}