Contents
- Primary amebic meningoencephalitis
- How does infection with Naegleria fowleri ameba occur?
- Where is Naegleria fowleri ameba found?
- Can I get a Naegleria fowleri infection from a disinfected swimming pool?
- How common is Naegleria fowleri in the environment?
- How will the public know if a lake or other water body has Naegleria fowleri?
- How common are Naegleria fowleri infections in the United States?
- Is there a routine and rapid test for Naegleria fowleri ameba in the water?
- When do Naegleria fowleri infections most commonly occur?
- What swimming behaviors have been associated with Naegleria fowleri infection?
- How can I reduce the risk of infection with Naegleria fowleri ameba?
- How does the risk of Naegleria fowleri infection compare to other water related risks?
- Can Naegleria fowleri infection be spread from one person to another?
- What is the cause of death from Naegleria fowleri infection?
- What is the fatality rate for an infected person who begins to show signs and symptoms?
- Is there effective treatment for Naegleria fowleri infection?
- What should I do if I have been swimming or playing in freshwater and now think I have symptoms associated with Naegleria fowleri infection?
- Meningoencephalitis causes
- Naegleria fowleri life cycle
- Meningoencephalitis symptoms
- Meningoencephalitis diagnosis
- Meningoencephalitis treatment
Primary amebic meningoencephalitis
Primary amebic meningoencephalitis also called primary amoebic meningoencephalitis or amoebic meningitis, is a rare and serious disease that leads to inflammation of the brain. It’s caused by the Naegleria Fowleri ameba, commonly referred to as the “brain-eating amoeba” or “brain-eating ameba”. The Naegleria fowleri ameba is commonly found in warm freshwater (e.g. lakes, rivers, and hot springs) and soil. The Naegleria Fowleri ameba (a single-cell organism) grows in warm, untreated water and flourishes in temperatures between 77°F (25°C) and 104 °F (40°C). Naegleria fowleri is a heat-loving (thermophilic) organism. Naegleria fowleri grows best at higher temperatures up to 115°F (46°C) and can survive for short periods at higher temperatures. Naegleria Fowleri ameba can be found in stagnant water such as lakes and rivers or poorly maintained swimming pools, water hoses and spas, although it’s extremely rare to contract primary amebic meningoencephalitis from a swimming pool. Naegleria fowleri usually infects people when contaminated water enters the body through the nose, through activities such as jumping, diving or falling into the water. Once the ameba enters the nose, it travels to the brain where it causes primary amebic meningoencephalitis, which is usually fatal. Infection typically occurs when people go swimming or diving in warm freshwater places, like lakes and rivers. In very rare instances, Naegleria infections may also occur when contaminated water from other sources (such as inadequately chlorinated swimming pool water or heated and contaminated tap water) enters the nose 1. You cannot get infected from swallowing water contaminated with Naegleria. You cannot get primary amebic meningoencephalitis from swallowing infected water.
Although it is believed many people come into contact with the parasite, only a handful of people have contracted primary amebic meningoencephalitis.
Symptoms of primary amebic meningoencephalitis infection includes:
- high fever
- severe and persistent headache
- stiff neck
- confusion or hallucinations
- sleepiness
- sore throat
- nausea and vomiting
- disturbances of taste and smell
- seizures (fits)
These symptoms are common for many other conditions, including viral and bacterial forms of meningitis. It’s important to urgently see a doctor for diagnosis.
While primary amebic meningoencephalitis infection can occur at any age, children and young adults seem more susceptible to the disease.
Primary amebic meningoencephalitis is very rare and unfortunately the infection usually leads to death 2. Only 4 people in the U.S. out of 145 have survived infection from 1962 to 2018 3.
Ways to help reduce the risk include:
- ensuring swimming pools are chlorinated and well maintained
- avoiding getting water up the nose in fresh water lakes and pools
- flush out old water before allowing children to play with hoses or sprinklers
- use fresh water in collapsible wading pools
- keeping your head above the water in spas
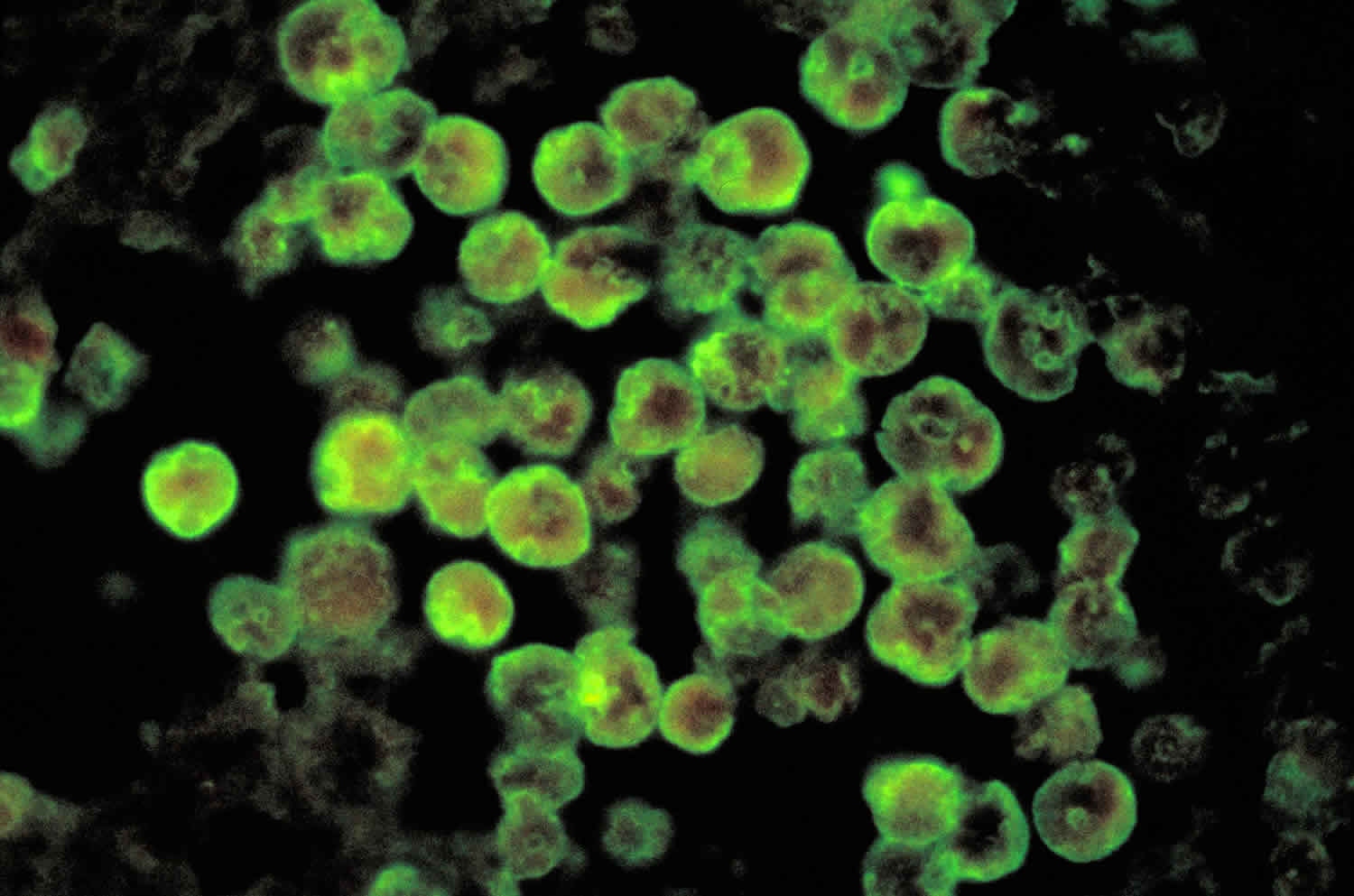
Figure 1. Naegleria Fowleri ameba
How does infection with Naegleria fowleri ameba occur?
Naegleria fowleri infects people when water containing the ameba enters the body through the nose. This typically occurs when people go swimming or diving in warm freshwater places, like lakes and rivers. The Naegleria fowleri ameba then travels up the nose to the brain where it destroys the brain tissue.
You cannot be infected with Naegleria fowleri by drinking contaminated water. In very rare instances, Naegleria infections may also occur when contaminated water from other sources (such as inadequately chlorinated swimming pool water or contaminated tap water) enters the nose, for example when people submerge their heads or cleanse their noses during religious practices, and when people irrigate their sinuses (nose) using contaminated tap water. Naegleria fowleri has not been shown to spread via water vapor or aerosol droplets (such as shower mist or vapor from a humidifier).
Where is Naegleria fowleri ameba found?
Naegleria fowleri is found around the world. In the United States, the majority of infections have been caused by Naegleria fowleri from freshwater located in southern-tier states. The ameba can be found in:
- Bodies of warm freshwater, such as lakes and rivers
- Geothermal (naturally hot) water, such as hot springs
- Warm water discharge from industrial plants
- Geothermal (naturally hot) drinking water sources
- Swimming pools that are poorly maintained, minimally-chlorinated, and/or un-chlorinated
- Water heaters. Naegleria fowleri grows best at higher temperatures up to 115°F (46°C) and can survive for short periods at higher temperatures.
- Soil
Naegleria fowleri is less likely to be found in the water as temperatures decline. The ameba can be found in lake or river sediment at temperatures well below where one would find the ameba in the water. Naegleria fowleri eats other organisms like bacteria found in the sediment in lakes and rivers.
Naegleria fowleri is not found in salt water, like the ocean 4.
Can I get a Naegleria fowleri infection from a disinfected swimming pool?
No. You cannot get a Naegleria fowleri infection from a properly cleaned, maintained, and disinfected swimming pool.
How common is Naegleria fowleri in the environment?
Naegleria fowleri is commonly found in lakes in southern-tier states during the summer but more recently has caused infections in northern states. This means that recreational water users should be aware that there will always be a low level risk of infection when entering these waters. In very rare instances, Naegleria has been identified in water from other sources such as inadequately chlorinated swimming pool water or heated and contaminated tap water. Naegleria fowleri grows best at higher temperatures up to 115°F (46°C) and can survive for short periods at higher temperatures.
How will the public know if a lake or other water body has Naegleria fowleri?
Recreational water users should assume that Naegleria fowleri is present in warm freshwater across the United States. Posting signs based on finding Naegleria fowleri in the water is unlikely to be an effective way to prevent infections. This is because:
- Naegleria fowleri occurrence is common, infections are rare.
- The relationship between finding Naegleria fowleri in the water and the occurrence of infections is unclear.
- The location and number of amebae in the water can vary over time within the same lake or river.
- There are no rapid, standardized testing methods to detect and quantitate Naegleria fowleri in water.
- Posting signs might create a misconception that bodies of water without signs or non-posted areas within a posted water body are Naegleria fowleri-free.
How common are Naegleria fowleri infections in the United States?
Naegleria fowleri infections are rare. In the 10 years from 2009 to 2018, 34 infections were reported in the U.S. Of those cases, 30 people were infected by recreational water, 3 people were infected after performing nasal irrigation using contaminated tap water, and 1 person was infected by contaminated tap water used on a backyard slip-n-slide.
Is there a routine and rapid test for Naegleria fowleri ameba in the water?
No. It can take weeks to identify the ameba, but new detection tests are under development. Previous water testing has shown that Naegleria fowleri is commonly found in freshwater venues. Therefore, recreational water users should assume that there is a low level of risk when entering all warm freshwater, particularly in southern-tier states.
When do Naegleria fowleri infections most commonly occur?
While infections with Naegleria fowleri are rare, they occur mainly during the summer months of July, August, and September. Infections are more likely to occur in southern-tier states, but can also occur in other more northern states. Infections usually occur when it is hot for prolonged periods of time, which results in higher water temperatures and lower water levels.
What swimming behaviors have been associated with Naegleria fowleri infection?
Behaviors associated with the infection include diving or jumping into the water, submerging the head under water or engaging in other water-related activities that cause water to go up the nose.
How can I reduce the risk of infection with Naegleria fowleri ameba?
Naegleria fowleri infects people when water containing the ameba enters the body through the nose. Infection is rare and typically occurs when people go swimming or diving in warm freshwater places, like lakes and rivers. Very rarely, infections have been reported when people submerge their heads or get water up their nose, cleanse their noses during religious practices, or irrigate their sinuses (nose) using contaminated tap or faucet water. Naegleria fowleri can grow in pipes, hot water heaters, and water systems, including treated public drinking water systems.
Personal actions to reduce the risk of Naegleria fowleri infection should focus on limiting the amount of water going up the nose and lowering the chances that Naegleria fowleri may be in the water.
The risk of Naegleria fowleri infection is very low. There have been 34 reported infections in the U.S. in the 10 years from 2009 to 2018, despite millions of recreational water exposures each year. By comparison, in the ten years from 2001 to 2010, there were more than 34,000 drowning deaths in the U.S.
Can Naegleria fowleri infection be spread from one person to another?
No. Naegleria fowleri infection cannot be spread from one person to another.
What is the cause of death from Naegleria fowleri infection?
The infection destroys brain tissue causing brain swelling and death.
What is the fatality rate for an infected person who begins to show signs and symptoms?
The fatality rate is over 97%. Only 4 people out of 145 known infected individuals in the United States from 1962 to 2018 have survived.
Is there effective treatment for Naegleria fowleri infection?
It is not clear. Several drugs are effective against Naegleria fowleri in the laboratory. However, their effectiveness is unclear since almost all infections have been fatal, even when people were treated with similar drug combinations. Recently, two people with Naegleria infection survived after being treated with a new drug called miltefosine that was given along with other drugs and aggressive management of brain swelling.
What should I do if I have been swimming or playing in freshwater and now think I have symptoms associated with Naegleria fowleri infection?
Infection with Naegleria fowleri is rare. The early symptoms of Naegleria fowleri infection are similar to those caused by other more common illnesses, such as bacterial meningitis. People should seek medical care immediately whenever they develop a sudden onset of fever, headache, stiff neck, and vomiting, particularly if they have been in warm freshwater recently.
Meningoencephalitis causes
Primary amebic meningoencephalitis, is a disease of the central nervous system 5. Primary amebic meningoencephalitis is caused by Naegleria fowleri, a free-living ameba. Humans become infected when water containing Naegleria fowleri enters the nose and the ameba migrates to the brain along the olfactory nerve 2. People do not become infected from drinking contaminated water. Symptoms start 1-9 days (median 5 days) after swimming or other nasal exposure to Naegleria-containing water. People die 1-18 days (median 5 days) after symptoms begin 6. primary amebic meningoencephalitis is difficult to detect because the disease progresses rapidly so that diagnosis is usually made after death 7.
Primary amebic meningoencephalitis is generally fatal 2; among well-documented cases, there are only five known survivors in North America: one from the U.S. in 1978 8, one from Mexico in 2003 9, two from the U.S. in 2013 10, and one from the U.S. in 2016. The original U.S. survivor’s condition gradually improved during a one-month hospitalization. The only reported side effect to treatment was a reduction in leg sensation for two months after discharge, which gradually improved. There was also no detection of Naegleria fowleri 3 days post-treatment 8. It has been suggested that the original survivor’s strain of Naegleria fowleri may have been less virulent, which contributed to the patient’s recovery. In laboratory experiments, the California survivor’s strain did not cause damage to cells as quickly as other strains, suggesting that it is less virulent than strains recovered from other fatal cases 11.
The Mexico survivor’s condition did not begin to improve until 40 hours after hospital admission. On day 22 of admission, there was no abnormality shown in the brain scan and the patient was discharged the next day. The patient was followed up for the next 12 months without any recurrence of disease 9.
After 35 years without a Naegleria survivor in the United States, during the summer of 2013, two children with Naegleria fowleri infection survived. The first, a 12-year-old girl, was diagnosed with primary amebic meningoencephalitis approximately 30 hours after becoming ill and was started on the recommended treatment within 36 hours. She also received the investigational drug miltefosine, and her brain swelling was aggressively managed with treatments that included therapeutic hypothermia (cooling the body below normal body temperature). This patient made a full neurologic recovery and returned to school. Her recovery has been attributed to early diagnosis and treatment and novel therapeutics including miltefosine and hypothermia 12.
The second, 8-year-old, child is also considered a primary amebic meningoencephalitis survivor, although he has suffered what is likely permanent brain damage. He was also treated with miltefosine but was diagnosed and treated several days after his symptoms began. Therapeutic hypothermia was not used in this case 10.
In the summer of 2016, a 16-year-old boy was reported as the 4th U.S. primary amebic meningoencephalitis survivor. This patient was diagnosed within hours of presentation to the hospital and was treated with the same protocol used for the 12-year-old 2013 survivor. This patient also made a full neurologic recovery and returned to school.
Overall, the outlook for people who get primary amebic meningoencephalitis is poor, although early diagnosis and new treatments might increase the chances for survival.
Risk of Infection
Naegleria fowleri is found naturally in freshwater lakes, rivers, and hot springs in the United States 5, particularly in southern-tier states 13, but has recently caused infections as far north as Minnesota 14. No data exist to accurately estimate the true risk of primary amebic meningoencephalitis. Hundreds of millions of visits to swimming venues occur each year in the U.S. that result in 0-8 infections per year 2. It is unknown why certain persons become infected with the amebae while millions of others exposed to warm recreational fresh waters do not, including those who were swimming with people who became infected. Attempts have been made to determine what concentration of Naegleria fowleri in the environment poses an unacceptable risk 15. However, no method currently exists that accurately and reproducibly measures the numbers of amebae in the water. This makes it unclear how a standard might be set to protect human health and how public health officials would measure and enforce such a standard. However, the risk of Naegleria fowleri infection is very low. There have been 34 reported infections in the U.S. in the 10 years from 2009 to 2018, despite hundreds of millions of recreational water exposures each year 16. By comparison, in the ten years from 2001 to 2010, there were more than 34,000 drowning deaths in the United States.
Naegleria fowleri life cycle
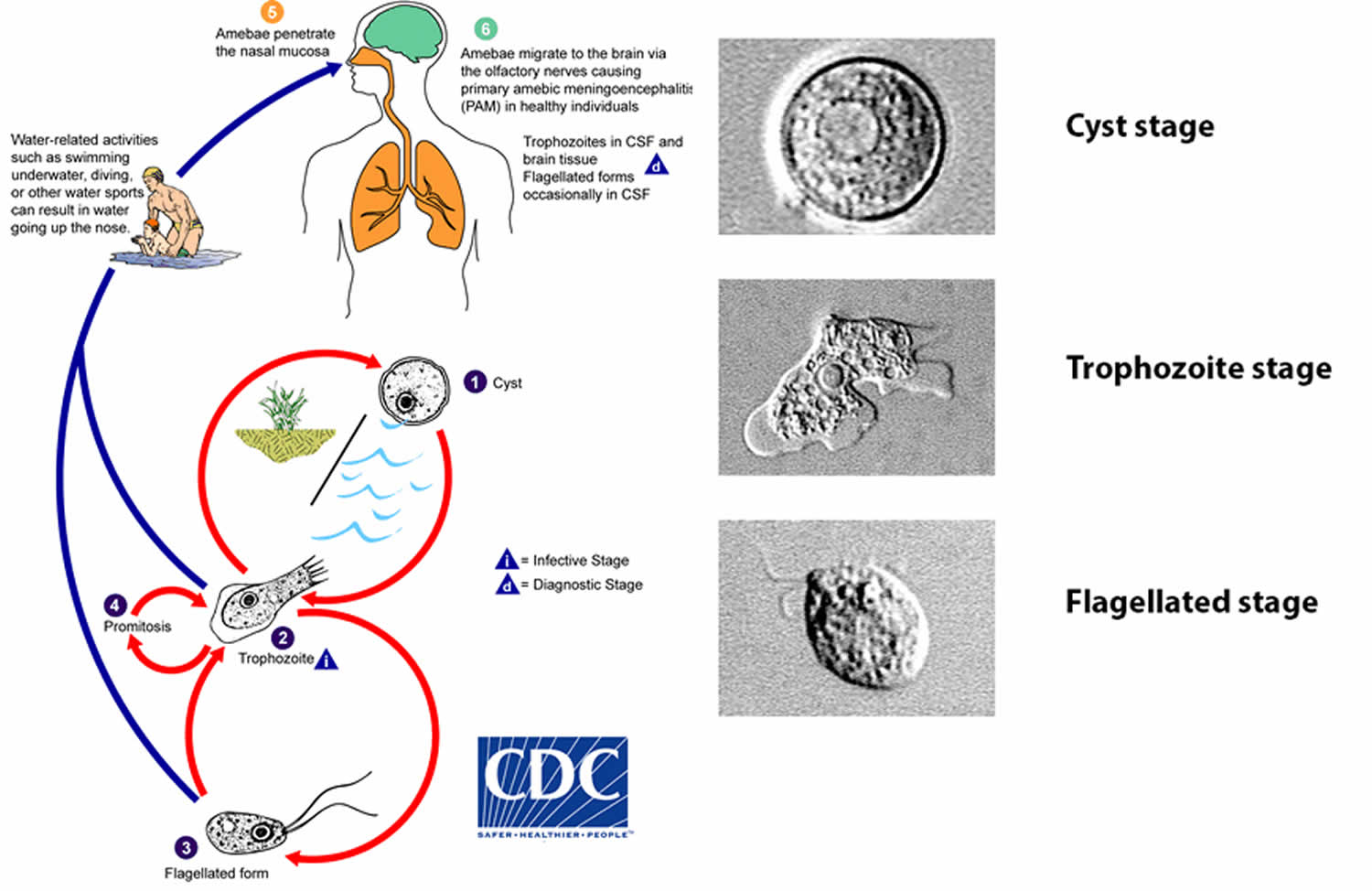
Naegleria fowleri has 3 stages in its life cycle: cyst (#1), trophozoite (#2), and flagellate (#3). The only infective stage of the ameba is the trophozoite. Trophozoites are 10-35 µm long with a granular appearance and a single nucleus. The trophozoites replicate by binary division during which the nuclear membrane remains intact (a process called promitosis) (#4). Trophozoites infect humans or animals by penetrating the nasal tissue (#5) and migrating to the brain (#6) via the olfactory nerves causing primary amebic meningoencephalitis (PAM).
Trophozoites can turn into a temporary, non-feeding, flagellated stage (10-16 µm in length) when stimulated by adverse environmental changes such as a reduced food source. They revert back to the trophozoite stage when favorable conditions return 17. Naegleria fowleri trophozoites are found in cerebrospinal fluid (CSF) and tissue, while flagellated forms are occasionally found in CSF. Cysts are not seen in brain tissue. If the environment is not conducive to continued feeding and growth (like cold temperatures, food becomes scarce) the ameba or flagellate will form a cyst. The cyst form is spherical and about 7-15 µm in diameter. It has a smooth, single-layered wall with a single nucleus. Cysts are environmentally resistant in order to increase the chances of survival until better environmental conditions occur 18.
Figure 2. Naegleria fowleri life cycle
Meningoencephalitis symptoms
Naegleria fowleri causes the disease primary amebic meningoencephalitis (PAM), a brain infection that leads to the destruction of brain tissue. In its early stages, signs and symptoms of Naegleria fowleri infection are clinically similar to bacterial meningitis, which lowers the chances of initially diagnosing primary amebic meningoencephalitis 3.
Initial symptoms of primary amebic meningoencephalitis start about 5 days (range 1 to 9 days) after infection. The initial symptoms may include headache, fever, nausea, or vomiting. Later symptoms can include stiff neck, confusion, lack of attention to people and surroundings, loss of balance, seizures, and hallucinations. After the start of symptoms, the disease progresses rapidly and usually causes death within about 5 days (range 1 to 12 days).
Symptoms of primary amebic meningoencephalitis infection includes:
- high fever
- severe and persistent headache
- stiff neck
- confusion or hallucinations
- sleepiness
- sore throat
- nausea and vomiting
- disturbances of taste and smell
- seizures (fits)
Stage 1
- Severe frontal headache
- Fever
- Nausea
- Vomiting
Stage 2
- Stiff neck
- Seizures
- Altered mental status
- Hallucinations
- Coma
These symptoms are common for many other conditions, including viral and bacterial forms of meningitis. It’s important to urgently see a doctor for diagnosis.
While primary amebic meningoencephalitis infection can occur at any age, children and young adults seem more susceptible to the disease.
Meningoencephalitis diagnosis
Primary amebic meningoencephalitis is diagnosed using specific laboratory tests available in only a few laboratories in the United States. Because of the rarity of the infection and difficulty in initial detection, about 75% of diagnoses are made after the death of the patient. For 24/7 diagnostic assistance, specimen collection guidance, shipping instructions, and treatment recommendations, please contact the CDC Emergency Operations Center at 770-488-7100.
Primary amebic meningoencephalitis and Naegleria fowleri infection can be diagnosed in the laboratory by detecting 19:
- Naegleria fowleri organisms in cerebrospinal fluid (CSF), biopsy, or tissue specimens, or
- Naegleria fowleri nucleic acid in CSF, biopsy, or tissue specimens, or
- Naegleria fowleri antigen in CSF, biopsy, or tissue specimens.
Direct visualization
The motile amebae can often be seen moving rapidly under a microscope when looking at a fresh sample of CSF. The amebae can also be stained with a variety of stains, such as Giemsa-Wright or a modified trichrome stain, for identification 20.
Antigen detection
A specific antibody to Naegleria fowleri can be used in conjunction with another antibody that deposits a chemical (immunohistochemistry) or glows under specific types of light (indirect immunofluorescence) to directly stain the amebic antigens in tissue 20.
Polymerase chain reaction (PCR)
Specific molecular tools can amplify DNA from the amebae in CSF or tissue to specifically identify if the amebae are present. Looking at strains or subtypes of Naegleria fowleri can be done, but little is known about the natural populations in the environment, which makes it difficult to interpret what the findings mean 21.
Ameba culture
The amebae can be grown in culture to increase the likelihood of detecting the ameba by direct visualization or PCR 22. The sample is added to a growth plate covered in bacteria that can serve as a food source for Naegleria fowleri. The initial screening is accomplished by incubating the plate at a higher temperature (108°F/42°C) that kills most free-living amebae, while selecting for heat-loving (thermophilic) amebae, such as Naegleria fowleri or other amebae. This initial screen shows up as tracks made by an ameba as it moves across the plate eating the bacteria. If there are no amebae on the plate grown at the higher temperature, then Naegleria fowleri is not present. If heat-loving (thermophilic) amebae are present on the plate grown at the higher temperature, then these amebae undergo further specific testing to determine whether Naegleria fowleri is present since other free-living amebae can also be heat-loving (thermophilic).
NOTE: Amebae 23, including thermophilic amebae 5 other than Naegleria fowleri, can be common in water systems but none of these other amebae cause primary amebic meningoencephalitis.
Meningoencephalitis treatment
Recently an investigational breast cancer and anti-leishmania drug, miltefosine 24, has shown some promise in combination with some of these other drugs. Miltefosine has shown ameba-killing activity against free-living amebae, including Naegleria fowleri, in the laboratory 25. Miltefosine has also been used to successfully treat patients infected with Balamuthia 26 and disseminated Acanthamoeba infection 27. If you are a clinician and have a patient with suspected Naegleria or other free-living ameba infection, please contact the CDC Emergency Operations Center at 1-770-488-7100 to consult with a CDC expert regarding the use of this drug.
After 35 years without a Naegleria survivor in the United States, during the summer of 2013, two children with Naegleria fowleri infection survived. The first, a 12-year-old girl, was diagnosed with primary amebic meningoencephalitis approximately 30 hours after becoming ill and was started on the recommended treatment within 36 hours. She also received the investigational drug miltefosine 28 and her brain swelling was aggressively managed with treatments that included cooling the body below normal body temperature (therapeutic hypothermia). This patient made a full neurologic recovery and returned to school. Her recovery has been attributed to early diagnosis and treatment and novel therapeutics including miltefosine and hypothermia 29.
The second child, an 8-year-old male, is also considered a primary amebic meningoencephalitis survivor, although he has suffered what is likely to be permanent brain damage. He was also treated with miltefosine but was diagnosed and treated several days after his symptoms began. Cooling of the body below normal body temperature was not used 30.
In the summer of 2016, a 16-year-old boy was reported as the 4th U.S. primary amebic meningoencephalitis survivor. This patient was diagnosed within hours of presentation to the hospital and was treated with the same protocol used for the 12-year-old 2013 survivor. This patient also made a full neurologic recovery and returned to school.
- Notes from the Field: Primary Amebic Meningoencephalitis Associated with Ritual Nasal Rinsing — St. Thomas, U.S. Virgin Islands, 2012[↩]
- Yoder JS, Eddy BA, Visvesvara GS, Capewell L, Beach MJ. The epidemiology of primary amoebic meningoencephalitis in the USA, 1962-2008. Epidemiol Infect. 2010;138:968-75.[↩][↩][↩][↩]
- Capewell LG, Harris AM, Yoder JS, Cope JR, Eddy BA, Roy SL, Visvesvara GS, Fox LM, Beach MJ. Diagnosis, clinical course, and treatment of primary amoebic meningoencephalitis in the United States, 1937–2013. J Pediatric Infect Dis Soc. 2014;Epub: 1–8[↩][↩]
- Tiewcharoen S, Junnu V. Factors affecting the viability of pathogenic Naegleria species isolated from Thai patients. J Trop Med Parasitol. 1999;22:15-21.[↩]
- Visvesvara GS. Free-living amebae as opportunistic agents of human disease. J Neuroparasitol. 2010;1.[↩][↩]
- Capewell LG, Harris AM, Yoder JS, Cope JR, Eddy BA, Roy SL, Visvesvara GS, Fox LM, Beach MJ. Diagnosis, clinical course, and treatment of primary amoebic meningoencephalitis in the United States, 1937–2013. J Pediatric Infect Dis Soc. 2014;Epub: 1–8.[↩]
- Marciano-Cabral F, Cabral G. The immune response to Naegleria fowleri amebae and pathogenesis of infection. FEMS Immunol Med Microbiol. 2007;51:243-59.[↩]
- Seidel J, Harmatz P, Visvesvara GS, Cohen A, Edwards J, Turner J. Successful treatment of primary amebic meningoencephalitis. New Engl J Med. 1982;306:346-8[↩][↩]
- Vargas-Zepeda J, Gomez-Alcala AV, Vasquez-Morales JA, Licea-Amaya L, De Jonckheere JF, Lores-Villa F. Successful treatment of Naegleria PAM using IV amphotericin B, fluconazole, and rifampin. Arch Med Res. 2005;36:83-6[↩][↩]
- Cope JR, Conrad DA, Cohen N, Cotilla M, DaSilva A, Jackson J, Visvesvara GS. Use of the novel therapeutic agent miltefosine for the treatment of primary amebic meningoencephalitis: report of 1 fatal and 1 surviving case. Clin Infect Dis. 2016;62(6):774-6.[↩][↩]
- John DT, John RA. Cytopathogenicity of Naegleria fowleri in mammalian cell cultures. Parasitol Res. 1989;76:20-5.[↩]
- Linam WM, Ahmed M, Cope JR, Chu C, Visvesvara GS, da Silva AJ, Qvarnstrom Y, Green J. Successful treatment of an adolescent with Naegleria fowleri primary amebic meningoencephalitis. Pediatrics. 2015;135:e744-748.[↩]
- Maclean RC, Richardson DJ, LePardo R, Marciano-Cabral F. The identification of Naegleria fowleri from water and soil samples by nested PCR. Parasitol Res. 2004;93: 211–17.[↩]
- Kemble SK, Lynfield R, DeVries AS, Drehner DM, Pomputius WF 3rd, Beach MJ, Visvesvara GS, da Silva AJ, Hill VR, Yoder JS, Xiao L, Smith KE, Danila R. Fatal Naegleria fowleri infection acquired in Minnesota: possible expanded range of a deadly thermophilic organism. Clin Infect Dis. 2012;54:805-9.[↩]
- Cabanes PA, Wallet F, Pringuez E, Pernin P. Assessing the risk of primary amoebic meningoencephalitis from swimming in the presence of environmental Naegleria fowleri. Appl Environ Microbiol. 2001;67:2927-31.[↩]
- US Census Bureau. Statistical Abstract of the United States: 2012. Arts, Recreation, and Travel: Participation in Selected Sports Activities 2009[↩]
- Visvesvara G, Yoder J, Beach MJ. Primary amebic meningoencephalitis Chapter 73. 2012. p. 442-7. In: Netter’s Infectious Diseases, Eds. Yong EC, Stevens DL. Elsevier Saunders. Philadelphia, PA.[↩]
- Visvesvara GS, Moura H, Schuster FL. Pathogenic and opportunistic free-living amoebae: Acanthamoeba spp., Balamuthia mandrillaris, Naegleria fowleri, and Sappinia diploidea. FEMS Immunol Med Microbiol. 2007;50(1):1-26.[↩]
- Council for State and Territorial Epidemiologists (CSTE). Case definitions for non-notifiable infections caused by free-living amebae (Naegleria fowleri, Balamuthia mandrillaris, and Acanthamoeba spp.). Infectious Disease Committee. 2012. https://c.ymcdn.com/sites/www.cste.org/resource/resmgr/PS/11-ID-15.pdf[↩]
- Visvesvara GS. Amebic meningoencephalitides and keratitis: challenges in diagnosis and treatment. Curr Opin Infect Dis. 2010;23(6):590-4.[↩][↩]
- Qvarnstrom Y, Visvesvara GS, Sriram R, da Silva AJ. Multiplex real-time PCR assay for simultaneous detection of Acanthamoeba spp., Balamuthia mandrillaris, and Naegleria fowleri. J Clin Microbiol. 2006;44(10):3589-95.[↩]
- Visvesvara GS. Parasite Culture: Acanthamoeba and Naegleria spp. In: Garcia LS, editor. Clinical Microbiology Procedures Handbook. 3rd ed. Washington, DC: ASM Press; 2010.[↩]
- Stockman LJ, Wright CJ, Visvesvara GS, Fields BS, Beach MJ. Prevalence of Acanthamoeba spp. and other free-living amoebae in household water, Ohio, USA–1990-1992. Parasitol Res. 2011;108(3):621-7.[↩]
- Kaminsky R. Miltefosine Zentaris. Curr Opin Investig Drugs. 2002;3(4):550-4[↩]
- Kim JH, Jung SY, Lee YJ, Song KJ, Kwon D, Kim K, Park S, Im KI, Shin HJ. Effect of therapeutic chemical agents in vitro and on experimental meningoencephalitis due to Naegleria fowleri. Antimicrob Agents Chemother. 2008;52:4010-16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2573150/pdf/0197-08.pdf[↩]
- Martínez DY, Seas C, Bravo F, Legua P, Ramos C, Cabello AM, Gotuzzo E. Successful treatment of Balamuthia mandrillaris amoebic infection with extensive neurological and cutaneous involvement. Clin Infect Dis. 2010;51:e7-11[↩]
- Aichelburg AC, Walochnik J, Assadian O, Prosch H, Steuer A, Perneczky G, Visvesvara GS, Aspöck H, Vetter N. Successful treatment of disseminated Acanthamoeba sp. infection with miltefosine.pdf icon. Emerg Infect Dis. 2008;14(11):1743-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2630722/pdf/07-0854_finalD.pdf[↩]
- Schuster FL, Guglielmo BJ, Visvesvara GS. In-vitro activity of miltefosine and voriconazole on clinical isolates of free-living amebas: Balamuthia mandrillaris, Acanthamoeba spp., and Naegleria fowleri. J Eukaryot Microbiol. 2006;53(2):121-6.[↩]
- Linam WM, Ahmed M, Cope JR, Chu C, Visvesvara GS, da Silva AJ, Qvarnstrom Y, Green J. Successful treatment of an adolescent with Naegleria fowleri primary amebic meningoencephalitis. Pediatrics. 2015;135:e744[↩]
- Cope JR, Conrad DA, Cohen N, Cotilla M, DaSilva A, Jackson J, Visvesvara GS. Use of the novel therapeutic agent miltefosine for the treatment of primary amebic meningoencephalitis: report of 1 fatal and 1 surviving case. Clin Infect Dis 2016;62(6):774-6[↩]





{kind=link}