Contents
What is Mirizzi syndrome
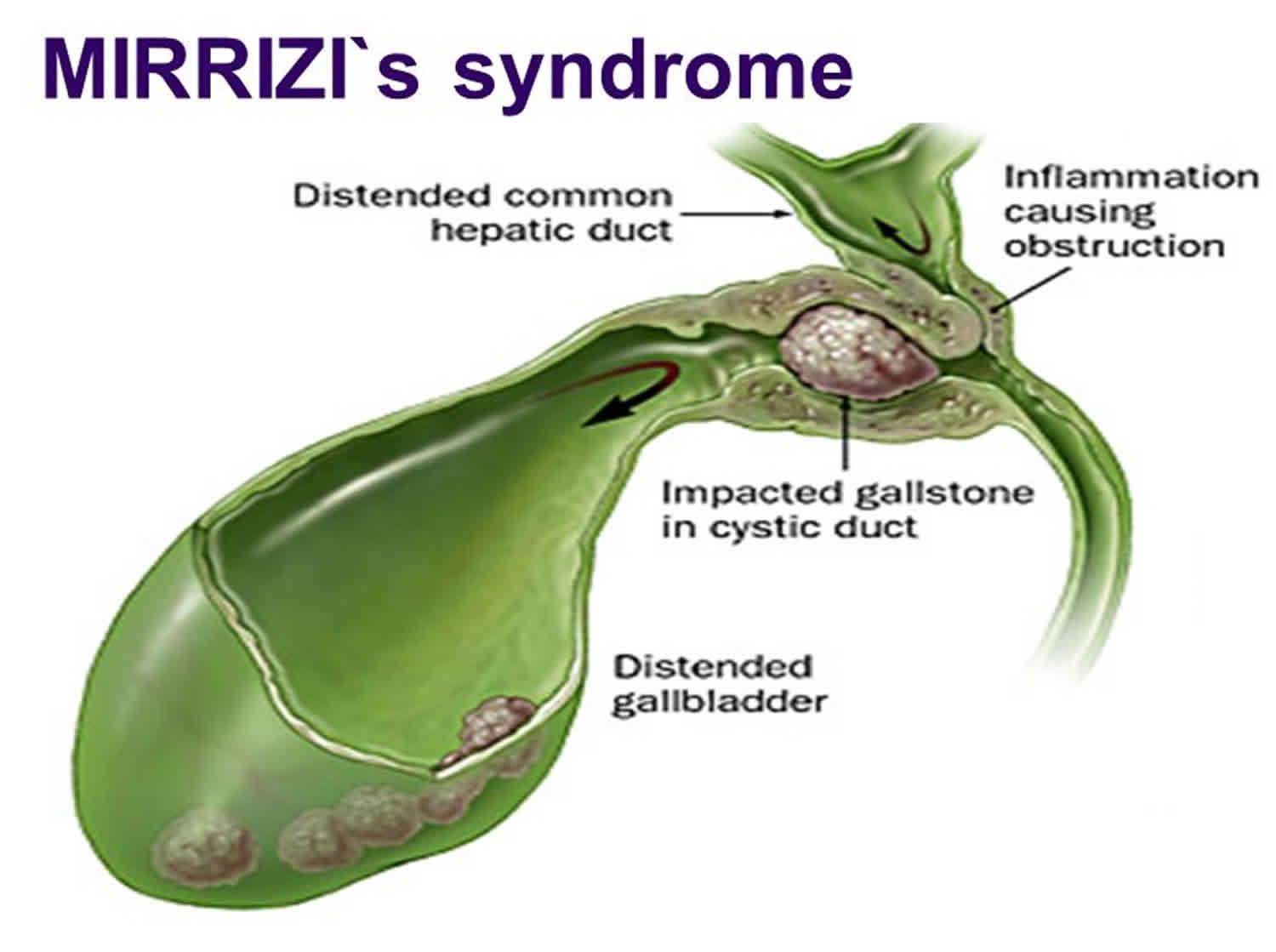
Mirizzi syndrome is a rare condition caused by the obstruction of the common bile duct or common hepatic duct by external compression from multiple impacted gallstones or a single large impacted gallstone in Hartman’s pouch 1, 2, 3, 4. There is an increased risk of developing gallbladder cancer with Mirizzi’s syndrome 5. 5% to 28% of patients with Mirizzi syndrome were found to have gallbladder cancer after cholecystectomy. Virtually all diagnoses were made postoperatively with pathologic examination of the specimens 6. Mirizzi syndrome clinical presentation varies from no symptoms to severe cholangitis 7. Mirizzi syndrome presenting symptoms are similar to cholecystitis but may be confused with other obstructing conditions such as common bile duct stones and ascending cholangitis due to the presence of recurrent episodes of jaundice and cholangitis. Mirizzi syndrome can be associated with acute cholecystitis. Fistulae can develop between the gallbladder and the common duct, and the stone may pass into the common duct 8. Generally, distinguishing between Mirizzi syndrome and other causes of obstructive jaundice is not possible with physical examination alone 9. Preoperative diagnosis of Mirizzi syndrome is often difficult and usually missed 5. Mirizzi syndrome is named after the Argentinean surgeon Pablo Luis Mirizzi. His most well-known contribution to surgery is having performed the first intraoperative cholangiogram in 1931. The first published paper describing Mirizzi syndrome which bears his name today was in 1940 10.
Mirizzi syndrome is characterized by increased occurrence of complications compared with routine surgery for cholecystolithiasis 11. Bile duct reconstruction becomes more difficult with increases in the size of the cholecystocholedochal fistula. In some cases, difficulty performing bile duct reconstruction makes it necessary to perform complex surgical procedures, such as bile duct resection and choledochojejunostomy by the Roux-en-Y method 12.
Mirizzi syndrome is relatively uncommon. Only 0.1% of patients with gallstones will develop Mirizzi syndrome and it has been found in 0.7% to 25% of patients who have undergone cholecystectomies 5. There may be an increased in occurrence in the older populations, but there has not been a predilection for either male or female patients who have gallstones. There also appears to be no prevalence for any particular ethnic population 13.
Surgical management is the mainstay treatment for Mirizzi Syndrome, although this is challenging for several reasons. First, there is a low index of suspicion for this condition among surgeons, largely owing to its rarity, as gallbladder surgery is often performed in patients with relatively shorter histories of illness, long before the onset of Mirizzi Syndrome 14. Secondly, preoperative diagnosis is often missed, thus impacting upon the ability to treat this condition during surgery. Thirdly, distortion of the anatomy by dense adhesions due to longstanding inflammation and the advancement of cholecystobiliary or cholecysto-enteric fistula, increases the risk of bile duct injury or massive bleeding during dissection of Calot’s triangle 15. Furthermore, inflammation can cause cutaneous fistula, secondary biliary cirrhosis, delayed onset biliary strictures, and even death.
Mirizzi syndrome types
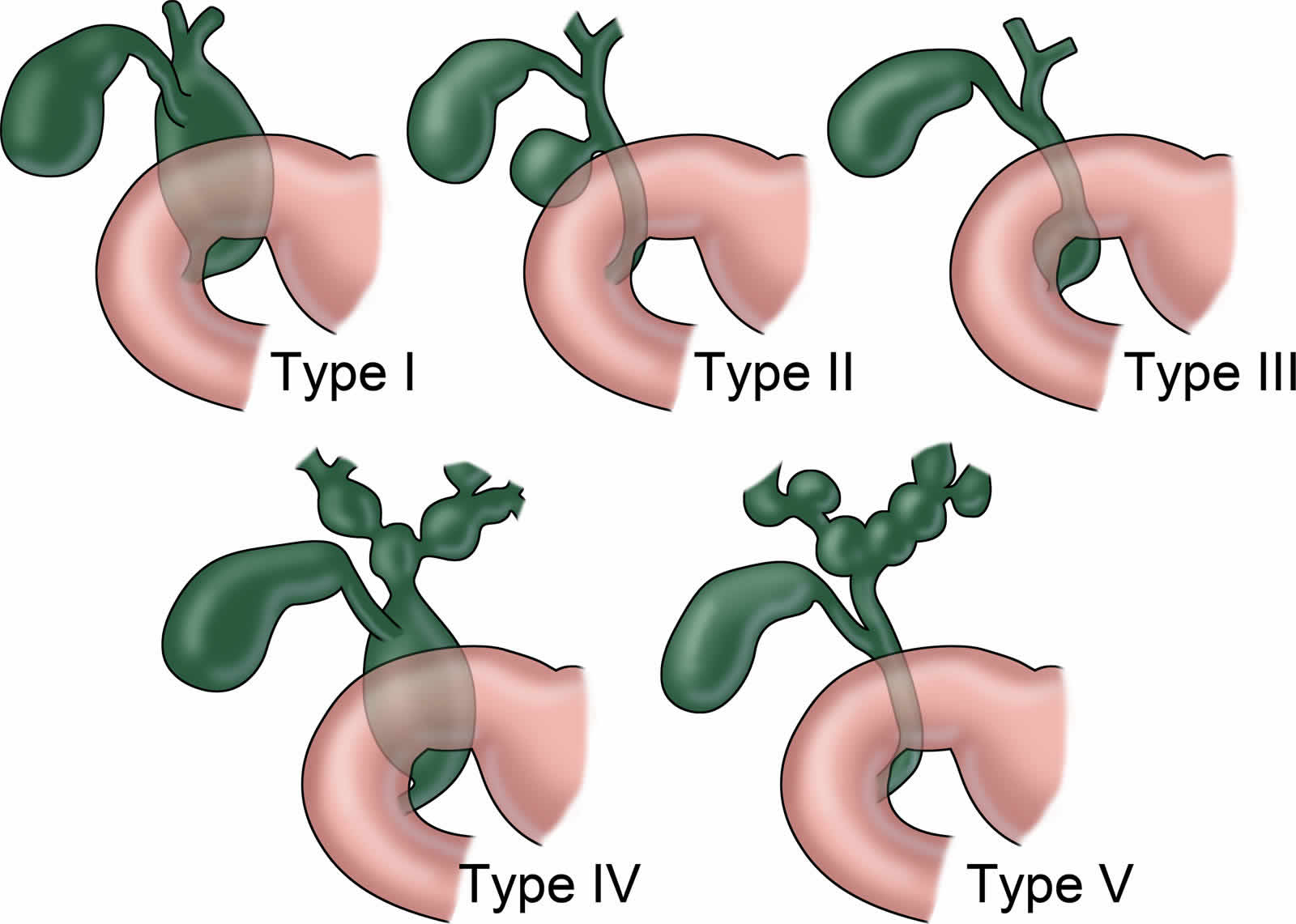
A grading system has been developed to categorize the various stages of Mirizzi syndrome. The Csendes system recognizes 5 major types of Mirizzi syndrome: type 1 is characterized by “classic” compression stenosis; types 2 to 4 involve formation of a cholecystocholedochal fistula; and type 5 is defined by the formation of a cholecystoenteric fistula in addition to the presence of types 1 to 4.
Mirizzi type 1 (10.5–51%) and Mirizzi type 2 (57%) are the most commonly reported types 7. Other types of Mirizzi syndrome are relatively low in incidence.
Type 1 Mirizzi syndrome – No Fistula Present
- Type 1A: Presence of the cystic duct
- Type 1B: Obliteration of the cystic duct
Types 2 to 5 Mirizzi syndrome – Fistula Present
- Type 2: Defect smaller than 33% of the common bile duct diameter
- Type 2A: Cholecystobiliary fistula and the diameter <50% of common bile duct
- Type 2B: Cholecystobiliary fistula and the diameter >50% of common bile duct
- Type 3: Defect 33% to 66% of the common bile duct diameter
- Type 3A: Cholecystobiliary fistula and cholecystoenteric fistula without gallstone ileus
- Type 3B: Cholecystobiliary fistula and cholecystoenteric fistula with gallstone ileus
- Type 4: Defect larger than 66% of the common hepatic duct diameter with complete destruction of the common bile duct wall 16
- Type 5: Types 1 to 4 with cholecystoenteric fistula.
- Type 5A: Cholecystoenteric fistula without gallstone ileus
- Type 5B: Cholecystoenteric fistula with gallstone ileus
Table 1. Csendes Classification of Mirizzi Syndrome
| Type | Description |
|---|---|
| Type 1 | External compression on common biliary duct (CBD) |
| Type 2 | Cholecystocholedochal fistula affecting less than one third of the common biliary duct |
| Type 3 | Cholecystocholedochal fistula affecting up to two thirds of the common biliary duct |
| Type 4 | Cholecystocholedochal fistula with complete destruction of common biliary duct wall |
| Type 5 | Types 1-4 with cholecystoenteric fistula |
Figure 1. Mirizzi syndrome types
Mirizzi syndrome causes
The exact cause of Mirizzi syndrome is unclear but is felt to be due to persistent and recurrent irritation of the area and chronic biliary stasis. Gallstones are usually formed from bile that is in stasis. When bile is not fully emptied from the gallbladder, bile becomes concentrated in the gallbladder, it becomes supersaturated, which in time precipitate into small crystals. These crystals, in turn, become stuck in the gallbladder mucus, resulting in gallbladder sludge. Over time, these crystals grow and form large and/or multiple gallstones. These gallstones may cause symptoms of cholecystitis (gallbladder inflammation), but if they become embedded in a floppy Hartman’s pouch, they can cause additional findings of jaundice. As this condition progresses, internal fistulas from the gallbladder into the common bile duct, common hepatic duct and the duodenum can develop. Biliary obstruction may also lead to gallstones including bile duct strictures and cancers, such as pancreatic cancer. The most common cause of cholelithiasis (gallstone formation) is from the precipitation of cholesterol that subsequently forms into cholesterol stones. The second form of gallstones is pigmented gallstones which are the result of increased red blood cell destruction in the intravascular system causing increased concentrations of bilirubin which subsequently get stored in the bile. These stones are typically black. The third type of gallstones is mixed pigmented stones which are a combination of calcium substrates such as calcium carbonate or calcium phosphate, cholesterol and bile. The fourth type is made up primarily of calcium and usually found in patients with hypercalcemia. When multiple gallstones or a singular large gallstone get impacted in Hartman’s pouch (the lower outpouching of the gallbladder), external compression of the common bile duct or the common hepatic duct can occur. The exact mechanism as to why this occurs is unknown, but it is felt to be related to a floppy Hartman’s pouch containing a higher mass of stones such as with multiple stones or a single large impacted stone. This causes subsequent inflammation of the are which can also lead to fistula formation over time 17.
Mirizzi syndrome symptoms
The clinical presentation of Mirizzi Syndrome ranges from asymptomatic to non-specific, with obstructive jaundice (27.8–100%) being the most common, elevated liver enzymes (AST/ALT), right upper quadrant abdominal pain (16.7–100%), and constitutional symptoms such as fever, nausea, vomiting, diarrhea, and constipation 18. Although rare, Mirizzi Syndrome may also present with gallstone ileus 19. The nature of these presentations often leads to this condition being confused with biliary tract neoplasm 20 and misdiagnosis is therefore common.
Patients with Mirizzi syndrome may present with acute or chronic cholecystitis with the addition of jaundice. Patients with chronic cholecystitis usually present with dull right upper abdominal pain that radiates to the mid back or right scapular tip. It is usually associated with fatty food ingestion. Nausea and occasional vomiting also accompany complaints of increased bloating and flatulence. Often the symptoms occur in the evening. Prolonged less acute symptoms are usually present over weeks or months. Increased frequency and severeness of acute exacerbations (acute biliary colic) is usually seen in the presence of more prolonged chronic symptoms. The classic physical examination will demonstrate right upper abdominal pain with deep palpation (Murphy’s sign). Patients are usually not acutely ill but are uncomfortable. Patients with advanced Mirizzi syndrome or of more severe acute cholecystitis may present with more pronounced symptoms and findings. Jaundice is usually present, and at times, significantly elevated bilirubin can be identified 21.
Mirizzi syndrome complications
The most common complication of Mirizzi syndrome is cholecystobiliary or cholecysto-enteric fistula formation due to prolonged inflammation 1. Surgical complications with prolonged procedure time due to dense adhesions may also occur. These include bile duct injury and hemorrhage. Massive hemorrhage during dissection of the Calot triangle can occur in complex cases. Other complications of prolonged inflammation that can be seen in patients with Mirizzi syndrome include:
- Cutaneous fistula formation
- Secondary biliary cirrhosis
- Delayed onset biliary strictures 15
Mirizzi syndrome diagnosis
The routine workup for cholecystitis should be initiated. The best test for diagnosing gallstones and subsequent acute cholecystitis is a right upper quadrant abdominal ultrasound. It is associated with a 90% specificity rate and depending on ultrasound operator, can detect stones as small as 2 mm as well as sludge and gallbladder polyps. Ultrasound findings that point toward acute cholecystitis versus cholelithiasis include gallbladder wall thickening (greater than 3 mm), pericholecystic fluid and a positive sonographic Murphy’s sign. Gallstones can also often be found on CT scans, and MRIs, however, these studies are not as sensitive for acute cholecystitis. Approximately 10% of gallstones may be found on routine plain films due to their high calcium content. Air in the biliary tree may also be detected on these radiographic studies if there is an enteric fistula present. If there is a suspected stone in the common bile duct based on ultrasound results, magnetic resonance cholangiopancreatography (MRCP) is the next step. If a common duct stone is identified on the magnetic resonance cholangiopancreatography (MRCP), then the gold-standard test of an endoscopic retrograde cholangiopancreatogram (ERCP) should be performed by a gastroenterologist. A percutaneous transhepatic cholangiogram (PTHC) is also useful in diagnosing common bile duct stones if an endoscopic retrograde cholangiopancreatogram (ERCP) is not possible. Usually, the diagnosis of Mirizzi syndrome is either mistaken for a simple common bile duct stone or is missed entirely on preoperative workup 22.
Mirizzi syndrome treatment
The treatment for Mirizzi syndrome is cholecystectomy. Laparoscopic cholecystectomy is preferable, but if the condition is advanced, then a more involved surgery may be needed. An open cholecystectomy is an option. In cases of a more progressed disease, a partial cholecystectomy can be considered. This would involve leaving Hartman’s pouch in place and removing the body of the gallbladder and the gallstones. This will lower the incidence of injury to the porta hepatis and bile ducts. If a fistula is present then an open cholecystectomy with bilioenteric anastomosis possibly with a Roux-en-Y has been shown to be effective 23.
Mirizzi syndrome prognosis
Delay in making an adequate diagnosis and treatment could lead to the progression of Mirizzi syndrome. Inflammation can cause cutaneous fistula, secondary biliary cirrhosis, delayed onset biliary strictures, and even death. 5% to 28% of patients with Mirizzi syndrome were found to have gallbladder cancer after cholecystectomy. Gallbladder cancer is thought to be due to prolonged inflammation leading to both diseases, rather than a result of Mirizzi syndrome itself 24. The prognosis for patients with fistula formation involves prolonged treatment with T-tube placement through the small-moderate sized fistula or biliary diversion with a choledochoduodenostomy or a Roux-en-Y choledochojejunostomy for larger fistulas 1. A prolonged surgical and hospital course for patients with fistula formation increases their risk of complications and increases their morbidity and mortality rate. In elderly patients with multiple comorbidities and a high risk of surgical complications, nonoperative methods should be considered to minimize morbidity associated with the surgery 25.
In patients without fistula formation, the surgical repair and outcome are usually favorable 1. Due to the distorted anatomy and high rate of conversion to open cholecystectomy for Mirizzi syndrome; however, some sources recommend an open surgical approach for all patients affected by Mirizzi syndrome.
- Jones MW, Ferguson T. Mirizzi Syndrome. [Updated 2023 Apr 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482491[↩][↩][↩][↩]
- Mirizzi PL. Síndrome del conducto hepático. J Int Chir. 1948;8:731–777.[↩]
- Csendes A, Díaz JC, Burdiles P, Maluenda F, Nava O. Mirizzi syndrome and cholecystobiliary fistula: a unifying classification. Br J Surg. 1989 Nov;76(11):1139-43. doi: 10.1002/bjs.1800761110[↩]
- Schäfer M, Schneiter R, Krähenbühl L. Incidence and management of Mirizzi syndrome during laparoscopic cholecystectomy. Surg Endosc. 2003 Aug;17(8):1186-90; discussion 1191-2. doi: 10.1007/s00464-002-8865-z[↩]
- Jones MW, Ferguson T. Mirizzi Syndrome. [Updated 2019 Feb 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482491[↩][↩][↩]
- Kuga D, Ebata T, Yokoyama Y, Igami T, Sugawara G, Mizuno T, Yamaguchi J, Nagino M. Long-term survival after multidisciplinary therapy for residual gallbladder cancer with peritoneal dissemination: a case report. Surg Case Rep. 2017 Dec;3(1):76.[↩]
- Kumar A, Senthil G, Prakash A, Behari A, Singh RK, Kapoor VK, et al. Mirizzi’s syndrome: lessons learnt from 169 patients at a single center. Korean J Hepatobiliary Pancreat Surg. 2016 Feb. 20 (1):17-22.[↩][↩]
- Aldekhayel M, Almohaimeed K, AlShahrani MS, Almweisheer S. Rare case of Mirizzi syndrome associated with cholecystogastric fistula. BMJ Case Rep. 2016 Jan 11. 2016[↩]
- Menias CO, Surabhi VR, Prasad SR, Wang HL, Narra VR, Chintapalli KN. Mimics of cholangiocarcinoma: spectrum of disease. Radiographics. 2008 Jul-Aug. 28(4):1115-29.[↩]
- Bellamlih H, Bouimetarhan L, En-Nouali H, Amil T, Chouaib N, Jidane S, Rafai M, Belkouch A, Belyamani L. [Mirizzi’s syndrome: a rare cause of biliary tract obstruction: about a case and review of the literature]. Pan Afr Med J. 2017;27:45[↩]
- Mirizzi Syndrome Imaging. https://emedicine.medscape.com/article/370808-overview[↩]
- Zhong H, Gong JP. Mirizzi syndrome: experience in diagnosis and treatment of 25 cases. Am Surg. 2012 Jan. 78(1):61-5.[↩]
- Clemente G, Tringali A, De Rose AM, Panettieri E, Murazio M, Nuzzo G, Giuliante F. Mirizzi Syndrome: Diagnosis and Management of a Challenging Biliary Disease. Can J Gastroenterol Hepatol. 2018;2018:6962090[↩]
- A Minimally Invasive Strategy for Mirizzi Syndrome Type II: Combined Endoscopic With Laparoscopic Approach. Yuan H, Yuan T, Sun X, Zheng M. Surg Laparosc Endosc Percutan Tech. 2016 Jun; 26(3):248-52.[↩]
- Chen H, Siwo EA, Khu M, Tian Y. Current trends in the management of Mirizzi Syndrome: A review of literature. Medicine (Baltimore). 2018 Jan;97(4):e9691. doi: 10.1097/MD.0000000000009691[↩][↩]
- Zhou J, Xiao R, Yang JR, Wang L, Wang JX, Zhang Q, Ren JJ. Mirizzi syndrome complicated by common hepatic duct fistula and left hepatic atrophy: a case report. J Int Med Res. 2018 Nov;46(11):4806-4812. doi: 10.1177/0300060518797246[↩]
- Falk V, Low G, Bigam D, Sandha G. Acute acalculous cholecystitis of an intrahepatic gallbladder causing Mirizzi’s syndrome. BMJ Case Rep. 2018 Apr 13[↩]
- Chen H, Siwo EA, Khu M, Tian Y. Current trends in the management of Mirizzi Syndrome: A review of literature. Medicine (Baltimore). 2018 Jan;97(4):e9691. doi: 10.1097/MD.0000000000009691 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5794376[↩]
- Laparoscopic treatment of Mirizzi syndrome: a systematic review. Antoniou SA, Antoniou GA, Makridis C. Surg Endosc. 2010 Jan; 24(1):33-9.[↩]
- Complications of gallstone disease: Mirizzi syndrome, cholecystocholedochal fistula, and gallstone ileus. Abou-Saif A, Al-Kawas FH. Am J Gastroenterol. 2002 Feb; 97(2):249-54.[↩]
- Pak S, Valencia D, Sheehy B, Agbim U, Askaroglu Y, Dee C. Ticking Bomb: Asymptomatic Mirizzi Syndrome. Cureus. 2017 Nov 16;9(11):e1854[↩]
- Shirah BH, Shirah HA, Albeladi KB. Mirizzi syndrome: necessity for safe approach in dealing with diagnostic and treatment challenges. Ann Hepatobiliary Pancreat Surg. 2017 Aug;21(3):122-130[↩]
- Kulkarni SS, Hotta M, Sher L, Selby RR, Parekh D, Buxbaum J, Stapfer M. Complicated gallstone disease: diagnosis and management of Mirizzi syndrome. Surg Endosc. 2017 May;31(5):2215-2222.[↩]
- Prasad TL, Kumar A, Sikora SS, Saxena R, Kapoor VK. Mirizzi syndrome and gallbladder cancer. J Hepatobiliary Pancreat Surg. 2006;13(4):323-6. doi: 10.1007/s00534-005-1072-2[↩]
- Chai LF, Xiao GS. Choledochoplasty with Gallbladder Wall Free Flap: A Novel Technique for Large Bile Duct Defects from Mirizzi Syndrome in High-Risk Patients-A Case Report and Literature Review. Case Rep Surg. 2019 Jul 30;2019:4615484. doi: 10.1155/2019/4615484[↩]





{kind=link}