
Contents
- What is Moebius syndrome
- Is Moebius syndrome inherited?
- What are the chances of having a second child with Moebius syndrome?
- How can I find a genetics professional in my area?
- Are there any concerns for a person with Moebius syndrome having anesthesia?
- Are individuals with Moebius syndrome considered to be handicapped/disabled?
- Cranial nerves
- Moebius syndrome prognosis
- Moebius syndrome life expectancy
- Moebius syndrome symptoms
- Moebius syndrome causes
- Moebius syndrome diagnosis
- Moebius syndrome treatment
What is Moebius syndrome
Moebius syndrome is a rare neurological birth defect (congenital) that primarily affects the muscles that control facial expression and eye movement 1. The first symptom, present at birth, is an inability to suck. Other signs and symptoms of Moebius syndrome may include weakness or paralysis of the facial muscles; feeding, swallowing, and choking problems; excessive drooling; crossed eyes; lack of facial expression; inability to smile; eye sensitivity; motor delays; high or cleft palate; hearing problems; dental abnormalities; bone abnormalities in the hands and feet; and/or speech difficulties.
Many babies with Moebius syndrome are born with a small chin (micrognathia) and a small mouth (microstomia) with a short or unusually shaped tongue. The roof of the mouth may have an abnormal opening (cleft palate) or be high and arched. These abnormalities contribute to problems with speech, which occur in many children with Moebius syndrome. Dental abnormalities, including missing and misaligned teeth, are also common.
Children with Moebius syndrome are unable to move their eyes back and forth. Affected individuals must move their head from side to side to read or follow the movement of objects. People with this disorder have difficulty making eye contact, and their eyes may not look in the same direction (strabismus). Additionally, the eyelids may not close completely when blinking or sleeping, which can result in dry or irritated eyes.
Decreased numbers of muscle fibers have been reported. Deformities of the tongue, jaw, and limbs, such as clubfoot and missing or webbed fingers, may also occur. As children get older, lack of facial expression and inability to smile become the dominant visible symptoms. Approximately 30 to 40 percent of children with Moebius syndrome have some degree of autism or autism spectrum disorders, which are a group of conditions characterized by impaired communication and social interaction. However, recent studies have questioned this association. Because people with Moebius syndrome have difficulty with eye contact and speech due to their physical differences, autism spectrum disorders can be difficult to diagnose in these individuals. Moebius syndrome may also be associated with a somewhat increased risk of intellectual disability; however, most affected individuals have normal intelligence.
Affected children often experience delayed development of motor skills (such as crawling and walking), although most eventually acquire these skills 2. Other features of Moebius syndrome can include bone abnormalities in the hands and feet, weak muscle tone (hypotonia), and hearing loss.
Moebius syndrome is caused by the absence or underdevelopment of the 6th and 7th cranial nerves, which control eye movement and facial expression 2. Many of the other cranial nerves may also be affected, including the 3rd, 5th, 8th, 9th, 11th and 12th. There is no cure for Moebius syndrome, but proper care and treatment give many individuals a normal life expectancy 2.
The exact incidence of Moebius syndrome is unknown. Researchers estimate that the condition affects 1 in 50,000 to 1 in 500,000 newborns.
There are four recognized categories of Moebius syndrome:
- Group I, characterized by small or absent brain stem nuclei that control the cranial nerves;
- Group II, characterized by loss and degeneration of neurons in the facial peripheral nerve;
- Group III, characterized by loss and degeneration of neurons and other brain cells, microscopic areas of damage, and hardened tissue in the brainstem nuclei, and,
- Group IV, characterized by muscular symptoms in spite of a lack of lesions in the cranial nerve.
There is no specific course of treatment for Moebius syndrome. Treatment is supportive and in accordance with symptoms. Infants may require feeding tubes or special bottles to maintain sufficient nutrition. Surgery may correct crossed eyes and improve limb and jaw deformities. Physical and speech therapy often improves motor skills and coordination, and leads to better control of speaking and eating abilities. Plastic reconstructive surgery may be beneficial in some individuals. Nerve and muscle transfers to the corners of the mouth have been performed to provide limited ability to smile.
For Moebius syndrome there is a very active support and advocacy group in the United States – but like most foundations for rare conditions, it welcomes international members. It has an active young adult and adult platform. And even has a Young Adult Advisory Board which is presently expanding and accepting applications for new young people to join.
- Moebius Syndrome Foundation: https://moebiussyndrome.org/
There is also a group in the United Kingdom. This group appears more focused on driving research to gain a better understanding of the condition and to develop treatments. However, in addition, the group does appear to hold a conference during which people affected by Moebius syndrome in the UK can connect in person with one another.
- Moebius Research Trust: http://www.moebiusresearchtrust.org/
Is Moebius syndrome inherited?
Most cases of Moebius syndrome are not inherited and occur as isolated cases in individuals with no history of the condition in their family (sporadically). A small percentage of cases of Moebius syndrome have been familial (occurring in more than one individual in a family), but there has not been a consistent pattern of inheritance among all affected families 3. In some families the pattern has been suggestive of autosomal dominant inheritance, while in other families it has been suggestive of autosomal recessive or X-linked recessive inheritance 3.
What are the chances of having a second child with Moebius syndrome?
Most cases of Moebius syndrome are isolated, occurring sporadically in only one individual in a family. Although a few familial cases have been reported, no specific genetic cause of the condition has been identified and the manner in which the condition may be inherited is unclear. While the exact recurrence risk for Moebius syndrome in a family with one affected individual is not known, it has been estimated to be about 2% (1 in 50) 3.
Individuals who are interested in learning more about their individual risk to have a child affected with Moebius syndrome may consider speaking with a genetics professional.
How can I find a genetics professional in my area?
To find a medical professional who specializes in genetics, you can ask your doctor for a referral or you can search for one yourself. Online directories are provided by the American College of Medical Genetics (https://www.acmg.net/) and the National Society of Genetic Counselors (https://www.findageneticcounselor.com/).
Are there any concerns for a person with Moebius syndrome having anesthesia?
Orphanet, the European information and resource database for rare and genetic conditions, maintains anesthesia guidelines for many rare and genetic conditions, including one for Moebius syndrome: Anesthesia guidelines for Moebius syndrome (https://www.orpha.net/data/patho/Pro/en/Moebius_EN.pdf).
Are individuals with Moebius syndrome considered to be handicapped/disabled?
This question is a bit difficult to answer due to the fact that not all individuals with Moebius syndrome are affected in the same way. Moebius syndrome primarily affects cranial nerves 6 and 7, causing those with the condition to be unable to move their faces (smile, frown, etc.) or move their eyes from side to side. However, there may also be skeletal involvement causing hand and feet abnormalities. Respiratory problems, speech disorders, visual impairments, and sensory integration dysfunction may also be present. In addition, approximately 30% of children with Moebius syndrome are on the autism spectrum. Children with Moebius syndrome may learn to walk and crawl later than other children but many will eventually catch up. In addition, speech therapy can address the speech problems seen in many children with this condition.
Cranial nerves
The cranial nerves contain the sensory and motor nerve fibers that innervate the head.
The twelve cranial nerves and the origins of their names are briefly described below.
- 1st. Olfactory. This is the sensory nerve of smell.
- 2nd. Optic. Because it develops as an outgrowth of the brain, this sensory nerve of vision is not a true nerve at all. It is more correctly called a brain tract.
- 3rd. Oculomotor. The name oculomotor means “eye mover.” This nerve innervates four of the extrinsic eye muscles—muscles that move the eyeball in the orbit.
- 4th. Trochlear. The name trochlear means “pulley.” This nerve innervates an extrinsic eye muscle that hooks through a pulley-shaped ligament in the orbit.
- 5th. Trigeminal. The name trigeminal means “threefold,” which refers to this nerve’s three major branches. The trigeminal nerve provides general sensory innervation to the face and motor innervation to the chewing muscles.
- 6th. Abducens. This nerve was so named because it innervates the muscle that abducts the eyeball (turns the eye laterally).
- 7th. Facial. This nerve innervates the muscles of facial expression as well as other structures.
- 8th. Vestibulocochlear. This sensory nerve of hearing and equilibrium was once called the auditory nerve.
- 9th. Glossopharyngeal. The name glossopharyngeal means “tongue and pharynx,” structures that this nerve helps to innervate.
- 10th. Vagus. The name vagus means “wanderer.” This nerve “wanders” beyond the head into the thorax and abdomen.
- 11th. Accessory. This nerve was once called the spinal accessory nerve. It originates from the cervical region of the spinal cord, enters the skull through the foramen magnum, and exits the skull with the vagus nerve. The accessory nerve carries motor innervation to the trapezius and sternocleidomastoid muscles.
- 12th. Hypoglossal. The name hypoglossal means “below the tongue.” This nerve runs inferior to the tongue and innervates the tongue muscles.
Based on the types of fibers they contain, the 12 cranial nerves can be classified into three functional groups:
1. Primarily or exclusively sensory nerves (1, 2, 8) that contain special sensory fibers for smell (1st), vision (2nd), and hearing and equilibrium (8th).
2. Primarily motor nerves (3, 4, 6, 11, 12) that contain somatic motor fibers to skeletal muscles of the eye, neck, and tongue.
3. Mixed (motor and sensory) nerves (5, 7, 9, 10). These mixed nerves supply sensory innervation to the face (through general somatic sensory fibers) and to the mouth and viscera (general visceral sensory), including the taste buds for the sense of taste (special visceral sensory). These nerves also innervate pharyngeal arch muscles (somatic motor), such as the chewing muscles (5th) and the muscles of facial expression (7th).
Additionally, four of the cranial nerves (3, 7, 9, 10) contain visceral motor fibers that regulate visceral muscle and glands throughout much of the body. These motor fibers belong to the parasympathetic division of the autonomic nervous system. The autonomic nervous system innervates body structures through chains of two motor neurons. The cell bodies of the second neurons occupy autonomic motor ganglia in the peripheral nervous system. The location of these peripheral autonomic ganglia are described in the pathway of these four nerves.
Cranial nerves are traditionally classified as sensory (I, II, VIII), motor (III, IV, VI, XI, XII), or mixed (V, VII, IX, X). In reality, only cranial nerves I and II (for smell and vision) are purely sensory, whereas all of the rest contain both afferent and efferent fibers and are therefore mixed nerves. Those traditionally classified as motor not only stimulate muscle contractions but also contain sensory fibers of proprioception, which provide the brain with feedback for controlling muscle action and make one aware of such things as the position of the tongue and orientation of the head. Cranial nerve VIII, concerned with hearing and equilibrium, is traditionally classified as sensory, but it also has motor fibers that return signals to the inner ear and tune it to sharpen the sense of hearing. The nerves traditionally classified as mixed have sensory functions quite unrelated to their motor functions. For example, the facial nerve (VII) has a sensory role in taste and a motor role in controlling facial expressions.
Figure 1. 12 Cranial nerves

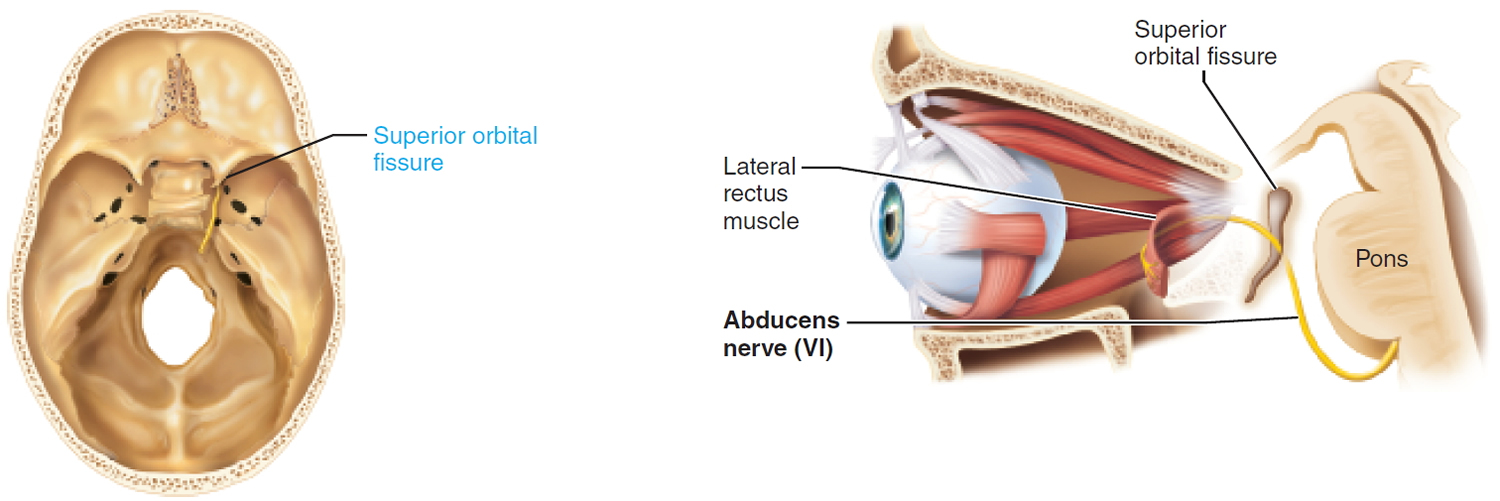
Abducens Nerve (cranial nerve 6)
Somatic motor function: Innervate the lateral rectus muscle. This muscle abducts the eye. Afferent proprioceptor fibers return from the lateral rectus.
Effect of Damage: In abducens nerve paralysis, the eye cannot be moved laterally; at rest, affected eyeball turns medially (internal strabismus).
Origin: Abducens nuclei in the inferior pons.
Pathway: Pass through the superior orbital fissure to enter the orbit.
Figure 2. Abducens nerve (Cranial nerve 6)
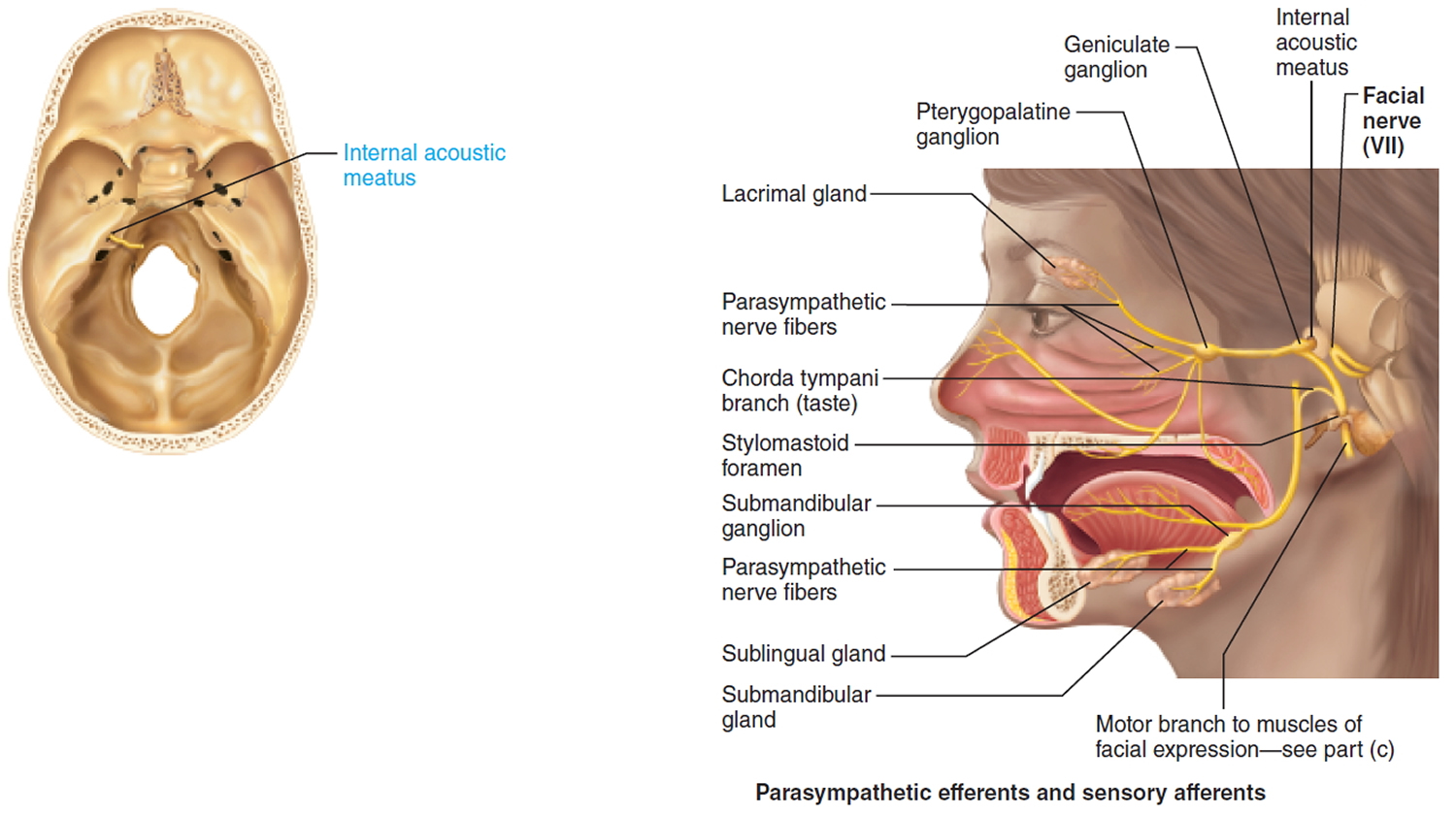
Facial Nerve (cranial nerve 7)
A mixed nerve: Chief somatic motor nerve to the facial muscles; parasympathetic innervation to glands; special sensory taste from the tongue.
Sensory function: Special visceral sensory from taste buds on anterior two-thirds of tongue. General somatic sensory from small patch of skin on the ear.
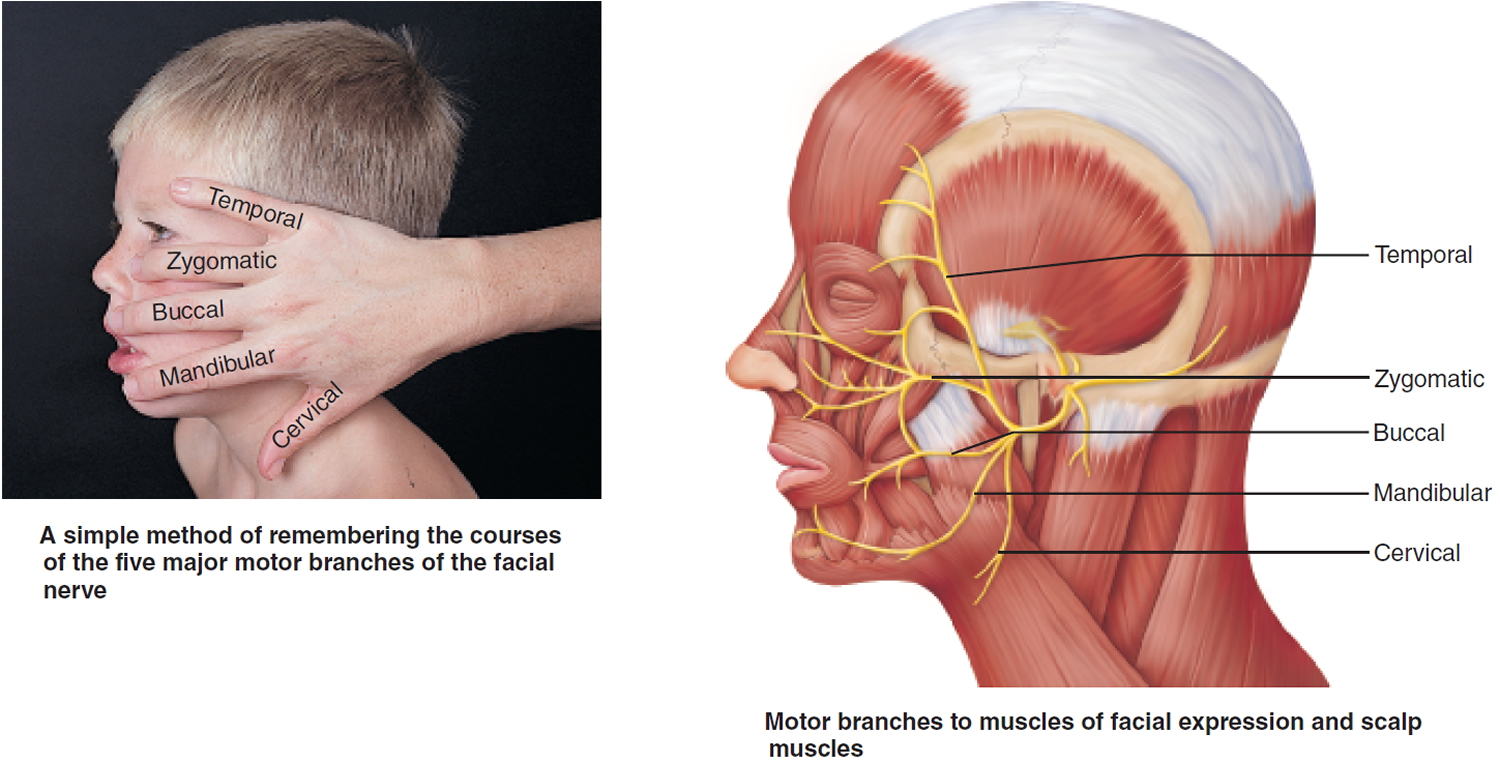
Somatic motor function: Five major branches on face: temporal, zygomatic, buccal, mandibular, and cervical, to innervate the facial muscles. Also innervates the posterior belly of digastric. Afferent proprioceptor fibers return from these muscles.
Visceral motor function (parasympathetic): Innervate the lacrimal (tear) glands, nasal and palatine glands, and the submandibular and sublingual salivary glands.
Effect of Damage: Bell’s palsy, characterized by paralysis of facial muscles on affected side and partial loss of taste sensation, may develop rapidly (often overnight). It is caused by herpes simplex (viral) infection, which produces inflammation and swelling of the facial nerve. The lower eyelid droops, the corner of the mouth sags (making it difficult to eat or speak normally), and the eye constantly drips tears and cannot be completely closed. The condition may disappear spontaneously without treatment.
Origin: Fibers emerge from the pons, just lateral to abducens.
Pathway: Fibers enter the temporal bone via the internal acoustic meatus. Chorda tympani branches off to innervate the two salivary glands and tongue. Branch to facial muscles emerges from the temporal bone through the stylomastoid foramen and courses to lateral aspect of face. Cell bodies of sensory neurons are in geniculate ganglion. Cell bodies of postganglionic parasympathetic neurons are in pterygopalatine and submandibular ganglia on the trigeminal nerve
Figure 3. Facial nerve (Cranial nerve 7)
Moebius syndrome prognosis
There is no cure for Moebius syndrome. In spite of the impairments that characterize the disorder, proper care and treatment give many individuals a normal life expectancy 4.
Moebius syndrome life expectancy
In spite of the impairments that characterize the disorder, proper care and treatment give many individuals a normal life expectancy 4.
Moebius syndrome symptoms
The abnormalities and severity of Moebius syndrome vary greatly from one person-to-another. The classically accepted diagnostic criteria include:
- Facial paralysis or weakness affecting at least one but usually both sides of the face (7th cranial nerve),
- Paralysis of sideways (lateral) movement of the eyes (6th cranial nerve); and
- Preservation of vertical movements of the eyes. Less often, other cranial nerves, including the 5th, 8th, 9th, 10th, 11th, and 12th may be affected.
Moebius syndrome symptoms include the following:
- Lack of facial expression; inability to smile
- Feeding, swallowing and choking problems
- Keeping head back to swallow
- Eye sensitivity due to inability to squint
- Motor delays due to upper body weakness
- Absence of lateral eye movement
- Absence of blinking
- Strabismus (crossed eyes)
- Drooling
- High palate
- Short or deformed tongue
- Limited movement of the tongue
- Submucous cleft palate
- Dental problems
- Hearing impairment
- Articulation / speech disorders
- Minor mid-line anomalies
- Club feet
- Hand/feet deformities
Infants with Moebius syndrome may drool excessively and exhibit crossed eyes (strabismus). Because the eyes do not move from side-to-side (laterally), the child is forced to turn the head to follow objects. Infants who lack facial expression often are described as having a “mask-like” face that is especially obvious when laughing or crying. Affected infants may also have difficulties feeding, including problems swallowing and poor sucking. Corneal ulceration may occur because the eyelids remain open during sleep.
There are a wide variety of additional abnormalities. Some children with Moebius syndrome have a short, malformed tongue and/or an abnormally small jaw (micrognathia). Cleft palate may also be present. These abnormalities contribute to feeding and breathing difficulties. Children with cleft palate are prone to ear infections (otitis media). There may be external ear anomalies including underdevelopment of the outer portion of the ear (microtia) or total absence of the outer portion of the ear (anotia). If the 8th cranial nerve is affected, there is likely hearing loss. Dental abnormalities are not uncommon. There is an increased risk for childhood cavities. Some affected children have difficulties with speech and delays in speech development.
Skeletal malformations of the limbs occur in over half of children with Moebius sydrome. Lower limb malformations include clubbed feet and underdevelopment of the lower legs; upper extremities may have webbing of the fingers (syndactyly), underdevelopment or absence of the fingers, and/or underdevelopment of the hand. In a few children there may be abnormal side-to-side curvature of the spine (scoliosis), and in approximately 15% of patients underdevelopment of the chest (pectoral) muscles and the breast on one side of the body also occur.
Some affected children exhibit delay in attaining certain milestones such as crawling or walking, most likely due to upper body weakness; however, most children eventually catch-up. Moebius syndrome rarely is associated with minor intellectual disability. Some children have been classified as being on the “autistic spectrum”. The exact relationship between Moebius syndrome and autism is unknown. Some studies have suggested that autism spectrum disorders occur with greater frequency in children with Moebius syndrome; other studies have not confirmed this and suggest that any such relationship is overstated. Moebius syndrome is often associated with a variety of social and psychological consequences. The lack of facial expressions and the inability to smile can cause observers to misinterpret what an affected individual is thinking or feeling or intends. Although clinical anxiety and depression are not more common in children and adolescents with Moebius syndrome, affected individuals may avoid social situations due to apprehension and frustration.
Moebius syndrome causes
The causes of Moebius syndrome are unknown, although Moebius syndrome probably results from a combination of environmental and genetic factors. Researchers are working to identify and describe specific genes related to Moebius syndrome. The disorder appears to be associated with changes in particular regions of chromosomes 3, 10, or 13 in some families. Certain medications taken during pregnancy and abuse of drugs such as cocaine may also be risk factors for Moebius syndrome.
Many of the signs and symptoms of Moebius syndrome result from the absence or underdevelopment of cranial nerves 6 and 7. These nerves, which emerge from the brainstem at the back of the brain, control back-and-forth eye movement and facial expressions. The disorder can also affect other cranial nerves that are important for speech, chewing, and swallowing. Abnormal development of cranial nerves leads to the facial muscle weakness or paralysis that is characteristic of Moebius syndrome.
Researchers speculate that Moebius syndrome may result from changes in blood flow to the brainstem during early stages of embryonic development. However, it is unclear what causes these changes to occur and why they specifically disrupt the development of cranial nerves 6 and 7. Even less is known about the causes of some other signs and symptoms of this condition, including hand and foot abnormalities.
Moebius syndrome inheritance pattern
Most cases of Moebius syndrome are sporadic, which means they occur in people with no history of the disorder in their family. A small percentage of all cases have been reported to run in families; however, the condition does not have a single clear pattern of inheritance.
Moebius syndrome diagnosis
A diagnosis of Moebius syndrome is based upon the characteristic signs/symptoms, a detailed patient history, and a thorough clinical evaluation. There are no diagnostic tests that confirm a diagnosis of Moebius syndrome. Some specialized tests may be performed to rule out other causes of facial palsy.
Moebius syndrome treatment
There is no definitive treatment available for Moebius syndrome. The treatment of Moebius syndrome is directed toward the specific abnormalities in each individual. Usually these children are managed by a multidisciplinary team, often in a craniofacial center.
It is important to surround yourself with a good medical team, which may include a mix of the following:
- Pediatricians
- General surgeons
- Pediatric dentists
- Orthopedic surgeons
- Ophthalmologists
- Pediatric otolaryngologists
- Psychologists
- Psychiatrists
- Occupational and physical therapists
- Audiologists
- Speech therapists
Clubfoot
Clubfoot occurs in almost one third of patients. In most cases, the deformity can be corrected partially or entirely by means of orthopedic procedures.
Ponseti Method: The majority of clubfeet can be corrected in infancy in about six to eight weeks with the proper gentle manipulations and plaster casts. The treatment is based on a sound understanding of the functional anatomy of the foot and of the biological response of muscles, ligaments and bone to corrective position changes gradually obtained by manipulation and casting.
Physical therapy may be needed for individuals with various orthopedic abnormalities. Occupational therapy may also be beneficial, especially in patients with abnormalities of the hands, fingers and toes. Speech therapy may be necessary for some affected children. Strabismus is usually surgically correctable, although some physicians recommend delaying these procedures as the condition sometimes improves with age. Operations may also be necessary for the various skeletal malformations affecting the limbs and jaws. Specialized procedures to correct abnormalities and/or underdevelopment of the chest wall and breast are available.
Splints, braces and prostheses may be necessary for individuals with congenital limb abnormalities. Genetic counseling may be of benefit for affected individuals and their families.
Surgical therapy
Surgical care may be an option to treat symptoms of Moebius syndrome, but are not a cure. Examples of surgical procedures:
Eyes
- Strabismus (crossed eyes) may be improved with surgery.
- Eyelid surgery for epicanthal folds, and eyelid surgery or gold weights to protect the cornea.
Hands
Underdevelopment of hand or fingers, or webbing of the fingers (syndactyly) – surgery often can be performed to separate fingers.
Smile Surgery
Corrective procedures for facial paralysis involve transfer of muscle and/or graft nerves from another area of the face or the body. An old procedure, known as temporalis tendon transfer, involves taking the temporalis muscle, one of the muscles normally used for chewing (mastication), and transferring it to the corners of the mouth. This same type of operation can be also used to improve closure of the eyelids. If the paralysis is on only one side (unilateral), a “cross-facial nerve graft” is an option. The procedure involves taking a sensory nerve from the calf, attaching it to a branch of the functioning facial nerve on the normal side of the face and then waiting until the regenerating nerve fibers cross over the face to reach the paralyzed side where it is joined to a motor nerve of a thin muscle transferred to the face by microvascular anastomosis.
The most recent procedure, called “the smile operation”, involves microvascular transfer of a muscle from the thigh (gracillis) to the face and connecting the nerves that normally supply the masseter muscle (one of the muscles used for chewing). This operation has shown remarkable results in terms of speech, facial mobility and self-esteem. Frequent lubrication for dry eyes is often necessary.
Airway
Airway functions commonly are compromised. Tracheotomy may be required to support the airway.
- Moebius syndrome. https://ghr.nlm.nih.gov/condition/moebius-syndrome[↩]
- Moebius Syndrome Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Moebius-Syndrome-Information-Page[↩][↩][↩]
- MOEBIUS SYNDROME. http://omim.org/entry/157900[↩][↩][↩]
- Matsui K, Kataoka A, Yamamoto A, Tanoue K, Kurosawa, K, Shibasaki, J, Ohyama M, and Aida N. Clinical characteristics and outcomes of Mobius syndrome in a Children’s Hospital. Pediatric Neurology. December 2014; 51(6):781-789. http://www.sciencedirect.com.ezproxy.nihlibrary.nih.gov/science/article/pii/S0887899414005177[↩][↩]



{kind=link}