What is myomectomy
Myomectomy is a surgical procedure to remove uterine fibroids (leiomyomas) 1. In myomectomy, only the fibroids are removed. The womb (uterus) remains intact. Uterine fibroids are common noncancerous growths that appear in the uterus, usually during childbearing years, but they can occur at any age.
Your doctor might recommend myomectomy for uterine fibroids causing symptoms that are troublesome or interfere with your normal activities. If you need surgery, reasons to choose a myomectomy instead of a hysterectomy for uterine fibroids include:
- You plan to bear children
- Your doctor suspects uterine fibroids might be interfering with your fertility
- You want to keep your uterus
Uterine fibroids can be removed in different ways:
- Through the vagina (hysteroscopic myomectomy)
- Through small cuts in your abdomen (laparoscopic myomectomy)
- Through a cut across your abdomen (abdominal myomectomy or laparotomy)
The surgeon’s goal during myomectomy is to take out symptom-causing fibroids and reconstruct the uterus. Unlike a hysterectomy, which removes your entire uterus, a myomectomy removes only the fibroids and leaves your uterus intact.
Women who undergo myomectomy report improvement in fibroid symptoms, including heavy menstrual bleeding and pelvic pressure.
General anesthetic is needed for all of myomectomy procedures. The most suitable treatment options will depend on the number, location and size of the fibroids. Abdominal myomectomies are usually avoided because they aren’t as gentle as the other procedures and leave a larger scar in the abdominal wall. Laparoscopy or hysteroscopic myomectomy aren’t always possible if the fibroids are very large or if there are so many of them that the womb has grown bigger.
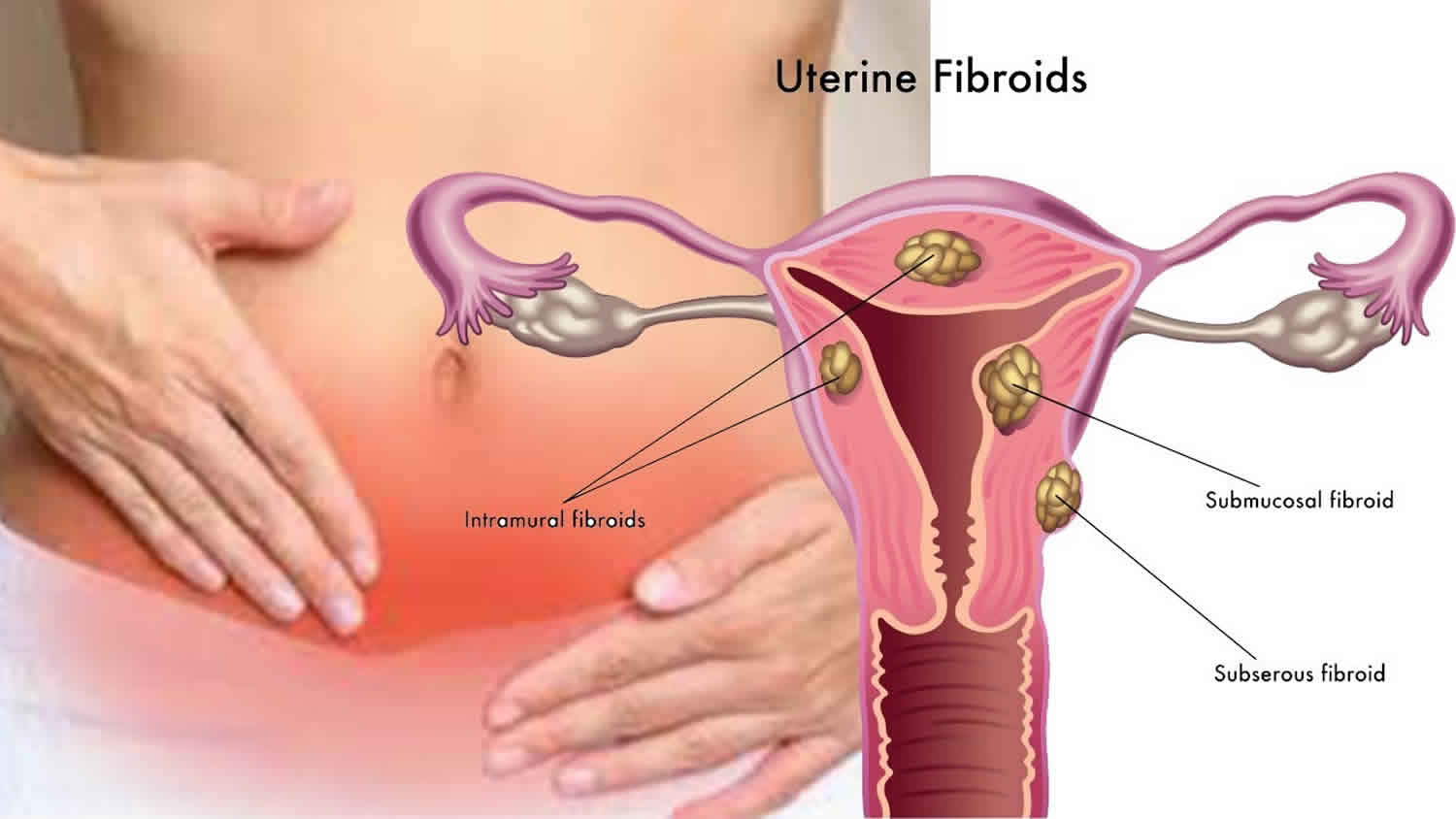
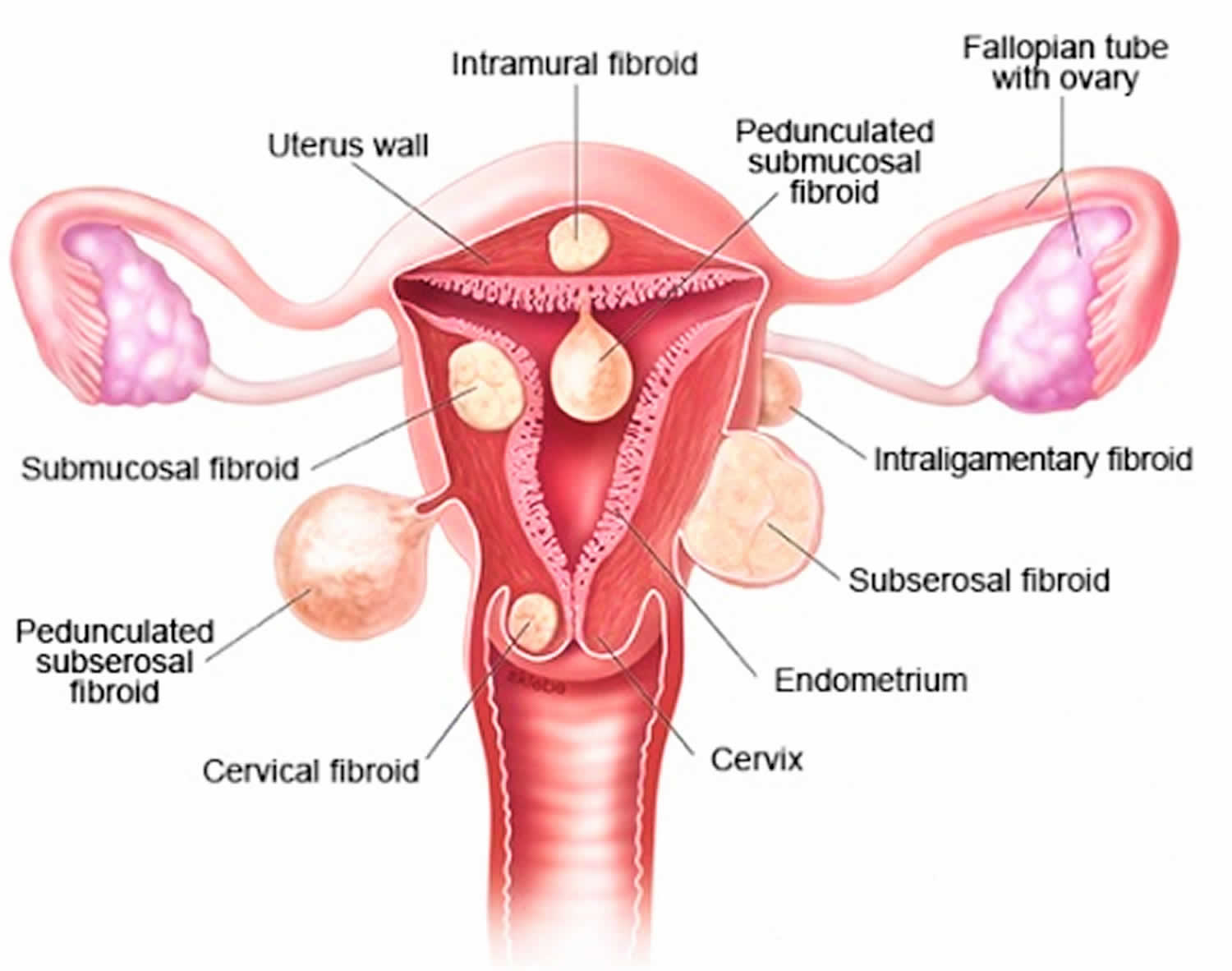
Laparoscopy and abdominal myomectomy also make it possible to remove fibroids outside of the womb that have grown into the abdominal cavity. This includes pedunculated fibroids (fibroids with a thin, “stem-like” attachment) and subserosal fibroids (located on the outer wall of the womb). These procedures can also be used to remove intramural fibroids (in the wall of the womb) that bulge outward, and intraligamentary fibroids (next to the womb).
Operating through the vagina (hysteroscopic myomectomy) is most suitable for fibroids that protrude into the space inside the womb. This may be the case with intramural fibroids (in the wall of the womb) or submucosal fibroids (just under the lining of the womb). Then removing the fibroids through the vagina is generally a more gentle approach than laparoscopy. Studies suggest that operating through the vagina is usually quicker and associated with less blood loss.
Figure 1. Uterine fibroids
How does myomectomy affect the symptoms?
Most women who have had fibroid symptoms for a long time notice a major improvement after myomectomy surgery or no longer have any symptoms at all. Research shows that about 90 out of 100 women who have myomectomy procedure are still satisfied with the results one to two years afterwards. In up to 20 out of 100 women, fibroids grow again within the first few years after the myomectomy procedure 1.
What is myomectomy recovery time?
You can expect to feel better and stronger each day, although you may tire quickly and need pain medicine for a week or two. You may need about 4 to 6 weeks to fully recover.
Do not lift anything heavy while you are recovering so that your incision and your belly muscles can heal.
Comparing myomectomy and hysterectomy
The risk of short-term complications is about the same when just the fibroids are removed through a large abdominal incision (abdominal myomectomy) and when the womb is removed through a large abdominal incision (abdominal hysterectomy). But the long-term pros and cons of these two approaches can’t be compared because there hasn’t been any research in this area.
Removing only the fibroids (myomectomy) has the advantage of leaving the womb intact, so the woman can still become pregnant after the operation. Myomectomy procedure often relieves fibroid symptoms just as well as removing the whole womb (hysterectomy) does. But fibroids can grow back again after a myomectomy, and then cause associated symptoms. This can’t happen after a hysterectomy.
Myomectomy risks
Myomectomy has a low complication rate. Still, myomectomy procedure poses a unique set of challenges. Risks of myomectomy include:
- Excessive blood loss. Many women already have low blood counts (anemia) due to heavy menstrual bleeding, so they’re at a higher risk of problems due to blood loss. Your doctor may suggest ways to build up your blood count before surgery. During myomectomy, surgeons take extra steps to avoid excessive bleeding, including blocking flow from the uterine arteries and injecting medications around fibroids to cause blood vessels to clamp down. Studies suggest blood loss is similar between a myomectomy and hysterectomy. Also, with both, blood loss is higher with a larger uterus.
- Scar tissue. Incisions into the uterus to remove fibroids can lead to adhesions — bands of scar tissue that may develop after surgery. Outside the uterus, adhesions could entangle nearby structures and lead to a blocked fallopian tube or a trapped loop of intestine. Rarely, adhesions may form within the uterus and lead to light menstrual periods and difficulties with fertility (Asherman’s syndrome). Laparoscopic myomectomy may result in fewer adhesions than abdominal myomectomy (laparotomy).
- Pregnancy or childbirth complications. A myomectomy can increase certain risks during delivery if you become pregnant. If your surgeon had to make a deep incision in your uterine wall, the doctor who manages your subsequent pregnancy may recommend cesarean delivery (C-section) to avoid rupture of the uterus during labor, a very rare complication of pregnancy. Fibroids themselves are also associated with pregnancy complications.
- Rare chance of hysterectomy. Rarely, the surgeon must remove the uterus if bleeding is uncontrollable or other abnormalities are found in addition to fibroids.
- Rare chance of spreading a cancerous tumor. Rarely, a cancerous tumor can be mistaken for a fibroid. Taking out the tumor, especially if it’s broken into little pieces to remove through a small incision, can lead to spread of the cancer. The risk of this happening increases after menopause and as women age.
Studies on myomectomy have shown that about 5 out of 100 women have complications such as injury to organs in the abdomen, or need to have the procedure again. Fewer than 1 out of 100 women needed to have a hysterectomy because of uncontrollable bleeding after myomectomy. Temporary problems like fever or wound infections may occur.
Laparoscopy causes less blood loss than laparotomy, and complications are equally rare after both procedures.
Surgery-related scar tissue may lead to adhesions in the abdominal cavity over the long term. These strands of connective tissue may cause organs to attach to the abdominal wall. Scars and adhesions can cause pain in the lower abdomen. Depending on their location, they may cause bowel problems or affect fertility too.
Strategies to prevent possible surgical complications
To minimize risks of myomectomy surgery, your doctor may recommend:
- Iron supplements and vitamins. If you have iron deficiency anemia from heavy menstrual periods, your doctor might recommend iron supplements and vitamins to allow you to build up your blood count before surgery.
- Hormonal treatment. Another strategy to correct anemia is hormonal treatment before surgery. Your doctor may prescribe a gonadotropin-releasing hormone (GnRH) agonist, birth control pills, or other hormonal medication to stop or decrease your menstrual flow. When given as therapy, a GnRH agonist blocks the production of estrogen and progesterone, stopping menstruation and allowing you to rebuild hemoglobin and iron stores.
- Therapy to shrink fibroids. Some hormonal therapies, such as gonadotropin-releasing hormone (GnRH) agonist therapy, can also shrink your fibroids and uterus enough to allow your surgeon to use a minimally invasive surgical approach — such as a smaller, horizontal incision rather than a vertical incision, or a laparoscopic procedure instead of an open procedure. In most women, GnRH agonist therapy causes symptoms of menopause, including hot flashes, night sweats and vaginal dryness. However, these discomforts end after you stop taking the medication. Treatment generally occurs over several months before surgery. Evidence suggests that not every woman should take GnRH agonist therapy before myomectomy. GnRH agonist therapy may soften and shrink fibroids enough to interfere with their detection and removal. The cost of the medication and the risk of side effects must be weighed against the benefits. Drugs that modulate progesterone action, such as ulipristal (ella), also may decrease symptoms and shrink fibroids. Outside the United States, ulipristal is approved for three months of therapy before a myomectomy.
Myomectomy procedure
Food and medications
You’ll need to fast — stop eating or drinking anything — in the hours before your surgery. Follow your doctor’s recommendation on the specific number of hours.
If you’re on medications, ask your doctor if you should change your usual medication routine in the days before surgery. Tell your doctor about any over-the-counter medications, vitamins or other dietary supplements that you’re taking.
Ask your doctor about the type of anesthesia you may receive:
- General anesthesia, which means you’re asleep during surgery, is used for abdominal, laparoscopic, robotic and some hysteroscopic myomectomies
- Spinal anesthesia, where medication is injected into your spinal canal to numb the nerves in the lower half of your body, is used for certain hysteroscopic myomectomies.
Finally, discuss with your doctor pain medication and how it will likely be given.
Other preparations
Whether you stay in the hospital for just part of the day or overnight depends on the type of procedure you have. Abdominal (open) myomectomy usually requires a hospital stay of two to three days. In most cases, laparoscopic or robotic myomectomy only requires an overnight stay. Hysteroscopic myomectomy is often done with no overnight hospital stay.
Your facility may require that you have someone accompany you on the day of surgery. Make sure you have someone lined up to help with transportation and to be supportive.
What you can expect
Depending on the size, number and location of your fibroids, your surgeon may choose one of three surgical approaches to myomectomy.
Abdominal myomectomy
In abdominal myomectomy (laparotomy), your surgeon makes an open abdominal incision to access your uterus and remove fibroids. Your surgeon enters the pelvic cavity through one of two incisions:
- A horizontal bikini-line incision that runs about an inch (about 2.5 centimeters) above your pubic bone. This incision follows your natural skin lines, so it usually results in a thinner scar and causes less pain than a vertical incision does. It may be only 3 to 4 inches (8 to 10 centimeters), but may be much longer. Because it limits the surgeon’s access to your pelvic cavity, a bikini-line incision may not be appropriate if you have a large fibroid.
- A vertical incision that starts in the middle of your abdomen and extends from just below your navel to just above your pubic bone. This gives your surgeon greater access to your uterus than a horizontal incision does and it reduces bleeding. It’s rarely used, unless your uterus is so big that it extends up past your navel.
Laparoscopic myomectomy
In laparoscopic myomectomy or robotic myomectomy, also called minimally invasive procedure, your surgeon accesses and removes fibroids through several small abdominal incisions.
- Laparoscopic myomectomy. Your surgeon makes a small incision in or near your bellybutton. Then he or she inserts a laparoscope ― a narrow tube fitted with a camera ― into your abdomen. Your surgeon performs the surgery with instruments inserted through other small incisions in your abdominal wall.
- Robotic myomectomy. Instruments are inserted through small incisions similar to those in a laparoscopic myomectomy, and the surgeon controls movement of instruments from a separate console.
Sometimes, the fibroid is cut into pieces and removed through a small incision in the abdominal wall. Other times the fibroid is removed through a bigger incision in your abdomen so it can be removed without being cut into pieces. Rarely, the fibroid may be removed through an incision in your vagina (colpotomy).
Laparoscopic and robotic surgery use smaller incisions than a myomectomy, or laparotomy, does. This means you may have less pain, lose less blood and return to normal activities more quickly than with a laparotomy.
Hysteroscopic myomectomy
To treat fibroids that bulge significantly into your uterine cavity (submucosal fibroids), your surgeon may suggest a hysteroscopic myomectomy. Your surgeon accesses and removes fibroids using instruments inserted through your vagina and cervix into your uterus.
A hysteroscopic myomectomy generally follows this process:
- Your surgeon inserts a small, lighted instrument — called a resectoscope because it cuts (resects) tissue using electricity or a laser beam — through your vagina and cervix and into your uterus.
- A clear liquid, usually a sterile salt solution, is inserted into your uterus to expand your uterine cavity and allow examination of the uterine walls.
- Using the resectoscope, your surgeon shaves pieces from the fibroid until it aligns with the surface of your uterine cavity.
- The removed fibroid tissue washes out with the clear liquid that’s used to expand your uterus during the procedure.
Rarely, your surgeon may use a laparoscope inserted through a small incision in your abdomen to view the pelvic organs and monitor the outside of the uterus during a complicated hysteroscopic myomectomy.
Myomectomy recovery
After surgery to remove one or more fibroids, you may feel some pain in your belly for several days. Your belly may also be swollen. You may have a change in your bowel movements for a few days. And you may have some cramping for the first week.
At discharge from the hospital, your doctor prescribes oral pain medication, tells you how to care for yourself, and discusses restrictions on your diet and activities.
It’s normal to also have some shoulder or back pain. This is caused by the gas your doctor put in your belly to help see your organs better.
You can expect some vaginal spotting or light bleeding for a few days up to 8 weeks, depending on the type of myomectomy procedure you’ve had. And each person recovers at a different pace. You may have a brown or reddish brown vaginal discharge or spotting for a few weeks or until your first period. This is normal. Expect your first two periods to start early or late. They may be more painful or heavy than usual.
To help with pain, your doctor will prescribe medicines. You will need 2 or more weeks to fully recover. It’s important not to lift anything heavy for about 1 week. Your doctor may talk to you about when you can have sex and when it’s safe to try to become pregnant.
How to care for yourself at home
Activity
- Rest when you feel tired.
- Be active. Walking is a good choice.
- Allow your body to heal. Don’t move quickly or lift anything heavy until you are feeling better.
- Ask your doctor when you can have sex.
- Hold a pillow over your incisions when you cough or take deep breaths. This will support your belly and may help to decrease your pain.
- Do breathing exercises at home as instructed by your doctor. This will help prevent pneumonia.
Diet
- You can eat your normal diet. If your stomach is upset, try bland, low-fat foods like plain rice, broiled chicken, toast, and yogurt.
- If your bowel movements are not regular right after surgery, try to avoid constipation and straining. Drink plenty of water. Your doctor may suggest fibre, a stool softener, or a mild laxative.
Medicines
Be safe with medicines. Read and follow all instructions on the label.
- If the doctor gave you a prescription medicine for pain, take it as prescribed.
- If you are not taking a prescription pain medicine, ask your doctor if you can take an over-the-counter medicine.
Your doctor will tell you if and when you can restart your medicines. He or she will also give you instructions about taking any new medicines.
If you take blood thinners, such as warfarin (Coumadin), clopidogrel (Plavix), or aspirin, be sure to talk to your doctor. He or she will tell you if and when to start taking those medicines again. Make sure that you understand exactly what your doctor wants you to do.
Incision care
- If you have strips of tape on the cut (incision) the doctor made, leave the tape on for a week or until it falls off.
- If you have skin adhesive on the incision, leave it on until it falls off. Skin adhesive is also called liquid stitches.
- Wash the area daily with warm, soapy water, and pat it dry. Don’t use hydrogen peroxide or alcohol. They can slow healing.
- You may cover the area with a gauze bandage if it oozes fluid or rubs against clothing.
- Change the bandage every day.
- Keep the area clean and dry.
Other instructions
- Wear loose, comfortable clothing. For a few weeks, avoid anything that puts pressure on your belly.
- You may have some light vaginal bleeding. Wear sanitary pads if needed. Do not douche or use tampons.
- You may want to use a heating pad on your belly to help with pain.
Follow-up care is a key part of your treatment and safety. Be sure to make and go to all appointments, and call your doctor or nurse call line if you are having problems. It’s also a good idea to know your test results and keep a list of the medicines you take.
Call your local emergency services number anytime you think you may need emergency care. For example, call if:
- You passed out (lost consciousness).
- You have chest pain, are short of breath, or cough up blood.
Call your doctor now or seek immediate medical care if:
- You have pain that does not get better after you take pain medicine.
- You cannot pass stools or gas.
- You have vaginal discharge that has increased in amount or smells bad.
- You are sick to your stomach or cannot drink fluids.
- You have loose stitches, or your incision comes open.
- Bright red blood has soaked through the bandage over your incision.
- You have signs of infection, such as:
- Increased pain, swelling, warmth, or redness.
- Red streaks leading from the incision.
- Pus draining from the incision.
- A fever.
- You have bright red vaginal bleeding that soaks one or more pads in an hour, or you have large clots.
- You have signs of a blood clot in your leg (called a deep vein thrombosis), such as:
- Pain in your calf, back of the knee, thigh, or groin.
- Redness and swelling in your leg.
Watch closely for changes in your health, and be sure to contact your doctor or nurse call line if you have any problems.
Myomectomy results
Outcomes from myomectomy may include:
- Symptom relief. After myomectomy surgery, most women experience relief of bothersome signs and symptoms, such as excessive menstrual bleeding and pelvic pain and pressure.
- Fertility improvement. Removing submucosal fibroids by hysteroscopic myomectomy can improve fertility and pregnancy outcomes. After a myomectomy, wait at least three months before attempting conception to allow the uterus enough healing time.
Tiny tumors (seedlings) that your doctor doesn’t detect during surgery could eventually grow and cause symptoms. New fibroids, which may or may not require treatment, also can develop. Women who had only one fibroid have a lower risk of needing to have treatment for additional fibroids ― often termed the recurrence rate ― than do women with multiple fibroids.
Pregnancy after myomectomy
Having a myomectomy doesn’t usually affect fertility – unless adhesions form later on, and hinder the ovaries or fallopian tubes. Studies have looked into whether the type of procedure influences a woman’s chances of becoming pregnant. The results showed no differences between laparotomy and laparoscopy. About one third of women in both groups gave birth within two years 1.
Sometimes fibroids are removed with the aim of improving fertility. A fibroid located under the lining of the womb may prevent a fertilized egg from attaching to it. But there has been very little good-quality research on the question of whether a myomectomy can improve a woman’s chances of getting pregnant. The few studies that are available don’t allow any conclusions to be drawn about whether surgery helps 1.

{kind=link}