
Contents
What is myringotomy
Myringotomy is a surgical procedure of the eardrum or tympanic membrane. Myringotomy is performed by making a small incision with a myringotomy knife through the layers of tympanic membrane. This surgical procedure permits direct access to the middle ear space and allows the release of middle-ear fluid, which is the end product of otitis media with effusion or “glue ear”, whether acute or chronic. Middle ear effusion (glue ear) is classified as serous, mucoid, or purulent.
Usually middle ear effusion (glue ear) improves on its own. But if it doesn’t, it can cause hearing problems.
The options for treating middle ear effusion (glue ear) include:
- Wait and see if the fluid goes away
- Myringotomy to insert myringotomy tubes or grommets
Middle ear effusion (glue ear) almost always gets better but it is not always possible to say when this will happen.
Myringotomy is recommended if the glue ear continues for longer than three months and is causing problems with poor hearing or repeated ear infections.
Myringotomy operation is usually performed under a general anesthetic but a local anesthetic can be used. Myringotomy usually takes about 20 minutes.
The fluid is suctioned from the middle ear through the myringotomy incision and, if indicated, sent for bacterial or viral cultures. Currently, bilateral myringotomy is often used in conjunction with placement of middle-ear ventilation tubes (myringotomy tubes or grommets), which permits the incised ear drum to remain open and allows better drainage of middle-ear fluid 1. This approach facilitates instillation of antibiotic ear drops, and ultimately results in faster resolution of the otitis media with effusion (glue ear) 2.
Middle ear effusions (glue ear) may spontaneously occur as a result of inadequate ventilation of the middle-ear space related to poor eustachian tube function or a persistent inflammatory response to acute otitis media (AOM). Additional contributors to the development of otitis media with effusion include the immaturity both of the infant or young child’s immune system and of the anatomy of the eustachian tube.
The eustachian tube is the communication between the middle ear and the nasopharynx. Its function is to equalize pressure across the tympanic membrane. Contraction of the tensor veli palatini and the salpingopharyngeus outside of the tympanic cavity (middle ear) dilate and open the auditory tube.
In children, the eustachian tube is shorter, more horizontally oriented, and less functionally mature, and these differences can predispose children to otitis media with effusion. Inflammation of the mucosa of the eustachian tube orifice (from conditions such as upper respiratory infection [URI] or allergy) and improper functioning of the eustachian tube musculature lead to negative middle-ear pressure. Thus, when the eustachian tube opens, bacteria and viruses from the nasopharynx are drawn into the middle-ear space and generate an inflammatory response.
Middle ear effusions (glue ear) has a strong correlation with upper respiratory tract infection. Children with craniofacial abnormalities that affect eustachian tube function (e.g., Down syndrome and cleft palate) are at increased risk for otitis media. Immune deficiency should be suspected in children with otitis media with effusion that occurs in association with recurrent sinusitis, bronchitis, or gastrointestinal (GI) abnormalities.
Other predisposing conditions include allergy, adenoid hypertrophy, ciliary dysfunction, and gastroesophageal reflux. otitis media with effusion may be seen in patients with prolonged nasal intubation or nasogastric tubes 2.
Figure 1. Ear anatomy
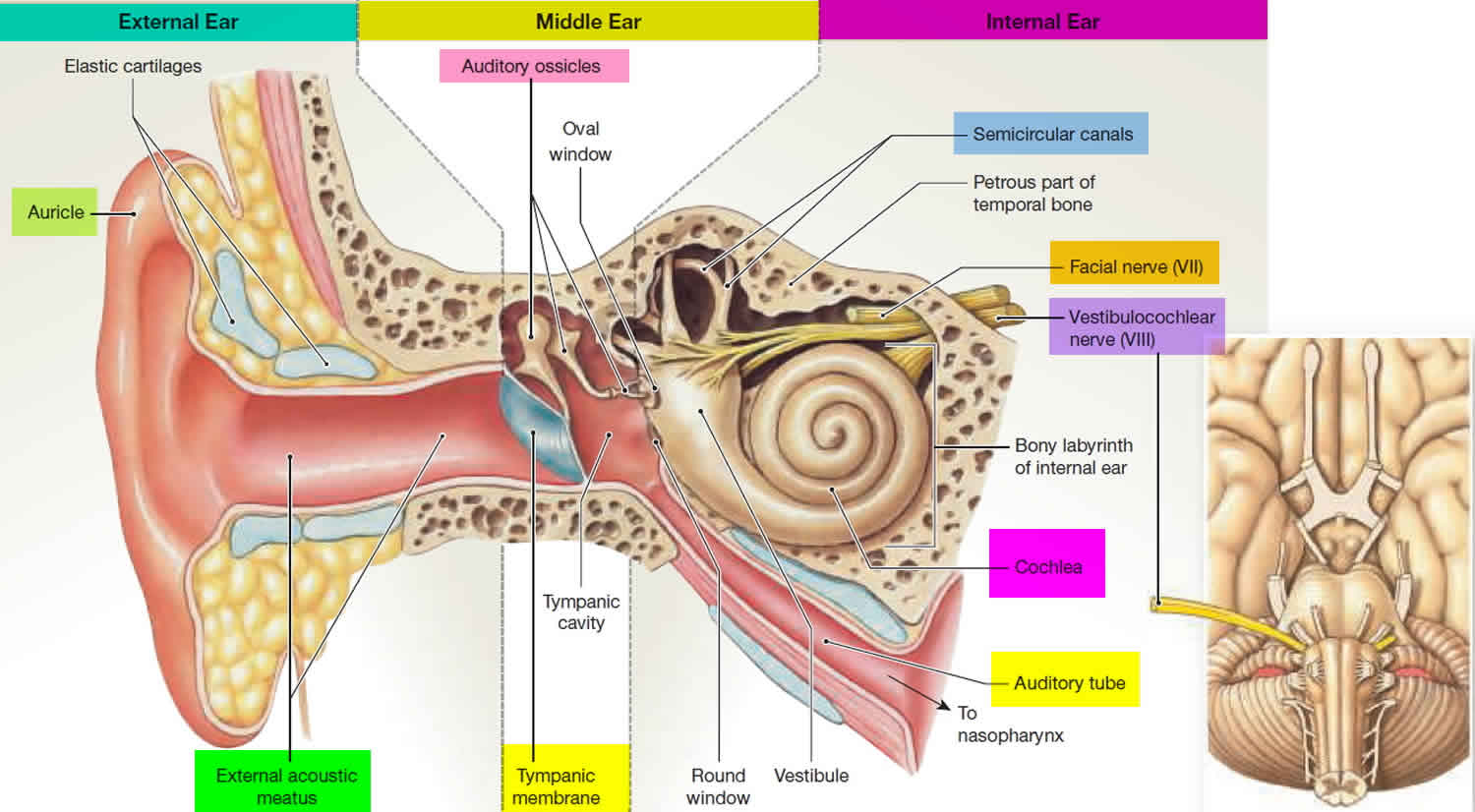
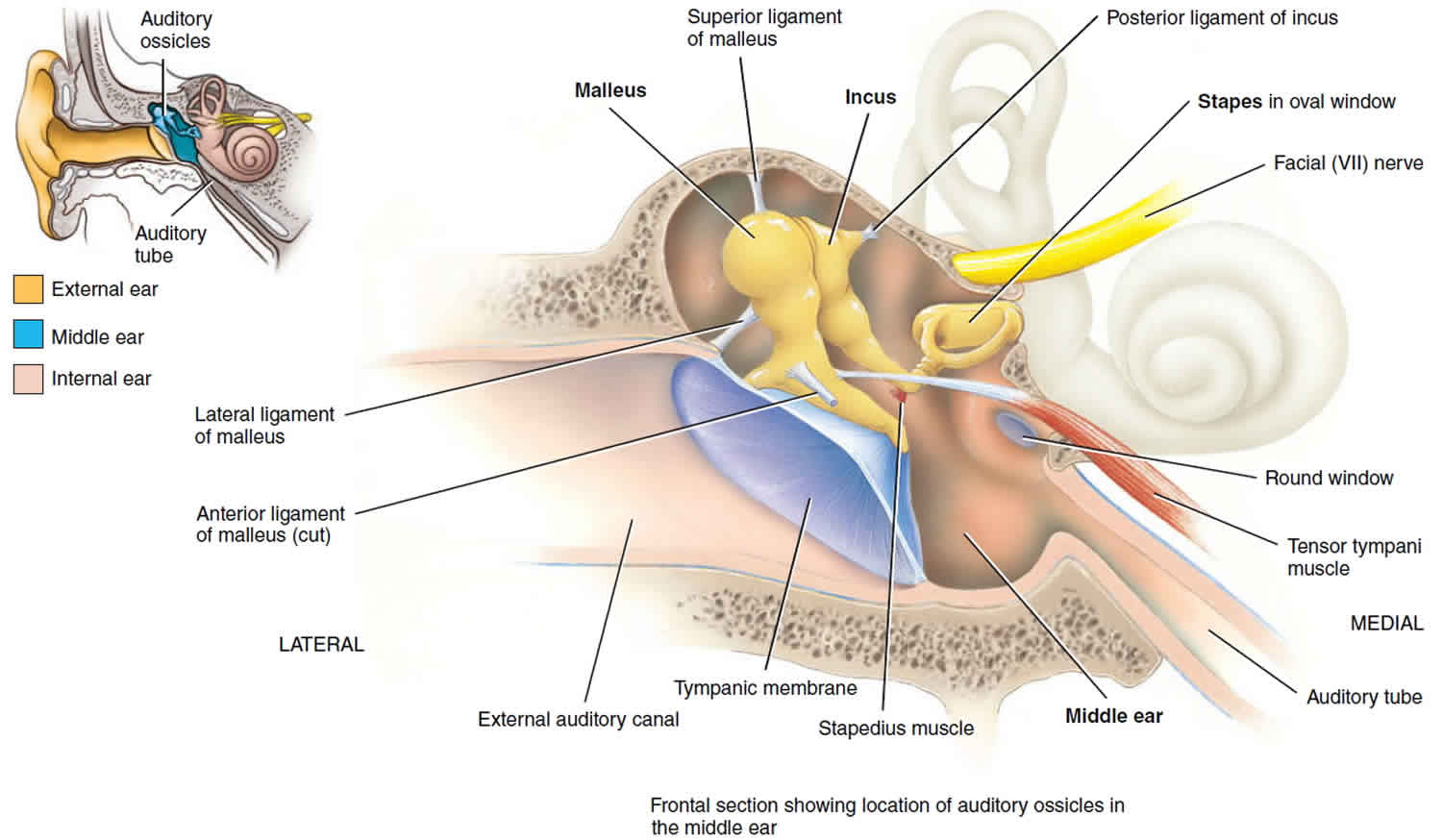
Figure 2. Middle ear anatomy
Myringotomy indications
Myringotomy may be indicated in cases of acute otitis media, recurrent acute otitis media with effusion and chronic otitis media with effusion. Patients with acute otitis media that is refractory to medical therapy or associated with signs of toxicity require myringotomy with or without middle-ear culture. Children with recurrent acute episodes of otitis media (usually understood as more than 4-5 infections in 6 months) benefit from myringotomy. The most common indication is for children with chronic middle ear effusion of more than 3 months duration.
Because of the rapid healing properties of the tympanic membrane, myringotomy with aspiration of effusion has a shorter-lived benefit than myringotomy performed in conjunction with myringotomy tube (grommet) placement. Studies have advocated myringotomy with tube insertion over myringotomy alone to decreased the time of effusion and improve hearing 3.
A child who displays speech and language delay secondary to middle ear infection should undergo prompt myringotomy with or without ear tubes. Additionally, certain subsets of children are more likely to need prompt surgical intervention (i.e, myringotomy), including the following 4:
- Children with permanent hearing loss independent of middle ear effusion
- Children with autism-spectrum disorder and other pervasive developmental disorders
- Children with syndromes (e.g., Down syndrome) or craniofacial disorders that result in eustachian tube dysfunction
- Children who are blind or have uncorrectable visual impairment
- Children who have cleft palate with or without cleft lip 5
Myringotomy tubes
Myringotomy tubes also known as grommets, ventilation tubes or tympanostomy tubes, are little tubes inserted into the eardrum after repeated ear infections which cause ‘glue ear’ (otitis media with effusion). Glue ear is caused by a build-up of fluid in the inner ear that tends to get thick and sticky if it persists for long enough. This often happens with frequent ear infections. If it lasts for longer than 3 months and causes significant hearing loss it is usually treated with myringotomy tubes.
Myringotomy tubes can be made of plastic or metal. Myringotomy tubes don’t hurt. They allow air to enter the middle ear and drain the fluid to the back of the nose and throat.
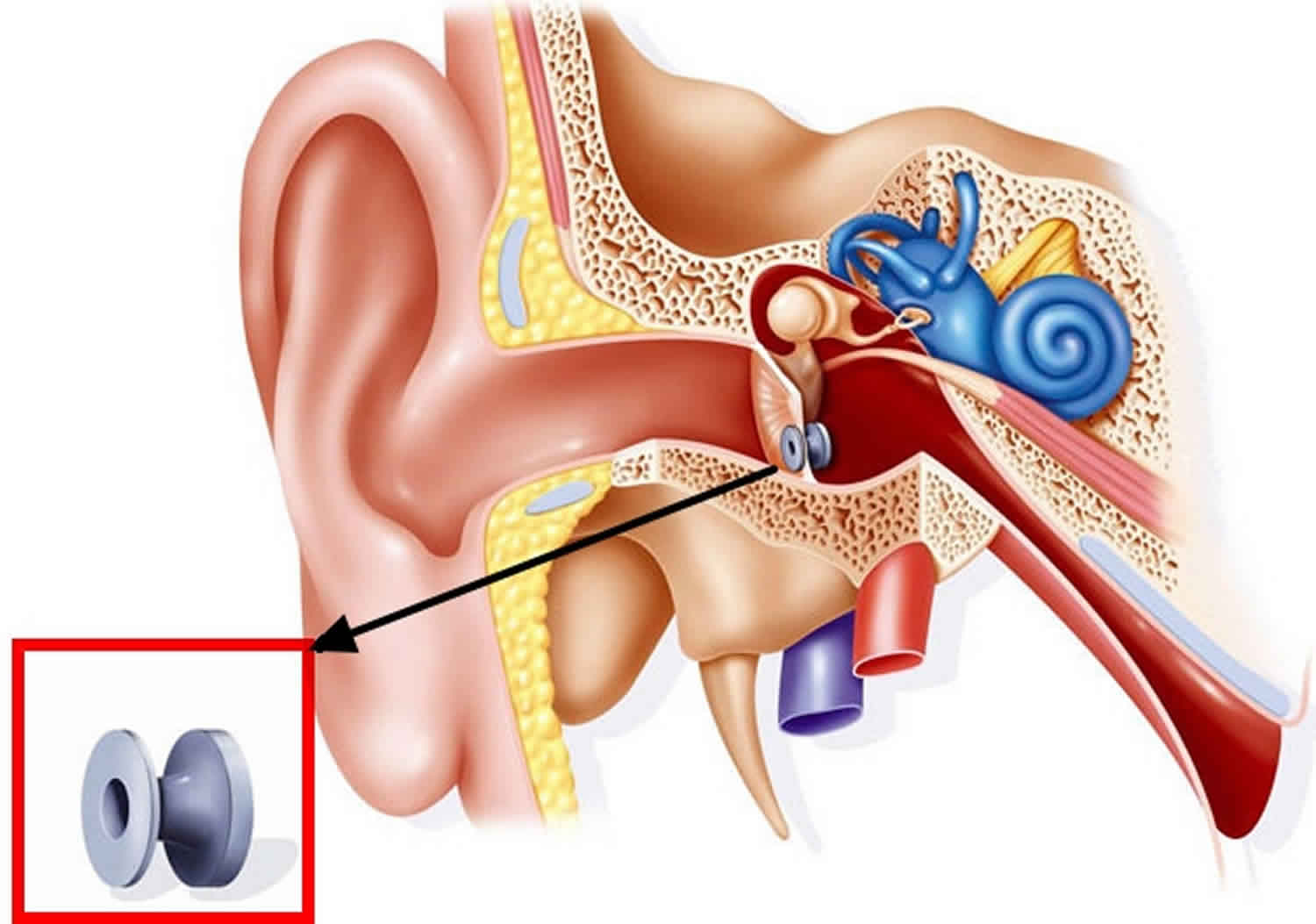
Figure 3. Myringotomy tube
When are myringotomy tubes used?
Myringotomy tubes might be recommended if you or your child has had middle ear effusion (glue ear) for at least 3 months and has trouble hearing. Myringotomy tubes might also be recommended for repeated ear infections as they usually reduce the incidence of ear infections.
Myringotomy tubes usually fall out naturally within 6 to 12 months, leaving the eardrum unharmed.
How are myringotomy tubes inserted?
Myringotomy tubes are inserted during minor surgery called ‘myringotomy’ where a small cut is made in the eardrum and any fluid is suctioned out. The myringotomy tubes, are then inserted into the eardrums to drain fluid and ventilate the middle ear.
The procedure usually takes about 15 minutes and is done under general anesthetic and is usually done as a day only procedure, so your child won’t feel anything and your child will not usually need to stay overnight in hospital. Hearing is generally restored quickly afterwards.
Myringotomy tubes for adults
Adults can also develop glue ear, and may also require insertion of myringotomy tubes.
Myringotomy tubes complications
It is normal for there to be a small amount of oozing or bleeding from the ear for a day or two after surgery.
Contact your doctor if there is a lot of pain, or if the oozing or bleeding continues for more than five days. There could be an ear infection or a small tear in the eardrum.
Caring for a child with myringotomy tubes
Most children recover well from the operation to insert myringotomy tubes. You should see your doctor if your child experiences pain, or any discharge from the ear that lasts for more than 5 days.
One of the complications of myringotomy tubes is ear infection from water getting into the middle ear cavity, so it is best to keep the ears dry. Your child should:
- avoid swimming for a week after the surgery
- use earplugs when bathing, showering and swimming
To avoid getting an ear infection, your doctor may suggest that your child avoids getting their ears wet with water that may have germs, such as bath water. Earplugs may be necessary when bathing and showering.
Earplugs should also be used when swimming. Swimming should be avoided altogether for the first week after the myringotomy tubes are inserted. If your child develops a discharge from the ears, see your doctor.
If your child had hearing problems before having myringotomy tubes, they should have a hearing test soon after the myringotomy tubes have been inserted to check that their hearing has improved. Most children have a full recovery in their hearing.
Myringotomy preprocedural tests
Pneumatic otoscopy by a physician is the primary diagnostic method for otitis media with effusion (OME) and acute otitis media (AOM). In addition, tympanometry can be performed by the audiologist to help diagnose and confirm fluid behind the eardrum. Alternatively, the ear can be examined under magnification.
Radiologic imaging and confirmatory blood chemistry studies usually are not indicated. Exceptions that benefit the patient occur if postauricular swelling or mental status changes develop or if the patient appears severely ill and toxic. In these clinical situations, computed tomography (CT) scans of the temporal bone can be done to confirm temporal bone diseases, such as mastoiditis, cholesteatoma, or a malignant process.
Unilateral effusions are less common and may indicate a nasopharyngeal mass or disease process, particularly in children older than 6 years. These circumstances mandate that a nasopharyngoscopy be performed.
Myringotomy procedure
For adult patients, the myringotomy procedure can be done in the outpatient setting with the use of phenol and topical lidocaine; young adolescents, children, and infants require brief general anesthesia.
The patient’s head is tilted slightly toward the ear opposite the one undergoing myringotomy. The operative microscope is brought into the field and focused on the external auditory meatus. An appropriately sized speculum is carefully placed into the external auditory canal, and cerumen is removed so that the entire tympanic membrane can be visualized.
Either the anteroinferior quadrant or the posteroinferior quadrant of the tympanic membrane is carefully incised with a myringotomy knife; the incision should be approximately 3-5 mm in length (see the image and the first video below). Next, a 3-mm, 5-mm, or 7-mm tube is inserted and used to release the serous or mucoid effusion 6.
Postoperatively, the patient is placed on antibiotic ear drops. In most cases, oral acetaminophen suffices for analgesia.
The patient is seen in follow-up after the procedure. Cultures taken from the time of surgery can be used to determine what antibiotics are most appropriate. Children with effusions or otitis media refractory to myringotomy alone should undergo tympanostomy tube placement in addition to myringotomy.
The tympanic membrane usually heals spontaneously. Repeat myringotomy or insertion of ear tubes may be needed if otitis persists.
Myringotomy recovery
You should be able to go home the same day.
Other than swimming, you should be able to return to normal activities after one to two days.
Regular exercise should help you to return to normal activities as soon as possible. Before you start exercising ask the healthcare team or your doctor for advice.
The myringotomy tube will fall out of your ear by itself, after 6 to 18 months depending on the material and design of the grommet.
Myringotomy complications
General surgery complications:
- Pain
- Bleeding
- Blood clots
- Anesthetic risks
- Infection
Specific complications of myringotomy:
- Fluid leaking from your ear
- Ear discharge
- Small hole left in your eardrum after the grommet falls out
- Repeated build-up of fluid in your middle ear
- Alberti PW. Myringotomy and ventilating tubes in the 19th century. Laryngoscope. 1974 May. 84(5):805-15.[↩]
- Anil Lalwani. Current diagnosis & treatment in otolaryngology–head & neck surgery. 3rd. New York: Lange Medical Books/McGraw-Hill; 2004.[↩][↩]
- Mandel EM, Rockette HE, Bluestone CD, Paradise JL, Nozza RJ. Efficacy of myringotomy with and without tympanostomy tubes for chronic otitis media with effusion. Pediatr Infect Dis J. 1992 Apr. 11(4):270-7[↩]
- Myringotomy. https://emedicine.medscape.com/article/1890977-overview[↩]
- Kenna MA. Otitis Media with Effusion. Bailey BJ JJ, Newlands SD. Head & Neck Surgery – Otolaryngology. 4th. Lippincott Williams & Wilkins; 2006.[↩]
- Isaacson G. Six Sigma tympanostomy tube insertion: achieving the highest safety levels during residency training. Otolaryngol Head Neck Surg. 2008 Sep. 139(3):353-7.[↩]




{kind=link}