
Contents
What is nephrocalcinosis
Nephrocalcinosis previous known as Anderson-Carr kidney or Albright’s calcinosis, is a disorder in which there is too much calcium deposited in the kidneys. Nephrocalcinosis is common in premature babies.
Nephrocalcinosis is divided into several types, with differing causes, based on the distribution:
- Medullary nephrocalcinosis: 95%
- Cortical nephrocalcinosis: 5%
- Partial, combined cortical and medullary nephrocalcinosis 1: rare
Radiologic detection is required to make the clinical diagnosis and nephrocalcinosis is noted in about 0.1% of radiographs of the kidney. Nephrocalcinosis is detected on microscopic analysis in about 10% of autopsies.
The natural course of nephrocalcinosis depends on the cause. Some causes such as medullary sponge kidney have a dramatic appearance on x-ray but uncommonly progression to long-term renal disease. The resolution of other causes such as hyperparathyroidism may result in the complete resolution of renal disease. Other causes, however, such as hyperoxaluria will progress to chronic renal failure over time.
Typically, the condition of nephrocalcinosis will result in a slow decline in renal function over time.
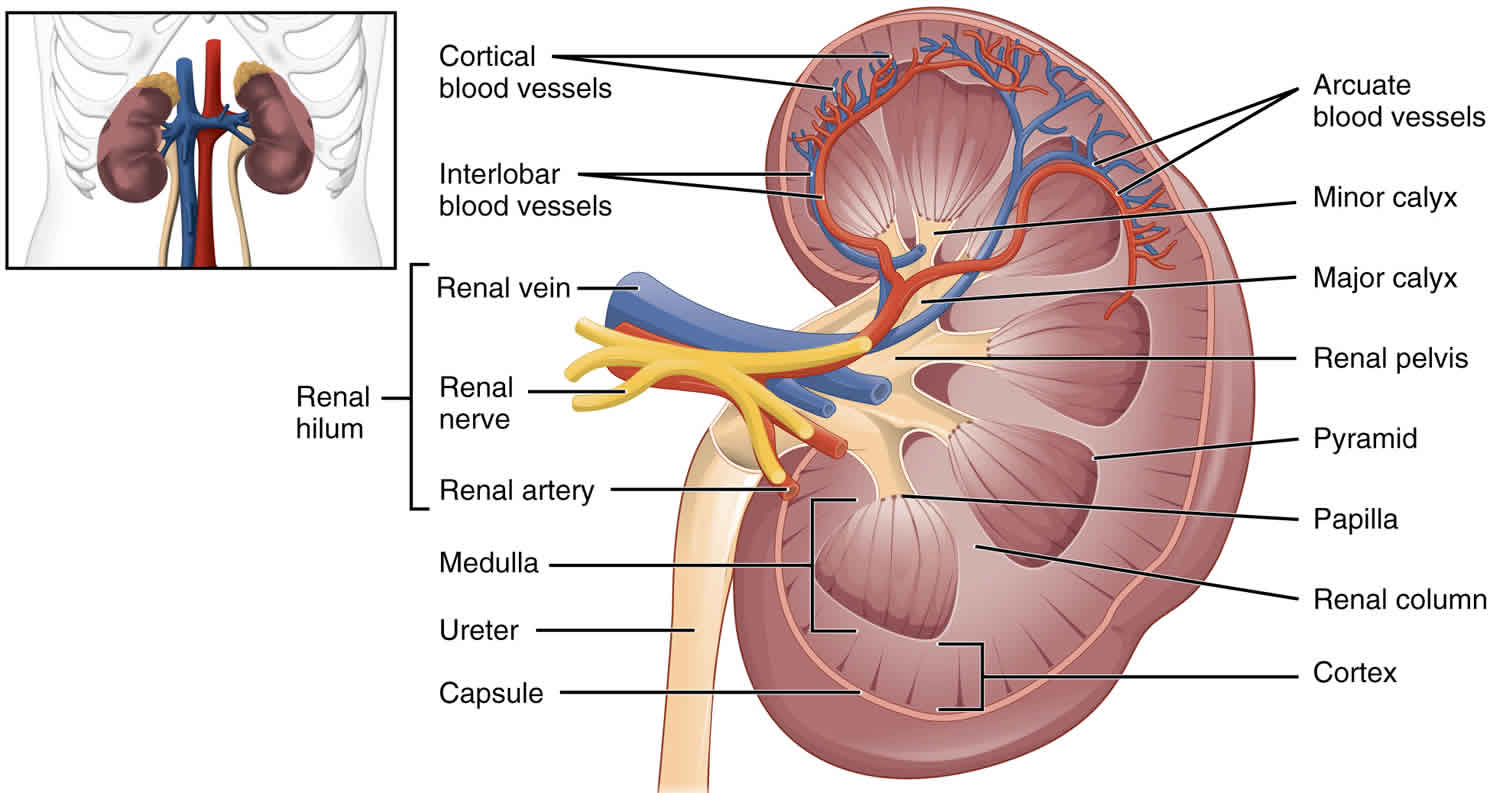
Figure 1. Kidney (normal)
Medullary nephrocalcinosis
Renal medullary nephrocalcinosis is the commonest form of nephrocalcinosis and refers to the deposition of calcium salts in the medulla of the kidney. Due to the concentrating effects of the loops of Henle, and the biochemical milieu of the medulla, compared to the cortex, it is 20 times more common than cortical nephrocalcinosis.
Often (and perhaps unsurprisingly) the same entities may also lead to nephrolithiasis (kidney stones).
Figure 2. Medullary nephrocalcinosis ultrasound
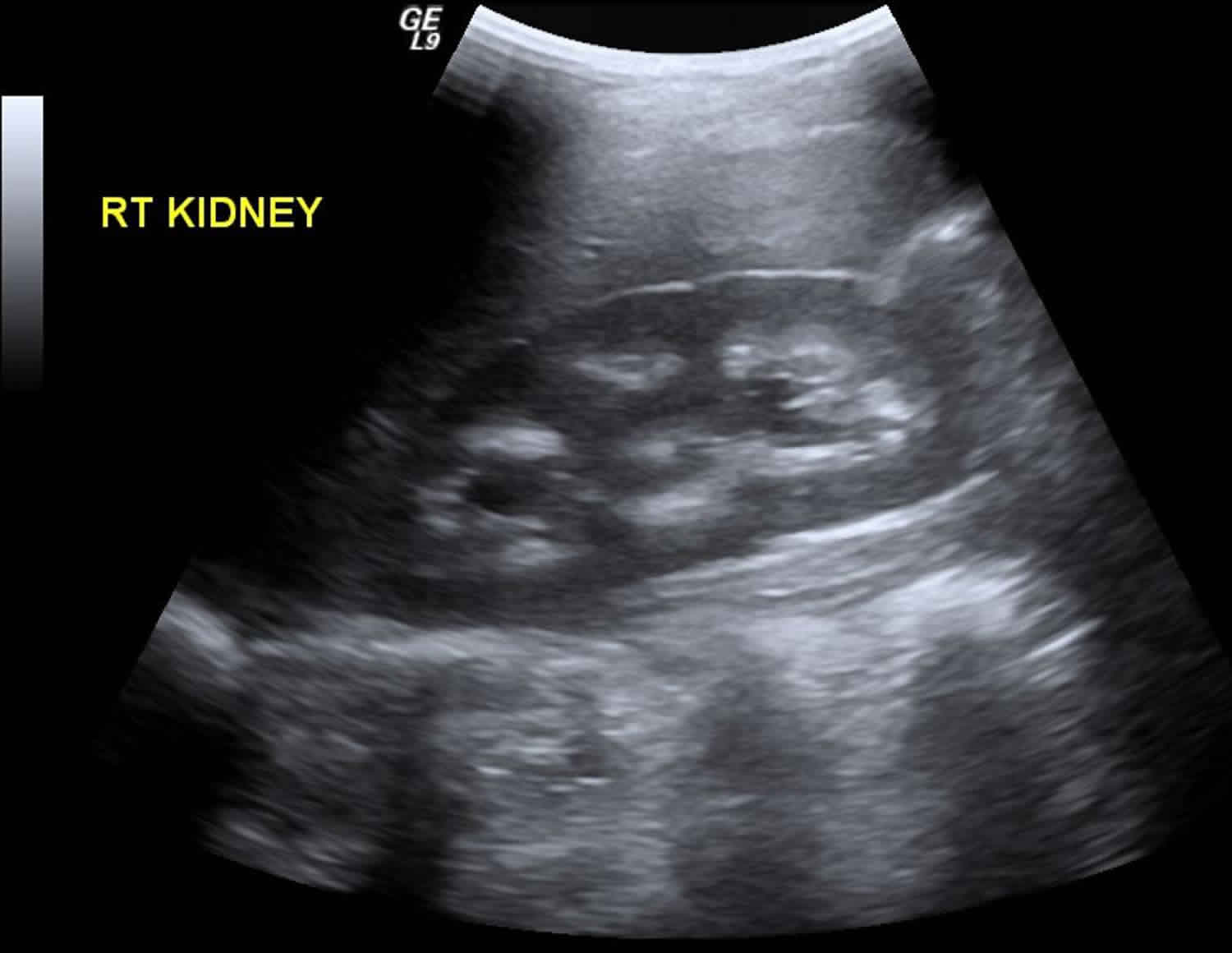
Footnote: An infant suspected to have Liddle’s syndrome, screened for nephrocalcinosis.
[Source 1 ]Medullary nephrocalcinosis causes
Medullary nephrocalcinosis causes include 2:
- Medulla
- hyperparathyroidism
- medullary sponge kidney
- renal tubular acidosis (type 1)
- hypervitaminosis D
- milk-alkali syndrome
- sarcoidosis
- hyperthyroidism or hypothyroidism 3
- other pathological hypercalcemic or hypercalciuric states
- Cushing syndrome
- multiple myeloma
- Bartter syndrome
- bone metastases
- Pyramids
- hyperuricemia
- infection (particularly renal tuberculosis)
- sickle cell disease (leading to infarction and subsequent dystrophic calcification)
- renal papillary necrosis
- drugs e.g., furosemide abuse 4
A common mnemonic used to remember the causes of medullary nephrocalcinosis is:
- HAM HOP
Mnemonic
- H: hyperparathyroidism
- A: (renal tubular) acidosis
- M: medullary sponge kidney
- H: hypercalcemia/hypercalciuria
- O: oxalosis
- P: papillary necrosis
Cortical nephrocalcinosis
Renal cortical nephrocalcinosis is ~20 times less common than medullary nephrocalcinosis.
Renal cortical nephrocalcinosis causes
Renal cortical nephrocalcinosis include:
- renal cortical necrosis: common 5
- renal infarction/ischemia
- sepsis
- toxaemia of pregnancy
- drugs
- snake bites
- arsenic poisoning
- extracorporeal shock wave lithotripsy (ESWL)
- hemolytic uremic syndrome (HUS)
- rejected renal transplant
- chronic glomerulonephritis: common 5
- Alport syndrome 6
- chronic pyelonephritis
- hyperoxaluria, or primary or secondary oxalosis
- vesicoureteral reflux (VUR)
- nephrotoxic drugs, e.g. Amphotericin B
- benign nodular cortical nephrocalcinosis
- intrarenal infection in HIV-seropositive patients
- Mycobacterium avium
- Pneumocystis carinii
- autosomal recessive polycystic kidney disease
- chronic paraneoplastic hypercalcemia 3
A handy mnemonic to recall the common causes of renal cortical nephrocalcinosis is:
- COAG
Mnemonic
- C: cortical necrosis
- O: oxalosis
- A: Alport syndrome
- G: (chronic) glomerulonephritis
Nephrocalcinosis causes
Any disorder that leads to high levels of calcium in the blood or urine may lead to nephrocalcinosis. In this disorder, calcium deposits in the kidney tissue itself. Most of the time, both kidneys are affected.
Nephrocalcinosis is related to, but not the same as, kidney stones (nephrolithiasis).
Conditions that can cause nephrocalcinosis include:
- Alport syndome
- Bartter syndrome
- Chronic glomerulonephritis
- Familial hypomagnesemia
- Medullary sponge kidney
- Primary hyperoxaluria
- Renal transplant rejection
- Renal tubular acidosis (RTA)
- Renal cortical necrosis
Other possible causes of nephrocalcinosis include:
- Ethylene glycol toxicity
- Hypercalcemia (excess calcium in the blood) due to hyperparathyroidism
- Use of certain medicines, such as acetazolamide, amphotericin B, and triamterene
- Sarcoidosis
- Tuberculosis of the kidney and infections related to AIDS
- Vitamin D toxicity
Nephrocalcinosis symptoms
Most of the time, there are no early symptoms of nephrocalcinosis. Symptoms of of nephrocalcinosis is primarily determined by the underlying cause, though in many cases, the condition remains asymptomatic and is identified only as a radiologic abnormality. The physical findings are nonspecific and reflect the underlying disorders responsible.
Clinical features of nephrocalcinosis may include the following:
- Relative vasopressin resistance with decreased renal concentrating ability and increased free water diuresis, manifesting as polyuria and polydipsia
- Renal glycosuria, reduced glucose tubular maximum, aminoaciduria, and nonglomerular proteinuria
- Reversible hypertension
- Renal failure, usually reversible but sometimes not
Clinical features of microscopic nephrocalcinosis (on the basis of animal studies) may include the following:
- Reduced concentration capacity
- Increased blood urea nitrogen (BUN)
- Prolongation of nephron transit time in the distal tubule
- Acute pyelonephritis or calculous ureteral obstruction with renal failure
Clinical features of macroscopic nephrocalcinosis (the form most commonly seen) may include the following:
- Renal colic
- Hematuria
- Passage of urinary stones
- Urinary tract infection
- Polyuria and polydipsia
- Hypertension
- Proteinuria
- In Dent disease, loss of low-molecular-weight proteins, hypercalciuria, and nephrolithiasis
- Microscopic pyuria
- Distal tubular dysfunction with a mild salt-losing defect
- Proximal tubular dysfunction (unusual)
- Secondary distal tubular acidosis
- Renal failure
People who also have kidney stones may have:
- Blood in the urine
- Fever and chills
- Nausea and vomiting
- Severe pain in the belly area, sides of the back (flank), groin, or testicles
Later symptoms related to nephrocalcinosis may be associated with long-term (chronic) kidney failure.
Nephrocalcinosis possible complications
Nephrocalcinosis complications may include:
- Acute kidney failure
- Long-term (chronic) kidney failure
- Kidney stones
- Obstructive uropathy (acute or chronic, unilateral or bilateral)
Nephrocalcinosis diagnosis
Nephrocalcinosis may be discovered when symptoms of renal insufficiency, kidney failure, obstructive uropathy, or urinary tract stones develop.
Imaging tests can help diagnose this condition. Tests that may be done include:
- Abdominal CT scan
- Ultrasound of the kidney
Other tests that may be done to diagnose and determine the severity of associated disorders include:
- Blood tests to check levels of calcium, phosphate, uric acid, and parathyroid hormone
- Urinalysis to see crystals and check for red blood cells
- 24-hour urine collection to measure acidity and levels of calcium, sodium, uric acid, oxalate, and citrate
Nephrocalcinosis treatment
The goal of treatment is to reduce symptoms and prevent more calcium from building up in the kidneys.
Treatment will involve methods to reduce abnormal levels of calcium, phosphate, and oxalate in the blood and urine. Options include making changes in your diet and taking medicines and supplements.
Pharmacologic and other nonsurgical treatments for hypercalcemia and nephrocalcinosis include the following:
- Adequate hydration with an isotonic sodium chloride solution (the single most effective measure for reversing hypercalcemia and protecting the kidneys)
- Cinacalcet (for correction of hyperparathyroidism)
- Chemotherapeutic agents (for osteolytic malignancies)
- Steroids (to decrease intestinal calcium absorption and vitamin-D activity)
- Hydroxychloroquine (for sarcoid granulomas)
- Calcitonin or bisphosphonates (to inhibit bone resorption)
Pharmacologic and other nonsurgical treatments for macroscopic nephrocalcinosis include the following:
- Thiazide diuretics (eg, hydrochlorothiazide)
- Dietary salt restriction
- Potassium and magnesium supplementation
- Citrate supplementation (preferably as potassium citrate)
- High-dose pyridoxine
Surgery options that may be considered for urinary stones causing obstruction include the following:
- Percutaneous nephrolithotomy
- Laser and shock wave lithotripsy
- Stent placement
- Open surgery (rarely necessary)
If you take medicine that causes calcium loss, your health care provider will tell you to stop taking it. Never stop taking any medicine before talking to your provider.
Other symptoms, including kidney stones, should be treated as appropriate.
Nephrocalcinosis prognosis
What to expect depends on the complications and cause of the nephrocalcinosis. Patients with idiopathic hypercalciuria and medullary sponge kidney have the least risk of renal failure and the best prognosis, whereas patients with primary type 1 hyperoxaluria have the worst prognosis 7.
The morbidity and mortality associated with nephrocalcinosis depend on the disease associated with the condition rather than on the nephrocalcinosis itself 8. The major long-term complication in patients with medullary nephrocalcinosis is renal failure. Early treatment of reversible causes of renal failure, such as urinary infections, obstruction, and hypertension, is essential. Once chronic renal failure has developed, treatment should focus on appropriate management of chronic kidney disease and its complications.
Proper treatment may help prevent further deposits in the kidneys. In most cases, there is no way to remove deposits that have already formed. Many deposits of calcium in the kidneys do NOT always mean severe damage to the kidneys.
- Medullary nephrocalcinosis. https://radiopaedia.org/cases/medullary-nephrocalcinosis-1[↩]
- Eisenberg RL, Margulis AR. The Right Imaging Study, A Guide for Physicians. Springer Verlag. (2008) ISBN:0387737731[↩]
- Wolfgang Dähnert. Radiology Review Manual. (2011) ISBN: 9781609139438[↩][↩]
- Kim YG, Kim B, Kim MK et-al. Medullary nephrocalcinosis associated with long-term furosemide abuse in adults. Nephrol. Dial. Transplant. 2002;16 (12): 2303-9[↩]
- Schepens D, Verswijvel G, Kuypers D et-al. Images in Nephrology. Renal cortical nephrocalcinosis. Nephrol. Dial. Transplant. 2000;15 (7): 1080-2. doi:10.1093/ndt/15.7.1080[↩][↩]
- Dähnert W. Radiology Review Manual. Lippincott Williams & Wilkins. (2007) ISBN:0781766206[↩]
- Tang X, Bergstralh EJ, Mehta RA, Vrtiska TJ, Milliner DS, Lieske JC. Nephrocalcinosis is a risk factor for kidney failure in primary hyperoxaluria. Kidney Int. 2015 Mar. 87 (3):623-31[↩]
- Gambaro G, Goldfarb DS, Baccaro R, Hirsch J, Topilow N, D’Alonzo S, et al. Chronic pain in medullary sponge kidney: a rare and never described clinical presentation. J Nephrol. 2018 Feb 21[↩]





{kind=link}