
Contents
- Opioid use disorder
- Opioid use disorder in pregnancy
- Opioid use disorder causes
- Opioid use disorder prevention
- Opioid use disorder symptoms
- Opioid use disorder complications
- Opioid use disorder diagnosis
- Opioid use disorder treatment
- Opioid use disorder prognosis
Opioid use disorder
Opioid use disorder also known as opioid abuse and addiction, is a problematic pattern of opioid use that causes significant dependence, addiction, tolerance and craving leading to an inability to control the use of a legal or illegal opioid despite adverse consequences 1, 2. Opioids, also called narcotics, are a class of drugs produced from opium that include the illegal drug heroin, synthetic opioids such as fentanyl, and pain medications available legally by prescription, such as oxycodone (OxyContin), hydrocodone (Vicodin), codeine, morphine, tramadol, hydrocodone, hydromorphone, meperidine and many others 3. Opioid abuse means you are not taking the opioid medicines according to your doctor’s instructions, you are using opioids to get high, or you are taking someone else’s opioids. Addiction is a chronic brain disease. Addiction causes you to compulsively seek out drugs even though they cause you harm 4. People with addiction cannot face daily life without drugs; denies problem; physical condition gets worse; loss of “control” over use; may become suicidal; financial and legal problems get worse; may have broken ties with family members or friends.
These are prescription opioids and some of their common brand names. A brand name is the name given to a product by the company that makes it.
- Buprenorphine (Belbuca®, Buprenex®, Butrans®, Probuphine®)
- Codeine
- Fentanyl (Actiq®, Duragesic®, Sublimaze®)
- Hydrocodone (Lorcet®, Lortab®, Norco®, Vicodin®)
- Hydromophone (Dalaudid®, Exalgo®)
- Meperidine (Demerol®)
- Methadone (Dolophine®, Methadose®)
- Morphine (Astramorph®, Avinza®, Duramorph®, Roxanol®)
- Oxycodone (OxyContin®, Percodan®, Percocet®)
- Oxymorphone (Opana®)
- Tramadol (ConZip®, Ryzolt®, Ultram®)
The illegal drug heroin is an opioid. Fentanyl and other prescription opioids are being made and sold illegally. When used illegally, fentanyl sold on the street often is mixed with heroin or cocaine, which makes it extremely dangerous.
According to the 2020 National Survey on Drug Use and Health, 9.5 million people age 12 or older had misused opioids in the past year, and 2.7 million people had an opioid use disorder including 2.3 million people with a prescription opioid use disorder 5. The majority of opioids in use are prescribed, but many are obtained illegally. According to the CDC, there were more than 191 million opioid prescriptions prescribed from 2012 to 2017. Opioid use disorder can even lead to overdose and death. Overdose deaths involving opioids have dramatically increased over the previous decade to 80,411 deaths in 2021 6. Besides opioid overdose, consequences of the opioid crisis include a rising incidence of infants born dependent on opioids because their mothers used these substances during pregnancy 7, 8 and increased spread of infectious diseases, including HIV and hepatitis C (HCV), as was seen in 2015 in southern Indiana 9.
A doctor may give you a prescription opioid to reduce pain after you have had a major injury or surgery. You may get opioid if you have severe pain from health conditions like cancer. Some doctors prescribe opioid for chronic pain. It may be hard for some people to stop using opioids because along with relieving pain, opioids release chemicals in your brain that can make you feel calm and intensely happy (also called euphoria). Drug addiction is a brain condition that makes you use drugs, even if they’re harmful to you. Addiction affects your self-control and your ability to stop taking a drug. Most people who take prescription opioids can stop using them without getting addicted to them. But using them regularly can make you dependent on them, even if you use them as directed by your doctor.
Opioid use disorder is a pattern of opioid use that makes it hard for you to stop using them, even when it causes problems in your life. You may have an opioid use disorder if you:
- Take more opioids than your provider says you can take
- Have cravings (a strong desire) for opioids
- Feel like you can’t stop taking opioids
- Need more opioids to get the same effect
- Have problems at home, work or school caused by taking opioids
- Spend time and effort trying to get opioids
- Feel sick when you stop using opioids or reduce the amount you take
A diagnosis of opioid use disorder is based on specific criteria such as unsuccessful efforts to cut down or control use or use resulting in a failure to fulfill obligations at work, school, or home, among other criteria.
Opioid Use Disorder DSM-5 Diagnostic Criteria 10, 11:
- Taking opioids in larger amounts or over a longer period of time than intended
- Having a persistent desire or unsuccessful attempts to reduce or control opioid use
- Spending excess time obtaining, using, or recovering from opioids
- Craving opioids
- Continued opioid use causing inability to fulfill work, home, or school responsibilities
- Continuing opioid use despite having persistent social or interpersonal problems
- Lack of involvement in social, occupational, or recreational activities
- Using opioids in physically hazardous situations
- Continuing opioid use in spite of awareness of persistent physical or psychological problems
- Exhibiting tolerance symptoms, as defined by either of the following:*
- A need for markedly increased amounts of opioids to achieve intoxication or desired effect, or
- Markedly diminished effect with continued use of the same amount of an opioid.
- Exhibiting withdrawal symptoms, as manifested by either of the following:*
- The characteristic opioid withdrawal syndrome, or
- Opioids (or a closely related substance) are taken to relieve or avoid withdrawal symptoms.
Note: * Tolerance and withdrawal are not considered to be met for those taking opioids solely under appropriate medical supervision.
To confirm a diagnosis of opioid use disorder, at least 2 out of 11 defined criteria should be observed within a 12-month period.
Severity of opioid use disorder is determined based on the number of criteria met.
- Mild: 2-3 criteria
- Moderate: 4-5 criteria
- Severe: greater than or equal 6 criteria
The good news is opioid use disorder is a treatable condition. The main treatment for prescription opioid addiction includes medicines, counseling, and support from family and friends. Medication-assisted treatment can help you stop using the drug, get through withdrawal, and cope with cravings. There is also a medicine called naloxone (brand name Narcan) which can reverse the effects of an opioid overdose and prevent death, if it is given in time. Naloxone is a medicine that rapidly reverses an opioid overdose. Naloxone is administered when a patient is showing signs of opioid overdose. However naloxone only reverses opioids overdose in people with opioids in their systems and will not reverse overdoses from other drugs like cocaine or methamphetamine. Naloxone can be given by intranasal spray (into the nose), intramuscular (into the muscle), subcutaneous (under the skin), or intravenous injection. Naloxone is an opioid antagonist, which means that it blocks opioid receptors from being activated and can reverse and block the effects of other opioids, such as heroin, morphine, and oxycodone. Naloxone knocks opioids off their receptors all around the body. In the brainstem, naloxone can restore the drive to breathe. And save a life. However, naloxone is a temporary treatment and its effects do not last long. Naloxone works to reverse opioid overdose in the body for only 30 to 90 minutes. Because of this, it is possible for a person to still experience the effects of an opioid overdose after a dose of naloxone wears off. Also, some opioids are stronger and might require multiple doses of naloxone. Therefore, one of the most important steps to take is to call your local emergency services number so the individual can receive immediate medical attention as soon as possible after administering or receiving naloxone. People who are given naloxone should be observed constantly until emergency care arrives. They should be monitored for another 2 hours after the last dose of naloxone is given to make sure their breathing does not slow or stop. Naloxone may promote opioid withdrawal because it knocks opioids off their receptors so quickly. But otherwise naloxone is safe and unlikely to produce side effects. People with physical dependence on opioids may have withdrawal symptoms within minutes after they are given naloxone. Withdrawal symptoms might include headaches, changes in blood pressure, rapid heart rate, sweating, nausea, vomiting, and tremors. While this is uncomfortable, it is usually not life threatening. The risk of death for someone overdosing on opioids is worse than the risk of having a bad reaction to naloxone. Clinicians in emergency room settings are being trained to offer patients immediate relief and referral to treatment for opioid use disorder with effective medications after an opioid overdose is reversed.
The U.S. Food and Drug Administration (FDA) approved opioid use disorder medications for the treatment of opioid use disorder include buprenorphine (often combined with naloxone), methadone, and naltrexone.
- Buprenorphine
- Partial mu-opioid receptor agonist.
- Suppresses and reduces cravings for opioids.
- Can be prescribed by any clinician with a current, standard Drug Enforcement Agency (DEA) registration with Schedule 3 authority, in any clinical setting.
- The following buprenorphine products are FDA approved for the treatment of opioid use disorder:
- Generic Buprenorphine/naloxone sublingual tablets
- Buprenorphine sublingual tablets (Subutex)
- Buprenorphine/naloxone sublingual films (Suboxone)
- Buprenorphine/naloxone) sublingual tablets (Zubsolv)
- Buprenorphine/naloxone buccal film (Bunavail)
- Buprenorphine implants (Probuphine)
- Buprenorphine extended-release injection (Sublocade)
- Methadone
- Full mu-opioid receptor agonist.
- Reduces opioid cravings and withdrawal and blunts or blocks the effects of opioids.
- Can only be provided for opioid use disorder through a Substance Abuse and Mental Health Services Administration (SAMHSA)-certified opioid treatment program (https://dpt2.samhsa.gov/treatment/directory.aspx)
- Naltrexone
- Opioid receptor antagonist.
- Blocks the euphoric and sedative effects of opioids and prevents feelings of euphoria.
- Should be started after a minimum of 7 to 10 days free of opioids to avoid precipitation of severe opioid withdrawal.
- Can be prescribed by any clinician with an active license to prescribe medications.
Methadone and buprenorphine are the most widely used medications for the treatment of opioid use disorder in the United States 12. Compared with naltrexone, the evidence base is stronger for the use of methadone and buprenorphine in the treatment of opioid use disorder 13, 14, 15. Another potential disadvantage of naltrexone is that patients must be opioid free for 7 to 10 days prior to treatment initiation, which is not the case for methadone or buprenorphine 16, 17.
A large body of research have demonstrated the effectiveness of medication for treatment of opioid use disorder 18, 19, 20, 13, 21, 22, 23. Opioid use disorder medications used in conjunction with psychosocial therapy are considered the gold standard in care for the treatment of opioid use disorder 24, 18, 21, 22. Opioid use disorder treatment medications are associated with reductions in opioid use, withdrawal, craving, and treatment dropout 21, 22, 24, 19, 25. A recent report by the National Academies of Sciences, Engineering, and Medicine concluded that “a lack of availability or utilization of behavioral interventions is not a sufficient justification to withhold medications to treat opioid use disorder” 26. This statement reflects mounting support for the use of medications in the absence of psychosocial therapy 12.
People struggling with addiction usually deny they have a problem and hesitate to seek treatment. If your drug use is out of control or causing problems, get help. The sooner you seek help, the greater your chances for a long-term recovery. Talk with your doctor or see a mental health professional, such as a doctor who specializes in addiction medicine or addiction psychiatry, or a licensed alcohol and drug counselor.
Make an appointment to see a a doctor or mental health professional if:
- You can’t stop using a drug
- You continue using the drug despite the harm it causes
- Your drug use has led to unsafe behavior, such as sharing needles or unprotected sex
- You think you may be having withdrawal symptoms after stopping drug use
If you’re not ready to approach a doctor or mental health professional, help lines or hotlines may be a good place to learn about treatment. You can find these lines listed on the internet or in the phone book.
Opioid use disorder in pregnancy
Opioid use disorder during pregnancy can cause serious problems for you and your baby. Opioid use disorder in pregnancy can even cause death in a pregnant mother. If you have an opioid use disorder, you may have trouble taking care of yourself during pregnancy. Opioid use disorder may also increase the risk of problems such as 27, 28, 29, 30, 31, 32, 1, 33:
- Birth defects in your baby. Birth defects are health conditions that are present at birth include those that affect your baby’s heart, belly, eyes, brain, spine and spinal cord. Birth defects change the shape or function of one or more parts of the body. Birth defects can cause problems in overall health, how the body develops or how the body works. Birth defects associated with opioid use during pregnancy include:
- Congenital heart defects. These conditions can affect the shape of a baby’s heart, how it works or both.
- Gastroschesis. This is a birth defect of a baby’s belly in which the intestines stick outside the body through a hole beside the belly button.
- Glaucoma. This is a group of eye conditions that damage the optic nerve. If untreated, glaucoma can cause blindness.
- Neural tube defects. These are birth defects of the brain, spine and spinal cord. Spina bifida is the most common neural tube defect.
- Neonatal abstinence syndrome (NAS). This is a group of conditions caused when a baby withdraws from certain drugs he’s exposed to in the womb (uterus) before birth.
- Neonatal abstinence syndrome (NAS) is when a baby is exposed to a drug in the womb before birth and goes through withdrawal from the drug after birth. Neonatal abstinence syndrome (NAS) is most often caused when a woman takes opioids during pregnancy. Neonatal abstinence syndrome (NAS) can cause serious problems for a baby, like being born too small and having breathing problems. Even if you use an opioid exactly as your health care provider tells you to, it may cause neonatal abstinence syndrome (NAS) in your baby. So tell your prenatal care provider about any opioid you take, even if it’s prescribed to you by another health care provider. If another health care provider prescribes you an opioid, make sure she knows you’re pregnant.
- Withdrawal among newborns during the first 28 days of life due to long-term exposure to opioids before birth is called neonatal opioid withdrawal syndrome (NOWS). Opioids given at the time of delivery do not cause neonatal opioid withdrawal syndrome (NOWS) 34. Neonatal opioid withdrawal syndrome (NOWS) is under the neonatal abstinence syndrome (NAS) umbrella and specific to opioid use.
- Problems with the placenta. The placenta grows in your uterus and supplies the baby with food and oxygen through the umbilical cord.
- Placental abruption is a serious condition in which the placenta separates from the wall of the uterus (womb) before birth. If this happens, your baby may not get enough oxygen and nutrients in the womb. And you may have serious bleeding.
- Problems with your baby’s growth. These include:
- Fetal growth restriction also called growth-restricted, small for gestational age and small for date. This is when a baby doesn’t gain the weight she should before birth.
- Low birthweight. This is when a baby is born weighing less than 5 pounds, 8 ounces.
- Preterm labor and premature birth. This is labor and birth that happen too early, before 37 weeks of pregnancy. Babies born this early may have more health problems at birth and later in life than babies born full term. Opioids also can cause premature rupture of membranes (also called PROM). This is when the sac around a baby breaks before a woman goes into labor.
- Miscarriage or stillbirth
- Miscarriage is the death of a baby in the womb before 20 weeks of pregnancy.
- Stillbirth is the death of a baby in the womb after 20 weeks of pregnancy.
- Sudden infant death syndrome (SIDS). This is the unexplained death of a baby younger than 1 year old. Sudden infant death syndrome (SIDS) usually happens when a baby is sleeping. Babies born to mothers who use opioids are at increased risk for SIDS.
- Fetal convulsions
- Fetal death
- Maternal death
Other indirect risks to the fetus include 28, 29, 30, 31:
- increased risk for maternal infection (e.g., human immunodeficiency virus (HIV), hepatitis B Virus (HBV), hepatitis C Virus (HCV)
- malnutrition and poor prenatal care
- dangers from drug seeking (e.g., violence and incarceration)
The effects of prenatal opioid exposure on children over time are largely unknown, including among those with or without neonatal abstinence syndrome (NAS) 35. Not all babies exposed to opioids during pregnancy experience signs of neonatal abstinence syndrome (NAS), but there could be long-term effects on development that aren’t obvious at birth 35. More research is needed to better understand the spectrum of possible outcomes related to opioid exposure during pregnancy.
Experts think that neonatal abstinence syndrome (NAS) may cause long-term problems for your baby, like 36:
- Developmental delays. Developmental delays are when your child doesn’t reach developmental milestones when expected. Developmental milestones are skills and activities that most children can do at a certain age, like sitting, walking, talking, having social skills and having thinking skills.
- Motor problems. These are problems with your baby’s bones, muscles and movement.
- Behavior and learning problems. Babies with neonatal abstinence syndrome (NAS) are more likely than babies who don’t have NAS to be checked for learning problems and to get special education services in school.
- Speech and language problems
- Sleep problems
- Ear infections
- Vision problems
Taking medication for opioid use disorder as prescribed during pregnancy has benefits that outweigh the risks 35. It is important for healthcare providers and pregnant women to work together to manage medical care, including substance use, during pregnancy and after delivery. Pregnant mothers should consult their physician before stopping or changing any prescribed medication.
If you have opioid use disorder and you share needles with other drug users, you’re at risk for infections like hepatitis and human immunodeficiency virus (HIV). Hepatitis is a virus that attacks the liver. Human immunodeficiency virus (HIV) attacks your immune system that usually helps protect you from infections. You can pass infections like these to your baby during pregnancy.
If you have opioid use disorder, you may have trouble taking care of yourself during pregnancy. For example, you may miss your prenatal care checkups and not make healthy choices for you and your baby. You’re also at risk for overdose and for mental health conditions, like depression. Depression is a medical condition that causes feelings of sadness and a loss of interest in things you like to do. It can affect how you feel, think and act and can interfere with your daily life. It needs treatment to get better.
Can opioids cause problems during pregnancy and after birth?
Yes. Using opioids during pregnancy can affect your health and your baby’s health. If you’re not pregnant and you’re using opioids, use effective birth control until you’re ready to get pregnant. This can help prevent complications when you do get pregnant.
Is it safe to suddenly quit taking opioids during pregnancy?
No. Quitting suddenly also called going cold turkey during pregnancy can cause severe problems for your baby, including death. If you’re pregnant and taking opioids, don’t go cold turkey. Talk to your doctor about safe ways to stop taking opioids.
What can I do to help prevent neonatal abstinence syndrome (NAS) in my baby?
Here’s what you can do:
- If you’re pregnant and you use any of the drugs that can cause neonatal abstinence syndrome (NAS), tell your doctor right away, but don’t stop taking the drug without getting treatment from your provider first. Quitting suddenly (sometimes called cold turkey) can cause severe problems for your baby, including death. If you need help to quit using these drugs, talk to your doctor about treatment. Getting treatment can help you stop using drugs and is safer for your baby than getting no treatment at all.
- If you’re pregnant and can’t stop using opioids without problems, ask your doctor about medication-assisted treatment (MAT). Neonatal abstinence syndrome (NAS) in babies may be easier to treat for babies whose moms get medication-assisted treatment (MAT) during pregnancy. Medicines used in medication-assisted treatment (MAT) include methadone and buprenorphine.
- If you’re pregnant and you go to a doctor who prescribes medicine to treat a health condition, make sure that doctor knows you’re pregnant. You may need to stop taking certain medicines or change to medicine that’s safer for your baby. Ask all your doctors if the medicine you take—even prescription drugs—can cause neonatal abstinence syndrome (NAS) in your baby. Even if you use a prescription drug exactly as your doctor tells you to, it may cause neonatal abstinence syndrome (NAS) in your baby.
- If you’re pregnant or thinking about getting pregnant, tell your doctor about any drugs or medicine you take. Your doctor can make sure that what you’re taking is safe for you and your baby. She also can help you get treatment for using street drugs or abusing prescription drugs if you need it. If you abuse prescription drugs, it means you take more than has been prescribed for you, you take someone else’s prescription drug, or you get the drug from someone without a prescription.
- If you’re not pregnant and you use any drug that can cause neonatal abstinence syndrome (NAS): Use birth control until you’re ready to get pregnant. Birth control also called contraception or family planning helps keep you from getting pregnant. Examples include intrauterine devices (also called IUDs), implants, the pill and condoms.
Opioid use disorder in pregnancy treatment
Treatment for opioid use disorder during pregnancy may include opioid replacement therapy, medication-assisted therapy (MAT) or opioid-assisted therapy. The American College of Obstetricians and Gynecologists 1 and the Substance Abuse and Mental Health Services Administration 37 recommend treatment with long-acting opioids, like methadone or buprenorphine, for pregnant women with opioid use disorder, in conjunction with behavioral therapy and medical services. Long-acting opioids means the opioids stay in your body for a long time. Some treatment centers use naltrexone to treat opioid use disorder in pregnant women, however, current information on its safety during pregnancy is limited. Methadone and buprenorphine help reduce your need for opioids in a way that’s safe for you and your baby. Methadone and buprenorphine don’t make you feel happy or calm the way some opioids do. These medicines can help reduce your baby’s risk for premature birth and growth problems. Your baby may have some opioid withdrawal symptoms or neonatal abstinence syndrome (NAS) after birth. A concern for neonatal abstinence syndrome (NAS) alone should not deter healthcare providers from prescribing methadone or buprenorphine. A close collaboration with your pediatric care team can help ensure that your baby are monitored for neonatal abstinence syndrome (NAS) and receive appropriate treatment, as well as be referred to needed services.
The American College of Obstetricians and Gynecologists 1 recommends that if a woman is stable on naltrexone prior to pregnancy, the decision regarding whether to continue naltrexone treatment during pregnancy should involve a careful discussion between the doctor and the patient, weighing the limited safety data on naltrexone with the potential risk of relapse with discontinuation of treatment.
Both methadone and buprenorphine treatment during pregnancy:
- stabilize fetal levels of opioids, reducing repeated prenatal withdrawal 27, 38
- improve neonatal outcomes 33
- increase maternal HIV treatment to reduce the likelihood of transmitting the virus to the fetus 33, 1
- link mothers to better prenatal care 33, 1
A meta-analysis showed that, compared to single-dose methadone treatment, buprenorphine resulted in 39, 40:
- 10 percent lower incidence of neonatal abstinence syndrome (NAS)
- shorter neonatal treatment time (an average of 8.4 days shorter)
- lower amount of morphine used for neonatal abstinence syndrome (NAS) treatment (an average of 3.6 mg lower)
- higher gestational age, weight, and head circumference at birth
Data from the National Institute on Drug Abuse-funded Maternal Opioid Treatment: Human Experimental Research (MOTHER) study show similar benefits of buprenorphine 41. Still, methadone is associated with higher treatment retention than buprenorphine 39. Divided dosing with methadone has been explored as a way to reduce fetal exposure to withdrawal periods, and recent data show low levels of neonatal abstinence syndrome (NAS) in babies born to mothers treated with divided doses of methadone 42. Larger comparison studies are needed to determine if split methadone dosing for opioid use disorders in pregnancy is associated with better outcomes.
Neonatal abstinence syndrome (NAS) still occurs in babies whose mothers have received buprenorphine or methadone, but it is less severe than it would be in the absence of treatment 43. Research does not support reducing maternal methadone dose to avoid neonatal abstinence syndrome (NAS), as this may promote increased illicit drug use, resulting in increased risk to the fetus 27.
If you’re in medication-assisted therapy (MAT), which includes medicines, counseling, and behavioral therapies, talk to your doctor about a medicine called naloxone (Narcan). Naloxone helps stop the harmful effects of opioids, and it can save your life if you have an opioid overdose. With your doctor’s OK, it’s safe to use during pregnancy in small doses. Your doctor may prescribe it as a nasal spray or a shot. If you’re using naloxone, keep it with you at all times. Your doctor can show you and your family how to use it if you have signs or symptoms of an opioid overdose.
Behavioral therapy also called counseling. Your doctor may recommend that you meet with a counselor by yourself, with a group or both. Counseling can help you change your feelings about drugs and help you develop healthy life skills. It also helps you learn how to avoid or manage situations that may make you likely to relapse. Relapse is when you go back to using a drug after trying to quit using it. People who get drug counseling are less likely to relapse than people who don’t get counseling.
According to American College of Obstetricians and Gynecologists 1 and Substance Abuse and Mental Health Services Administration 37, people with opioid use disorder should continue medication for opioid use disorder as prescribed after the baby is born. Healthcare providers should monitor mothers during this time and adjust the dosage if needed. Discontinuation of medication for opioid use disorder should generally be avoided in the time immediately after the baby is born. At the very least, it should be avoided until the baby is consistently sleeping through the night and has completed breastfeeding. However, ending medication for opioid use disorder later may be considered if the mother is stable, if the mother and child are well-bonded, if the mother and child have a safe and stable home and social environment, and only with medical supervision and when it is in the best interest of the mother and child.
Plans to stop medication for opioid use disorder should be made together with the healthcare team 44. Medication for opioid use disorder must be reduced slowly to prevent withdrawal. A safety plan for the mother and family needs to be in place before slowly stopping medication for opioid use disorder, so that plans are in place if opioid relapse occurs. Mothers can safely continue medication for opioid use disorder for as long as they need it. For some, this may be months or years, and for others, it may be a lifetime 44.
In general, breastfeeding is encouraged for newborns with neonatal abstinence syndrome (NAS), as studies have found that breastfeeding can reduce length of hospital stay and need for morphine treatment in infants. However, sometimes breastfeeding is not recommended. For example, breastfeeding is not recommended if mothers are using illicit drugs, are using more than one drug, or are HIV-positive 44.
Neonatal abstinence syndrome (NAS)
Neonatal Abstinence Syndrome (NAS) is a group of conditions caused when a baby withdraws from certain drugs he’s exposed to in the womb before birth. Neonatal Abstinence Syndrome (NAS) is most often caused when a woman takes opioids during pregnancy. But it can also be caused by antidepressants (used to treat depression), barbiturates or benzodiazepines (sleeping pills). When you take these drugs during pregnancy, they can pass through the placenta and cause serious problems for your baby. The placenta grows in your uterus (womb) and supplies your baby with food and oxygen through the umbilical cord.
Signs of neonatal abstinence syndrome (NAS) usually begin within 72 hours after birth and may include the following:
- Tremors (trembling), seizures (convulsions), overactive reflexes (twitching) and tight muscle tone
- Irritability, including excessive crying or high-pitched crying
- Breathing problems, including breathing really fast
- Sleep problems
- Hyperactive reflexes
- Fever, sweating or blotchy skin
- Trouble sleeping and lots of yawning
- Stuffy nose or sneezing
- Poor feeding and sucking or slow weight gain
- Vomiting
- Loose stools and dehydration
- Increased sweating
The signs a newborn might experience, and how severe the signs will be, depend on different factors. Some factors include the type and amount of substance the newborn was exposed to before birth, the last time a substance was used, whether the baby is born full-term or premature, and if the newborn was exposed to other substances (e.g., alcohol, tobacco, other medications) before birth 45, 46, 47, 48.
Your baby’s doctor can use these tests to see if your baby has neonatal abstinence syndrome (NAS):
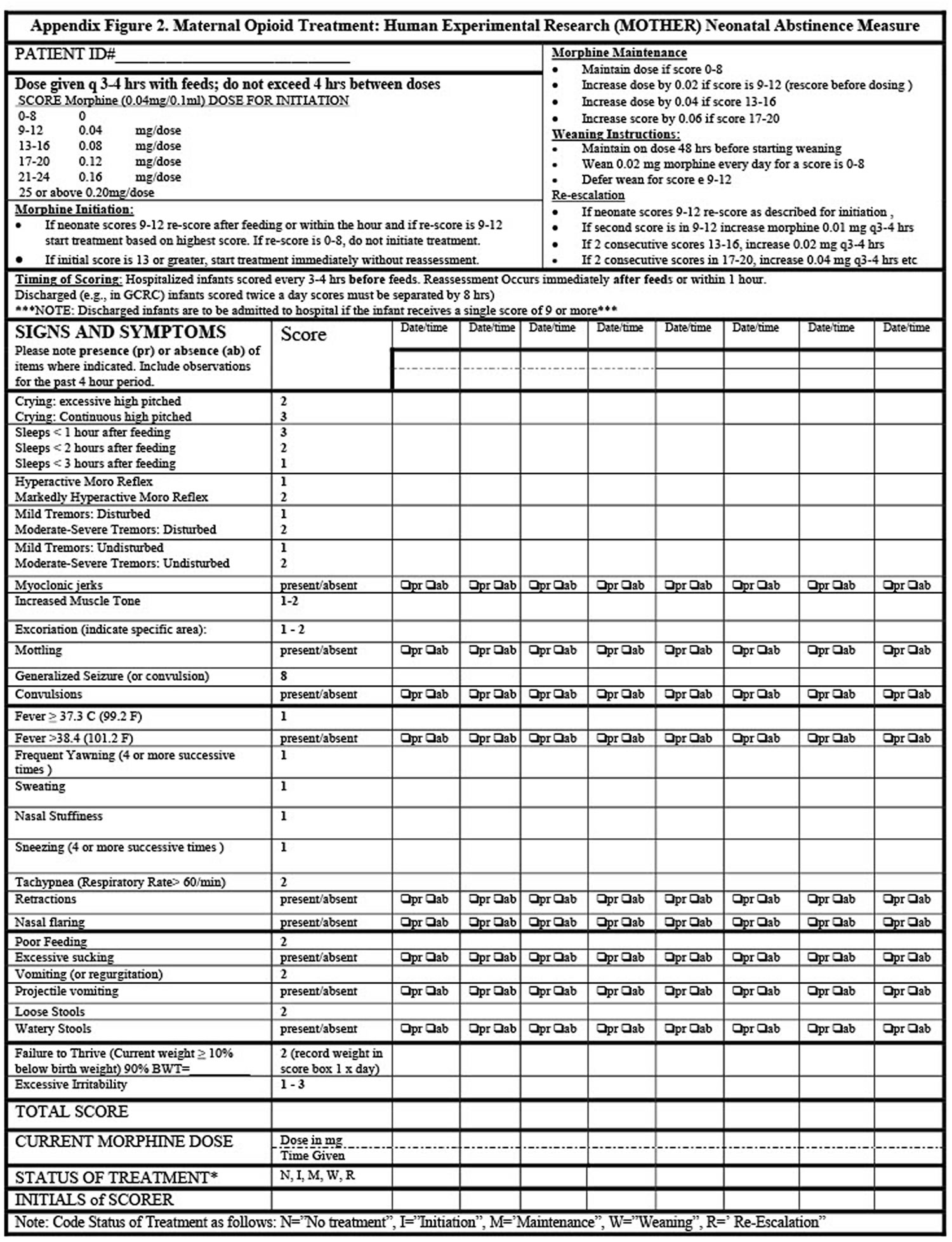
- Neonatal abstinence syndrome (NAS) scoring system (Figure 1). With this system, your baby’s provider uses points to grade how severe your baby’s withdrawal is. Your baby’s provider uses the score to decide what kind of treatment your baby needs.
- Urine and meconium tests to check for drugs. Meconium is your baby’s first bowel movement.
In the 1970s, several scoring systems were developed to guide the diagnosis and treatment of neonatal abstinence syndrome (NAS) 49, 50. Still today, however, there is not one agreed-on neonatal abstinence syndrome (NAS) scoring tool, and each scoring tool is prone to challenges of interrater reliability because each contains clinical signs that can be subjective or related to infant adaptation to extrauterine life 34. The most commonly used scoring tool in the United States today is a modification of the original Finnegan score, developed in the early 1970s by Dr Loretta Finnegan 49, 51. Another commonly used score is a Finnegan scale modification created from the Maternal Opioid Treatment: Human Experimental Research (MOTHER) Neonatal Abstinence Measure trial (Figure 1) 41. Similar to other tools, the MOTHER modification includes common central nervous system, gastrointestinal tract, and autonomic clinical signs. Clinical signs are weighted to reflect severity; for example, sleeping <1 hour after feeding reflects a score of 3, whereas sleeping <3 hours after feeding reflects a score of 1. The score is used for initiation, advancement, and weaning of pharmacotherapy for neonatal opioid withdrawal syndrome on the basis of severity. The MOTHER modification suggests initiating pharmacotherapy if there is a consistent score of 9 to 12 or a single score of 13 34.
Figure 1. Neonatal Abstinence Score
Neonatal abstinence syndrome treatment
Treatment for neonatal abstinence syndrome (NAS) depends on many factors 44, 34:
- The opioids or other medicines the newborn was exposed to during pregnancy;
- The your baby’s overall health; and
- Whether your baby was born full-term (after 37 weeks of pregnancy).
Initial treatment of infants showing signs of neonatal opioid withdrawal syndrome is focused on supportive care that involves and supports the mother is very important.
Other strategies for managing neonatal abstinence syndrome (NAS) include 44:
- Placing the infant in a dark, quiet area to lessen both light and sound;
- Swaddling the infant;
- Gently rocking the infant or using other positioning or comforting methods;
- Providing frequent, small amounts of high-calorie formula or breast milk to help with feeding problems;
- Getting fluids through a needle into a vein (also called intravenous or IV) to prevent your baby from getting dehydrated. Dehydrated means not having enough water in the body. Babies with neonatal abstinence syndrome (NAS) can get dehydrated from having diarrhea or vomiting a lot.
- Allowing the infant to stay in the same hospital room as the mother.
Some babies, especially those with more severe withdrawal symptoms, may need medications, such as liquid oral morphine or liquid oral methadone in smaller doses so your baby’s body can adjust to being off opioid, in addition to the other care strategies listed above that do not include the use of medicines 37.
Most babies with neonatal abstinence syndrome (NAS) who get treatment get better in 5 to 30 days.
During treatment for neonatal abstinence syndrome (NAS), your baby may be fussy and hard to soothe. Doing these things can help calm your baby:
- Room in with your baby. This means you and your baby stay in the same room together at the hospital before you take your baby home.
- Give your baby skin-to-skin care (also called kangaroo care). This is when you put your baby, dressed only in a diaper, on your bare chest.
- Be gentle with your baby. Rock your baby gently. If she’s sleeping, don’t wake her up.
- Swaddle your baby (wrap him snuggly) in a blanket.
- Keep your baby’s room quiet and the lights dim.
- Breastfeed your baby. Feed your baby on demand. This means you feed your baby when he’s hungry.
- Give your baby a pacifier.
Your baby’s doctor checks your baby often in the neonatal intensive care unit (NICU) after birth to make sure he’s getting better and having fewer and less severe withdrawal signs.
Your baby can go home from the hospital when she:
- Is feeding well
- Is sleeping well
- Is gaining weight
- Has a good neonatal abstinence syndrome (NAS) score
The discharge plan for infants treated for neonatal abstinence syndrome (NAS) may include home visits and services, such as parenting support and links to home nurses and social workers 44. The plan may also include referrals to healthcare workers who know about neonatal abstinence syndrome (NAS) and are available to the family immediately after discharge. The American Academy of Pediatrics recommends this simple Discharge Checklist for Infants With Opioid Exposure to help with discharge planning and proper care after leaving the hospital 34:
Discharge Checklist for Infants With Opioid Exposure (Completed (Check Yes))
- Task
- No significant clinical signs of withdrawal for 24–48 hours
- Parent education about Neonatal Opioid Withdrawal Syndrome (NOWS) and routine newborn care, emphasizing safe sleep
- Pediatrician or primary care provider follow-up visit scheduled within 48 hour of discharge
- Early intervention services referral. Early Head Start programs can be identified by using the Center Locator (https://eclkc.ohs.acf.hhs.gov/center-locator).
- Home-nurse visitation referral
- Hepatitis C testing follow-up, including referral to pediatric infectious disease when appropriate
- Plan of safe care, coordinating with child welfare as appropriate
- Developmental-behavioral pediatrician referral as appropriate
After your baby is home, take her to all of her follow-up and well-baby checkups, even if she’s doing well. Your baby’s doctor checks your baby at these visits for problems that may be linked to neonatal abstinence syndrome (NAS), like:
- Developmental delays and problems with motor and learning skills and behavior
- Problems with nutrition and growth
- Problems with hearing and vision
- Problems at home, including using harmful substances. This can include misusing prescription drugs and using illegal drugs.
If your baby has developmental delays, talk to your doctor about early intervention services. These services can help children from birth through 3 years old learn important skills. Services include therapy to help a child talk, walk, learn self-help skills and interact with others. Getting services as early as possible can help improve your child’s development.
Opioid use disorder causes
Like many mental health disorders, several factors may contribute to development of opiate use disorder. The main factors are 52, 53:
- Environmental factors. Environmental factors, including your family’s beliefs and attitudes and exposure to a peer group that encourages drug use, seem to play a role in initial drug use.
- Genetics. Once you’ve started using a drug, the development into addiction may be influenced by inherited (genetic) traits, which may delay or speed up the disease progression.
- Psychosocial factors.
- Changes in the brain. Physical addiction appears to occur when repeated use of a drug changes the way your brain feels pleasure. The addicting drug causes physical changes to some nerve cells (neurons) in your brain. Neurons use chemicals called neurotransmitters to communicate. These changes can remain long after you stop using the drug.
Opioids, including prescription analgesics, derive from the poppy plant called opium (Papaver somniferum). Clinicians prescribe various opioids to control pain, decrease cough, or relieve diarrhea. Opioid-use disorders occur in individuals from all educational and socioeconomic backgrounds. There is a biological base of addiction. Patients can be deficient in neurotransmitters such as dopamine, making them more likely to seek external sources of endorphins 54. In an attempt to self-correct this deficit, some individuals may turn to opioids. Separately, a patient with first-degree relatives (i.e., parents, brother & sister) who have a substance abuse disorder is more likely to develop an opiate use disorder. There is an estimated 50% heritability to opioid use disorder 55.
Patients diagnosed with opioid use disorder exposed to an environment that includes opioid use may be more likely to develop substance abuse disorder. Environmental influence on opioid use may be secondary to peer relationships or be from a physician’s prescription for a previous injury 54. Patients with a history of depression, post-traumatic stress disorder (PTSD), or anxiety are more likely to suffer from substance abuse, as well as patients with histories of childhood trauma and abuse 56. Opioid dependence includes physical or psychological dependence or both.
Genetics may also play a role in the development of opioid use disorder. Mu, delta, and kappa are the three different principal receptors for opioids. Mu acts in the brain by decreasing the release of neurotransmitters 57. Research has demonstrated a genetic basis in the treatment of pain for opioid use disorder. There are no specific interaction between genetic predisposition and responses to therapeutic drugs, as there is no clear evidence connecting genotype to drug effect, toxicity, or dependence 58.
Risk factors for opioid use disorder
People of any age, sex or economic status can become addicted to a drug. Scientists don’t know why some people have problems when they try to stop using opioids and others can stop using them without problems. Scientists do know that some things make you more likely than others to have problems with opioids. These are called risk factors. Having a risk factor doesn’t mean for sure that you’llhave these problems. But it may increase your chances.
Certain factors can affect the likelihood and speed of developing an addiction:
- Family history of addiction or problems with drugs. Drug addiction is more common in some families and likely involves an increased risk based on genes. If you have a blood relative, such as a parent, brother or sister, with alcohol or drug addiction, you’re at greater risk of developing a drug addiction.
- Mental health disorder. Pregnant women with opioid use disorder often have a mental health condition like anxiety, depression, attention-deficit/hyperactivity disorder (ADHD) or post-traumatic stress disorder (PTSD), you’re more likely to become addicted to drugs. Using drugs can become a way of coping with painful feelings, such as anxiety, depression and loneliness, and can make these problems even worse. Anxiety is strong feelings of worry or fear, and depression is strong feelings of sadness. These feelings last for a long time and interfere with your daily life. PTSD can happen if you’ve experienced a shocking, scary or dangerous event, like a disaster, rape, abuse or the sudden death of a loved one. People with PTSD may have serious anxiety, flashbacks, nightmares or physical responses (like sweating or a racing heartbeat) when reminded of the event. Tell your provider if you have or think you have a mental health condition, like anxiety, depression or PTSD.
- Peer pressure. Peer pressure is a strong factor in starting to use and misuse drugs, particularly for young people.
- Lack of family involvement. Difficult family situations or lack of a bond with your parents or siblings may increase the risk of addiction, as can a lack of parental supervision.
- Early use. Using drugs at an early age can cause changes in the developing brain and increase the likelihood of progressing to drug addiction.
- Taking a highly addictive drug. Some drugs, such as stimulants, cocaine or opioid painkillers, may result in faster development of addiction than other drugs. Smoking or injecting drugs can increase the potential for addiction. Taking drugs considered less addicting — so-called “light drugs” — can start you on a pathway of drug use and addiction.
Opioid use disorder prevention
The best way to prevent an addiction to a drug is not to take the drug at all. To prevent problems with prescription opioids, be sure to follow your doctor’s instructions when taking them. Do not share your medicines with anyone else. Contact your doctor if you have any concerns about taking opioids.
Your doctor should prescribe these medicines at safe doses and amounts and monitor their use so that you’re not given too great a dose or for too long a time. If you feel you need to take more than the prescribed dose of a medicine, talk to your health care provider.
Preventing drug use in children and teenagers
Take these steps to help prevent drug misuse in your children and teenagers:
- Communicate. Talk to your children about the risks of drug use and misuse.
- Listen. Be a good listener when your children talk about peer pressure and be supportive of their efforts to resist it.
- Set a good example. Don’t misuse alcohol or addictive drugs. Children of parents who misuse drugs are at greater risk of drug addiction.
- Strengthen the bond. Work on your relationship with your children. A strong, stable bond between you and your child will reduce your child’s risk of using or misusing drugs.
Opioid use disorder symptoms
Signs and symptoms of opioids or narcotic use and dependence can include:
- A sense of feeling “high”
- Reduced sense of pain
- Agitation, drowsiness or sedation
- Slurred speech
- Problems with attention and memory
- Pupils that are smaller than usual
- Lack of awareness or inattention to surrounding people and things
- Problems with coordination
- Depression
- Confusion
- Constipation
- Runny nose or nose sores (if snorting drugs)
- Needle marks (if injecting drugs)
Drug addiction symptoms or behaviors include, among others:
- Feeling that you have to use the drug regularly — daily or even several times a day
- Having intense urges for the drug that block out any other thoughts
- Over time, needing more of the drug to get the same effect
- Taking larger amounts of the drug over a longer period of time than you intended
- Making certain that you maintain a supply of the drug
- Spending money on the drug, even though you can’t afford it
- Not meeting obligations and work responsibilities, or cutting back on social or recreational activities because of drug use
- Continuing to use the drug, even though you know it’s causing problems in your life or causing you physical or psychological harm
- Doing things to get the drug that you normally wouldn’t do, such as stealing
- Driving or doing other risky activities when you’re under the influence of the drug
- Spending a good deal of time getting the drug, using the drug or recovering from the effects of the drug
- Failing in your attempts to stop using the drug
- Experiencing withdrawal symptoms when you attempt to stop taking the drug.
Opioid use disorder symptoms reflect compulsive, prolonged self administration of opioid substances that are used for no legitimate medical purpose or, if another medical condition is present that requires opioid treatment, that are used in doses greatly in excess of the amount needed for that medical condition. For example, an individual prescribed analgesic opioids for pain relief at adequate dosing will use significantly more than prescribed dosage and not only because of persistent pain. Individuals with opioid use disorder tend to develop such regular patterns of compulsive drug use that daily activities are planned around obtaining and administering opioids.
Opioids are usually purchased on the illegal market but may also be obtained from physicians by falsifying or exaggerating general medical problems or by receiving simultaneous prescriptions from several physicians. Health care professionals with opioid use disorder will often obtain opioids by writing prescriptions for themselves or by diverting opioids that have been prescribed for
patients or from pharmacy supplies. Most individuals with opioid use disorder have significant levels of tolerance and will experience withdrawal on abrupt discontinuation of opioid substances.
Individuals with opioid use disorder often develop conditioned responses to drug-related stimuli (e.g., craving on seeing any heroin powder-like substance), a phenomenon that occurs with most drugs that cause intense psychological changes. These responses probably contribute to relapse, are difficult to extinguish, and typically persist long after detoxification is completed.
Opioid use disorder can also be associated with a history of drug-related crimes (e.g., possession or distribution of drugs, forgery, burglary, robbery, larceny, receiving stolen goods). Among health care professionals and individuals who have ready access to controlled substances, there is often a different pattern of illegal activities involving problems with state licensing boards, professional staffs of hospitals, or other administrative agencies. Marital difficulties (including divorce), unemployment, and irregular employment are often associated with opioid use disorder at all socioeconomic levels.
Recognizing unhealthy drug use in family members
Sometimes it’s difficult to distinguish normal teenage moodiness or anxiety from signs of drug use. Possible signs that your teenager or other family member is using drugs include:
- Problems at school or work — frequently missing school or work, a sudden disinterest in school activities or work, or a drop in grades or work performance
- Physical health issues — lack of energy and motivation, weight loss or gain, or red eyes
- Neglected appearance — lack of interest in clothing, grooming or looks
- Changes in behavior — major efforts to bar family members from entering the teenager’s room or being secretive about going out with friends; or drastic changes in behavior and in relationships with family and friends
- Money issues — sudden requests for money without a reasonable explanation; or your discovery that money is missing or has been stolen or that items have disappeared from your home, indicating maybe they’re being sold to support drug use.
Opioid use disorder complications
Drug use can have significant and damaging short-term and long-term effects. Taking opioids can be particularly risky, especially if you take high doses or combine them with other drugs or alcohol. Opioids can cause side effects such as drowsiness, mental fog, nausea, and constipation. They may also cause slowed breathing, which can lead to overdose deaths.
If you have opioid use disorder, you’re at risk for overdose. This is when you take too much of a drug. Opioid overdose can slow or stop your breathing. Opioid overdose can cause you to pass out and even die. If you’re using opioids and have any of these signs and symptoms of overdose, call your local emergency services number immediately:
- Blurred vision
- Cold, clammy skin (your face is extremely pale and/or feels clammy to the touch)
- Feeling dizzy, faint or very sleepy
- Feeling sick to your stomach
- Loose, floppy muscles (your body goes limp)
- Slowed or trouble breathing or a slow heartbeat
- Your fingernails or lips have a purple or blue color
- Started vomiting or making gurgling noises
- Cannot be awakened or are unable to speak.
Dependence on drugs can create a number of dangerous and damaging complications, including:
- Getting an infectious disease. People who are addicted to a drug are more likely to get an infectious disease, such as HIV, either through unsafe sex or by sharing needles with others.
- Other health problems. Drug addiction can lead to a range of both short-term and long-term mental and physical health problems. These depend on what drug is taken.
- Accidents. People who are addicted to drugs are more likely to drive or do other dangerous activities while under the influence.
- Suicide. People who are addicted to drugs die by suicide more often than people who aren’t addicted.
- Family problems. Behavioral changes may cause relationship or family conflict and custody issues.
- Work issues. Drug use can cause declining performance at work, absenteeism and eventual loss of employment.
- Problems at school. Drug use can negatively affect academic performance and motivation to excel in school.
- Legal issues. Legal problems are common for drug users and can stem from buying or possessing illegal drugs, stealing to support the drug addiction, driving while under the influence of drugs or alcohol, or disputes over child custody.
- Financial problems. Spending money to support drug use takes away money from other needs, could lead to debt, and can lead to illegal or unethical behaviors.
Opioid use disorder diagnosis
Diagnosing opioid use disorder or drug addiction (substance use disorder) requires a thorough evaluation and often includes an assessment by a psychiatrist, a psychologist, or a licensed alcohol and drug counselor. Blood, urine or other lab tests are used to assess drug use, but they’re not a diagnostic test for addiction. However, these tests may be used for monitoring treatment and recovery.
For diagnosis of an opioid use disorder, most mental health professionals use criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association 59, 60.
Urine drug tests are necessary before starting and while maintaining methadone or buprenorphine 61.
If the patients have a history of IV drug abuse, tests for HIV, hepatitis B, and C should be ordered 62, 63, 64. A patient who is unconscious or obtunded secondary to opioid intoxication or overdose may require a non-contrast CT of the head for possible hemorrhage or a chest X-ray for possible aspiration pneumonia. Furthermore, IV opioid users with bacteremia will require an echocardiogram to rule out endocarditis.Neuroimaging and neuropsychological studies demonstrate dysregulation of the circuits associated with emotion, impulsivity, and stress. Neuroimaging shows both functional and structural brain alterations for patients in patients with a substance use disorder 65.
DSM 5 opioid use disorder
In the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) opioid use disorder is defined as a problematic pattern of opioid use leading to clinically significant impairment or distress, as manifested by at least two of the following, occurring within a 12-month period 11:
- Criterion A
- Opioids are often taken in larger amounts or over a longer period than was intended.
- There is a persistent desire or unsuccessful efforts to cut down or control opioid use.
- A great deal of time is spent in activities necessary to obtain the opioid, use the opioid, or recover from its effects.
- Craving, or a strong desire or urge to use opioids.
- Recurrent opioid use resulting in a failure to fulfill major role obligations at work, school, or home.
- Continued opioid use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of opioids.
- Important social, occupational, or recreational activities are given up or reduced because of opioid use.
- Recurrent opioid use in situations in which it is physically hazardous.
- Continued opioid use despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance.
- Tolerance, as defined by either of the following:
- a. A need for markedly increased amounts of opioids to achieve intoxication or desired effect.
- b. A markedly diminished effect with continued use of the same amount of an opioid.
- Note: This criterion is not considered to be met for those taking opioids solely under appropriate medical supervision.
- Withdrawal, as manifested by either of the following:
- a. The characteristic opioid withdrawal syndrome (refer to Criteria A and B of the criteria set for opioid withdrawal, pp. 547-548).
- b. Opioids (or a closely related substance) are taken to relieve or avoid withdrawal symptoms.
- Note: This criterion is not considered to be met for those individuals taking opioids solely under appropriate medical supervision.
Specify if:
- In early remission: After full criteria for opioid use disorder were previously met, none of the criteria for opioid use disorder have been met for at least 3 months but for less than 12 months (with the exception that Criterion A4, “Craving, or a strong desire or urge to use opioids,” may be met).
- In sustained remission: After full criteria for opioid use disorder were previously met, none of the criteria for opioid use disorder have been met at any time during a period of 12 months or longer (with the exception that Criterion A4, “Craving, or a strong desire or urge to use opioids,” may be met).
Specify if:
- On maintenance therapy: This additional specifier is used if the individual is taking a prescribed agonist medication such as methadone or buprenorphine and none of the criteria for opioid use disorder have been met for that class of medication (except tolerance to, or withdrawal from, the agonist). This category also applies to those individuals being maintained on a partial agonist, an agonist/antagonist, or a full antagonist such as oral naltrexone or depot naltrexone.
- In a controlled environment: This additional specifier is used if the individual is in an environment where access to opioids is restricted.
Opioid use disorder treatment
Treatments for opioid use disorder include:
- Medications for opioid use disorder. The medicines used to treat opioid misuse and addiction are methadone, buprenorphine, and naltrexone.
- Counseling and behavioral therapies.
- Medication-assisted therapy (MAT), which includes medication for opioid use disorder, counseling, and behavioral therapies. This offers a “whole patient” approach to treatment, which can increase your chance of a successful recovery.
- Residential and hospital-based treatment.
- Residential programs combine housing and treatment services. You are living with your peers, and you can support each other to stay in recovery.
- Inpatient hospital-based programs combine health care and addiction treatment services for people with medical problems. Hospitals may also offer intensive outpatient treatment. All these types of treatments are very structured, and usually include several different kinds of counseling and behavioral therapies. They also often include medicines.
Methadone and buprenorphine can decrease withdrawal symptoms and cravings. They work by acting on the same targets in the brain as other opioids, but they do not make you feel high. Some people worry that if they take methadone or buprenorphine, it means that they are substituting one addiction for another. But it is not; these medicines are a treatment. They restore balance to the parts of the brain affected by addiction. This allows your brain to heal while you work toward recovery.
There is also a combination drug that includes buprenorphine and naloxone. Naloxone is a drug to treat an opioid overdose. If you take it along with buprenorphine, you will be less likely to misuse the buprenorphine.
You may safely take these medicines for months, years, or even a lifetime. If you want to stop taking them, do not do it on your own. You should contact your health care provider first, and work out a plan for stopping.
Naltrexone works differently than methadone and buprenorphine. It does not help you with withdrawal symptoms or cravings. Instead, it takes away the high that you would normally get when you take opioids. Because of this, you would take naltrexone to prevent a relapse, not to try to get off opioids. You have to be off opioids for at least 7-10 days before you can take naltrexone. Otherwise you could have bad withdrawal symptoms.
Clonidine or lofexidine treats the signs and symptoms of withdrawal as an adjunctive therapy 54. In some countries, not including the United States, long-term injecting drug users who fail methadone are treated with pure injectable diamorphine 54. Dihydrocodeine in both extended-release and immediate-release forms are useful in the maintenance treatment as an alternative to methadone or buprenorphine 66. Clonidine or tizanidine are helpful to decrease anxiety associated with opioid withdrawal. They also cause piloerection and other signs and symptoms of autonomic overactivity. The treatment of anxiety and insomnia associated with opioid withdrawal is with benzodiazepines or other sedating drugs. Diarrhea, nausea, and vomiting are treated with loperamide. Prochlorperazine, along with sports drinks or intravenous fluids, is also helpful. Pain mitigation is through the use of nonsteroidal anti-inflammatory agents such as naproxen. Combination therapies are superior to placebo for symptomatic relief.
Because each medication works differently, your treatment provider should decide on the optimal medication in consultation with you and should consider your unique history and circumstances.
Buprenorphine
Buprenorphine is a partial opioid agonist at the mu-opioid receptor, meaning that it binds to those same opioid receptors but activates them less strongly than full opioid agonists do. Buprenorphine is the first medication to treat opioid use disorder that can be prescribed or dispensed in physician offices (with a current standard DEA registration with Schedule 3 authority), significantly increasing access to treatment 67. As with all medications used in opioid use disorder treatment, buprenorphine should be prescribed as part of a comprehensive treatment plan that includes counseling and other services to provide patients with a whole-person approach.
Buprenorphine is a partial opioid agonist. Like methadone, it can reduce cravings and withdrawal symptoms in a person with an opioid use disorder without producing euphoria, and patients tend to tolerate it well. Research has found buprenorphine to be similarly effective as methadone for treating opioid use disorders, as long as it is given at a sufficient dose and for sufficient duration 68. The U.S. Food and Drug Administration (FDA) approved buprenorphine in 2002, making it the first medication eligible to be prescribed by certified physicians through the Drug Addiction Treatment Act 69. This approval eliminates the need to visit specialized treatment clinics, thereby expanding access to treatment for many who need it. Additionally, the Comprehensive Addiction and Recovery Act (CARA), which was signed into law in July 2016, temporarily expands eligibility to prescribe buprenorphine-based drugs for medication-assisted treatment (MAT) to qualifying nurse practitioners and physician assistants through October 1, 2021 69. Buprenorphine has been available for opioid use disorders since 2002 as a tablet and since 2010 as a sublingual film 70. The FDA approved a 6-month subdermal buprenorphine implant in May 2016 and a once-monthly buprenorphine injection in November 2017 69. These formulations are available to patients stabilized on buprenorphine and will eliminate the treatment barrier of daily dosing for these patients.
When taken as prescribed, buprenorphine is safe and effective.
Buprenorphine has unique pharmacological properties that help:
- Diminish the effects of physical dependency to opioids, such as withdrawal symptoms and cravings
- Increase safety in cases of overdose
- Lower the potential for misuse
The following buprenorphine products are FDA approved for the treatment of opioid use disorder:
- Generic Buprenorphine/naloxone sublingual tablets
- Buprenorphine sublingual tablets (Subutex)
- Buprenorphine/naloxone sublingual films (Suboxone)
- Buprenorphine/naloxone) sublingual tablets (Zubsolv)
- Buprenorphine/naloxone buccal film (Bunavail)
- Buprenorphine implants (Probuphine)
- Buprenorphine extended-release injection (Sublocade)
To begin treatment with buprenorphine, an opioid use disorder patient must abstain from using opioids for at least 12 to 24 hours and be in the early stages of opioid withdrawal. Patents with opioids in their bloodstream or who are not in the early stages of withdrawal, may experience acute withdrawal. Long acting opioids, such as methadone, require at least 48-72 hours since last use before initiating buprenorphine. Short acting opioids (for example, heroin) require approximately 12 hours since last use for sufficient withdrawal to occur in order to safely initiate buprenorphine treatment. Some opioid such as fentanyl may require greater than 12 hours. Clinical presentation should guide this decision as individual presentations will vary.
After a patient has discontinued or greatly reduced their opioid use, no longer has cravings, and is experiencing few, if any, side effects, if needed, the dose of buprenorphine may be adjusted. Due to the long-acting agent of buprenorphine, once patients are stabilized, it may be possible to switch from every day to alternate-day dosing.
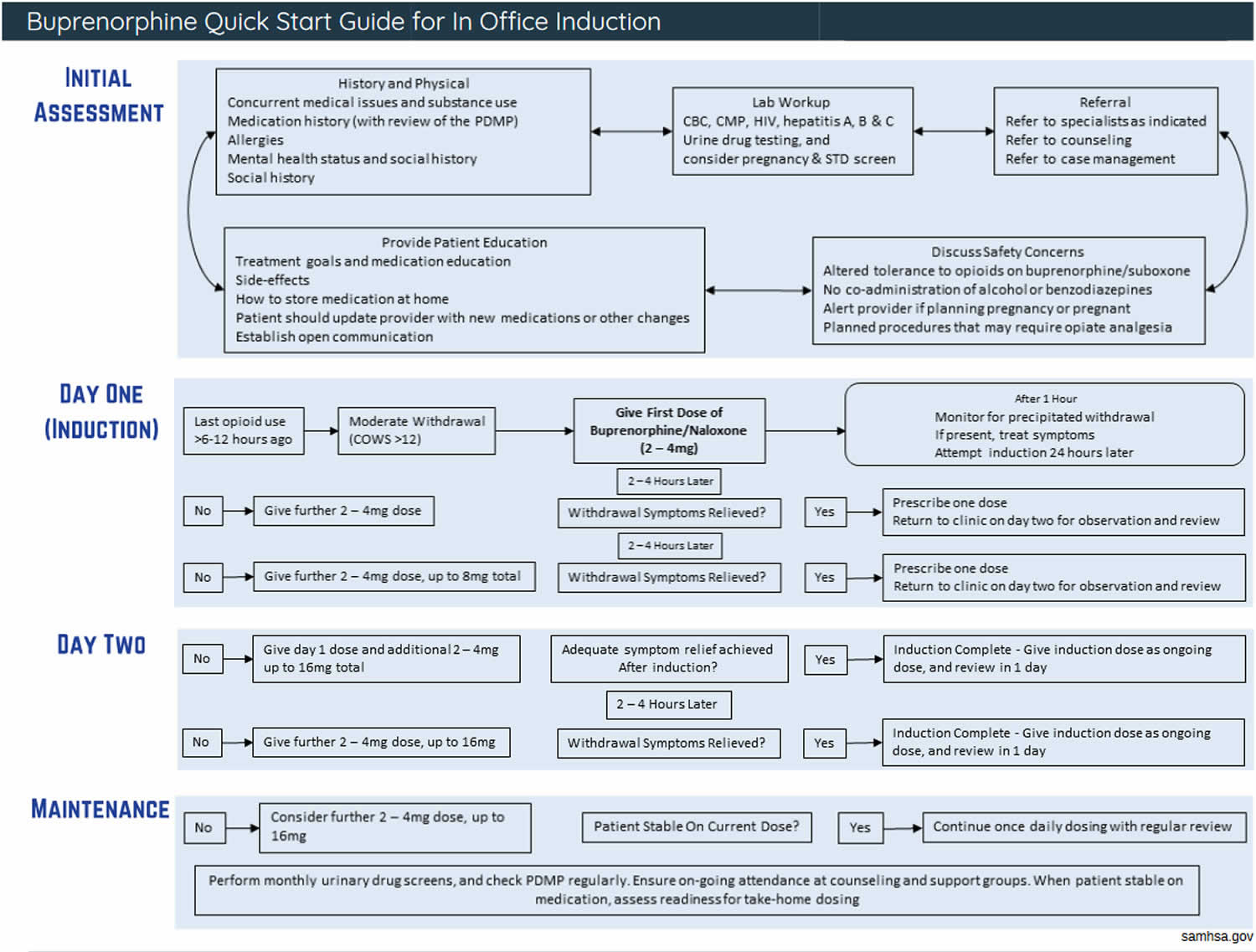
The dose of buprenorphine depends on the severity of withdrawal symptoms, and the history of last opioid use (see Figure 2 flowchart for dosing advice).
The length of time a patient receives buprenorphine is tailored to meet the needs of each patient, and in some cases, treatment can be indefinite. To prevent possible relapse, individuals can engage in on-going treatment—with or without medication for opioid use disorder.
Common side effects of buprenorphine include 71:
- Constipation, headache, nausea, and vomiting
- Dizziness
- Drowsiness and fatigue
- Sweating
- Dry mouth
- Tooth decay
- Muscle aches and cramps
- Inability to sleep
- Fever
- Blurred vision or dilated pupils
- Tremors
- Palpitations
- Disturbance in attention
Serious side effects of buprenorphine include 71:
- Respiratory distress
- Overdose
- Adrenal insufficiency
- Dependence
- Withdrawal
- Itching, pain, swelling, and nerve damage (implant)
- Pain at injection site (injection)
- Neonatal abstinence syndrome (in newborns)
Figure 2. Buprenorphine quick start guide
Methadone
Methadone is a medication used to treat opioid use disorder as well as for pain management 72. Methadone is a long-acting full opioid agonist that eliminates withdrawal symptoms and relieves drug cravings by acting on opioid receptors in the brain—the same receptors that other opioids such as heroin, morphine, and opioid pain medications activate. Although it occupies and activates these opioid receptors, it does so more slowly than other opioids and, in an opioid-dependent person, treatment doses do not produce euphoria. Methadone has been used successfully for more than 40 years to treat opioid use disorder and must be dispensed through a Substance Abuse and Mental Health Services Administration (SAMHSA) certified opioid treatment programs 73. Taken daily, it is available in liquid, powder and diskettes forms.
Methadone is one component of a comprehensive treatment plan, which includes counseling and other behavioral health therapies to provide patients with a whole-person approach. Methadone helps individuals achieve and sustain recovery and to reclaim active and meaningful lives.
Patients taking methadone to treat opioid use disorder must receive the medication under the supervision of a practitioner. After a period of stability (based on progress and proven, consistent compliance with the medication dosage), patients may be allowed to take methadone at home between program visits 72.
The length of time a person receives methadone treatment varies 72. According to the National Institute on Drug Abuse publication Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition), the length of methadone treatment should be a minimum of 12 months 74. Some patients may require long-term maintenance. Patients must work with their practitioner to gradually reduce their methadone dosage to prevent withdrawal.
When taken as prescribed, methadone is safe and effective.
Methadone medication is specifically tailored for the individual patient (and doses are often adjusted and readjusted) and is never to be shared with or given to others. This is particularly important for patients who take methadone at home and are not required to take medication under direct supervision at a Substance Abuse and Mental Health Services Administration (SAMHSA) certified opioid treatment program.
Other medications may interact with methadone and cause heart conditions. Even after the effects of methadone wear off, the medication’s active ingredients remain in the body for much longer. Unintentional overdose is possible if patients do not take methadone as prescribed.
The following tips can help you achieve the best treatment results:
- Never use more than the amount prescribed, and always take at the times prescribed. If a dose is missed, or if it feels like it’s not working, do not take an extra dose of methadone
- Do not consume alcohol while taking methadone.
- Be careful driving or operating machinery on methadone.
- Call your local emergency services number if too much methadone is taken or if an overdose is suspected.
- Prevent children and pets from accidental ingestion by storing it out of reach.
- Store methadone at room temperature and away from light.
- Do not shared your methadone with anyone even if they have similar symptoms or suffer from the same condition.
- Dispose of unused methadone safely.
Common side effects of methadone include:
- Restlessness
- Nausea or vomiting
- Slow breathing
- Itchy skin
- Heavy sweating
- Constipation
- Sexual problems
Serious side effects of methadone include:
- Experience difficulty breathing or shallow breathing
- Feel lightheaded or faint
- Experience hives or a rash; swelling of the face, lips, tongue, or throat
- Feel chest pain
- Experience a fast or pounding heartbeat
- Experience hallucinations or confusion.
Naltrexone
Naltrexone is a medication approved by the Food and Drug Administration (FDA) to treat both alcohol use disorder and opioid use disorder 75. Naltrexone is an opioid antagonist, which means that it works by blocking the activation of opioid receptors 69. Naltrexone works differently than methadone and buprenorphine. Instead of controlling withdrawal symptoms and cravings, naltrexone treats opioid use disorder by preventing any opioid drug from producing rewarding effects such as euphoria. Naltrexone blocks the euphoric and sedative effects of opioids such as heroin, morphine, and codeine. Because of this, you would take naltrexone to prevent a relapse, not to try to get off opioids. You have to be off opioids for at least 7 days after you last use of short-acting opioids and 10 to 14 days for long-acting opioids, before starting naltrexone. Otherwise you could have bad withdrawal symptoms.
Naltrexone is not an opioid, is not addictive, and does not cause withdrawal symptoms with stop of use. There is no abuse and diversion potential with naltrexone.
Naltrexone use for ongoing opioid use disorder treatment has been somewhat limited because of poor adherence and tolerability by patients. However, in 2010, an injectable, long-acting form of naltrexone (Vivitrol), originally approved for treating alcohol use disorder, was FDA-approved for treating opioid use disorder 69. Because the long-acting form of naltrexone effects last for weeks, Vivitrol is a good option for patients who do not have ready access to health care or who struggle with taking their medications regularly.
While the oral naltrexone formulation will also block opioid receptors, only the long acting injectable naltrexone formulation (Vivitrol) is FDA approved as a medication for opioid use disorder and requires Risk Evaluation and Mitigation Strategy (REMS) 75.
Patients on naltrexone, who discontinue use or relapse after a period of abstinence, may have a reduced tolerance to opioids. Therefore, taking the same, or even lower doses of opioids used in the past can cause life-threatening consequences 75.
You should not take naltrexone if you:
- Currently use or have a physical dependence on opioid-containing medicines or opioid drugs, such as heroin, or currently experiencing opioid withdrawal symptoms
- Experience opioid withdrawal symptoms. Withdrawal symptoms may happen when a patient was taking opioid-containing medicines or opioid drugs regularly and then stopped.
- Symptoms of opioid withdrawal may include: anxiety, sleeplessness, yawning, fever, sweating, teary eyes, runny nose, goose bumps, shakiness, hot or cold flushes, muscle aches, muscle twitches, restlessness, nausea and vomiting, diarrhea, or stomach cramps.
Common side effects of naltrexone may include:
- nausea
- sleepiness
- headache
- dizziness
- vomiting
- decreased appetite
- painful joints
- muscle cramps
- cold symptoms
- trouble sleeping
- toothache
Serious side effects of naltrexone may include:
- Severe reactions at the site of injection:
- intense pain
- tissue death, surgery may be required
- swelling, lumps, or area feels hard
- scabs, blisters, or open wounds
- Liver damage or hepatitis is possible:
- stomach area pain lasting more than a few days
- dark urine
- yellowing of the whites of your eyes
- tiredness
- Serious allergic reactions
- skin rash
- swelling of face, eyes, mouth, or tongue
- trouble breathing or wheezing
- chest pain
- feeling dizzy or faint
- Pneumonia
- Depressed mood
- Risk of Opioid Overdose. Patients should tell family and the people they are closest to about the increased sensitivity to opioids and the risk of overdose. Accidental overdose can happen in two ways:
- Naltrexone blocks the effects of opioids, such as heroin or opioid pain medicines. Patients who try to overcome this blocking effect by taking large amounts of opioids may experience serious injury, coma, or death.
- After receiving a dose of naltrexone, the blocking effect slowly decreases and completely goes away over time. Patients who are taking naltrexone for an opioid use disorder can become more sensitive to the effects of opioids at the dose used before, or even lower amounts. Using opioids while on naltrexone can lead to overdose and death.
Behavior therapy
As part of a drug treatment program, behavior therapy — a form of psychotherapy or counseling — can be done by a psychologist or psychiatrist, or you may receive counseling from a licensed alcohol and drug counselor. Therapy and counseling may be done with an individual, a family or a group. The therapist or counselor can:
- Help you develop ways to cope with your drug cravings
- Suggest strategies to avoid drugs and prevent relapse
- Change your attitudes and behaviors related to drug use
- Offer suggestions on how to deal with a relapse if it occurs
- Talk about issues regarding your job, legal problems, and relationships with family and friends
- Include family members to help them develop better communication skills and be supportive
- Address other mental health conditions
- Build healthy life skills
There are different types of counseling to treat opioid use disorder, including:
- Individual counseling, which may include setting goals, talking about setbacks, and celebrating progress. You may also talk about legal concerns and family problems. Counseling often includes specific behavioral therapies, such as:
- Cognitive-behavioral therapy (CBT) helps you recognize and stop negative patterns of thinking and behavior. It teaches you coping skills, including how to manage stress and change the thoughts that cause you to want to misuse opioids.
- Motivational enhancement therapy helps you build up motivation to stick with your treatment plan
- Contingency management focuses on giving you incentives for positive behaviors such as staying off the opioids
- Group counseling, which can help you feel that you are not alone with your issues. You get a chance to hear about the difficulties and successes of others who have the same challenges. This can help you to learn new strategies for dealing with the situations you may come across.
- Family counseling includes partners or spouses and other family members who are close to you. It can help to repair and improve your family relationships.
Counselors can also refer you to other resources that you might need, such as:
- Peer support groups, including 12-step programs like Narcotics Anonymous (https://na.org) or SMART Recovery (https://www.smartrecovery.org)
- Spiritual and faith-based groups
- HIV testing and hepatitis screening
- Case or care management
- Employment or educational supports
- Organizations that help you find housing or transportation
Self-help groups
Self-help support groups, such as Narcotics Anonymous (https://na.org) or SMART Recovery (https://www.smartrecovery.org), help people who are addicted to drugs. The self-help support group message is that addiction is an ongoing disorder with a danger of relapse. Self-help support groups can decrease the sense of shame and isolation that can lead to relapse.
You can also find help and treatment resources by visiting the Substance Abuse and Mental Health Services Administration website (https://www.samhsa.gov) or by calling the helpline at 1-800-662-HELP (4357).
Your therapist or licensed counselor can help you locate a self-help support group. You may also find support groups in your community or on the internet.
Ongoing treatment
Even after you’ve completed initial treatment, ongoing treatment and support can help prevent a relapse. Follow-up care can include periodic appointments with your counselor, continuing in a self-help program or attending a regular group session. Seek help right away if you relapse.
Relapse prevention
Once you’ve been addicted to a drug, you’re at high risk of falling back into a pattern of addiction. If you do start using the drug, it’s likely you’ll lose control over its use again — even if you’ve had treatment and you haven’t used the drug for some time.
- Follow your treatment plan. Monitor your cravings. It may seem like you’ve recovered and you don’t need to keep taking steps to stay drug-free. But your chances of staying drug-free will be much higher if you continue seeing your therapist or counselor, going to support group meetings and taking prescribed medicine.
- Avoid high-risk situations. Don’t go back to the neighborhood where you used to get your drugs. And stay away from your old drug crowd.
- Get help immediately if you use the drug again. If you start using the drug again, talk to your doctor, your mental health provider or someone else who can help you right away.
Studies show that people with opioid use disorder who follow detoxification with complete abstinence are very likely to relapse, or return to using the drug 76. While relapse is a normal step on the path to recovery, it can also be life threatening, raising the risk for a fatal overdose 77. Therefore, an important way to support recovery from heroin or prescription opioid use disorder is to maintain abstinence from those drugs. Someone in recovery can also use medications that reduce the negative effects of withdrawal and cravings without producing the euphoria that the original drug of abuse caused. For example, the FDA recently approved lofexidine, a non-opioid medicine designed to reduce opioid withdrawal symptoms 69. Methadone and buprenorphine are other medications approved for this purpose.
Opioid use disorder prognosis
Evidence suggest that individuals who are actively using other substances during opioid use disorder treatment may have a poorer prognosis 78, 79, 80.
During and after tapering off methadone, close contact with the patient should be maintained because discontinuation of maintenance carries high risks of relapse to the use of illicit drugs and overdoses that may lead to death 81. The mortality during induction with buprenorphine is lower than that during induction with methadone 82. The advantage of buprenorphine and methadone therapy is a reduction in morbidity (sickness) and mortality (rate of death) 54. Opioid replacement therapy reduces the incidence of long-term opioid addiction while decreasing illegal opiate use and decreasing mortality 54. The cost to society with opioid replacement is lessened, including crimes associated with drugs and the expense of dealing with HIV, sepsis, and other medical complications. Opioid replacement therapy has the support of most national and international organizations as a cost-effective method of reducing injection infections and lowering HIV/AIDS exposure. Methadone treatment for opioid use disorder is associated with a 50% reduction in all-cause mortality, as well as a 50% reduction in the incidence of hepatitis C. Methadone also decreases drug-related crimes, illicit drug use, improved social interactions, and increased rates of retention in rehabilitation programs 82, 83, 84.
Over 90% of patients go through opioid withdrawal and relapse one month later 81.
- Opioid Use and Opioid Use Disorder in Pregnancy. https://www.acog.org/-/media/project/acog/acogorg/clinical/files/committee-opinion/articles/2017/08/opioid-use-and-opioid-use-disorder-in-pregnancy.pdf[↩][↩][↩][↩][↩][↩][↩]
- The Science of Drug Use and Addiction: The Basics. https://archives.nida.nih.gov/publications/media-guide/science-drug-use-addiction-basics[↩]
- Opioid Misuse and Addiction. https://medlineplus.gov/opioidmisuseandaddiction.html[↩]
- Opioid Misuse and Addiction Treatment. https://medlineplus.gov/opioidmisuseandaddictiontreatment.html[↩]
- 2020 National Survey of Drug Use and Health (NSDUH) Releases. https://www.samhsa.gov/data/release/2020-national-survey-drug-use-and-health-nsduh-releases[↩]
- Multiple Cause of Death 1999-2021. Centers for Disease Control and Prevention, National Center on Health Statistics. https://wonder.cdc.gov/wonder/help/mcd-expanded.html[↩]
- Patrick SW, Davis MM, Lehmann CU, Lehman CU, Cooper WO. Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009 to 2012. J Perinatol Off J Calif Perinat Assoc. 2015;35(8):650-655. doi:10.1038/jp.2015.36[↩]
- Tolia VN, Patrick SW, Bennett MM, et al. Increasing incidence of the neonatal abstinence syndrome in U.S. neonatal ICUs. N Engl J Med. 2015;372(22):2118-2126. doi:10.1056/NEJMsa1500439[↩]
- Conrad C, Bradley HM, Broz D, et al. Community Outbreak of HIV Infection Linked to Injection Drug Use of Oxymorphone–Indiana, 2015. MMWR Morb Mortal Wkly Rep. 2015;64(16):443-444. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6416a4.htm[↩]
- Opioid Use Disorder: Diagnostic Criteria. https://www.cdc.gov/opioids/healthcare-professionals/prescribing/pdf/Opioid-Use-Disorder-Checklist.pdf[↩]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596[↩][↩]
- Abraham AJ, Andrews CM, Harris SJ, Friedmann PD. Availability of Medications for the Treatment of Alcohol and Opioid Use Disorder in the USA. Neurotherapeutics. 2020 Jan;17(1):55-69. doi: 10.1007/s13311-019-00814-4[↩][↩]
- Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014 Feb 6;(2):CD002207. doi: 10.1002/14651858.CD002207.pub4[↩][↩]
- Minozzi S, Amato L, Vecchi S, Davoli M, Kirchmayer U, Verster A. Oral naltrexone maintenance treatment for opioid dependence. Cochrane Database Syst Rev. 2011 Apr 13;2011(4):CD001333. doi: 10.1002/14651858.CD001333.pub4[↩]
- Volkow ND, Wargo EM. Overdose Prevention Through Medical Treatment of Opioid Use Disorders. Ann Intern Med. 2018 Aug 7;169(3):190-192. doi: 10.7326/M18-1397[↩]
- Volkow ND, Frieden TR, Hyde PS, Cha SS. Medication-assisted therapies—tackling the opioid-overdose epidemic. N Engl J Med. 2014;370(22):2063–6. doi: 10.1056/NEJMp1402780[↩]
- Kampman K, Jarvis M. American Society of Addiction Medicine (ASAM) National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use. J Addict Med. 2015 Sep-Oct;9(5):358-67. doi: 10.1097/ADM.0000000000000166[↩]
- Amass L, Ling W, Freese TE, Reiber C, Annon JJ, Cohen AJ, et al. Bringing buprenorphine-naloxone detoxification to community treatment providers: the NIDA Clinical Trials Network field experience. Am J Addict. 2004;13(Suppl 1):S42–66. doi: 10.1080/10550490490440807[↩][↩]
- Comer SD, Sullivan MA, Yu E, Rothenberg JL, Kleber HD, Kampman K, et al. Injectable, sustained-release naltrexone for the treatment of opioid dependence: a randomized, placebo-controlled trial. Arch Gen Psychiatry. 2006;63(2):210–8. doi: 10.1001/archpsyc.63.2.210[↩][↩]
- Fiellin DA, Pantalon MV, Chawarski MC, Moore BA, Sullivan LE, O’Connor PG, et al. Counseling plus buprenorphine-naloxone maintenance therapy for opioid dependence. N Engl J Med. 2006;355(4):365–74. doi: 10.1056/NEJMoa055255[↩]
- Amato L, Minozzi S, Davoli M, Vecchi S. Psychosocial combined with agonist maintenance treatments versus agonist maintenance treatments alone for treatment of opioid dependence. Cochrane Database Syst Rev. 2011 Oct 5;(10):CD004147. doi: 10.1002/14651858.CD004147.pub4[↩][↩][↩]
- Amato L, Minozzi S, Davoli M, Vecchi S. Psychosocial and pharmacological treatments versus pharmacological treatments for opioid detoxification. Cochrane Database Syst Rev. 2011 Sep 7;(9):CD005031. doi: 10.1002/14651858.CD005031.pub4[↩][↩][↩]
- Johansson, B.A., Berglund, M. and Lindgren, A. (2006), Efficacy of maintenance treatment with naltrexone for opioid dependence: a meta-analytical review. Addiction, 101: 491-503. https://doi.org/10.1111/j.1360-0443.2006.01369.x[↩]
- Krupitsky E, Nunes EV, Ling W, Illeperuma A, Gastfriend DR, Silverman BL. Injectable extended-release naltrexone for opioid dependence. Lancet. 2011;378(9792):665. doi: 10.1016/S0140-6736(11)61331-7[↩][↩]
- Ziedonis DM, Amass L, Steinberg M, Woody G, Krejci J, Annon JJ, et al. Predictors of outcome for short-term medically supervised opioid withdrawal during a randomized, multicenter trial of buprenorphine-naloxone and clonidine in the NIDA clinical trials network drug and alcohol dependence. Drug Alcohol Depend. 2009;99(1–3):28–36. doi: 10.1016/j.drugalcdep.2008.06.016[↩]
- National Academies of Sciences E, and Medicine. Medications for opioid use disorder save lives. Washington, DC; 2019.[↩]
- Kaltenbach K, Berghella V, Finnegan L. Opioid dependence during pregnancy. Effects and management. Obstet Gynecol Clin North Am. 1998 Mar;25(1):139-51. doi: 10.1016/s0889-8545(05)70362-4[↩][↩][↩]
- Metz TD, Rovner P, Hoffman MC, Allshouse AA, Beckwith KM, Binswanger IA. Maternal Deaths From Suicide and Overdose in Colorado, 2004-2012. Obstet Gynecol. 2016 Dec;128(6):1233-1240. doi: 10.1097/AOG.0000000000001695[↩][↩]
- Smid MC, Stone NM, Baksh L, Debbink MP, Einerson BD, Varner MW, Gordon AJ, Clark EAS. Pregnancy-Associated Death in Utah: Contribution of Drug-Induced Deaths. Obstet Gynecol. 2019 Jun;133(6):1131-1140. doi: 10.1097/AOG.0000000000003279[↩][↩]
- Yazdy MM, Desai RJ, Brogly SB. Prescription Opioids in Pregnancy and Birth Outcomes: A Review of the Literature. J Pediatr Genet. 2015 Apr 1;4(2):56-70. doi: 10.1055/s-0035-1556740[↩][↩]
- Lind JN, Interrante JD, Ailes EC, Gilboa SM, Khan S, Frey MT, Dawson AL, Honein MA, Dowling NF, Razzaghi H, Creanga AA, Broussard CS. Maternal Use of Opioids During Pregnancy and Congenital Malformations: A Systematic Review. Pediatrics. 2017 Jun;139(6):e20164131. doi: 10.1542/peds.2016-4131[↩][↩]
- Kaltenbach K, Berghella V, Finnegan L. Opioid dependence during pregnancy. Effects and management. Obstet Gynecol Clin North Am. 1998 Mar;25(1):139-51. https://doi.org/10.1016/S0889-8545(05)70362-4[↩]
- Center for Substance Abuse Treatment. Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2005. (Treatment Improvement Protocol (TIP) Series, No. 43.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK64164[↩][↩][↩][↩]
- Stephen W. Patrick, Wanda D. Barfield, Brenda B. Poindexter, COMMITTEE ON FETUS AND NEWBORN, COMMITTEE ON SUBSTANCE USE AND PREVENTION, James Cummings, Ivan Hand, Ira Adams-Chapman, Susan W. Aucott, Karen M. Puopolo, Jay P. Goldsmith, David Kaufman, Camilia Martin, Meredith Mowitz, Lucien Gonzalez, Deepa R. Camenga, Joanna Quigley, Sheryl A. Ryan, Leslie Walker-Harding; Neonatal Opioid Withdrawal Syndrome. Pediatrics November 2020; 146 (5): e2020029074. 10.1542/peds.2020-029074[↩][↩][↩][↩][↩]
- About Opioid Use During Pregnancy. https://www.cdc.gov/pregnancy/opioids/basics.html[↩][↩][↩]
- Neonatal Abstinence Syndrome (NAS). https://www.marchofdimes.org/find-support/topics/planning-baby/neonatal-abstinence-syndrome-nas[↩]
- Clinical Guidance for Treating Pregnant and Parenting Women With Opioid Use Disorder and Their Infants. https://store.samhsa.gov/sites/default/files/d7/priv/sma18-5054.pdf[↩][↩][↩]
- Kandall SR, Doberczak TM, Jantunen M, Stein J. The methadone-maintained pregnancy. Clin Perinatol. 1999 Mar;26(1):173-83. https://doi.org/10.1016/S0095-5108(18)30077-0[↩]
- Susan B. Brogly, Kelley A. Saia, Alexander Y. Walley, Haomo M. Du, Paola Sebastiani, Prenatal Buprenorphine Versus Methadone Exposure and Neonatal Outcomes: Systematic Review and Meta-Analysis, American Journal of Epidemiology, Volume 180, Issue 7, 1 October 2014, Pages 673–686, https://doi.org/10.1093/aje/kwu190[↩][↩]
- Fajemirokun-Odudeyi O, Sinha C, Tutty S, Pairaudeau P, Armstrong D, Phillips T, Lindow SW. Pregnancy outcome in women who use opiates. Eur J Obstet Gynecol Reprod Biol. 2006 Jun 1;126(2):170-5. doi: 10.1016/j.ejogrb.2005.08.010[↩]
- Jones HE, Kaltenbach K, Heil SH, Stine SM, Coyle MG, Arria AM, O’Grady KE, Selby P, Martin PR, Fischer G. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010 Dec 9;363(24):2320-31. doi: 10.1056/NEJMoa1005359[↩][↩][↩]
- McCarthy JJ, Leamon MH, Willits NH, Salo R. The effect of methadone dose regimen on neonatal abstinence syndrome. J Addict Med. 2015;9(2):105-110. doi:10.1097/ADM.0000000000000099[↩]
- Fajemirokun-Odudeyi O, Sinha C, Tutty S, et al. Pregnancy outcome in women who use opiates. Eur J Obstet Gynecol Reprod Biol. 2006;126(2):170-175. doi:10.1016/j.ejogrb.2005.08.010[↩]
- Treatment for Opioid Use Disorder Before, During, and After Pregnancy. https://www.cdc.gov/pregnancy/opioids/treatment.html[↩][↩][↩][↩][↩][↩]
- Desai RJ, Huybrechts KF, Hernandez-Diaz S, Mogun H, Patorno E, Kaltenbach K, Kerzner LS, Bateman BT. Exposure to prescription opioid analgesics in utero and risk of neonatal abstinence syndrome: population based cohort study. BMJ. 2015 May 14;350:h2102. doi: 10.1136/bmj.h2102[↩]
- Huybrechts KF, Bateman BT, Desai RJ, Hernandez-Diaz S, Rough K, Mogun H, Kerzner LS, Davis JM, Stover M, Bartels D, Cottral J, Patorno E. Risk of neonatal drug withdrawal after intrauterine co-exposure to opioids and psychotropic medications: cohort study. BMJ. 2017 Aug 2;358:j3326. doi: 10.1136/bmj.j3326[↩]
- Patrick SW, Dudley J, Martin PR, Harrell FE, Warren MD, Hartmann KE, Ely EW, Grijalva CG, Cooper WO. Prescription opioid epidemic and infant outcomes. Pediatrics. 2015 May;135(5):842-50. doi: 10.1542/peds.2014-3299[↩]
- Sanlorenzo LA, Cooper WO, Dudley JA, Stratton S, Maalouf FI, Patrick SW. Increased Severity of Neonatal Abstinence Syndrome Associated With Concomitant Antenatal Opioid and Benzodiazepine Exposure. Hosp Pediatr. 2019 Aug;9(8):569-575. doi: 10.1542/hpeds.2018-0227[↩]
- Finnegan LP, Connaughton JF Jr., Kron RE, Emich JP. Neonatal abstinence syndrome: assessment and management. Addict Dis. 1975;2(1–2):141–158.[↩][↩]
- Lipsitz PJ. A proposed narcotic withdrawal score for use with newborn infants. A pragmatic evaluation of its efficacy. Clin Pediatr (Phila). 1975;14(6):592–594.[↩]
- Finnegan LP, Kron RE, Connaughton JF, Emich JP. Assessment and treatment of abstinence in the infant of the drug-dependent mother. Int J Clin Pharmacol Biopharm. 1975;12(1–2):19–32.[↩]
- Schuckit MA. Treatment of Opioid-Use Disorders. N Engl J Med. 2016 Jul 28;375(4):357-68. doi: 10.1056/NEJMra1604339[↩]
- Brat GA, Agniel D, Beam A, Yorkgitis B, Bicket M, Homer M, Fox KP, Knecht DB, McMahill-Walraven CN, Palmer N, Kohane I. Postsurgical prescriptions for opioid naive patients and association with overdose and misuse: retrospective cohort study. BMJ. 2018 Jan 17;360:j5790. doi: 10.1136/bmj.j5790[↩]
- Dydyk AM, Jain NK, Gupta M. Opioid Use Disorder. [Updated 2022 Jun 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553166[↩][↩][↩][↩][↩][↩]
- Dick DM, Agrawal A. The genetics of alcohol and other drug dependence. Alcohol Res Health. 2008;31(2):111-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3860452[↩]
- Sharma B, Bruner A, Barnett G, Fishman M. Opioid Use Disorders. Child Adolesc Psychiatr Clin N Am. 2016 Jul;25(3):473-87. doi: 10.1016/j.chc.2016.03.002[↩]
- Peechakara BV, Tharp JG, Gupta M. Codeine. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526029[↩]
- Mistry CJ, Bawor M, Desai D, Marsh DC, Samaan Z. Genetics of Opioid Dependence: A Review of the Genetic Contribution to Opioid Dependence. Curr Psychiatry Rev. 2014 May;10(2):156-167. doi: 10.2174/1573400510666140320000928[↩]
- John WS, Zhu H, Mannelli P, Schwartz RP, Subramaniam GA, Wu LT. Prevalence, patterns, and correlates of multiple substance use disorders among adult primary care patients. Drug Alcohol Depend. 2018 Jun 1;187:79-87. doi: 10.1016/j.drugalcdep.2018.01.035[↩]
- Ober AJ, Watkins KE, McCullough CM, Setodji CM, Osilla K, Hunter SB. Patient predictors of substance use disorder treatment initiation in primary care. J Subst Abuse Treat. 2018 Jul;90:64-72. doi: 10.1016/j.jsat.2018.04.004[↩]
- Johnson RE, Strain EC, Amass L. Buprenorphine: how to use it right. Drug Alcohol Depend. 2003 May 21;70(2 Suppl):S59-77. doi: 10.1016/s0376-8716(03)00060-7[↩]
- LeFevre ML; U.S. Preventive Services Task Force. Screening for hepatitis B virus infection in nonpregnant adolescents and adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014 Jul 1;161(1):58-66. doi: 10.7326/M14-1018[↩]
- Moyer VA; U.S. Preventive Services Task Force. Screening for hepatitis C virus infection in adults: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2013 Sep 3;159(5):349-57. doi: 10.7326/0003-4819-159-5-201309030-00672[↩]
- Moyer VA; U.S. Preventive Services Task Force*. Screening for HIV: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2013 Jul 2;159(1):51-60. doi: 10.7326/0003-4819-159-1-201307020-00645[↩]
- Meyerhoff DJ. Structural Neuroimaging in Polysubstance Users. Curr Opin Behav Sci. 2017 Feb;13:13-18. doi: 10.1016/j.cobeha.2016.07.006[↩]
- Rahimi-Movaghar A, Gholami J, Amato L, Hoseinie L, Yousefi-Nooraie R, Amin-Esmaeili M. Pharmacological therapies for management of opium withdrawal. Cochrane Database Syst Rev. 2018 Jun 21;6(6):CD007522. doi: 10.1002/14651858.CD007522.pub2[↩]
- Buprenorphine Quick Start Guide. https://www.samhsa.gov/sites/default/files/quick-start-guide.pdf[↩][↩]
- Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;(2):CD002207. doi:10.1002/14651858.CD002207.pub4[↩]
- How do medications to treat opioid use disorder work? https://nida.nih.gov/publications/research-reports/medications-to-treat-opioid-addiction/how-do-medications-to-treat-opioid-addiction-work[↩][↩][↩][↩][↩][↩]
- Center for Substance Abuse Treatment. Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2004. (Treatment Improvement Protocol (TIP) Series, No. 40.) Available from: https://www.ncbi.nlm.nih.gov/books/NBK64245[↩]
- Buprenorphine. https://www.samhsa.gov/medications-substance-use-disorders/medications-counseling-related-conditions/buprenorphine[↩][↩]
- Methadone. https://www.samhsa.gov/medications-substance-use-disorders/medications-counseling-related-conditions/methadone[↩][↩][↩]
- Mattick RP, Breen C, Kimber J, Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database Syst Rev. 2009;(3):CD002209. doi:10.1002/14651858.CD002209.pub2[↩]
- NIDA. 2018, January 17. Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). Retrieved from https://archives.nida.nih.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition[↩]
- Naltrexone. https://www.samhsa.gov/medications-substance-use-disorders/medications-counseling-related-conditions/naltrexone[↩][↩][↩]
- Bart G. Maintenance medication for opiate addiction: the foundation of recovery. J Addict Dis. 2012;31(3):207-225. doi:10.1080/10550887.2012.694598[↩]
- Davoli M, Bargagli AM, Perucci CA, et al. Risk of fatal overdose during and after specialist drug treatment: the VEdeTTE study, a national multi-site prospective cohort study. Addict Abingdon Engl. 2007;102(12):1954-1959. doi:10.1111/j.1360-0443.2007.02025.x[↩]
- Lions C, Carrieri MP, Michel L, et al. Predictors of non-prescribed opioid use after one year of methadone treatment: an attributable-risk approach (ANRS-Methaville trial). Drug Alcohol Depend. 2014;135:1–8. doi:10.1016/j.drugalcdep.2013.10.018[↩]
- Preston KL, Silverman K, Higgens ST, et al. Cocaine use early in treatment predicts outcome in a behavioral treatment program. J Consult Clin Psychol. 1998;66(4):691–696. doi:10.1037/0022-006x.66.4.691[↩]
- Ghitza UE, Epstein DH, Preston KL. Nonreporting of cannabis use: Predictors and relationship to treatment outcome in methadone maintained patients. Addict Behav. 2007;32(5):938–949. doi:10.1016/j.add-beh.2006.06.034[↩]
- Gandhi, D.H., Jaffe, J.H., McNary, S., Kavanagh, G.J., Hayes, M. and Currens, M. (2003), Short-term outcomes after brief ambulatory opioid detoxification with buprenorphine in young heroin users. Addiction, 98: 453-462. https://doi.org/10.1046/j.1360-0443.2003.00334.x[↩][↩]
- Sordo L, Barrio G, Bravo MJ, Indave BI, Degenhardt L, Wiessing L, Ferri M, Pastor-Barriuso R. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies. BMJ. 2017 Apr 26;357:j1550. doi: 10.1136/bmj.j1550[↩][↩]
- Fullerton CA, Kim M, Thomas CP, Lyman DR, Montejano LB, Dougherty RH, Daniels AS, Ghose SS, Delphin-Rittmon ME. Medication-assisted treatment with methadone: assessing the evidence. Psychiatr Serv. 2014 Feb 1;65(2):146-57. doi: 10.1176/appi.ps.201300235[↩]
- Sorensen JL, Copeland AL. Drug abuse treatment as an HIV prevention strategy: a review. Drug Alcohol Depend. 2000 Apr 1;59(1):17-31. doi: 10.1016/s0376-8716(99)00104-0[↩]





{kind=link}