
Contents
What is osteoid osteoma
Osteoid osteoma is a benign (noncancerous) bone tumor that usually develops in the long bones such as the femur (thighbone) and tibia (shinbone). The foot is less commonly affected (2-10%) with the talus being most commonly involved 1. Osteoid osteoma accounts for 10% of all benign bone tumors 2. Osteoid osteomas classically cause night pain and discomfort that is relieved by the use of over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs), e.g. aspirin, ibuprofen, and naproxen. Osteoid osteomas are benign (noncancerous) and do not spread throughout the rest of the body (metastasize). Osteoid osteomas can affect people of all ages but they occur more frequently in children (particularly adolescents) and young adults. Osteoid osteomas are usually found in children and adolescents, between the ages of 10 and 35 years 3. Osteoid osteomas account for ~10% of all benign bone lesions and there is a male predilection (M:F 2-4:1) 3.
Osteoid osteomas tend to be small, less than 1.5-2 cm in size and they do not grow. It is very rare to have two osteoid osteomas in the same patient 4. Osteoid osteoma do, however, typically cause a large amount of reactive bone to form around them. Osteoid osteoma also make a new type of abnormal bone material called osteoid bone. This osteoid bone, along with the tumor cells, forms the nidus of vascular osteoid with surrounding sclerotic bone, which is a clear spot seen on x-rays.
Osteoid osteomas are classified into cortical, cancellous, and subperiosteal subtypes. According to Musculoskeletal Tumor Society staging system for benign tumors, osteoid osteoma is a stage-2 lesion. It is classified as cortical, cancellous, or subperiosteal. Cortical lesions are most common 4.
Osteoid osteomas may occur in any bone in the body, but are most often found in the long bones of the leg such as the femur (thighbone) and tibia (shinbone). They are also found in the hands, fingers, and spine. Osteoid osteomas that occur in long bones are predominantly intracortical more often situated in the cortico-diaphyseal or metaphyseal regions, but other localizations such as intramedullary, subperiosteal, epiphyseal or apophyseal have also been noted 5. The majority of osteoid osteomas that present in the foot exhibit minimal periosteal reaction and are of the cancellous and subperiosteal subtypes. The size of the nidus is used to differentiate an osteoid osteoma from an osteoblastoma. Osteoblastomas are typically greater than 2 cm.
Osteoid osteomas may occur at any age, but it is most commonly found in individuals between the ages of 5 and 25 years of age. Males are affected approximately three times more often than females 6.
Figure 1. Osteoid osteoma X-ray

Footnote: Radiographs show increased cortical thickness involving the lower third of femoral shaft. There is also focal round lucente / lytic focus within the center of the sclerotic lesion suggestive of a nidus. Leg length discrepancy due to the lesion. Bilateral coxa valga
Figure 2. Osteoid osteoma CT scan
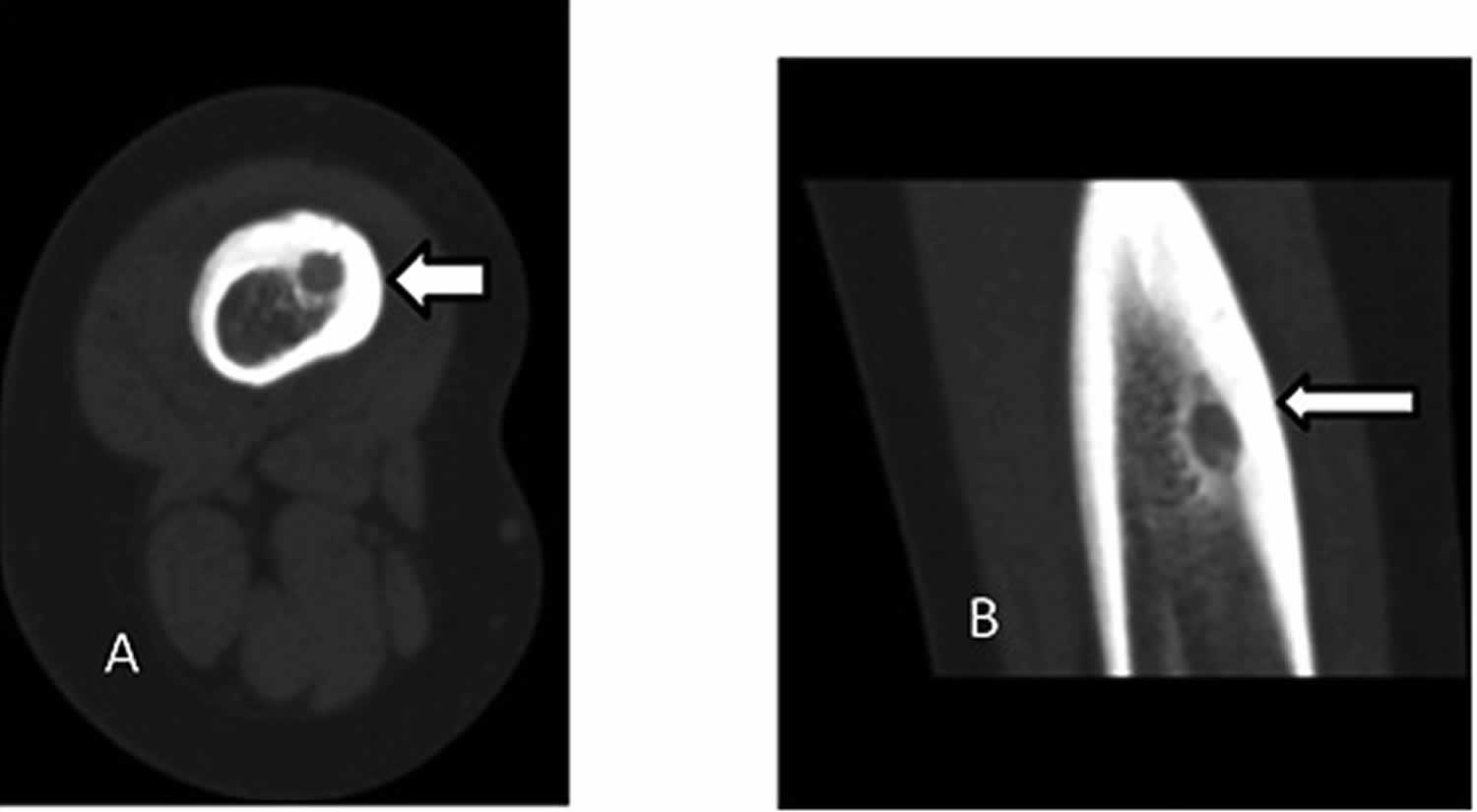
Footnote: A 14 years old boy osteoid osteoma of right femur. A) axial and B) coronal CT images show hypoattenuating nidus with surrounding sclerosis.
Figure 3. Osteoid osteoma bone scan (Technetium-99-labeled bone scintigraphy)
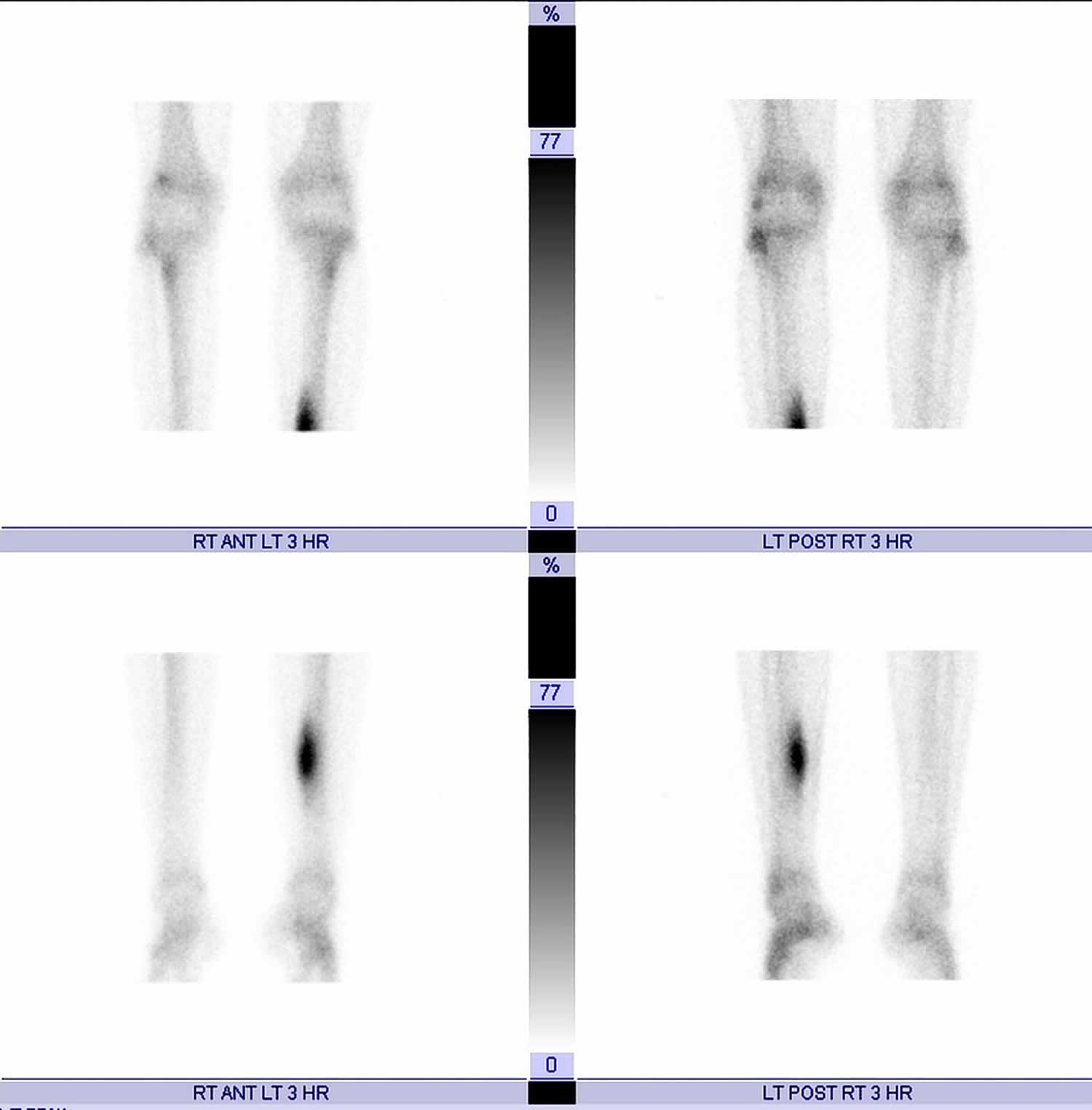
Footnote: 20 year old male with ongoing left mid-calf pain, aggravating at night. No prior medical or surgical history. Intense delayed focal uptake seen in the medial left mid-tibial cortex correlating with the thick periosteal reaction on the radiographs. At the epicenter of the increased uptake lies a 5 mm photopenic lesion located in the medial tibial cortex consistent with nidus of an osteoid osteoma.
[Source 7 ]Osteoid osteoma vs Osteoblastoma
Osteoblastoma consists of tissue histologically similar to that of an osteoid osteoma. Some experts simply consider them large osteoid osteomas (> 2 cm). Osteoblastoma is a rare benign (noncancerous) slow-growing bone tumor that dissolves normal, healthy bone and makes a new type of abnormal bone material called osteoid. This osteoid bone material builds up around normal bone. Because the osteoid bone is weaker than normal bone, the area surrounding the tumor becomes more vulnerable to fracture. A bone weakened by an osteoblastoma can break with just a minor injury. Osteoblastoma accounts for about 1% of all primary bone tumors that often develops in the posterior elements of the spine and the sacrum (40 to 55%) 8, as well as the legs, hands, and feet 9. In the appendicular sites, the proximal femur, distal femur, and proximal tibia are the most frequent. Osteoblastoma less commonly involves the tarsal bones (talus and calcaneum). The majority of the cases are intraosseous (medullary). Although osteoblastoma is considered a benign tumor, there have been very rare cases in which an osteoblastoma has transformed into a malignant (cancerous) tumor.
Osteoblastoma is much more common among males and appears typically between ages 10 and 35. The tumor develops in the bone of the spine, legs, hands, and feet. It is a slow-growing tumor that destroys normal bone. This tumor is painful.
Adolescents and young adults (mean age, 20 years) are most often affected by osteoblastoma 9. Osteoblastomas typically appear between the ages of 10 and 30 years, and are twice as common in males as in females.
Osteoblastomas generally grow slowly with minimal symptomatology, but aggressive lesions may cause severe symptoms such as soft tissue edema, joint stiffness, and contracture 9. Pain is the most common presenting symptom, and diagnosis may be delayed up to two years from the onset of symptoms 10. Osteoblastomas of the spine have similar symptoms to that of osteoid osteoma; namely back pain, scoliosis, and nerve root compression 11. The appendicular tumors also produce pain and/or swelling, but these symptoms may be mild enough to last for months before the patient will see a clinician. Toxic osteoblastoma is a very rare variant of osteoblastoma associated with systemic symptoms, including fever, anorexia, and weight loss.
Accurate diagnosis of osteoblastoma is critical in determining the appropriate treatment modality and prognosis. In most cases, the basis for diagnosis is from clinical, radiological and mainly histopathological examination. Osteoblastomas have a variable radiologic appearance ranging from indolent to very aggressive 10. Because osteoblastomas destroy healthy bone and can grow to a large size, treatment always involves surgery to remove the tumor. Treatment of osteoblastoma requires surgery, often curettage and bone grafting.
In general, osteoblastoma has a good prognosis with a local recurrence rate of about 15% to 20% 8 and patients are often cancer free after surgical treatments of intralesional curettage or marginal en bloc resection 12. The local recurrence rate for lesions that are treated with intralesional curettage may be as high as 10 to 20%. More aggressive-appearing lesions are treated with surgical en bloc resection and bony reconstruction. A variation called aggressive osteoblastoma is similar to osteosarcoma both radiographically and histologically.
Long-term follow-up of patients with osteoblastoma is essential due to recurrence 13. Osteoblastomas located near the central neural axis has a worse prognosis due to the difficulty of complete excision. Progression of osteoblastoma to osteosarcoma is exceptional but has been reported 8.
A number of factors can influence the diagnosis of aggressive osteoblastoma, including 13:
- Radiographic
- Clinical
- Pathologic features
Osteoid osteoma causes
The cause of osteoid osteomas remains uncertain. Some scientists believe it is a benign neoplasm while others maintain it is due to trauma or an inflammatory process.
A few hypotheses exist regarding the pathophysiology of osteoid osteomas. One proposal is that the formation of the tumor may be due to neoplasia or is the result of prior trauma to the area 1. Although a history of trauma has been evident in one-third of documented cases, further research is warranted to explore the relationship 14. Nerve fibers have been identified within the nidus by special immunohistochemical techniques and concentrate within the area of sclerosis surrounding the nidus 15. Nerve fibers are stimulated by increased blood flow to the area from the release of prostaglandins. Studies have shown prostaglandin levels to be 100 to 1000 times more than levels found in normal bone, resulting in localized pain to the area 15.
High levels of prostaglandin E2 and prostacyclin have been found within the nidus that is believed to cause local inflammation and vasodilatation. A study by Mungo et al. 16 revealed increased levels of cyclooxygenase-2 expression in nidus osteoblasts. Cyclooxygenase-2 inhibition is believed to be a mechanism by which NSAIDs provide symptomatic relief in osteoid osteomas. These inflammatory mediators may also contribute to perilesional sclerosis exhibited by most osteoid osteomas. In addition, high concentrations of intralesional unmyelinated nerve fibers have been implicated in the pathogenesis of the exquisite nocturnal pain. These processes probably function in parallel to produce the characteristic inflammatory symptoms 17.
Osteoid osteoma symptoms
Pain is the most common symptom. Usually it is a dull ache, which is unremitting and starts off as mild and intermittent that gradually increases in intensity and persistence. The pain has a tendency to become increasingly severe at night and usually responds to salicyclates (e.g., aspirin) and non-steroidal anti-inflammatory medications (NSAIDs). The pain is not usually activity-related. In some cases, a person will suffer the aching bothersome pain of an osteoid osteoma for years before seeing a doctor for diagnosis. If osteoid osteoma involves a bone in a subcutaneous location, then the patient usually presents with swelling, erythema and tenderness.
Swelling is the next most common symptom and is thought to be due to the increased vascular supply to the tumor from prostaglandin release within the nidus 18. Other symptoms include bone deformity, muscle atrophy, and gait disturbances. If the tumor is intra-articular or located close to a joint, synovitis, effusion, arthritic changes, and contractures may be present. Osteoid osteomas that affect the femur and tibia have been shown to cause a limb length discrepancy. In a study of 4 patients, the affected limb was longer than the unaffected limb. The authors postulated this was likely the result of increased blood supply to a lesion close to an open growth plate 12.
If the proximal femur or pelvis is involved, the patient can present with referred pain in the knee. Lesions that are within the joint or juxta-articular can present with synovitis. If this continues to progress, the patient can present with joint pain, flexion contracture, decreased range of motion, and a limp or antalgic gait. Sometimes in children, a limp may be the only presenting symptom. If the lesion involves the open physis, it can result in limb length discrepancy with potential coronal and/or sagittal malalignment.
Referred pain and muscle atrophy can result in misdiagnosis of a neurological disorder commonly seen in axial skeleton involvement with postural scoliosis due to paravertebral muscle spasm, which is reversible after treatment 19.
Osteoid osteoma diagnosis
Your doctor will perform a physical examination and use imaging studies and other tests to diagnose your tumor.
Osteoid osteoma radiology
As with any other bone tumor, plain radiography is the initial exam of choice. The appearance of an osteoid osteoma on plain film is classically a small, round, radiolucent nidus with surrounding sclerosis. The nidus itself may contain areas of calcification. Three-phase skeletal scintigraphy is an option if conventional radiographs are inconclusive 20. The “double density sign” is characteristic of an osteoid osteoma when evaluating three-phase bone scintigraphy; this is demonstrated as intense focal uptake centrally surrounded by an area of less intense uptake peripherally 20. Thin-slice CT imaging is considered the imaging modality of choice. CT scans are effective in identifying the anatomic location of the nidus. The characteristic finding on a CT scan is a target-shaped nidus 21. Bone marrow edema appreciated on MRI can mask the typical features of the tumor, and therefore, MRI is less useful than CT for the evaluation of osteoid osteomas. However, MRI is more accurate than CT in diagnosing cancellous lesions. Hosalkar et al. compared the diagnostic accuracy of MRI versus CT in a prospective study in children. They concluded the correct diagnosis of osteoid osteoma was only 3% with MRI images versus 67% of CT images 12.
X-rays. X-rays create clear pictures of dense structures such as bone and are helpful in diagnosing an osteoid osteoma. An x-ray of the painful area may reveal thickened bone surrounding a small central core of lower density—a distinctive characteristic of the tumor. Osteoid osteoma have a characteristic lucent nidus <2 cm and a surrounding solid periosteal reaction.
Computed tomography (CT) scan. A CT scan provides a cross-sectional image of your bone and can also be helpful in evaluating the lesion. A CT scan will commonly show the nidus—or center of the tumor.
Biopsy
A biopsy may be necessary to confirm the diagnosis of osteoid osteoma. In a biopsy, a tissue sample of the tumor is taken and examined under a microscope. Your doctor may give you a local anesthetic to numb the area and take a sample using a needle. A biopsy can also be performed as a small operation.
Osteoid osteoma histology
When removed intact, osteoid osteomas are usually small, and round to oval in shape 22. The cut surface is red to pink when fresh, and brown to granular after formalin fixation. They are well demarcated from the surrounding white sclerotic cortical bone. The nidus color is related to vascularity of intertrabecular areas. As osteoid osteomas are now treated by radiofrequency ablation, such intact specimens as described above are rarely received for histopathology 23.
Microscopically, the central nidus is comprised of highly vascularized bone and intertwined osteoid 18. Remodeling of the bone occurs through osteoblastic activity. In the periphery of the nidus, an area of lucency is visible due to resorption of bone from osteoclastic activity. New bone formation occurs around the nidus and appears as sclerotic bone.
Figure 4. Osteoid osteoma histology
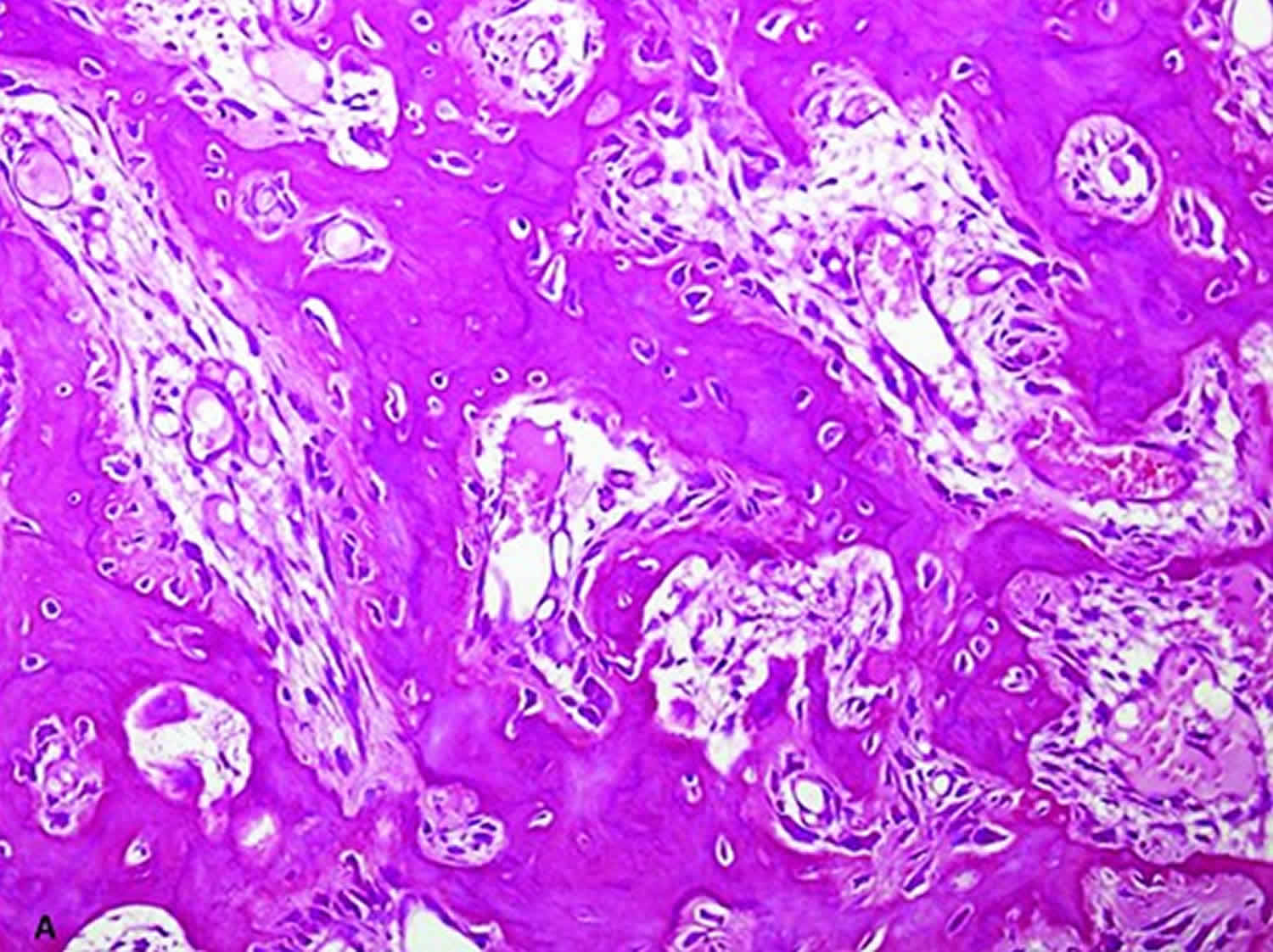
Footnote: Histology of osteoid osteoma. The nidus is composed of densely broad sclerotic bone trabecuale show osteoblastic rimming and fibrovascular connective tissue.
[Source 22 ]Other tests
To exclude other possible bone problems such as an infection or malignant tumor, your doctor may order additional imaging studies (e.g., bone scan). Certain blood tests may also be used to rule out an infection.
Bone scintigraphy (bone scan)
Technetium-99-labeled bone scintigraphy has high sensitivity for confirming diagnosis of osteoid osteoma. The sensitivity of skeletal scintigraphy for detection is 100% 24. On bone scan characteristic feature is very intense, round activity at nidus surrounded by less intensity of reactive bone. This is known as double density sign 25. The increased intensity of nidus is because of increased bone turn over. The less intense peripheral radiotracer uptake, represents the host bone tumor response. The sign is infrequently seen with spinal osteoid osteoma because of less peripheral sclerosis in vertebral bodies 26. A study done by PARK et al 27 found out that all the patients in their study with or without conclusive appearance on plain radiography, were correctly identified on bone scintigraphy. They recommended that if the radionuclide imaging is positive, CT scans should be next imaging modality for further evaluation but in cases where radionuclide imaging is negative, MRI should be done for the diagnosis of other underlying bone pathologies 27.
PET scan
PET may have role in initial diagnosis and post treatment follow-up. A study previously reported that tumor nidus exhibits 18FFDG-avid glucose metabolism, whereas the surrounding sclerosis does not. In follow up cases of radiofrequency ablation (RFA), hypermetabolic activity is absent. Some authors 28 suggested role of PET specifically in cases of spinal osteoid osteoma. But this modality requires more research work to be done to prove its utility in diagnosis and follow up.
In addition to FDGPET/CT, 68Ga- PSMA PET/CT, which is used in prostate cancer staging and restaging, has been used to detecta case of osteoid osteoma. This uptake was likely because of osteoblastic activity in osteoid osteoma but needs further evaluation to investigate its specific role and accuracy in diagnosis of osteoid osteoma 29.
Osteoid osteoma treatment
Nonsurgical treatment
Most osteoid osteomas will disappear on their own over several years. For some people, over-the-counter nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin, ibuprofen, and naproxen will provide pain relief.
Resolution of symptoms from conservative management has been documented to occur at 33 months 12. However, the negative effects of long term NSAID use prohibit it from being a definitive treatment. Furthermore, recurrence rates following the discontinuation of NSAIDs have no clear documentation in the literature.
Many patients, however, have painful symptoms that are not relieved by nonsteroidal anti-inflammatory drugs (NSAIDs), or don’t want to wait years for the tumor to shrink. In these cases, a patient or family may wish to consider surgery.
Surgical treatment
Surgical excision is the preferred treatment for an osteoid osteoma 18. Historically, open en bloc surgical resection with removal of the nidus was considered curative. However, wide block resection of bone in a weight-bearing area has disadvantages including prolonged restriction of physical activity, the potential for pathologic fracture, and requirement of bone grafting with internal fixation.
Less invasive surgical options have been explored to minimize damage to the normal, surrounding bone. Currently, the treatment of choice is CT guided percutaneous radiofrequency ablation 15. With the guidance of CT, the radiofrequency electrode gets inserted into the nidus, and the nidus is thermally ablated. Documented success with this procedure is as high as 90% 15.
Curettage
The standard surgical treatment for an osteoid osteoma is to scrape or scoop out the entire tumor, particularly the nidus—or central core. Your doctor will take great care to ensure that the entire tumor is removed; otherwise, it may grow back.
This is a traditional open procedure in which your surgeon makes an incision in the skin and soft tissues over the tumor site in order to reach the bone. In most cases, this type of surgery is highly successful. It does, however, carry risks including general anesthesia, infection, bleeding, and possible damage to surrounding tissues.
Radiofrequency ablation
A newer treatment option is to remove the center core of the tumor with minimally invasive techniques such as CT-guided radiofrequency ablation. In this outpatient procedure, the tumor is heated and destroyed with a high-frequency electrical current. The procedure can be done by either an interventional radiologist or an orthopaedic surgeon.
Before the procedure, you will be given either general anesthesia or a regional pain block with sedation. Your doctor will identify the site of the tumor using fine CT scans. A radiofrequency probe is then inserted into the tumor. The probe heats the tumor tissues to about 90 degrees Celsius, effectively killing them. There is minimal damage to surrounding tissues.
The tumor is adequately removed in most patients following one radiofrequency probe treatment. The procedure takes approximately 2 hours followed by a 2-hour recovery period, after which you may go home with a mild pain reliever.
Osteoid osteoma post surgery recovery
The time to return to daily activities will vary depending on the procedure and the location of the tumor. In many cases patients return to work or school in a few days with some restrictions. Your doctor will provide you with specific instructions to guide your recovery.
Osteoid osteoma prognosis
An osteoid osteoma has a good prognosis as it is a benign process with no potential for malignant degeneration. If conservative management fails, complete surgical excision is curative 18.
- Jordan RW, Koç T, Chapman AW, Taylor HP. Osteoid osteoma of the foot and ankle–A systematic review. Foot Ankle Surg. 2015 Dec;21(4):228-34.[↩][↩]
- Ren X, Yang L, Duan XJ. Three-dimensional printing in the surgical treatment of osteoid osteoma of the calcaneus: A case report. J. Int. Med. Res. 2017 Feb;45(1):372-380.[↩]
- Greenspan A, Jundt G, Remagen W. Differential diagnosis in orthopaedic oncology. Lippincott Williams & Wilkins. (2006) ISBN:0781779308.[↩][↩]
- Osteoid osteoma. Kitsoulis P, Mantellos G, Vlychou M. Acta Orthop Belg. 2006 Apr; 72(2):119-25.[↩][↩]
- The management of osteoid osteoma: updates and controversies. Ghanem I. Curr Opin Pediatr. 2006 Feb; 18(1):36-41.[↩]
- Gökalp MA, Gözen A, Ünsal SŞ, Önder H, Güner S. An Alternative Surgical Method for Treatment of Osteoid Osteoma. Med. Sci. Monit. 2016 Feb 22;22:580-6.[↩]
- Osteoid osteoma. https://radiopaedia.org/cases/osteoid-osteoma-23[↩]
- Lucas DR. Osteoblastoma. Arch. Pathol. Lab. Med. 2010 Oct;134(10):1460-6.[↩][↩][↩]
- Limaiem F, Singh R. Cancer, Osteoblastoma. [Updated 2019 Feb 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536954[↩][↩][↩]
- Sharma V, Chew FS, Hoch B. Periosteal osteoblastoma: Multimodal imaging of a rare neoplasm. Radiol Case Rep. 2009;4(4):329.[↩][↩]
- Nemoto O, Moser RP, Van Dam BE, Aoki J, Gilkey FW. Osteoblastoma of the spine. A review of 75 cases. Spine. 1990 Dec;15(12):1272-80.[↩]
- Atesok KI, Alman BA, Schemitsch EH, Peyser A, Mankin H. Osteoid osteoma and osteoblastoma. J Am Acad Orthop Surg. 2011 Nov;19(11):678-89.[↩][↩][↩][↩]
- Lu ZH, Cao WH, Qian WX. Aggressive osteoblastoma of the temporal bone: a case report and review of the literature. Clin Imaging. 2013 Mar-Apr;37(2):386-9[↩][↩]
- Gurkan V, Erdogan O. Foot and Ankle Osteoid Osteomas. J Foot Ankle Surg. 2018 Jul – Aug;57(4):826-832.[↩]
- Laurence N, Epelman M, Markowitz RI, Jaimes C, Jaramillo D, Chauvin NA. Osteoid osteomas: a pain in the night diagnosis. Pediatr Radiol. 2012 Dec;42(12):1490-501; quiz 1540-2.[↩][↩][↩][↩]
- COX-1 and COX-2 expression in osteoid osteomas. Mungo DV, Zhang X, O’Keefe RJ, Rosier RN, Puzas JE, Schwarz EM. J Orthop Res. 2002 Jan; 20(1):159-62.[↩]
- Mechanism of pain in osteoid osteomas: an immunohistochemical study. Hasegawa T, Hirose T, Sakamoto R, Seki K, Ikata T, Hizawa K. Histopathology. 1993 May; 22(5):487-91.[↩]
- Dookie AL, Joseph RM. Osteoid Osteoma. [Updated 2019 Jun 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537279[↩][↩][↩][↩]
- Osteoid osteoma. Boscainos PJ, Cousins GR, Kulshreshtha R, Oliver TB, Papagelopoulos PJ. Orthopedics. 2013 Oct 1; 36(10):792-800.[↩]
- Kumar R, Chandrashekhar N, Dasan JB, Ashok S, Rastogi S, Gupta V, Hadi M, Choudhury S. Recurrent osteoid osteoma: a case report with imaging features. Clin Imaging. 2003 Jul-Aug;27(4):269-72.[↩][↩]
- Lewis VO, Morris CD, Parsons TW. Malignant and benign bone tumors that you are likely to see. Instr Course Lect. 2013;62:535-49.[↩]
- Noordin S, Allana S, Hilal K, et al. Osteoid osteoma: Contemporary management. Orthop Rev (Pavia). 2018;10(3):7496. Published 2018 Sep 25. doi:10.4081/or.2018.7496 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6187004[↩][↩]
- Benign Bone-Forming Tumors: Approach to Diagnosis and Current Understanding of Pathogenesis. Bhusnurmath S, Hoch B. Surg Pathol Clin. 2012 Mar; 5(1):101-16.[↩]
- Wells RG, Miller JH, Sty JR. Scintigraphic patterns in osteoid osteoma and spondylolysis. Clin Nucl Med 1987;12:39-44.[↩]
- Helms CA. Osteoid Osteoma: The Double Density Sign. Clin Orthop Relat Res 1987;222:167-73.[↩]
- Roach P, Connolly L, Zurakowski D, Treves S. Osteoid osteoma: comparative utility of high-resolution planar and pinhole magnification scintigraphy. Pediatr Radiol 1996;26:222-5[↩]
- Park JH, Pahk K, Kim S, et al. Radionuclide imaging in the diagnosis of osteoid osteoma. Oncol Lett 2015;10:1131-4.[↩][↩]
- Farid K, El-Deeb G, Vigneron NC. SPECT-CT improves scintigraphic accuracy of osteoid osteoma diagnosis. Clin Nucl Med 2010;35:170-1.[↩]
- Castello A, Lopci E. Incidental identification of osteoid osteoma by 68Ga- PSMA PET/CT. Eur J Nucl Med Mol Imag 2017. [Epub ahead of print].[↩]





{kind=link}