Contents
- Can you get a pancreas transplant?
- Benefits of pancreas transplants
- Pancreas transplant risks
- Can a pancreas transplant cure diabetes?
- What will happen when I get a pancreas transplant?
- Indications for pancreas transplant and candidate selection
- During the pancreas transplant procedure
- After the pancreas transplant
- Pancreas transplant success rate
- Early and late post-pancreas transplant complications
- How to keep you and your pancreas healthy after pancreas transplant
Can you get a pancreas transplant?
Yes. More than 50,000 pancreas transplant have been performed worldwide (> 29,000 from the United States and >19,000 from other countries), and patient survival rates have improved significantly over time in all categories of recipients 1. A pancreas transplant is a surgical procedure to place a healthy pancreas from a deceased donor into a person whose pancreas no longer functions properly. Pancreas transplants are performed in patients who require insulin administration because of diabetes type 1 (a cellular autoimmune destruction beta cells), diabetes type 2 (resulting from impaired glucose regulation due to a combination of relative insulin deficiency and reduced insulin sensitivity) or total pancreatectomy 2.
Most pancreas transplants are done to treat type 1 diabetes. A pancreas transplant offers a potential cure for this condition. But it is typically reserved for those with serious diabetes complications, because the side effects of a pancreas transplant are significant.
In some cases, pancreas transplants may also treat type 2 diabetes. Rarely, pancreas transplants may be used in the treatment of pancreatic, bile duct or other cancers.
There are several different types of pancreas transplants:
- Combined kidney-pancreas transplant (simultaneous pancreas-kidney transplant). This transplant is for patients who have diabetes and kidney failure. This is the kind of transplant a patient has when there is no living kidney donor. Surgeons often may perform combined (simultaneous) kidney-pancreas transplants for people with diabetes who have or are at risk of kidney damage. More than two-thirds of pancreas transplants are done simultaneously with a kidney transplant. The goal of this approach is to give you a healthy kidney and pancreas that are unlikely to contribute to diabetes-related kidney damage in the future. But waiting for a donor pancreas and kidney to become available at the same time may increase time spent on the organ donor waiting list.
- Pancreas transplant after a kidney transplant. This is for patients with diabetes who have already had a kidney transplant (from a live or deceased donor). For those facing a long wait for both a donor kidney and pancreas to become available, a kidney transplant may be recommended first if a living- or deceased-donor kidney becomes available. If you get a kidney from a living donor, you will not have to spend as much time on dialysis. You may not even need dialysis. After you recover from kidney transplant surgery, you’ll receive the pancreas transplant once a donor pancreas becomes available.
- Pancreas transplant only (pancreas transplant alone). This transplant is for patients with diabetes who have major complications like dangerously low blood sugar or severe eye problems. This transplant is also for patients with diabetes who do not have kidney disease. A pancreas transplant surgery involves only a pancreas transplant without other surgeries.
- Pancreatic islet cell transplant. During pancreatic islet cell transplantation, insulin-producing cells (islet cells) taken from a deceased donor’s pancreas are injected into a vein that takes blood to your liver. More than one injection of transplanted islet cells is often necessary. Islet cell transplantation is an experimental procedure and may only be performed as part of a Food and Drug Administration-approved clinical trial.
Although it’s possible for a living donor to donate part of a pancreas, nearly all pancreas transplants involve a deceased-donor pancreas.
The doctors at your transplant center will help you decide which type of transplant is best for you.
Since the first pancreas transplant in December 1966, performed by Drs. William Kelly and Richard Lillehei, the majority (almost 80%) of pancreas transplants have been performed simultaneously with a kidney in diabetic and uremic patients 3. An additional 15% of pancreas transplants have been performed after a kidney transplant in diabetic and posturemic patients 2. Only ~8% of all pancreas transplants have been a pancreas transplant alone, performed in nonuremic patients with brittle (or labile) diabetes (including recurrent episodes of hypoglycemia and/or hypoglycemic unawareness) 2.
- According to the Organ Procurement and Transplantation Network, the overall survival rate at five years after pancreas transplant is about 91 percent.
- Survival rates vary by procedure type and transplant center. The Scientific Registry of Transplant Recipients maintains current statistics regarding transplantation for all U.S. transplant centers.
Pancreas rejection rates tend to be slightly higher among pancreas-only transplant recipients. It’s unclear why results are better for those who receive a kidney and pancreas at the same time. But some research suggests it may be because it’s more difficult to monitor and detect rejection of a pancreas alone versus a pancreas and a kidney.
If your new pancreas fails, you can resume insulin treatments and consider a second transplant. This decision will depend on your current health, your ability to withstand surgery and your expectations for maintaining a certain quality of life.
The reason simultaneous pancreas-kidney transplant are most common is that pancreas transplant with kidney transplant recipients are already obligated to immunosuppressive therapy by the kidney graft, so they incur only the added surgical risk of the pancreas transplant 2. A pancreas transplant alone is less commonly performed because only a relatively small percentage of insulin-dependent patients truly have brittle diabetes that cannot be controlled despite their own best efforts and the help of diabetologists, endocrinologists, and other health professionals. In general, pancreas transplant alone candidates have not yet developed advanced secondary complications of diabetes; yet, halting the development or progression of such complications significantly improves both quality of life and life expectancy (more so for pancreas transplant alone recipients than for pancreas transplant with kidney transplant or pancreas transplant after a kidney transplant recipients) 2.
Pancreas transplant alone recipients, in addition to the surgical risk of the pancreas transplant procedure itself, also incur the risk of immunosuppressive therapy (in the absence of a transplanted kidney graft). Immunosuppression in pancreas transplant alone recipients is required to prevent rejection (in order to establish insulin independence), to avoid hypoglycemic episodes, and to prevent the progression of secondary diabetes complications. Because of the required immunosuppressive therapy and its side effects—in the absence of advanced diabetic nephropathy—the pancreas transplant alone option has not been widely accepted 2. Moreover, in the first two decades after the first pancreas transplant alone was performed in 1968, pancreas transplant surgical risk was high, with considerable technical morbidity and poor outcomes 4. Only after the introduction of calcineurin inhibitors (and, specifically, tacrolimus) did the immunologic graft failure rates significantly decrease in pancreas transplant alone recipients. Despite improvements in exogenous insulin therapy, including the use of devices such as insulin pumps, the risk of hypoglycemic episodes (and their detrimental side effects) remains substantial in patients with brittle diabetes 5.
It is important to note that a pancreas transplant alone is not a procedure for every nonuremic, insulin-dependent patient. Most transplant centers offer a pancreas transplant alone only to patients with labile or brittle diabetes, defined as patients with 1) recurrent hypoglycemic episodes and/or hypoglycemic unawareness and 2) failure to improve on intensive exogenous insulin administration, including insulin pumps and other devices 2.
The pancreas transplant alone surgical technique has undergone significant changes since 1966. Enteric drainage, as in the early eras, is now again the most common technique for managing exocrine secretions, as a consequence of improved immunosuppressive therapy with tacrolimus and mycophenolate mofetil. In contrast, in era 1, which was dominated by cyclosporine maintenance immunosuppression, the less physiologic bladder drainage was the preferred technique; the reason was that exocrine rejection precedes endocrine rejection by several days, so a diagnosis of hypoamylasuria allowed successful rejection treatment before hyperglycemia could occur. By era 5, the vast majority of pancreas transplant alone recipients underwent systemic drainage—not portal drainage (despite systemic drainage’s association with hyperinsulinemia).
Benefits of pancreas transplants
- You may be able to maintain a normal blood glucose level without taking insulin.
- Many of the diabetes-related side effects are prevented or delayed.
- Most people with nerve damage who receive a pancreas transplant do not get worse and sometimes show improvement.
Pancreas transplant for diabetes type 1
Diabetes Type 1 is also called juvenile diabetes, because it is the diabetes type that affects children and young adults. With type 1 diabetes, the pancreas does not make insulin. People with type 1 diabetes must take daily insulin shots. About 1.7 million people have type 1 diabetes in the United States today.
Some patients with type 1 diabetes have experienced positive results from pancreas transplants. Typically, part or all of a new pancreas is surgically implanted. The old pancreas is left alone; it still makes digestive enzymes, even though it doesn’t make insulin. Most organs are obtained from someone who has died but has decided to be an organ donor.
A transplant of the pancreas is usually reserved for those with serious complications. Pancreas transplants are most often done when a patient also receives a new kidney. The pancreas transplant adds little further risk in this situation and offers big benefits. However, transplant surgery is risky. Each person needs to carefully weigh the potential benefits and risks.
Pancreas transplant for diabetes type 2
Diabetes Type 2 is type of diabetes that happens when your body cannot use insulin the right way or does not make enough insulin. People can often control type 2 diabetes with lifestyle changes like eating healthy and exercising. It is important to maintain a healthy weight. Some people may need to take pills, inject insulin, or both to control their diabetes. About 16 million Americans have type 2 diabetes.
A pancreas transplant usually isn’t a treatment option for people with type 2 diabetes, because type 2 diabetes occurs when the body becomes resistant to insulin or unable to use it properly rather than due to a problem with insulin production in the pancreas.
But for some people with type 2 diabetes who have both low insulin resistance and low insulin production, pancreas transplant is an emerging treatment option. About 10 percent of all pancreas transplants are performed in people with type 2 diabetes.
Note: Most transplant centers will perform a pancreas transplant on patients with type 1 diabetes but not diabetes type 2.
Pancreas transplant risks
- Your body treats the new pancreas as foreign and the immune system attacks the transplanted pancreas.
- Transplant patients must take powerful immunosuppressant drugs to prevent rejection of the new pancreas. Drugs that suppress the immune system can lower resistance to other diseases, such as cancer, and to bacterial and viral infections.
Complications of the procedure
Pancreas transplant surgery carries a risk of significant complications, including:
- Blood clots
- Bleeding
- Infection
- Excess sugar in the blood (hyperglycemia) or other metabolic problems
- Urinary complications, including leaking or urinary tract infections
- Failure of the donated pancreas
- Rejection of the donated pancreas
Anti-rejection medication side effects
After a pancreas transplant, you’ll take medications for the rest of your life to help prevent your body from rejecting the donor pancreas. These anti-rejection medications can cause a variety of side effects, including:
- Bone thinning (osteoporosis)
- High cholesterol
- High blood pressure
- Nausea, diarrhea or vomiting
- Sun sensitivity
- Puffiness
- Weight gain
- Swollen gums
- Acne
- Excessive hair growth or loss
All anti-rejection drugs work by suppressing your immune system, which also makes it harder for your body to defend itself against infection and disease.
Can a pancreas transplant cure diabetes?
After a successful pancreas transplant, your new pancreas will make the insulin your body needs, so you’ll no longer need insulin therapy to treat type 1 diabetes.
- You will no longer need insulin shots.
- You will be able to eat a regular diet.
- You will have fewer or no reactions from low blood sugar or insulin.
- You can be more active and independent.
- High blood sugar cannot damage your kidney, especially if you have already had a kidney transplant or will receive one with the pancreas transplant.
But even with the best possible match between you and the donor, your immune system will try to reject your new pancreas.
To avoid rejection, you’ll need anti-rejection medications to suppress your immune system. You’ll likely take these drugs for the rest of your life. Because medications to suppress your immune system make your body more vulnerable to infection, your doctor may also prescribe antibacterial, antiviral and antifungal medications.
Signs and symptoms that your body might be rejecting your new pancreas include:
- Belly pain
- Fever
- Excessive tenderness at the transplant site
- Increased blood glucose levels
- Vomiting
- Decreased urine output
If you experience any of these symptoms, notify your transplant team immediately.
It’s not unusual for pancreas transplant recipients to experience an acute rejection episode within the first few months after the procedure. If you do, you’ll need to return to the hospital for treatment with intensive anti-rejection medications.
What will happen when I get a pancreas transplant?
There are several steps to getting a transplant.
There are four steps involved in getting a pancreas transplant. Your transplant team will:
- Decide if you qualify for a new pancreas and are healthy enough for the operation.
- Prepare you for your operation.
- Perform the pancreas transplant.
- Help keep you and your pancreas healthy after the transplant.
Step 1. Decide if You Qualify for a New Pancreas and are Healthy Enough for the Operation
Before you get a pancreas transplant, you need to know that getting a transplant depends on your physical and mental health. It depends on the people who give you social support. It also depends on your ability to get the transplant medicines you need.
There are four parts to this step.
1) First, you will visit a transplant center.
You, your doctor, a nurse, or a social worker can schedule this visit. Your doctor’s office will send your medical records to the transplant center before your appointment. Your records should show that you are taking your medicine properly and are on a restricted diet. Your records will also confirm that you have no medical conditions that can keep you from receiving a transplant.
2) You will have a physical health evaluation.
A transplant doctor and transplant nurse coordinator will evaluate your medical condition. They will decide if you are healthy enough for surgery. They will need to know your medical history. They will need to evaluate how well you control your diabetes and how old you were when you were told you had it. They will talk with you about insulin and any problems you are having because of your diabetes.
Other tests you may have:
- Blood tests
- Chest x-ray
- Mammogram or prostate exam
- Colon exam
- EKG (electrocardiogram) and other heart tests
- You may have a stress test and a cardiac catheterization to look at your
- heart’s blood supply. This is done by inserting a catheter into an artery in
- your leg. Doctors may also test the blood supply to your legs.
- Your dentist may need to check your teeth and gums.
- Women will need an OB-GYN exam and Pap smear test.
- If you smoke, you will need to stop.
- You will need to stop any substance use.
- You may need to lose some weight. This is important because if you are overweight, you might go from having type 1 diabetes before transplant to having type 2 diabetes after your transplant. Your transplant team will tell you how much weight you need to lose.
3) You will have a mental health evaluation.
You may need to see a social worker or psychologist to make sure you are not addicted to alcohol or drugs. It is also important to make sure you have no emotional problems that can interfere with your health.
Step 2. Prepare You for Your Operation
This step involves finding a pancreas for you. This can sometimes take a long time.
Your transplant center may give you some handouts to read about your operation. This information will help you get ready for surgery. It will also tell you about your care after the operation.
While you are waiting for your pancreas transplant, it is important that you keep in touch with your transplant center. If your health condition changes, be sure to let the transplant center know. If you change medical insurance, you also need to call the center. It is very important that you notify your center immediately if you have an address or phone number change. The transplant center always needs to know how to contact you when an organ becomes available
It is very important to stay healthy while you wait for your new pancreas.
- If you smoke, please quit. If you need help quitting, talk to your regular doctor. Patients who smoke after a pancreas transplant do worse than those who do not smoke and many transplant centers will not perform pancreas transplants on people who continue to smoke.
- If you need to lose weight, ask your regular doctor to help you with a weight loss plan.
- Keep all your appointments.
- Do your best to control your blood sugar.
Step 3. Perform the pancreas transplant
During this surgery, a healthy pancreas (and kidney if you are getting them together) is placed inside your body. Surgeons will connect the pancreas to your own blood vessels. They will also connect the pancreas to either your own small intestine or your bladder so the pancreatic juices can drain. The operation will last three to six hours, depending on whether you are getting one or two organs.
Your own kidneys and pancreas will stay in your body. You will have a tube (catheter) inserted into your bladder. You will also have an IV (intravenous line) inserted into a vein in your arm and/or neck. You might also have a tube in your nose that drains to your stomach.
You will stay in the hospital until your doctor feels you are ready to go home. How long you stay in the hospital will depend on your health and how well the new organ(s) is working. It will also depend on how quickly you learn to take care of your new organ/s. The average stay in the hospital is seven to 12 days.
Indications for pancreas transplant and candidate selection
Pancreas transplant is performed with the aim of replacing the lost beta cell mass and hence restoring an endogenous source of servo regulated insulin production ensuring normal blood glucose 6. In addition, kidney transplantation may be required in patients with diabetes, due to the damage caused by diabetic nephropathy 6.
Pancreas transplantation, when technically successful, is expected to restore insulin independence in patients with diabetes, but at the expense of significant surgical morbidity and life-long immunosuppression 7. Therefore, pancreas transplant is indicated in selected patients with complicated diabetes, in whom the risks of surgery and immunosuppression are deemed to be lower than those of ineffective insulin therapy 7, which may be also influenced by genetic factors 8. Once a favorable risk/benefit balance has been established, additional benefits of pancreas transplant can also be appreciated on the side of improved quality of life 9.
Since the primary goal of pancreas transplant is restoring a critical mass of viable beta cells, the prototype recipient for this transplant is a patient with type 1 diabetes without detectable C-peptide. Recent evidence suggests that some patients with type 2 diabetes, but requiring high dose insulin and having low to mild insulin resistance (usually non- or mildly obese, may also regain insulin independence with pancreas transplant and enjoy benefits similar to those experienced by prototype recipients 7.
Because pancreas transplant is convenient only in patients in whom insulin-based therapies have failed, most recipients become transplant candidates after some 20-25-year history of diabetes 6. By this time, many of them have developed clinically relevant diabetic nephropathy and are often in end-stage renal failure. Ideally, these patients should receive a simultaneous pancreas-kidney transplant. Since nephropathy is a grim prognosticator in diabetic patients 10, simultaneous pancreas-kidney transplant is the therapy of choice for insulin-dependent patients with end-stage renal failure. Seventy-five percent of insulin-dependent patients do not survive longer than 5 years while receiving dialysis 11. However, simultaneous pancreas-kidney transplant improves patient survival compared to dialysis treatment or deceased donor kidney transplant 12.
When a live renal donor is available, a further option is to proceed with the kidney transplant first and then correct diabetes with a pancreas transplant 7. Actually, a live donor kidney and a deceased donor pancreas may be transplanted simultaneously but this option has high organizational needs, and has not been practiced frequently (Boggi U, Vistoli F, Egidi FM, Marchetti P, De Lio N, Perrone V, Caniglia F, Signori S, Barsotti M, Bernini M, Occhipinti M, Focosi D, Amorese G. Transplantation of the pancreas. Curr Diab Rep. 2012;12(5):568-79.)). Although sequential kidney and pancreas transplantation requires two surgical operations and a dual course of induction therapy, correcting uremia is key in these patients, and the chance of a kidney transplant should not be denied simply because of the wish to pursue the “ideal” pancreas-kidney transplant path. Furthermore, the excellent kidney function provided by a live donor kidney is especially rewarding in the fragile recipient with diabetes and uremia. The rationale for pancreas transplantation is to prevent the recurrence of diabetic nephropathy in the renal graft in the long-term period. Pancreas transplantation, however, is associated with all the typical complications of pancreas transplant which, paradoxically, may jeopardize renal function in the short-term period. Although there is no agreed cut-off of renal function to safely proceed with pancreas transplant, a stable renal function with a creatinine clearance of at least 60 ml/min/1.73 m2, and a negative urinanalysis are all very much welcome 7.
Selected patients with diabetes may also be considered for pancreas transplant alone when the kidney function is normal or “acceptable”. According to the American Diabetes Association, patients with brittle diabetes, suffering from hypoglycemia unawareness, and/or having medical or psychological problems with insulin therapy are eligible for pancreas transplant alone 13. Recent evidence suggests that patients having progressive diabetic complications (i.e. reversible nephropathy, progressive retinopathy, and severe neuropathy) may also significantly benefit from pancreas transplant alone 14. Whereas the impact of pancreas transplant alone on patient survival is still debated 15, in suitable recipients, pancreas transplant alone improves the course of diabetic retinopathy 16, diabetic neuropathy 14, and diabetic nephropathy 14, and reduces the level of cardiovascular risk 14. Regarding native renal function, the anticipated long-term improvement of diabetic nephropathy is thought to exceed the yet concrete risk of accelerated deterioration of renal function, which is mostly caused by the nephrotoxic effects of immunosuppressants 12.
All patients with diabetes who are potentially eligible for pancreas transplant are at high risk for cardiovascular disease, making cardiac and vascular work up key in this transplant population. In pancreas transplant alone recipients, great attention should be paid to the level of grafted and native renal function, respectively. In pancreas transplant alone, the risk of developing native kidney failure due to toxicity of immunosuppression is low with a glomerular filtration rate (GFR) greater than 60-70 ml/min 17. The indication to proceed with a solitary pancreas transplant (either pancreas transplant after a successful kidney transplant or pancreas transplant alone) should be well balanced against the inherent risk of a complex procedure such as pancreas transplant. On the contrary, there is no good medical reason to contraindicate a simultaneous pancreas-kidney transplant in patients with diabetes who have end stage renal failure, excluding the usual absolute contraindications to any type of transplant. These patients, if left on insulin and dialysis, do very poorly and die soon. Thus, the evaluation process should focus on exploring all possible venues permitting to each patient to receive his/her “life saving” simultaneous pancreas-kidney transplant. Sometimes, despite all efforts, a patient with diabetes and end-stage renal failure may be felt too sick to undergo any kind of transplant (including kidney transplant alone) with a reasonable chance of success. These are simply the patients in whom the transplant evaluation was started too late in the natural course of the diseases or in whom the disease pursued a very high-grade biologic course, with virtually no chance of rescue at any time.
During the pancreas transplant procedure
Surgeons perform pancreas transplants with general anesthesia, so you’re unconscious during the procedure. The anesthesiologist or anesthetist gives you an anesthetic medication as a gas to breathe through a mask or injects a liquid medication into a vein.
After you’re unconscious:
- An incision is made down the center of your abdomen.
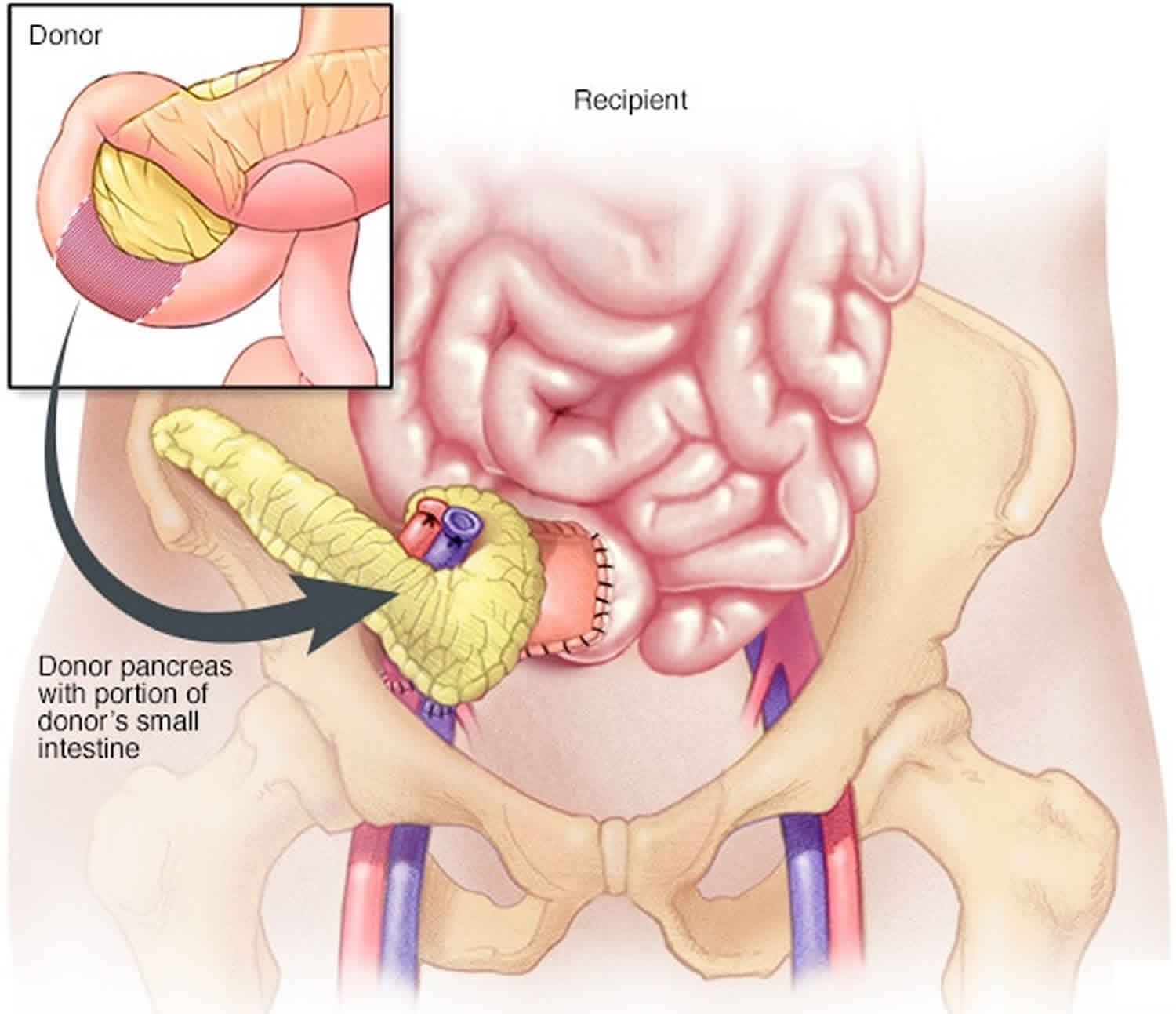
- The surgeon places the new pancreas and a small portion of the donor’s small intestine into your lower abdomen.
- The donor intestine is attached to either your small intestine or your bladder, and the donor pancreas is connected to blood vessels that also supply blood to your legs.
- Your own pancreas is left in place to aid digestion.
- If you’re also receiving a kidney transplant, the blood vessels of the new kidney will be attached to blood vessels in the lower part of your abdomen.
- The new kidney’s ureter — the tube that links the kidney to the bladder — will be connected to your bladder. Unless your own kidneys are causing complications, such as high blood pressure or infection, they’re left in place.
The surgical team monitors your heart rate, blood pressure and blood oxygen throughout the procedure with a blood pressure cuff on your arm and heart monitor leads attached to your chest.
Pancreas transplant surgery usually lasts about two to four hours. Simultaneous kidney-pancreas transplant surgery takes a few more hours.
After the procedure
After your pancreas transplant, you can expect to:
- Stay in the intensive care unit for a couple days. Doctors and nurses monitor your condition to watch for signs of complications. Your new pancreas should start working immediately, and your old pancreas will continue to perform its other functions. If you have a new kidney, it’ll make urine just like your own kidneys did when they were healthy. Often this starts immediately. But in some cases, it may take up to a few weeks to reach normal urine production.
- Spend about one week in the hospital. Once you’re stable, you’re taken to a transplant recovery area to continue recuperating. Expect soreness or pain around the incision site while you’re healing.
- Have frequent checkups as you continue recovering. After you leave the hospital, close monitoring is necessary for three to four weeks. Your transplant team will develop a checkup schedule that’s right for you. During this time, if you live in another town, you may need to make arrangements to stay close to the transplant center.
- Take medications for the rest of your life. You’ll take a number of medications after your pancreas transplant. Drugs called immunosuppressants help keep your immune system from attacking your new pancreas. Additional drugs may help reduce the risk of other complications, such as infection and high blood pressure, after your transplant.
After the pancreas transplant
After your operation, you will take strong immunosuppressive medicines every day to help your body accept the new transplant. Your body is smart and can detect that the organ comes from another person. These medicines will keep your body from rejecting the new pancreas. These medicines are called anti-rejection medicines. You will need to take these every day for as long as the transplanted organ is in your body. If you stop taking these medicines, even for a short period of time, your body will destroy your new pancreas. You must tell your transplant center if you miss or run out of your medicines.
Some tests you might need to have
Transplant ultrasound
With an ultrasound, doctors can see your pancreas, kidney, and blood supply on a screen. This shows them if there are any problems.
Transplant biopsy
Your doctors will biopsy your new organ. They use a needle to remove a tiny piece of kidney or pancreas. This piece is then looked at under a microscope. By looking at the cells, your doctors can find problems like rejection. This test also provides important information that will help the transplant team decide the best treatment for you.
CT Scan or Magnetic Resonance Scan
This test is used to see if you have a leak of digestive juices or an infection after a pancreas transplant. It can also be used to check the blood vessels going to your new pancreas.
Pancreas transplant success rate
Despite pancreas transplant invasive surgical nature, a pancreas transplant alone has become an extremely safe procedure 2. The risk of death within the first year post-transplant is now less than 2 percent (<2%), less than the risk of death on the waiting list while waiting for a pancreas transplant alone 18. Pancreas transplant alone results since the first such procedure more than four decades ago have significantly improved, with patient survival rates of almost 100% and graft function rates of up to 94% at 1 year. According to the newest analysis of the large population-based Allegheny County Type 1 Diabetes Registry (for patients diagnosed with diabetes type 1 from 1965 to 1979), the overall mortality rate is 812 deaths per 100,000 person-years and for pancreas transplant alone recipients, only 320 deaths per 100,000 19.
According to the International Pancreas Transplant Registry, unadjusted patient survival rates are >96% at 1 year post-transplant and >80% at 5 years 6. In some single center experiences, high actual patient survival at 10 years has been reported in both simultaneous pancreas-kidney transplant and pancreas transplant alone 20, 14. Cardiovascular and/or cerebrovascular problems and infections remain the leading causes of early (<3 months post-transplant) and late (>1-year post-transplant) death after pancreas transplant 21. In patients with type 1 diabetes, an simultaneous pancreas-kidney transplant has been shown in several studies to increase the observed versus expected lifespan, as compared with a kidney transplant alone 22. According to a large study of 13,467 patients that used data from the US Scientific Renal Transplant Registry and the US Renal Data System, the patient survival rate at 10 years post-transplant was significantly higher in recipients of simultaneous pancreas-kidney transplant than of kidney transplant from a deceased donor. In fact, recipients of simultaneous pancreas-kidney transplant had the greatest longevity (23.4 years), as compared with 20.9 years for recipients of a kidney transplant from a living donor and 12.8 years for recipients of a kidney transplant from a deceased donor 23.
In recipients of pancreas transplant after a successful kidney transplant, evidence shows that the pancreas transplant improves long-term patient and kidney graft survival rates. Also, glomerular filtration rates are significantly higher in the kidney graft of recipients of pancreas transplant after a successful kidney transplant than in recipients of kidney transplants alone 24 In recipients of pancreas transplant alone who have brittle diabetes mellitus, the mortality rate at 4 years is lower than that in the waiting list candidates 15. Earlier reports stating a survival disadvantage for recipients of solitary pancreas transplant (pancreas transplant alone and pancreas transplant after a successful kidney transplant) compared with patients on the waiting list for a transplant now seem to be unsubstantiated 25.
Pancreas graft survival rate is based on insulin independence. In the past decade, unadjusted graft survival rates at 1 year were 89% (simultaneous pancreas-kidney transplant), 86% (pancreas transplant after a successful kidney transplant) and 82% (pancreas transplant alone). The figures at 5 years were 71% (simultaneous pancreas-kidney transplant), 65% (pancreas transplant after a successful kidney transplant) and 58% (pancreas transplant alone) 21. More recently 14, 10-year actual insulin independence rates have been reported to be >80% in simultaneous pancreas-kidney transplant and >60% in pancreas transplant alone.
The most impressive improvements are seen in the gains over time in the estimated half-life (50% function) of pancreas grafts. The estimated half-life is now 14 years (simultaneous pancreas-kidney transplant), 7 years (pancreas transplant after a successful kidney transplant) and 7 years (pancreas transplant alone). Moreover, the estimated half-life has increased to 10 years in recipients of pancreas transplant after a successful kidney transplant or pancreas transplant alone with a functioning pancreas graft at 1 year post-transplant. The longest pancreas graft survival time, by category, has been 26 years (simultaneous pancreas-kidney transplant), 24 years (pancreas transplant after a successful kidney transplant) and 23 years (pancreas transplant alone).
The leading cause of pancreas loss is rejection 26. Autoimmunity is also increasingly recognized as a cause of beta cell failure 27. The diagnosis of pancreatic rejection is based on laboratory markers and imaging techniques with the understanding that the core biopsy remains the diagnostic gold standard tool. In simultaneous pancreas-kidney transplant, a rise in serum creatinine can be a surrogate for pancreas rejection suspicion; however, dyssynchronous kidney and pancreas rejection have been described 28. An increase in serum amylase and lipase, although not specific, can be an initial sign of pancreatic immune-activation. Hyperglycemia occurs only in cases of severe beta cell dysfunction or destruction, and therefore it is a late marker of rejection 29. Guidelines for the diagnosis of pancreas transplant rejection have been recently updated with major implementation for the identification of antibody-mediated rejection 30. Pancreatic antibody-mediated rejection is a combination of serological and immunohistological findings consisting of DSA detection, morphological evidence of microvascular injury, and C4d staining in interacinar capillaries. The newest Banff schema recognizes different patterns of immunoactivation, including the recurrence of autoimmune diabetes that is characterized by insulitis and/or selective beta-cell destruction. Among the different causes of graft loss, recent studies have proven that despite immunosuppression, the recurrence of autoimmune disease is not a rare event 27. Early experience with segmental pancreas transplant in identical twins without immunosuppression showed that autoimmune destruction of beta cells occurs early after pancreas transplant 31.
Immunosuppression prevents such recurrence in most, but not in all, patients 32.
Differently from the more frequent alloimmune reaction, producing graft rejection, recurrence of autoimmunity is characterized by isolated hyperglycemia without functional impairment of the exocrine pancreas or renal allograft function. In these patients, islet cell autoantibodies against GAD, IA-2, and ZnT8 antigens have usually persisted, have increased, or have reappeared after pancreas transplant 32, and are accompanied by the presence of circulating autoreactive CD4 or CD8 T-cells 33. Biopsy shows insulitis and beta-cell loss and lack features typically associated with graft rejection 32. Although the presence of autoantibodies does not contraindicate pancreas transplant, and most pancreas transplant recipients have detectable autoantibodies at the time of pancreas transplant, autoantibody conversion increases the risk of developing recurrent type 1 diabetes 32. In the presence of immunosuppression, rise of autoantibodies precedes hyperglycemia by several years 32.
Treatment options are nonspecific and include more sophisticated immunosuppressive therapies to target T-cells, B-cells, and autoantibodies. Plasmapheresis may be used to lower islet cell antibodies although, as shown in patients with newly diagnosed type 1 diabetes, the level of GAD autoantibodies may not be affected 32. Polyoma virus (BK) can induce a severe nephropathy (BKVN), an important cause of kidney graft loss following simultaneous pancreas-kidney transplant and pancreas transplant after a successful kidney transplant. Routine screening for BK viremia and early treatment in case of positivity may protect from BKVN development. Recent data have shown that calcineurin inhibitor and mycophenolate reduction and introduction of leflunomide may be crucial for stopping polyoma virus reactivation 34.
Graft failure of any organ has a negative impact on survival. In recipients of simultaneous pancreas-kidney transplant, kidney graft loss increases the relative risk of death by a factor of 17.6 and pancreas graft loss by a factor of 3.1. In recipients of pancreas transplant after a successful kidney transplant, kidney graft loss increases the relative risk of death by a factor of 4.3 and pancreas graft loss by a factor of 4.1. In recipients of pancreas transplant alone, pancreas graft loss increases the relative risk of death by a factor of 4.1 1.
Early and late post-pancreas transplant complications
The fragility of recipients with diabetes, with their high burden of medical comorbidities, the propensity of the pancreas allograft to vascular thrombosis, and the need to manage the exocrine secretions of the allograft contribute to the historically high rate of early complications of pancreas transplant after a successful kidney transplant. These events, although not always of surgical origin, often require surgical reintervention and are hence defined as the “surgical complications” of the procedure. However, their incidence has declined over time, although some 20% of patients still require at least 1 re-laparotomy after pancreas transplant after a successful kidney transplant 35. Fortunately, complications requiring allograft pancreatectomy, although still representing the leading cause of early graft loss 36, now occur in less than 5% of all recipients 35. Intuitively, graft survival is reduced in the recipients who develop surgical complications, but patient survival is not affected 35. Life threatening complications may still occur in around 3% of recipients, in the form of arterial pseudoaneurysm or arteroenteric fistula 37. Duodenal graft complications are a poorly reported complication of pancreas transplant after a successful kidney transplant, but are an important clinical problem as they can bring to graft loss and even to patient demise. A recently published manuscript shows that in the setting of delayed duodenal graft complications, of either septic or hemorrhagic origin, timely reintervention may permit graft rescue 38. Adoption of this policy requires early recognition of duodenal graft complications and the ability to remove the entire graft duodenum with individual drainage of the pancreatic duct in the bowel. Centers without these skills, or with insufficient experience, should send patients thought to have duodenal graft complications to qualified Institutions for attempted patient and graft rescue.
Over the past decade, patient and graft survival rates in pancreas transplant after a successful kidney transplant have significantly improved (see below). Nonetheless, malignancies and infections remain a significant cause of mortality and morbidity 39. In a recent study 40, the authors retrospectively analysed the incidence of a neoplasm among 360 diabetic subjects who consecutively underwent simultaneous pancreas-kidney transplantT in their institution. The overall 5-year patient survival was 84%. Twenty-five patients developed malignant tumors. Almost one-fourth of the cancers were represented by skin tumors (3 squamous cell and 4 basal cell carcinomas) and posttransplant lymphoproliferative disease was diagnosed in 5 recipients. The cumulative incidence of posttransplant lymphoproliferative disease from SRTR/Annual Data Report at 4 years is 2.3% after pancreas transplant alone, 0.9% after simultaneous pancreas-kidney transplant, and 1.1% after pancreas transplant after a successful kidney transplant. The higher frequency of posttransplant lymphoproliferative disease in pancreas transplant alone patients is likely related to their increased immunosuppression and higher rates of acute rejection 41. The incidence of other cancers is 3- to 4-fold higher compared with the background population 40.
How to keep you and your pancreas healthy after pancreas transplant
The most important part of the pancreas transplant is staying healthy after the pancreas transplant operation.
Here is what you will need to do after you leave the hospital:
- Visit the transplant center often and keep all your appointments.
- Take your medicines properly. This is very important. Also, do not take any other medicines (prescription or over-the-counter) or supplements of any kind without checking with your transplant team.
- Have your blood drawn and directed by your transplant center.
- Tell the staff at the transplant center about any problems you are having. Be sure to let them know if you have trouble keeping an appointment or taking your medicines. Call immediately if you are having trouble getting or taking your medicines (payment troubles, side effects). Your transplant center can help!
- Call your transplant center if you have any of these symptoms:
- Fever or chills
- Stomach pain
- Burning when you urinate
- High or low blood sugar
- Trouble breathing
- Bad cough
- Trouble taking your medicines
- High blood pressure
- Diarrhea, nausea, vomiting, or constipation
- Weight loss or weight gain
If your body begins to reject your new pancreas, you may not know it. Some patients may have signs, but most do not recognize them. If your body is rejecting the new pancreas or kidney, your doctors and nurses will know it. This is why it is so important to go to all your medical appointments. Your health care providers watch closely for signs of rejection and side effects from the medicines.
Your doctors will only be able to tell if you are rejecting the new organ by examining you. The doctor can detect rejection through blood tests or a biopsy. Your doctor and transplant staff will be watching for the following:
1. Rejection
The risk of rejection never goes away. You will always need to take anti-rejection drugs. Your doctor may lower the dosage, but you should never skip or stop taking the drugs.
2. Infections
Immunosuppressant drugs can increase the chance of getting infections. These infections can be treated. However, you need to tell your doctor if you have a fever, unusual pain, or any other new feelings. The risk of infection will go down when your doctor lowers the dosage.
3. High Blood Pressure
High blood pressure is a common problem after transplant. It can damage your kidneys. It can also cause strokes and heart attacks.
4. High Cholesterol
You may develop high cholesterol blood levels after transplant. This can put you at risk for a heart attack or stroke. Your health history and diet may contribute to this as well as some of your anti-rejection medicines. There are some medications called statins that control cholesterol and help prevent rejection because they also control inflammation.
5. Cancer
Transplant patients are at a greater risk for skin cancer. The anti-rejection medications can add to these chances. It is important that you use sunscreen lotions and wear clothing to protect your skin from the sun. It is also important for you to do other cancer screening such as pap smears and mammograms for women, and prostate screening for men. All patients should have their colon checked as recommended by your primary care physician.
6. Other health issues
Be sure to see your eye doctor for regular check-ups. You will need to also see other specialists on a regular basis. For example, doctors who specialize in feet, the brain and nerve system, and the endocrine system. Also, be sure to see your primary care doctor on a regular basis.
7. Pregnancy
It is possible to get pregnant after transplant, but you must talk with your transplant team to find out if pregnancy is safe for you. If you want to get pregnant, tell the transplant team before you stop using birth control. This is because some of your anti-rejection drugs may need to be changed before you get pregnant. If you find out you are pregnant, tell the transplant team right away. If your pancreas drains into your bladder, and you use a store-bought urine pregnancy test, it may test negative even if it is positive. Therefore, you need a blood test to be sure.
- Gruessner RW, Gruessner AC. The current state of pancreas transplantation. Nat Rev Endocrinol. 2013;9(9):555-62[↩][↩]
- Gruessner RW, Gruessner AC. Pancreas transplant alone: a procedure coming of age. Diabetes Care. 2013;36(8):2440-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3714504/[↩][↩][↩][↩][↩][↩][↩][↩]
- Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery 1967;61:827–837[↩]
- Gruessner AC, Sutherland DE, Gruessner RWG. Pancreas transplantation in the United States: a review. Curr Opin Organ Transplant 2010;15:93–101[↩]
- Golden SH, Sapir T. Methods for insulin delivery and glucose monitoring in diabetes: summary of a comparative effectiveness review. J Manag Care Pharm 2012;18(Suppl.):S1–S17[↩]
- Lombardo C, Baronti W, Amorese G, et al. Transplantation of the Pancreas. [Updated 2017 Dec 26]. In: Feingold KR, Anawalt B, Boyce A, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK278979[↩][↩][↩][↩]
- Boggi U, Vistoli F, Egidi FM, Marchetti P, De Lio N, Perrone V, Caniglia F, Signori S, Barsotti M, Bernini M, Occhipinti M, Focosi D, Amorese G. Transplantation of the pancreas. Curr Diab Rep. 2012;12(5):568-79.[↩][↩][↩][↩][↩]
- Freedman BI, Bostrom M, Daeihagh P, Bowden DW. Genetic factors in diabetic nephropathy. Clin J Am Soc Nephrol. 2007;2(6):1306-16.[↩]
- Gross CR, Gruessner AC, Treesak C. Quality of life for pancreas recipients. In: Gruessner RW, Sutherland DE, editors. Transplantation of the pancreas. New York (USA): Springer Verlag; 2004. p. 509-19.[↩]
- Allen KV, Walker JD. Microalbuminuria and mortality in long-duration type 1 diabetes. Diabetes Care. 2003;26(8):2389-91.[↩]
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725-30.[↩]
- White SA, Shaw JA, Sutherland DE. Pancreas transplantation. Lancet. 2009;373(9677):1808-17.[↩][↩]
- Robertson RP, Davis C, Larsen J, Stratta R, Sutherland DE; American Diabetes Association. Pancreas and islet transplantation in type 1 diabetes. Diabetes Care. 2006;29(4):935.[↩]
- Boggi U, Vistoli F, Amorese G, Giannarelli R, Coppelli A, Mariotti R, Rondinini L, Barsotti M, Signori S, De Lio N, Occhipinti M, Mangione E, Cantarovich D, Del Prato S, Mosca F, Marchetti P. Long-term (5 years) efficacy and safety of pancreas transplantation alone in type 1 diabetic patients. Transplantation. 2012;93(8):842-6.[↩][↩][↩][↩][↩][↩]
- Gruessner RW, Sutherland DE, Gruessner AC. Mortality assessment for pancreas transplants. Am J Transplant. 2004;4(12):2018-26.[↩][↩]
- Giannarelli R, Coppelli A, Sartini M, Aragona M, Boggi U, Vistoli F, et al. Effects of pancreas-kidney transplantation on diabetic retinopathy. Transpl Int 2005;18:619-22.[↩]
- Kim SJ, Smail N, Paraskevas S, Schiff J, Cantarovich M. Kidney function before pancreas transplant alone predicts subsequent risk of end-stage renal disease. Transplantation. 2014;97(6):675-80.[↩]
- Dean PG, Kudva YC, Stegall MD. Long-term benefits of pancreas transplantation. Curr Opin Organ Transplant 2008;13:85–90[↩]
- Secrest AM, Becker DJ, Kelsey SF, LaPorte RE, Orchard TJ. All-cause mortality trends in a large population-based cohort with long-standing childhood-onset type 1 diabetes: the Allegheny County type 1 diabetes registry. Diabetes Care 2010;33:2573–2579[↩]
- Gruessner AC, Gruessner RW. Pancreas transplant outcomes for United States and non United States cases as reported to the United Network for Organ Sharing and the International Pancreas Transplant Registry as of December 2011. Clin. Transpl. 2012:23-40[↩]
- Smets YF, Westendorp RG, van der Pijl JW, de Charro FT, Ringers J, de Fijter JW, Lemkes HH. Effect of simultaneous pancreas-kidney transplantation on mortality of patients with type 1 diabetes mellitus and end-stage renal failure. Lancet. 1999;353(9168):1915-9[↩][↩]
- Reddy KS, Stablein D, Taranto S, Stratta RJ, Johnston TD, Waid TH, McKeown JW, Lucas BA, Ranjan D. Long-term survival following simultaneous kidney-pancreas transplantation versus kidney transplantation alone in patients with type 1 diabetes mellitus and renal failure. Am. J. Kidney Dis. 2003;41(2):464-70[↩]
- Kleinclauss F, Fauda M, Sutherland DE, Kleinclauss C, Gruessner RW, Matas AJ, Kasiske BL, Humar A, Kandaswamy R, Kaul S, Gruessner AC. Pancreas after living donor kidney transplants in diabetic patients: impact on long-term kidney graft function. Clin. Transplant. 2009;23(4):437-46[↩]
- Oberholzer J, Tzvetanov G, Benedetti E. Surgical complication of pancreas transplantation. In: Hakim NS, Stratta RJ, Gray D, Friend P, Colman A, editors. Pancreas, islet, and stem cell transplantation for diabetes. New York: Oxford University Press; 2010. p. 179-89[↩]
- Venstrom JM, McBride MA, Rother KI, Hirshberg B, Orchard TJ, Harlan DM. Survival after pancreas transplantation in patients with diabetes and preserved kidney function. JAMA. 2003;290(21):2817-23.[↩]
- Burke GW 3rd, Vendrame F, Pileggi A, Ciancio G, Reijonen H, Pugliese A. Recurrence of autoimmunity following pancreas transplantation. Curr Diabet Rep. 2011;11(5):413-9[↩]
- Occhipinti M, Lampasona V, Vistoli F, Bazzigaluppi E, Scavini M, Boggi U, Marchetti P, Bosi E. Zinc transporter 8 autoantibodies increase the predictive value of islet autoantibodies for function loss of technically successful solitary pancreas transplant. Transplantation. 2011; 92:674-7[↩][↩]
- Drachemberg CB, Torrealba JR, Nankivell BJ, Rangel EB, Bajema IM, Kim DU, Arend L, Bracamonte ER, Bromberg JS, Bruijn JA, Cantarovich D, Chapman JR, Farris AB, Gaber L, Goldberg JC, Haririan A, Honsová E, Iskandar SS, Klassen DK, Kraus E, Lower F, Odorico J, Olson JL, Mittalhenkle A, Munivenkatappa R, Paraskevas S, Papadimitriou JC, Randhawa P, Reinholt FP, Renaudin K, Revelo P, Ruiz P, Samaniego MD, Shapiro R, Stratta RJ, Sutherland DE, Troxell ML, Voska L, Seshan SV, Racusen LC, Bartlett ST. Guidelines for the diagnosis of antibody-mediated rejection in pancreas allografts-updated banff grading schema. Am J Transplant. 2011;11(9):1792-802[↩]
- Egidi MF. Management of hyperglycaemia after pancreas transplantation. Are new immunosuppressants the answer? Drugs. 2005;65(2):153-6.[↩]
- Pugliese A, Reijonen HK, Nepom J, Burke GW 3rd. Recurrence of autoimmunity in pancreas transplant patients: research update. Diabetes Manag (Lond). 2011;1(2)229-38[↩]
- Santamaria P, Nakhleh RE, Sutherland DE, Barbosa JJ. Characterization of T lymphocytes infiltrating human pancreas allograft affected by isletitis and recurrent diabetes. Diabetes. 1992;41(1):53-61[↩]
- Vendrame F, Pileggi A, Laughlin E, Allende G, Martin-Pagola A, Molano RD, Diamantopoulos S, Standifer N, Geubtner K, Falk BA, Ichii H, Takahashi H, Snowhite I, Chen Z, Mendez A, Chen L, Sageshima J, Ruiz P, Ciancio G, Ricordi C, Reijonen H, Nepom GT, Burke GW 3rd. Recurrence of type 1 diabetes after simultaneous pancreas-kidney transplantation, despite immunosuppression, is associated with autoantibodies and pathogenic autoreactive CD4 T-cells. Diabetes. 2010;59(4):947-57[↩][↩][↩][↩][↩][↩]
- Marselli L, Dotta F, Piro S, Santangelo C, Masini M, Lupi R, Realacci M, del Guerra S, Mosca F, Boggi U, Purrello F, Navalesi R, Marchetti P. Th2 cytokines have a partial, direct protective effect on the function and survival of isolated human islets exposed to combined proinflammatory and Th1 cytokines. J Clin Endocrinol Metab. 2001; 86(10):4974-8.[↩]
- Mujtaba M, Fridell J, Sharfuddin A, Kandula P, Yaqub MS, Phillips CL, Mishler D, Taber T. polyoma virus (BK virus) nephropathy in simultaneous pancreas kidney transplant: a potentially preventable cause of kidney allograft loss. Clin Transplant. 2012;26(2): E87-93[↩]
- Banga N, Hadjianastassiou VG, Mamode N, Calder F, Olsburgh J, Drage M, Sammartino C, Koffman G, Taylor J. Outcome of surgical complications following simultaneous pancreas-kidney transplantation. Nephrol Dial Transplant. 2012;27(4):1658-63.[↩][↩][↩]
- Fernandez-Cruz L, Ricart MJ, Astudillo E, Sabater L, Fondevila C, Prados M. Enteric drainage as primary procedure and after cystoenteric conversion in whole pancreaticoduodenal transplantation. Transplant Proc. 1997;29(1-2):643-4.[↩]
- Fridell JA, Johnson MS, Goggins WC, Beduschi T, Mujtaba MA, Goble ML, Powelson J. Vascular catastrophes following pancreas transplantation: an evolution in strategy at a single center. Clin Transplant. 2012;26(1):164-72.[↩]
- Pieroni E, Napoli N, Lombardo C, Marchetti P, Occhipinti M, Cappelli C, Caramella D, Consani G, Amorese G, De Maria M, Vistoli F, Boggi U. Duodenal graft complications requiring duodenectomy after pancreas and pancreas-kidney transplantation. Am J Transplant. 2017 Dec 4. doi: 10.1111/ajt.14613[↩]
- Rostambeigi N, Kudva YC, John S, Mailankody S, Pedersen RA, Dean PG, Prieto M, Cosio FG, Kremers WK, Walker RC, Abraham RS, Stegall MD. Epidemiology of infections requiring hospitalization during long-term follow-up of pancreas transplantation. Transplantation. 2010;89(9):1126-33[↩]
- Girman P, Lipar K, KocikM, Kriz J, Marada T, Saudek F. Neoplasm incidence in simultaneous pancreas and kidney transplantation: a single-center analysis. Transplant Proc. 2011;43(9):3288-91[↩][↩]
- Caillard S, Lamy FX, Quelen C, Dantal J, Lebranchu Y, Lang P, Velten M, Moulin B; French Transplant Centers. Epidemiology of posttransplant lymphoproliferative disorders in adult kidney and kidney pancreas recipients: report of the French registry and analysis of subgroups of lymphomas. Am J Transplant. 2012;12(3):682-93[↩]





{kind=link}