Contents
What is periodontitis
Periodontitis is inflammation and infection of the ligaments and bones that support your teeth. Periodontitis is a form of severe gum disease. In periodontitis, your gums pull away from the teeth, forming pockets that become infected. Your body’s immune system fights the bacteria as the plaque spreads and grows below the gum line. The infection starts to break down the bone and connective tissue holding the teeth. If not treated, the bones, gums, and tissue are destroyed. Eventually the teeth loosen and may have to be removed.
Periodontitis is one of the main causes of tooth loss in adults and is the main cause of tooth loss in older people. Infection destroys the bone that holds the teeth in place. The erosion weakens the attachments and loosens the teeth. An affected tooth may eventually fall out or need to be pulled (extracted).
Many diseases and disorders, including diabetes (especially type 1 diabetes), Down syndrome, Crohn disease, leukopenia, and AIDS, can predispose a person to periodontitis. In people with AIDS, periodontitis progresses quickly. Smoking, vitamin C deficiency (scurvy), and emotional distress also are risk factors for periodontitis.
Periodontitis can affect people of any age, including young children. Some people have severe gingivitis for many years without developing periodontitis. Others may develop periodontitis, especially at early ages (20 to 30 years old), without first having significant gingivitis.
Chronic periodontitis affects 47.2% of adults over 30 in the United States. It can lead to the loss of tissue and bone that support the teeth and it may become more severe over time. If it does, your teeth will feel loose and start moving around in your mouth. This is the most common form of periodontitis in adults but can occur at any age. It usually gets worse slowly, but there can be periods of rapid progression.
Aggressive periodontitis is a highly destructive form of periodontal disease that occurs in patients who are otherwise healthy. Common features include rapid loss of tissue and bone and may occur in some areas of the mouth, or in the entire mouth.
Research between systemic diseases and periodontal diseases is ongoing. While a link is not conclusive, in some studies, researchers have observed that people with gum disease (when compared to people without gum disease) were more likely to develop heart disease or have difficulty controlling blood sugar. Other studies showed that women with gum disease were more likely than those with healthy gums to deliver preterm, low birth weight babies. But so far, it has not been determined whether gum disease is the cause of these conditions.
There may be other reasons people with gum disease sometimes develop additional health problems. For example, something else may be causing both the gum disease and the other condition, or it could be a coincidence that gum disease and other health problems are present together.
More research is needed to clarify whether gum disease actually causes health problems beyond the mouth, and whether treating gum disease can keep other health conditions from developing.
In the meantime, it’s a fact that controlling gum disease can save your teeth – a very good reason to take care of your teeth and gums.
How is periodontitis treated?
Have your teeth cleaned thoroughly by your dentist or periodontist. This may involve the use of various tools to loosen and remove plaque and tartar from your teeth.
Oral hygiene instruction and advice
- The aim of the oral hygiene phase of treatment is to reduce the number of bacteria in the mouth and therefore reduce the level of inflammation. Your dental practitioner will first explain the causes of your periodontitis and explain exactly how to keep your teeth and gums clean. You will be given individual advice on how to use the various cleaning aids most effectively; for example, the most appropriate tooth brushing technique and the correct use of dental floss and interdental brushes.
Professional cleaning
- All soft deposits will be removed from accessible areas of the teeth and the teeth polished and treated with fluoride. Depending on the improvement seen in plaque control and gum health, further instruction and cleaning may be carried out in subsequent visits. The next step would be for your practitioner to remove all bacterial deposits and tartar from the root surfaces and gingival pockets.
Antibiotic therapy
- In some cases, with or without microbiological evaluation, antibiotics are prescribed to deal with active or persistent gum infections, which have not responded to oral hygiene measures.
Reassessment
- After several weeks, your dentist or periodontist will make a full assessment of your gums to check the progress of your treatment. A special instrument called a periodontal probe is used to record the depth of any periodontal pockets and check for bleeding from the gums. If periodontal pockets are still present, further treatment options may be suggested, including surgical corrective therapy.
Corrective (surgical) treatment
- Sometimes, a surgical procedure is carried out to clean away plaque bacteria and deposits that are under the gum within periodontal pockets and on the root surfaces at the furcations (where the roots diverge). These areas are inaccessible to brushes and floss and inflammation will persist in these sites as long as bacteria are allowed to colonize them. Under local anaesthesia, the gum is lifted away and the root surfaces are cleaned under direct vision to ensure that all bacteria are removed. Sometimes, it is possible to treat bone loss at the same time using a special regenerative treatment. At the end of the procedure, the gums are sutured back into place around the teeth.
Periodontitis cure
Successful periodontal treatment requires your full co-operation in regard to daily oral hygiene practices and attendance at regular follow-up appointments.
Figure 1. Periodontitis

Figure 2. Tooth anatomy
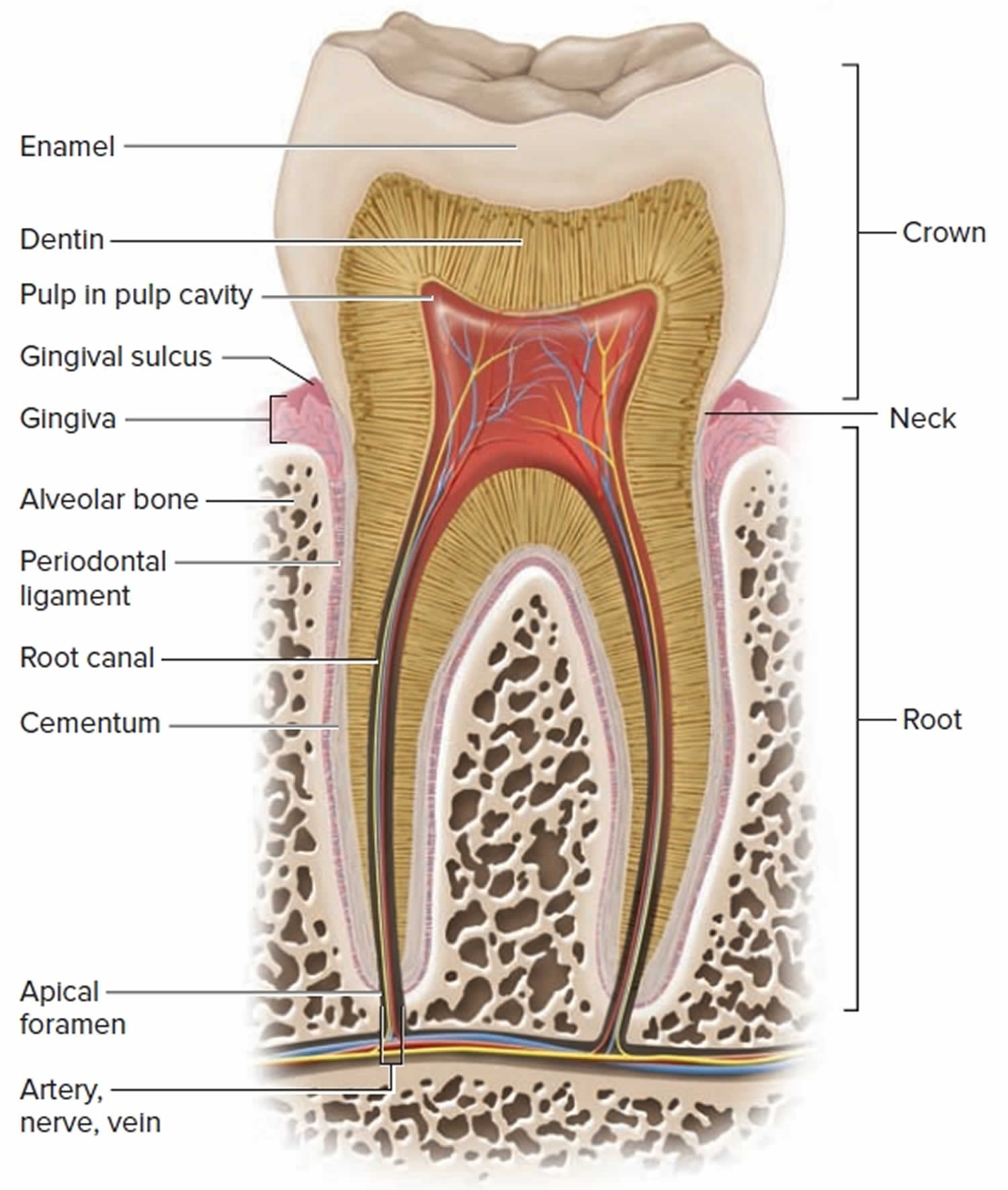 Figure 3. Stages of gum disease
Figure 3. Stages of gum disease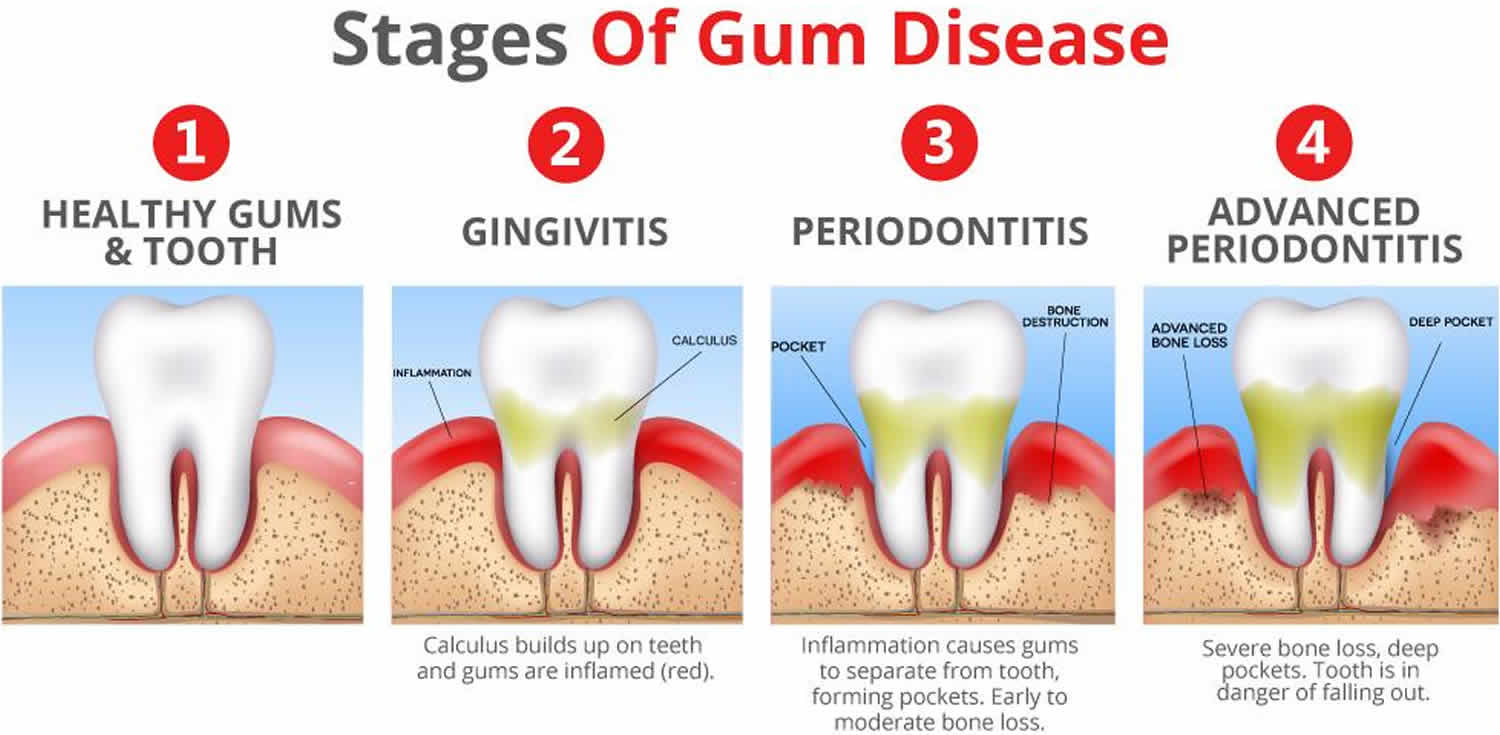
How can I recognise periodontitis?
Periodontitis always begins with inflammation of the gums, known as gingivitis. This is not always easy to recognize but one of the first signs that you may become aware of is bleeding from the gums when you brush your teeth. The gums may look red and swollen and you might notice a discoloured layer of bacterial plaque on the teeth.
Left untreated, gingivitis may progress to periodontitis, often without any obvious signs to alert you. However, some changes that you might experience over time include: increased bleeding from the gums, which may be provoked by brushing or eating, or even be spontaneous; bad breath; changes in the positioning of the teeth in the jaws; lengthening of the teeth (gum recession); and possibly pain. Bleeding from the gums may be less noticeable in smokers, because of the effect of nicotine on blood vessels, and so the disease process may be masked.
It often happens that the presence of periodontitis is not recognized by an individual until they are 40 or 50 years of age, by which time a great deal of damage may have occurred. However, a dentist is able to detect signs of the disease at a much earlier stage during a routine examination and can monitor your periodontal status using a special assessment known as the Periodontal Screening Index.
Figure 4. Stages of periodontitis
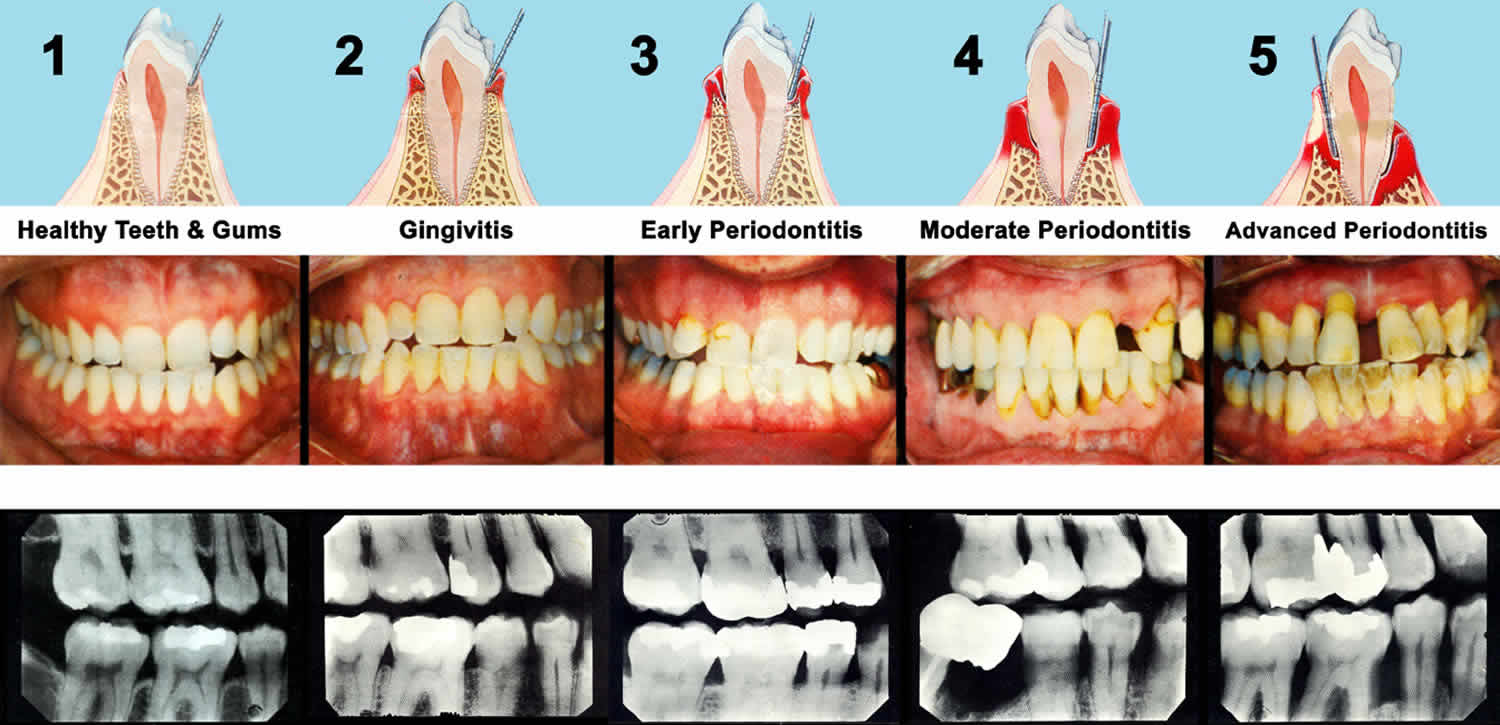
Footnote: Five illustrations of a cross section of a tooth, the outer gingival or gum tissue, the inner connective tissue which supports the tooth and a depiction of a graduated probe being inserted into the crevice or periodontal ‘pocket.’ The probe measures the pocket depth, giving the hygienist an idea of the severity of the decayed area. The redder color of the gum tissue at the neck of the tooth indicates inflammation, which increases with the severity of the condition. Notice how connective tissue is being destroyed during the progression. Periodontal disease is a seperate issue from caries or ‘tooth decay’ and caused by the infection of different pathogens, although lack of proper and thorough oral hygiene will promote the disease process in either case – and one can certainly exist without the other. For this reason, many may feel that, because they are not or no longer developing cavities, their oral health is not at risk. However, studies show that between 75% and 95% of all adults are suffering some stage of periodontal disease. The x-rays above show the progression of the disease. Note how, in the space between the teeth, the supporting tissue gradually disappears, looking from 1-5. By looking at only 1 and 5 you have a stark comparison of the loss of binding tissue.
The rate at which periodontitis develops differs considerably, even among people with similar amounts of tartar. Such differences occur because each person’s plaque contains different types and numbers of bacteria and because periodontitis results from the person’s unique immune system response to bacteria in the plaque. Periodontitis may cause bursts of destructive activity that lasts for months followed by periods when the disease apparently causes no further damage.
Gingivitis vs Periodontitis
Gingivitis is a mild form of gum disease. Gingivitis is an inflammation of the gums (gingiva) caused by plaque and bacteria accumulation. Bacteria in plaque around your teeth release enzymes (collagenases) that can damage and erode the gum tissues. The infected gums swell, bleed easily, recede, and loosen from the teeth. Tooth loss is caused more frequently by gum disease than tooth decay. Red, swollen and bleeding gums on brushing is an indication that you may have gingivitis (inflamed gums). Bad breath is another sign of gum disease. Usually gingivitis can be reversed with daily brushing and flossing and regular cleaning by a dentist or dental hygienist. Typically, there is no loss of bone or tissue that hold teeth in place.
Gingivitis is caused by plaque, which is a sticky layer of germs that builds up on teeth. Plaque irritates the gums, causing them to bleed easily. If the plaque is not brushed off, it can become hard and further irritate the gums. Hardened plaque is called calculus or tartar. The longer plaque and tartar remain, the more harmful they become. Plaque can only be removed by a dental health professional.
If you do not remove plaque, it turns into a hard deposit called tartar (or calculus) that becomes trapped at the base of the tooth. Plaque and tartar irritate and inflame the gums. Bacteria and the toxins they produce cause the gums to become infected, swollen, and tender.
These things raise your risk for gingivitis:
- Certain infections and body-wide (systemic) diseases
- Poor dental hygiene
- Pregnancy (hormonal changes increase the sensitivity of the gums)
- Uncontrolled diabetes
- Misaligned teeth, rough edges of fillings, and ill-fitting or unclean mouth appliances (such as braces, dentures, bridges, and crowns)
- Use of certain medicines, including phenytoin, bismuth, and some birth control pills
The most common cause of gingivitis is poor oral hygiene. Good oral health habits, such as brushing at least twice a day, flossing daily and getting regular dental checkups, can help prevent and reverse gingivitis. If you have an existing health condition, such as diabetes, you may be more likely to have oral hygiene problems such as gingivitis.
Gingivitis is reversible if treated. If left untreated, gingivitis will progress to an irreversible condition called periodontitis where the inflammation spreads to the bone supporting the teeth. Periodontitis may cause the area of the gum closest to the tooth to become weak. Spaces may form between the tooth and the gum, and these may trap germs, leading to even more swelling. Over time, the bone supporting the teeth can be lost, causing the teeth to become loose and possibly fall out.
How can I keep my teeth and gums healthy?
- Brush your teeth twice a day (with a fluoride toothpaste).
- Floss regularly to remove plaque from between teeth. Or use a device such as a special brush or wooden or plastic pick recommended by a dental professional.
- Visit the dentist routinely for a check-up and professional cleaning.
- Don’t smoke
Periodontitis causes
Most periodontitis is the result of inflammation of the gums (gingivitis) and a long-term accumulation of plaque (a filmlike substance made up primarily of bacteria) and tartar (hardened plaque) on the teeth and the gums. Pockets form between the teeth and gums and extend downward between the root of the tooth and the underlying bone. These pockets collect plaque in an oxygen-poor environment, which promotes, in people with certain immune system susceptibilities, the growth of aggressive forms of bacteria. The plaque and bacteria cause chronic inflammation that damages the tissue and bone that hold teeth in place. If the disease continues, eventually so much bone is lost that the tooth may become painfully loose and the gums recede. Tooth loss typically starts in a person’s 40s. Periodontitis is uncommon in young children, but it increases during the teen years.
Plaque and tartar build up at the base of the teeth. Inflammation from this buildup causes an abnormal “pocket,” or gap, to form between the gums and the teeth. This pocket then fills with more plaque, tartar, and bacteria. Soft tissue swelling traps the plaque in the pocket. Continued inflammation leads to damage of the tissues and bone surrounding the tooth. Because plaque contains bacteria, infection is likely, and a tooth abscess may also develop. This also increases the rate of bone destruction.
Risk factors for periodontitis
There are a number of factors that increase your chance of developing periodontitis and make it more likely to progress. Well-known risk factors include stress, some systemic diseases such as diabetes, and most importantly – smoking.
Smoking and periodontitis
- Smokers are significantly more likely to develop periodontitis than non-smokers.
- Periodontal treatments (such as gum/ bone grafts and implants) are less successful in smokers than non-smokers due to poorer healing.
- Periodontitis progresses much faster, with more rapid tooth loss, in smokers.
- Of cases of periodontitis which does not respond to treatment, about 90% are in smokers.
Periodontitis prevention
Good oral hygiene is the best way to prevent periodontitis. This includes thorough tooth brushing and flossing, and regular professional dental cleaning. Preventing and treating gingivitis reduces your risk of developing periodontitis.
The basic elements of a good oral hygiene regime are:
- Cleaning the chewing surfaces and sides of the teeth twice daily, with a toothbrush (of an appropriate size and in good condition) and toothpaste.
- Cleaning the spaces between the teeth where the toothbrush bristles cannot reach, using either dental floss or an interdental brush, depending on the size of the space. This should be done once daily.
Dental floss should be used where the teeth are close together, with little or no space between them, while interdental brushes are suitable for larger gaps. Special care should be taken to clean thoroughly around crooked or crowded teeth, or around fillings, crowns and dentures, as plaque accumulates readily in these places and access might be limited.
Antibacterial mouthwashes (non-alcoholic) are a useful supplement to brushing, as they inhibit bacterial growth and dampen inflammatory changes. They should be used after tooth brushing.
If, as a result of an inadequate cleaning technique, plaque deposits are left on the teeth, these will become mineralised and turn into hard, fixed deposits (calculus, commonly known as tartar) that cannot be removed with a toothbrush. Your dentist or periodontist will identify these tartar deposits during your regular dental inspection and remove them as part of a professional clean. After the deposits are removed, the teeth are polished with special pastes and cups to create a smooth surface that is less likely to accumulate plaque.
Periodontitis symptoms
The early symptoms of periodontitis are tender, swollen, bleeding, and red gums and bad breath (halitosis). As more and more bone is lost, the teeth loosen and shift position, and chewing becomes painful. Frequently, the front teeth tilt outward. Periodontitis usually does not cause pain unless an infection, such as a collection of pus (abscess) forms in a pocket, the teeth loosen enough to move while chewing, or the person has periodontitis caused by HIV.
Symptoms of periodontitis include:
- Bad breath odor (halitosis)
- Gums that are bright red or reddish-purple
- Gums that look shiny
- Gums that bleed easily (when flossing or brushing)
- Gums that are tender when touched but are painless otherwise
- Loose teeth
- Swollen gums
- Gaps between the teeth and gums
- Shifting teeth
- Yellow, brown green or white hard deposits on your teeth
- Tooth sensitivity
Note: Early symptoms are similar to gingivitis (inflammation of the gums).
Periodontitis possible complications
These complications can occur:
- Infection or abscess of the soft tissue
- Infection of the jaw bones
- Return of periodontitis
- Tooth abscess
- Tooth loss
- Tooth flaring (sticking out) or shifting
- Trench mouth
Periodontitis diagnosis
Your dentist will examine your mouth and teeth. Your gums will be soft, swollen, and reddish-purple. (Healthy gums are pink and firm.) You may have plaque and tartar at the base of your teeth, and the pockets in your gums may be enlarged. In most cases, the gums are painless or only mildly tender, unless a tooth abscess is also present. Your gums will be tender when checking your pockets with a probe. Your teeth may be loose and gums may be pulled back, exposing the base of your teeth.
Dental x-rays show the loss of supporting bone. They may also show plaque deposits under your gums.
How to treat periodontitis
The goal of treatment is to reduce inflammation, remove pockets in your gums, and treat any underlying causes of gum disease. Rough surfaces of teeth or dental appliances should be repaired.
Deep Cleaning (Scaling and Root Planing)
Your dentist, periodontist, or dental hygienist removes the plaque through a deep-cleaning method called scaling and root planing. Scaling means scraping off the tartar from above and below the gum line. Root planing gets rid of rough spots on the tooth root where the germs gather, and helps remove bacteria that contribute to the disease. In some cases a laser may be used to remove plaque and tartar. This procedure can result in less bleeding, swelling, and discomfort compared to traditional deep cleaning methods.
Flossing and brushing is always needed to reduce your risk for gum disease, even after professional tooth cleaning. Your dentist or hygienist will show you how to brush and floss properly. You may benefit from medicines that are put directly on your gums and teeth. People with periodontitis should have a professional teeth cleaning every 3 months.
People who have risk factors, such as poor oral hygiene, diabetes, and smoking, should receive treatment for these risk factors. Treatment of risk factors increases the success of the dentist’s treatments of periodontitis.
Unlike gingivitis, which usually disappears with good oral hygiene (daily brushing and flossing), periodontitis requires repeat professional care. People who have good oral hygiene can clean only 2 to 3 millimeters (1/12 inch) below the gum line. However, dentists can clean pockets up to 6 to 7 millimeters (¼ inch) deep using scaling and root planing techniques, which thoroughly remove plaque and tartar and the diseased root surface.
Surgical Treatments
Surgery may be needed to:
- Open and clean deep pockets in your gums
- Build support for loose teeth
- Remove a tooth or teeth so that the problem doesn’t get worse and spread to nearby teeth
For pockets 5 millimeters (1/5 inch) deep or more, surgery is often required. Dentists or periodontists may access the tooth below the gumline by surgically opening a flap of gum tissue (periodontal flap surgery). They thoroughly clean the teeth and correct bone defects (sometimes by bone grafting) under the flap and then sew the flap back in place. Dentists or periodontists may also remove part of the infected and separated gum (a gingivectomy) so that the rest of the gum can reattach tightly to the teeth and people can then remove the plaque at home. Sometimes teeth are removed (extracted). If the mouth is sore after surgery, a chlorhexidine mouth rinse used for 1 minute twice a day may be temporarily substituted for brushing and flossing.
Dentists may prescribe antibiotics (such as amoxicillin or metronidazole), especially if a collection of pus (abscess) has developed. Dentists may also insert materials (filaments or gels) that contain antibiotics into deep gum pockets, so that high concentrations of the drug can reach the diseased area. Periodontal abscesses cause a burst of bone destruction, but immediate treatment with surgery and antibiotics may allow much of the damaged bone to quickly grow back.
Flap Surgery
Surgery might be necessary if inflammation and deep pockets remain following treatment with deep cleaning and medications. A dentist or periodontist may perform flap surgery to remove tartar deposits in deep pockets or to reduce the periodontal pocket and make it easier for the patient, dentist, and hygienist to keep the area clean. This common surgery involves lifting back the gums and removing the tartar. The gums are then sutured back in place so that the tissue fits snugly around the tooth again. After surgery the gums will heal and fit more tightly around the tooth. This sometimes results in the teeth appearing longer.
Bone and Tissue Grafts
In addition to flap surgery, your periodontist or dentist may suggest procedures to help regenerate any bone or gum tissue lost to periodontitis. Bone grafting, in which natural or synthetic bone is placed in the area of bone loss, can help promote bone growth. A technique that can be used with bone grafting is called guided tissue regeneration. In this procedure, a small piece of mesh-like material is inserted between the bone and gum tissue. This keeps the gum tissue from growing into the area where the bone should be, allowing the bone and connective tissue to regrow. Growth factors – proteins that can help your body naturally regrow bone – may also be used. In cases where gum tissue has been lost, your dentist or periodontist may suggest a soft tissue graft, in which synthetic material or tissue taken from another area of your mouth is used to cover exposed tooth roots.
Since each case is different, it is not possible to predict with certainty which grafts will be successful over the long-term. Treatment results depend on many things, including how far the disease has progressed, how well the patient keeps up with oral care at home, and certain risk factors, such as smoking, which may lower the chances of success. Ask your periodontist what the level of success might be in your particular case.
Medications
Medications may be used with treatment that includes scaling and root planning, but they cannot always take the place of surgery. Depending on how far the disease has progressed, the dentist or periodontist may still suggest surgical treatment. Long-term studies are needed to find out if using medications reduces the need for surgery and whether they are effective over a long period of time.
Some medications that are currently used:
- Prescription mouthrinse containing an antimicrobial called chlorhexidine. It is used like a regular mouthwash to control bacteria when treating gingivitis and after gum surgery.
- Antiseptic chip: A tiny piece of gelatin filled with the medicine chlorhexidine. After root planing, it’s placed in the pockets where the medicine is slowly released over time to control bacteria and reduce the size of periodontal pockets.
- Antibiotic gel: A gel that contains the antibiotic doxycycline. The periodontist puts it in the pockets after scaling and root planing. The antibiotic is released slowly over a period of about seven days to control bacteria and reduce the size of periodontal pockets.
- Antibiotic microspheres: Tiny, round particles that contain the antibiotic minocycline. The periodontist puts the microspheres into the pockets after scaling and root planing. The particles release minocycline slowly over time to control bacteria and reduce the size of periodontal pockets.
- Enzyme suppressant: A low dose of the medication doxycycline that keeps destructive enzymes in check. Enzyme suppressant holds back your body’s enzyme response — if not controlled, certain enzymes can break down gum tissue. This medication is in tablet form. It is used in combination with scaling and root planing.
- Oral antibiotics: Antibiotic tablets or capsules for the short term treatment of an acute or locally persistent periodontal infection.
Aftercare – supportive periodontal therapy
The long-term success of periodontal treatment depends both on your own efforts with oral hygiene and those of the practice team who provide your regular care and ongoing assessment. After the first phase of treatment has been completed, your dentist will need to review the condition of your gums at regular intervals to check that the inflammation has been halted. The frequency of your follow-up appointments will depend on the severity of disease and your individual risk of disease progression. Usually, follow-up visits are scheduled for every three to six months.
Regular follow-up appointments are vitally important to ensure that the disease process does not recur, causing further destruction of the gums and supporting bone. If there are signs of continuing disease, your dentist will be able to identify new or recurring sites of inflammation and treat them at an early stage. You will also be given advice on how to modify your oral hygiene practices to tackle the inflammation.
Periodontitis prognosis
Some people find the removal of dental plaque from inflamed gums to be uncomfortable. You may need to be numb during this process. Bleeding and tenderness of the gums should go away within 3 to 4 weeks of treatment.
You need to perform careful home brushing and flossing for your entire life so that the problem does not return.





{kind=link}