Contents
- What is peripheral vascular disease
- Peripheral vascular disease causes
- Risk factors for peripheral vascular disease
- Peripheral vascular disease pathophysiology
- Peripheral vascular disease prevention
- Peripheral vascular disease signs and symptoms
- Peripheral vascular disease complications
- Peripheral vascular disease diagnosis
- Peripheral vascular disease treatment
What is peripheral vascular disease
Peripheral vascular disease involves damage to or blockage in the blood vessels distant from your heart—the peripheral arteries and veins. Your peripheral arteries and veins carry blood to and from your arm and leg muscles and the organs in and below your stomach area. Peripheral vascular disease may also affect the arteries leading to your head (carotid artery disease). When peripheral vascular disease affects only the arteries and not the veins, it is called peripheral arterial disease. The main forms that peripheral vascular disease may take include blood clots (for example, deep vein thrombosis or DVT), swelling (inflammation), or narrowing and blockage of the blood vessels.
Peripheral vascular diseases of the arteries may lead to:
- Arterial blockage (including peripheral artery disease)
- Aortic aneurysms
- Buerger’s Disease
- Raynaud’s Phenomenon
Peripheral vascular disease of the veins may lead to:
- Venous blood clots (including deep vein thrombosis or DVT)
- Pulmonary embolism
- Phlebitis
- Varicose veins
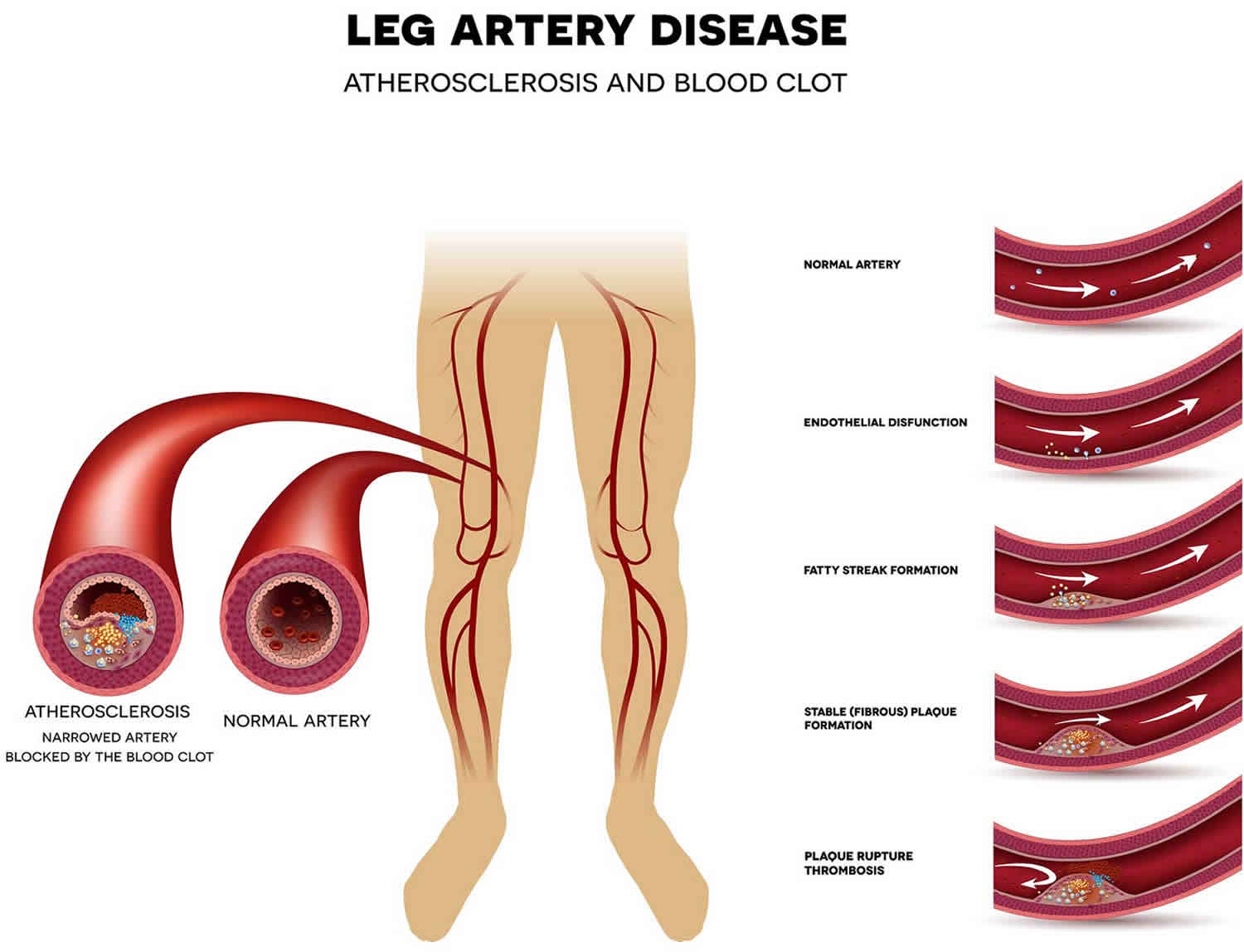
Peripheral artery disease is a common circulatory problem in which narrowed arteries reduce blood flow to your limbs. When you develop peripheral vascular disease, your extremities — usually your legs — don’t receive enough blood flow to keep up with demand. This causes symptoms, most notably leg pain when walking (intermittent claudication). Intermittent claudication is a tight, cramp like pain in the muscles of your calf, thigh or buttock which comes on only after walking and is relieved by resting 1. The pain is caused by diminished circulation or “poor circulation” to your lower limbs.
Peripheral vascular disease is also likely to be a sign of a more widespread accumulation of fatty deposits in your arteries (atherosclerosis). Atherosclerosis may be reducing blood flow to your heart and brain, as well as your legs.
In most cases of peripheral vascular disease, atherosclerotic plaques narrow the arterial flow lumen which restricts blood flow to the distal extremity. Reduced blood flow can cause thigh or calf pain with walking due to temporary ischemia of the leg muscles during exertion. Walking pain from peripheral vascular disease is referred to as intermittent claudication which means “to limp.” Many patients with peripheral vascular disease have either no symptoms or atypical complaints that do not strictly conform to the definition of claudication. Making the diagnosis of peripheral vascular disease even in asymptomatic patients still, has a significant clinical impact because peripheral vascular disease acts as a marker for systemic atherosclerosis. Patients with peripheral vascular disease have an equivalent cardiovascular risk to patients with previous heart attack (myocardial infarction) and require aggressive risk factor modification to improve their long-term survival 2.
The management of peripheral vascular disease varies depending on the disease severity and symptom status. Treatment options for peripheral vascular disease include lifestyle changes, cardiovascular risk factor reduction, pharmacotherapy, endovascular intervention, and surgery 3.
You often can successfully treat peripheral vascular disease by quitting tobacco, exercising and eating a healthy diet.
Peripheral vascular disease affects over 200 million adults worldwide and the incidence of peripheral vascular disease increases to as high as 20% in people over the age of 70 2. Although peripheral vascular disease has traditionally been perceived as a disease affecting men, the prevalence of peripheral vascular disease appears to be equal among senior men and women. Under-diagnosis of peripheral vascular disease in the primary care setting may be a significant issue, as most patients with peripheral vascular disease do not present with stereotypical claudication symptoms described in textbooks. Smoking increases the risk of developing peripheral vascular disease fourfold and has the greatest impact on disease severity. Compared to non-smokers, smokers with peripheral vascular disease have shorter life spans and progress more frequently to critical limb ischemia and amputation. Additional risk factors for peripheral vascular disease include diabetes, hyperlipidemia, hypertension, race, and ethnicity 4.
If you have leg pain, numbness or other symptoms, don’t dismiss them as a normal part of aging. Call your doctor and make an appointment.
Even if you don’t have symptoms of peripheral vascular disease, you may need to be screened if you are:
- Over age 65
- Over age 50 and have a history of diabetes or smoking
- Under age 50, but have diabetes and other peripheral vascular disease risk factors, such as obesity or high blood pressure
Peripheral vascular disease causes
Peripheral vascular disease is often caused by atherosclerosis. In atherosclerosis, fatty deposits (plaques) build up on your artery walls and reduce blood flow.
Although discussions of atherosclerosis usually focus on the heart, the disease can and usually does affect arteries throughout your body. When it occurs in the arteries supplying blood to your limbs, it causes peripheral vascular disease.
Less commonly, the cause of peripheral vascular disease may be blood vessel inflammation, injury to your limbs, unusual anatomy of your ligaments or muscles, or radiation exposure 5.
Risk factors for peripheral vascular disease
Factors that increase your risk of developing peripheral vascular disease include:
- Smoking
- Diabetes
- Obesity (a body mass index over 30)
- High blood pressure
- High cholesterol
- Increasing age, especially after reaching 50 years of age
- A family history of peripheral vascular disease, heart disease or stroke
- High levels of homocysteine, a protein component that helps build and maintain tissue
People who smoke or have diabetes have the greatest risk of developing peripheral vascular disease due to reduced blood flow.
Peripheral vascular disease pathophysiology
Peripheral vascular disease usually involves atherosclerotic disease in the abdominal aorta, iliac, and femoral arteries 2. The pathophysiology of atherosclerosis involves complex interactions between cholesterol and vascular cells the details of which are beyond the scope of this article. Atherosclerotic plaque builds up slowly on the inside of arteries. In the early stages of peripheral vascular disease, the arteries compensate for the plaque buildup by dilating to preserve flow through the vessel. Eventually, the artery cannot dilate any further, and the atherosclerotic plaque starts to narrow the arterial flow lumen.
The hemodynamic consequences of atherosclerosis depend on the degree of arterial narrowing. A 50% decrease in vessel diameter corresponds to a 75% loss of cross-sectional area which is usually considered flow limiting 2. As the narrowing progresses or completely obstructs the artery, blood flow shifts to smaller arteries which parallel the diseased artery. Although this collateral flow preserves distal perfusion, the network of smaller vessels never carries as much blood flow as the main artery. This blood flow restriction represents the hallmark of peripheral vascular disease and its typical symptoms. The muscles of the lower extremity require increased blood flow during ambulation to meet the increased energy demand. Patients with peripheral vascular disease reach a point during walking at which collateral blood flow is maximized and cannot provide any more perfusion to the lower extremity muscles. This supply-demand mismatch causes temporary ischemia of the muscles which manifests as pain, cramping, or fatigue and ultimately makes the patient with peripheral vascular disease slow down or stop walking. Lowering the energy demands of the muscle (by slowing or stopping) allows the blood supply to “catch up,” and the ischemic symptoms resolve. This cycle of blood flow restriction increased energy demand, and temporary muscle ischemia describes the pathophysiology of claudication due to peripheral vascular disease.
Patients with peripheral vascular disease usually have enough collateral blood flow that they only have symptoms during activities that increase energy demand such as walking. Rarely, peripheral vascular disease becomes progressively more severe, and the blood flow cannot meet the resting metabolic demands of the lower extremity. Poor perfusion to the nerves can result in ischemic rest pain which is often described as intractable, burning pain in the soles of the feet. Non-healing wounds and ischemic ulcers represent tissue loss due to poor blood flow. In the most severe cases, the toes or entire forefoot can become black and mummified as gangrene develops 6.
Peripheral vascular disease prevention
The best way to prevent claudication is to maintain a healthy lifestyle. That means:
- Quit smoking if you’re a smoker.
- If you have diabetes, keep your blood sugar in good control.
- Exercise regularly. Aim for 30 to 45 minutes several times a week after you’ve gotten your doctor’s OK.
- Lower your cholesterol and blood pressure levels, if applicable.
- Eat foods that are low in saturated fat.
- Maintain a healthy weight.
Peripheral vascular disease signs and symptoms
While many people with peripheral vascular disease have mild or no symptoms, some people have leg pain when walking (claudication).
Claudication symptoms include muscle pain or cramping in your legs or arms that’s triggered by activity, such as walking, but disappears after a few minutes of rest. The location of the pain depends on the location of the clogged or narrowed artery. Calf pain is the most common location.
The severity of claudication varies widely, from mild discomfort to debilitating pain. Severe claudication can make it hard for you to walk or do other types of physical activity.
Peripheral vascular disease signs and symptoms include:
- Painful cramping in one or both of your hips, thighs or calf muscles after certain activities, such as walking or climbing stairs (claudication)
- Leg numbness or weakness
- Coldness in your lower leg or foot, especially when compared with the other side
- Sores on your toes, feet or legs that won’t heal
- A change in the color of your legs
- Hair loss or slower hair growth on your feet and legs
- Slower growth of your toenails
- Shiny skin on your legs
- No pulse or a weak pulse in your legs or feet
- Erectile dysfunction in men
If peripheral vascular disease progresses, pain may even occur when you’re at rest or when you’re lying down (ischemic rest pain). It may be intense enough to disrupt sleep. Hanging your legs over the edge of your bed or walking around your room may temporarily relieve the pain.
Arterial blockage
Much like the coronary arteries, the peripheral arteries can be blocked by plaque. peripheral vascular disease can result from a condition known as atherosclerosis, where a waxy substance forms inside of the arteries. This substance is called plaque. When enough plaque builds up on the inside of an artery, the artery becomes clogged, and blood flow is slowed or stopped. This slowed blood flow may cause “ischemia,” which means that your body’s cells are not getting enough oxygen. Clogged peripheral arteries in the lower part of the body (also referred to as peripheral artery disease) most often cause pain and cramping in the legs. The risk factors for atherosclerosis in the peripheral arteries are the same as those for atherosclerosis in the coronary arteries. Smoking, diabetes, high blood pressure, and high cholesterol are believed to lead to the development of plaque.
Aortic aneurysms
An aneurysm is a balloon-like bulge in the wall of a weakened blood vessel. If the bulging stretches the vessel wall too far, the vessel may burst. The aorta is the artery that carries blood from the heart to the rest of the body. An aneurysm in the aorta is called an aortic aneurysm. You can die if an aneurysm causes this main artery to burst and it is not treated in time. An aortic aneurysm may be located in your chest (thoracic aneurysm), but most are located below the kidneys in the lower stomach area (abdominal aneurysms).
Buerger’s Disease
Buerger’s disease is related to smoking. The disease causes swelling of the small and medium-sized arteries (and sometimes the veins) in your feet and legs. This rare disorder, which causes the peripheral vessels to tighten or constrict, is more common in men, especially smokers aged 20 to 40. Smoking causes the blood vessels to tighten in everyone who smokes. But in people with Buerger’s disease, there is so much tightening in the vessels that a lack of oxygen to the cells (ischemia) or tissue death (necrosis) may result. The symptoms may be different for everyone, but the condition most often causes tender, swollen areas over the vessels, followed by coldness of the feet and hands. Pain in the legs during walking (called intermittent claudication) may happen because of an arterial blockage. The most serious cases sometimes cause the tissue to die, and amputation of the fingers and toes may be needed. People with Buerger’s disease must stop smoking completely, and circulation usually improves soon after.
Raynaud’s Phenomenon
Raynaud’s phenomenon happens more often in women. It is a circulation disorder that causes the arteries in the fingers and toes to tighten or spasm when they are exposed to cold temperatures, smoking, or emotional stress. Often, the cause of Raynaud’s phenomenon is not known. Sometimes, it is a side effect of other conditions, such as connective tissue disease, trauma, or diseases of the glands or central nervous system. People with the disorder may feel numbness or tingling in their fingers and toes. They may also notice that their skin turns pale or blue, followed by reddening in the affected areas. Attacks may last from a few minutes to several hours and are usually treated with gradual warming of the fingers and toes to restore blood flow. Therapy may also include pain relievers, calcium channel blockers, quitting smoking, and avoiding cold temperatures and emotional upset.
Venous blood clots
Nearly 6 million Americans have a blood clot in their veins (also called venous thrombus, venous thrombosis, or vein thrombosis). When the clot develops in a vein deep within the leg, it is called deep vein thrombosis (DVT). The condition can be life threatening if the clot breaks loose from the vein and travels to the lungs, where it can completely block blood flow.
Pulmonary embolism
Pulmonary embolism is caused by a blood clot (pulmonary embolus) that breaks loose from where it formed in a vein and travels to your lungs. Pulmonary embolism may have no symptoms, so it can cause sudden, unexpected death. When symptoms do happen, they may include
- Chest pain, especially when you breathe in
- Shortness of breath
- Coughing up blood
- Dizziness
- Fainting
Phlebitis
There are two forms of phlebitis. The most common form is swelling of a vein near the skin’s surface, usually in the leg. This is called superficial phlebitis. Swelling of the veins inside the leg is less common but more serious. This is called deep phlebitis. For superficial phlebitis, the area looks reddish and feels painful. The pain of this condition can usually be treated with moist heat, aspirin, or anti-inflammatory medicines. The more dangerous form of phlebitis, deep phlebitis, usually causes greater pain. People with deep phlebitis tend to have a fever. Nuclear scans, venous Doppler flow studies, or the use of a blood pressure cuff around the leg to measure blood flow (plethysmography) will usually confirm if the deep veins are involved. This type of phlebitis is more likely to lead to blood clots in the veins and a possible blood clot in the lungs (pulmonary embolus). If you are diagnosed with deep phlebitis, doctors will usually give you a week-long treatment with a blood-thinning, or anticoagulant, medicine. During this time, doctors will also check for signs of blood clots in your lungs. Your doctor will probably give you an anticoagulant in pill-form to be taken longer-term.
Varicose veins
Varicose veins are swollen, purple veins in the legs that are visible under your skin. They are caused by damage to blood vessels close to the surface of your skin, slowed blood flow, or the damage or absence of normal valves in your veins. Normally, blood flow in the veins is aided by valves, which keep the blood moving upward, against the force of gravity. If these valves are weak or blood flows slowly in the veins, the blood may pool and cause the veins to bulge. Varicose veins are more common in women than in men. The condition also runs in families. Pregnant women may get varicose veins because of hormonal changes and the extra pressure that the baby puts on the lower-stomach area. Varicose veins may also be caused by being severely overweight or by standing for long periods.
Peripheral vascular disease complications
If your peripheral vascular disease is caused by a buildup of plaques in your blood vessels (atherosclerosis), you’re also at risk of developing:
- Critical limb ischemia. This condition begins as open sores that don’t heal, an injury, or an infection of your feet or legs. Critical limb ischemia occurs when such injuries or infections progress and cause tissue death (gangrene), sometimes requiring amputation of the affected limb.
- Stroke and heart attack. The atherosclerosis that causes the signs and symptoms of peripheral vascular disease isn’t limited to your legs. Fat deposits also build up in arteries supplying blood to your heart and brain.
- Blood clots
- Erectile Dysfunction
- Infection
- Ulceration
Limb ischemia
Limb ischemia (lacking blood supply) occurs when blood flow to the limbs is severely restricted by fatty deposits on artery walls. It only happens in severe cases of peripheral vascular disease, and is a very serious situation.
Symptoms include:
- A severe burning pain in your legs and feet even when you are resting; the pain often occurs at night and episodes of pain can last several hours.
- Your skin turns pale, shiny, smooth and dry.
- You have wounds and ulcers (open sores) in your feet and legs that show no sign of healing.
- The muscles in your legs begin to waste away.
- The skin on your toes or lower limbs become cold and numb and turns reddish and then black or begins to swell and produce foul-smelling pus, causing severe pain.
If you think you are developing the symptoms of limb ischemia, contact your doctor immediately.
Treatment includes angioplasty or bypass graft. However, these may not always be successful and you may later require an amputation below the knee.
It is an extremely serious complication that can be challenging to treat and if combined with an infection can result in death.
Heart attacks or stroke
The cause of your peripheral vascular disease can also affect the arteries supplying blood to your heart and brain. If you have the condition, you’re more likely to have angina, a heart attack, a stroke or coronary heart disease.
Peripheral vascular disease diagnosis
Some of the tests your doctor may rely on to diagnose peripheral vascular disease are:
- Physical exam. Your doctor may find signs of peripheral vascular disease during a physical examination, such as a weak or absent pulse below a narrowed area of your artery, whooshing sounds (bruits) over your arteries that can be heard with a stethoscope, evidence of poor wound healing in the area where your blood flow is restricted, and decreased blood pressure in your affected limb.
- Ankle-brachial index (ABI). This is a common test used to diagnose peripheral vascular disease. As its name implies, the ankle-brachial index (ABI) compares the systolic blood pressure in your ankle to the systolic pressure in your arm. To get a blood pressure reading, your doctor uses a regular blood pressure cuff and a special ultrasound device to evaluate blood pressure and flow. You may walk on a treadmill and have readings taken before and immediately after exercising to capture the severity of the narrowed arteries during walking. A manual blood pressure cuff should be placed just above the ankle while locating the posterior tibial artery or dorsalis pedis artery with a handheld Doppler probe. While listening to the Doppler signal, the blood pressure cuff is inflated until it obliterates the Doppler signal. As the cuff slowly deflates, the pressure at which the Doppler signal returns is recorded as the systolic ankle pressure. The same steps are repeated for the other pedal artery and your other leg. Likewise, the brachial pressure can be measured with a blood pressure cuff on the upper arm and a Doppler probe positioned over the radial or ulnar artery at your wrist. The ankle-brachial index (ABI) is the highest systolic pressure measured at each ankle divided by the higher of the two systolic brachial pressures. A normal ankle-brachial index (ABI) ranges from 0.9 to 1.3. peripheral vascular disease is defined as an ABI less than 0.9 and most patients with claudication have an ABI between 0.5 and 0.9. Patients with extremely low ABI’s (less than 0.5) usually have ischemic rest pain or tissue loss. An ABI greater than 1.3 indicates arterial wall stiffening which can occur in patients with diabetes or renal failure. If a cuff pressure of 250mmHg does not obliterate the Doppler signal, the ABI is classified as “non-compressible.” Patients with falsely elevated (greater than 1.3) or non-compressible ABI’s require alternative imaging or physiologic studies to confirm the diagnosis of peripheral vascular disease 7.
- A common mistake when taking an ankle-brachial index (ABI) involves failure to measure the brachial pressure in both arms. Using the higher brachial pressure as the denominator for both ankle pressures ensures that the ankle-brachial index will not be underestimated in patients with upper extremity blood pressure discrepancy due to subclavian artery stenosis. Other measures to increase the accuracy of the ankle-brachial index include having the patient rest supine for at least 5 minutes to allow their blood pressure to stabilize and choosing an appropriately sized blood pressure cuff. The bladder length of the cuff should be 80%, and the width 40% of the circumference of the extremity.
- Ultrasound. Special ultrasound imaging techniques, such as Doppler ultrasound, can help your doctor evaluate blood flow through your blood vessels and identify blocked or narrowed arteries.
- Angiography. Using a dye (contrast material) injected into your blood vessels, this test allows your doctor to view blood flow through your arteries as it happens. Your doctor is able to trace the flow of the contrast material using imaging techniques, such as X-ray imaging or procedures called magnetic resonance angiography (MRA) or computerized tomography angiography (CTA). Catheter angiography is a more invasive procedure that involves guiding a catheter through an artery in your groin to the affected area and injecting the dye that way. Although invasive, this type of angiography allows for simultaneous diagnosis and treatment. After finding the narrowed area of a blood vessel, your doctor can then widen it by inserting and expanding a tiny balloon or by administering medication that improves blood flow.
- Blood tests. A sample of your blood can be used to measure your cholesterol and triglycerides and to check for diabetes.
Peripheral vascular disease treatment
Treatment for peripheral vascular disease has two major goals:
- Manage symptoms, such as leg pain, so that you can resume physical activities
- Stop the progression of atherosclerosis throughout your body to reduce your risk of heart attack and stroke
You may be able to accomplish these goals with lifestyle changes, especially early in the course of peripheral vascular disease. If you smoke, quitting is the single most important thing you can do to reduce your risk of complications.
If you have signs or symptoms of peripheral vascular disease, you likely will need additional medical treatment. Your doctor may prescribe medicine to prevent blood clots, lower blood pressure and cholesterol, and control pain and other symptoms.
Peripheral vascular disease medication
- Cholesterol-lowering medications. You may take a cholesterol-lowering drug called a statin to reduce your risk of heart attack and stroke. The goal for people who have peripheral artery disease is to reduce low-density lipoprotein (LDL) cholesterol, the “bad” cholesterol, to less than 100 milligrams per deciliter (mg/dL), or 2.6 millimoles per liter (mmol/L). The goal is even lower if you have additional major risk factors for heart attack and stroke, especially diabetes or continued smoking.
- High blood pressure medications. If you also have high blood pressure, your doctor may prescribe medications to lower it. A blood pressure reading, given in millimeters of mercury (mm Hg), has two numbers. The top number in the reading measures the pressure in your arteries when your heart beats (systolic pressure). The bottom number in the reading measures the pressure in your arteries between beats (diastolic pressure). Your blood pressure treatment goal should be less than 130/80 mm Hg. This is the guideline for anyone with coronary artery disease, diabetes or chronic kidney disease. Achieving 130/80 mm Hg is also the goal for healthy adults age 65 and older and healthy adults younger than age 65 with a 10 percent or higher risk of developing cardiovascular disease in the next 10 years. A widely used type of antihypertensive is an angiotensin-converting enzyme (ACE) inhibitor. ACE inhibitors block the actions of some of the hormones that help to regulate blood pressure. They help to reduce the amount of water in your blood and widen your arteries, which will both decrease your blood pressure. A medicine that works in a similar way to ACE inhibitors, known as an ‘angiotensin-2 receptor antagonist’, may also be recommended. ACE inhibitors and angiotensin-2 receptor antagonists can cause unpredictable effects if taken with other medicines, including some over-the-counter ones, so check with your doctor or pharmacist before taking anything in combination with this medicine.
- Medication to control blood sugar. If you also have diabetes, it becomes even more important to control your blood sugar (glucose) levels. Talk with your doctor about what your blood sugar goals are and what steps you need to take to achieve these goals.
- Medications to prevent blood clots. Because peripheral artery disease is related to reduced blood flow to your limbs, it’s important to improve that flow. Your doctor may prescribe daily aspirin therapy or another medication, such as clopidogrel (Plavix).
- Symptom-relief medications. The drug cilostazol increases blood flow to the limbs both by keeping the blood thin and by widening the blood vessels. It specifically helps treat symptoms of claudication, such as leg pain, for people who have peripheral artery disease. Common side effects of this medication include headache and diarrhea. Cilostazol is not recommended if you are pregnant or breastfeeding. An alternative to cilostazol is pentoxifylline. Side effects are rare with this medication, but it’s generally less effective than cilostazol.
Peripheral vascular disease surgery
In some cases, angioplasty or surgery may be necessary to treat peripheral vascular disease that’s causing claudication:
- Angioplasty. In this procedure, a small hollow tube (catheter) is threaded through a blood vessel to the affected artery. There, a small balloon on the tip of the catheter is inflated to reopen the artery and flatten the blockage into the artery wall, while at the same time stretching the artery open to increase blood flow. Your doctor may also insert a mesh framework called a stent in the artery to help keep it open. This is the same procedure doctors use to open heart arteries.
- Bypass surgery. Your doctor may create a graft bypass using a vessel from another part of your body or a blood vessel made of synthetic (man-made) fabric. This technique allows blood to flow around — or bypass — the blocked or narrowed artery.
- Thrombolytic therapy. If you have a blood clot blocking an artery, your doctor may inject a clot-dissolving drug into your artery at the point of the clot to break it up.
Supervised exercise program
In addition to medications or surgery, your doctor likely will prescribe a supervised exercise training program to increase the distance you can walk pain-free. Regular exercise improves symptoms of peripheral vascular disease in a number of ways, including helping your body use oxygen more efficiently.
Peripheral vascular disease can be frustrating, especially when the exercise that will help you get better causes you pain. Don’t get discouraged, however. As you continue exercising, you’ll increase the distance you can walk without pain.
There is a lot of high-quality evidence showing that taking part in regular exercise helps to reduce the severity and frequency of peripheral vascular disease symptoms, while at the same time reducing the risk of developing another cardiovascular disease.
Research has found that after six months of regular exercise, a person can:
- walk for longer and further before experiencing pain
- see an improvement in their ABI score (a test done to assess the circulation in your lower legs)
The preferred exercise is walking. It is normally recommended that you walk as far and as long as you can before the symptoms of pain become intolerable. Once this happens, rest until the pain goes and begin walking again until the pain returns. Keep using this ‘stop-start’ method until you have spent at least 30 minutes walking.
You will probably find the exercise course challenging, as the frequent episodes of pain can be upsetting and off-putting. But if you persevere, you should gradually notice a marked improvement in your symptoms and you will begin to go longer and longer without experiencing any pain.
Lifestyle and home remedies
Many people can manage the symptoms of peripheral vascular disease and stop the progression of the disease through lifestyle changes, especially quitting smoking. To stabilize or improve peripheral vascular disease:
- Stop smoking. Smoking contributes to constriction and damage of your arteries and is a significant risk factor for the development and worsening of peripheral vascular disease. If you smoke, quitting is the most important thing you can do to reduce your risk of complications. If you’re having trouble quitting on your own, ask your doctor about smoking cessation options, including medications to help you quit. You use an anti-smoking treatment such as nicotine replacement therapy or bupropion (a medicine used to reduce cravings for cigarettes). People who use these treatments have a much greater success rate in permanently quitting than people who try to quit using willpower alone.
- Exercise. This is a key component. Success in the treatment of peripheral vascular disease is often measured by how far you can walk without pain. Proper exercise helps condition your muscles to use oxygen more efficiently. Your doctor can help you develop an appropriate exercise plan. He or she may refer you to a claudication exercise rehabilitation program.
- Eat a healthy diet. A heart-healthy diet low in saturated fat can help control your blood pressure and cholesterol levels, which contribute to atherosclerosis.
- Avoid certain cold medications. Over-the-counter cold remedies that contain pseudoephedrine (Advil Cold & Sinus, Aleve-D Sinus & Cold, others) constrict your blood vessels and may increase your peripheral vascular disease symptoms.
- You may find it helpful to raise the head of your bed by 4 to 6 inches (10 to 15 centimeters), because keeping your legs below the level of your heart usually lessens pain.
- Another tip for reducing your symptoms is to avoid cold temperatures as much as possible. If you can’t avoid the cold, be sure to dress in warm layers.
Careful foot care
In addition to the above suggestions, take good care of your feet. People with peripheral vascular disease, especially those who also have diabetes, are at risk of poor healing of sores and injuries on the lower legs and feet.
Poor blood circulation can postpone or prevent proper healing and increases the risk of infection. Follow this advice to care for your feet:
- Wash your feet daily, dry them thoroughly and moisturize often to prevent cracks that can lead to infection. Don’t moisturize between the toes, however, as this can encourage fungal growth.
- Wear well-fitting shoes and thick, dry socks.
- Promptly treat any fungal infections of the feet, such as athlete’s foot.
- Take care when trimming your nails.
- Inspect your feet daily for injuries.
- Have a foot doctor (podiatrist) treat bunions, corns or calluses.
- See your doctor at the first sign of a sore or injury to your skin.
Alternative medicine
The blood-thinning effects of ginkgo may allow people with intermittent claudication to walk longer distances with less pain. However, this herbal remedy can cause bleeding when taken in high doses, and it could be dangerous if paired with anti-platelet medications, including aspirin, that are commonly prescribed to people with peripheral vascular disease.
Don’t take ginkgo before talking with your doctor.
- National Clinical Guideline Centre (UK). Lower Limb Peripheral Arterial Disease: Diagnosis and Management [Internet]. London: Royal College of Physicians (UK); 2012 Aug. (NICE Clinical Guidelines, No. 147.) 9, Management of intermittent claudication. Available from: https://www.ncbi.nlm.nih.gov/books/NBK327437[↩]
- Bhimji SS, Bah F, Dreyer MA. Peripheral Arterial Disease. [Updated 2019 Apr 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430745[↩][↩][↩][↩]
- Aysert Yıldız P, Özdil T, Dizbay M, Güzel Tunçcan Ö, Hızel K. Peripheral arterial disease increases the risk of multidrug-resistant bacteria and amputation in diabetic foot infections. Turk J Med Sci. 2018 Aug 16;48(4):845-850[↩]
- Jelani QU, Petrov M, Martinez SC, Holmvang L, Al-Shaibi K, Alasnag M. Peripheral Arterial Disease in Women: an Overview of Risk Factor Profile, Clinical Features, and Outcomes. Curr Atheroscler Rep. 2018 Jun 02;20(8):40[↩]
- Simon F, Oberhuber A, Floros N, Düppers P, Schelzig H, Duran M. Pathophysiology of chronic limb ischemia. Gefasschirurgie. 2018;23(Suppl 1):13-18.[↩]
- Kim HO, Kim W. Elucidation of the Diagnosis and Treatment of Peripheral Arterial Disease. Korean Circ J. 2018 Sep;48(9):826-827[↩]
- Santoro L, Flex A, Nesci A, Ferraro PM, De Matteis G, Di Giorgio A, Giupponi B, Saviano L, Gambaro G, Franceschi F, Gasbarrini A, Landolfi R, Santoliquido A. Association between peripheral arterial disease and cardiovascular risk factors: role of ultrasonography versus ankle-brachial index. Eur Rev Med Pharmacol Sci. 2018 May;22(10):3160-3165[↩]





{kind=link}