Contents
Pigmentary glaucoma
Pigmentary glaucoma is a type of secondary open-angle glaucoma where small pigment granules from the back of the iris breaks off and clogs the eye’s drainage system at the angle where the iris and cornea meet, leading to increased intraocular pressure (IOP) and potential optic nerve damage 1, 2, 3, 4, 5, 6. Pigment gives your iris its color. Pigment dispersion syndrome (PDS) is characterized by the presence of melanin pigment granules that circulate within the aqueous humor and accumulate on different structures found in the anterior chamber of the eye, including corneal endothelium deposits also known as the Krukenberg spindle, lens surface, zonules, iris, iridocorneal angle, and trabecular meshwork 7. The pigment granules that accumulate in the angular structures and trabecular meshwork can give rise to reduced aqueous outflow, leading to elevated intraocular pressure (IOP). Pigment dispersion syndrome (PDS) can cause ocular hypertension and can lead to secondary rise in intraocular pressure (IOP) that can damage the optic nerve resulting in pigmentary glaucoma development, which is a secondary type of glaucoma. Pigment dispersion syndrome (PDS) and pigmentary glaucoma in reality reflect different levels of severity on a continuum disease spectrum 5. Pigment dispersion syndrome (PDS) is used to classify individuals who exhibit these features but who have not progressed to optic nerve damage and/or visual field loss (signifiers of pigmentary glaucoma), even if the intraocular pressure (IOP) is elevated. Pigment dispersion syndrome (PDS) is an important risk factor in the development of ocular hypertension and pigmentary glaucoma 6.
Pigmentary glaucoma is a result of pigment dispersion syndrome (PDS), where pigment granules detach from the iris and accumulate in the trabecular meshwork, which is the main drainage channel of the eye. Pigment dispersion syndrome (PDS) happens when the pigment rubs off the back of your iris. The pigment then floats around to other parts of your eye. The tiny bits of pigment can clog your eye’s drainage angle. This pigment can raise eye pressure and lead to pigmentary glaucoma. Features of pigment dispersion syndrome (PDS) include anterior chamber pigment dispersion, spoke-like iris defects on trans-illumination, central corneal endothelial deposits also known as the Krukenberg spindle, and increased pigmentation in the iridocorneal angle 5. However, not everyone who has pigment dispersion syndrome (PDS) will develop pigmentary glaucoma. Approximately 15% of patients with pigment dispersion syndrome (PDS) will convert to pigmentary glaucoma after 15 years 1. Some people with pigment dispersion syndrome (PDS) or pigmentary glaucoma may see halos or have blurry vision after activities like jogging or playing basketball that stir up the pigment granules. See your ophthalmologist if you have these or other symptoms.
The iris of your eye is a flat ring of muscle that contains melanin, the pigment that gives your eyes their color. In front of and behind your iris are spaces filled with a fluid called aqueous humor. Pressure from the aqueous humor helps your eye hold its globe-like shape. When you have pigment dispersion syndrome (PDS), your iris can’t hold its shape and dips back too far 8, 9. That makes the back of your iris press against the muscle fibers that control your lens shape. As your iris widens or narrows, the iris rubs against those fibers and pigment granules in the iris wear away, like flakes of paint chipping away from a piece of wood 8, 9. Patients with pigment dispersion syndrome or pigmentary glaucoma have a 15-fold higher concentration of aqueous pigment granules in their anterior chamber compared to normal controls 10.
The release of pigment showers in the anterior chamber is mainly due to the friction and rubbing between the iris pigment epithelium and posterior surface and zonules of the lens, which is favored by the backward posterior bowing of the iris that can be found in moderate myopic eyes that have more space 11 and by reverse pupillary block mechanisms due to increased iridolenticular touch 12. Ultrasonographical studies have shown that events leading to increased friction and contact between anterior chamber structures that favor reverse pupillary block include physiological events such as accommodation, blinking, eye movements, head positions, and exercise 13. The increased contact between the iris and lens structures in eyes at risk of having a deep anterior chamber and/or a large iris can create a ball-valve mechanism in certain conditions in which the aqueous humor moves from the posterior chamber to the anterior chamber in a unidirectional mode, thus creating a high pressure in the anterior chamber that favors further apposition between the iris and lens surface 14. The aqueous humor trapped in the anterior chamber can cause posterior bowing and further friction between the peripheral posterior iris and zonules and lens structures leading to pigment dispersion showers.
Once those pigment granules are loose and floating in the aqueous humor, the flow of fluid carries them to other places inside your eye. The aqueous humor has a drainage system, the trabecular meshwork, and granules can accumulate in that meshwork and damage it 15, 10, 16. When that happens, aqueous humor fluid can’t drain out of your eye properly, causing high pressure inside your eye (ocular hypertension) and eventually causing glaucoma 9, 17. Without treatment, glaucoma causes irreversible, severe vision loss and blindness.
It was originally thought that pigment dispersion syndrome (PDS) and pigmentary glaucoma had a congenital cause or may be inherited (passed from parent to child), due to pigment loss from the iris from congenital mesodermal dysgenesis 18 or atrophy or degeneration of the iris pigment epithelium (IPE) 19, 20. Possible genetic factors have been hypothesized to explain the familial presence of Krukenberg spindle 21. Although the low incidence of familial pigment dispersion syndrome and pigmentary glaucoma, studies have reported a possible autosomal dominant inheritance for pigment dispersion syndrome 22 and multifactorial pattern of inheritance 23, which may play a role in the clinical expression of factors related to iris color, gender, and refractive error. Anderson et al. 24 reported a possible gene responsible for pigment dispersion syndrome located on chromosome 7Q35-q36 based on an autosomal dominant pattern observed in patients from 4 Irish families with pigment dispersion syndrome. Studies have reported several genetic locus associated with pigment dispersion syndrome, which include Glycoprotein nmb (GpnmbR150x), Gene Gpigment dispersion syndrome1 (glaucoma-related pigment dispersion syndrome 1), and (OMIM ID 600510) 25.
There are other reasons why pigment granules might break free from your iris. When there’s another cause for pigment displacement, that’s called “secondary pigment dispersion syndrome”.
Some causes of secondary pigment dispersion syndrome include:
- Eye injuries
- Tumors or growths inside your eye
- An artificial intraocular lens (IOL) that moves out of position
There are are several possible contributing factors for developing pigmentary glaucoma:
- Genetics. Research connects several DNA mutations with pigment dispersion syndrome and pigmentary glaucoma. That’s why pigment dispersion syndrome and pigmentary glaucoma can run in families but it’s usually in an unpredictable way. Direct examination of a small set of family members of patients with pigment dispersion syndrome showed that the disease was present in 2 out of 19 related individuals (12%) 26. In another family, signs of pigment dispersion syndrome were present in 36% of subjects’ parents and 50% of their siblings (but in no children), suggesting a possible autosomal dominant inheritance pattern with incomplete penetrance 27, 28, 29. Pigmentary glaucoma or pigment dispersion syndrome has also been described in families across multiple generations, with roughly 50% of family members described as having either condition, reinforcing the idea of an autosomal dominant inheritance pattern 30, 31.
- Male sex. Pigment dispersion syndrome and pigmentary glaucoma disproportionately affects males with case series showing a male to female ratio of between 2:1 and 5:1. Much less of a male predominance is noted for pigment dispersion syndrome, with case series describing male to female ratios between 1:1 and 2:1 32, 28, 33, 34, 35.
- Age. Diagnosis of pigment dispersion syndrome generally happens sometime between ages 20 and 50. Male patients with pigmentary glaucoma or pigment dispersion syndrome most often present in their 30s, whereas female patients typically present roughly a decade later in life 28, 33, 34, 36, 37. However, cases of pigment dispersion syndrome have been identified in patients as young as 12–15 years of age 38, 39, 40. Pigment dispersion syndrome and pigmentary glaucoma may be most common in middle age once the lens has enlarged and the iris is flexible enough to form a concave position 8.
- Race. People who are of Black or Asian descent have a lower risk for pigment dispersion syndrome and pigmentary glaucoma, while the risk for white people is higher 32, 33.
- Being nearsighted. People with myopia (nearsightedness) have a higher risk of pigment dispersion syndrome and pigmentary glaucoma. The more nearsighted you are (typically in the range of -3 to -4 D), the higher the risk of having pigment dispersion syndrome or having it turn into pigmentary glaucoma.
- Eye structure. Pigment dispersion syndrome and pigmentary glaucoma are more likely to happen when you have a deep anterior chamber. A deeper chamber means it can hold more fluid, which can make the iris “bow” backward toward the lens. Having flatter corneas can also be a contributing factor.
- Concave iris and posterior iris insertion. Concave iris and more posterior iris insertion are more common in patients with pigment dispersion syndrome or pigmentary glaucoma than in the normal population and result in greater iridolenticular contact in these individuals 41, 42, 43.
- Flat corneas. Patients with pigment dispersion syndrome and pigmentary glaucoma have significantly flatter corneas than control subjects of similar age and refractive error 44, 45. A flat cornea might be more likely to result in burping of aqueous humor from the posterior chamber to the anterior chamber with blinking, resulting in increased irido-zonular contact 45.
- Excessive activity level. Research links pigment dispersion syndrome and pigmentary glaucoma to excessive exercise or physical activity. If you have pigment dispersion syndrome or pigmentary glaucoma, your eye specialist will likely ask about how physically active you are. If your activity level could contribute to your pigment dispersion syndrome or pigmentary glaucoma — either now or in the future — your eye specialist will likely recommend reducing your activity level.
The treatments for pigment dispersion syndrome and pigmentary glaucoma are very similar to treatments for other forms of glaucoma. The treatments can involve one or more of the following:
- Medications. Glaucoma medications lower pressure inside your eye in different ways. Some of them cause your pupil to relax more, improving aqueous humor drainage. Others slow the production of aqueous humor.
- Glaucoma surgery. This approach usually aims to improve fluid flow and drainage. Examples of glaucoma surgeries that do this include laser trabeculoplasty, and incisional surgery with either trabeculectomy or glaucoma drainage implant.
In many cases, a combination approach may offer the best results for people with pigment dispersion syndrome and pigmentary glaucoma. An example would be combining medications with laser surgery. This works well when medication alone doesn’t lower pressure inside your eye as much as you need.
Your eye specialist is your best source of information about treatment approaches. Your eye specialist can advise you on how treatments are likely to affect you, what your alternatives are and what kinds of side effects you can expect.
Figure 1. Krukenberg spindle
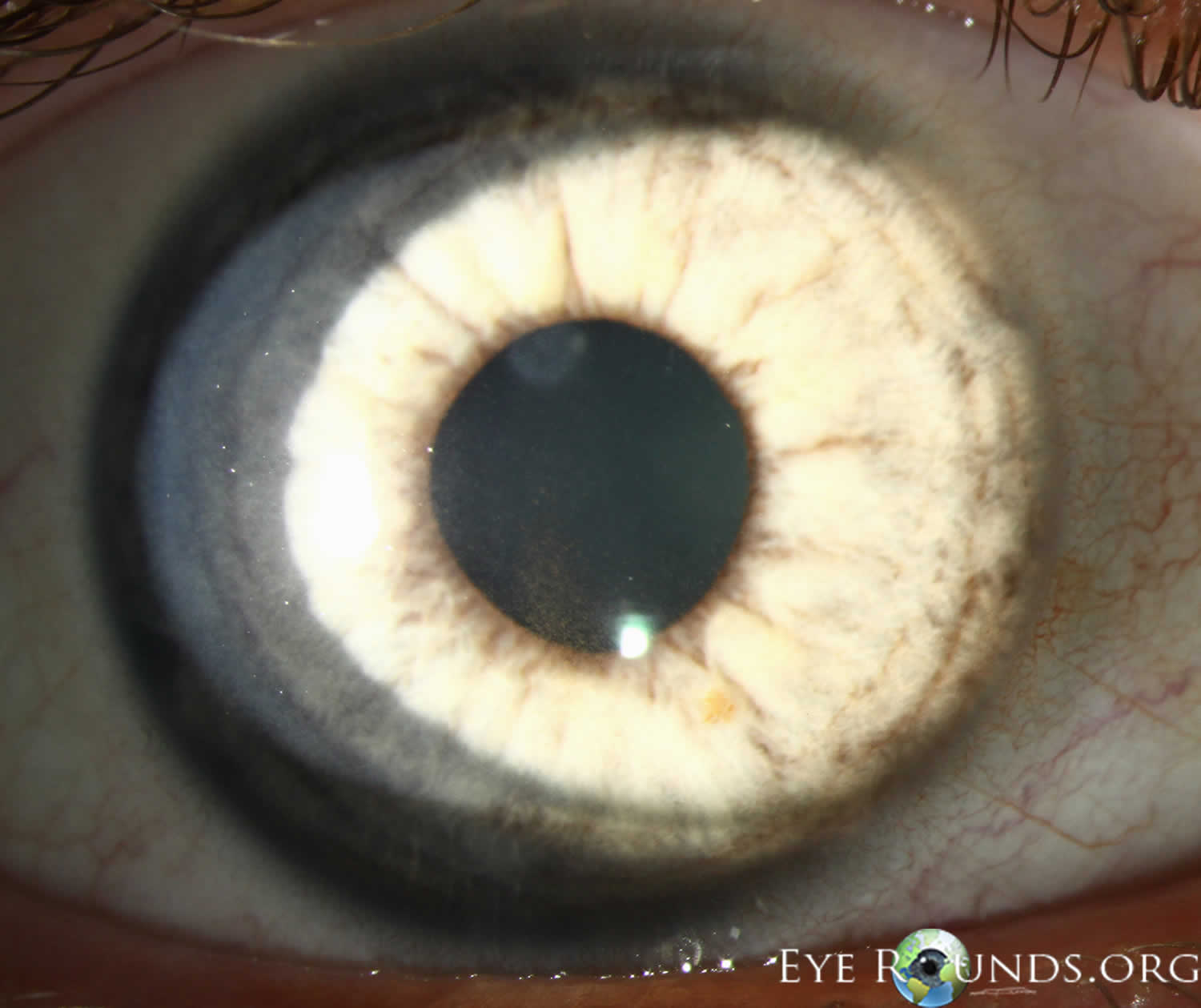
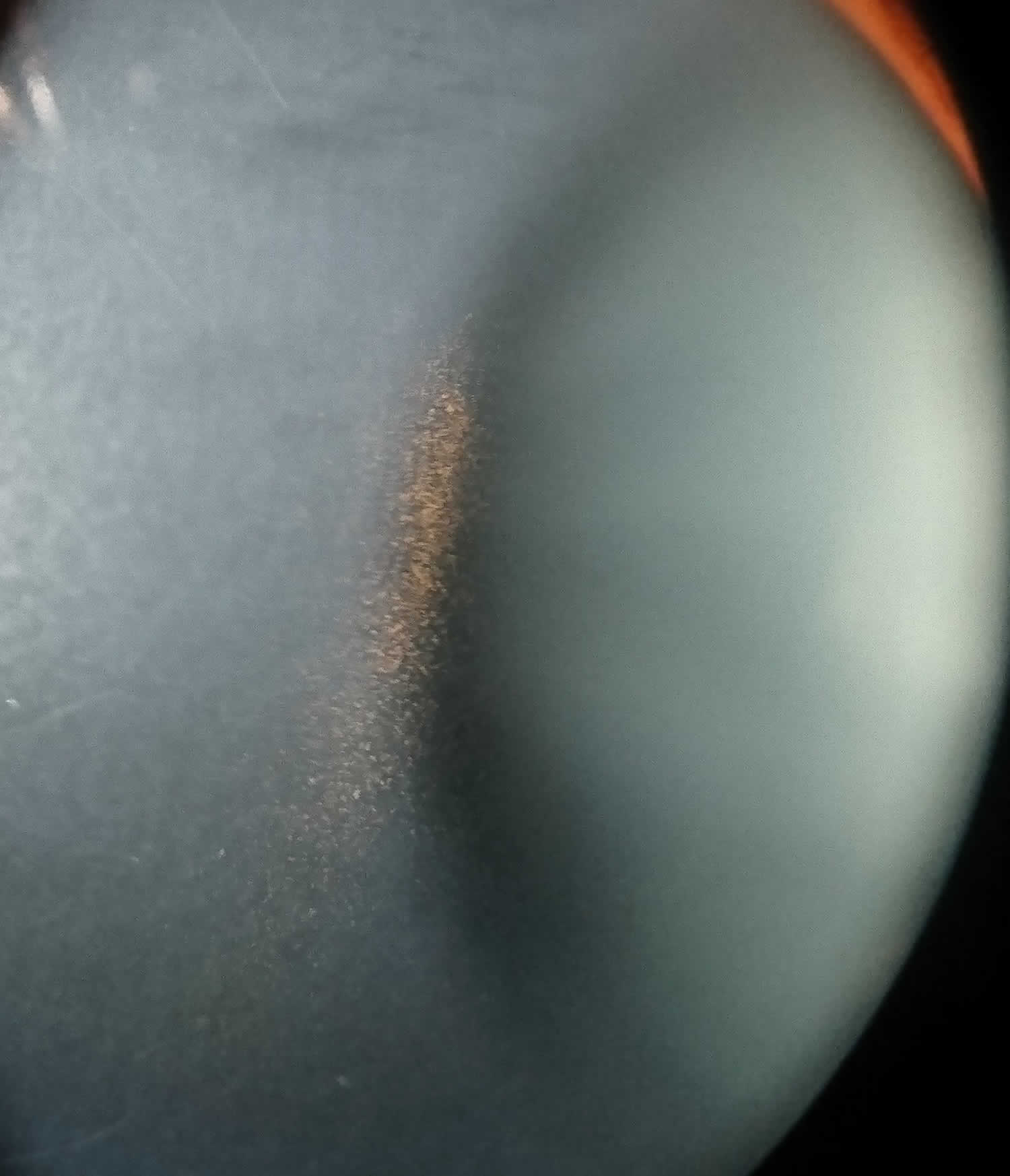
Footnote: Slit lamp photograph showing a Krukenberg spindle visible on the corneal endothelium.
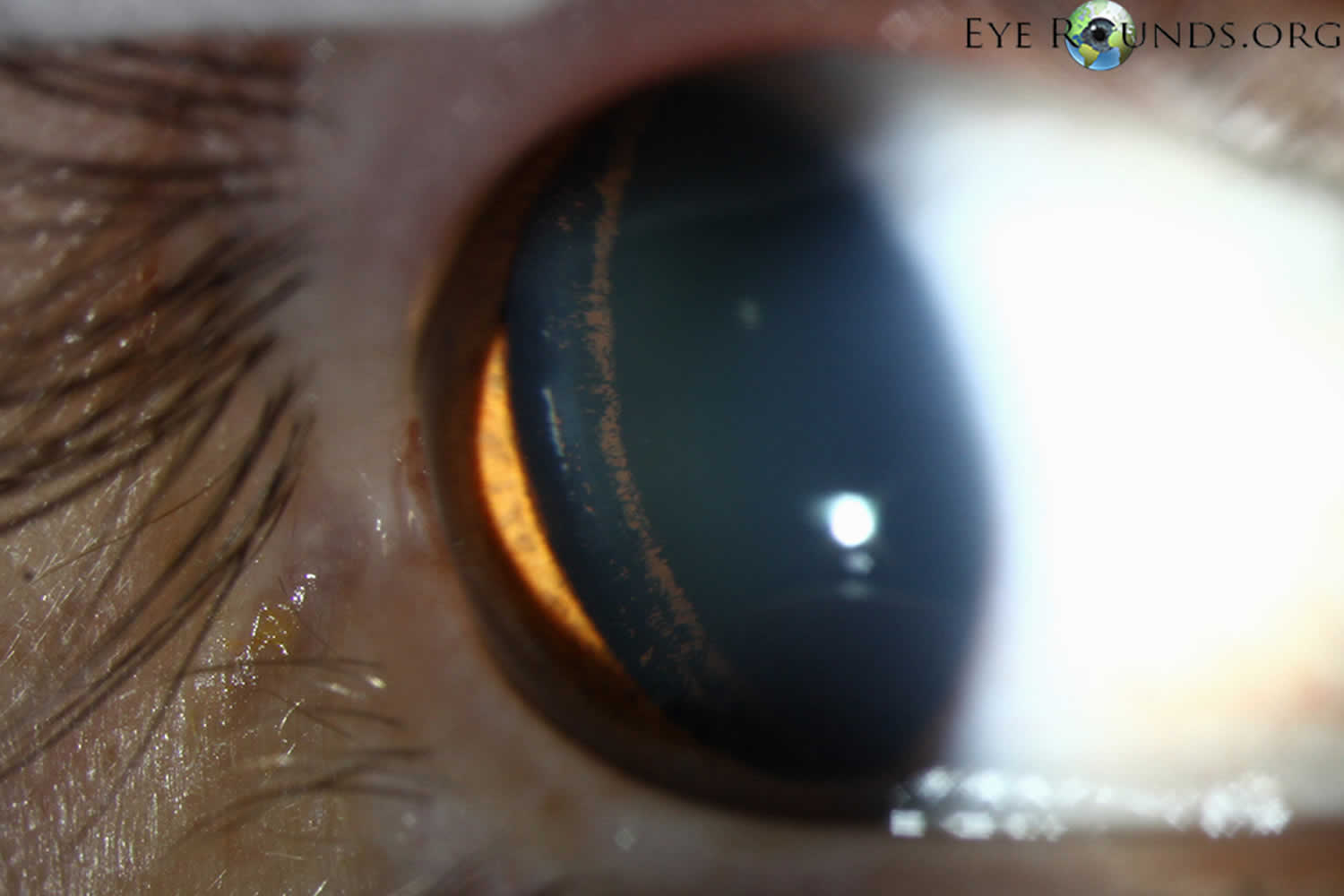
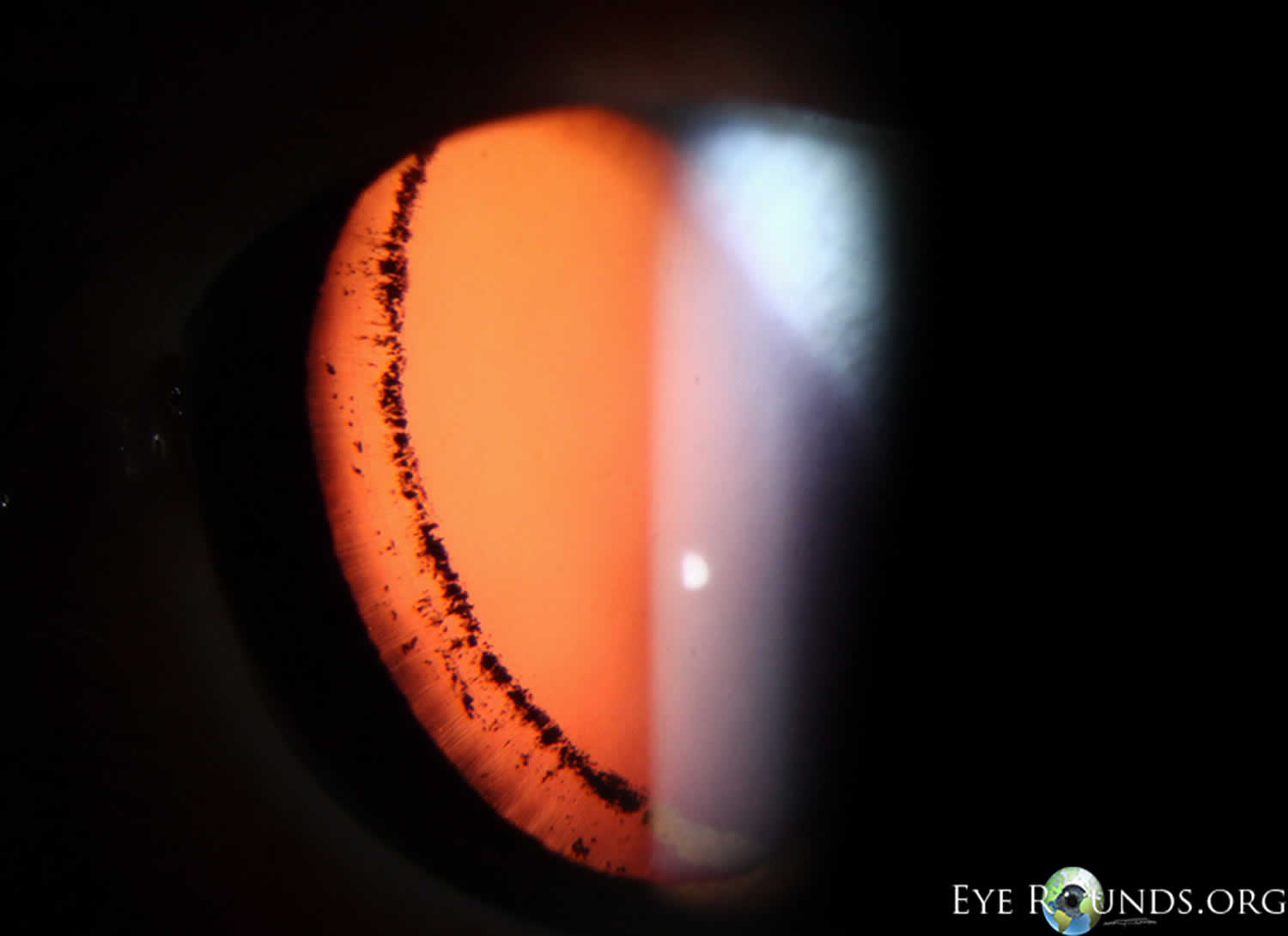
[Source 2 ]Figure 2. Scheie stripe (pigment deposition along the insertion of the zonular fibers to the lens)
Some eye symptoms mean you need medical attention quickly. Not getting treatment can lead to irreversible eye damage. You should talk to your eye specialist after your diagnosis to learn about the symptoms that are most relevant to your specific case and what you should do if you have any of these symptoms.
Symptoms that mean you need emergency medical attention include:
- Sudden vision changes like blurring or low vision
- Noticeable new or worsening halos or glare around lights
- Sudden, severe eye pain and/or headaches
- Sudden vision loss (either partial or total)
Aqueous Humor Production and Physiology
The aqueous humor is a water-like fluid that is produced by the ciliary body epithelium that sits directly behind the iris (the colored part of your eye). Aqueous humor is produced at a rate of 2-3 microliters per minute (2-3 μL/minute) 47, 48. The aqueous humor is composed of organic and inorganic ions, carbon dioxide, amino acids, carbohydrates, glutathione, and water 47, 49. The aqueous humor fills the anterior chamber of your eye with continual production, secretion, and reabsorption 47. The production, circulation and reabsorption of aqueous humor are vital processes maintaining homeostasis of the eye. Imbalances between the production and secretion of aqueous humor may lead to increased intraocular pressure (IOP) and optic nerve damage such as in the setting of ocular hypertension or glaucoma.
Aqueous humor functions as a physical component allowing clear optics and filling the anterior chamber of the eye 47, 48. The aqueous humor is responsible for providing nourishment to the avascular components of the anterior chamber including the cornea and lens 47, 48. In addition, aqueous humor is responsible for removing waste products, blood, macrophages and other debris from the anterior chamber, including the trabecular meshwork 47, 48. The structure and function of the trabecular meshwork may become compromised by chronic oxidative stress from reactive oxygen species and insufficient antioxidant defense in the aqueous humor 47, 48, 50, 51. Decreased levels of antioxidants in aqueous humor are present in glaucomatous eyes versus normal eyes, consistent with the presence of increased oxidative stress and low-grade inflammation 50, 51.
The primary anatomic structures vital to the homeostasis of aqueous humor include the ciliary body as the site of principle production, and the trabecular meshwork and uveoscleral pathway as the sites of primary outflow 47, 52. Aqueous humor is produced by the ciliary body via a multistep process closely correlating with systemic vascular blood flow 47, 53, 54. Initially, blood enters the ciliary processes, which propels ultrafiltrate from the blood into the ciliary interstitial space via a pressure gradient 47, 53, 54. Next, the ciliary epithelium transports plasma components from the basal to the apical surface in order to synthesize aqueous humor and transport it into the posterior chamber 47, 53, 54. Passive diffusion and ultrafiltration are key in initial synthesis, and active secretion across a blood-aqueous barrier via aquaporins, Na-K-ATPase and carbonic anhydrase enzymes are necessary for final synthesis 47, 53, 54, 55. These active transport enzymes necessary for final synthesis are common pharmacologic targets in decreasing aqueous humor production. Although systemic blood flow via the ciliary artery is required for the initial production of ultrafiltrate, the production of aqueous humor is independent from systemic blood pressure due to a fixed rate of 4% filtration of plasma 54. Therefore, there is minimal association between systemic high blood pressure (hypertension) and elevated intraocular pressure (IOP). The estimated rate of aqueous humor production is approximately 2.4 microliters per minute (2.4 μL/minute), with diurnal variations leading to higher aqueous humor flow in the morning and lower flow in the evening 47, 53.
While aqueous humor production is well documented, the mechanism of drainage is still poorly understood.
There are 2 main drainage pathways for aqueous humor 47, 56, 53:
- The conventional pathway via trabecular meshwork, Schlemm’s canal, collector channels, and the episcleral venous system), and
- The unconventional pathway via uveoscleral, uveovortex, uveolymphatic.
The conventional pathway drainage pathways for aqueous humor involves passive drainage throughout the trabecular meshwork although the Schlemm’s canal has been documented with paracellular and intracellular pores 47, 56, 53. The trabecular meshwork is a triangular porous structure composed of a layer of connective tissue and endothelium with sympathetic innervation from superior sympathetic ganglion, and parasympathetic innervation from the ciliary ganglion 47, 56, 53. The trabecular meshwork may be divided into the uveal meshwork (iris root, ciliary body, peripheral cornea), corneoscleral meshwork (scleral spur), and juxtacanalicular meshwork (transition into Schlemm’s canal) 47, 56, 53. Schlemm’s canal is a structure with composition similar to venous vasculature, with fenestrated thin endothelium surrounded by connective tissue 47, 56, 53. After drainage through the trabecular meshwork and the Schlemm’s canal, aqueous humor continues through collector channels into the episcleral venous system which deposits into the main venous system 47, 56, 53.
Resistance to outflow through the trabecular meshwork and Schlemm’s canal has been documented although it is poorly understood, yet resistance remains an important factor in regulating intraocular pressure and the pathogenesis of glaucomatous processes. In humans, up to 75% of aqueous outflow resistance is contributed by the trabecular meshwork while the remaining 25% is due to resistance beyond Schlemm’s canal 47. The rate of outflow is directly influenced by iris and ciliary muscles which contract and relax based on cholinergic innervation and pharmacodynamics 47, 56, 53, 52, 57. In ciliary contraction, the trabecular meshwork and Schlemm’s canal dilate, decreasing resistance and increasing outflow 47, 56, 53, 52, 57. The rate of outflow is also influenced by intraocular pressure, with higher intraocular pressure altering the structure of endothelial lining in Schlemm’s canal to increase the number of porous vacuoles allowing increased outflow 47, 56, 53, 52, 57. However, it is still debated if this finding substantially contributes to increasing outflow in glaucomatous eyes 47, 56, 53, 52, 57.
The unconventional pathway involves drainage into the orbital vasculature, vortex veins and ciliary lymphatics, contributing up to 25-40% of total aqueous outflow in cynomolgus and vervet monkey models.2,5 The uveoscleral pathway involves diffusion into the sclera and episcleral through the orbital vasculature.2,5 The uveovortex pathway involves osmotic absorption of fluid through the choroid, passing into the vortex veins 56. Lastly, the uveolymphatic pathway involves drainage into lymphatic vessels within the ciliary body, although the extent of drainage under normal physiological conditions remains controversial 56. In addition, the unconventional pathway also includes corneal, iridial and retinal routes, albeit less clinically significant 58. Regardless of downflow pathway, all unconventional paths require drainage through the interstitial spaces of the ciliary muscle 56, 58. Resistance also exists within the unconventional pathway likely due to ciliary muscle tone, as seen with changes in outflow in the setting of pilocarpine, increasing ciliary tone and decreasing flow, and atropine, decreasing ciliary tone and increasing flow 56, 58. Therefore, the unconventional pathways are also clinically important in moderating intraocular pressure, and serve as a potential target in glaucoma therapy.
Figure 3. Eye anatomy

Figure 4. Normal aqueous outflow
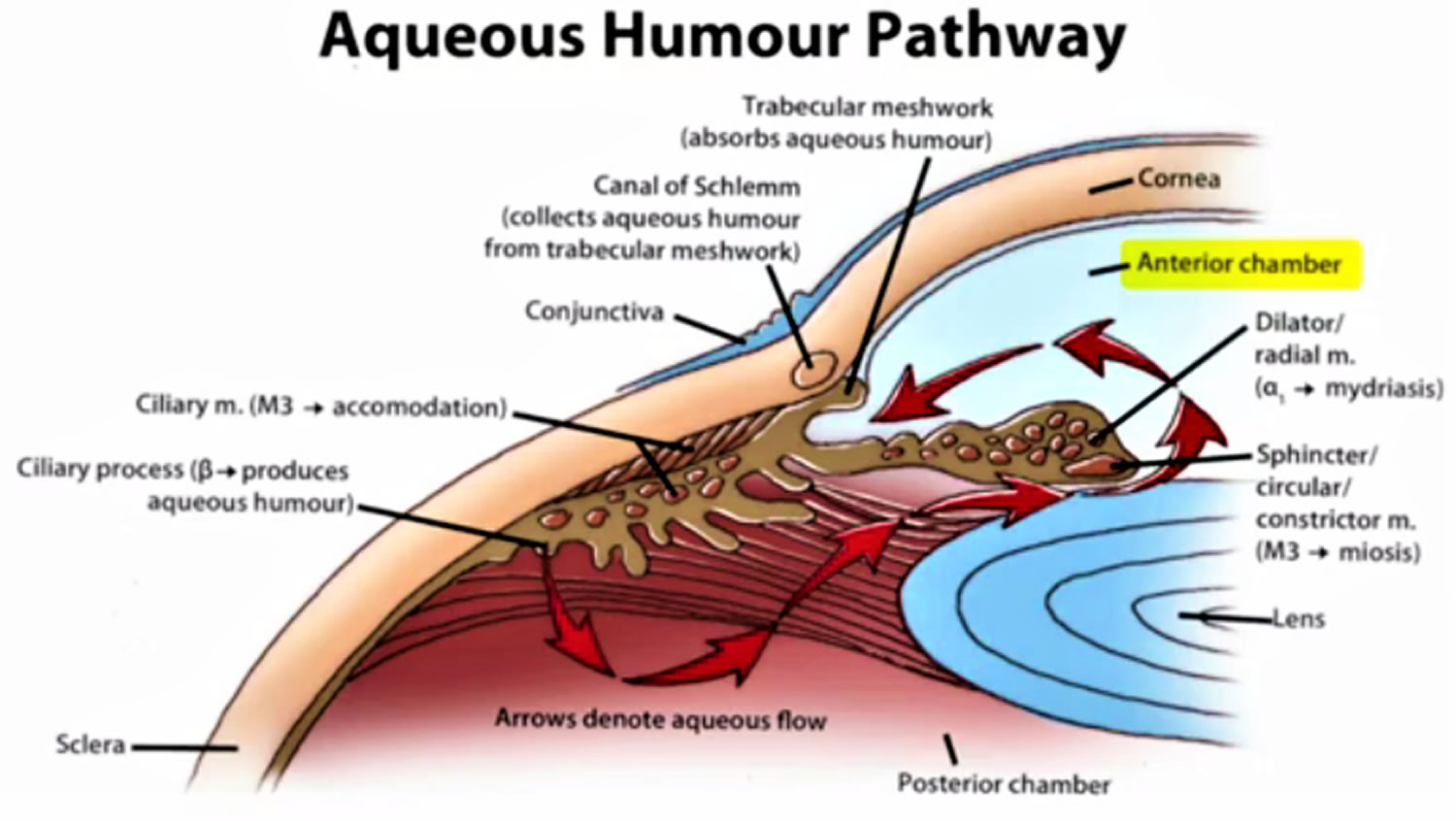
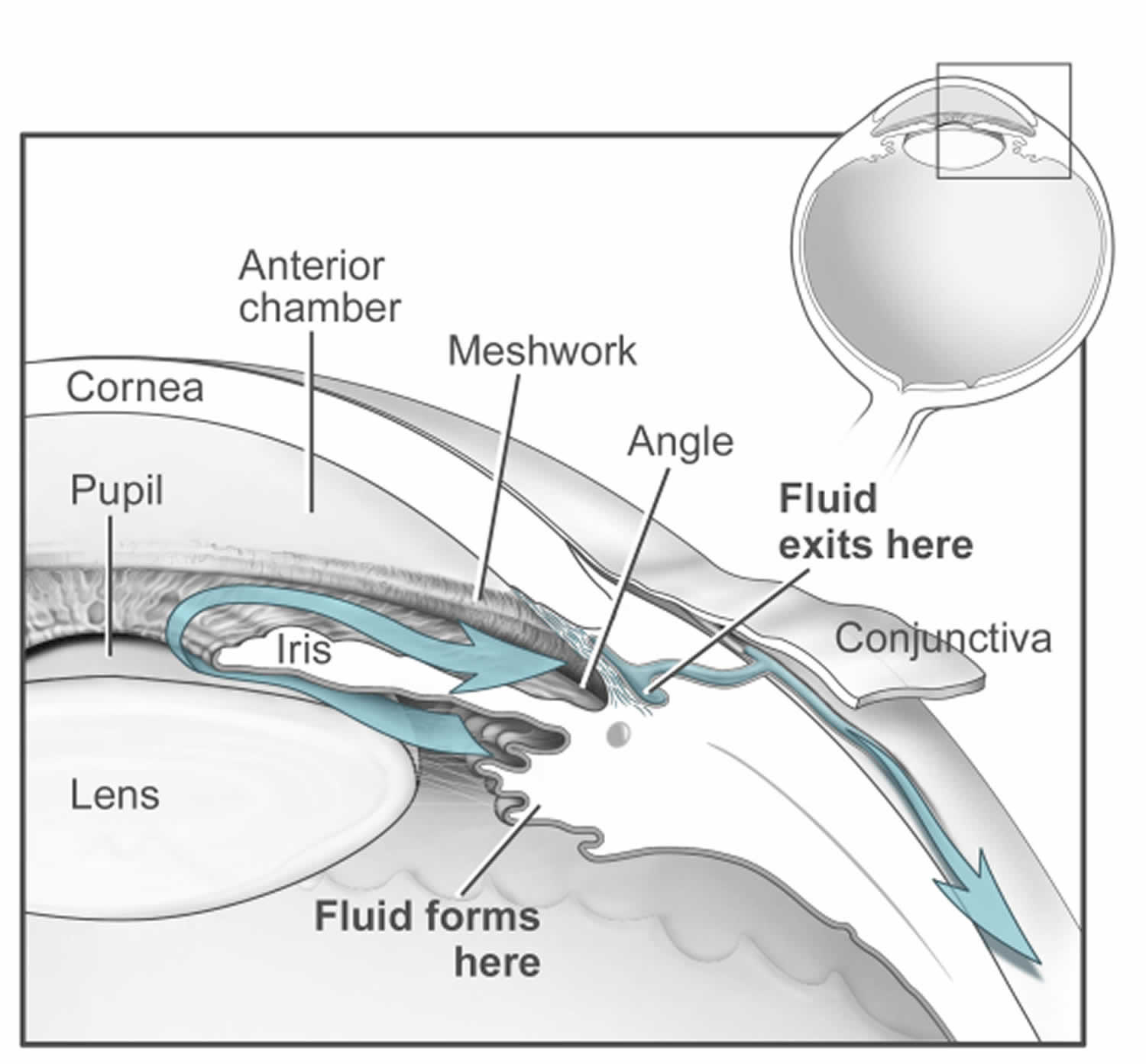
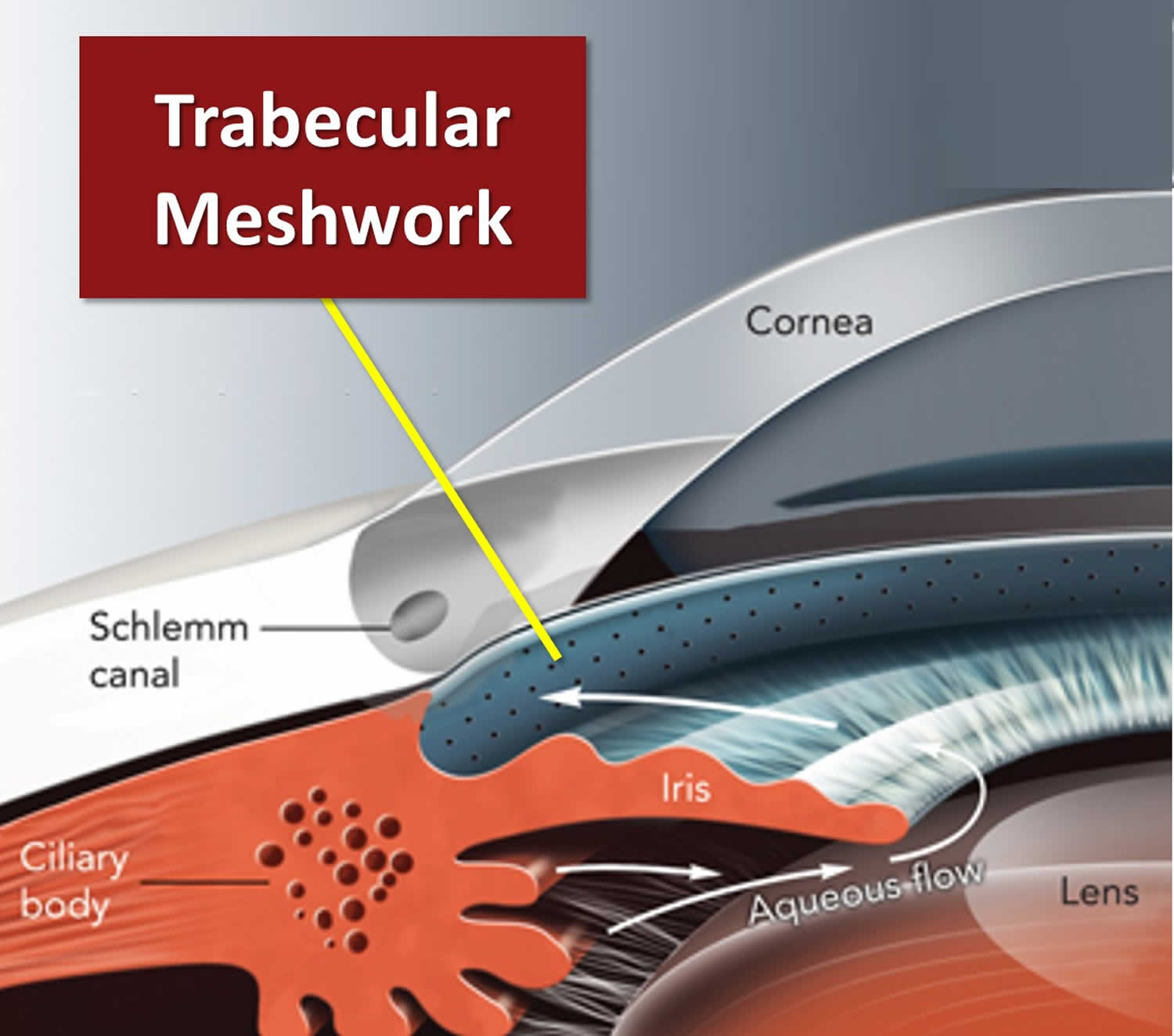
Footnotes: The ciliary body is a structure that sits directly behind the iris (the colored part of your eye). One of ciliary body’s jobs is to create an important fluid called aqueous humor, a fluid that nourishes the cornea and lens. Aqueous humor flows through a specific route into the front of the eye (the anterior chamber). This route allows aqueous humor to send important nutrients and oxygen to other parts of the eye, such as the lens and cornea. The aqueous humor is produced behind the iris, flows into the anterior chamber through the pupil, and exits the eye between the iris and cornea via the trabecular meshwork, a specialized eye tissue located at the chamber angle of the eye next to the cornea 59. In a healthy eye, this is a constant process. The ciliary body is always producing aqueous humor, and 80%-90% aqueous humor is always draining through the trabecular meshwork. The trabecular meshwork is a specialized spongy tissue in the anterior chamber of the eye that regulates the outflow of aqueous humor 59. The trabecular meshwork acts as a filter, controlling how quickly aqueous humor drains out of the eye through a structure called Schlemm’s canal, ultimately maintaining intraocular pressure (IOP). The canal of Schlemm, also known as Schlemm’s canal or the scleral venous sinus, is a circular, lymphatic-like vessel in the eye that drains aqueous humor from the anterior chamber into the episcleral blood vessels. The canal of Schlemm and the trabecular meshwork (TM) play a crucial role in maintaining intraocular pressure (IOP) by facilitating the outflow of aqueous humor. Too much aqueous humor production or obstruction of its outflow causes a rise in intraocular pressure (IOP) that can lead to glaucoma.
[Source 60 ]Pigmentary glaucoma causes
The iris of your eye is a flat ring of muscle that contains melanin, the pigment that gives your eyes their color. In front of and behind your iris are spaces filled with a fluid called aqueous humor. Pressure from the aqueous humor helps your eye hold its globe-like shape. When you have pigment dispersion syndrome (PDS), your iris can’t hold its shape and dips back too far 8, 9. That makes the back of your iris press against the muscle fibers that control your lens shape. As your iris widens or narrows, the iris rubs against those fibers and pigment granules in the iris wear away, like flakes of paint chipping away from a piece of wood 8, 9. Patients with pigment dispersion syndrome or pigmentary glaucoma have a 15-fold higher concentration of aqueous pigment granules in their anterior chamber compared to normal controls 10.
The release of pigment showers in the anterior chamber is mainly due to the friction and rubbing between the iris pigment epithelium and posterior surface and zonules of the lens, which is favored by the backward posterior bowing of the iris that can be found in moderate myopic eyes that have more space 11 and by reverse pupillary block mechanisms due to increased iridolenticular touch 12. Ultrasonographical studies have shown that events leading to increased friction and contact between anterior chamber structures that favor reverse pupillary block include physiological events such as accommodation, blinking, eye movements, head positions, and exercise 13. The increased contact between the iris and lens structures in eyes at risk of having a deep anterior chamber and/or a large iris can create a ball-valve mechanism in certain conditions in which the aqueous humor moves from the posterior chamber to the anterior chamber in a unidirectional mode, thus creating a high pressure in the anterior chamber that favors further apposition between the iris and lens surface 14. The aqueous humor trapped in the anterior chamber can cause posterior bowing and further friction between the peripheral posterior iris and zonules and lens structures leading to pigment dispersion showers.
Once those pigment granules are loose and floating in the aqueous humor, the flow of fluid carries them to other places inside your eye. The aqueous humor has a drainage system, the trabecular meshwork, and granules can accumulate in that meshwork and damage it 15, 10, 16. When that happens, aqueous humor fluid can’t drain out of your eye properly, causing high pressure inside your eye (ocular hypertension) and eventually causing glaucoma 9, 17. Without treatment, glaucoma causes irreversible, severe vision loss and blindness.
It was originally thought that pigment dispersion syndrome (PDS) and pigmentary glaucoma had a congenital cause or may be inherited (passed from parent to child), due to pigment loss from the iris from congenital mesodermal dysgenesis 18 or atrophy or degeneration of the iris pigment epithelium (IPE) 19, 20. Possible genetic factors have been hypothesized to explain the familial presence of Krukenberg spindle 21. Although the low incidence of familial pigment dispersion syndrome and pigmentary glaucoma, studies have reported a possible autosomal dominant inheritance for pigment dispersion syndrome 22 and multifactorial pattern of inheritance 23, which may play a role in the clinical expression of factors related to iris color, gender, and refractive error. Anderson et al. 24 reported a possible gene responsible for pigment dispersion syndrome located on chromosome 7Q35-q36 based on an autosomal dominant pattern observed in patients from 4 Irish families with pigment dispersion syndrome. Studies have reported several genetic locus associated with pigment dispersion syndrome, which include Glycoprotein nmb (GpnmbR150x), Gene Gpigment dispersion syndrome1 (glaucoma-related pigment dispersion syndrome 1), and (OMIM ID 600510) 25.
There are other reasons why pigment granules might break free from your iris. When there’s another cause for pigment displacement, that’s called “secondary pigment dispersion syndrome”.
Some causes of secondary pigment dispersion syndrome include:
- Eye injuries
- Tumors or growths inside your eye
- An artificial intraocular lens (IOL) that moves out of position
Risk factors for developing pigmentary glaucoma
There are are several possible contributing factors for developing pigmentary glaucoma:
- Genetics. Research connects several DNA mutations with pigment dispersion syndrome and pigmentary glaucoma. That’s why pigment dispersion syndrome and pigmentary glaucoma can run in families but it’s usually in an unpredictable way. Direct examination of a small set of family members of patients with pigment dispersion syndrome showed that the disease was present in 2 out of 19 related individuals (12%) 26. In another family, signs of pigment dispersion syndrome were present in 36% of subjects’ parents and 50% of their siblings (but in no children), suggesting a possible autosomal dominant inheritance pattern with incomplete penetrance 27, 28, 29. Pigmentary glaucoma or pigment dispersion syndrome has also been described in families across multiple generations, with roughly 50% of family members described as having either condition, reinforcing the idea of an autosomal dominant inheritance pattern 30, 31.
- Male sex. Pigment dispersion syndrome and pigmentary glaucoma disproportionately affects males with case series showing a male to female ratio of between 2:1 and 5:1. Much less of a male predominance is noted for pigment dispersion syndrome, with case series describing male to female ratios between 1:1 and 2:1 32, 28, 33, 34, 35.
- Age. Diagnosis of pigment dispersion syndrome generally happens sometime between ages 20 and 50. Male patients with pigmentary glaucoma or pigment dispersion syndrome most often present in their 30s, whereas female patients typically present roughly a decade later in life 28, 33, 34, 36, 37. However, cases of pigment dispersion syndrome have been identified in patients as young as 12–15 years of age 38, 39, 40. Pigment dispersion syndrome and pigmentary glaucoma may be most common in middle age once the lens has enlarged and the iris is flexible enough to form a concave position 8.
- Race. People who are of Black or Asian descent have a lower risk for pigment dispersion syndrome and pigmentary glaucoma, while the risk for white people is higher 32, 33.
- Being nearsighted. People with myopia (nearsightedness) have a higher risk of pigment dispersion syndrome and pigmentary glaucoma. The more nearsighted you are (typically in the range of -3 to -4 D), the higher the risk of having pigment dispersion syndrome or having it turn into pigmentary glaucoma.
- Eye structure. Pigment dispersion syndrome and pigmentary glaucoma are more likely to happen when you have a deep anterior chamber. A deeper chamber means it can hold more fluid, which can make the iris “bow” backward toward the lens. Having flatter corneas can also be a contributing factor.
- Concave iris and posterior iris insertion. Concave iris and more posterior iris insertion are more common in patients with pigment dispersion syndrome or pigmentary glaucoma than in the normal population and result in greater iridolenticular contact in these individuals 41, 42, 43.
- Flat corneas. Patients with pigment dispersion syndrome and pigmentary glaucoma have significantly flatter corneas than control subjects of similar age and refractive error 44, 45. A flat cornea might be more likely to result in burping of aqueous humor from the posterior chamber to the anterior chamber with blinking, resulting in increased irido-zonular contact 45.
- Excessive activity level. Research links pigment dispersion syndrome and pigmentary glaucoma to excessive exercise or physical activity. If you have pigment dispersion syndrome or pigmentary glaucoma, your eye specialist will likely ask about how physically active you are. If your activity level could contribute to your pigment dispersion syndrome or pigmentary glaucoma — either now or in the future — your eye specialist will likely recommend reducing your activity level.
Disease Progression
- Intraocular pressure (IOP). A retrospective study from Olmstead County Minnesota found IOP > 21 mm Hg to be the only risk factor for progression from pigment dispersion syndrome to pigmentary glaucoma 28.
- Degree of iridolenticular contact in patients with asymmetric disease. More iris–lens contact in one eye vs the other may be associated with greater risk of disease progression 43.
- Greater trabecular meshwork pigmentation. In eyes with bilateral pigment dispersion syndrome, worse disease is typically found in the eye with more severe trabecular meshwork pigmentation.
Pigmentary glaucoma prevention
There’s nothing you can do to prevent pigment dispersion syndrome and pigmentary glaucoma. They happen unpredictably and people often don’t know they have these conditions until an eye specialist sees the changes during a routine eye exam or they start developing symptoms.
Pigmentary glaucoma signs and symptoms
Pigment dispersion syndrome (PDS) often doesn’t cause symptoms, so many people don’t know they have it. When it does, they’re usually similar to the most common glaucoma symptoms. Those include:
- Eye pain
- Eye redness
- Light sensitivity (photophobia)
- Blurred vision
- Seeing a glare or halos around lights after exercise.
In time, as the optic nerve becomes more damaged, you may notice that blank spots begin to appear in your field of vision. You usually won’t notice these blank spots in your day-to-day activities until the optic nerve is significantly damaged and these spots become large. If all of the optic nerve fibers die, blindness results. That is why it is so important to have an eye exam with your eye doctor.
Pigmentary glaucoma diagnosis
The most useful test for detecting pigment dispersion syndrome before it causes symptoms is a routine eye exam.
Some of the changes that pigment dispersion syndrome or pigmentary glaucoma can cause that show up on an eye exam include:
- Krukenberg spindle. This is a faint, vertical line in front of your pupil that’s the same color as your iris (see Figure 1 above). It happens when higher pressure inside your eye pushes fluid forward and keeps loose pigment granules pressed against the inside surface of your cornea.
- Radial iris defects. These are thin lines on your iris with worn-away pigment. They look like the spokes on a bicycle wheel. An eye specialist can see them using special lighting techniques.
- Pigment accumulation near the outer rim of your iris. Your eye specialist can use a technique called gonioscopy to see pigment granules deposited there.
Several glaucoma tests can help with diagnosing pigment dispersion syndrome and pigmentary glaucoma. Some of these are common features of a routine eye exam, while others are a little more specific. Your eye specialist can tell you which tests they think will be the most helpful for diagnosing or ruling out pigment dispersion syndrome and pigmentary glaucoma.
These tests often include one or more of the following:
- Visual acuity testing. A visual acuity test assesses how clearly someone can see at a distance, typically using a Snellen chart or other standardized chart. The test is performed by an optometrist or ophthalmologist and involves reading progressively smaller letters or identifying shapes, with the results expressed as a fraction like 20/20 or 6/6, indicating the distance at which the person can see the letters or shapes
- Visual field testing also called perimetry. This check of your peripheral (side) vision allows your eye care provider to find out how well you can see objects off to the side of your vision without moving your eyes. This test measures the entire area the forward-looking eye sees to document straight-ahead (central) and side (peripheral) vision. It measures the dimmest light seen at each spot tested. Each time patients perceive a flash of light, they respond by pressing a button.
- Depth perception testing. A depth perception test assesses your ability to see the world in three dimensions (3D) and judge distances accurately. It checks if your eyes work together and if your brain processes the visual information correctly. These tests use 3D images or patterns like the Randot Stereo test to gauge how well your eyes coordinate to perceive depth. Some tests involve holding a finger in front of your eyes and focusing on a distant object, checking for double vision of the finger.
- Tonometry. This measures the pressure inside your eye. Increased eye pressure is the most important risk factor for glaucoma. There are several methods of measuring eye pressure. The most common method is known as applanation, in which a tiny instrument contacts the eye’s surface after it is numbed with an eye drop.
- Air-puff test. You’ll rest your chin on a machine and your eye specialist will blow a puff of air into your eye. This quick and painless test is used as part of a routine glaucoma screening. If the results show that your eye pressure is high, your eye specialist will do other eye-pressure tests to get a more accurate measurement.
- Applanation tonometry. Your eye specialist will numb your eyes with drops before measuring your eye pressure using one of these methods:
- You’ll rest your chin on a special magnifying device called a slit lamp. Your eye care specialist will examine your eye through the slit lamp while gently pressing a special tool on your eye to test the pressure.
- Your eye care specialist will gently press a handheld device against your eye. The device measures your eye pressure.
- Pachymetry. Pachymetry is a simple, painless test that measures the thickness of the cornea, the clear front part of the eye. The eye doctor uses an ultrasonic wave instrument to help determine the thickness of the cornea and better evaluate eye pressure.
- Ophthalmoscopy. Your eye care specialist will do a dilated eye exam to look for damage to your optic nerve. This exam is part of a routine glaucoma check-up. You’ll be given eye drops that widen (dilate) your pupils (the openings that let light into your eyes). You’ll look straight ahead while your eye care specialist looks into your eye using a device with a light and magnifying lens.
- Slit lamp exam. A slit lamp exam is a common eye test that uses a microscope with a focused beam of light to examine the front of your eye and the back of your eye with the aid of special lenses.
- Gonioscopy. Gonioscopy is a specialized eye examination that allows an ophthalmologist to visualize the anterior chamber angle, the space between the iris and the cornea where fluid drains out of the eye. Gonioscopy is a crucial part of diagnosing and monitoring glaucoma and other eye conditions
If your eye specialist has a reason to suspect damage to your retina and/or optic nerve, they may also use additional types of eye imaging. These include:
- Optical coherence tomography (OCT). Optical Coherence Tomography (OCT) measures the reflection of laser light similar to the way that ultrasound measures the reflection of sound. Using this device, a 3D reconstruction of the optic nerve can be created. Optical coherence tomography (OCT) is valuable for monitoring morphological changes in the optic nerve and retinal nerve fiber layer, especially in patients with ocular hypertension and early-to-moderate glaucoma 61. The most recent advances of OCT include OCT-A, or OCT-Angiography, whereby the blood flow to vessels surrounding the optic nerve and in the macula can be measured. This is still an active area of research, but scientists do know that some patients’ optic nerves are very vulnerable to changes in optic nerve blood flow, and this new measurement may be useful in evaluating these patients.
- Heidelberg Retina Tomograph (HRT): Heidelberg Retina Tomograph (HRT) is also a laser that can produce a 3D representation of the optic nerve.
- Nerve Fiber Analyzer (GDx): Nerve Fiber Analyzer (GDx) uses laser light to measure the thickness of the nerve fiber layer.
- Fluorescein angiography. Fluorescein angiography is a diagnostic test used to examine the blood vessels in the retina and choroid of the eye. Fluorescein angiography involves injecting a fluorescent dye into the bloodstream and taking photographs of your retina and its blood vessels as the dye circulates, revealing potential blockages, leaks, or other abnormalities in the blood vessels. Fluorescein angiography is often recommended to find and diagnose eye disease including 62:
- macular edema (swelling in the retina that distorts vision)
- diabetic retinopathy (damaged or abnormal blood vessels in the eye caused by diabetes)
- macular degeneration
- blockage of veins inside the eye, called branch retinal vein occlusion (BRVO) or central retinal vein occlusion (CRVO)
- macular pucker (a wrinkle in the retina caused by a buildup of fluid behind it)
- ocular melanoma (a type of cancer affecting the eye)
- rack changes in eye disease over time
- target treatment areas
- Less commonly, ultrasound, computed tomography (CT) or magnetic resonance imaging (MRI).
Pigmentary glaucoma treatment
Pigment dispersion syndrome treatment varies depending on how it is affecting your eye pressure (IOP):
- For pigment dispersion syndrome with normal or only slightly elevated intraocular pressure (IOP), there is a low risk of damage to the optic nerve. No treatment is needed other than seeing your ophthalmologist one time each year. They will monitor your condition by checking your IOP and looking for any changes in your vision.
- For pigment dispersion syndrome with elevated intraocular pressure (IOP), there is a greater risk of damage to the optic nerve. To lower IOP, you may be treated with medicated eye drops or laser therapy.
- When intraocular pressure (IOP) from pigment dispersion syndrome is so high that it damages the optic nerve, this is then called “pigmentary glaucoma”. In this case, treatment is needed and it may be medicated eye drops, laser therapy, or surgery.
Table 1. Glaucoma medications
| Intraocular pressure lowering agents | ||||||
|---|---|---|---|---|---|---|
| Drug Class | Example | Mechanism | IOP Lowering | Dosing | Side Effects | Notes |
| Prostaglandin F2a analogues | Latanoprost (Xalatan) Travoprost (Travatan) Bimatoprost (Lumigan) Tafluprost (Zioptan; preservative free) Latanoprostene bunod (Vyzulta) | Increase outflow via uveoscleral pathway; decrease outflow resistance; mechanism unclear | Latanaprost and Travoprost: 25-32% Bimatoprost: 27-33% Tafluprost: 27-31% Latanoprostene: As a class, most potent | Once daily, usually in evening | Ocular: Irritation, increased pigmentation of iris, lashes, and skin, hypertrichosis, prostaglandin associated periorbitopathy, loss of orbital fat over time | Often preferred as first line; highly effective at IOP lowering, with minimal systemic side effects. Among preservative containing drops, side effects tend to be greatest with bimatoprost, and least with latanoprost. Preservative free tafluprost may reduce irritation and ocular side effects and improve compliance in some patients.2 |
| Systemic: flu-like symptoms, myalgias and arthralgias, nasal congestion; generally very well tolerated | ||||||
| Beta blockers (beta-adrenergic antagonists) | Non-Selective: Timolol maleate (Timoptic; Timoptic occudose = preservative free)Timolol hemihydrate (Betimol)Levobunolol (Betagan)MetipranololCarteolol HCl (partial alpha agonist) | Decrease aqueous production | 20-30% | 1-2 times daily OR Once daily in morning; more effective in AM | Ocular: Blurring, irritation, punctate keratitis; metipranolol associated with uveitis | Generally well tolerated from the perspective of ocular side effects. History of asthma or other airway disease is a strong contraindication. Suspect side effects of therapy in a patient with new onset depression, lethargy, or sexual dysfunction. Carteolol may have less detrimental effect on lipid profile in some patients.3 Betaxolol may be slightly less likely to cause asthma or lung disease exacerbation, but still carries significant risk.4 |
| Systemic: symptoms of b-blockade: heart block and bradycardia, decreased exercise tolerance, asthma and lung disease exacerbation, decreased symptoms of hypoglycemia in diabetes, depression, sexual dysfunction, lipid profile changes | ||||||
| Selective b 1: Betaxalol | Same | 15-20% | 2 times daily | |||
| Alpha agonists (Alpha2-adrenergic agonists) | Apraclonidine HCl (Iopidine) Brimonidine tartrate (Alphagan) | Decreases aqueous production, increases uveoscleral outflow to lesser extent | 20-30% | 2-3 times daily | Ocular: Irritation, allergy, pruritis, dry eye | As a class, most likely to cause ocular irritation. High risk of apnea and CNS depression in infants with brimonidine. If CNS depression is a particular concern in any patient, apraclonidine does not cross blood-brain barrier and may be better choice.5,6 |
| Systemic: Lethargy, hypotension, vasovagal attack, headache, dry mouth and nose, insomnia, anxiety; risk of apnea and CNS depression in infants with brimonidine, apraclonidine will not cross blood-brain barrier | ||||||
| Carbonic anhydrase inhibitors | Oral: Acetazolamide (Diamox)Methazolamide (Neptazane) | Decreases aqueous production | 15-20% | Acetazolamide: 500-1000mg per day in 2-4 doses Methazolamide: 25-50mg 2-3 times per day IV Acetazolamide: 5-10mg/kg q6-8 hours | Ocular: None | Sulfa allergies are often cited as a contraindication to use of these drugs, but there is little structural overlap with antibiotic sulfa drugs, and thus most patients allergic to sulfa drugs will not be affected by carbonic anhydrase inhibitors. 7 |
| Systemic: hypokalemia, poor tolerance of carbonated beverages, acidosis, paresthesias, blood dyscrasias, lethargy, nephrolithiasis, others
| ||||||
| Topical: Dorzolamide (Trusopt)Brinzolamide (Azopt) | Same | Generally not as effective as oral acetazolamide | 2 times daily (only FDA approved for 3 times daily) | Ocular: Induced myopia, blurred vision, stinging (less with Brinzolamide), allergic conjunctivitis, keratopathy | Generally very safe, often used in infants and pregnant women. | |
| Systemic: Less than with oral agents; bad taste in mouth | ||||||
| Parasympathomimetic agents | Pilocarpine HCl Echothiophate iodide (Phospholine iodide) | Miotics; increase trabecular outflow; ciliary muscles contract, put traction on scleral spur, open trabecular meshwork | 15-25% | Pilocarpine: 2-4 times daily, usually 4 times daily Echothiopentate: 1-2 times daily, usually 2 times daily | Ocular: Posterior synechiae, intense miosis, keratitis, cataract, retinal detachment, angle closure, epiphora, induced myopia | Consider echothiophate in patients with a complicated anterior segment, e.g. aphakia, PK, ACIOL, etc., with inadequate pressure control. In certain patients it can be the sole effective drug.8 |
| Systemic: increased salivation, increased gastric secretion, abdominal cramps | ||||||
| Rho kinase inhibitors | Netarsudil (Rhopressa) | Increases trabecular outflow, decreases episcleral venous pressure9 | Reduces IOP by ~5.5-6 mmHg regardless of baseline IOP10 | FDA approved for once daily, more efficacious when used twice daily in studies | Ocular: conjunctival hyperemia and hemorrhage, corneal deposits (verticillata), blurry vision, epiphora, pruritis, punctate keratitis, eyelid erythema, conjunctival edema, foreign body sensation | Though not as effective at IOP reduction as other classes, may have benefit in patients with lower baseline IOP (IOP reduction less dependent on baseline IOP than other classes), and as an adjunct to other drugs, as mechanism of action (increases trabecular outflow rather than uveoscleral) is different from the most commonly used classes.10 |
| Systemic: None achieving statistical significance in recent studies10 | ||||||
| Hyperosmotic agents | Mannitol 20% (parenteral) Glycerol 50% (oral) | Creates osmotic gradient, dehydrates vitreous | Mannitol: 0.5-2.0 g/kg Glycerol: 1-1.5 g/kg | Ocular: IOP rebound, aqueous flare | ||
| Systemic: urinary retention, headache, nausea, vomiting, diarrhea, electrolyte disturbances, cardiac complications, contraindicated in renal failure | ||||||
Eye drops
Glaucoma treatment often starts with prescription eye drops. Some may decrease eye pressure by improving how fluid drains from your eye. Others decrease the amount of fluid your eye makes. Depending on how low your eye pressure needs to be, more than one eye drop may be prescribed.
Prescription eye drop medicines include:
- Prostaglandins. These increase the outflow of the fluid in your eye, helping to reduce eye pressure (IOP). Medicines in this category include latanoprost (Xalatan), travoprost (Travatan Z), tafluprost (Zioptan), bimatoprost (Lumigan) and latanoprostene bunod (Vyzulta). Possible side effects include mild reddening and stinging of the eyes, darkening of the iris, darkening of the pigment of the eyelashes or eyelid skin, and blurred vision. This class of medicine is prescribed for once-a-day use.
- Beta blockers. These reduce the production of fluid in your eye, helping to lower eye pressure. Examples include timolol (Betimol, Istalol, Timoptic) and betaxolol (Betoptic S). Possible side effects include difficulty breathing, slowed heart rate, lower blood pressure, impotence and fatigue. This class of medicine can be prescribed for once- or twice-daily use depending on your condition.
- Alpha-adrenergic agonists. These reduce the production of the fluid that flows throughout the inside of your eye. They also increase the outflow of fluid in the eye. Examples include apraclonidine (Iopidine) and brimonidine (Alphagan P, Qoliana). Possible side effects include irregular heart rate; high blood pressure; fatigue; red, itchy or swollen eyes; and dry mouth. This class of medicine is usually prescribed for twice-daily use but sometimes can be prescribed for use three times a day.
- Carbonic anhydrase inhibitors. These medicines reduce the production of fluid in your eye. Examples include dorzolamide and brinzolamide (Azopt). Possible side effects include a metallic taste, frequent urination, and tingling in the fingers and toes. This class of medicine is usually prescribed for twice-daily use but sometimes can be prescribed for use three times a day.
- Rho kinase inhibitor. This medicine lowers eye pressure by suppressing the rho kinase enzymes responsible for fluid increase. It is available as netarsudil (Rhopressa) and is prescribed for once-a-day use. Possible side effects include eye redness and eye discomfort.
- Miotic or cholinergic agents. These increase the outflow of fluid from your eye. An example is pilocarpine (Isopto Carpine). Side effects include headache, eye pain, smaller pupils, possible blurred or dim vision, and nearsightedness. This class of medicine is usually prescribed to be used up to four times a day. Because of potential side effects and the need for frequent daily use, these medicines are not prescribed very often anymore.
Combination drugs:
- Timolol/Brinzolamide (Azarga-not available in the US)
- Timolol/Dorzolamide (Cosopt)
- Timolol/Latanoprost (Xalacom-not available in the US)
- Timolol/Bimatoprost (Ganfort-not available in the US)
- Timolol/Brimonidine (Combigan)
- Brinzolamide/Brimonidine (Simbrinza)
Because some of the eye drop medicine is absorbed into the bloodstream, you may experience some systemic side effects unrelated to your eyes. To minimize this absorption, close your eyes for 1 to 2 minutes after putting the drops in. You also may press lightly at the corner of your eyes near your nose to close the tear duct for 1 to 2 minutes. Wipe off any unused drops from your eyelid.
You may be prescribed multiple eye drops or need to use artificial tears. Make sure you wait at least five minutes in between using different drops.
Never change or stop taking your glaucoma medications without talking to your ophthalmologist. If you are about to run out of your medication, ask your ophthalmologist if you should have your prescription refilled.
Alpha agonists for glaucoma
Alpha agonists also called alpha2-adrenergic agonists work by reducing the amount of fluid your eye produces. Alpha agonists also increase the amount of fluid that drains out of the eyes. This helps lower eye pressure and, hopefully, saves your vision.
Possible side effects of alpha agonists include:
- red, stinging or painful eyes after using drops
- blurry vision
- allergy (redness, itching, tearing and swelling of the eye)
- a large (dilated) pupil
- headaches
- dry mouth
- feeling tired, weak or dizzy
- decreased blood pressure
- a fast or irregular heartbeat
- feeling nervous
Blurry vision, stinging, and redness may improve with time. But if the side effects still bother you, call your ophthalmologist. They may be able to lower your dose or change your medicine. Most side effects go away when the medicine is stopped. If you feel you need to stop taking this medication due to side effects or other concerns, please discuss with your doctor.
Beta-blockers for glaucoma
Beta-blockers also called beta-adrenergic antagonists work by reducing the amount of fluid your eye produces. This helps lower pressure in your eye and, hopefully, saves your vision.
Possible side effects of beta-blockers include:
- red, stinging or painful eyes after using drops.
- blurry vision
- breathing problems in people with asthma, emphysema, or chronic obstructive pulmonary disease (COPD)
- a slow or irregular heartbeat
- feeling tired
- depression
- dizziness
- a change in sex drive or sexual function
- getting overly tired during exercise
- in people with diabetes, low blood sugar symptoms becoming difficult to notice
Blurry vision, stinging, and redness may improve with time. But if the side effects still bother you, call your ophthalmologist. They may be able to lower your dose or change your medicine. Most side effects go away when the medication is stopped. Never suddenly quit taking your medicine unless your doctor tells you to.
Carbonic anhydrase inhibitors for glaucoma
Carbonic anhydrase inhibitors work by reducing the amount of fluid your eye produces. This helps lower eye pressure and, hopefully, saves your vision. Your ophthalmologist may have you take this medicine as an eye drop or by mouth as a pill.
Possible side effects of carbonic anhydrase inhibitors include:
- stinging eyes after putting drops in.
- red eyes
- blurry vision
- a skin rash (especially in people who are allergic to sulfa drugs)
- changes in how things taste to you (especially with carbonated drinks)
- bad taste or upset stomach (nausea)
- feeling tired
- decreased energy
- increase in urination (with the pills)
- tingling around the mouth and fingertips (with the pills)
- lower potassium (with the pills)
Blurry vision, stinging, and redness may improve with time. But if the side effects still bother you, call your ophthalmologist. They may be able to lower your dose or change your medicine. Most side effects go away when the medication is stopped. Never suddenly quit taking your medicine unless your doctor tells you to.
Miotics for glaucoma
Miotics also called cholinergic agents make your pupil constrict (get smaller or miosis), increasing the amount of fluid that drains out of the eye. This helps lower eye pressure and, hopefully, helps protect your vision.
Possible side effects of miotics include:
- blurred vision
- nearsightedness (trouble focusing on distant objects)
- dim vision with difficulty seeing in the dark or at night
- headache or brow ache (aching around eye)
While very rare, there is the possibility that your retina could detach. This is when the light-sensitive tissue lining the back of the eye pulls away. You would suddenly notice dark specks or spots (floaters) or flashing lights in your vision. If you have these symptoms, see your ophthalmologist immediately.
Side effects may go away after you take the medicine for a while. But if the side effects still bother you, call your ophthalmologist. They may be able to lower your dose or change your medicine. If you feel you need to stop taking this medication due to side effects or other concerns, please discuss with your doctor.
Prostaglandin analogs for glaucoma
Prostaglandin analogs also called prostaglandin F2a analogues work by increasing the drainage of fluid out of your eye. This helps lower eye pressure and, hopefully, saves your vision.
Possible side effects of prostaglandin analogs include:
- red, stinging or painful eyes after using drops.
- feeling like something is in your eye
- blurry vision
- a permanent change in your eye color (occurs mostly in hazel eyes)
- an increase in thickness, number and length of eyelashes
- darkening of the eyelid
- worsening of existing angina and asthma
- joint aches
- light sensitivity
- eyes gradually sinking deeper into their sockets, keeping eyelids from working properly
Blurry vision, stinging, and redness may improve with time. But if the side effects still bother you, call your ophthalmologist. They may be able to lower your dose or change your medicine. Most side effects go away when the medication is stopped. Never suddenly quit taking your medicine unless your doctor tells you to.
Oral medicines
Eye drops alone may not bring eye pressure down to the desired level. So an eye doctor also may prescribe oral medicine. This medicine is usually a carbonic anhydrase inhibitor. Possible side effects include frequent urination, tingling in the fingers and toes, depression, stomach upset, and kidney stones.
Surgery, laser and other therapies
Other treatment options include laser therapy and surgery. The following techniques may help to drain fluid within the eye and lower eye pressure:
- Laser trabeculoplasty is an option if eye drops can’t be tolerated. Laser trabeculoplasty also may be used if medicine hasn’t slowed the progression of the glaucoma. An eye doctor also may recommend laser surgery before using eye drops. It’s done in the eye doctor’s office. An eye doctor uses a small laser to improve the drainage of the tissue located at the angle where the iris and cornea meet. It may take a few weeks before the full effect of this procedure becomes apparent.
- Laser iridotomy. Laser iridotomy is for people who have angle-closure glaucoma. The ophthalmologist uses a laser to create a tiny hole in the iris. This hole helps fluid flow to the drainage angle.
- Glaucoma filtration surgery also called a trabeculectomy. The eye doctor (ophthalmologist) creates an opening in the white of your eye, which also is known as the sclera. This is where your eye surgeon creates a tiny flap in the sclera. They will also create a bubble like a pocket in the conjunctiva called a filtration bleb. It is usually hidden under the upper eyelid and cannot be seen. Aqueous humor will be able to drain out of the eye through the flap and into the bleb, lowering eye pressure. In the bleb, the fluid is absorbed by tissue around your eye.
- Drainage tubes. In this procedure, the eye surgeon inserts a small drainage tube in your eye to drain excess fluid to lower eye pressure. The glaucoma drainage implant sends the fluid to a collection area called a reservoir. Your eye surgeon creates this reservoir beneath the conjunctiva. The fluid is then absorbed into nearby blood vessels.
- Minimally invasive glaucoma surgery (MIGS). An eye doctor may suggest a minimally invasive glaucoma surgery (MIGS) procedure to lower eye pressure. This procedure generally require less immediate postoperative care and have less risk than trabeculectomy or using a drainage device. A minimally invasive glaucoma surgery (MIGS) procedure is often combined with cataract surgery. There are a number of minimally invasive glaucoma surgery (MIGS) techniques available.
- Cataract surgery. For some people with narrow angles, removing the eye’s natural lens can lower eye pressure. With narrow angles, the iris and the cornea are too close together. This can cover (block) the eye’s drainage channel. Removing the eye’s lens with cataract surgery creates more space for fluid to leave the eye. This can lower eye pressure.
After your procedure, you’ll need to see your eye doctor for follow-up exams. You can expect to visit your ophthalmologist about every 3 to 6 months. However, this can vary depending on your treatment needs. And you may eventually need to undergo additional procedures if your eye pressure begins to rise or other changes happen in your eye.
Laser iridotomy
Some reports have demonstrated that laser iridotomy can eliminate iris concavity and reduce iridolenticular contact in eyes with pigment dispersion syndrome 64, 65, 66, 14. However, some eyes may retain a concave iris configuration even after laser treatment 67. In addition, laser iridotomy may not always prevent exercise-induced pigment release and intraocular pressure (IOP) elevation 68, 69. There is limited data on whether laser iridotomy is effective in controlling intraocular pressure (IOP) in patients with pigment dispersion syndrome or pigmentary glaucoma. While one small randomized controlled trial of 21 patients demonstrated a lower rate of IOP elevation over 2 years of follow-up in eyes treated with laser iridotomy as compared to eyes that were not 70, a retrospective study of 60 patients did not suggest any laser iridotomy benefit 71. A 2016 Cochrane review based on 5 randomized controlled trials showed that there was inadequate evidence to use peripheral iridotomy to treat pigmentary glaucoma, and further studies are needed to evaluate the clinical use of this laser treatment in pigment dispersion syndrome and pigmentary glaucoma patients 72.
Follow-up after laser iridotomy is similar to the follow-up for iridotomy performed for angle closure glaucoma.
Rise in IOP after laser iridotomy is greater in pigment dispersion syndrome and pigmentary glaucoma patients than in patients with occludable angles. Ways to mitigate this concern include the use of lower energy levels for surgery, the administration of alpha-adrenergic agonists before and after the laser treatment, and the use of argon laser instead of YAG laser, as it is less disruptive in terms of pigment liberation and inflammation 73.
Pigmentary glaucoma prognosis
Not everyone who has pigment dispersion syndrome will have it lead to pigmentary glaucoma. But the risk of it doing so goes up over time. About 10% of people with pigment dispersion syndrome will develop pigmentary glaucoma within 10 years. That number rises to 15% after 15 years 1. The lifetime risk is between 35% and 50%.
Because pigment dispersion syndrome and pigmentary glaucoma usually start much earlier in life than other forms of glaucoma, it’s important to manage this condition as best you can. Part of that is seeing your eye specialist for regular follow-ups. Those visits can happen every three to six months or yearly, depending on the details of your case. Follow-up visits allow your eye doctor to detect pressure increases and recommend treatment to prevent damage or at least stop it from getting worse.
Ongoing monitoring and managing of your pigment dispersion syndrome or pigmentary glaucoma are key to keeping your eyesight. It’s rare for people who prioritize follow-up visits and manage their condition based on their specialist’s recommendations to have permanent blindness 74.
In a community-based study of 113 patients with pigment dispersion syndrome or pigmentary glaucoma who were followed for a median of 6 years, 1 patient experienced unilateral blindness and another became bilaterally blind 28. In the same study, 10% of patients with pigment dispersion syndrome progressed to pigmentary glaucoma at 5 years, while 15% progressed at 10 years; 23% of patients were noted to have pigmentary glaucoma at diagnosis 28. Visual fields worsened in 44% of patients with pigmentary glaucoma over a mean follow-up period of 6 years. A group of patients followed from a glaucoma clinic showed higher rates of progression (35% over a median follow-up at 15 years), and roughly 40% of patients with pigmentary glaucoma experienced worsening of optic nerve damage 37. In some cases, trabecular meshwork pigmentation and iris transillumination defects have been observed to normalize over time, as has elevated IOP, suggesting return of normal trabecular meshwork function 75, 35, 40, 76. Some older patients with a diagnosis of normal tension glaucoma have been identified with iris transillumination defects and dense trabecular meshwork pigmentation, suggesting they may have had pigmentary glaucoma at some point with subsequent IOP normalization due to cessation of pigment release 77. In such patients, the presence of “pigment reversal sign” helps to distinguish between different types of glaucoma.
- Gurnani B, Kaur K. Pigment Dispersion Syndrome. [Updated 2023 Jun 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK580526[↩][↩][↩]
- Pigmentary Glaucoma and Pigment Dispersion Syndrome. https://eyewiki.org/Pigmentary_Glaucoma_and_Pigment_Dispersion_Syndrome[↩][↩]
- What Is Pigment Dispersion Syndrome? https://www.aao.org/eye-health/diseases/what-is-pigment-dispersion-syndrome[↩]
- Pigmentary Glaucoma. https://glaucoma.org/types/pigmentary-glaucoma[↩]
- Zeppieri M. Pigment dispersion syndrome: A brief overview. J Clin Transl Res. 2022 Sep 7;8(5):344-350. https://pmc.ncbi.nlm.nih.gov/articles/PMC9741933[↩][↩][↩]
- Scuderi G, Contestabile MT, Scuderi L, Librando A, Fenicia V, Rahimi S. Pigment Dispersion Syndrome and Pigmentary Glaucoma:A Review and Update. Int Ophthalmol. 2019;39:1651–62. doi: 10.1007/s10792-018-0938-7[↩][↩]
- Niyadurupola N, Broadway DC. Pigment dispersion syndrome and pigmentary glaucoma–a major review. Clin Exp Ophthalmol. 2008;36:868–82. doi: 10.1111/j.1442-9071.2009.01920.x[↩]
- Campbell DG. Pigmentary Dispersion and Glaucoma: A New Theory. Arch Ophthalmol. 1979;97(9):1667–1672. doi:10.1001/archopht.1979.01020020235011[↩][↩][↩][↩][↩][↩]
- Kampik A, Green WR, Quigley HA, Pierce LH. Scanning and transmission electron microscopic studies of two cases of pigment dispersion syndrome. Am J Ophthalmol. 1981 May;91(5):573-87. doi: 10.1016/0002-9394(81)90055-6[↩][↩][↩][↩][↩][↩]
- Mardin CY, Küchle M, Nguyen NX, Martus P, Naumann GO. Quantification of aqueous melanin granules, intraocular pressure and glaucomatous damage in primary pigment dispersion syndrome. Ophthalmology. 2000 Mar;107(3):435-40. doi: 10.1016/s0161-6420(99)00089-5[↩][↩][↩][↩]
- Campbell DG, Schertzer RM. Pathophysiology of Pigment Dispersion Syndrome and Pigmentary Glaucoma. Curr Opin Ophthalmol. 1995;6:96–101. doi: 10.1097/00055735-199504000-00015[↩][↩]
- Ritch R. A unification hypothesis of pigment dispersion syndrome. Trans Am Ophthalmol Soc. 1996;94:381-405; discussion 405-9. https://pmc.ncbi.nlm.nih.gov/articles/instance/1312105/pdf/taos00005-0402.pdf[↩][↩]
- Potash SD, Tello C, Liebmann J, Ritch R. Ultrasound Biomicroscopy in Pigment Dispersion Syndrome. Ophthalmology. 1994;101:332–9. doi: 10.1016/s0161-6420(94)31331-5[↩][↩]
- Karickhoff JR. Pigmentary dispersion syndrome and pigmentary glaucoma: a new mechanism concept, a new treatment, and a new technique. Ophthalmic Surg. 1992 Apr;23(4):269-77.[↩][↩][↩]
- Jewelewicz DA, Radcliffe NM, Liebmann J, Ritch R. Temporal evolution of intraocular pressure elevation after pupillary dilation in pigment dispersion syndrome. J Glaucoma. 2009 Mar;18(3):184-5. doi: 10.1097/IJG.0b013e318182edbf[↩][↩]
- Richter CU, Richardson TM, Grant WM. Pigmentary Dispersion Syndrome and Pigmentary Glaucoma: A Prospective Study of the Natural History. Arch Ophthalmol. 1986;104(2):211–215. doi:10.1001/archopht.1986.01050140065021[↩][↩]
- Richardson TM, Hutchinson BT, Grant WM. The Outflow Tract in Pigmentary Glaucoma: A Light and Electron Microscopic Study. Arch Ophthalmol. 1977;95(6):1015–1025. doi:10.1001/archopht.1977.04450060101010[↩][↩]
- Lichter PR. Pigmentary glaucoma–current concepts. Trans Am Acad Ophthalmol Otolaryngol. 1974 Mar-Apr;78(2):OP309-13.[↩][↩]
- Kupfer C, Kuwabara T, Kaiser-Kupfer M. The Histopathology of Pigmentary Dispersion Syndrome with Glaucoma. Am J Ophthalmol. 1975;80:857–62. doi: 10.1016/0002-9394(75)90283-4[↩][↩]
- Fine BS, Yanoff M, Scheie HG. Pigmentary “glaucoma”. A histologic study. Trans Am Acad Ophthalmol Otolaryngol. 1974 Mar-Apr;78(2):OP314-25.[↩][↩]
- Mauksch H. Über Idiopathischen Zerfall des Retinalen Pigmentblattes der Iris bei Zwei Brudern. Z Augenheilkd. 1925;57:262.[↩][↩]
- McDermott JA, Ritch R, Berger A, Wang RF. Inheritance of Pigmentary Dispersion Syndrome. Invest Ophthalmol Vis Sci. 1987;28:153.[↩][↩]
- Scheie HG, Cameron JD. Pigment Dispersion Syndrome:A Clinical Study. Br J Ophthalmol. 1981;65:264–9. doi: 10.1136/bjo.65.4.264[↩][↩]
- Andersen JS, Pralea AM, DelBono EA, Haines JL, Gorin MB, Schuman JS, et al. A Gene Responsible for the Pigment Dispersion Syndrome Maps to Chromosome 7q35-q36. Arch Ophthalmol. 1997;115:384–8. doi: 10.1001/archopht.1997.01100150386012[↩][↩]
- Lascaratos G, Shah A, Garway-Heath DF. The Genetics of Pigment Dispersion Syndrome and Pigmentary Glaucoma. Surv Ophthalmol. 2013;58:164–75. doi: 10.1016/j.survophthal.2012.08.002[↩][↩]
- Roberts DK, Meetz RE, Chaglasian MA. The inheritance of the pigment dispersion syndrome in blacks. J Glaucoma. 1999 Aug;8(4):250-6.[↩][↩]
- McDermott JA et al. Familial occurrence of pigmentary dispersion syndrome. Invest Ophthalmolol Vis Sci. 1987;28(suppl):136.[↩][↩]
- Siddiqui Y, Ten Hulzen RD, Cameron JD, Hodge DO, Johnson DH. What is the risk of developing pigmentary glaucoma from pigment dispersion syndrome? Am J Ophthalmol. 2003 Jun;135(6):794-9. doi: 10.1016/s0002-9394(02)02289-4. Erratum in: Am J Ophthalmol. 2003 Sep;136(3):592.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Gaton D, Barak A, Segev S, Yassur Y, Treister G. [Prevalence of pigmentary dispersion syndrome in Israel]. Harefuah. 1998 Mar 1;134(5):337-9, 424. Hebrew.[↩][↩]
- STANKOVIC I. [A contribution to the knowledge of the heredity of pigment glaucoma]. Klin Monbl Augenheilkd Augenarztl Fortbild. 1961 Sep;139:165-74. German.[↩][↩]
- Andersen JS, Pralea AM, DelBono EA, Haines JL, Gorin MB, Schuman JS, Mattox CG, Wiggs JL. A gene responsible for the pigment dispersion syndrome maps to chromosome 7q35-q36. Arch Ophthalmol. 1997 Mar;115(3):384-8. doi: 10.1001/archopht.1997.01100150386012[↩][↩]
- Scheie HG, Cameron JD. Pigment dispersion syndrome: a clinical study. Br J Ophthalmol. 1981 Apr;65(4):264-9. doi: 10.1136/bjo.65.4.264[↩][↩][↩][↩]
- Sugar HS. Pigmentary glaucoma. A 25-year review. Am J Ophthalmol. 1966 Sep;62(3):499-507. doi: 10.1016/0002-9394(66)91330-4[↩][↩][↩][↩][↩][↩]
- Gillies WE, Brooks AM. Clinical features at presentation of anterior segment pigment dispersion syndrome. Clin Exp Ophthalmol. 2001 Jun;29(3):125-7. doi: 10.1046/j.1442-9071.2001.00391.x[↩][↩][↩][↩]
- Lichter PR, Shaffer RN. Diagnostic and prognostic signs in pigmentary glaucoma. Trans Am Acad Ophthalmol Otolaryngol. 1970 Sep-Oct;74(5):984-98.[↩][↩][↩]
- BICK MW. Sex differences in pigmentary glaucoma. Am J Ophthalmol. 1962 Nov;54:831-7. doi: 10.1016/0002-9394(62)94170-3[↩][↩]
- Migliazzo CV, Shaffer RN, Nykin R, Magee S. Long-term analysis of pigmentary dispersion syndrome and pigmentary glaucoma. Ophthalmology. 1986 Dec;93(12):1528-36. doi: 10.1016/s0161-6420(86)33526-7[↩][↩][↩]
- SCHEIE HG, FLEISCHHAUER HW. Idiopathic atrophy of the epithelial layers of the iris and ciliary body; a clinical study. AMA Arch Ophthalmol. 1958 Feb;59(2):216-28. doi: 10.1001/archopht.1958.00940030084007[↩][↩]
- Kaiser-Kupfer MI, Kupfer C, McCain L. Asymmetric pigment dispersion syndrome. Trans Am Ophthalmol Soc. 1983;81:310-24. https://pmc.ncbi.nlm.nih.gov/articles/instance/1312456/pdf/taos00018-0336.pdf[↩][↩]
- Rodrigues MM, Spaeth GL, Weinreb S, Sivalingam E. Spectrum of trabecular pigmentation in open-angle glaucoma: a clinicopathologic study. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol. 1976 Mar-Apr;81(2):258-76.[↩][↩][↩]
- Doyle JW, Hansen JE, Smith MF, Hamed LM, McGorray S, Sherwood MB. Use of scheimpflug photography to study iris configuration in patients with pigment dispersion syndrome and pigmentary glaucoma. J Glaucoma. 1995 Dec;4(6):398-405.[↩][↩]
- Mora P, Sangermani C, Ghirardini S, Carta A, Ungaro N, Gandolfi S. Ultrasound biomicroscopy and iris pigment dispersion: a case–control study. Br J Ophthalmol. 2010 Apr;94(4):428-32. doi: 10.1136/bjo.2009.162065[↩][↩]
- Kanadani FN, Dorairaj S, Langlieb AM, Shihadeh WA, Tello C, Liebmann JM, Ritch R. Ultrasound biomicroscopy in asymmetric pigment dispersion syndrome and pigmentary glaucoma. Arch Ophthalmol. 2006 Nov;124(11):1573-6. doi: 10.1001/archopht.124.11.1573[↩][↩][↩]
- Lord FD, Pathanapitoon K, Mikelberg FS. Keratometry and axial length in pigment dispersion syndrome: a descriptive case-control study. J Glaucoma. 2001 Oct;10(5):383-5. doi: 10.1097/00061198-200110000-00003[↩][↩]
- Yip LW, Sothornwit N, Berkowitz J, Mikelberg FS. A comparison of interocular differences in patients with pigment dispersion syndrome. J Glaucoma. 2009 Jan;18(1):1-5. doi: 10.1097/IJG.0b013e31816f767b[↩][↩][↩][↩]
- Scheie stripe in pigment dispersion syndrome. https://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/Scheie-stripe/index.htm#gsc.tab=0[↩]
- Goel M, Picciani RG, Lee RK, Bhattacharya SK. Aqueous humor dynamics: a review. Open Ophthalmol J. Sep 3 2010;4:52-9. doi:10.2174/1874364101004010052[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Toris CB, Koepsell SA, Yablonski ME, Camras CB. Aqueous humor dynamics in ocular hypertensive patients. J Glaucoma. 2002 Jun;11(3):253-8. doi: 10.1097/00061198-200206000-00015[↩][↩][↩][↩][↩]
- Macknight AD, McLaughlin CW, Peart D, Purves RD, Carré DA, Civan MM. Formation of the aqueous humor. Clin Exp Pharmacol Physiol. 2000 Jan-Feb;27(1-2):100-6. doi: 10.1046/j.1440-1681.2000.03208.x[↩]
- Ferreira SM, Lerner SF, Brunzini R, Evelson PA, Llesuy SF. Oxidative stress markers in aqueous humor of glaucoma patients. Am J Ophthalmol. 2004 Jan;137(1):62-9. doi: 10.1016/s0002-9394(03)00788-8[↩][↩]
- Kaeslin MA, Killer HE, Fuhrer CA, Zeleny N, Huber AR, Neutzner A. Changes to the Aqueous Humor Proteome during Glaucoma. PLoS One. 2016 Oct 27;11(10):e0165314. doi: 10.1371/journal.pone.0165314[↩][↩]
- Brubaker RF. The flow of aqueous humor in the human eye. Trans Am Ophthalmol Soc. 1982;80:391-474. https://pmc.ncbi.nlm.nih.gov/articles/instance/1312276/pdf/taos00019-0414.pdf[↩][↩][↩][↩][↩]
- R TCYMT. Aqueous humor dynamics. In: DC CNL, ed. Atlas of Glaucoma. Second edition ed. Informa HK; 2007:13 – 28:chap 3.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Kiel JW, Hollingsworth M, Rao R, Chen M, Reitsamer HA. Ciliary blood flow and aqueous humor production. Prog Retin Eye Res. Jan 2011;30(1):1-17. doi:10.1016/j.preteyeres.2010.08.001[↩][↩][↩][↩][↩]
- Macknight AD, McLaughlin CW, Peart D, Purves RD, Carre DA, Civan MM. Formation of the aqueous humor. Clin Exp Pharmacol Physiol. Jan-Feb 2000;27(1-2):100-6. doi:10.1046/j.1440-1681.2000.03208.x[↩]
- Johnson M, McLaren JW, Overby DR. Unconventional aqueous humor outflow: A review. Exp Eye Res. May 2017;158:94-111. doi:10.1016/j.exer.2016.01.017[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Roy Chowdhury U, Hann CR, Stamer WD, Fautsch MP. Aqueous humor outflow: dynamics and disease. Invest Ophthalmol Vis Sci. May 2015;56(5):2993-3003. doi:10.1167/iovs.15-16744[↩][↩][↩][↩]
- Fautsch MP, Johnson DH. Aqueous humor outflow: what do we know? Where will it lead us? Invest Ophthalmol Vis Sci. Oct 2006;47(10):4181-7. doi:10.1167/iovs.06-0830[↩][↩][↩]
- Trabecular Meshwork Research. https://ethier.gatech.edu/anterior-segmenttrabecular-meshwork-biomechanics[↩][↩]
- J. Buffault, A. Labbé, P. Hamard, F. Brignole-Baudouin, C. Baudouin. The trabecular meshwork: Structure, function and clinical implications. A review of the literature. Journal Français
d’Ophtalmologie, 2020, 43 (7), pp.e217-e230. https://hal.sorbonne-universite.fr/hal-02962228v1/document[↩] - Mahmoudinezhad G, Moghimi S, Proudfoot JA, Brye N, Nishida T, Yarmohammadi A, Kamalipour A, Zangwill LM, Weinreb RN. Effect of Testing Frequency on the Time to Detect Glaucoma Progression With Optical Coherence Tomography (OCT) and OCT Angiography. Am J Ophthalmol. 2023 Jan;245:184-192. doi: 10.1016/j.ajo.2022.08.030[↩]
- What Is Fluorescein Angiography? https://www.aao.org/eye-health/treatments/what-is-fluorescein-angiography[↩]
- Medical Management of Glaucoma. https://morancore.utah.edu/section-10-glaucoma/medical-management-of-glaucoma[↩]
- Laemmer R, Mardin CY, Juenemann AG. Visualization of changes of the iris configuration after peripheral laser iridotomy in primary melanin dispersion syndrome using optical coherence tomography. J Glaucoma. 2008 Oct-Nov;17(7):569-70. doi: 10.1097/IJG.0b013e318168f02c[↩]
- Carassa RG, Bettin P, Fiori M, Brancato R. Nd:YAG laser iridotomy in pigment dispersion syndrome: an ultrasound biomicroscopic study. Br J Ophthalmol. 1998 Feb;82(2):150-3. doi: 10.1136/bjo.82.2.150[↩]
- Breingan PJ, Esaki K, Ishikawa H, Liebmann JM, Greenfield DS, Ritch R. Iridolenticular contact decreases following laser iridotomy for pigment dispersion syndrome. Arch Ophthalmol. 1999 Mar;117(3):325-8. doi: 10.1001/archopht.117.3.325[↩]
- Jampel HD. Lack of effect of peripheral laser iridotomy in pigment dispersion syndrome. Arch Ophthalmol. 1993 Dec;111(12):1606. doi: 10.1001/archopht.1993.01090120028009[↩]
- Haynes WL, Johnson AT, Alward WL. Inhibition of exercise-induced pigment dispersion in a patient with the pigmentary dispersion syndrome. Am J Ophthalmol. 1990 May 15;109(5):601-2. doi: 10.1016/s0002-9394(14)70696-8[↩]
- Haynes WL, Alward WL, Tello C, Liebmann JM, Ritch R. Incomplete elimination of exercise-induced pigment dispersion by laser iridotomy in pigment dispersion syndrome. Ophthalmic Surg Lasers. 1995 Sep-Oct;26(5):484-6.[↩]
- Gandolfi SA, Vecchi M. Effect of a YAG laser iridotomy on intraocular pressure in pigment dispersion syndrome. Ophthalmology. 1996 Oct;103(10):1693-5. doi: 10.1016/s0161-6420(96)30445-4[↩]
- Reistad CE, Shields MB, Campbell DG, Ritch R, Wang JC, Wand M; American Glaucoma Society Pigmentary Glaucoma Iridotomy Study Group. The influence of peripheral iridotomy on the intraocular pressure course in patients with pigmentary glaucoma. J Glaucoma. 2005 Aug;14(4):255-9. doi: 10.1097/01.ijg.0000169383.05605.4b[↩]
- Michelessi M, Lindsley K. Peripheral iridotomy for pigmentary glaucoma. Cochrane Database Syst Rev. 2016 Feb 12;2(2):CD005655. doi: 10.1002/14651858.CD005655.pub2[↩]
- Birt CM. Intraocular pressure spike after YAG iridotomy in patients with pigment dispersion. Can J Ophthalmol. 2004 Apr;39(3):234-9. doi: 10.1016/s0008-4182(04)80119-4[↩]
- European Glaucoma Society Terminology and Guidelines for Glaucoma, 4th Edition – Chapter 2: Classification and terminologySupported by the EGS Foundation: Part 1: Foreword; Introduction; Glossary; Chapter 2 Classification and Terminology. Br J Ophthalmol. 2017 May;101(5):73-127. doi: 10.1136/bjophthalmol-2016-EGSguideline.002[↩]
- Richter CU, Richardson TM, Grant WM. Pigmentary dispersion syndrome and pigmentary glaucoma. A prospective study of the natural history. Arch Ophthalmol. 1986 Feb;104(2):211-5. doi: 10.1001/archopht.1986.01050140065021[↩]
- Speakman JS. Pigmentary dispersion. Br J Ophthalmol. 1981 Apr;65(4):249-51. doi: 10.1136/bjo.65.4.249[↩]
- Ritch R. Nonprogressive low-tension glaucoma with pigmentary dispersion. Am J Ophthalmol. 1982 Aug;94(2):190-6. doi: 10.1016/0002-9394(82)90074-5[↩]




{kind=link}