
Contents
What is pressure urticaria
Pressure urticaria also called delayed pressure urticaria or angioedema, is a form of chronic inducible urticaria (also known as hives, is a common skin condition that causes itchy, raised red or pink bumps or blotches on the skin) characterized by the appearance of weals (a red swollen mark left on flesh) and/or angioedema (a condition that causes swelling under the skin or in mucous membranes when small blood vessels leak fluid into the surrounding tissues) after pressure to the skin 1, 2, 3, 4. In delayed pressure urticaria there is red swelling on skin at a site where sustained pressure is applied after a delay of 30 minute to 12 hours 5, 6. This swelling is accompanied by urticaria (hives, a common skin condition that causes itchy, raised red or pink bumps or blotches on the skin). Pain or blisters are occasionally seen 6.
Delayed pressure urticaria is usually found in patients with known history of urticaria or angioedema 5. Pressure urticaria symptoms may occur immediately at sites of sustained pressure such as over areas of tight clothing, exercise bands, or on the buttocks after sitting on hard surfaces for prolonged periods, carrying heavy groceries and even after compression of the face against the pillow while sleeping 7. Delayed pressure urticaria are commonly seen after a delay of 4–6 hours and can last between 12 and 72 hours 8.
Pressure urticaria can be induced by a variety of stimuli including standing, walking, wearing tight clothes or sitting on a hard surface. Pressure urticaria can occasionally be aggravated by heat, aspirin or menstruation. Pressure urticaria diagnosis is usually missed unless direct questions about development of weals at an area of sustained pressure are asked to the patient.
Pressure urticaria is uncommon but probably not rare. It is a chronic disease with a mean duration of 9 years. The peak age of onset is in the 20’s and 30’s.
The cause of delayed pressure urticaria is not clear and is theorized by various authors to be type 3 hypersensitivity reaction, response to a food allergen, mast cell mediated or leukotriene mediated 5.
Pressure urticaria diagnosis is made clinically by reproducing the lesion by application of pressure. Although there is no standard method of pressure testing the area is usually inspected for lesions 6 hours after performing the test 6, 9.
Pressure urticaria treatment with antihistamines alone is usually not sufficient and requires additional therapy with oral steroids 10. Other agents reported to be useful in treatment of delayed pressure urticaria include non-steroidal anti-inflammatory drugs (NSAIDs), colchicine, dapsone, sulfasalazine, intravenous immunoglobulins (IVIG) and omalizumab 11, 12, 6, 9, 13, 10, 14 .
Figure 1. Delayed pressure urticaria

Footnote: Delayed pressure urticaria on left arm at the site of blood pressure monitoring cuff application with erythema and blisters
[Source 5 ]Figure 2. Delayed pressure urticaria

Footnote: Delayed pressure urticaria with erythema and blisters linearly along the 10th rib due to prolonged pressure because of inadequate padding while patient positioning in operation theater
[Source 5 ]Pressure urticaria causes
The cause of pressure urticaria is unclear but it is likely to be an autoimmune disease. Cells called mast cells are an important part in the process. Mast cells are tissue cells that contain chemicals, including histamine, which provoke wealing. The pathogenesis of pressure urticaria is believed to involve mast cell degranulation triggered by pathogenic autoreactive immunoglobulin G (IgG) and/or immunoglobulin E (IgE) antibodies, complex interplay of mast cells and other skin-resident and infiltrating cells (e.g., T and B lymphocytes, monocytes, eosinophils, basophils, and neutrophils), as well as the activation of coagulation and complement systems 15, 16, 17, 18.
Direct evidence of histamine release in delayed pressure urticaria comes from 3 studies. Two of them measured histamine release in skin lesions of delayed pressure urticaria patients. Kaplan et al 19 assessed suction blister fluid obtained at 2-hour intervals from skin sites exposed to pressure and found histamine levels to be increased between 4-10 hours, with peak levels of approximately 30 ng/ml at 6-8 hours. Czarnetzki et al. 20 reported that mean histamine levels were elevated in wheals induced by pressure. They also reported indirect evidence that peripheral blood leukocytes had significantly increased intracellular histamine levels and increased histamine releasability 20. Mijailović et al. 21 reported that pressure challenge on a patient’s forearm caused increased histamine levels in blood collected from the draining cubital vein 14 hours later as compared with the contralateral cubital vein and to baseline. Of note, 18 hours after challenge the patient developed systemic anaphylaxis and received adrenaline 21.
For indirect evidence, a systematic review of treatment of delayed pressure urticaria showed that second-generation H1 antihistamines were effective in 3 randomized controlled trials 22. Combining a second-generation H1 antihistamine with montelukast (2 randomized controlled trials) or theophylline (1 non-randomized controlled trial) was more effective than the second-generation H1 antihistamine alone 22.
Pressure urticaria symptoms
The weal in pressure urticaria consists of redness and swelling of the skin and subcutaneous tissues 3. Lesions may last for 8–72 hours 3.
- The hands, feet, trunk, buttocks, legs and face are most commonly affected.
- Weals may be accompanied by fever, malaise, fatigue, and occasionally chills, headache and general joint aches.
- Affected areas may be resistant to the development of new lesions for 1-2 days.
- Up to 60% of patients with pressure urticaria also have chronic urticaria, immediate and/or delayed dermographism, and/or angioedema.
Pressure urticaria has a significant adverse impact on the quality of life of patients, with important limitations in everyday activities such as prolonged walking or standing. It can be disabling in patients who perform manual labor 3.
Pressure urticaria diagnosis
The diagnosis of delayed pressure urticaria is made clinically 3. It can be confirmed if a delayed weal occurs after a standardized pressure stimulus. For the diagnosis of delayed pressure urticaria different weights are applied to the skin, which exert a defined pressure on the skin surface 23. Different test methods, using various weights, application times or test areas, e.g., the back, thighs or forearms are described in the literature 23. This is often painful. In immediate pressure urticaria, a weal will appear within minutes of the stimulus.
A blood count may show an increased white cell count and ESR, but it is often normal.
A skin biopsy of delayed pressure urticaria shows inflammatory infiltrates which vary with the age of the weal. No vasculitis is found.
Figure 3. Delayed pressure urticaria pressure testing
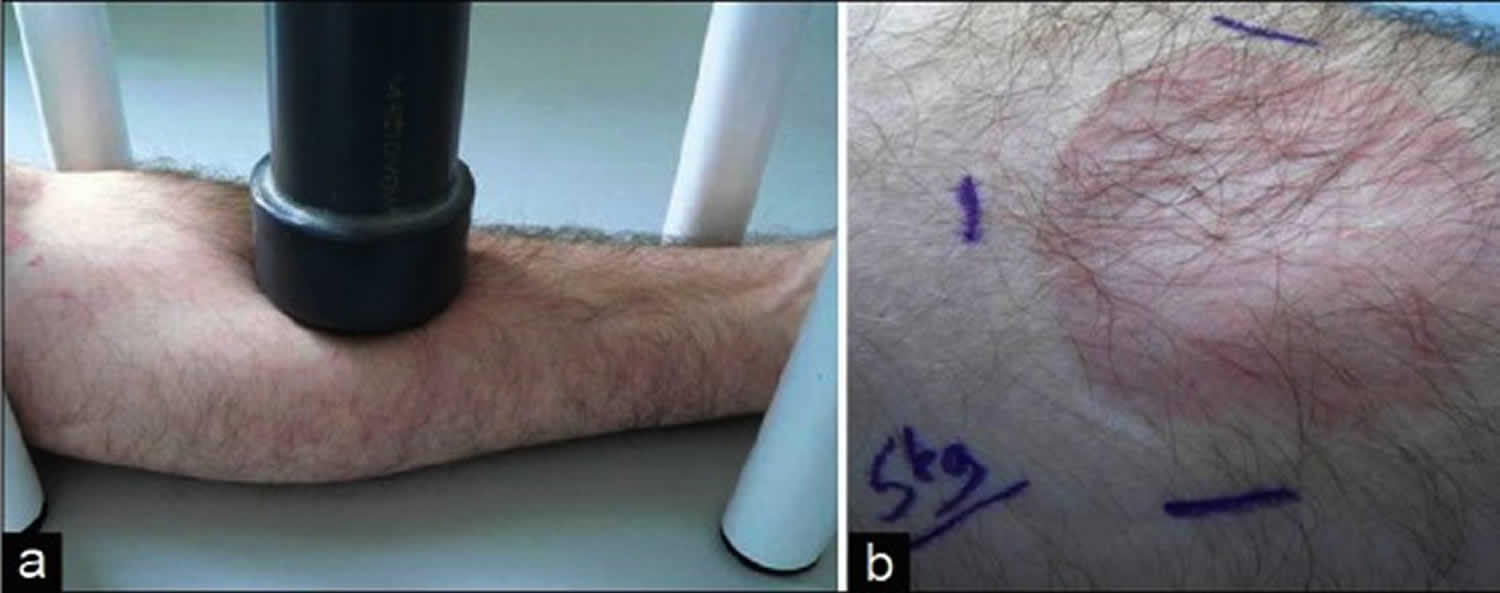
Footnotes: (a) Swelling after application of 14.6 kPa pressure with a 5 kg heavy metal rod for 15 minutes (b). The test reaction is rated as positive, if a delayed red palpable swelling occurs. Burning or painful sensations can occur simultaneously. False negative test results might be related to the refractory period after previous pressure application or to different sensitivities in different parts of the body. In case of a negative test result, with an indicative history, the test should be repeated after 48 h. A positive test result should be followed by threshold testing in order to evaluate the disease activity and the efficacy of initiated therapies (initial weight 0.5 kg, increments: 0.5 kg) 24, 25.
Pressure urticaria treatment
The results of treatment of pressure urticaria are relatively disappointing 3.
- Reduce pressure stimuli as far as practicable.
- Antihistamines help control associated chronic urticaria but rarely reduce pressure urticaria.
- The ultrapotent topical corticosteroid clobetasol propionate may reduce inflammation. Skin thinning can result from regular use. Milder topical steroids are not of benefit.
- Systemic corticosteroids produce variable responses and long-term use is associated with many potential adverse side effects.
- Other possible therapies include nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, dapsone, sulfasalazine and montelukast.
- Ciclosporin, methotrexate and intravenous gamma globulin have been used in a small number of patients with severe and refractory disease.
- Tumor necrosis factor-alpha inhibitors have been reported of benefit in a few patients.
- Barlow R.J., Warburton F., Watson K., Black A.K., Greaves M.W. Diagnosis and incidence of delayed pressure urticaria in patients with chronic urticaria. J Am Acad Dermatol. 1993;29(6):954–958. doi: 10.1016/0190-9622(93)70273-v[↩]
- Kobza-Black A. Delayed pressure urticaria. J Investig Dermatol Symp Proc. 2001 Nov;6(2):148-9. doi: 10.1046/j.0022-202x.2001.00030.x[↩]
- Delayed pressure urticaria. https://dermnetnz.org/topics/pressure-urticaria[↩][↩][↩][↩][↩][↩]
- Lawlor F, Black AK. Delayed pressure urticaria. Immunol Allergy Clin North Am. 2004 May;24(2):247-58, vi-vii. doi: 10.1016/j.iac.2004.01.006[↩]
- Pandey S, Sinha RJ, Sharma D, Singh V. Delayed pressure urticaria due to non-invasive blood pressure monitoring in a previously non-atopic man. BMJ Case Rep. 2018 Sep 15;2018:bcr2018227267. doi: 10.1136/bcr-2018-227267[↩][↩][↩][↩][↩]
- Kobza-Black A. Delayed pressure urticaria. J Investig Dermatol Symp Proc 2001;6:148–9. 10.1046/j.0022-202x.2001.00030.x[↩][↩][↩][↩]
- Greaves M. Chronic urticaria. J Allergy Clin Immunol. 2000 Apr;105(4):664-72. doi: 10.1067/mai.2000.105706[↩]
- Kulthanan K, et al. Delayed Pressure Urticaria A Systematic Review of Treatment Options. J Allergy Clin Immunol Pract. 2020;8(6):2035-2049e5. 10.1016/j.jaip.2020.03.004[↩]
- Lawlor F, Black AK. Delayed pressure urticaria. Immunol Allergy Clin North Am 2004;24:247–58. 10.1016/j.iac.2004.01.006[↩][↩]
- Kulthanan K, Ungprasert P, Tuchinda P, Chularojanamontri L, Charoenpipatsin N, Maurer M. Delayed pressure urticaria: A systematic review of treatment options. J Allergy Clin Immunol Pract (2020) 8(6):2035–49.e5. doi: 10.1016/j.jaip.2020.03.004[↩][↩]
- Quintero O.P., Arrondo A.P., Veleiro B. Rapid response to omalizumab in 3 cases of delayed pressure urticaria. J All Clin Immunol. 2017;5(1):179–180. doi: 10.1016/j.jaip.2016.07.016[↩]
- Soliman YS, Lim HW, Kerr HA. Recalcitrant, delayed pressure urticaria treated with long-term intravenous immunoglobulin. JAAD Case Rep. 2020 Feb 18;6(3):176-177. doi: 10.1016/j.jdcr.2019.01.033[↩]
- Kasperska-Zajac A, Jarząb J, Żerdzińska A, Bąk K, Grzanka A. Effective treatment of different phenotypes of chronic urticaria with omalizumab: Case reports and review of literature. Int J Immunopathol Pharmacol. 2016 Jun;29(2):320-8. doi: 10.1177/0394632015623795[↩]
- Lawlor F., Black A.K. Delayed pressure urticaria. Immunol All Clin North Am. 2004;24(2):247–258. doi: 10.1016/j.iac.2004.01.006[↩]
- Kaplan A, Lebwohl M, Gimenez-Arnau AM, Hide M, Armstrong AW, Maurer M. Chronic spontaneous urticaria: focus on pathophysiology to unlock treatment advances. Allergy. (2023) 78:389–401. 10.1111/all.15603[↩]
- Gimenez-Arnau AM, DeMontojoye L, Asero R, Cugno M, Kulthanan K, Yanase Y, et al. The pathogenesis of chronic spontaneous urticaria: the role of infiltrating cells. J Allergy Clin Immunol Pract. (2021) 9:2195–208. 10.1016/j.jaip.2021.03.033[↩]
- Koren A, Dejanović L, Rijavec M, Kopač P, Bizjak M, Zidarn M, et al. Autoimmune mast cell activation test as a diagnostic tool in chronic spontaneous urticaria. Int J Mol Sci. (2024) 25:9281. 10.3390/ijms25179281[↩]
- Rijavec M, Kosnik M, Koren A, Kopac P, Selb J, Vantur R, et al. A very low number of circulating basophils is predictive of a poor response to omalizumab in chronic spontaneous urticaria. Allergy. (2021) 76:1254–7. 10.1111/all.14577[↩]
- Kaplan AP, Horáková Z, Katz SI. Assessment of tissue fluid histamine levels in patients with urticaria. J Allergy Clin Immunol (1978) 61(6):350–4. doi: 10.1016/0091-6749(78)90113-6[↩]
- Czarnetzki BM, Meentken J, Rosenbach T, Pokropp A. Clinical, pharmacological and immunological aspects of delayed pressure urticaria. Br J Dermatol (1984) 111(3):315–23. doi: 10.1111/j.1365-2133.1984.tb04729.x[↩][↩]
- Mijailović BB, Karadaglić DM, Ninković MP, Mladenović TM, Zecević RD, Pavlović MD. Bullous delayed pressure urticaria; pressure testing may produce a systemic reaction. Br J Dermatol (1997) 136(3):434–6. doi: 10.1111/j.1365-2133.1997.tb14962.x[↩][↩]
- Kulthanan K, Ungprasert P, Tuchinda P, Chularojanamontri L, Charoenpipatsin N, Maurer M. Delayed Pressure Urticaria: A Systematic Review of Treatment Options. J Allergy Clin Immunol Pract. 2020 Jun;8(6):2035-2049.e5. doi: 10.1016/j.jaip.2020.03.004[↩][↩]
- Schoepke N, Doumoulakis G, Maurer M. Diagnosis of urticaria. Indian J Dermatol. 2013 May;58(3):211-8. doi: 10.4103/0019-5154[↩][↩]
- Siebenhaar F, Weller K, Mlynek A, Magerl M, Altrichter S, Vieira Dos Santos R, et al. Acquired cold urticaria: Clinical picture and update on diagnosis and treatment. Clin Exp Dermatol. 2007;32:241–5. doi: 10.1111/j.1365-2230.2007.02376.x[↩]
- Fleischer M, Grabbe J. Physical urticaria. Hautarzt. 2004;55:344–9. doi: 10.1007/s00105-004-0691-x[↩]
- Schoepke N, Doumoulakis G, Maurer M. Diagnosis of urticaria. Indian J Dermatol. 2013 May;58(3):211-8. doi: 10.4103/0019-5154.110831[↩]





{kind=link}