
Contents
What is pudendal neuralgia
Pudendal neuralgia is a type of long-term (chronic) pelvic pain that originates from damage or irritation of the pudendal nerve. Pudendal neuralgia occurs when the pudendal nerve is injured, irritated, inflamed or compressed 1. Pudendal neuralgia is pain caused by the pudendal nerve that supplies the skin between your pubic bone and your tail bone (Figures 1 to 3). The pudendal nerve carries the sensations of touch and pain from the skin between the anus and the clitoris (females)/ penis (males), as well as the sphincters (muscles that keep the openings of the bladder and bowel closed). Sometimes pudendal neuralgia is referred to as cyclist’s syndrome, pudendal canal syndrome, or Alcock’s syndrome. Pudendal neuralgia can occur in men and women although about 2/3 of patients are female. Pudendal neuralgia is defined by burning vaginal or vulval pain (anywhere between the anus and the clitoris) associated with tenderness over the course of the pudendal nerve 2. Pudendal neuralgia is characterized by pelvic pain, including bowel, bladder regional pain or discomfort, sexual dysfunction, severe burning sensations and needle-like pain, which are aggravated when seated and relieved after standing.
According to the International Association of Pudendal Neuropathy, the incidence of pudendal neuralgia in the general population is about 1/100,000 3. Pudendal neuralgia may be associated with childbirth, pelvic surgery, strenuous exercise, abnormalities of the sacroiliac joint, and also, it is connected to age-related changes 4.
Pudendal neuralgia symptoms include burning pain (often unilateral), tingling, or numbness in any of the following areas: buttocks, genitals, or perineum (area between the buttocks and genitals). Pudendal neuralgia symptoms are typically present when a person is sitting but often go away when the person is standing or lying down. The pain tends to increase as the day progresses. Additional symptoms include pain during sex and needing to urinate frequently and/or urgently.
The pudendal nerve is one of the main nerves in the pelvis, supplying areas such as the:
- lower buttocks
- area between the buttocks and genitals (perineum)
- area around the back passage (rectum)
- vulva, labia, and clitoris in women
- scrotum and penis in men
Damage to the pudendal nerve can result from surgical procedures, childbirth, trauma, spasms of the pelvic floor muscles, or tumors. Pudendal neuralgia may also result from certain infections (such as herpes simplex infections) or certain activities (such as cycling and squatting exercises).
There are no imaging studies that diagnose pudendal neuralgia; however, MRI and CT may help to exclude other causes of the pain.
Pudendal neuralgia can be very uncomfortable and distressing, but help is available and there are several treatments that can be tried. Currently, the clinical treatments of pudendal neuralgia include drug therapy, pudendal nerve block, pudendal nerve decompression, nervous regulation by the implanted pulse generator, radiofrequency ablation, spinal cord electrical stimulation and so on. The ideal clinical treatment for pudendal neuralgia has not yet been determined. Physical therapy is often the first line of treatment 5. About 30% of patients are refractory to pain management and surgical procedure. In a published preliminary study 6 involving 27 patients with refractory pudendal neuralgia, researchers demonstrated that 74% of patients implanted with stimulation electrodes at the conus medullaris responded to stimulation.
Pudendal nerve anatomy
The pudendal nerve originates in the S2-S4 sacral foramina. The pudendal nerve is the major nerve of the perineum innervates skin and skeletal muscles of the perineum, including the external anal and external urethral sphincters. The pudendal nerve directly associated with the ischial spine of the pelvis. The pudendal nerve leaves the pelvic cavity through the greater sciatic foramen and then immediately enters the perineum inferiorly to the pelvic floor by passing around the ischial spine and through the lesser sciatic foramen (Figures 1 to 3). The ischial spine can be palpated transvaginally in women and is the landmark for administering a pudendal nerve block.
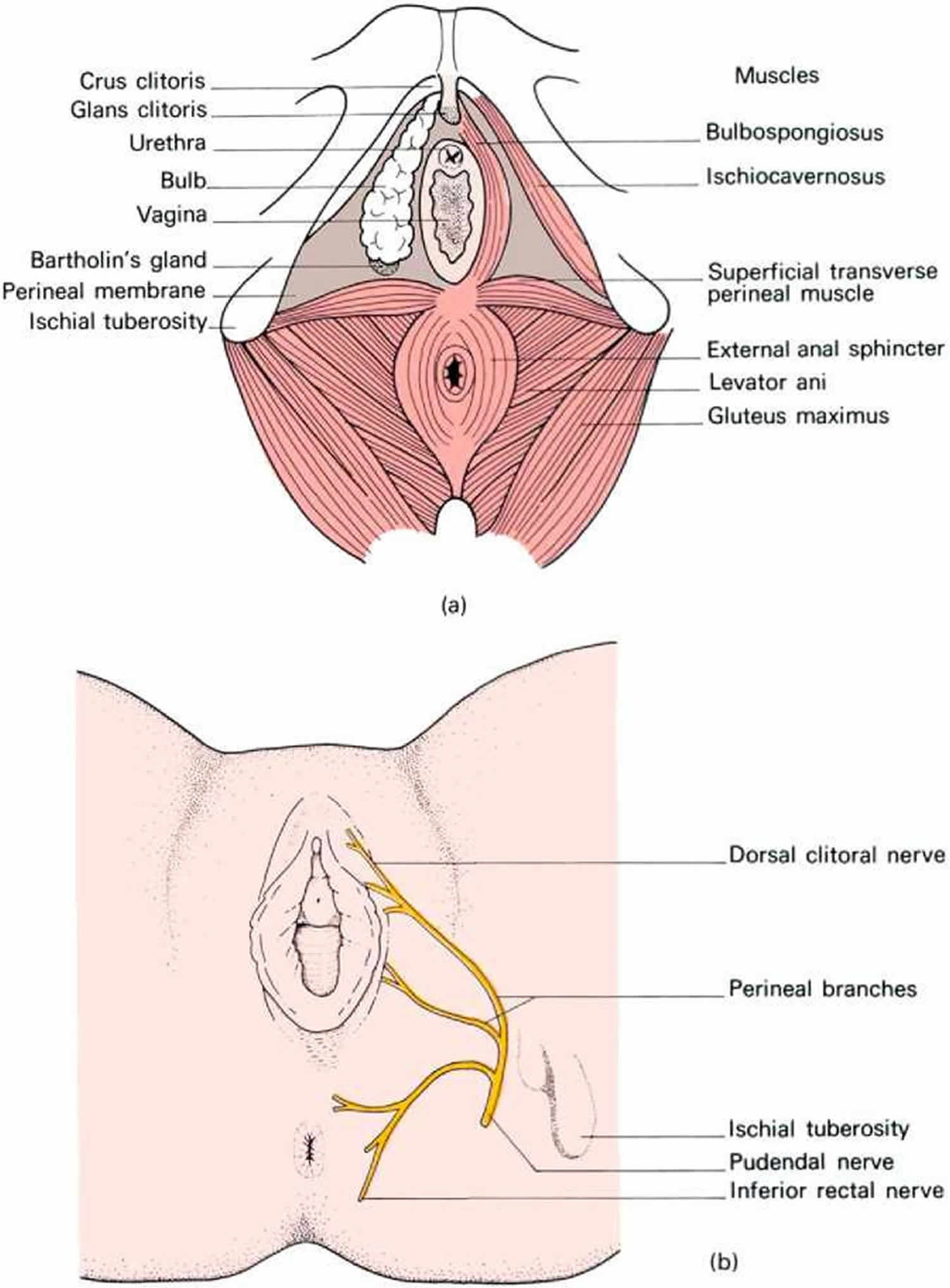
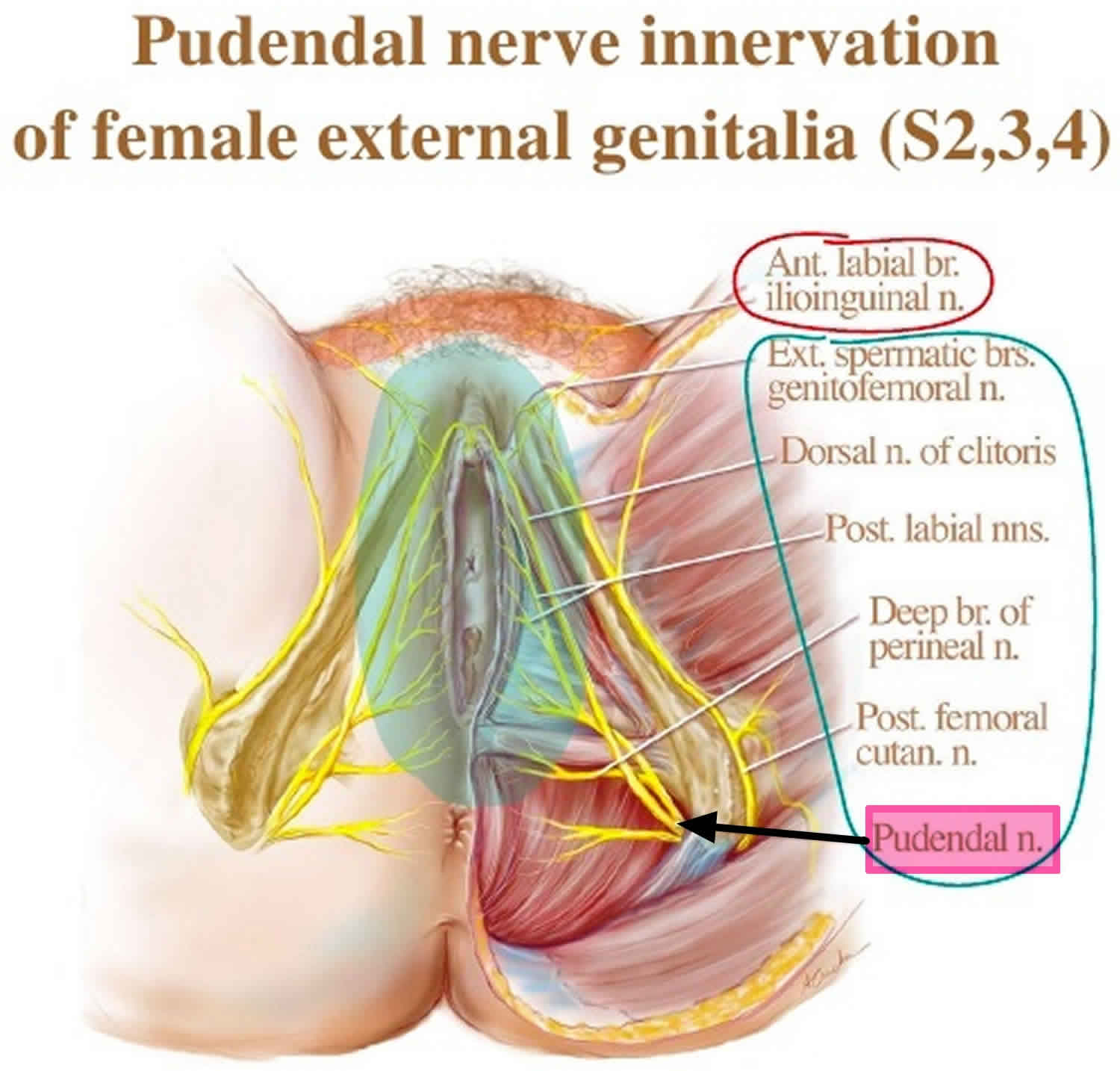
In women, the pudendal nerve divides into three branches – the inferior rectal nerve, the perineal nerve, and the dorsal clitoral nerve. The pudendal nerve thus innervates the clitoris, vulva, labia, vagina, perineum, and rectum. Pain can be present along the entire nerve, or localized to the sites of nerve innervation. Symptoms can be unilateral or bilateral, although with bilateral pain there usually is a more affected side. In most cases, patients will describe neuropathic pain – a burning, tingling, or numbing pain – that is worse with sitting, and less severe or absent when standing or lying down.
Initially, pain may be present only with sitting, but with time pain becomes more constant and severely aggravated by sitting. Many of my patients cannot tolerate sitting at all. Interestingly, patients usually report less pain when sitting on a toilet seat, a phenomenon that we believe is associated with pressure being applied to the ischial tuberosities rather than to the pelvic floor muscles. Pain usually gets progressively worse through the day.
Patients often will report the sensation of having a foreign body, frequently described as a golf ball or tennis ball, in the vagina, perineum, or rectum.
Pain with urination and/or bowel movements, and problems with frequency and urgency, also are often reported, as is pain with intercourse. Dyspareunia may be associated with penetration, sexual arousal, or orgasm, or any combination. Some patients report feeling persistent sexual arousal.
Occasionally, patients report having pain in regions outside the areas of innervation for the pudendal nerve, such as the lower back or posterior thigh. The presence of sciatica, or pain that radiates down the leg, for instance, should not rule out consideration of pudendal neuralgia.
Just as worsening pain with sitting is a defining characteristic, almost all patients also have an acute onset of discomfort or pain; their pain can be traced to some type of traumatic event.
Figure 1. Pudendal nerve origin

Figure 2. Pudendal nerve male
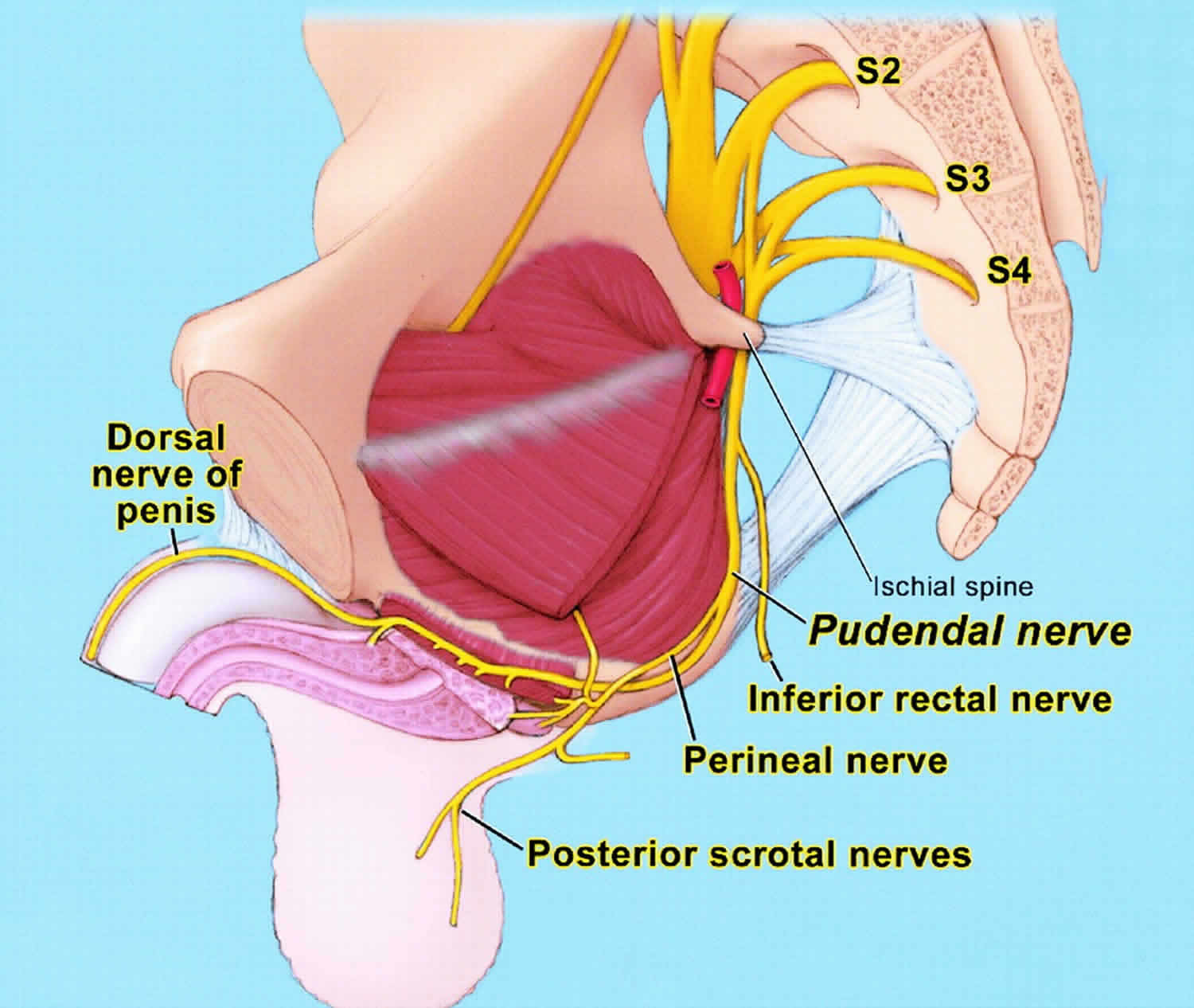
Figure 3. Pudendal nerve female
Is there any evidence that shows Botox is an effective treatment for pudendal neuralgia?
Unfortunately, there is no identifiable evidence that shows Botox is an effective treatment for pudendal neuralgia. There is currently one research study 6 which is investigating Botox as a possible treatment for this condition.
Does pudendal neuralgia go away?
Unfortunately there is no “cure” for pudendal neuralgia. Rather, pudendal neuralgia, as any chronic pain condition, is ‘managed’ through a variety of measures involving everyday life, from work to leisure activity adjustments, as well as medical interventions. The crucial element in the process is that you, the patient, are the driver of this management plan.
Lifestyle changes
Avoid or minimize specific physical activities that are known to irritate the pudendal nerve. Spending hours on a bicycle is an activity to avoid, as is horse riding. Other activities that may contribute to pudendal neuralgia are trampoline jumping, bench pressing and excessive ‘core muscle’ exercises.
Manage your sitting: the aim is to avoid pressure on the perineum, which is the area inside the ‘sit bones’, as this could lead to compression of the nerve. Coccyx-cut-out memory foam cushions are available commercially. You can increase the size of the cut-out to accommodate your particular need.
When you sit, do not take any weight on the perineum, all the weight is on your bottom and ‘sit’ bones. Decrease your sitting by standing at your desk for part of the day. You may need to adjust the height of your desk to allow this.
Bowel and bladder management strategies
To minimize constipation and straining, increase your intake of foods high in fiber, such as fresh fruit, vegetables, bran and wholemeal breads, and drink plenty of water. Place your feet on a stool when sitting on the toilet. This should make bowel movements easier and less painful. It is advisable to avoid straining when emptying your bladder or bowels, as this could possibly stretch the nerve.
Physical therapy
Physiotherapy treatments aim to relax and/or stretch the often over-contracted pelvic floor muscles and thus decrease the pressure on the pudendal nerve.
TENS (Trans-epithelial Nerve Stimulation)
TENS (Trans-epithelial Nerve Stimulation), the so-called ‘tingly machine’ may also help relieve pain. It is important to ask the physiotherapist for guidance in correctly placing the electrodes, which are taped to the bare skin.
Medication
Medical management of pudendal neuralgia involves the same medications as for any other chronic pain condition. In addition, direct application of creams and ointments provide an alternative with fewer side effects than oral medications. The most commonly prescribed topical treatment involves the drug amitriptyline. This is a low-dose antidepressant, although you do not have to be depressed to gain benefit from the use of this drug.
Acupuncture
When the pain is acute, for instance within a few weeks or months after childbirth, acupuncture can be a great alternative to traditional medical management.
Pudendal neuralgia causes
Pudendal neuralgia can occur if the pudendal nerve is damaged, irritated or squashed (compressed).
Possible causes include:
- Compression of the pudendal nerve by nearby muscles or tissue – sometimes called pudendal nerve entrapment or Alcock canal syndrome
- Prolonged sitting, cycling, horse riding or constipation (usually for months or years) – this can cause repeated minor damage to the pelvic area
- Previous gynecological or colo-rectal surgery to the pelvic area
- A break in one of the bones in the pelvis
- Childbirth trauma or damage to the pudendal nerve during childbirth – this may improve after a few months
- A non-cancerous or cancerous growth (tumor) pressing on the pudendal nerve
- Excessive physical exercise
- Past pelvic or perineal trauma
- Injury
- Straining
- Musculoskeletal issues
- Posture
- Stress
In some cases, a specific cause isn’t identified.
If the pelvic floor is over-stretched, acutely (e.g. prolonged or difficult childbirth) or chronically (e.g. chronic straining during defecation caused by constipation), the pudendal nerve is vulnerable to stretch-induced neuropathy. Pudendal nerve entrapment, also known as Alcock canal syndrome, is very rare and is associated with professional cycling. Systemic diseases such as diabetes and multiple sclerosis can damage the pudendal nerve via demyelination or other mechanisms.
Pudendal neuralgia symptoms
The main symptom of pudendal neuralgia is pelvic pain. Any of the areas supplied by the pudendal nerve can be affected.
The most common complaint of pudendal neuralgia is pain with sitting, which gets worse as the day goes on. However, as the pudendal nerve is also involved with bladder and bowel function, other problems, such as bladder frequency, feeling of a bladder infection, pain with intercourse and the sensation of an urgent need to open the bowels, can also occur.
Typically, the pudendal neuralgia pain resolves during the night or when lying down. Pudendal neuralgia can be related to intense physical exercise involving the pelvic floor and neighbouring muscles. The exercises that are most commonly associated are: ‘Kegel’ exercises (exercises to strengthen the pelvic floor muscles), cycling and weight lifting/ bench pressing.
The most common association however is with childbirth. During vaginal delivery, the pudendal nerve is slightly stretched and may therefore malfunction and cause symptoms. This resolves spontaneously in most cases within a few weeks. Some women, however, will continue to suffer pain for longer periods of time, or the pudendal neuralgia pain may come back months or years after the delivery.
Some types of surgery can lead to persistent postoperative pain. This surgery might have been a simple cut for the removal of a cyst or following childbirth (episiotomy) or a more complicated procedure, such as for correction of prolapse, for example. Doctors do not have any way of predicting who will develop chronic pudendal neuralgia pain after surgery. Pain after surgery is not necessarily the result of incorrectly performed surgery.
Pudendal neuralgia pain may:
- feel like a burning, crushing, shooting or prickling sensation
- develop gradually or suddenly
- be constant – but worse at some times and better at others
- be worse when sitting down and improve when standing or lying down
Other pudendal neuralgia symptoms can include:
- numbness and pins and needles in the pelvic area
- increased sensitivity to pain – you may find just a light touch or wearing clothes uncomfortable
- feeling as though there’s swelling or an object in your perineum – often described as feeling like a golf or tennis ball
- needing to go the toilet frequently or suddenly
- pain during sex, difficulty reaching orgasm, and erectile dysfunction in men
See your doctor if you have persistent pelvic pain. Don’t delay seeking advice if the pain is causing problems. Pudendal neuralgia can continue to get worse if left untreated, and early treatment may be more effective.
The stress of living with the condition can also have a significant impact on your physical and mental health if it’s not treated.
Pudendal neuralgia diagnosis
Your doctor will ask about your symptoms and may carry out an examination of the area to check for any obvious causes of your pain.
If they think you could have pudendal neuralgia, or they’re not sure what’s causing your pain, they may refer you to a specialist for further tests.
These tests may include:
- a vaginal or rectal exam – to see if the pain occurs when your doctor applies pressure to the pudendal nerve with their finger
- a magnetic resonance imaging (MRI) scan – to check for problems such as entrapment (compression) of the pudendal nerve and rule out other possible causes of your pain
- nerve studies – a small device inserted into your rectum is used to stimulate nearby nerves with mild electrical impulses to check how well the nerves are working
- nerve block injections – painkilling medication is injected around the pudendal nerve to see if your pain improves.
Pudendal nerve block
Local anesthetic is injected into the canal through which the nerve travels. The perineal skin should go numb and, while you are numb, we would expect your pain to be eliminated or significantly decreased.
Other tests may be requested to rule out other problems. These tests include special scans (ultrasound or MRI) of the joints, ligaments and muscles of the pelvis.
Pudendal neuralgia treatment
Many physicians suggest using a step-ladder approach to therapy for individuals with pudendal neuralgia. Physical therapy with professionals who specialize in pelvic floor therapy is often the first line of treatment. Electrical stimulation and biofeedback have been used to assist therapists with treatment. Patients are also given exercises and lifestyle modifications to use at home. For muscle spasms that are not responsive to physical therapy, botulinum toxin has been used in some cases. Medications such as gabapentin, pregabalin, cyclobenzaprine, and tricyclic antidepressants have also been used in the treatment of patients with pudendal neuralgia 7. In some cases, treatment may include nerve blocks, electrical stimulation of the lower end of the spinal cord, or surgery to remove tissues that might be pressing on the pudendal nerve 8.
Treatments for pudendal neuralgia include:
- Avoiding things that make the pain worse, such as cycling, constipation or prolonged sitting – it may help to use a special cushion with a gap down the middle when sitting and try constipation treatments
- Medications to alter the pain such as anticonvulsants – these will normally be special medications for nerve pain, rather than ordinary painkillers like paracetamol
- Physical therapy – a physiotherapist can teach you exercises to relax your pelvic floor muscles (muscles used to control urination) and other muscles that can irritate the pudendal nerve
- Painkilling injections – injections of local anesthetic and steroid medication may relieve the pain for a few months at a time. This study 9 demonstrates that corticosteroid infiltration is no more effective than the use of local anaesthetics alone, regardless of the method used to assess pain. The use of corticosteroids is therefore unnecessary. The use of a large volume of normal saline also did not improve the result.
- Decompression surgery – if something is pressing on the pudendal nerve, such as a piece of tissue, surgery to reposition it away from the pudendal nerve may help improve your pain
- Nerve stimulation – a special device is surgically implanted under the skin to deliver mild electrical impulses to the nerve and interrupt pain signals sent to the brain
You may be referred to a specialist pain management team or pain management programme for support and advice about treatment.
Relaxation techniques for stress relief
Relaxation is a state where you feel calm and can manage your symptoms of stress or anxiety. Relaxation has many mental and physical health benefits, and relaxation techniques can be practised almost anywhere.
Relaxation can help you calm down and take a step back from a stressful situation.
Relaxation reduces stress and the symptoms of mental health conditions like depression,anxiety and schizophrenia. Relaxation also has other related health benefits, including:
- lowering your heart rate, blood pressure and breathing rate
- reducing muscle tension and chronic pain
- improving concentration and mood
- reducing fatigue
- reducing anger and frustration
- boosting confidence to handle problems.
Although the cause of the anxiety won’t disappear, you will probably feel more able to deal with it once you’ve released the tension in your body and cleared your thoughts.
Relaxation techniques focus on muscle relaxation or breathing. An example is progressive muscle relaxation, where you tense then relax different muscle groups.
Other techniques include:
- visualization, where you create a mental image of a calming place for you
- deep breathing, where you refocus your attention on your breathing
- hypnosis
- meditation
- mindfulness
- exercise.
Many relaxation techniques combine breathing more deeply with relaxing the muscles.
Don’t worry if you find it difficult to relax at first. It’s a skill that needs to be learned and it will come with practice.
Yoga and tai chi are both good forms of exercise that can help to improve breathing and relaxation.
Find a relaxation technique that works for you and make it part of your daily routine, even if it’s just for 5 or 10 minutes a day.
If you’re interested in mindfulness, you may want to use mindfulness coloring books to help you focus on the present moment and take your mind off other things. This includes an aspect of art therapy, another relaxation technique.
Keeping a healthy work life balance helps with relaxation and managing stress.
Relaxed breathing
Practise deep breathing at a regular time and in a quiet place where you won’t be disturbed. Loosen or remove any tight clothes you have on, such as shoes or jackets. Make yourself feel completely comfortable.
Sit in a comfy chair which supports your head or lie on the floor or bed. Place your arms on the chair arms, or flat on the floor or bed, a little bit away from the side of your body with the palms up. If you’re lying down, stretch out your legs, keeping them hip-width apart or slightly wider. If you’re sitting in a chair, don’t cross your legs.
Relaxation techniques usually start with focusing on your breathing. The way to do it is to breathe in and out slowly and in a regular rhythm as this will help you to calm down.
- Fill up the whole of your lungs with air, without forcing. Imagine you’re filling up a bottle, so that your lungs fill from the bottom.
- Breathe in through your nose and out through your mouth.
- Breathe in slowly and regularly counting from one to five (don’t worry if you can’t reach five at first).
- Then let the breath escape slowly, counting from one to five.
- Keep doing this until you feel calm. Breathe without pausing or holding your breath.
Practise this relaxed breathing for three to five minutes, two to three times a day (or whenever you feel stressed).
Progressive muscle relaxation
This technique takes around 20 minutes. It stretches different muscles in turn and then relaxes them, to release tension from the body and relax your mind.
Find a warm, quiet place with no distractions. Get completely comfortable, either sitting or lying down. Close your eyes and begin by focusing on your breathing, breathing slowly and deeply, as described above.
If you have pain in certain muscles, or if there are muscles that you find it difficult to focus on, spend more time on relaxing other parts.
You may want to play some soothing music to help relaxation. As with all relaxation techniques, deep muscle relaxation will require a bit of practice before you start feeling its benefits.
Pudendal neuralgia exercises
For each exercise, hold the stretch for a few seconds, then relax. Repeat it a couple of times. It’s useful to keep to the same order as you work through the muscle groups:
- Face – push the eyebrows together, as though frowning, then release.
- Neck – gently tilt the head forwards, pushing chin down towards chest, then slowly lift again.
- Shoulders – pull them up towards the ears (shrug), then relax them down towards the feet.
- Chest – breathe slowly and deeply into the diaphragm (below your bottom rib) so that you’re using the whole of the lungs. Then breathe slowly out, allowing the belly to deflate as all the air is exhaled.
- Arms – stretch the arms away from the body, reach, then relax.
- Legs – push the toes away from the body, then pull them towards the body, then relax.
- Wrists and hands – stretch the wrist by pulling the hand up towards you, and stretch out the fingers and thumbs, then relax.
Spend some time lying quietly after your relaxation with your eyes closed. When you feel ready, stretch and get up slowly.
- Fang H, Zhang J, Yang Y, Ye L, Wang X. Clinical effect and safety of pulsed radiofrequency treatment for pudendal neuralgia: a prospective, randomized controlled clinical trial. J Pain Res. 2018;11:2367-2374. Published 2018 Oct 16. doi:10.2147/JPR.S167866 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6200082[↩]
- Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn 2010;29:4–20[↩]
- Pudendal neuralgia. Hibner M, Desai N, Robertson LJ, Nour M. J Minim Invasive Gynecol. 2010 Mar-Apr; 17(2):148-53.[↩]
- Management of pudendal neuralgia. Pérez-López FR, Hita-Contreras F. Climacteric. 2014 Dec; 17(6):654-6.[↩]
- Pudendal neuralgia. Obstet Gynecol Clin North Am. 2014 Sep;41(3):443-52. doi: 10.1016/j.ogc.2014.04.002. Epub 2014 Jul 9. https://doi.org/10.1016/j.ogc.2014.04.002[↩]
- Conus Medullaris Stimulation With 5 Columns Lead Versus Medical Treatment in Refractory Pudendal Neuralgia (STIMCONE). https://clinicaltrials.gov/ct2/show/NCT02564172[↩][↩]
- Khoder W and Hale D.. Pudendal neuralgia. Obstet Gynecol Clin North Am. September, 2014; 41(3):443-52. https://www.ncbi.nlm.nih.gov/pubmed/?term=25155124[↩]
- Pérez-López FR and Hita-Contreras F.. Management of pudendal neuralgia. Climacteric. December, 2014; 17(6):654-6. https://www.ncbi.nlm.nih.gov/pubmed/?term=24716710[↩]
- Labat JJ, Riant T, Lassaux A, et al. Adding corticosteroids to the pudendal nerve block for pudendal neuralgia: a randomised, double-blind, controlled trial. BJOG. 2016;124(2):251-260. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5215631[↩]





{kind=link}