Contents
What is reverse transcriptase
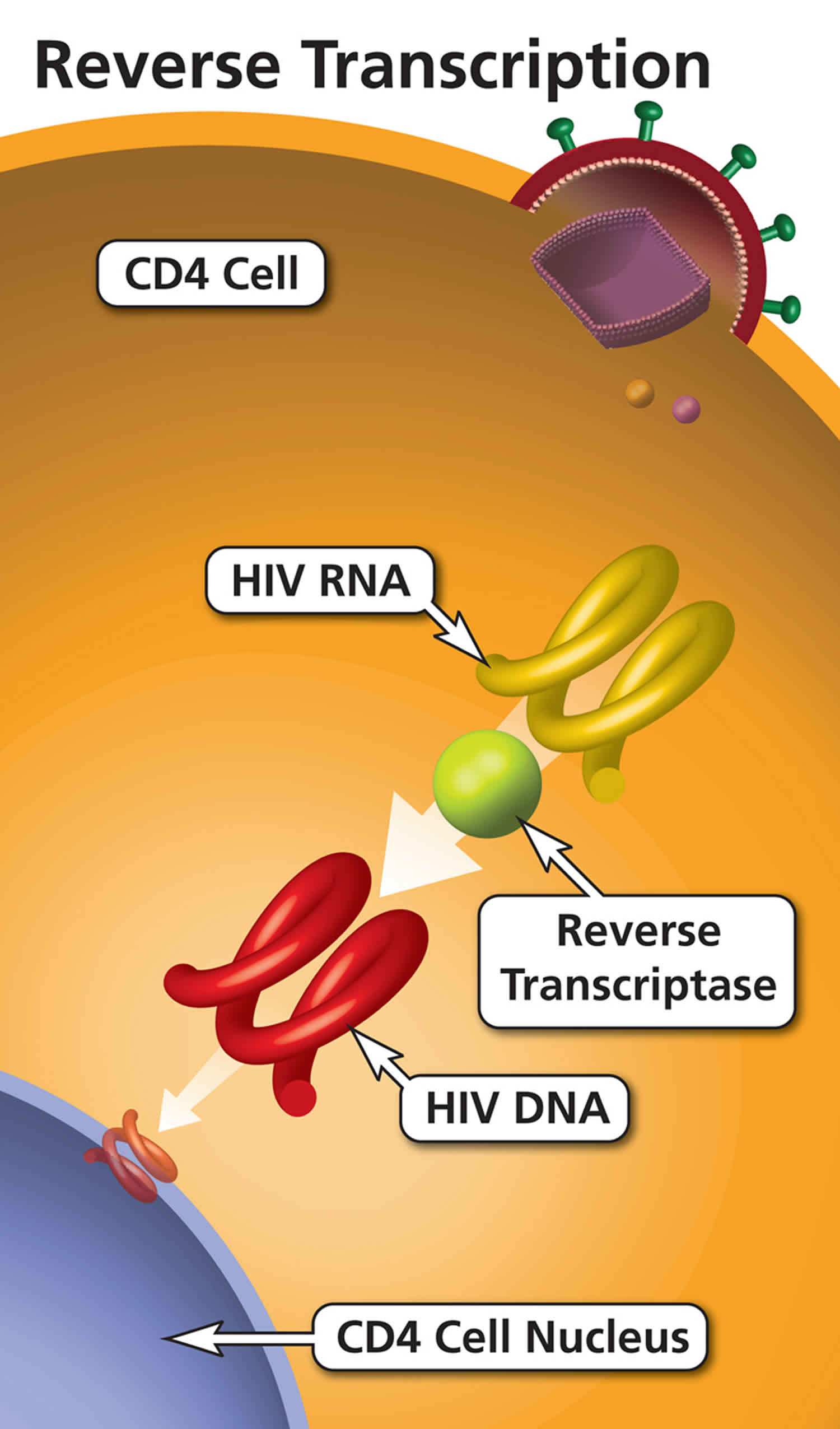
Reverse transcriptase is an enzyme found in HIV (and other retroviruses). HIV uses reverse transcriptase to convert its RNA into viral DNA, a process called reverse transcription. Non-nucleoside reverse transcriptase inhibitors prevent HIV from replicating by blocking reverse transcriptase.
What does reverse transcriptase do?
Reverse transcriptase is an enzyme found in HIV (and other retroviruses). HIV uses reverse transcriptase to convert its RNA into viral DNA, a process called reverse transcription.
What are reverse transcriptase inhibitors?
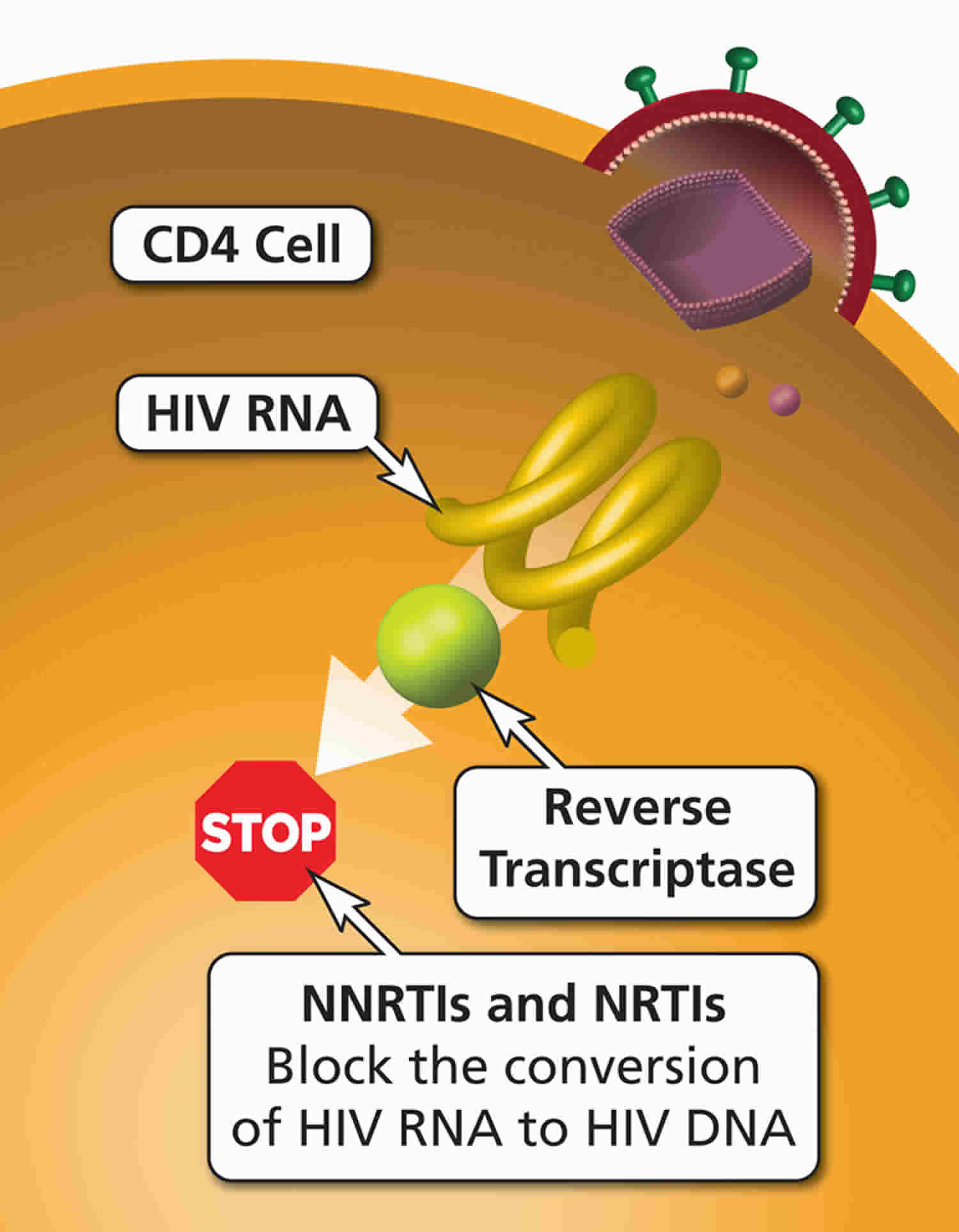
Nucleoside reverse transcriptase inhibitors (NRTIs or ‘nukes’) and non-nucleoside reverse transcriptase inhibitors (NNRTIs or ‘non-nukes’) are antiretroviral HIV drugs. Nucleoside reverse transcriptase inhibitors (NRTIs or ‘nukes’) and non-nucleoside reverse transcriptase inhibitors (NNRTIs or ‘non-nukes’) bind to and block HIV reverse transcriptase (an HIV enzyme). HIV uses reverse transcriptase to convert its RNA into DNA (reverse transcription). Blocking reverse transcriptase and reverse transcription prevents HIV from replicating. Usually a person with HIV will be prescribed a few different antiretrovirals at the same time. This is known as combination therapy.
There are six classes of drugs used in antiretroviral therapy. These drugs are generally classified by the phase of the HIV life cycle inhibited by them. More common combinations include two nucleoside reverse transcriptase inhibitors (NRTIs) and one non-nucleoside reverse transcriptase inhibitor (NNRTI), protease inhibitor (PI), or integrase inhibitor (II). The drugs are listed below according to their class and generic names.
People who are exposed to HIV-positive infectious bodily fluids either by skin puncture, damaged skin, or direct mucous membrane contact are at risk for transmission and should start antiretroviral therapy as soon as possible. The United States Public Health Service guidelines recommend starting prophylactics up to 72 hours post exposure. The recommended regimen is emtricitabine plus tenofovir plus raltegravir for 4 weeks. Those who are exposed to HIV should have follow-up HIV testing at 6, 12, and 24 weeks. If the test results are negative at 24 weeks, they are considered uninfectious 1.
A recent HIV Infection is one that occurs up to 6 months after infection. An HIV regimen often varies based on potential drug interactions with the patient’s current medications and the adverse effects experienced 2.
Patients who are pregnant should begin treatment immediately to prevent mother-to-child transmission of HIV and protect the health of the woman 3.
The following includes all FDA-approved HIV medications:
- Nucleoside reverse transcriptase inhibitors (NRTIs or ‘nukes’): Abacavir, emtricitabine, lamivudine; Tenofovir disoproxil fumarate, zidovudine
- Non-nucleoside reverse transcriptase inhibitors (NNRTIs or ‘non-nukes’): Doravirine (Pifeltro, DOR), Efavirenz (Sustiva, EFV), Etravirine (Intelence, ETR), Nevirapine (Viramune, NVP), Rilpivirine (Edurant. RPV)
- Fusion inhibitors (FIs): Enfuvirtide
- Protease inhibitors (PIs): Atazanavir, darunavir, fosamprenavir, ritonavir, saquinavir, tipranavir
- CCR5 Antagonist: Maraviroc
- Integrase inhibitors: Dolutegavir, raltegravir, elritegnavir, bivtogravir
- Post-Attachment Inhibitors: Ibalizumab
- Pharmacokinetic Enhancers: Cobicistat
The following includes all FDA-approved HIV combination medicines:
- Abacavir and lamivudine
- Abacavir, dolutegravir, and lamivudine
- Abacavir, lamivudine, and zidovudine
- Atazanavir and cobicistat
- Bictegravir, emtricitabine, and tenofovir alafenamide
- Darunavir and cobicistat
- Dolutegravir and rilpivirine
- Efavirenz, emtricitabine, and tenofovir disoproxil fumarate
- Efavirenz, lamivudine, and tenofovir disoproxil fumarate
- Efavirenz, lamivudine, and tenofovir disoproxil fumarate
- Elvitegravir, cobicistat, emtricitabine, and tenofovir alafenamide fumarate
- Elvitegravir, cobicistat, emtricitabine, and tenofovir disoproxil fumarate
- Emtricitabine, rilpivirine, and tenofovir alafenamide
- Emtricitabine, rilpivirine, and tenofovir disoproxil fumarate
- Emtricitabine and tenofovir alafenamide
- Emtricitabine and tenofovir disoproxil fumarate
- Lamivudine and tenofovir disoproxil fumarate
- Lamivudine and zidovudine
- Lopinavir and ritonavir
The FDA does not approve investigational HIV drugs. Investigational drugs include those used to treat or prevent HIV and vaccines to treat or prevent HIV. These drugs are only offered in clinical trials. No vaccines exist yet; however, researchers are studying this possibility 4.
Reverse transcriptase inhibitors mechanism of action
Nucleoside reverse transcriptase inhibitors (NRTIs or ‘nukes’) compete with natural deoxynucleotides for incorporation into a growing viral DNA chain. However, nucleoside reverse transcriptase inhibitors lack a 3′-hydroxyl group on the deoxyribose moiety. This results in incorporation of an nucleoside reverse transcriptase inhibitor and the next incoming deoxynucleotide cannot form the next 5′, 3′ phosphodiester bond needed to extend the DNA chain. The result is a chain termination in DNA synthesis.
Non-nucleoside reverse transcriptase inhibitors (NNRTIs or ‘non-nukes’) block reverse transcriptase by directly binding to the enzyme. Though non-nucleoside reverse transcriptase inhibitors are not incorporated into the viral DNA, they inhibit movement of protein domains of reverse transcriptase that are essential to carry out the DNA synthesis.
Reverse transcriptase inhibitors side effects
Nucleoside reverse transcriptase inhibitors (NRTIs or ‘nukes’) side effects
Hypersensitivity reaction or rash, neutropenia, myopathy, anemia, neuropathy, mitochondrial toxicity, lactic acid build up, pancreatitis, fever, rash, nausea, vomiting, diarrhea, abdominal pain, fatigue, achiness, shortness of breath, sore throat, dark-colored urine, lipoatrophy, and jaundice 5.
Non-nucleoside reverse transcriptase inhibitors (NNRTIs or ‘non-nukes’) side effects
Severe rash, allergic reactions, depression, impaired concentration, headache, sleep disturbance, abnormal dreams, mood changes, jaundice, dark-colored urine, fatigue, nausea and vomiting, peripheral neuropathy, mouth sores, conjunctivitis, myopathy, blisters, and trouble breathing
- Riddell J, Amico KR, Mayer KH. HIV Preexposure Prophylaxis: A Review. JAMA. 2018 Mar 27;319(12):1261-1268[↩]
- Kemnic TR, Gulick PG. HIV Antiretroviral Therapy. [Updated 2019 Feb 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513308[↩]
- O’Donovan K, Emeto TI. Mother-to-child transmission of HIV in Australia and other high-income countries: Trends in perinatal exposure, demography and uptake of prevention strategies. Aust N Z J Obstet Gynaecol. 2018 Oct;58(5):499-505[↩]
- Trovato M, D’Apice L, Prisco A, De Berardinis P. HIV Vaccination: A Roadmap among Advancements and Concerns. Int J Mol Sci. 2018 Apr 19;19, 4[↩]
- Guzman N, Al Aboud AM. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Oct 27, 2018. HIV-associated Lipodystrophy.[↩]





{kind=link}