Contents
Sartorius muscle
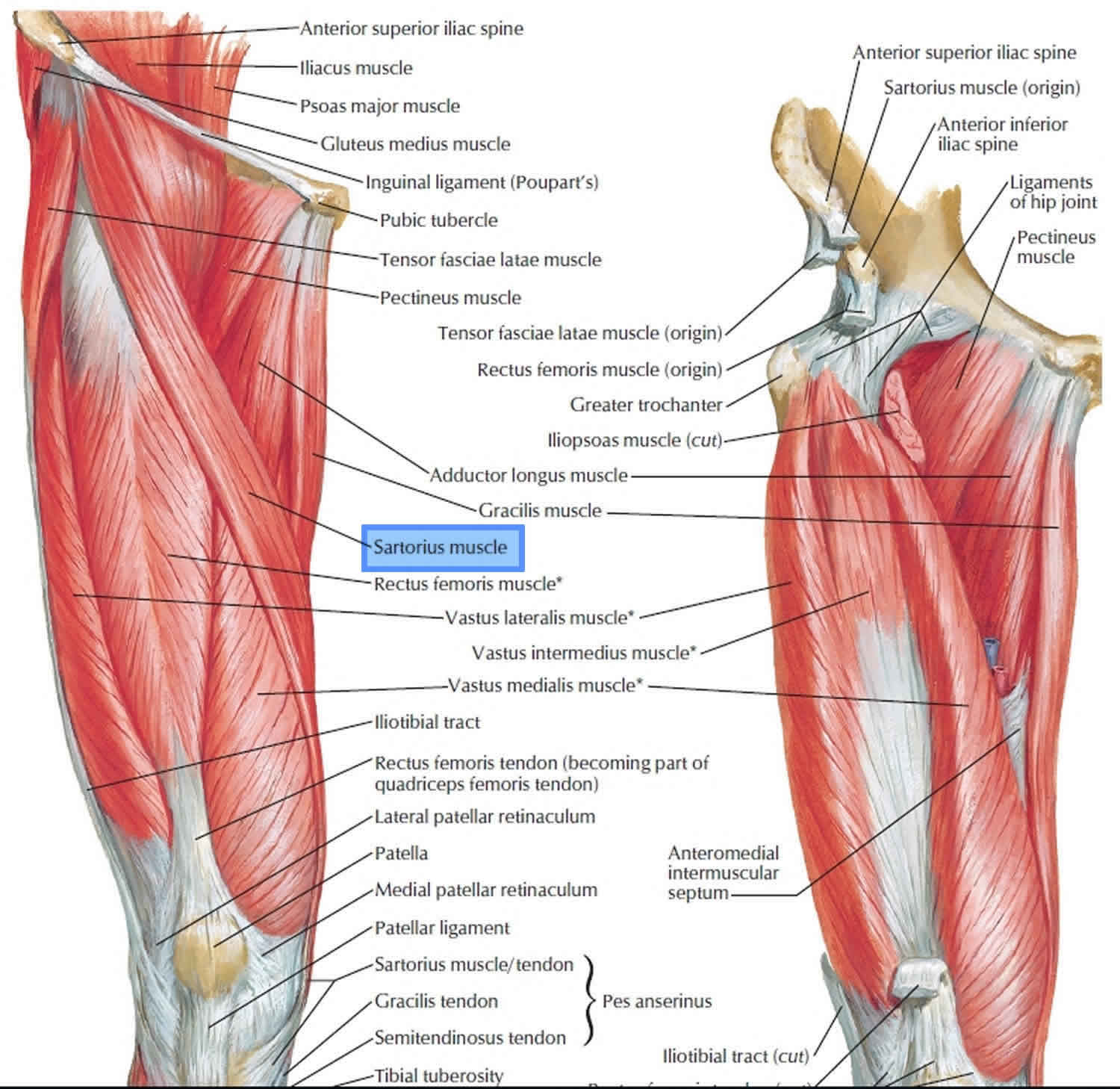
Sartorius muscle is the most superficial muscle in the anterior compartment of the thigh and is the longest muscle in the body spanning both the hip and the knee joints. Sartorius muscle descends obliquely through the thigh from the anterior superior iliac spine (ASIS) to the medial surface of the proximal shaft of the tibia at the pes anserine (Latin for ” goose foot”). Sartorius muscle flat aponeurotic insertion into the tibia is immediately anterior to the insertion of the gracilis and semitendinosus muscles. The sartorius muscle acts synergistically in concert with the other musculature of the hip, thigh, and knee.
The word sartorius is derived from the Latin word sartor, which translates to patcher or tailor, due to the way the individual will position their leg while working. The sartorius muscle assists in flexing the thigh at the hip joint and the leg at the knee joint. Sartorius muscle also abducts the thigh and rotates it laterally, as when resting the foot on the opposite knee when sitting.
The sartorius, gracilis, and semitendinosus muscles attach to the tibia in a three-pronged pattern on the tibia, so their combined tendons of insertion are often termed the pes anserinus.
In the upper one-third of the thigh, the medial margin of the sartorius forms the lateral margin of the femoral
triangle.
In the middle one-third of the thigh, the sartorius forms the anterior wall of the adductor canal.
The sartorius muscle assists in flexing the thigh at the hip joint and the leg at the knee joint. It also abducts the thigh and rotates it laterally, as when resting the foot on the opposite knee when sitting.
The sartorius muscle is innervated by the femoral nerve.
The blood supply to sartorius muscle is mostly comprised of muscular branches of the femoral artery 1. Over half of the blood supply comes from these muscular branches of the femoral artery, but collateral flow does come from elsewhere. A study researching contributing blood flow to the sartorius demonstrated collateral blood flow arising from the superficial circumflex iliac artery, lateral circumflex femoral artery, superficial femoral artery, descending genicular artery, and superior medial genicular artery 2.
Where is the sartorius muscle?
Sartorius muscle is the most superficial muscle in the anterior compartment of the thigh.
Sartorius muscle action
The sartorius muscle assists in flexing the thigh at the hip joint and the leg at the knee joint. Sartorius muscle also abducts the thigh and rotates it laterally, as when resting the foot on the opposite knee when sitting.
Sartorius muscle function
The function of the sartorius is unique in that it can serve as both a hip and knee flexor. The origin for the sartorius is the anterior superior iliac spine, sharing this origin with the tensor fascia lata. At the hip, it acts to both flex the hip as well as externally rotate. Other hip flexors include, most dramatically, the iliopsoas muscle, and, to a lesser degree, the rectus femoris, tensor fascia lata, pectineus, adductor longus, adductor brevis, and gracilis. Antagonists to flexion at the hip include the gluteus maximus, the hamstrings (specifically the long head of biceps femoris), and the semimembranosus and semitendinosus, which all act to extend at the hip.
The primary muscles responsible for internal rotation at the hip are the gluteus medius and gluteus minimus, but the tensor fascia lata also assists. Antagonists and external rotators of the hip include the piriformis, both the superior and inferior gemelli, both the obturator internus and obturator externus, and the quadratus femoris 3.
The insertion for the sartorius muscle is the superior medial aspect of the tibial shaft, near the tibial tubercle. Two other tendons join it at its insertion: the gracilis and semitendinosus, to create the conjoined tendons known as the pes anserinus. At the knee, it acts to flex as well as internally rotate. Other knee flexors include the hamstrings, which are composed of the long and short head of biceps femoris, semitendinosus, and semimembranosus. The popliteus has some function in knee flexion, but more importantly as an internal rotator of the tibia. The antagonists to these muscles belong to the quadriceps muscle group, comprised of the rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius, all of which act to extend the knee.
Along with the popliteus as mentioned above, other internal rotators of the knee acting in concert with sartorius include the semimembranosus, semitendinosus, and gracilis. These muscles are opposed by the long and short heads of the biceps femoris, which act to rotate the knee externally 4.
These synergistic movements of the muscles mentioned above performing with sartorius allow the leg to be moved into the figure-4 position, much like a tailor would position him or herself while working as described earlier.
Sartorius muscle strain
Much like other overuse injuries like tennis elbow, chronic overuse of the sartorius muscle, along with the gracilis and semitendinosus, can create inflammation at the insertion point of the conjoined tendon of these three muscles. This inflammation can irritate the local tissue surrounding the tendon, including the bursa, a condition known as pes anserine bursitis. This is most commonly seen in male athletes in their fourth decade of life. These patients often involved in endurance sporting activities like cycling or running and complain of pain in the posteromedial aspect of the knee, directly at the pes anserine insertion. There are reports of underlying osteoarthritis or rheumatoid arthritis as causes of chronic bursitis 5.
Like avulsions of the anterior superior iliac spine, the vast majority of these injuries improve with conservative treatment. First-line treatment involves physical therapy, including stretching and strengthening. In cases with no apparent improvement with therapy alone, steroid injections can be used as adjunctive therapy 6.
Anterior superior iliac spine avulsion
Young athletes are susceptible to anterior superior iliac spine (ASIS) avulsion injuries through the physis (growth plate). These injuries typically occur secondary to indirect trauma via a sudden, forceful contraction of the sartorius, along with the tensor fascia lata. The ossification of the apophysis usually does not occur until age 21 to 25. Before this ossification occurs, there is a weak point at the muscle-tendon-bone interface, and it is susceptible to an avulsion. This commonly takes place while the hip is in an extended position, like sprinting or swinging a bat.
Avulsions of the ASIS are most often treated conservatively. This involves rest, stretching, protected weight bearing with the aid of crutches, and early range of motion. There are indications, however, for operative treatment of this injury. If there is displacement of the fragment, there is a risk of irritation, loss of strength, as well as healing of the fragment in a displaced position if the injury is treated by conservative means.
Open reduction internal fixation (ORIF) is indicated when the avulsion of the ASIS displaces by a distance of more than 2-3 centimeters. Painful non-unions are also an indication for surgical fixation. There are several different options, including lag screw and tension band fixation 7.
Sartorius muscle stretch
People commonly stretch the sartorius when they do typical lower-body flexibility exercises, such as the standing quad stretches, but it’s pretty common for people to forget to add hip flexor stretches to their routine. Because of the sartorius’ role in hip flexion, it’s critical to use this type of stretch to loosen up the front of the upper hip.
Kneeling Hip Flexor Stretch
Kneel on the ground with your left knee on the ground and your right foot planted in front of you, knee bent at a 90-degree angle, as if you were about to propose. Place your hands on your hips, and keeping your torso upright, squeeze your glutes and press your hips forward until you feel a stretch at the top of your left hip. Hold the stretch for 10 seconds, release, then repeat three to five times before switching legs.
Foam Rolling Exercises
You may also want to loosen up the sartorius muscle with foam rolling exercises. Because the sartorius starts on the outside of your hip and wraps around the front of your thigh before attaching just below the knee on the inside of your lower leg, there are a number of ways you can hit this muscle with a foam roller.
- Roll on the hip crease: Lie prone on top of a foam roller so it’s positioned at a slight angle in the hip crease between your right thigh and your pelvis. Use your forearms, hands, and your other leg to prop yourself up to make this position comfortable and to control the amount of pressure you place on the roller. Avoid hitting any bony points and simply rock forward and backward in small, slow movements, gradually shifting your weight side to side to identify any knots or adhesions in your hip flexors that could use a massage. Continue for 30 to 60 seconds before switching sides.
- Roll at an angle across the thigh: Position the foam roller at the top of your right thigh, your body angled slightly upward so the pressure is on the outside of your upper right thigh. Using your forearms, hands, and your opposite leg to control the movement, slowly roll at an angle down the length of your thigh, so you end with the roller placing pressure on the inside of your thigh, just above your knee. Reverse the movement and roll back up your thigh at an angle, ending on the outside of your right hip. Continue rolling up and down your thigh for about 30 to 60 seconds before switching sides.
- Roll between the legs: Lie on your right side, propped up on your right forearm, your legs stacked on top of each other. Place a foam roller between your legs, just above your knee, allowing gravity to initiate the pressure on the inside of your legs. Move your top leg forward and backward slowly, internally and externally rotating your hip to target the muscles from different angles. Keep the roller in a single spot for about 15 seconds, then move the roller up or down your thigh by about an inch to target the sartorius from a different position. The roller should always be relatively close to your knee, but never directly on the joint.
Sartorius muscle exercises
Hip and Knee Flexing Exercises
There are several variations of the hip flexion exercise that you can perform. You can do the movement by lying face-up on the ground with your legs straight, by sitting on the end of a bench with your torso back at an incline angle and with your legs straight, and by hanging from a pullup bar with your arms and legs straight. During each exercise, you flex your hips and knees until your knees are close to your chest, and then extend your hips and knees until you return to the starting position.
Knee Flexing Exercises
You can also work the sartorius muscle by doing strict knee-flexing exercises. These include the standing leg curl, seated leg curl and lying leg curl. In each of these exercises, you flex your knees to bring the machine pad up toward your buttocks in the case of the standing and lying variation, and downward toward the ground in the case of the seated variation. You then extend your knees to return your legs to the initial point.
Other Muscles Worked
When you do the aforementioned hip- and knee-flexing exercises, you will also be working many other muscles, such as the rectus femoris of the front thigh, the tensor fasciae latae of the hips, and iliopsoas of the hips. In the case of the leg curl exercises, you would be mainly working the hamstrings. The sartorius is acting as an assisting muscle during all of these exercises, and thus you are not isolating the muscle.
Sartorius muscle flap
Sartorius muscle flap is the most used in case of small tissue defect requiring reconstruction because of the ease in harvesting and low donor-site complications 8. Sartorius muscle has all the qualities of an ideal donor for flap 9. It is dispensable highly vascular, long muscle. According to Mathes and Nahai, it is classified as class IV muscle 10 with segmental blood supply. Various studies have shown that 80%–90% of muscle can survive with a single vascular pedicle; either on the proximal or distal 11. It is apparent that larger the diameter of the pedicle, the greater is the chance that it supplies the majority of the muscle. Use of sartorius muscle as proximally based flap for coverage of exposed femoral vessels is well known 12. After the muscle flap is performed, a negative pressure wound therapy system can be used to hasten granulation, remove exudate, reduce edema and act as an effective barrier to bacterial penetration 13:144–150)).
- Walters BB, Varacallo M. Anatomy, Bony Pelvis and Lower Limb, Thigh Sartorius Muscle. [Updated 2018 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532889[↩]
- Buckland A, Pan WR, Dhar S, Edwards G, Rozen WM, Ashton MW, Taylor GI. Neurovascular anatomy of sartorius muscle flaps: implications for local transposition and facial reanimation. Plast. Reconstr. Surg. 2009 Jan;123(1):44-54[↩]
- Mendis MD, Hides JA. Effect of motor control training on hip muscles in elite football players with and without low back pain. J Sci Med Sport. 2016 Nov;19(11):866-871[↩]
- Cleather DJ. An important role of the biarticular hamstrings is to exert internal/external rotation moments on the tibia during vertical jumping. J. Theor. Biol. 2018 Oct 14;455:101-108.[↩]
- Rennie WJ, Saifuddin A. Pes anserine bursitis: incidence in symptomatic knees and clinical presentation. Skeletal Radiol. 2005 Jul;34(7):395-8[↩]
- Beutler A. Musculoskeletal Therapies: Adjunctive Physical Therapy. FP Essent. 2018 Jul;470:16-20.[↩]
- Willinger L, Schanda JE, Lorenz S, Imhoff AB, Buchmann S. Surgical treatment of two adolescent athletes with dislocated avulsion fracture of the anterior superior iliac spine (ASIS). Arch Orthop Trauma Surg. 2017 Feb;137(2):173-177[↩]
- Patrut GV, Neamtu C, Ionac M. Leg for life? The use of sartorius muscle flap for the treatment of an infected vascular reconstructions after VA-ECMO use. A case report. Int J Surg Case Rep. ;16:25–28. doi:10.1016/j.ijscr.2015.09.017 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4643442[↩]
- Classification of the vascular anatomy of muscles: experimental and clinical correlation. . Mathes SJ, Nahai F. Plast Reconstr Surg. 1981 Feb; 67(2):177-87.[↩]
- Classification of the vascular anatomy of muscles: experimental and clinical correlation. Mathes SJ, Nahai F. Plast Reconstr Surg. 1981 Feb; 67(2):177-87.[↩]
- Mojallal A, Wong C, Shipkov C, Ho Quoc C, Recchiuto J, Brown S, et al. Redefining the vascular anatomy and clinical applications of the sartorius muscle and myocutaneous flap. Plast Reconstr Surg. 2011;127:1946–57[↩]
- Soyka P, Favez C, Ganzoni N. Treatment of an infected inguinal wound following vascular reconstruction with a sartorius muscle flap. Helv Chir Acta. 1990;57:355–8[↩]
- Saziye K., Afksendiyos K. The vacuum-assisted closure (V. A. C®) system for surgical site infection with involved vascular grafts. Vascular. 2015;23(April (2[↩]





{kind=link}