
Contents
What is scalp micropigmentation
Scalp micropigmentation is a cosmetic tattoo mimicking shaven scalp that is used as a treatment for thinning hair or hair loss in men and women 1. Scalp micropigmentation requires that the tattoo pigment be placed in microdots of less than 1 mm in size and 1 mm apart, similar to the distance between scalp hair follicular units evident on a shaved scalp 2. Scalp micropigmentation uses a tattoo in a stippling pattern that mimics hair follicles that are cut close to the scalp 3.
Scalp micropigmentation looks simple, but this novel technique must be customized for each patient because the skin in each patient differs with regard to how the scalp reacts as it holds on to the tattoo dye. There are many variables involved with performing scalp micropigmentation that makes this process more of an art form than a science 3. Scalp micropigmentation is a very labor-intensive process that could require multiple sessions and up to 20 hours of procedural time to satisfy the patient 3.
The medical and surgical problems that can be addressed by scalp micropigmentation concealment include:
- Scalp scars from scarring alopecias (Figure 1)
- People with autoimmune diseases such as refractory alopecia areata or alopecia totalis.
- Women who are balding or thinning who are not responsive to minoxidil or other medical treatments and do not qualify for hair transplantation (Figure 2)
- Neurosurgery scars and scars from head trauma, surgeries, and/or hair restoration procedures
- Chemotherapy patients, who do not grow back significant amounts of their hair after treatment
- Deformities in hair restoration patients resulting from unplanned progressive hair loss in men, whose hair transplants have failed to achieve the amount of “fullness” they expected
- People with wide or obvious scars from donor strip harvesting techniques
- People who have open donor scars, as a complication of hair transplant surgery from harvesting techniques between the 1950s and the early 1990s, from strip harvesting surgeries, or from the more modern follicular unit extraction techniques that create punctate scars
- Patients who have the old pluggy or corn-row look with or without donor site depletion and a see-through donor area
- People who dislike using topical concealers or wigs
- Hair thinning or regional balding, where the patient desires to appear to have a fuller head of hair, with or without a shaved scalp.
Scalp micropigmentation is not used to diagnose, prevent, or treat diseases or other conditions, and does not achieve its purpose through chemical action within or on the body. It, like all tattoo instruments and pigments used for these purposes, is a cosmetic process that merely covers up the appearance of unsightly scars, deformities, and balding and thinning areas.
There are no formalized training programs so doctors often hire tattooists or go on Youtube and watch the process and then try to replicate what they see. What they see, however, does not address all of the variables discussed above. Professional tattooists have no experience dealing with the many variables of the human disease or scarred scalp. Experts have seen an increasing number of problems caused by novices that reflect poor judgments in the technical and artistic delivery of scalp micropigmentation. Pigment bleeding is common, as are color changes from poor choices in pigments and poor post-procedure follow-through 4.
It is important to explain to the patient that there may be a blue or green tint to the pigment. The greenish color of the black or gray pigment is similar to how the red blood vessels appear green under the skin, where the increased absorption of the red spectrum of light gives rise to a phenomenon explained by the trichromatic theory of color vision 5. The actual color of some pigments may actually change as well, resulting from direct ultraviolet light exposure on the pigment through the skin and, as such, it can enhance the trichromatic process.
Figure 1. Scalp micropigmentation for scalp scar (patient with scar from multiple surgeries with significant donor area depletion with a shaved scalp)

Figure 2. Scalp micropigmentation women (woman with thinning hair from female genetic hair loss)

Safety and regulatory practices
The United States Food and Drug Administration (FDA) considers the inks used in intradermal tattoos, including permanent makeup, to be cosmetics. When FDA identifies a safety problem associated with a cosmetic, including a tattoo ink, it investigates and takes action, as appropriate, to prevent consumer illness or injury. The FDA states, “consumers should be aware of the risks involved in order to make an informed decision.” The FDA has not traditionally regulated tattoo inks or the pigments used in them because of “competing public health priorities and a previous lack of evidence of safety problems specifically associated with these pigments”.
The actual practice of tattooing is regulated by local jurisdictions in the United States. The growth of the tattoo industry has pushed some state or local governments to increase regulation in this industry and license those delivering tattoo and body piercing services. The primary regulatory actions are activities by the departments of health in most states, reacting to sanitary conditions by those offering these services. Some state governments require completion of a defined educational process and internships and will issue licenses based on examination results and a physical inspection of the facility. Most state governments allow tattooists to work under the general supervision of a medical doctor or dentist, with little regulation.
Scalp micropigmentation procedure
The skin of the scalp has an intricate anatomy. The normal thickness of the scalp has a significant supporting infrastructure for hair (i.e., glands, blood vessels, nerves, muscles, and fat) in much greater abundance than other areas of body skin because of the higher hair densities of terminal hairs. In androgenetic alopecia (genetic hair loss), the large terminal hairs become miniaturized over time, as the hair cycles between catagen and anagen phases. When hair bulk is lost through miniaturization or apoptosis, the supporting infrastructure is reduced in proportion to the loss of the hair.
Scalp micropigmentation functions as a permanent concealer, and the targeted artistic effect is similar to the visual effect of a stippled painting as dots are created between the pores of a balding scalp 4. This can be done with the hair remaining long or on a shaved scalp. The density of the stippling does not necessarily match the number of pores that contain the hair in the average adult. The average Caucasian has 50,000 pores (i.e., 50,000 follicular units), Asians have an average of 40,000 pores (i.e., 40,000 follicular units), and Africans have an average of 30,000 pores (i.e., 30,000 follicular units) 4. The density of the stippling created in the scalp micropigmentation process can be designed to produce shading and create the illusion of texture and fullness to address the desired results worked out between the provider and the patient.
The establishment of a realistic expectation is a critical goal in the first consultation. What the patient sees and what the provider does must be designed to meet the patient’s initial objectives; however, if the patient wants to change his or her goal after the procedure is complete by trying to push the provider to create a painted scalp for more fullness, the patients should be brought to the understanding that seeing through the hair with some visible scalp, is the norm.
The tools in the operator’s hand include pigments of different hues in a variety of formulas and viscosities and instruments employing needle groupings from one to six needles packaged together, in various sizes and shapes 4.. The requirements for each targeted area varies based upon numerous aesthetic factors, including the presence of blemishes or scars on the scalp, skin color, hair color, the amount of hair that is present, and the color and viscosity of the pigments used.
The scalp micropigmentation process begins by inserting a micro droplet of pigment through the skin and into the upper dermis, using a standard tattoo instrument, which supports between one and six needles cycling between 100 to 150 cycles per second. The needle(s) must perforate the epidermis to get to the upper dermis. The depth of needle insertion varies by “feel” and visual judgments made by the operator that reflect the undulating thickness of the epidermis at the point of introduction. The thicker scalp, with more fat and supporting infrastructure, will produce a different skin turgor than an atrophic or scarred scalp, impacting what the operator feels and sees as the scalp micropigmentation process is performed. The operator creates a constant mental feedback loop as he/she constantly adjusts to the effects that are felt and seen. There are additional factors that become important to place the correct amount of pigment, at the correct level, into the scalp for the desired effect. These can be summed in a proportional mathematical “relationship” as shown below:
Ideal pigment deposit correlates to 4:
α [ (A) x (D) x (T) / (R) ] x C x V
A= Angle of needle against the scalp (operator variable factor)
D= Depth of needle into the scalp (operator variable factor)
T= Time the needle is left in the scalp (operator variable factor)
R= Resistance of the scalp (atrophic vs. normal scalp is an intrinsic factor that varies locally in the scalp of the individual)
C= Color of pigment (extraneous factor, such as the choice of the best color)
V= viscosity of pigment (extraneous factor)
N= Needle size, type, number, cycling speeds
α= the approximate mathematical relationship between the variables.
Because every patient is different, every area of the scalp is different, and every point of insertion is different from the prior and subsequent points, the operator is trained to make technical and artistic judgments as the process advances, millimeter by millimeter. Scars retain pigment very differently than the skin of an atrophic or normal scalp. It is not unusual to have both normal and abnormal scalp conditions proximate to each other in the same patient. The artistic judgments in managing this often extend into the normal scalp since a scar that is white will have to blend into the tan or dark skin that surrounds the scar.
The stippling will vary in dot size based upon artistic judgments needed once the process starts. If the pigment is placed only in the epidermis, the process will fail because the pigment will leak out within a few days after the procedure is done. If the pigment is placed too deep into the dermis, it will fail as it diffuses outside the confines of its original area of placement. The observable size of the stippling may change into a noticeable confluent visual amalgam (bleeding) of ink.
Some experts usually recommend multiple sessions for scalp micropigmentation. The number of “dots” may be higher than 40,000 points in each session. The sessions are often long, extending up to eight hours per session 4. Pigment bleeding, in any one session, will have to be addressed, possibly with a Q-switched laser before the next phase of the treatment is undertaken.
Many of the authors’ patients 4 will have two to four sessions before the process is complete since they want to have good assurance that only the upper layer of the dermis is penetrated. Pigment bleeding will be minimized with a cautious, slow, and judicious approach in each session. This process is very stressful for the operator, both mentally and physically, and it is critical for the operators to take frequent breaks during the process.
Figure 3. Scalp micropigmentation pigment placement
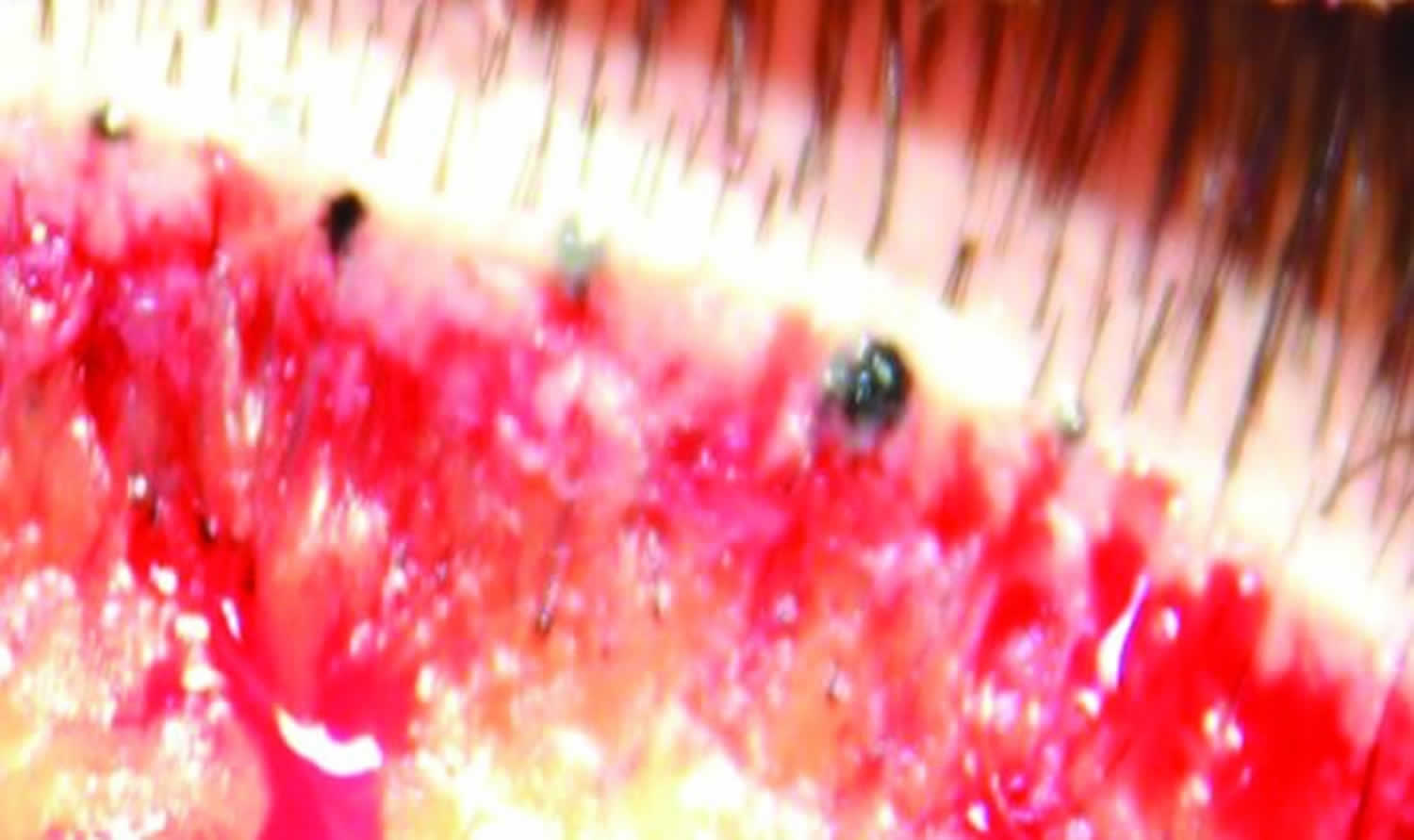
Footnote: Pigment should be placed as high in the dermis as possible. This photo shows proper location of the pigment in the high dermis with different “dot” sizes, which controls the degree of darkness.
[Source 4 ]Once the pigment is placed into the scalp, the amount of pigment that remains over the first few days reflects the quantity and depth of placement. The epidermis ranges in thickness between 0.5 to 1.5mm. Both the stratum corneum and stratum granulosum, constitute the primary barriers for the protection of the skin. The largest layer in the epidermis is the stratum spinosum, and this area fills with pigment in the track created by the needle(s). The deepest layer of the epidermis is the stratum basale, a row of columnar cells resting on the basal lamina that separates the epidermis from the dermis. These cells are mitotically active and they migrate upward toward the surface. Experts try to limit the depth of the needle(s) to the upper dermis.
Significant amounts of pigment may be found in the basal cell layer immediately after the process is done. Pigment particles are found within the cytoplasm of both keratinocytes and phagocytic cells, including fibroblasts, macrophages, and mast cells. At one month, the basement membrane is reforming, and aggregates of pigment particles that are present within the stratum basale are starting to disappear, as these cells migrate upward toward the surface. In the dermis, phagocytic cells that contain pigment may concentrate along the epidermal-dermal border below a layer of granulation tissue that is closely surrounded by collagen. The cells of the stratum granulosum and the stratum spinosum contain particles of pigment, as they migrate upward. Eventually, all of the pigments found in the epidermis will be pushed upward with the exfoliation of the stratum corneum. The only pigment that will remain will be the pigment originally placed in the dermis. This represents a satisfactory outcome.
The portion of ink that washes away on the patient’s first hair wash (2-3 days) reflects the pigment on the surface of the scalp or from the needle track within the stratum corneum and stratum granulosum. With the normal stratum corneum turnover of ~27 days, it is likely that the pigment remains below the stratum corneum in the lower layers of the epidermis for a few months. How much of the pigment remains in the stratum basale and how long it stays there probably varies in different people, especially those with skin diseases that impact skin cycling. Eventually, all of the epidermis becomes free of pigments.
The depth of the stratum basale from the surface of the skin varies significantly along the skin, millimeter by millimeter, reflecting an undulating depth of the epidermis at the dermal border. This makes the depth control by an operator who manually controls the needle by the feel of the resistance a very difficult skill that takes considerable experience. The needles are worked into the superficial dermis and this is the portion of the pigment that remains long term. Black pigment granules vary in diameter from 0.5 to 4.0µm. At one month, transepidermal elimination of ink particles through the upward movement of cells in the stratum spinosum is still in process with ink particles present in keratinocytes, macrophages, and fibroblasts. This is what causes changes in the appearance the patient sees in the first few weeks/months. Touch-ups are an important part of the service in follow-up for these patients, as the initial uniformity in appearance, after the first procedure, changes.
An active foreign body reaction is induced by the pigment and the speed of the reaction varies with individuals; the quality and quantity of pigments used; and the local anatomy, physiology, and pathology of the scalp. In biopsy specimens reported at two to three months and at 40 years after tattooing, ink particles are no longer found in the epidermis, but they are found in dermal fibroblasts, predominantly in a perivascular location beneath a layer of fibrosis that replaced the granulation tissue. Tattoo pigments are found both intracellularly and extracellularly, with mild fibrosis and occasional foreign-body giant cell reactions. Pigment particles are initially dispersed diffusely as fine granules in the upper dermis, as well as in the epidermis in the tract at the point of the injection. The ink particles normally aggregate to a more focal location in the upper dermis from Days 7 to 13 5.
Some of the soluble components of the pigment may be absorbed initially and taken away by the lymphatic system, while the insoluble components are incorporated with the connective tissue that surrounds each of the fibroblasts containing ink particles. The changes that can often be seen in these early days after the process has taken place include washing out of the surface epidermal pigments and extravasation (bleeding) of the dermal pigment beyond the area it was placed. The experienced operator has to balance what is seen at the surface at the time the first procedure is performed with an anticipated loss of some of the more superficial epidermal pigments after a number of days pass. With the stratum corneum penetrated, some leakage of pigments can be seen in the first couple of days after the procedure is performed. Since the pigment in the dermis is not initially stable under the body’s foreign body reaction, some pigments may be absorbed or change color over time 6.
Exposure to ultraviolet light can accelerate changes in color. The authors have seen an almost complete loss of pigment within a few weeks of the initial treatment at one extreme, which might reflect a needle insertion that was too superficial. Considerable extravasation (a bleeding amalgam) of the pigment outside the areas where it was placed in the dermis could also negatively impact the visual aesthetic process as early as in the first week.
Scalp micropigmentation side effects
Common risks and complications include the following: a) infection, where reported outbreaks of non- tuberculous mycobacterial infections associated with contaminated tattoo inks have raised questions about the adequacy of packaging, sterilization, the use of dirty or reused needles, and faulty techniques at the tattoo-parlor level, b) mycobacterium chelonae infection, c) allergies to the component in the pigments producing scarring, granulomas from foreign body reactions, and d) magnetic resonance imaging (MRI) complications, such as swelling and pain from the metals in the pigments when exposed to the powerful MRI magnets. It has been reported that unsterile tattooing equipment and needles can transmit infectious diseases, such as human immunodeficiency virus, hepatitis, and skin infections caused by Staphylococcus aureus and other bacteria.
Little is known about the chemical composition, adsorption, distribution, metabolism, and excretion of inks. Little information is available on short-term and long- term safety of the pigments, their carcinogenic potential, how they affect the cells that take up the inks, and how the body responds to the interaction of ultraviolet light with the inks. We do know that some tattoos fade or turn color when they are exposed to light. Research has also shown that some pigments migrate from the tattoo site to the body’s lymph nodes. The long-term health significance of this is unclear.
- Rassman W, Pak J, Kim J. Combining Follicular Unit Extraction and Scalp Micropigmentation for the Cosmetic Treatment of Alopecias. Plast Reconstr Surg Glob Open. 2017;5(11):e1420. Published 2017 Nov 7. doi:10.1097/GOX.0000000000001420 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5732651/[↩]
- Scalp MicropigmentationA Useful Treatment for Hair Loss. Facial Plast Surg Clin N Am 21 (2013) 497–503 http://dx.doi.org/10.1016/j.fsc.2013.05.010[↩]
- Scalp micropigmentation: a useful treatment for hair loss. Rassman WR, Pak JP, Kim J. Facial Plast Surg Clin North Am. 2013 Aug; 21(3):497-503. https://www.ncbi.nlm.nih.gov/pubmed/24017991/[↩][↩][↩]
- Rassman WR, Pak JP, Kim J, Estrin NF. Scalp micropigmentation: a concealer for hair and scalp deformities. J Clin Aesthet Dermatol. 2015;8(3):35–42. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4382144/[↩][↩][↩][↩][↩][↩][↩][↩]
- Tattoo ink-related infections–awareness, diagnosis, reporting, and prevention. LeBlanc PM, Hollinger KA, Klontz KC. N Engl J Med. 2012 Sep 13; 367(11):985-7.[↩][↩]
- Light and electron microscopic analysis of tattoos treated by Q-switched ruby laser. Taylor CR, Anderson RR, Gange RW, Michaud NA, Flotte TJ. J Invest Dermatol. 1991 Jul; 97(1):131-6.[↩]





{kind=link}