Contents
Sciatica
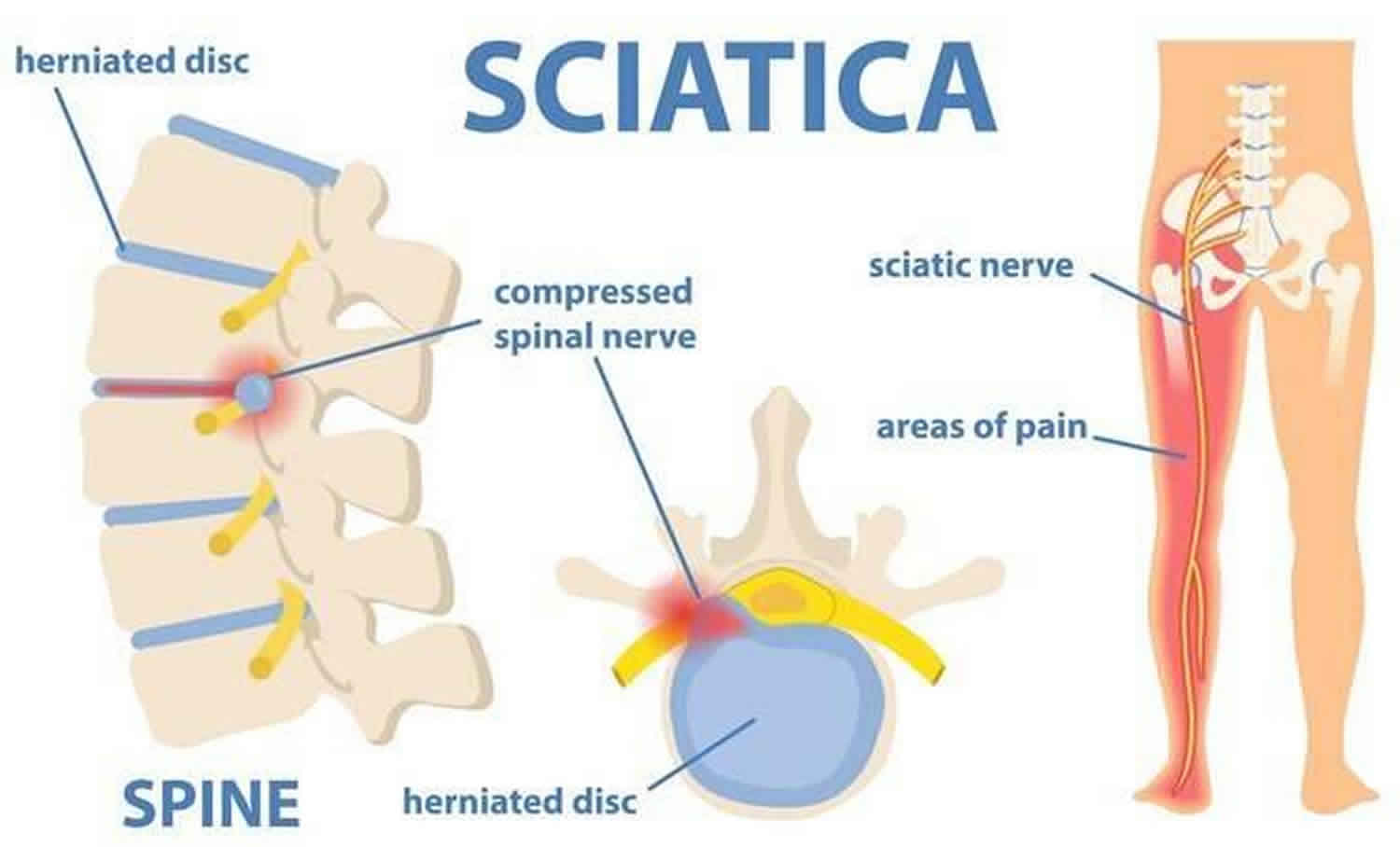
Sciatica also known as lumbosacral radicular pain or lumbar radiculopathy, is a nerve pain in the buttock area with radiation to the lower leg caused by irritation or compression of the sciatic nerve (L4-S3). Sciatica is a very broad term describing nerve pain (a collection of symptoms of what you feel), not a disorder (the cause of the problem) 1. According to International Association for the Study of Pain 1994, the term “sciatica” should be avoided because it might suggest that the condition is a disorder of the sciatic nerve rather than a lumbosacral nerve root 2. Sciatica is described as a radiating, aching or sharp (“knife-like”) pain, sometimes with tingling and numbness, that starts in your lower back or hips (buttock) and extends down the back or side of one leg with the possibility of affecting your feet 3. This is the path of the sciatic nerve and it’s branches – it is the longest nerve in your body and runs from your spinal cord to your buttock and hip area and down the back of each leg. Sciatica may feel like a bad leg cramp that lasts for weeks before it goes away. It may be come on suddenly and can persist for days or weeks. Typically, sciatica affects only one side of your body.
The most important symptom of sciatica is lumbosacral radicular leg pain that follows a dermatomal pattern radiating below the knee and into the foot and toes 4. The pain worsens with coughing; patients may report sensory symptoms, limited forward flexion of the lumbar spine, gait deformity and unilateral spasm of the paraspinal muscles. However, most patients present with a less clear clinical picture 5.
The sciatic nerve is actually two nerves—tibial nerve and common fibular nerve—bound together by a common sheath of connective tissue. The sciatic nerve splits into its two divisions, usually at your knee. The sciatic nerve may be irritated or compressed because of a herniated disc (slipped disc), dislocated hip, osteoarthritis or bone spur on the lumbosacral spine, lumbar spinal stenosis (occurs when the space around the spinal cord in the lumbar spine narrows), pathological shortening of the lateral rotator muscles of the thigh (especially piriformis), piriformis syndrome, pressure from the uterus during pregnancy, inflammation, irritation, or an improperly administered gluteal intramuscular injection. In addition, sitting on a wallet or other object for a long period of time can compress the sciatic nerve and induce pain. This causes inflammation, pain and often some numbness in the affected leg.
Sciatica is a very common condition, especially in men and women between the ages of 30 and 50 6. The cause of sciatica in people under the age of 40 is typically a herniated disk, while older adults typically experience sciatica due to bone spurs and arthritis.
Although the pain associated with sciatica can be severe, ninety percent of acute attacks of sciatica resolve with non-operative treatments in a few weeks 7. Treatments for sciatica are similar to those for a herniated (slipped) disc—rest, pain medications, exercises, ice or heat, and massage. People who have severe sciatica that’s associated with significant leg weakness or bowel or bladder changes might be candidates for surgery 7.
Figure 1. Sciatic nerve origin
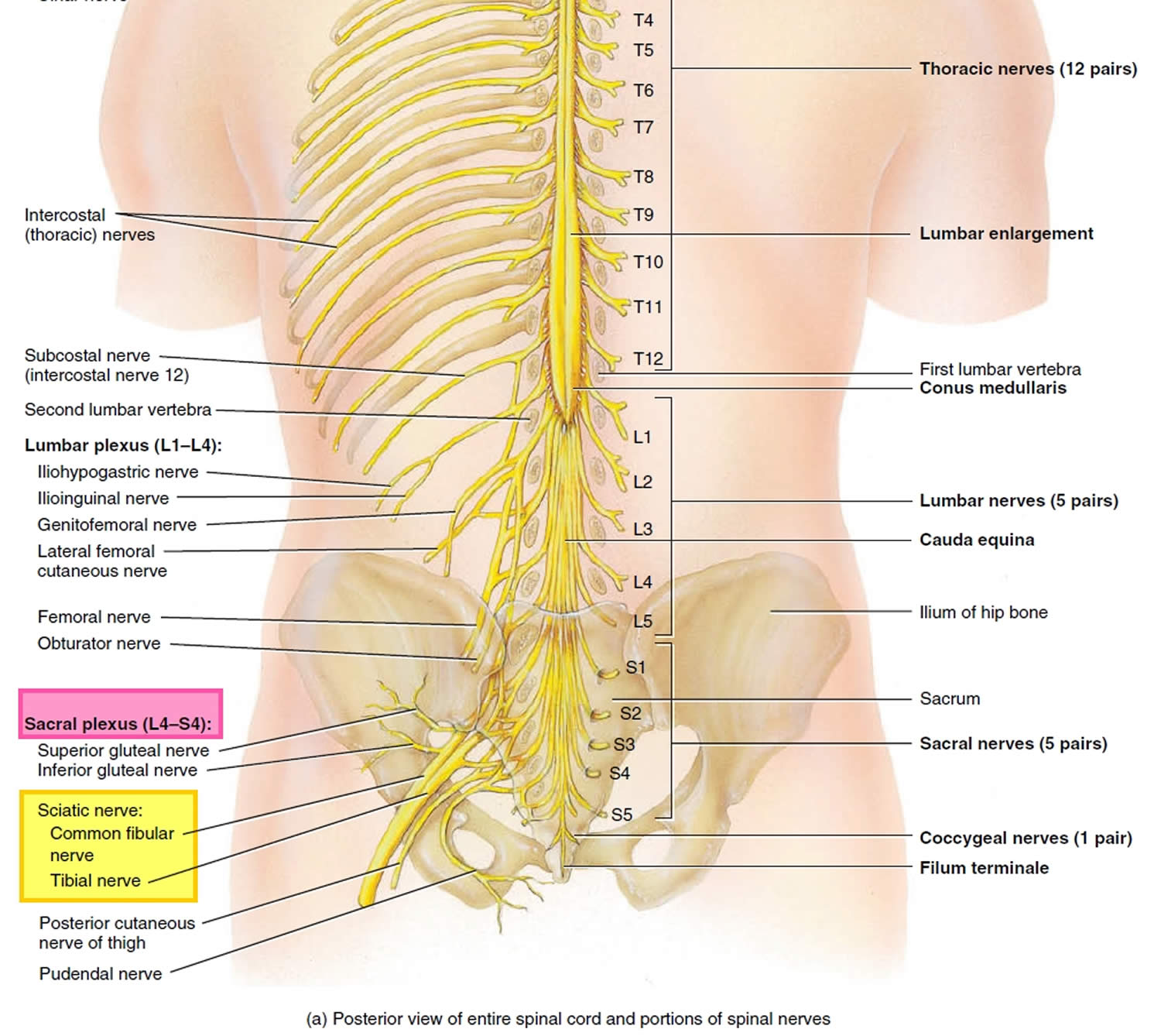
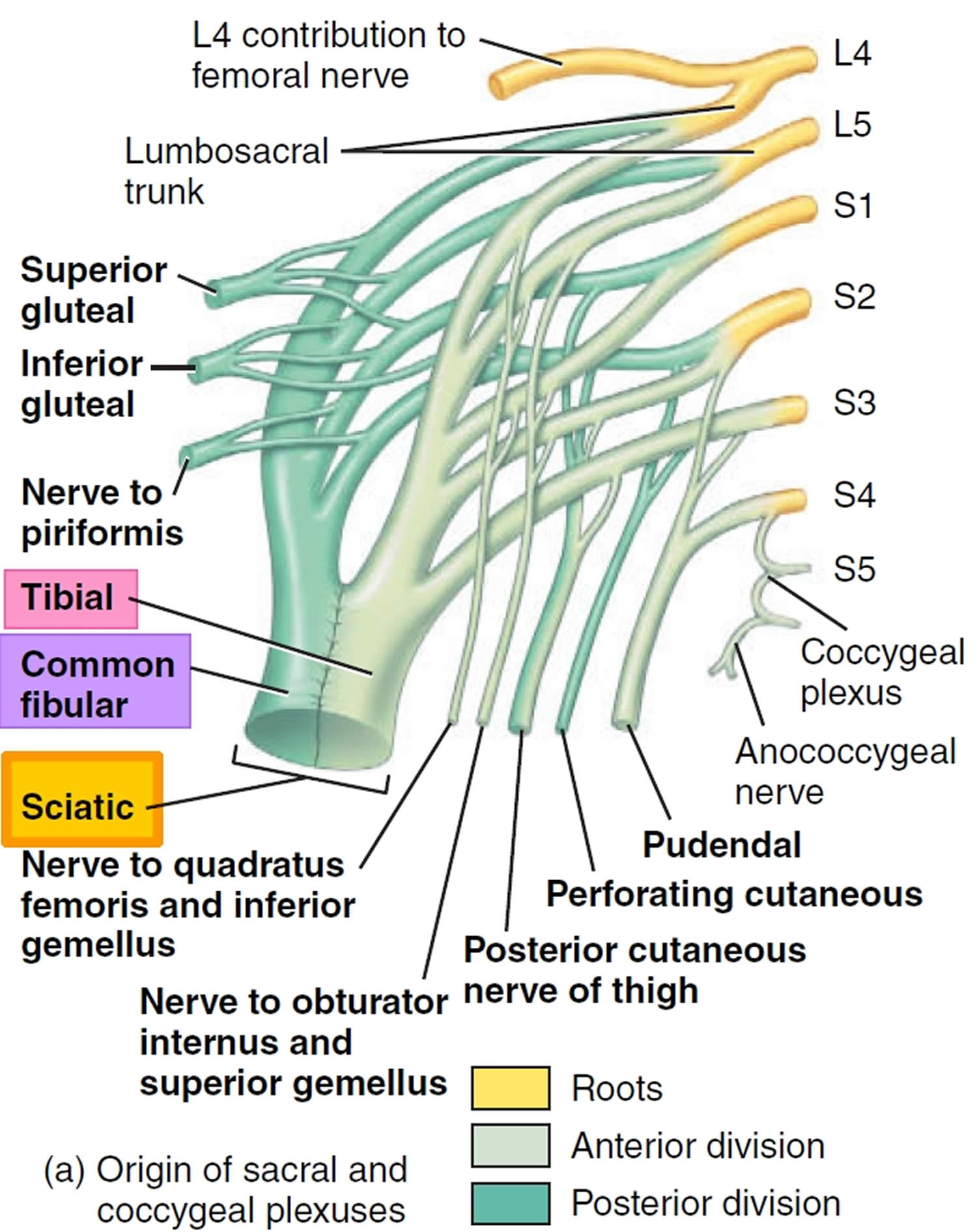
Figure 2. Sciatic nerve branches
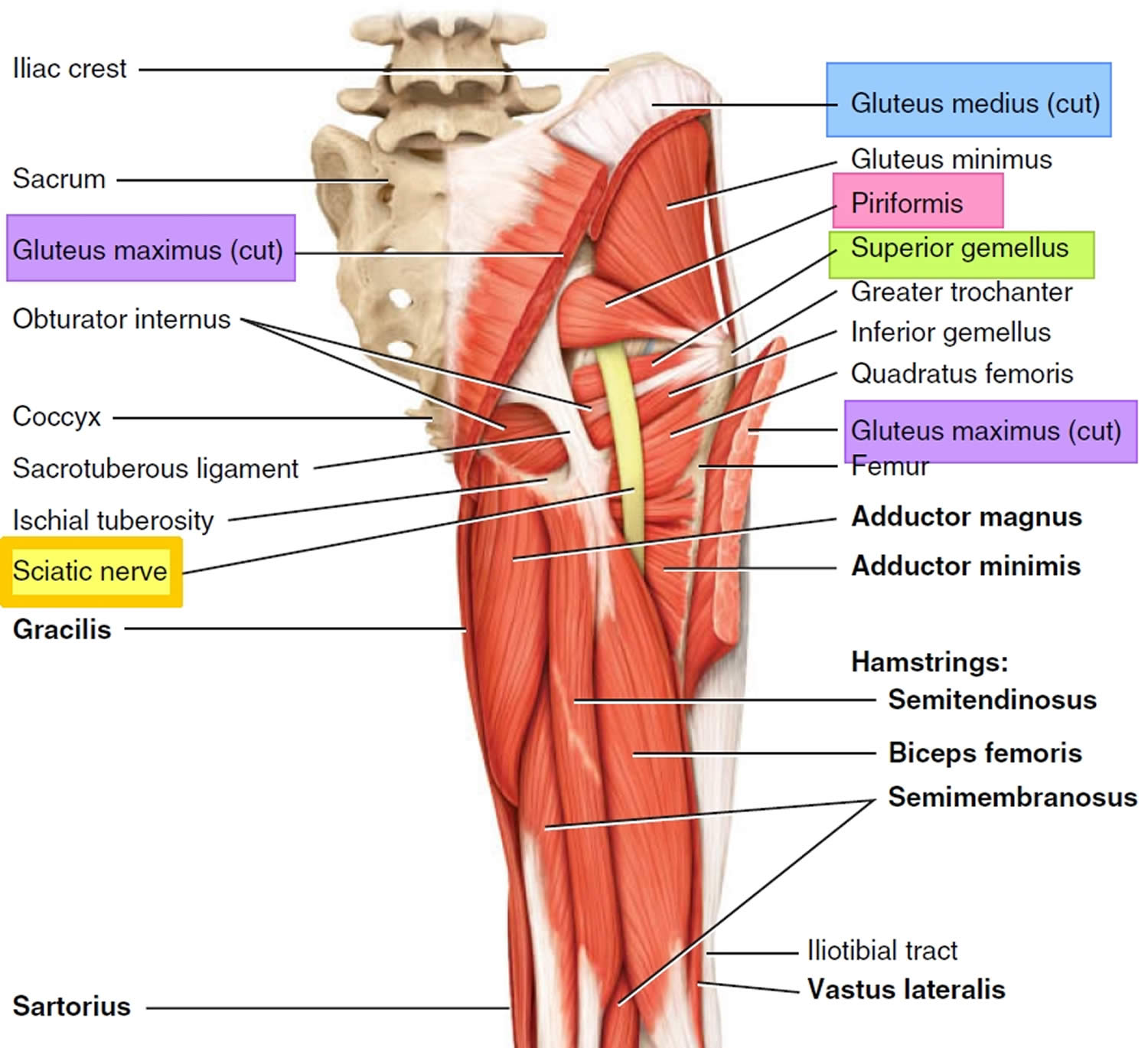
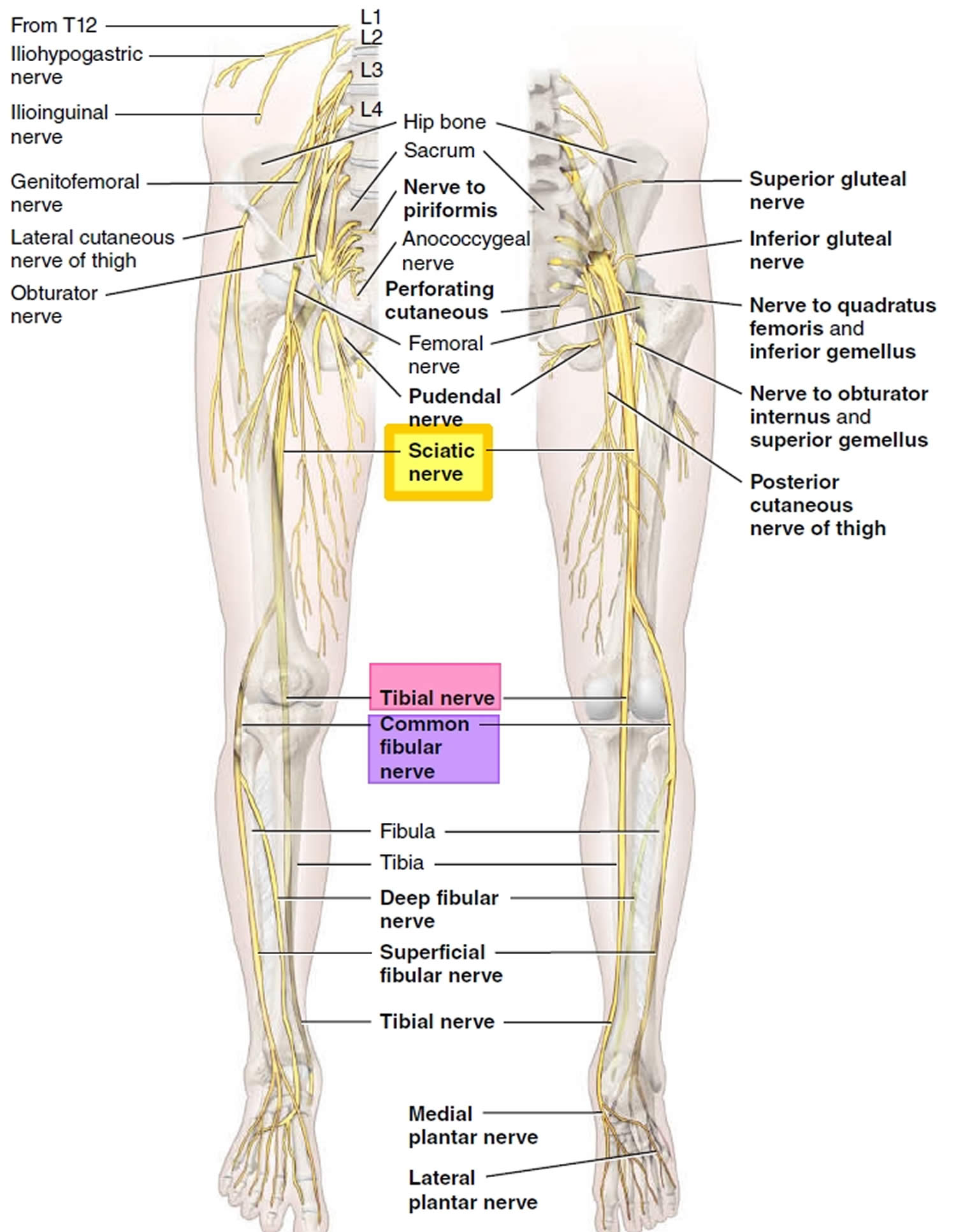
Figure 3. Variations on sciatic nerve anatomy
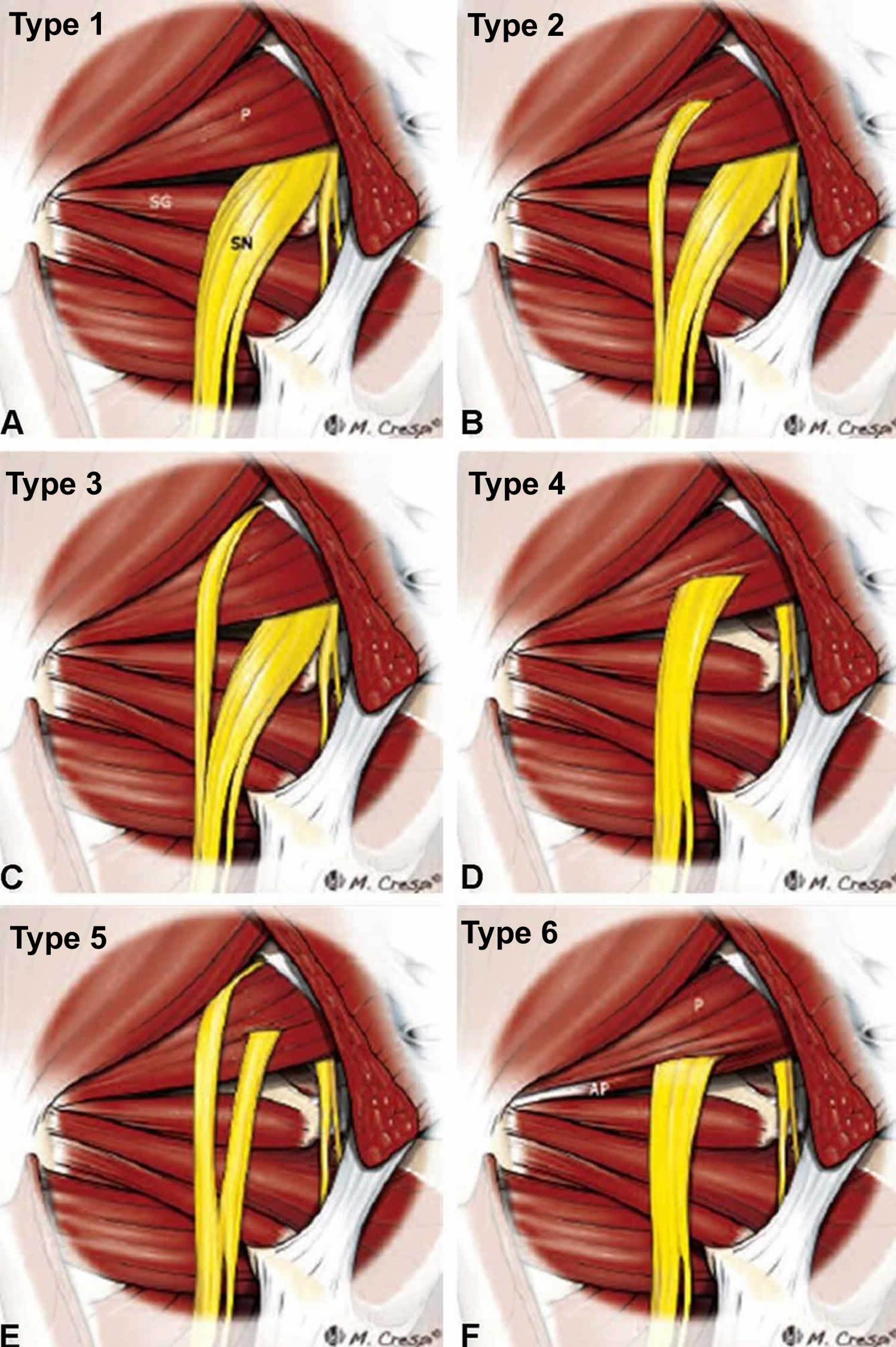
Footnotes: Anatomic variations of the relationship between the piriformis muscle and sciatic nerve. Left posterior view of the piriformis syndrome (deep gluteal syndrome). Diagrams illustrate the six variants, originally described by Beaton and Anson in 1937. (a) An undivided nerve emerges below the piriformis muscle (normal course). (b) A divided sciatic nerve passing through and below the piriformis muscle. (c) A divided nerve passing above and below an undivided muscle. (d) An undivided sciatic nerve passing through the piriformis muscle. (e) A divided nerve passing through and above the muscle heads. (f) Diagram showing an additional unreported B-type variation consisting of a smaller accessory piriformis (AP) with its own separate tendon.
Abbreviations: SN = sciatic nerve; P = piriformis muscle; SG superior gemellus muscle
[Source 8 ]Figure 4. Herniated disc
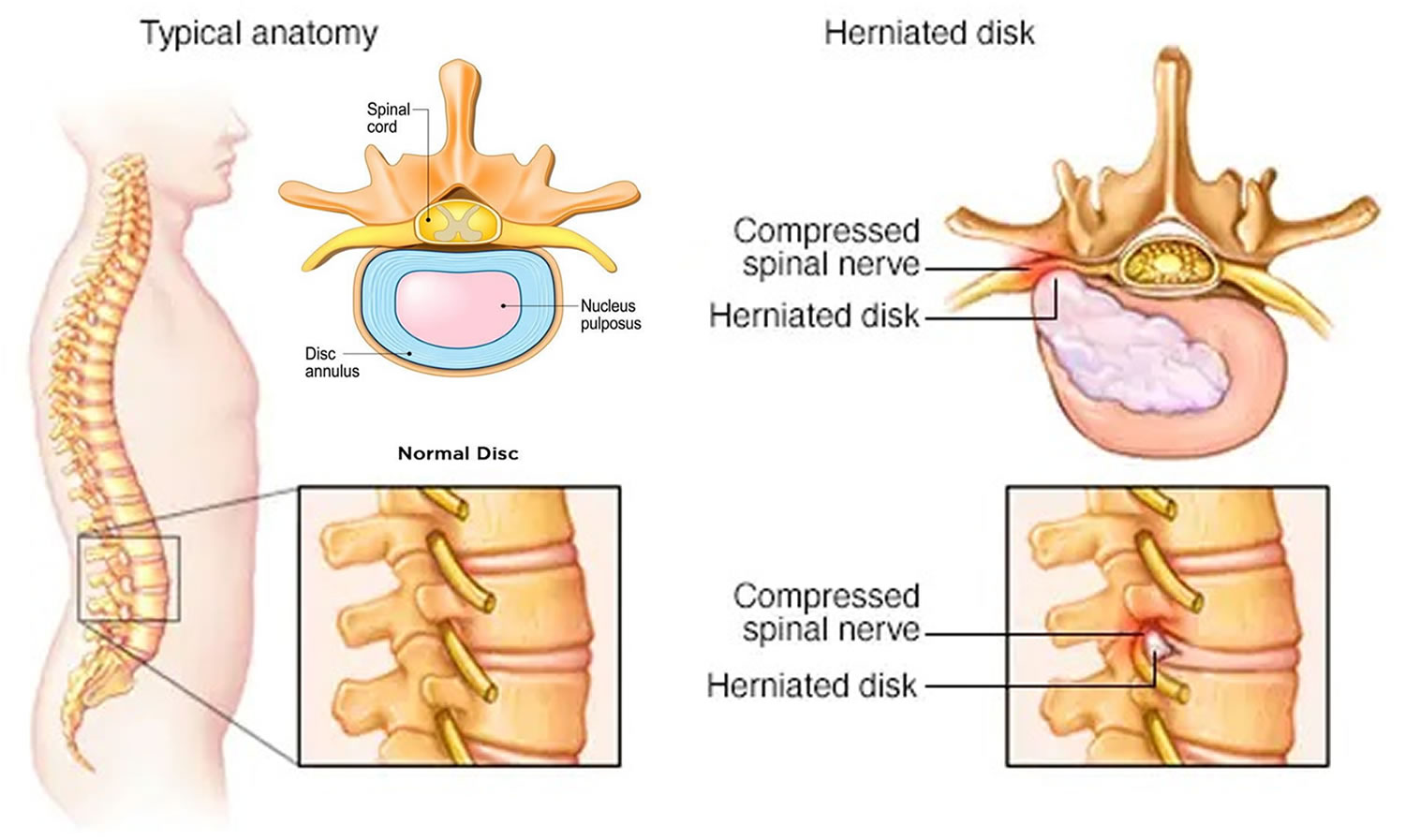
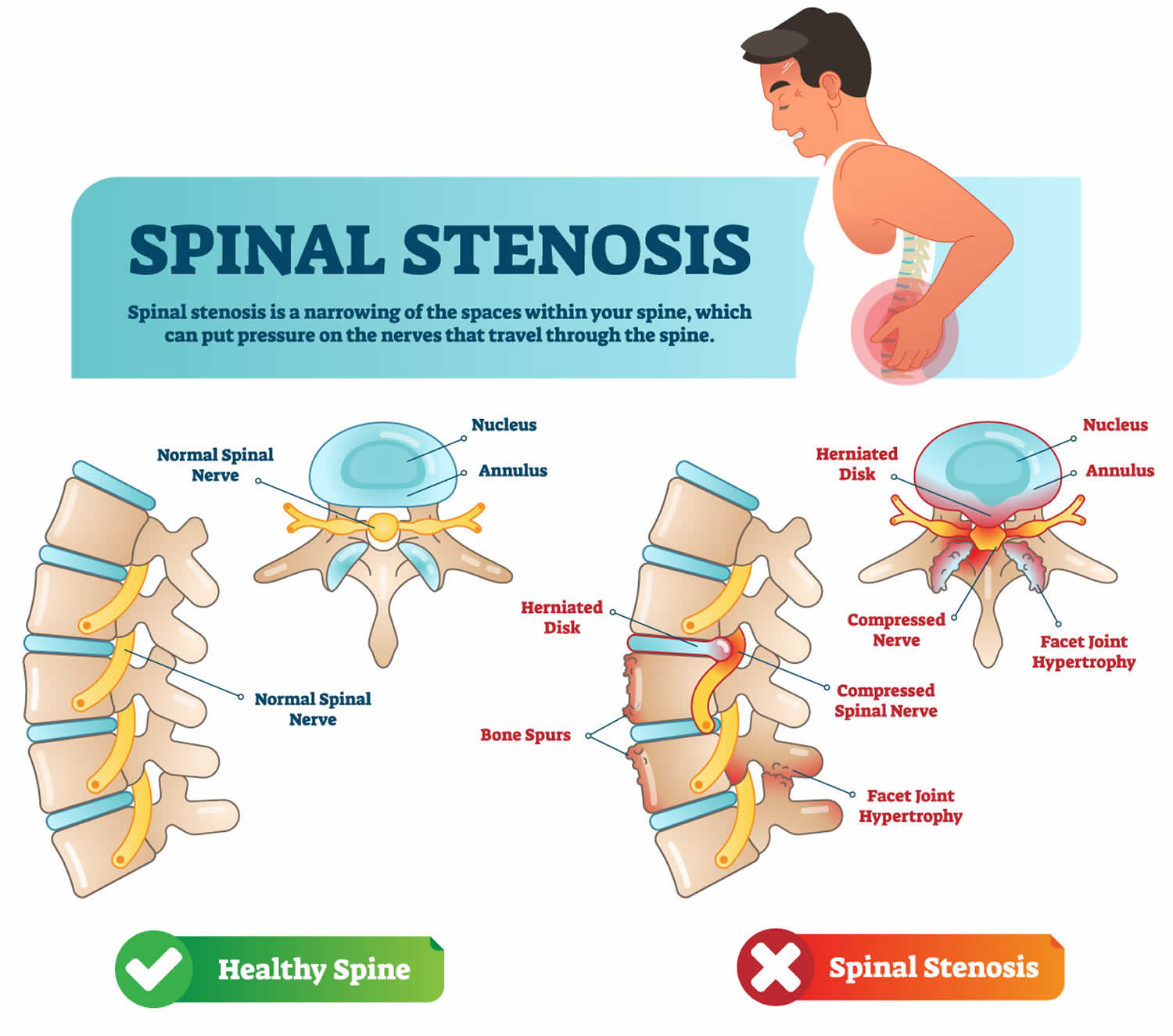
Figure 5. Spinal stenosis
Mild sciatica usually goes away over time. See your doctor if self-care measures fail to ease your symptoms or if your pain lasts longer than a week, is severe or becomes progressively worse. Get immediate medical care if:
- You have sudden, severe pain in your low back or leg and numbness or muscle weakness in your leg
- The pain follows a violent injury, such as a traffic accident
- You have trouble controlling your bowels or bladder
History of intravenous (IV) drug abuse is a risk for epidural abscess and seeding of bacteria anywhere in the body (endocarditis, cerebral abscess, among others). Additionally, those with HIV (human immunodeficiency virus), diabetes, or who are immunocompromised have a much higher risk of all infections, and epidural abscess must be considered. Any history of bowel or bladder incontinence, urinary retention, or lower extremity weakness suggests acute neurologic deficit and should prompt a more aggressive workup. Anticoagulant use is a risk for all sources of bleeding, including epidural abscess. A history of trauma, malignancy, or tuberculosis may suggest fracture, metastasis, and more serious causes of the back pain should be ruled out before a simple diagnosis of sciatica is used. And lastly, fevers, night sweats, chills would not be typical symptoms seen in simple sciatica and thus should prompt further consideration in the workup.
Should I stretch my sciatic nerve?
Nerves do not stretch well, but they do slide and glide as the body moves. Many people with sciatica have the urge to stretch the hamstrings due to feeling pain in the back of the thigh. Those symptoms may actually be sciatica.
Stretching the sciatic nerve may increase pain due to pulling on an irritated nerve or lower back structures. Typically, gentle movements of irritated structures are best helping the nerve slide and glide the way it is supposed to move. This may reduce the symptoms.
Sciatica during pregnancy
Lower back pain and sciatica are common issues during pregnancy. During pregnancy, the sacroiliac joint is one of the main sources of pain for a woman. This is typically due to the increased strain on the lower back and hips from increased weight as well as the possibility for increased laxity in tendons and ligaments that occurs during pregnancy. This laxity allows for increased movement of the sacroiliac joint which can trigger the supporting muscles around the joint to tighten in an attempt to compensate and provide stability for the joint. This prolonged muscle tightness/activation is a likely source for both hip and radiating (nerve) pain.
The good news is that it usually improves with the exercises and stretches for sciatica. But there should be modifications in the 2nd and 3rd trimesters. Typically, it is recommended that women avoid lying face down after about 16 weeks gestation. They may lie prone for a short time to exercise after this point but not for ling periods. It is recommended that women who are pregnant consult their OB/GYN doctor before performing stretches for sciatica.
If sciatica during pregnancy is coming from the sacroiliac joints, a pregnancy sacroiliac (SI) belt may help. A pregnancy sacroiliac belt is a supportive belt or brace that applies pressure around the pelvis. The pressure or support helps to stabilize the sacroiliac joints during later stages of pregnancy. An sacroiliac joint belt is similar to a lumbar support brace but is worn lower around the hips. Most sacroiliac joint belts are typically one piece with multiple tightening straps to allow for it to be a mostly universal fit. Depending on the thickness of the belt, it could possibly be worn under clothing as well.
There are few risks to wearing an sacroiliac (SI) belt, but it is always recommended to speak with your OB/GYN doctor before using any piece of medical equipment. Depending on your physician and style of SI belt, the amount of time that you should spend wearing the belt can vary, but many physicians will recommend wearing the belt 24 hours a day during pregnancy as long as the person is experiencing symptoms from sacroiliac joint instability.
If your physician prescribes an SI belt during pregnancy, they may also recommend physical therapy. A physical therapist will perform a physical assessment of mobility as well as strength to determine a proper plan of care. Most patients who experience sacroiliac joint pain during pregnancy need to work on hip and core strengthening exercises to promote natural stability of the lumbar spine and hips.
Figure 6. Pregnancy sacroiliac joint belt

Sciatic nerve
The sciatic nerve is the longest and largest nerve in the human body, originating the ventral rami of spinal nerves L4 through S3 and contains fibers from both the posterior and anterior divisions of the lumbosacral plexus (see Figure 1). After leaving the lower vertebrae, the nerve fibers converge to form a single nerve. It exits the pelvis through the greater sciatic foramen inferior to the piriformis muscle along with the pudendal nerve and vessels, inferior gluteal nerve and vessels, nerve to obturator internus, and posterior cutaneous nerve (see Figure 2). The sciatic nerve then progresses down the posterior compartment of the thigh deep to the long head of the biceps femoris muscle, superficial to adductor magnus and short head of biceps femoris muscle, and laterally to semitendinosus and semimembranosus muscles (see Figure 2). Just before reaching the popliteal fossa, it divides into 2 important branches. One branch is the tibial nerve, which continues to descend in the posterior compartment of leg and foot. The other branch is the common fibular nerve (also called common peroneal nerve), which travels down the lateral and anterior compartment of the leg and foot (see Figure 2).
Most often the undivided sciatic nerve exits the greater sciatic foramen inferior to the piriformis muscle, but this is not always the case 9. In the most common anatomic variant, the sciatic nerve splits above the piriformis muscle and one division exits through the piriformis muscle while the other exits below. There are 6 anatomic variants described in the current literature 9, 10 (Figure 3):
- Type 1: sciatic nerve exits inferior to piriformis, undivided
- Type 2: sciatic nerve divides above piriformis, one portion exits through piriformis, the other inferior to it
- Type 3: sciatic nerve divides above piriformis, one portion courses anterior to piriformis, the other posterior to it
- Type 4: sciatic nerve exits through piriformis, undivided
- Type 5: sciatic nerve divides above piriformis, one portion exits through piriformis, the other superior to it
- Type 6: sciatic nerve divides exists from superior aspect of piriformis posteriorly, undivided
The sciatic nerve provides motor innervation to the posterior compartment of the thigh 10. This includes the biceps femoris, semimembranosus, semitendinosus, and the ischial portion of the adductor magnus which allow for knee flexion and hip adduction. The tibial nerve innervates the posterior compartment of the leg and foot which includes the gastrocnemius, soleus, plantaris, popliteus, flexor hallucis longus, flexor digitorum longus, and tibialis posterior. These muscles are primarily responsible for plantarflexion and flexion of the toes. The common fibular nerve innervates the anterior and lateral compartments of the leg and foot. The anterior compartment includes tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius. These muscles are primarily responsible for dorsiflexion of the foot and extension of toes. The lateral compartment includes peroneus longus and brevis, which are responsible for foot eversion 11.
The sciatic nerve also provides sensory innervation to the skin of the foot and the lower leg (except for the medial leg which is innervated by the saphenous nerve) 10. The tibial nerve further divides into the medial and lateral plantar nerves, which are responsible for the sensation of the sole. The common peroneal nerve further divides into the superficial peroneal nerve and deep peroneal nerve. The superficial peroneal nerve provides sensory innervation to the lateral leg and dorsum of the foot. The deep peroneal nerve is responsible for sensation in between the first and second toes. The medial and lateral sural nerves are made up of collateral branches from both the tibial and common peroneal nerves and provide sensation to the calf and a small lateral portion of the foot.
In many sciatic nerve injuries, the common fibular portion is the most affected, frequently from fractures of the fibula or by pressure from casts or splints over the thigh or leg. Damage to the common fibular nerve (common peroneal nerve) causes the foot to be plantar flexed, a condition called foot drop, and inverted, a condition called equinovarus (where the foot points downward and inward). There is also loss of function along the anterolateral aspects of the leg and dorsum of the foot and toes. Injury to the tibial portion of the sciatic nerve results in dorsiflexion of the foot plus eversion, a condition called calcaneovalgus (where the foot points upward and outward). Loss of sensation on the sole also occurs.
Sciatic nerve pain
Sciatica is a symptom (what you feel), not a disorder (the cause of the problem). Sciatica refers to pain that radiates along the path of the sciatic nerve, from your lower (lumbar) spine to your buttock and down the back of your leg is the hallmark of sciatica. You might feel the discomfort almost anywhere along the sciatic nerve pathway, but it’s especially likely to follow a path from your low back to your buttock and the back of your thigh and calf. Typically, sciatica affects only one side of your body.
The pain can vary widely, from a mild ache to a sharp, burning sensation or excruciating pain. Sometimes it can feel like a jolt or electric shock. It can be worse when you cough or sneeze, and prolonged sitting can aggravate symptoms. Usually only one side of your body is affected.
Some people also have numbness, tingling or muscle weakness in the affected leg or foot. You might have pain in one part of your leg and numbness in another part.
If you have sciatica you may experience the following:
- Pain in your lower back or hip that radiates down from your buttock to the back of one thigh and into your leg, especially when you sit, sneeze or cough.
- Weakness.
- Pins and needles, numbness, or a burning or tingling sensation down your leg.
Sciatica complications
Although most people recover fully from sciatica, often without treatment, sciatica can potentially cause permanent nerve damage. Seek immediate medical attention if you have:
- Loss of feeling in the affected leg
- Weakness in the affected leg
- Extreme pain/numbness/weakness in both legs
- Loss of bowel or bladder function.
These are symptoms of cauda equina syndrome, a rare but serious condition that requires emergency care. If you experience either of these symptoms, seek medical help immediately 12.
It is also important to let your doctor know if you are experiencing fever, increased night pain & night sweats, as they may indicate a more sinister cause for your sciatica.
Sciatica causes
Sciatica occurs when the sciatic nerve becomes pinched, usually by a herniated disk in your spine or by an overgrowth of bone (bone spur) on your vertebrae 13. More rarely, the sciatic nerve can be compressed by a tumor or damaged by a disease such as diabetes.
- Herniated disc. Herniated disc is the most common cause of sciatica. The spine is made up of a series of vertebrae (bones) cushioned by intervertebral discs (also called intervertebral fibrocartilage). The intervertebral gel-like discs are the cushioning material between the spine’s vertebrae and they act like shock absorbers. The disc has an outer layer called an annulus which is made of tough tissue. The annulus protects a softer interior tissue called the nucleus pulposis. A rupture or tear in the disc annulus allows the nucleus to be pushed out and into the spinal canal hitting the nerves of the spine producing the symptoms of sciatica.
- Degenerative arthritis. Due to wear and tear of the bones of the spine. This can lead to narrowing of the spinal canal (spinal stenosis) or stress fractures or instability of spinal joints (spondylolysis and spondylolisthesis).
- Spinal tumors. Rarely, tumors will compress the nerve roots or spinal cord causing compressing symptoms such as sciatica. Tumors can occur in the spinal cord, between the covering layers of the spinal cord (meninges) or in the spaces between the spinal cord and the spinal bones (vertebrae). These are uncommon and identifiable on spine imaging with an MRI or CT.
- Infection and inflammation. Infection and inflammation cause tissue swelling around the nerve roots, hence may increase pressure around the affected areas.
- Trauma (single or cumulative small trauma). A fall or blow to the spine or buttock can affect the nerves of the lower back producing symptoms of sciatica.
- Piriformis syndrome also known as deep gluteal syndrome, extra-spinal sciatica or wallet neuritis. Piriformis syndrome is generally due to shortening or spasm of the piriformis muscle (a muscle in your buttock) from trauma or overuse, compressing the sciatic nerve beneath it to cause sciatica 11. The piriformis muscle connects the sacral spine to the upper portions of the femur and aids in hip extension and leg rotation. Due to the proximity of the sciatic nerve, any injury or inflammation to the piriformis muscle can cause “sciatica symptoms.” Often overuse injuries, particularly in runners or other endurance athletes, cause inflammation of the piriformis muscle, and the ensuing symptoms mimic sciatica. Therefore, these patients tend to have increased pain from applying direct pressure to the piriformis muscle, increased pain when walking up inclines or stairs, and decreased range of motion of the hip joint. Piriformis syndrome is reportedly common in females, and its prevalence among patients with sciatica diagnosis ranges between 6% and 36% 14. Nevertheless, it appears as a low back pain association in men of various ages as well, as observed in a recent study 15. Piriformis-specific stretches, as well as hamstring stretches, are helpful to release this muscle tension and to treat this painful condition. Lumbar and sacroiliac manipulation may also prove beneficial for some patients 16. In addition, rest from the activity causing the pain is helpful 11.
- Pelvic instability
- Uterine pressure during pregnancy
- Vascular problems. Abnormal blood vessels in and around the spinal canal.
Risk factors for sciatica
Risk factors for sciatica include:
- Age. Age-related changes in the spine, such as herniated disks and bone spurs, are the most common causes of sciatica.
- Obesity. By increasing the stress on your spine, excess body weight can contribute to the spinal changes that trigger sciatica.
- Occupational loading of the low back. A job that requires you to twist your back, carry heavy loads or drive a motor vehicle for long periods might play a role in sciatica, but there’s no conclusive evidence of this link.
- Prolonged sitting. People who sit for prolonged periods or have a sedentary lifestyle are more likely to develop sciatica than active people are.
- Diabetes. This condition, which affects the way your body uses blood sugar, increases your risk of nerve damage.
- History of low back trauma
- Heavy smoking
- Pregnancy
- Tall skeletal frame
- Back strain from unaccustomed physical exertion
Factors in 14-year-old adolescents that predicted sciatica in adulthood 17:
- Smoking
- Obesity (i.e., body mass index (BMI) > 95th percentile for age)
- Sports participation
Sciatica prevention
It’s not always possible to prevent sciatica, and the condition may recur. The following can play a key role in protecting your back:
- Exercise regularly. To keep your back strong, pay special attention to your core muscles — the muscles in your abdomen and lower back that are essential for proper posture and alignment. Ask your doctor to recommend specific activities.
- Maintain proper posture when you sit. Choose a seat with good lower back support, armrests and a swivel base. Consider placing a pillow or rolled towel in the small of your back to maintain its normal curve. Keep your knees and hips level.
- Use good body mechanics. If you stand for long periods, rest one foot on a stool or small box from time to time. When you lift something heavy, let your lower extremities do the work. Move straight up and down. Keep your back straight and bend only at the knees. Hold the load close to your body. Avoid lifting and twisting simultaneously. Find a lifting partner if the object is heavy or awkward.
- Reduce your risk factors such as obesity and smoking.
Sciatica differential diagnosis
A thorough differential diagnosis list is important in considering a diagnosis of sciatica and should include.
- Herniated lumbosacral disc
- Muscle spasm
- Nerve root impingement
- Epidural abscess
- Epidural hematoma
- Tumor
- Potts disease, also known as spinal tuberculosis
- Piriformis syndrome
Sciatica diagnosis
Sciatica is mainly diagnosed by history taking and physical examination. During the physical exam, your doctor may check your muscle strength and reflexes. For example, you may be asked to walk on your toes or heels, rise from a squatting position and, while lying on your back, lift your legs one at a time. Pain that results from sciatica will usually worsen during these activities.
Your doctor may also want to test the following:
- Your gait – by asking you to walk
- Power of your legs
- Range of motion of your back and leg joints
- Reflexes
- Sensation
- Straight Leg Raising Test – this may reproduce your symptoms. Your doctor will ask you to keep your knee straight while bending your hip. He or she may also bend your ankle. Let your doctor know if you feel pain or numbness. The straight leg raising test is positive if there is pain on occurring on the same side of the body between 10 to 60 degrees. This test is quite sensitive (90%), but not specific. If this test elicits pain in the contralateral leg (occurring on the opposite side of the body), one should suspect disc herniation and order an imaging test. MRI is very useful when the exact level of compression in the spine is unclear. MRI can also assess the soft tissues or presence of an infection or a neoplastic cause. If there is urine retention or dysesthesia (painful burning, prickling, or aching feeling) around the anus in a patient with sciatica, one should suspect cauda equina syndrome. Prompt surgical decompression is indicated for this disorder.
Imaging tests
Many people have herniated discs or bone spurs that will show up on X-rays and other imaging tests but have no symptoms. So doctors don’t typically order these tests unless your pain is severe, or it doesn’t improve within a few weeks.
To further investigate the cause of your sciatica, your doctor may suggest a few tests including 18, 19:
- X-ray. An X-ray of your spine may reveal an overgrowth of bone (bone spur) that may be pressing on a nerve.
- MRI scan. This procedure uses a powerful magnet and radio waves to produce cross-sectional images of your back. An MRI produces detailed images of bone and soft tissues such as herniated disks. During the test, you lie on a table that moves into the MRI machine.
- CT scan. When a CT is used to image the spine, you may have a contrast dye injected into your spinal canal before the X-rays are taken — a procedure called a CT myelogram. The dye then circulates around your spinal cord and spinal nerves, which appear white on the scan.
- Electromyography (EMG). This test measures the electrical impulses produced by the nerves and the responses of your muscles. This test can confirm nerve compression caused by herniated disks or narrowing of your spinal canal (spinal stenosis).
Sciatica treatment
For most people (80 to 90% of patients with sciatica), sciatica responds to self-care measures 3. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, aspirin, or naproxen, or muscle relaxants may offer relief. You may find it soothing to put gentle heat or cold on your painful muscles. You are encouraged to return to your normal daily activities as soon as possible. Although resting for a day or so may provide some relief, prolonged inactivity will make your signs and symptoms worse. Bed rest has not been found to improve the symptoms of sciatica and instead may worsen the pain. There are also physical exercises you can do to improve your strength and range of movements.
If your sciatica pain doesn’t improve with self-care measures, your doctor might suggest some of the following treatments.
Sciatic nerve pain relief
Sciatica usually gets better in 4 to 6 weeks, but it can sometimes last longer. To help relieve your pain and speed up recovery:
- DO
- carry on with your normal activities as much as possible
- regular exercises for sciatica
- start gentle exercise as soon as you can – anything that gets you moving can help
- hold heat packs to the painful areas – you can buy these from pharmacies
- ask your pharmacist about painkillers (acetaminophen [paracetamol], non-steroidal anti-inflammatory drugs (NSAIDs) may help with sciatica)
- put a small, firm cushion between your knees when sleeping on your side, or several firm pillows underneath your knees when lying on your back
- DON’T
- do not sit or lie down for long periods – even if moving hurts, it’s not harmful and can help you get better faster
- do not use hot water bottles to ease the pain – you could scald yourself if your skin is numb
Exercises for sciatica
Many people find relief with gentle basic exercises. The exercises should not increase pain in the sciatic nerve and should be performed slowly. Some sciatic pain improves with McKenzie exercises or extension exercises. Others respond to flexion exercises to decrease pain from the sciatic nerve.
There are 4 simple stretches that can help with sciatica. They are are easy to do at home in bed or on a yoga mat on the floor. The 4 exercises include:
- Double Knee to Chest: Lying flat on your back, take both your hands and place them on top of your lower leg below the knee. Next, gently pull your knee to your chest in a controlled manner. Hold 10 seconds, repeat 3 times. This helps stretch the lower back gently.
- Prone on Elbows: Lay on your stomach and keep your hips flat to the table. Next, press your upper trunk up until you can place both elbows under each shoulder. Hold 5 seconds, repeat 10 times. This helps stretch the lower back.
- Lower Trunk Rotation: Lay on your back with the knees bent. Rotate the back to allow both legs to move together from side to side. Keep the shoulders flat on the surface. Hold 5 seconds, repeat 10 times on each side.
- Piriformis stretch: If the problem is a tight piriformis muscle, lie flat, cross the leg you want to stretch over the other leg, which is bent at a 90-degree angle. Reach down to the bent leg around the knee area and pull toward the opposite shoulder. You should feel a stretch in the buttock of the crossed leg. Again, hold 30 seconds and repeat two to three times. If pain increases, stop immediately. This is also an exercise for the hip for some with lower back and hip pain.
McKenzie back exercises are a series of exercises to help reduce pain in the spine. These exercises are based on putting the back into extension.
- Repeated Extension in Lying
- Repeated Extension in Lying (on elbows)
- Repeated Extension in Standing
- Neck Retraction
McKenzie’s exercises for the lower back often involves extension of the spine. This was a novel concept when it was first used. Before this, patients with back pain avoided extension movements for fear of aggravating the symptoms.
What if stretching exercises for sciatica do not help?
If simple lower back stretching exercises does not help sciatica pain, it is best to seek a medical professional help. In most cases, patients with lower back pain and sciatica will improve with physical therapy. If symptoms do not completely improve, spine physicians my order an MRI and consider steroid injections. In some rare cases, surgery may be needed to treat sciatica.
Sciatica pain treatment at home
Other self-care treatments that might help include:
- Cold packs. Initially, you might get relief from a cold pack placed on the painful area for up to 20 minutes several times a day. Use an ice pack or a package of frozen peas wrapped in a clean towel.
- Hot packs. After two to three days, apply heat to the areas that hurt. Use hot packs, a heat lamp or a heating pad on the lowest setting. If you continue to have pain, try alternating warm and cold packs.
- Stretching. Stretching exercises for your low back can help you feel better and might help relieve nerve root compression. Avoid jerking, bouncing or twisting during the stretch, and try to hold the stretch for at least 30 seconds.
- Over-the-counter medications. Pain relievers such as ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve) are sometimes helpful for sciatica.
- Do not do heavy lifting or twisting of your back for the first 6 weeks after the pain begins.
Alternative medicine
Alternative therapies commonly used for low back pain include:
- Acupuncture. In acupuncture, the practitioner inserts hair-thin needles into your skin at specific points on your body. Some studies have suggested that acupuncture can help back pain, while others have found no benefit. If you decide to try acupuncture, choose a licensed practitioner to ensure that he or she has had extensive training.
- Chiropractic. Spinal adjustment (manipulation) is one form of therapy chiropractors use to treat restricted spinal mobility. The goal is to restore spinal movement and, as a result, improve function and decrease pain. Spinal manipulation appears to be as effective and safe as standard treatments for low back pain.
Medications
The types of drugs that might be prescribed for sciatica pain include:
- Anti-inflammatories.
- Muscle relaxants
- Narcotics
- Tricyclic antidepressants
- Anti-seizure medications
It is reasonable that your doctor will put you on a trial of painkillers. The type of painkillers (acetaminophen [paracetamol], non-steroidal anti-inflammatory drugs (NSAIDs), opioids etc.) will depend on the severity of your pain and he or she may change the strength of painkillers as your symptoms change. You may also be prescribed muscle relaxants to reduce spasm of muscle around the nerve. This has shown to work for some people. It is important to discuss the side effects of these medications, if any, with your doctor.
Steroid injections
If the pain does not improve with oral medications, your doctor might recommend injection of a corticosteroid medication into the area around the involved nerve root (epidural corticosteroid injections) 20. This involves the injection of steroids into the space within the spinal cord that surrounds the nerves using a needle, around the lower back. Corticosteroids help reduce pain by suppressing inflammation around the irritated nerve. Studies have shown positive short-term effects for reducing pain in a proportion of people 21. The effects usually wear off in a few months. The number of steroid injections you can receive is limited because the risk of serious side effects increases when the injections occur too frequently.
Physical therapy
Once your acute pain improves, your doctor or a physical therapist can design a rehabilitation program to help you prevent future injuries. This typically includes exercises to correct your posture, strengthen the muscles supporting your back and improve your flexibility.
Surgery
Surgery is usually reserved for when the compressed sciatic nerve causes significant weakness, loss of bowel or bladder control, or when you have pain that progressively worsens or doesn’t improve with other therapies 5. Surgeons can remove the bone spur or the portion of the herniated disk that’s pressing on the pinched nerve.
Discectomy (surgery to remove all or part of the intervertebral disc) is a safe and effective procedure for patients with primary lumbar disc herniation and sciatica who do not respond to nonsurgical care or have severe and deteriorating symptoms 22. The current evidence is consistently in favor of discectomy, rather than continuing nonsurgical care, for greater and/or faster alleviation of pain, reduction of disability, and higher patient satisfaction 22. Clinical evidence indicates that microtubular discectomy and endoscopic discectomy result in reduced incision size, soft tissue damage, and hospital stay and yield similar improvements in symptoms compared to open discectomy. Currently, evidence-based clinical recommendations for annular repair after discectomy do not exist. Patients who are indicated for discectomy and have a large annular defect are exposed to a greater risk of symptom recurrence and revision surgery and may benefit from annular repair. Current level 1 evidence demonstrates that, in appropriately selected patient populations, implantation of a bone-anchored annular closure device reduces the risk of symptom recurrence and revision surgery compared to discectomy alone 22. The current evidence supports the use of discectomy as well as consideration for bone-anchored annular repair for the treatment of indicated patients with primary symptomatic lumbar disc herniation who may otherwise be at higher risk for recurrent disc herniation.
Sciatica prognosis
In general the clinical course of acute sciatica is favourable and most cases of sciatica pain and related disability resolves in less than 4 to 6 weeks with no long-term complications even if no medical therapy is sought 23. In more severe cases or cases where the neurologic deficit is present, the patient may have a more prolonged course of recovery. However, recovery is still excellent. For example, in a randomized trial that compared non-steroidal anti-inflammatory drugs with placebo for acute sciatica in primary care 60% of the patients recovered within three months and 70% within 12 months 24. About 50% of patients with acute sciatica included in placebo groups in randomized trials of non-surgical interventions reported improvement within 10 days and about 75% reported improvement after four weeks 25. In most patients therefore the prognosis is good, but at the same time a substantial proportion (up to 30%) continues to have pain for one year or longer 26. Some studies have shown that poor occupational mechanics, psychological depression, and poor socioeconomic situations lead to an increased chance of chronic, recurrent sciatica.
- Koes BW, van Tulder MW, Peul WC. Diagnosis and treatment of sciatica. BMJ. 2007 Jun 23;334(7607):1313-7. doi: 10.1136/bmj.39223.428495[↩]
- IASP. Part I Topics and Codes. In: Mersky H, Bogduk N editor(s). Classification of Chronic Pain. 2nd Edition. Seattle, WA: IASP Press, 1994.[↩]
- Valat JP, Genevay S, Marty M, Rozenberg S, Koes B. Sciatica. Best Pract Res Clin Rheumatol. 2010 Apr;24(2):241-52. doi: 10.1016/j.berh.2009.11.005[↩][↩]
- van Tulder M, Peul W, Koes B. Sciatica: what the rheumatologist needs to know. Nat Rev Rheumatol. 2010 Mar;6(3):139-45. doi: 10.1038/nrrheum.2010.3[↩]
- Jacobs WC, van Tulder M, Arts M, Rubinstein SM, van Middelkoop M, Ostelo R, Verhagen A, Koes B, Peul WC. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review. Eur Spine J. 2011 Apr;20(4):513-22. doi: 10.1007/s00586-010-1603-7[↩][↩]
- Konstantinou K, Dunn KM. Sciatica: review of epidemiological studies and prevalence estimates. Spine (Phila Pa 1976). 2008 Oct 15;33(22):2464-72. doi: 10.1097/BRS.0b013e318183a4a2[↩]
- Gibson JN, Waddell G. Surgical interventions for lumbar disc prolapse. Cochrane Database Syst Rev. 2007 Apr 18;2007(2):CD001350. doi: 10.1002/14651858.CD001350.pub4[↩][↩]
- Capurro, Bruno & Tey, Marc & Monllau, Juan & Carrera, Ana & Marqués, Fernando & de la Torre, Francisco. (2021). Anatomic Landmarks for a Safe Arthroscopic Approach to the Deep Gluteal Space: A Cadaveric Study Hitos Anatómicos para un Abordaje Artroscópico Seguro del Espacio Glúteo Profundo: Un Estudio Cadavérico. International Journal of Insect Morphology and Embryology. 359-365. https://www.researchgate.net/profile/Fernando-Marques-9/publication/350399906_Anatomic_Landmarks_for_a_Safe_Arthroscopic_Approach_to_the_Deep_Gluteal_Space_A_Cadaveric_Study_Hitos_Anatomicos_para_un_Abordaje_Artroscopico_Seguro_del_Espacio_Gluteo_Profundo_Un_Estudio_Cadaverico/links/605da5e2458515e83470780a/Anatomic-Landmarks-for-a-Safe-Arthroscopic-Approach-to-the-Deep-Gluteal-Space-A-Cadaveric-Study-Hitos-Anatomicos-para-un-Abordaje-Artroscopico-Seguro-del-Espacio-Gluteo-Profundo-Un-Estudio-Cadaverico.pdf[↩]
- Eastlack J, Tenorio L, Wadhwa V, Scott K, Starr A, Chhabra A. Sciatic neuromuscular variants on MR neurography: frequency study and interobserver performance. Br J Radiol. 2017 Nov;90(1079):20170116. doi: 10.1259/bjr.20170116[↩][↩]
- Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2021 Jul 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482431[↩][↩][↩]
- Siddiq MAB. Piriformis Syndrome and Wallet Neuritis: Are They the Same? Cureus. 2018 May 10;10(5):e2606. doi: 10.7759/cureus.2606[↩][↩][↩]
- Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr, Shekelle P, Owens DK; Clinical Efficacy Assessment Subcommittee of the American College of Physicians; American College of Physicians; American Pain Society Low Back Pain Guidelines Panel. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007 Oct 2;147(7):478-91. https://doi.org/10.7326/0003-4819-147-7-200710020-00006[↩]
- Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. Br J Anaesth. 2007 Oct;99(4):461-73. https://www.bjanaesthesia.org/article/S0007-0912(17)35461-2/fulltext[↩]
- Boyajian-O’Neill LA, McClain RL, Coleman MK, Thomas PP. Diagnosis and management of piriformis syndrome: an osteopathic approach. J Am Osteopath Assoc. 2008 Nov;108(11):657-64. doi: 10.7556/jaoa.2008.108.11.657[↩]
- Siddiq MA, Hossain MS, Uddin MM, Jahan I, Khasru MR, Haider NM, Rasker JJ. Piriformis syndrome: a case series of 31 Bangladeshi people with literature review. Eur J Orthop Surg Traumatol. 2017 Feb;27(2):193-203. doi: 10.1007/s00590-016-1853-0[↩]
- Snyder MJ, Hawks MK, Moss DA, Crawford PF 3rd. Integrative Medicine: Manual Therapy. FP Essent. 2021 Jun;505:11-17.[↩]
- Anni E. Rivinoja, Markus V. Paananen, Simo P. Taimela, Svetlana Solovieva, Annaleena Okuloff, Paavo Zitting, Marjo-Riitta Järvelin, Päivi Leino-Arjas, Jaro I. Karppinen, Sports, Smoking, and Overweight During Adolescence as Predictors of Sciatica in Adulthood: A 28-Year Follow-up Study of a Birth Cohort, American Journal of Epidemiology, Volume 173, Issue 8, 15 April 2011, Pages 890–897, https://doi.org/10.1093/aje/kwq459[↩]
- Jensen TS, Albert HB, Soerensen JS, Manniche C, Leboeuf-Yde C. Natural course of disc morphology in patients with sciatica: an MRI study using a standardized qualitative classification system. Spine (Phila Pa 1976). 2006 Jun 15;31(14):1605-12; discussion 1613. doi: 10.1097/01.brs.0000221992.77779.37[↩]
- Bartret AL, Beaulieu CF, Lutz AM. Is it painful to be different? Sciatic nerve anatomical variants on MRI and their relationship to piriformis syndrome. Eur Radiol. 2018 Nov;28(11):4681-4686. doi: 10.1007/s00330-018-5447-6[↩]
- Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. Br J Anaesth. 2007 Oct;99(4):461-73. https://doi.org/10.1093/bja/aem238[↩]
- Oliveira CB, Maher CG, Ferreira ML, Hancock MJ, Oliveira VC, McLachlan AJ, Koes BW, Ferreira PH, Cohen SP, Pinto RZ. Epidural corticosteroid injections for lumbosacral radicular pain. Cochrane Database Syst Rev. 2020 Apr 9;4(4):CD013577. doi: 10.1002/14651858.CD013577[↩]
- Lorio M, Kim C, Araghi A, Inzana J, Yue JJ. International Society for the Advancement of Spine Surgery Policy 2019-Surgical Treatment of Lumbar Disc Herniation with Radiculopathy. Int J Spine Surg. 2020 Feb 29;14(1):1-17. doi: 10.14444/7001[↩][↩][↩]
- Davis D, Maini K, Vasudevan A. Sciatica. [Updated 2022 May 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507908[↩]
- Weber H, Holme I, Amlie E. The natural course of acute sciatica with nerve root symptoms in a double-blind placebo-controlled trial evaluating the effect of piroxicam. Spine (Phila Pa 1976). 1993 Sep 1;18(11):1433-8.[↩]
- Vroomen PC, de Krom MC, Slofstra PD, Knottnerus JA. Conservative treatment of sciatica: a systematic review. J Spinal Disord. 2000 Dec;13(6):463-9. doi: 10.1097/00002517-200012000-00001[↩]
- Koes BW, van Tulder MW, Peul WC. Diagnosis and treatment of sciatica. BMJ. 2007 Jun 23;334(7607):1313-7. doi: 10.1136/bmj.39223.428495.BE[↩]





{kind=link}