

Contents
- What is Selenium
- Selenium Benefits
- Selenium and Cancer
- Should men take vitamin E or selenium supplements for cancer prevention ? 20
- Why didn’t the selenium supplement in SELECT prevent prostate cancer ? 27
- Selenium and Cancer Prevention
- How much selenium do you need ?
- What foods provide selenium ?
- Table 2: Selected Food Sources of Selenium
- Are you getting enough selenium ?
- What happens if you don’t get enough selenium ?
- Health Risks from Excessive Selenium
- What are some effects of selenium on health ?
- Selenium and healthy eating
What is Selenium
Selenium is a trace element that is naturally present in many foods, added to others, and available as a dietary supplement. Selenium, which is nutritionally essential for humans, is a constituent of more than two dozen selenoproteins that play critical roles in reproduction, thyroid hormone metabolism, DNA synthesis, and protection from oxidative damage and infection 1.
Selenium exists in two forms:
- inorganic (selenate and selenite) and
- organic (selenomethionine and selenocysteine) 2.
Both forms can be good dietary sources of selenium 3. Soils contain inorganic selenites and selenates that plants accumulate and convert to organic forms, mostly selenocysteine and selenomethionine and their methylated derivatives.
Most selenium is in the form of selenomethionine in animal and human tissues, where it can be incorporated nonspecifically with the amino acid methionine in body proteins. Skeletal muscle is the major site of selenium storage, accounting for approximately 28% to 46% of the total selenium pool 3. Both selenocysteine and selenite are reduced to generate hydrogen selenide, which in turn is converted to selenophosphate for selenoprotein biosynthesis 4.
The most commonly used measures of selenium status are plasma and serum selenium concentrations 1. Concentrations in blood and urine reflect recent selenium intake. Analyses of hair or nail selenium content can be used to monitor longer-term intakes over months or years. Quantification of one or more selenoproteins (such as glutathione peroxidase and selenoprotein P) is also used as a functional measure of selenium status 3. Plasma or serum selenium concentrations of 8 micrograms (mcg)/dL or higher in healthy people typically meet needs for selenoprotein synthesis 5.
Selenium Benefits
Selenium is a nutrient that the body needs to stay healthy. Selenium is important for reproduction, thyroid gland function, DNA production, and protecting the body from damage caused by free radicals and from infection 6, 7. Selenium is incorporated into selenoproteins that have a wide range of pleiotropic effects, ranging from antioxidant and anti-inflammatory effects to the production of active thyroid hormone 8. In the past 10 years, the discovery of disease-associated polymorphisms in selenoprotein genes has drawn attention to the relevance of selenoproteins to health. Low selenium status has been associated with increased risk of mortality, poor immune function, and cognitive decline. Higher selenium status or selenium supplementation has antiviral effects, is essential for successful male and female reproduction, and reduces the risk of autoimmune thyroid disease. Prospective studies have generally shown some benefit of higher selenium status on the risk of prostate, lung, colorectal, and bladder cancers, but findings from trials have been mixed, which probably emphasises the fact that supplementation will confer benefit only if intake of a nutrient is inadequate. Supplementation of people who already have adequate intake with additional selenium might increase their risk of type-2 diabetes. The crucial factor that needs to be emphasised with regard to the health effects of selenium is the inextricable U-shaped link with status; whereas additional selenium intake may benefit people with low status, those with adequate-to-high status might be affected adversely and should not take selenium supplements.
Selenium and Cancer
There have been numerous animal studies indicating the important role of selenium in reducing and preventing the incidence of cancer initiated by a variety of carcinogens, including chemicals and radiation. These findings from animal studies have led to significant interest in the investigation of the role of selenium as a chemoprevention in humans. Evidence from human epidemiological studies has increasingly indicated a inverse relationship between selenium status and cancer risk in human populations. The hallmark study of Clark and colleagues 9 reported that people who supplemented their diet with selenized yeast, predominantly in the form of selenomethionine (200 μg/day), did not protect against development of basal or squamous cell carcinomas of the skin, but had a reduction of nearly 50% in overall reduced the incidence of, and mortality from, carcinomas of several sites. This study, designed as a randomised, double-blind and placebo controlled trial, also showed low incidence of prostate, lung and colon cancers. Subsequent epidemiological studies by other researchers have obtained inconclusive findings on the relationship between selenium status and the incidence of some forms of cancer, particularly prostate cancer. In a prospective study of case-control design, high toenail selenium levels were associated with a reduced risk of advanced prostate cancer 10. In another study, no association was observed between toenail selenium levels and breast cancer in women or prostate cancer in men 11. These investigators suggested that the effects of smoking and dietary habits of the subjects could have contributed to these inconclusive findings. In a British study, the levels of selenium in fingernails and the risk of prostate cancer in men also did not show any correlation 12. Similarly, a recent study also showed that the overall serum Se level was not associated with prostate cancer risk in a large cohort study of nested case-control design 13. However, when the data were analysed to include high intake of vitamin E, multivitamin and smoking by these men, there were associations between serum selenium concentrations and reduced prostate cancer risks. A recent meta-analysis also indicated a possible inverse association between selenium levels and risk of prostate cancer 14. A larger prospective study, the selenium and vitamin E chemoprevention trial (SELECT) involving 32,400 healthy North American men, was started in 2001 and is to be completed in 2013. This study is designed as a randomised, double-blind, and placebo-controlled trial to determine the effect of selenium and vitamin E, individually and in combination, on the incidence of prostate cancer 15, 16.
SELECT was a randomized, controlled clinical trial. The men who participated took two capsules a day. They were randomly assigned (that is, assigned by chance) to receive:
- Selenium and vitamin E
- Selenium and a placebo
- Vitamin E and a placebo, or
- Two placebos. Two placebos were used in the trial: one looked like a selenium capsule; the other looked like a vitamin E capsule. Each placebo contained only inactive ingredients. Neither the participants nor the researchers knew who received the selenium and vitamin E, or the placebos, a process known as blinding or masking.
Who was eligible to participate in SELECT ? Were there restrictions on eligibility ?
African-American men had to be age 50 or older to participate, and men of other races and ethnicities had to be 55 or older. The age for eligibility was lower for African-American men because, on average, they develop prostate cancer at an earlier age and have an overall increased risk of developing prostate cancer.
Many diseases, including prostate cancer, occur more frequently in older persons. The risk of developing prostate cancer increases with age. More than 90 percent of prostate cancer cases occur in men age 55 or older 17.
The updated results of SELECT published in 2011 18 : the data published in 2011 include 18 months of additional follow-up information on the participants through July 5, 2011. During this time, SELECT men were no longer taking study supplements. These additional data provide an average of seven years of information on the participants: 5.5 years taking study supplements plus 1.5 years of observation or follow-up.
- The additional data show that the men who took vitamin E alone had a 17 percent relative increase in numbers of prostate cancers compared to men on placebo.
- This difference in prostate cancer incidence between the vitamin E only group and the placebos only group is now statistically significant, and not likely to be due to chance.
- Men taking selenium alone, or vitamin E and selenium, were also more likely to develop prostate cancer than men taking placebo, but those increases were smaller and are not statistically significant and may be due to chance. Updated results of SELECT were published in JAMA on October 12, 2011 19.
Should men take vitamin E or selenium supplements for cancer prevention ? 20
No. Scientists do not understand how these supplements really work and more importantly, the interactions that these supplements have together or with foods, drugs, or other supplements. There are no clinical trials that show a benefit from taking vitamin E or selenium to reduce the risk of prostate cancer or any other cancer or heart disease 21, 19, 22, 23, 24, 25, 26. While the men in SELECT who took both vitamin E and selenium did not have a statistically significant increase in their risk for prostate cancer, they also did not have a reduced risk of prostate cancer or any other cancer or heart disease. SELECT researchers were surprised by the findings in the men who took both vitamin E and selenium, and while the 2014 analysis suggests possible reasons for the findings, the mechanism remains unclear.
Why didn’t the selenium supplement in SELECT prevent prostate cancer ? 27
Researchers don’t know why. There are several possible explanations why selenium supplements did not prevent prostate cancer in men on SELECT. These reasons include:
- The findings of reduced prostate cancer incidence associated with selenium supplementation in the Nutritional Prevention of cancer (NPC) study may not have been correct and selenium may not affect prostate cancer risk.
- The participants in the Nutritional Prevention of cancer (NPC) study were deficient in selenium compared to the men in SELECT who were not selected because of a likely selenium-deficiency; it may be that selenium only reduces the risk of prostate cancer in selenium-deficient men and not in the general population.
- The supplements given to the men in SELECT may have exceeded the best dose to prevent prostate cancer.
- The formulation of selenium used in the NPC trial (high-selenium yeast) may have been more active than the l-selenomethionine used in SELECT and this may have prevented researchers from seeing a cancer prevention effect. Arguing against this was the fact that early tests showed that, for the selenium yeast, the amount of selenium per dose varied in the NPC trial – this was why this form of selenium was not used in SELECT. Additionally, the inorganic compounds present in the yeast can be toxic and can lead to lower body reserves of selenium. The SELECT biorepository data and samples will help to support research that may answer this question.
Did the researchers find any difference in the effect of the supplements based on the level of vitamin E or selenium in participants when they joined the trial ? 28
Yes. In an analysis published in 2014, men who had high levels of selenium at the start of the trial, as assessed by measures of selenium in their toenail clippings, had almost double the chance of developing a high-grade prostate cancer if they took the selenium supplement compared to men with low levels of selenium at the start of the trial. This finding was unexpected, as previous studies had shown that men with low levels of selenium had an increased risk of prostate cancer that was reduced with supplements 29, 30. Additionally, men with low levels of selenium at the start of the trial had double the chance of developing a high-grade prostate cancer if they took the vitamin E supplement.
Did the African American men in SELECT have any different outcomes compared to the rest of the participants ?
Probably not, but the number of African American men in the trial is too small to be certain that separate analyses would be statistically sound. In SELECT, African American men were permitted to join the trial at a younger age than men of other races (at age 50 vs. 55) because of their increased risk of prostate cancer. About 12 percent of the participants (4,314 of 34,888) identified themselves as African-American, and they were represented equally across the study arms (as would be expected in a randomized trial). Although this percentage reflects the proportional representation of African Americans in the United States, the number of men is not large enough to do thorough, separate statistical analyses of each SELECT study endpoint. However, SELECT researchers did look at cancer rates and other measures by race and did not see any differences in the response to the supplements.
Do the new findings about the men’s selenium status help to explain the overall trial results better ?
Yes. In 2011, data showed that men taking vitamin E alone had a significantly increased risk of prostate cancer, but men taking vitamin E plus selenium did not. If men had low selenium levels at the start of the trial, the selenium supplement may have counteracted a negative effect of the vitamin E supplement.
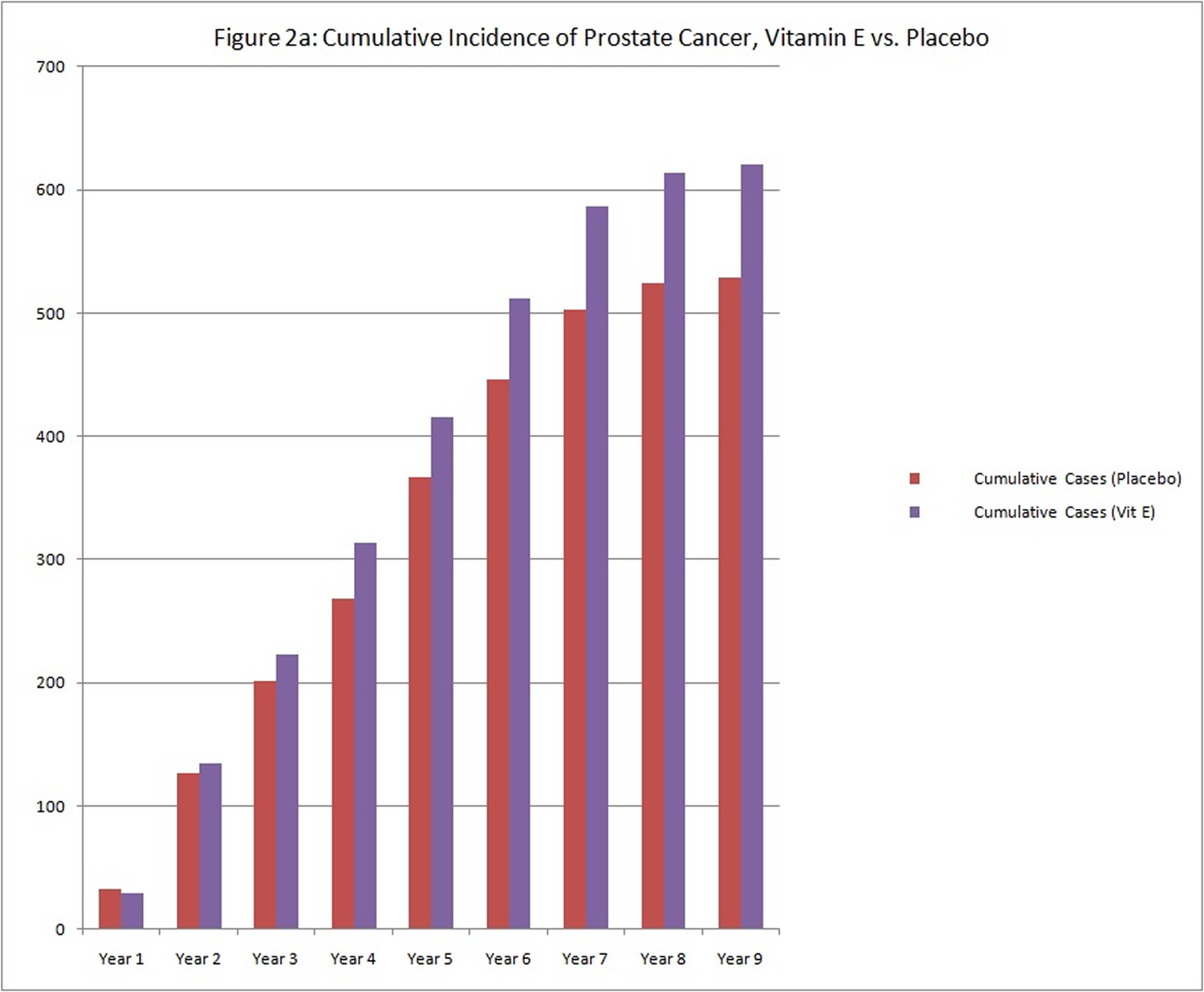
Why an increased risk for prostate cancer was found in 2011 SELECT results ?
As with many medications, the actions of vitamin E may last long after the last pill is taken. The differences in prostate cancer incidence between the vitamin E group and the placebo group began to emerge at about the third year of study supplementation (see graph below of cumulative cases).
The observation that the risk of prostate cancer has continued to increase suggests that vitamin E may have long-term effects on prostate cancer risk.
There continued to be no differences in the incidence of lung or colorectal cancers, all cancers combined, all deaths combined, or the overall incidence of cardiovascular events between the study groups. Although initial results showed that more men taking selenium were diagnosed with diabetes, longer follow-up showed no increased risk of this disease 31.
(Source 32))).
What does a 17 percent increased risk of prostate cancer in 2011 SELECT mean ?
In SELECT, this measure means that there were 17 percent more prostate cancer cases diagnosed in the group of men assigned to take 400 International Units (IU) of vitamin E (and no selenium) daily compared to the men taking two placebos (no vitamin E and no selenium) after an average of seven years — 5.5 of the years on supplements followed by 1.5 years not taking supplements.
In the men in SELECT who took only placebos, after seven years, 65 prostate cancer cases were diagnosed for every 1,000 men. For the men assigned to take vitamin E only, for every 1,000 men, there were 76 cases of prostate cancer diagnosed (11 additional cases of prostate cancer per 1,000 men over seven years).
What does a 17 percent increased risk of prostate cancer mean to men who take vitamin E but who were not SELECT participants ?
The incidence rate of prostate cancer in the placebo arm of SELECT is similar to the incidence rate for men in the U.S. age 65 and older 17. Thus, the estimate of increased risk for men of SELECT age taking vitamin E supplements of 400 IUs daily would be about the same as for the men on SELECT taking vitamin E only (i.e. about 17 percent).
In other words, if 1,000 men similar to those on SELECT were followed with annual physician visits, one would expect 65 of them to be diagnosed with prostate cancer over a seven year period. If these same men took 400 IUs of vitamin E daily for 5.5 years, researchers would expect 76 of them to be diagnosed with prostate cancer over a seven year period (i.e., 11 additional cases over seven years).
Why didn’t the vitamin E supplements prevent prostate cancer as expected ? Why did the men taking vitamin E have more prostate cancers ?
There are many reasons why the vitamin E supplements may not have prevented prostate cancer. Two of the most likely reasons look back at the Alpha-Tocopherol Beta Carotene (ATBC) Cancer Prevention trial, a study designed to test vitamin E and beta carotene for lung cancer prevention in smokers 33. In the Alpha-Tocopherol Beta Carotene (ATBC) Cancer Prevention trial, a reduction in prostate cancer incidence was observed, but this secondary finding may have been due to chance, as the study was not designed to determine prostate cancer risk. Another possible reason that men in Alpha-Tocopherol Beta Carotene (ATBC) Cancer Prevention trial had a reduction in prostate cancer incidence, while men on SELECT did not, is that the dose of vitamin E used in SELECT (400 IU/day) was higher than the dose used in the ATBC (50 IU/day). Researchers sometimes talk about a “U-shaped response curve” where very low or very high blood levels of a nutrient are harmful but more moderate levels are beneficial; while the Alpha-Tocopherol Beta Carotene (ATBC) Cancer Prevention trial dose may have been preventive, the SELECT dose may have been too large to have a prevention benefit.
Why did SELECT use a dose of 400 IU of vitamin E ? What form of vitamin E was used ?
At the time SELECT was being designed, trials to test vitamin E in other common diseases were also under way. These trials were studying 400 IU to 660 IU of vitamin E to prevent macular degeneration, Alzheimer’s disease, or heart disease. Preliminary evidence suggested the outcomes would be favorable. SELECT researchers matched the doses in these trials to ensure data at the 400 IU dose was available if using the supplement for other diseases became common.
The form of vitamin E given was dl-alpha tocopheryl acetate, the form of vitamin E found to reduce prostate cancer incidence in the Alpha-Tocopherol Beta Carotene (ATBC) Cancer Prevention trial.
Selenium and Cancer Prevention
In a Cochrane Review March 2014 34 that included 55 studies in which adults observed to have high or low selenium levels were followed over time to determine whether they developed cancer, along with eight trials in which adults were randomly assigned to receive selenium supplements or placebo.
Cochrane Review March 2014 34 found limited evidence suggesting that individuals observed to have higher selenium levels have a lower incidence of cancer. However, it is not possible to conclude from these studies that selenium was the reason for the lower cancer risk, because a high selenium level might be associated with other factors that reduce cancer risk, such as a healthier diet or lifestyle. Also, selenium comes in many different chemical forms that have different biological activity, and these studies did not identify which chemical forms were being measured. Selenium levels in body tissues in which people might develop cancer (e.g. the prostate) also were not examined.
The randomised controlled trials that assessed whether taking selenium supplements might prevent cancer differed considerably in methodological quality and are not equally reliable. Several studies reported that individuals receiving selenium supplements decreased their liver cancer risk, but these studies reported insufficient details about their randomisation process and participant follow-up to be convincing. Recent trials that were judged to be well conducted and reliable have found no effects of selenium on reducing the overall risk of cancer or on reducing the risk of particular cancers, including prostate cancer. In contrast, some trials suggest that selenium may increase the risk of non-melanoma skin cancer, as well as of type 2 diabetes, raising concern about the safety of selenium supplements.
Overall, no convincing evidence suggests that selenium supplements can prevent cancer. However, for a full understanding of the role of this metalloid in cancer development, more research is needed on how selenium may act differently in individuals with different genetic backgrounds or nutritional status, and on the different biological activities of the various selenium compounds, which are still largely unknown.
Although an inverse association between selenium exposure and the risk of some types of cancer was found in some observational studies, this cannot be taken as evidence of a causal relation, and these results should be interpreted with caution.
Double blind randomised clinical trials assessing the effects of selenium supplementation on cancer risk have yielded inconsistent results, although the most recent studies, characterised by a low risk of bias, found no beneficial effect on cancer risk, more specifically on risk of prostate cancer, as well as little evidence of any influence of baseline selenium status. Rather, some trials suggest harmful effects of selenium exposure. To date, no convincing evidence suggests that selenium supplements can prevent cancer in humans.
- Antioxidant supplements cannot be recommended for gastrointestinal cancer prevention
Cochrane Review 35 could not find convincing evidence that antioxidant supplements prevent gastrointestinal cancers. On the contrary, antioxidant supplements seem to increase overall mortality. The potential cancer preventive effect of selenium should be tested in adequately conducted randomised trials.
- Antioxidant supplements for preventing lung cancer in healthy people
Cochrane Review 36 concluded there is no evidence for recommending supplements of selenium, vitamins A, C, E either alone or in different combinations, for the prevention of lung cancer and lung cancer mortality in healthy people. There is some evidence that the use of beta-carotene supplements could be associated with a small increase in lung cancer incidence and mortality in smokers or persons exposed to asbestos.
How much selenium do you need ?
Intake recommendations for selenium and other nutrients are provided in the Dietary Reference Intakes (DRIs) developed by the Food and Nutrition Board (FNB) at the Institute of Medicine of the National Academies (formerly National Academy of Sciences) 37. DRI is the general term for a set of reference values used for planning and assessing nutrient intakes of healthy people. These values, which vary by age and sex, include:
- Recommended Dietary Allowance (RDA): average daily level of intake sufficient to meet the nutrient requirements of nearly all (97%–98%) healthy individuals.
- Adequate Intake (AI): established when evidence is insufficient to develop an RDA and is set at a level assumed to ensure nutritional adequacy.
- Estimated Average Requirement (EAR): average daily level of intake estimated to meet the requirements of 50% of healthy individuals. It is usually used to assess the adequacy of nutrient intakes in population groups but not individuals.
- Tolerable Upper Intake Level (UL): maximum daily intake unlikely to cause adverse health effects.
Table 1 lists the current RDAs for selenium in mcg. For infants from birth to 12 months, the Food and Nutrition Board established an AI for selenium that is equivalent to the mean intake of selenium in healthy, breastfed infants.
Table 1: The amount of selenium that you need each day depends on your age. Average daily recommended amounts are listed below in micrograms (mcg).
| Life Stage | Recommended Amount |
|---|---|
| Birth to 6 months | 15 mcg |
| Infants 7–12 months | 20 mcg |
| Children 1–3 years | 20 mcg |
| Children 4–8 years | 30 mcg |
| Children 9–13 years | 40 mcg |
| Teens 14–18 years | 55 mcg |
| Adults 19–50 years | 55 mcg |
| Adults 51–70 years | 55 mcg |
| Adults 71 years and older | 55 mcg |
| Pregnant teens and women | 60 mcg |
| Breastfeeding teens and women | 70 mcg |
*Adequate Intake (AI)
What foods provide selenium ?
Seafoods and organ meats are the richest food sources of selenium 1. Other sources include muscle meats, cereals and other grains, and dairy products. The amount of selenium in drinking water is not nutritionally significant in most geographic regions 2, 37. The major food sources of selenium in the American diet are breads, grains, meat, poultry, fish, and eggs 38.
The amount of selenium in a given type of plant-based food depends on the amount of selenium in the soil and several other factors, such as soil pH, amount of organic matter in the soil, and whether the selenium is in a form that is amenable to plant uptake 2, 37, 39, 40. As a result, selenium concentrations in plant-based foods vary widely by geographic location 1, 2. For example, according to the U.S. Department of Agriculture Food Composition Database, Brazil nuts have 544 mcg selenium/ounce, but values from other analyses vary widely 41, 42, 43.
The selenium content of soil affects the amounts of selenium in the plants that animals eat, so the quantities of selenium in animal products also vary 2, 5. However, selenium concentration in soil has a smaller effect on selenium levels in animal products than in plant-based foods because animals maintain predictable tissue concentrations of selenium through homeostatic mechanisms. Furthermore, formulated livestock feeds generally contain the same levels of selenium.
Several food sources of selenium are listed in Table 2.
| Food | Micrograms (mcg) per serving | Percent DV* |
|---|---|---|
| Brazil nuts, 1 ounce (6–8 nuts) | 544 | 777 |
| Tuna, yellowfin, cooked, dry heat, 3 ounces | 92 | 131 |
| Halibut, cooked, dry heat, 3 ounces | 47 | 67 |
| Sardines, canned in oil, drained solids with bone, 3 ounces | 45 | 64 |
| Ham, roasted, 3 ounces | 42 | 60 |
| Shrimp, canned, 3 ounces | 40 | 57 |
| Macaroni, enriched, cooked, 1 cup | 37 | 53 |
| Beef steak, bottom round, roasted, 3 ounces | 33 | 47 |
| Turkey, boneless, roasted, 3 ounces | 31 | 44 |
| Beef liver, pan fried, 3 ounces | 28 | 40 |
| Chicken, light meat, roasted, 3 ounces | 22 | 31 |
| Cottage cheese, 1% milkfat, 1 cup | 20 | 29 |
| Rice, brown, long-grain, cooked, 1 cup | 19 | 27 |
| Beef, ground, 25% fat, broiled, 3 ounces | 18 | 26 |
| Egg, hard-boiled, 1 large | 15 | 21 |
| Puffed wheat ready-to-eat cereal, fortified, 1 cup | 15 | 21 |
| Bread, whole-wheat, 1 slice | 13 | 19 |
| Baked beans, canned, plain or vegetarian, 1 cup | 13 | 19 |
| Oatmeal, regular and quick, unenriched, cooked with water, 1 cup | 13 | 19 |
| Spinach, frozen, boiled, 1 cup | 11 | 16 |
| Milk, 1% fat, 1 cup | 8 | 11 |
| Yogurt, plain, low fat, 1 cup | 8 | 11 |
| Lentils, boiled, 1 cup | 6 | 9 |
| Bread, white, 1 slice | 6 | 9 |
| Spaghetti sauce, marinara, 1 cup | 4 | 6 |
| Cashew nuts, dry roasted, 1 ounce | 3 | 4 |
| Corn flakes, 1 cup | 2 | 3 |
| Green peas, frozen, boiled, 1 cup | 2 | 3 |
| Bananas, sliced, 1 cup | 2 | 3 |
| Potato, baked, flesh and skin, 1 potato | 1 | 1 |
| Peaches, canned in water, solids and liquids, 1 cup | 1 | 1 |
| Carrots, raw, 1 cup | 0 | 0 |
| Lettuce, iceberg, raw, 1 cup | 0 | 0 |
*DV = Daily Value. DVs were developed by the U.S. Food and Drug Administration (FDA) to help consumers compare the nutrient contents of products within the context of a total diet. The DV for selenium is 70 mcg for adults and children aged 4 and older. Foods providing 20% or more of the DV are considered to be high sources of a nutrient. The U.S. Department of Agriculture’s (USDA’s) Nutrient Database Web site 44 lists the nutrient content of many foods and provides a comprehensive list of foods containing selenium arranged by nutrient content and by food name.
[Source 45]Selenium is found naturally in many foods. The amount of selenium in plant foods depends on the amount of selenium in the soil where they were grown. The amount of selenium in animal products depends on the selenium content of the foods that the animals ate. You can get recommended amounts of selenium by eating a variety of foods, including the following:
- Seafood
- Meat, poultry, eggs, and dairy products
- Breads, cereals, and other grain products
Are you getting enough selenium ?
Most Americans get enough selenium from their diet because they eat food grown or raised in many different areas, including areas with soil that is rich in selenium. According to an analysis of data from the 2009–2010 National Health and Nutrition Examination Survey (NHANES), the average daily selenium intake in Americans aged 2 years and older from foods is 108.5 mcg and from both foods and supplements is 120.8 mcg 46. Adult men have higher daily intakes (134 mcg from foods and 151 mcg from foods and supplements) than adult women (93 mcg from foods and 108 mcg from foods and supplements). In the United States, 18% to 19% of adults and children use a dietary supplement containing selenium 47.
Certain groups of people are more likely than others to have trouble getting enough selenium:
- People undergoing kidney dialysis
- People living with HIV
- People who eat only local foods grown in soils that are low in selenium
What happens if you don’t get enough selenium ?
Selenium deficiency is very rare in America. Selenium deficiency produces biochemical changes that might predispose people who experience additional stresses to develop certain illnesses 37. For example, selenium deficiency in combination with a second stress (possibly a viral infection) leads to Keshan disease, a cardiomyopathy that occurred in parts of China prior to a government-sponsored selenium supplementation program that began in the 1970s 2, 5, 39, 48. Before the Chinese government supplementation program, adults in the Keshan disease areas had average selenium intakes of no more than 11 mcg/day; intakes of at least 20 mcg/day protect adults from Keshan disease 49.
Selenium deficiency is also associated with male infertility and might play a role in Kashin-Beck disease, a type of osteoarthritis that occurs in certain low-selenium areas of China, Tibet, and Siberia 1, 2, 5, 37, 39, 50. Selenium deficiency could exacerbate iodine deficiency, potentially increasing the risk of cretinism in infants 2, 5.
What kinds of selenium dietary supplements are available ?
Selenium is available in multivitamin/multimineral supplements and as a stand-alone supplement, often in the forms of selenomethionine or of selenium-enriched yeast (grown in a high-selenium medium) or as sodium selenite or sodium selenate 2, 5, 37. The human body absorbs more than 90% of selenomethionine but only about 50% of selenium from selenite37.
Few studies have compared the relative absorption and bioavailability of different forms of selenium. In one investigation, 10 groups of selenium-replete subjects were randomly assigned to receive a placebo or either 200 or 600 mcg/day selenium as selenomethionine, sodium selenite, or high-selenium yeast (in which an estimated 75% of selenium was in the form of selenomethionine) for 16 weeks 51. Selenium bioavailability, based on urinary excretion, was greatest for selenomethionine and lowest for selenite. However, supplementation with any of these forms only affected plasma selenium levels and not glutathione peroxidase activity or selenoprotein P concentration, confirming that study participants were selenium replete before they began taking selenium supplements.
Health Risks from Excessive Selenium
Chronically high intakes of the organic and inorganic forms of selenium have similar effects 37. Early indicators of excess intake are a garlic odor in the breath and a metallic taste in the mouth. The most common clinical signs of chronically high selenium intakes, or selenosis, are hair and nail loss or brittleness. Other symptoms include lesions of the skin and nervous system, nausea, diarrhea, skin rashes, mottled teeth, fatigue, irritability, and nervous system abnormalities.
As discussed earlier, Brazil nuts contain very high amounts of selenium (68–91 mcg per nut) and could cause selenium toxicity if consumed regularly. Acute selenium toxicity has resulted from the ingestion of misformulated over-the-counter products containing very large amounts of selenium 2, 5. In 2008, for example, 201 people experienced severe adverse reactions from taking a liquid dietary supplement containing 200 times the labeled amount 52. Acute selenium toxicity can cause severe gastrointestinal and neurological symptoms, acute respiratory distress syndrome, myocardial infarction, hair loss, muscle tenderness, tremors, lightheadedness, facial flushing, kidney failure, cardiac failure, and, in rare cases, death 2, 37.
The FNB has established ULs for selenium from food and supplements based on the amounts of selenium that are associated with hair and nail brittleness and loss (see Table 3) 37.
| Age | Male | Female | Pregnancy | Lactation |
|---|---|---|---|---|
| Birth to 6 months | 45 mcg | 45 mcg | ||
| 7–12 months | 60 mcg | 60 mcg | ||
| 1–3 years | 90 mcg | 90 mcg | ||
| 4–8 years | 150 mcg | 150 mcg | ||
| 9–13 years | 280 mcg | 280 mcg | ||
| 14–18 years | 400 mcg | 400 mcg | 400 mcg | 400 mcg |
| 19+ years | 400 mcg | 400 mcg | 400 mcg | 400 mcg |
*Breast milk, formula, and food should be the only sources of selenium for infants.
What are some effects of selenium on health ?
Scientists are studying selenium to understand how it affects health. Here are some examples of what this research has shown.
- Cancer
Studies suggest that people who consume lower amounts of selenium could have an increased risk of developing cancers of the colon and rectum, prostate, lung, bladder, skin, esophagus, and stomach. But whether selenium supplements reduce cancer risk is not clear. More research is needed to understand the effects of selenium from food and dietary supplements on cancer risk. - Cardiovascular disease
Scientists are studying whether selenium helps reduce the risk of cardiovascular disease. Some studies show that people with lower blood levels of selenium have a higher risk of heart disease, but other studies do not. More studies are needed to better understand how selenium in food and dietary supplements affects heart health.
Selenoproteins help prevent the oxidative modification of lipids, reducing inflammation and preventing platelets from aggregating 40. For these reasons, experts have suggested that selenium supplements could reduce the risk of cardiovascular disease or deaths associated with cardiovascular disease.
The epidemiological data on the role of selenium in cardiovascular disease have yielded conflicting conclusions. Some observational studies have found an inverse association between serum selenium concentrations and risk of hypertension or coronary heart disease. A meta-analysis of 25 observational studies found that people with lower selenium concentrations had a higher risk of coronary heart disease 53. However, other observational studies failed to find statistically significant links between selenium concentrations and risk of heart disease or cardiac death, or they found that higher selenium concentrations are associated with an increased risk of cardiovascular disease 54, 55, 56.
Several clinical trials have examined whether selenium supplementation reduces the risk of cardiovascular disease. In one randomized, placebo-controlled study, for example, 474 healthy adults aged 60 to 74 years with a mean baseline plasma selenium concentration of 9.12 mcg/dL were supplemented with 100, 200, or 300 mcg selenium per day or placebo for 6 months 57. The supplements lowered levels of total plasma cholesterol and non–high-density-lipoprotein (HDL) plasma cholesterol (total cholesterol levels minus HDL levels) compared with the placebo group, whereas the 300 mcg/day dose significantly increased HDL levels. Other trials have provided evidence that selenium supplementation (200 mcg/day) or supplementation with a multivitamin/multimineral pill containing selenium (100 mcg/day) does not reduce the risk of cardiovascular disease or cardiac death 58, 59, 60. A review of trials of selenium-only supplementation for the primary prevention of cardiovascular disease found no statistically significant effects of selenium on fatal and nonfatal cardiovascular events 61. Almost all of the subjects in these clinical trials were well-nourished male adults in the United States.
The limited clinical-trial evidence to date does not support the use of selenium supplements for preventing heart disease, particularly in healthy people who already obtain sufficient selenium from food. Additional clinical trials are needed to better understand the contributions of selenium from food and dietary supplements to cardiovascular health.
- Cognitive decline
Blood selenium levels decrease as people age, and scientists are studying whether low selenium levels contribute to a decline in brain function in the elderly. Some studies suggest that people with lower blood selenium levels are more likely to have poorer mental function. But a study of elderly people in the United States found no link between selenium levels and memory. More research is needed to find out whether selenium dietary supplements might help reduce the risk of or treat cognitive decline in elderly people.
Serum selenium concentrations decline with age. Marginal or deficient selenium concentrations might be associated with age-related declines in brain function, possibly due to decreases in selenium’s antioxidant activity 62, 63.
The results of observational studies are mixed 64. In two large studies, participants with lower plasma selenium levels at baseline were more likely to experience cognitive decline over time, although whether the participants in these studies were selenium deficient is not clear 62, 65, 66. An analysis of NHANES data on 4,809 elderly people in the United States found no association between serum selenium levels (which ranged from lower than 11.3 to higher than 13.5 mcg/dL) and memory test scores 67.
Researchers have evaluated whether taking an antioxidant supplement containing selenium reduces the risk of cognitive impairment in elderly people. An analysis of data from the Supplémentation en Vitamines et Minéraux Antioxydants (SU.VI.MAX) study on 4,447 participants aged 45 to 60 years in France found that, compared with placebo, daily supplementation with 120 mg ascorbic acid, 30 mg vitamin E, 6 mg beta-carotene, 100 mcg selenium, and 20 mg zinc for 8 years was associated with higher episodic memory and semantic fluency test scores 6 years after the study ended 68. However, selenium’s independent contribution to the observed effects in this study cannot be determined. The authors of a systematic review that included nine placebo-controlled studies concluded that the available clinical evidence is insufficient to determine whether selenium supplements can prevent Alzheimer’s disease 64.
More evidence is required to determine whether selenium supplements might help prevent or treat cognitive decline in elderly people.
- Thyroid disease
The thyroid gland has high amounts of selenium that play an important role in thyroid function. Studies suggest that people—especially women—who have low blood levels of selenium (and iodine) might develop problems with their thyroid. But whether selenium dietary supplements can help treat or reduce the risk of thyroid disease is not clear. More research is needed to understand the effects of selenium on thyroid disease.
Selenium concentration is higher in the thyroid gland than in any other organ in the body, and, like iodine, selenium has important functions in thyroid hormone synthesis and metabolism.
Epidemiological evidence supporting a relationship between selenium levels and thyroid gland function includes an analysis of data on 1,900 participants in the SU.VI.MAX study indicating an inverse relationship between serum selenium concentrations and thyroid volume, risk of goiter, and risk of thyroid tissue damage in people with mild iodine deficiency 69. However, these results were statistically significant only in women. A cross-sectional study in 805 adults with mild iodine deficiency in Denmark also found a significant inverse association between serum selenium concentration and thyroid volume in women 70.
Randomized, controlled trials of selenium supplementation in patients with thyroid disease have had varied results. In one randomized, double-blind, placebo-controlled trial, 100, 200, or 300 mcg/day selenium for 6 months in 368 healthy adults aged 60 to 74 years had no effect on thyroid function, even though plasma selenium levels increased significantly 71. Another randomized, double-blind, placebo-controlled trial compared the effects of 200 mcg/day selenium (as sodium selenite), 1,200 mg/day pentoxifylline (an antiinflammatory agent), or placebo for 6 months in 159 patients with mild Graves’ orbitopathy 72. Compared with patients treated with placebo, those treated with selenium but not pentoxifylline reported a higher quality of life. Furthermore, ophthalmic outcomes improved in 61% of patients in the selenium group compared with 36% of those in the placebo group, and only 7% of the selenium group had mild progression of the disease, compared with 26% of those in the placebo group.
Women with thyroid peroxidase antibodies tend to develop hypothyroxinemia while they are pregnant and thyroid dysfunction and hypothyroidism after giving birth 40. The authors of a Cochrane review of hypothyroidism interventions during pregnancy concluded, based on a trial that administered supplements containing 200 mcg selenium as selenomethionine daily to 151 pregnant women with thyroid peroxidase antibodies 73, that selenomethionine supplementation in this population is a promising strategy, especially for reducing postpartum thyroiditis 74. However, the authors called for large randomized clinical trials to provide high-quality evidence of this effect.
Additional research is needed to determine whether selenium supplements can help prevent or treat thyroid disease.
Selenium and healthy eating
People should get most of their nutrients from food because foods contain vitamins, minerals, dietary fiber and other substances that benefit health. In some cases, fortified foods and dietary supplements may provide nutrients that otherwise may be consumed in less-than-recommended amounts.
- Sunde RA. Selenium. In: Ross AC, Caballero B, Cousins RJ, Tucker KL, Ziegler TR, eds. Modern Nutrition in Health and Disease. 11th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2012:225-37[↩][↩][↩][↩][↩]
- Sunde RA. Selenium. In: Bowman B, Russell R, eds. Present Knowledge in Nutrition. 9th ed. Washington, DC: International Life Sciences Institute; 2006:480-97[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Terry EN, Diamond AM. Selenium. In: Erdman JW, Macdonald IA, Zeisel SH, eds. Present Knowledge in Nutrition. 10th ed. Washington, DC: Wiley-Blackwell; 2012:568-87[↩][↩][↩]
- Davis CD. Selenium supplementation and cancer prevention. Curr Nutr Rep 2012;1:16-23.[↩]
- Sunde RA. Selenium. In: Coates PM, Betz JM, Blackman MR, et al., eds. Encyclopedia of Dietary Supplements. 2nd ed. London and New York: Informa Healthcare; 2010:711-8[↩][↩][↩][↩][↩][↩][↩]
- Environ Health Prev Med. 2008 Mar; 13(2): 102–108. Selenium: its role as antioxidant in human health. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2698273/[↩]
- Br J Nutr. 2008 Aug;100(2):254-68. doi: 10.1017/S0007114508939830. Epub 2008 Mar 18. Food-chain selenium and human health: emphasis on intake. https://www.ncbi.nlm.nih.gov/pubmed/18346308?dopt=Abstract[↩]
- Lancet. 2012 Mar 31;379(9822):1256-68. doi: 10.1016/S0140-6736(11)61452-9. Epub 2012 Feb 29. Selenium and human health. https://www.ncbi.nlm.nih.gov/pubmed/22381456?dopt=Abstract[↩]
- Clark LC, Combs GF Jr, Turnbull BW, Slate EH, Chalker DK, Chow J, et al. Effects of selenium supplementation for cancer prevention in patients with carcinoma of the skin. A randomized controlled trial. Nutritional prevention of cancer study group. JAMA. 1996;276:1957–63. https://www.ncbi.nlm.nih.gov/pubmed/8971064[↩]
- Yoshizawa K, Willett WC, Morris SJ, Stampfer MJ, Spiegelman D, Rimm EB, et al. Study of prediagnostic selenium level in toenails and the risk of advanced prostate cancer. J Natl Cancer Inst. 1998;90:1219–24. https://www.ncbi.nlm.nih.gov/pubmed/9719083[↩]
- Ghadirian P, Maisonneuve P, Perret C, Kennedy G, Boyle P, Krewski D, et al. A case-control study of toenail selenium and cancer of the breast, colon, and prostate. Cancer Detect Prev. 2000;24:305–13. https://www.ncbi.nlm.nih.gov/pubmed/11059562[↩]
- Allen NE, Morris JS, Ngwenyama RA, Key TJ. A case-control study of selenium in nails and prostate cancer risk in British men. Br J Cancer. 2004;90:1392–6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2409674/[↩]
- Peters U, Foster CB, Chatterjee N, Schatzkin A, Reding D, Andriole GL, et al. Serum selenium and risk of prostate cancer-a nested case-control study. Am J Clin Nutr. 2007;85:209–17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1839923/[↩]
- Brinkman M, Reulen RC, Kellen E, Buntinx F, Zeegers MP. Are men with low selenium levels at increased risk of prostate cancer? Eur J Cancer. 2006;42:2463–71. https://www.ncbi.nlm.nih.gov/pubmed/16945521[↩]
- Lippman SM, Goodman PJ, Klein EA, Parnes HL, Thompson IM Jr, Kristal AR, et al. Designing the selenium and vitamin E cancer prevention trial (SELECT). J Natl Cancer Inst. 2005;97:94–102.https://www.ncbi.nlm.nih.gov/pubmed/15657339[↩]
- Klein EA, Thompson IM, Lippman SM, Goodman PJ, Albanes D, Taylor PR, et al. SELECT: the selenium and vitamin E cancer prevention trial: rationale and design. Prostate Cancer Prostatic Dis. 2000;3:145–51. https://www.ncbi.nlm.nih.gov/pubmed/12497090[↩]
- Howlader N, Noone AM, Krapcho M, et al (eds). SEER Cancer Statistics Review, 1975-2008, National Cancer Institute. Bethesda, MD, http://seer.cancer.gov/csr/1975_2008, based on November 2010 SEER data submission, posted to the SEER web site, 2011.[↩][↩]
- National Cancer Institute. Selenium and Vitamin E Cancer Prevention Trial (SELECT): Questions and Answers. https://www.cancer.gov/types/prostate/research/select-trial-results-qa#3[↩]
- EA Klein, IM Thompson, CM Tangen, et al. Vitamin E and the Risk of Prostate Cancer: Results of The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2011; 306(14) 1549-1556.[↩][↩]
- National Cancer Institute. Selenium and Vitamin E Cancer Prevention Trial (SELECT): Questions and Answers. https://www.cancer.gov/types/prostate/research/select-trial-results-qa#10[↩]
- Lippman SM, Klein EA, Goodman PJ, et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers. JAMA 2009; 301(1). Published online December 9, 2008. Print edition January 2009.[↩]
- Heinonen OP, Albanes D, Virtamo J, et al. Prostate cancer and supplementation with alpha-tocopherol and beta-carotene: Incidence and mortality in a controlled trial. JNCI 1998; 90(6):440-446.[↩]
- Kristal AR, Darke AK, Morris S, et al. Baseline selenium status and effects of selenium and vitamin E supplementation on prostate cancer risk. J Natl Cancer Inst 2014.[↩]
- Clark LC, Combs GF Jr., Turnbull BW, et al. Effects of selenium supplementation for cancer prevention in patients with carcinoma of the skin. A randomized controlled trial: Nutritional Prevention of Cancer Study Group. JAMA 1996; 276(24):1957-1963.[↩]
- Duffield-Lillico AJ, Reid ME, Turnbull BW, et al. Baseline characteristics and the effect of selenium supplementation on cancer incidence in a randomized clinical trial: A summary report of the Nutritional Prevention of Cancer Trial. Cancer Epidemiology, Biomarkers & Prevention 2002; 11(7):630-639.[↩]
- Yusuf S, Dagenais G, Pogue J, et al. Vitamin E supplementation and cardiovascular events in high risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. New England Journal of Medicine. 2000;342:154-60.[↩]
- National Cancer Institute. Selenium and Vitamin E Cancer Prevention Trial (SELECT): Questions and Answers. https://www.cancer.gov/types/prostate/research/select-trial-results-qa#16[↩]
- National Cancer Institute. Selenium and Vitamin E Cancer Prevention Trial (SELECT): Questions and Answers. https://www.cancer.gov/types/prostate/research/select-trial-results-qa#8[↩]
- Lee IM, Cook NR, Gaziano JM, et al. Vitamin E in the primary prevention of cardiovascular disease and cancer: the Women’s Health Study: a randomized controlled trial. JAMA. 2005; 294(1):56-65.[↩]
- Lonn E, Bosch J, Yusuf S, et al. Effects of long-term vitamin E supplementation on cardiovascular events and cancer: A randomized controlled trial. JAMA 2005; 293(11):1338-1347.[↩]
- National Cancer Institute. Selenium and Vitamin E Cancer Prevention Trial (SELECT): Questions and Answers. https://www.cancer.gov/types/prostate/research/select-trial-results-qa#4[↩]
- ((National Cancer Institute. Selenium and Vitamin E Cancer Prevention Trial (SELECT): Questions and Answers. https://www.cancer.gov/types/prostate/research/select-trial-results-qa#4[↩]
- Sesso HD, Buring JE, Christen WG, et al. Vitamins E and C in the prevention of cardiovascular disease in men: the Physicians’ Health Study II randomized controlled trial. JAMA. 2008; 300(18):2123-33.[↩]
- Cochrane Review 30 March 2014. Selenium for preventing cancer. http://www.cochrane.org/CD005195/GYNAECA_selenium-preventing-cancer[↩][↩]
- Cochrane Review 16 July 2008. Antioxidant supplements cannot be recommended for gastrointestinal cancer prevention. http://www.cochrane.org/CD004183/LIVER_antioxidant-supplements-cannot-be-recommended-for-gastrointestinal-cancer-prevention[↩]
- Cochrane Review 17 October 2012. Antioxidant drugs for preventing lung cancer in healthy people. http://www.cochrane.org/CD002141/LUNGCA_antioxidant-drugs-for-preventing-lung-cancer-in-healthy-people[↩]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes: Vitamin C, Vitamin E, Selenium, and Carotenoids. National Academy Press, Washington, DC, 2000.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Chun OK, Floegel A, Chung SJ, Chung CE, Song WO, Koo SI. Estimation of antioxidant intakes from diet and supplements in U.S. adults. J Nutr 2010;140:317-24. https://www.ncbi.nlm.nih.gov/pubmed/20032488?dopt=Abstract[↩]
- Rayman MP. Food-chain selenium and human health: emphasis on intake. Br J Nutr 2008;100:254-68. https://www.ncbi.nlm.nih.gov/pubmed/18346308?dopt=Abstract[↩][↩][↩]
- Rayman MP. Selenium and human health. Lancet 2012;379:1256-68. https://www.ncbi.nlm.nih.gov/pubmed/22381456?dopt=Abstract[↩][↩][↩]
- U.S. Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 25. https://www.ars.usda.gov/northeast-area/beltsville-md/beltsville-human-nutrition-research-center/nutrient-data-laboratory/[↩]
- Thomson CD, Chisholm A, McLachlan SK, Campbell JM. Brazil nuts: an effective way to improve selenium status. Am J Clin Nutr. 2008 Feb;87(2):379-84. https://www.ncbi.nlm.nih.gov/pubmed/18258628?dopt=Abstract[↩]
- Bodó ET, Stefánka Z, Ipolyi I, Sörös C, Dernovics M, Fodor P. Preparation, homogeneity and stability studies of a candidate LRM for Se speciation. Anal Bioanal Chem. 2003 Sep;377(1):32-8. https://www.ncbi.nlm.nih.gov/pubmed/12750870?dopt=Abstract[↩]
- https://ndb.nal.usda.gov/ndb/[↩]
- U.S. Department of Agriculture, Agricultural Research Service. USDA National Nutrient Database for Standard Reference, Release 27. Nutrient Data Laboratory home page, 2014. https://ndb.nal.usda.gov/ndb/[↩]
- U.S. Department of Agriculture, Agricultural Research Service. What We Eat in America, 2009-2010. https://www.ars.usda.gov/northeast-area/beltsville-md/beltsville-human-nutrition-research-center/food-surveys-research-group/docs/wweia-data-tables/[↩]
- Bailey RL, Gahche JJ, Lentino CV, Dwyer JT, Engel JS, Thomas PR, et al. Dietary supplement use in the United States, 2003-2006. J Nutr 2011;141:261-6. https://www.ncbi.nlm.nih.gov/pubmed/21178089?dopt=Abstract[↩]
- Chen J. An original discovery: selenium deficiency and Keshan disease (an endemic heart disease). Asia Pac J Clin Nutr 2012;21:320-6. https://www.ncbi.nlm.nih.gov/pubmed/22705420?dopt=Abstract[↩]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes: Vitamin C, Vitamin E, Selenium, and Carotenoids. National Academy Press, Washington, DC, 2000. [↩]
- Jirong Y, Huiyun P, Zhongzhe Y, Birong D, Weimin L, Ming Y, et al. Sodium selenite for treatment of Kashin-Beck disease in children: a systematic review of randomised controlled trials. Osteoarthritis Cartilage 2012;20:605-13. https://www.ncbi.nlm.nih.gov/pubmed/22370124?dopt=Abstract[↩]
- Burk RF, Norsworthy BK, Hill KE, Motley AK, Byrne DW. Effects of chemical form of selenium on plasma biomarkers in a high-dose human supplementation trial. Cancer Epidemiol Biomarkers Prev 2006;15:804-10. https://www.ncbi.nlm.nih.gov/pubmed/16614127?dopt=Abstract[↩]
- MacFarquhar JK, Broussard DL, Melstrom P, Hutchinson R, Wolkin A, Martin C, et al. Acute selenium toxicity associated with a dietary supplement. Arch Intern Med 2010;170:256-61. https://www.ncbi.nlm.nih.gov/pubmed/20142570?dopt=Abstract[↩]
- Flores-Mateo G, Navas-Acien A, Pastor-Barriuso R, Guallar E. Selenium and coronary heart disease: a meta-analysis. Am J Clin Nutr 2006;84:762-73. https://www.ncbi.nlm.nih.gov/pubmed/17023702?dopt=Abstract[↩]
- Xun P, Liu K, Morris JS, Daviglus ML, He K. Longitudinal association between toenail selenium levels and measures of subclinical atherosclerosis: the CARDIA trace element study. Atherosclerosis 2010;210:662-7. https://www.ncbi.nlm.nih.gov/pubmed/20138620?dopt=Abstract[↩]
- Bleys J, Navas-Acien A, Guallar E. Serum selenium levels and all-cause, cancer, and cardiovascular mortality among US adults. Arch Intern Med 2008;168:404-10. https://www.ncbi.nlm.nih.gov/pubmed/18299496?dopt=Abstract[↩]
- Bleys J, Navas-Acien A, Laclaustra M, Pastor-Barriuso R, Menke A, Ordovas J, et al. Serum selenium and peripheral arterial disease: results from the national health and nutrition examination survey, 2003-2004. Am J Epidemiol 2009;169:996-1003. https://www.ncbi.nlm.nih.gov/pubmed/19221120?dopt=Abstract[↩]
- Rayman MP, Stranges S, Griffin BA, Pastor-Barriuso R, Guallar E. Effect of supplementation with high-selenium yeast on plasma lipids: a randomized trial. Ann Intern Med 2011;154:656-65. https://www.ncbi.nlm.nih.gov/pubmed/21576533?dopt=Abstract[↩]
- Hercberg S, Galan P, Preziosi P, Bertrais S, Mennen L, Malvy D, et al. The SU.VI.MAX Study: a randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch Intern Med 2004;164:2335-42. Hercberg S, Galan P, Preziosi P, Bertrais S, Mennen L, Malvy D, et al. The SU.VI.MAX Study: a randomized, placebo-controlled trial of the health effects of antioxidant vitamins and minerals. Arch Intern Med 2004;164:2335-42.[↩]
- Hercberg S, Kesse-Guyot E, Druesne-Pecollo N, Touvier M, Favier A, Latino-Martel P, et al. Incidence of cancers, ischemic cardiovascular diseases and mortality during 5-year follow-up after stopping antioxidant vitamins and minerals supplements: a postintervention follow-up in the SU.VI.MAX Study. Int J Cancer 2010;127:1875-81. https://www.ncbi.nlm.nih.gov/pubmed/20104528?dopt=Abstract[↩]
- Stranges S, Marshall JR, Trevisan M, Natarajan R, Donahue RP, Combs GF, et al. Effects of selenium supplementation on cardiovascular disease incidence and mortality: secondary analyses in a randomized clinical trial. Am J Epidemiol 2006;163:694-9. https://www.ncbi.nlm.nih.gov/pubmed/16495471?dopt=Abstract[↩]
- Rees K, Hartley L, Day C, Flowers N, Clarke A, Stranges S. Selenium supplementation for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2013 Jan 31;(1):CD009671. https://www.ncbi.nlm.nih.gov/pubmed/23440843?dopt=Abstract[↩]
- Akbaraly TN, Hininger-Favier I, Carriere I, Arnaud J, Gourlet V, Roussel AM, et al. Plasma selenium over time and cognitive decline in the elderly. Epidemiology 2007;18:52-8. https://www.ncbi.nlm.nih.gov/pubmed/17130689?dopt=Abstract[↩][↩]
- Shahar A, Patel KV, Semba RD, Bandinelli S, Shahar DR, Ferrucci L, et al. Plasma selenium is positively related to performance in neurological tasks assessing coordination and motor speed. Mov Disord 2010;25:1909-15. https://www.ncbi.nlm.nih.gov/pubmed/20687175?dopt=Abstract[↩]
- Loef M, Schrauzer GN, Walach H. Selenium and Alzheimer’s disease: a systematic review. J Alzheimers Dis 2011;26:81-104. https://www.ncbi.nlm.nih.gov/pubmed/21593562?dopt=Abstract[↩][↩]
- Berr C, Balansard B, Arnaud J, Roussel AM, Alpérovitch A. Cognitive decline is associated with systemic oxidative stress: the EVA study. Etude du Vieillissement Artériel. J Am Geriatr Soc 2000;48:1285-91. https://www.ncbi.nlm.nih.gov/pubmed/11037017?dopt=Abstract[↩]
- Gao S, Jin Y, Hall KS, Liang C, Unverzagt FW, Ji R, et al. Selenium level and cognitive function in rural elderly Chinese. Am J Epidemiol 2007;165:955-65. https://www.ncbi.nlm.nih.gov/pubmed/17272290?dopt=Abstract[↩]
- Perkins AJ, Hendrie HC, Callahan CM, Gao S, Unverzagt FW, Xu Y, et al. Association of antioxidants with memory in a multiethnic elderly sample using the Third National Health and Nutrition Examination Survey. Am J Epidemiol 1999;150:37-44. https://www.ncbi.nlm.nih.gov/pubmed/10400551?dopt=Abstract[↩]
- Kesse-Guyot E, Fezeu L, Jeandel C, Ferry M, Andreeva V, Amieva H, et al. French adults’ cognitive performance after daily supplementation with antioxidant vitamins and minerals at nutritional doses: a post hoc analysis of the Supplementation in Vitamins and Mineral Antioxidants (SU.VI.MAX) trial. Am J Clin Nutr 2011;94:892-9. https://www.ncbi.nlm.nih.gov/pubmed/21775560?dopt=Abstract[↩]
- Derumeaux H, Valeix P, Castetbon K, Bensimon M, Boutron-Ruault MC, Arnaud J, Hercberg S. Association of selenium with thyroid volume and echostructure in 35- to 60-year-old French adults. Eur J Endocrinol 2003;148(3):309-15.[↩]
- Rasmussen LB, Schomburg L, Kohrle J, Pedersen IB, Hollenbach B, Hog A, et al. Selenium status, thyroid volume, and multiple nodule formation in an area with mild iodine deficiency. Eur J Endocrinol 2011;164:585-90. https://www.ncbi.nlm.nih.gov/pubmed/21242171?dopt=Abstract[↩]
- Rayman MP, Thompson AJ, Bekaert B, Catterick J, Galassini R, Hall E, et al. Randomized controlled trial of the effect of selenium supplementation on thyroid function in the elderly in the United Kingdom. Am J Clin Nutr 2008;87:370-8. https://www.ncbi.nlm.nih.gov/pubmed/18258627?dopt=Abstract[↩]
- Marcocci C, Kahaly GJ, Krassas GE, Bartalena L, Prummel M, Stahl M, et al. Selenium and the course of mild Graves’ orbitopathy. N Engl J Med 2011;364:1920-31. https://www.ncbi.nlm.nih.gov/pubmed/21591944?dopt=Abstract[↩]
- Negro R, Greco G, Mangieri T, Pezzarossa A, Dazzi D, Hassan H. The influence of selenium supplementation on postpartum thyroid status in pregnant women with thyroid peroxidase autoantibodies. J Clin Endocrinol Metab 2007;92:1263-8. https://www.ncbi.nlm.nih.gov/pubmed/17284630?dopt=Abstract[↩]
- Reid SM, Middleton P, Cossich MC, Crowther CA. Interventions for clinical and subclinical hypothyroidism in pregnancy. Cochrane Database Syst Rev 2010:CD007752. https://www.ncbi.nlm.nih.gov/pubmed/20614463?dopt=Abstract[↩]





{kind=link}