Contents
What is solitary pulmonary nodule
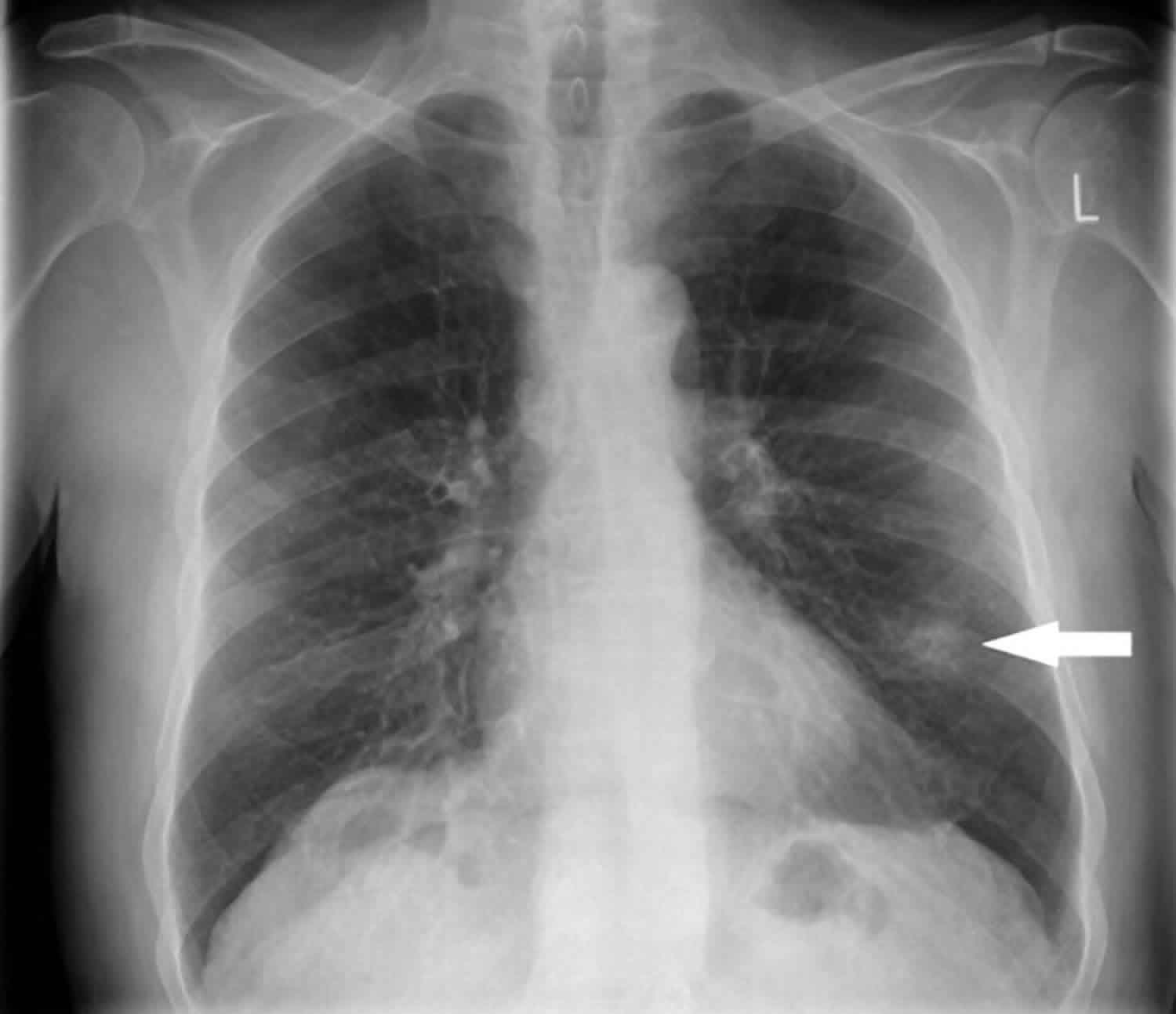
Solitary pulmonary nodule is defined as a discrete, well-marginated, rounded opacity less than or equal to 3 cm in diameter in the lung that is completely surrounded by lung parenchyma, does not touch the hilum or mediastinum, and is not associated with adenopathy, atelectasis, or pleural effusion that is seen with a chest x-ray or CT scan 1. Lesions larger than 3 cm are considered masses and are treated as malignancies until proven otherwise. Generally, a pulmonary nodule must reach 1 cm in diameter before it can be identified on a chest radiograph 1. For a malignant nodule to reach this size, approximately 30 doublings would have occurred. The average doubling time for a malignant tumor is 120 days (range 7-590 days). A lesion at this growth rate may be present for 10 years before discovery.
Solitary pulmonary nodules present a diagnostic dilemma, as these lesions may be due to a vast array of benign and malignant causes. Although some patients are eligible for imaging follow-up, certain patients will require tissue diagnosis.
Patients with solitary pulmonary nodules are usually asymptomatic. However, solitary pulmonary nodules can pose a challenge to clinicians and patients. Whether detected serendipitously or during a routine investigation, a nodule on chest imaging raises the following questions:
- Is the nodule benign or malignant?
- Should it be investigated or observed?
- Should it be surgically resected?
Most solitary pulmonary nodules are benign. However, they may represent an early stage of lung cancer. Lung cancer is the leading cause of cancer death in the United States, accounting for more deaths annually than breast, colon, and prostate cancers combined.
Solitary pulmonary nodules are one of the most common thoracic imaging abnormalities. A revised estimate of over 1 million nodules are detected each year as an incidental finding, either on chest radiographs or thoracic computed tomography (CT) scans 2. In lung cancer screening studies that enrolled people at high risk for lung cancer, the prevalence of solitary pulmonary nodules ranged from 8-51% 3.
Approximately 40-50% of solitary pulmonary nodules are malignant. Gould et al 4 reported after a review of the literature that most of these are adenocarcinoma (47%), followed by squamous cell carcinoma (22%). Small cell lung cancer makes up only 4% of malignant solitary pulmonary nodules.
Patients with early lung cancer, when the primary tumor is less than 3 cm in diameter without evidence of lymph node involvement or distant metastasis (stage 1A), have a 5-year survival rate of 70-80% 5. Therefore, prompt diagnosis and management of early lung cancer manifesting as a solitary pulmonary nodule is the the best chance for cure.
Can solitary pulmonary nodule be cancerous?
Yes, lung nodules can be cancerous, though most lung nodules are noncancerous (benign).
Lung nodules — small masses of tissue in the lung — are quite common. They appear as round, white shadows on a chest X-ray or computerized tomography (CT) scan.
Lung nodules are usually about 0.2 inch (5 millimeters) to 1.2 inches (30 millimeters) in size. A larger lung nodule, such as one that’s 30 millimeters or larger, is more likely to be cancerous than is a smaller lung nodule.
If your doctor detects a lung nodule on an imaging test, it’s helpful to compare your current imaging scan with a previous one. If the nodule on earlier images hasn’t changed in size, shape or appearance in two years, it’s probably noncancerous.
Noncancerous lung nodules are often caused by previous infections. Noncancerous lung nodules usually require no treatment. In some cases your doctor may recommend annual chest imaging to see if a lung nodule grows or changes over time.
If a lung nodule is new or has changed in size, shape or appearance, your doctor may recommend further testing — such as a CT scan, positron emission tomography (PET) scan, bronchoscopy or tissue biopsy — to determine if it’s cancerous.
Solitary pulmonary nodule causes
Bearing in mind that the major distinction that must be made is between cancer and inflammatory lesions, solitary pulmonary nodules have several causes. More than half of all solitary pulmonary nodules are noncancerous (benign). Benign nodules have many causes, including scars and past infections.
Infectious granulomas (which are formed by cells as a reaction to a past infection) cause most benign lesions. Common infections that often result in granulomas or other healed scars include:
- Tuberculosis (TB) or exposure to TB
- Fungus, such as aspergillosis, coccidioidomycosis, cryptococcosis, or histoplasmosis
Primary lung cancer is the most common cause of cancerous (malignant) pulmonary nodules. This is cancer that starts in the lung.
Neoplastic (malignant or benign) tumors can be caused by the following:
- Bronchogenic carcinoma
- Adenocarcinoma (including bronchoalveolar carcinoma)
- Squamous cell carcinoma
- Large cell lung carcinoma
- Small cell lung cancer
- Metastasis
- Lymphoma
- Carcinoid
- Hamartoma
- Connective-tissue and neural tumors – Fibroma, neurofibroma, blastoma, and sarcoma
Inflammatory (infectious) nodules can result from the following:
- Granuloma – Tuberculosis (TB), histoplasmosis, coccidioidomycosis, blastomycosis, cryptococcosis, and nocardiosis
- Lung abscess
- Round pneumonia
- Hydatid cyst
Inflammatory (noninfectious) nodules can be caused by the following:
- Rheumatoid arthritis
- Granulomatosis with polyangiitis previously known as Wegener’s granulomatosis
- Sarcoidosis
- Lipoid pneumonia
Congenital nodules can be produced by the following:
- Arteriovenous malformation
- Pulmonary sequestration
- Bronchogenic cyst
Other causes of pulmonary nodules include the following:
- Pulmonary infarct
- Rounded atelectasis
- Mucoid impaction
- Progressive massive fibrosis
Solitary pulmonary nodule symptoms
A solitary pulmonary nodule itself rarely causes symptoms.
Solitary pulmonary nodule diagnosis
A solitary pulmonary nodule is most often found on a chest x-ray or chest CT scan. These imaging tests are often done for other symptoms or reasons.
Your health care provider must decide whether the nodule in your lung is most likely benign or of concern. A nodule more likely benign if:
- The nodule is small, has a smooth border, and has a solid and even appearance on an x-ray or CT scan.
- You are young and do not smoke.
Your doctor may then choose to monitor the nodule over time by repeating a series of x-rays or CT scans.
- Repeat chest x-rays or chest CT scans are the most common way to monitor the nodule. Sometimes, lung positron-emission tomography (PET) scans may be done.
- If repeated x-rays show that the nodule size has not changed in 2 years, it is most likely benign and a biopsy is not needed.
Your doctor may choose to biopsy the nodule to rule out cancer if:
- You are a smoker.
- You have other symptoms of lung cancer.
- The nodule has grown in size or has changed when compared to earlier images.
A lung needle biopsy may be done by placing a needle directly through the wall of your chest, or during procedures called bronchoscopy or mediastinoscopy.
Tests to rule out TB and other infections may also be done.
Solitary pulmonary nodule treatment
Ask your doctor about the risks of having a biopsy versus monitoring the size of the solitary pulmonary nodule with regular x-rays or CT scans. Treatment may be based on the results of the biopsy or other tests.
Solitary pulmonary nodule prognosis
The outlook is usually good if the solitary pulmonary nodule is benign. If the nodule does not grow larger over a 2-year period, often nothing more needs to be done.
Although most solitary pulmonary nodules are benign, they may represent an early stage of lung cancer. While lung cancer survival rates remain dismally low at around 14-18% at 5 years, a diagnosis of early lung cancer (ie, when the primary tumor has a diameter <3 cm with no lymph node involvement and no distant metastasis [stage 1A]) can be associated with a 5-year survival rate upwards of 80%. Accordingly, the best chance for cure of early lung cancer manifesting as a solitary pulmonary nodule is prompt diagnosis and management.
Surgical resection is curative for most benign lung tumors. The 5- and 10-year survival rates following surgical resection of typical carcinoid tumors of the lung are above 90%. The 5- and 10-year survival rates for patients with atypical carcinoids are 40-70% and 18-50%, respectively 6.
In one study, complete bronchoscopic resection for endobronchial carcinoid tumors at 1 and 10 years provided disease-free states at rates of 100% and 94%, respectively 7.
- Solitary Pulmonary Nodule. https://emedicine.medscape.com/article/2139920-overview[↩][↩]
- Gould MK, Tang T, Liu IL, Lee J, Zheng C, Danforth KN, et al. Recent Trends in the Identification of Incidental Pulmonary Nodules. Am J Respir Crit Care Med. 2015 Nov 15. 192 (10):1208-14.[↩]
- Wahidi MM, Govert JA, Goudar RK, Gould MK, McCrory DC. Evidence for the treatment of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007 Sep. 132(3 Suppl):94S-107S.[↩]
- Gould MK, Fletcher J, Iannettoni MD, Lynch WR, Midthun DE, Naidich DP, et al. Evaluation of patients with pulmonary nodules: when is it lung cancer?: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007 Sep. 132(3 Suppl):108S-130S.[↩]
- Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016 Jan. 11 (1):39-51.[↩]
- Travis WD, Rush W, Flieder DB, Falk R, Fleming MV, Gal AA, et al. Survival analysis of 200 pulmonary neuroendocrine tumors with clarification of criteria for atypical carcinoid and its separation from typical carcinoid. Am J Surg Pathol. 1998 Aug. 22(8):934-44.[↩]
- Luckraz H, Amer K, Thomas L, Gibbs A, Butchart EG. Long-term outcome of bronchoscopically resected endobronchial typical carcinoid tumors. J Thorac Cardiovasc Surg. 2006 Jul. 132(1):113-5.[↩]





{kind=link}