
Contents
- Sexually transmitted diseases
- Chlamydia
- Chlamydia trachomatis bacteria
- Chlamydia infection causes
- Chlamydia prevention
- Chlamydia signs and symptoms
- Chlamydia in women
- Chlamydia in men
- Chlamydia infections in infants and children
- Chlamydia complications
- Chlamydia diagnosis
- Chlamydia test
- Chlamydia treatment
- Treatment of chlamydial infections during pregnancy
- Adults with oropharyngeal chlamydial infections
- Treatment for lymphogranuloma venereum
- Management of sex partners
- Infants born to mothers with chlamydial infection
- Neonates with ophthalmia neonatorum
- Infant pneumonia
- Chlamydial infections in infants and children
- Chlamydia prognosis
- Gonorrhea
- Neisseria gonorrhoeae bacteria
- How do you get gonorrhea?
- Risk factors for getting gonorrhea
- Gonorrhea prevention
- Gonorrhea signs and symptoms
- Gonorrhea complications
- Gonorrhea diagnosis
- Gonorrhea test
- Gonorrhea treatment
- Antibiotics for gonorrhea
- Uncomplicated Gonococcal Infections of the Cervix, Urethra, and Rectum
- Uncomplicated Gonococcal Infections of the throat (pharynx)
- Gonococcal conjunctivitis
- Gonococcal Infections in Pregnancy
- Gonorrhea treatment for babies
- Disseminated Gonococcal Infection
- Treatment of Arthritis and Arthritis-Dermatitis Syndrome
- Treatment of Gonococcal Meningitis and Endocarditis
- Management of Antibiotic-Resistant Gonorrhea
- Allergy to Penicillins or Cephalosporin
- Management of Suspected Gonococcal Treatment Failure
- Follow-Up
- Management of Sex Partners
- Genital herpes
- Genital warts
- Syphilis
- How is syphilis spread?
- What is the treatment for syphilis?
- Is syphilis curable?
- Will syphilis recur?
- How common is syphilis?
- Who should be tested for syphilis?
- How can I reduce my risk of getting syphilis?
- Am I at risk for syphilis?
- I’ve been treated. Can I get syphilis again?
- I’m pregnant. How does syphilis affect my baby?
- What causes syphilis?
- Syphilis stages
- Syphilis signs and symptoms
- Syphilis diagnosis
- Syphilis treatment
- Latent Syphilis Treatment
- Management of Sex Partners
- Primary and Secondary Syphilis among Persons with HIV Infection
- Syphilis During Pregnancy
- Congenital syphilis treatment
- Tertiary Syphilis
- Neurosyphilis Treatment
- Penicillin Allergy
- Management of Persons Who Have a History of Penicillin Allergy
- Trichomoniasis
- How do you get trichomoniasis?
- Trichomoniasis symptoms
- Trichomoniasis causes
- Trichomoniasis complications
- Trichomoniasis prevention
- Trichomoniasis diagnosis
- Trichomoniasis test
- Trichomoniasis treatment
- Trichomoniasis cure
- Treatment of persistent or recurrent trichomoniasis
- Follow-up
- Management of Sex Partners
- Treatment of women during pregnancy
- Treatment of women with HIV
- Allergy, Intolerance, and Adverse Reactions
Sexually transmitted diseases
The term “sexually transmitted disease” or “STD” refers to a recognizable disease state that has developed from an sexually transmitted infection (STI) 1. Sexually transmitted infections (STIs) refer infections that are passed from one person to another by having sex with someone who has an infection. Sexually transmitted diseases (STDs) are usually spread during vaginal sex, oral sex, anal sex or skin-to-skin contact. But sometimes they can spread through other sexual contact involving the penis, vagina, mouth, or anus. This is because some STDs, like herpes and HPV, are spread by skin-to-skin contact. Your risk for catching sexually transmitted diseases (STDs) is higher if you have had many sex partners, have had sex with someone who has had many partners, or have had sex without using condoms. Some STDs can be passed from a pregnant woman to her baby, either during pregnancy or when giving birth. Other ways that STDs may be spread include during breastfeeding, through blood transfusions, or by sharing needles.
STDs can be caused by bacteria, viruses, or parasites. There are more than 20 types of STDs, including:
- Chlamydia
- Genital herpes
- Gonorrhea
- Hepatitis B
- Human immunodeficiency virus (HIV)
- Human papilloma virus (HPV) causing genital warts
- Pubic lice
- Syphilis
- Trichomoniasis
What are the symptoms of STD?
Sexually transmitted diseases (STDs) don’t always cause symptoms or may only cause mild symptoms. So it is possible to have an STD and not know it. And even without symptoms, STDs can still be harmful and may be passed on during sex. For example, chlamydia can lead to problems that can cause women not to be able to have children (infertility). HPV can lead to cancer of the cervix or penis. Syphilis can lead to paralysis, mental problems, heart damage, blindness, and even death.
The most common symptoms of STDs include:
- Unusual discharge from the penis or vagina.
- Itching around the vagina and/or discharge from the vagina.
- Discharge from the penis.
- Sores or warts on the genital area
- Chancre sores (painless red sores) on the genital area, anus, tongue, and/or throat.
- Pain during sex
- Painful or frequent urination (peeing)
- Itching and redness in the genital area
- Blisters or sores in or around the mouth
- Abnormal vaginal odor
- Anal itching, soreness, or bleeding
- Abdominal pain
- Pain in the pelvic area.
- Pain in or around the anus for people who have anal sex.
- Fever
- Sore throats in people who have oral sex.
- A scaly rash on the palms of your hands and the soles of your feet.
- Dark urine, loose, light-colored stools, and yellow eyes and skin.
- Small blisters that turn into scabs on the genital area.
- Swollen glands, fever, and body aches.
- Unusual infections, unexplained fatigue, night sweats, and weight loss.
- Soft, flesh-colored warts around the genital area.
Can STD be prevented or avoided?
The only sure way to prevent STD is by not having anal, vaginal, or oral sex. If you have sex, you can lower your risk of getting a STD by only having sex with someone who isn’t having sex with anyone else and who doesn’t have a STD.
You should always use condoms when having sex, including oral and anal sex. Latex condoms greatly reduces, but does not completely eliminate, the risk of catching or spreading STDs
If your or your partner is allergic to latex, you can use polyurethane condoms.
How to use male condoms
- Put the condom on before any contact is made.
- Unroll the condom over an erect penis to the base of the penis. (Uncircumcised men should pull back their foreskin before unrolling.) The unrolled ring should be on the outside. Leave about 1/2 inch of space in the tip so semen can collect there. Squeeze the tip to get the air out.
- Pull out after ejaculating and before the penis gets soft. To pull out, hold the rim of the condom at the base of the penis to make sure it doesn’t slip off.
- Don’t reuse condoms.
How to use female condoms
- Follow the directions on the condom package for correct placement. Be sure the inner ring goes as far into the vagina as it can. The outer ring stays outside the vagina.
- Guide the penis into the condom.
- After sex, remove the condom before standing up by gently pulling it out.
- Don’t reuse condoms.
Do condoms prevent STDs?
Male latex condoms can reduce your risk of getting a STD if used correctly. Be sure to use them every time you have sex. Female condoms aren’t as effective as male condoms. However, you should use them when a man won’t use a male condom.
Remember, though, that condoms aren’t 100% safe. They can’t protect you from coming into contact with some sores (such as those that can occur with herpes) or warts (which can be caused by HPV infection).
How are STDs diagnosed?
If you are sexually active, you should talk to your health care provider about your risk for STDs and whether you need to be tested. This is especially important since many STDs do not usually cause symptoms.
Some STDs may be diagnosed during a physical exam or through microscopic examination of a sore or fluid swabbed from the vagina, penis, or anus. Blood tests can diagnose other types of STDs.
STD testing near you
Although it may be embarrassing, if you are sexually active, getting tested for STDs is one of the most important things you can do to protect your health. Make sure you have an open and honest conversation about your sexual history and STD testing with your doctor and ask whether you should be tested for STDs. If you are not comfortable talking with your regular health care provider about STDs, there are many clinics that provide confidential and free or low-cost testing. Follow this link to find an STD testing center near you https://www.cdc.gov/std/prevention/screeningreccs.htm
What are the treatments for STDs?
Antibiotics can treat STDs caused by bacteria (such as chlamydia, syphilis) or parasites. There is no cure for STDs caused by viruses (such as HIV or herpes), but medicines can often help with the symptoms and lower your risk of spreading the infection. Your doctor can only treat the symptoms that the virus causes.
Don’t wait to be treated. Early treatment helps prevent serious health problems. Even if medicine can’t completely cure the STD, it can help keep you from getting really sick. If you are given medicine for an STD, take it exactly as your doctor says.
Correct usage of latex condoms greatly reduces, but does not completely eliminate, the risk of catching or spreading STDs. The most reliable way to avoid infection is to not have anal, vaginal, or oral sex.
There are vaccines to prevent HPV and hepatitis B.
Chlamydia
Chlamydia is a common sexually transmitted disease (STD) caused by bacteria called Chlamydia trachomatis (Figure 9). Anyone can get chlamydia. You can get chlamydia during oral, vaginal, or anal sex with someone who has chlamydia.You are more likely to get infected with chlamydia if you don’t consistently use a condom or if you have multiple partners. Chlamydia often doesn’t cause symptoms, so people may not know that they have it. A pregnant woman can also pass chlamydia to her baby during childbirth. Antibiotics can cure it. But if it’s not treated, chlamydia can cause serious health problems and you may need to stay in the hospital and get medicine delivered through a needle in your arm. Sometimes people who have chlamydia will have another STD. You should also be tested for gonorrhea, syphilis, and HIV. If you’ve had chlamydia and were treated in the past, you can get re-infected if you have unprotected sex with someone who has it.
According to the Centers for Disease Control and Prevention (CDC) in 2009, the rate of sexually transmitted chlamydia infections in the United States was 426 cases per population of 100,000, which represents a 24 percent increase in the rate of infection since 2006 2. More recent data from 2016 indicates that 1,598,354 chlamydia infections were reported to the CDC from all 50 states and the District of Columbia 3. The CDC estimates that there are 2.86 million chlamydia cases in the United States annually—more than twice the number actually reported 4. This is an increase of 5 percent over the past year, and 27 percent from four years ago 5. A large number of cases are not reported because most people with chlamydia are asymptomatic and do not seek testing.
Chlamydia is most common among young people, especially young women. Almost two-thirds of new chlamydia infections occur among youth aged 15-24 years 4. It is estimated that 1 in 20 sexually active young women aged 14-24 years has chlamydia 6.
Substantial racial/ethnic disparities in chlamydial infection exist, with prevalence among non-Hispanic blacks 5.6 times the prevalence among non-Hispanic whites 3. Chlamydia is also common among men who have sex with men. Among men who have sex with men screened for rectal chlamydial infection, positivity has ranged from 3.0% to 10.5% 7. Among men who have sex with men screened for pharyngeal chlamydial infection, positivity has ranged from 0.5% to 2.3% 8.
The Centers for Disease Control and Prevention (CDC) recommends chlamydia screening for:
- Sexually active women age 25 or younger. The rate of chlamydia infection is highest in this group, so a yearly screening test is recommended. Even if you’ve been tested in the past year, get tested when you have a new sex partner.
- Pregnant women. You should be tested for chlamydia during your first prenatal exam. If you have a high risk of infection — from changing sex partners or because your regular partner might be infected — get tested again later in your pregnancy.
- Women and men at high risk. People who have multiple sex partners, who don’t always use a condom or men who have sex with men should consider frequent chlamydia screening. Other markers of high risk are current infection with another sexually transmitted infection and possible exposure to an STD through an infected partner.
Screening and diagnosis of chlamydia is relatively simple. Chlamydia tests include:
- A urine test. A sample of your urine is analyzed in the laboratory for presence of this infection.
- A swab. For women, your doctor takes a swab of the discharge from your cervix for culture or antigen testing for chlamydia. This can be done during a routine Pap test. Some women prefer to swab their vaginas themselves, which has been shown to be as diagnostic as doctor-obtained swabs.
For men, your doctor inserts a slim swab into the end of your penis to get a sample from the urethra. In some cases, your doctor will swab the anus.
If you’ve been treated for an initial chlamydia infection, you should be retested in about three months.
Chlamydia trachomatis is treated with antibiotics (e.g., doxycycline, azithromycin or levofloxacin). You might receive a one-time dose, or you might need to take the medication daily or multiple times a day for five to 10 days.
In most cases, chlamydia infection resolves within one to two weeks. During that time, you should abstain from sex. Your sexual partner or partners also need treatment even if they have no signs or symptoms. Otherwise, the chlamydia infection can be passed back and forth between sexual partners.
Having chlamydia or having been treated for it in the past doesn’t prevent you from getting it again.
Chlamydia often has no symptoms, but it can cause serious health problems, even without symptoms. If symptoms occur, they may not appear until several weeks after having sex with a partner who has chlamydia.
See your doctor if you have a discharge from your vagina, penis or rectum, or if you have pain during urination. Also, see your doctor if you learn your sexual partner has chlamydia. Your doctor will likely prescribe an antibiotic even if you have no symptoms.
Chlamydia infection symptoms in women may include:
- An abnormal vaginal discharge; and
- A burning sensation when peeing.
Chlamydia infection symptoms in men may include:
- A discharge from their penis;
- A burning sensation when peeing; and
- Pain and swelling in one or both testicles (although this is less common).
Men and women can also get chlamydia in their rectum. This happens either by having receptive anal sex, or by spread from another infected site (such as the vagina). While these infections often cause no symptoms, they can cause:
- Rectal pain;
- Discharge; and
- Bleeding.
See a doctor if you notice any of these symptoms. You should also see a doctor if your partner has an STD or symptoms of one. Symptoms can include
- An unusual sore;
- A smelly discharge;
- Burning when peeing; or
- Bleeding between periods.
Who should be tested for chlamydia?
Sexually active people can get chlamydia through vaginal, anal, or oral sex without a condom with a partner who has chlamydia. You should go to your doctor or a STD clinic for a test if you have symptoms of chlamydia or if you have a partner who has an STD. Pregnant women should get a test when they go to their first prenatal visit.
People at higher risk should get checked for chlamydia every year:
- Sexually active women 25 and younger
- Older women who have new or multiple sex partners or a sex partner who has an STD
- Men who have sex with men (MSM)
Sexually active young people are at a higher risk of getting chlamydia. This is due to behaviors and biological factors common among young people 9. Gay and bisexual men are also at risk since chlamydia can spread through oral and anal sex.
If you are sexually active, have an honest and open talk with your healthcare provider. Ask them if you should get tested for chlamydia or other STDs. Gay or bisexual men and pregnant people should also get tested for chlamydia.
STD clinic near you
Although it may be embarrassing, if you are sexually active, getting tested for STDs is one of the most important things you can do to protect your health. Make sure you have an open and honest conversation about your sexual history and STD testing with your doctor and ask whether you should be tested for STDs. If you are not comfortable talking with your regular health care provider about STDs, there are many clinics that provide confidential and free or low-cost testing. Below or following this link to find an STD testing center near you https://www.cdc.gov/std/prevention/screeningreccs.htm
Is there a cure for chlamydia?
Yes, antibiotics will cure chlamydia infection. You may get a one-time dose of the antibiotics, or you may need to take medicine every day for 7 days. It is important to take all the medicine that your doctor prescribed for you to cure your infection. When taken properly antibiotic will stop chlamydia infection and could decrease your chances of having problems later (see Chlamydia complications below). Antibiotics cannot repair any permanent damage that chlamydia has caused.
To prevent spreading chlamydia to your partner, you should not have sex until the chlamydia infection has cleared up. If you got a one-time dose of antibiotics, you should wait 7 days after taking the medicine to have sex again. If you have to take medicine every day for 7 days, you should not have sex again until you have finished taking all of the doses of your medicine.
It is common to get a repeat chlamydia infection, so you need to get tested again about three months after your treatment, even if your sex partner(s) receives treatment.
When can I have sex again after my chlamydia treatment?
You should not have sex again until you and your sex partner(s) complete treatment. If given a single dose of medicine, you should wait seven days after taking the medicine before having sex. If given medicine to take for seven days, wait until you finish all the doses before having sex.
If you’ve had chlamydia and took medicine in the past, you can still get it again. This can happen if you have sex without a condom with a person who has chlamydia.
What happens if I don’t get treated my for chlamydia?
The initial damage that chlamydia causes often goes unnoticed. However, chlamydia can lead to serious health problems.
In women, untreated chlamydia can cause pelvic inflammatory disease (PID). Some of the complications of pelvic inflammatory disease are:
- Formation of scar tissue that blocks fallopian tubes;
- Ectopic pregnancy (pregnancy outside the womb);
- Infertility (not being able to get pregnant); and
- Long-term pelvic/abdominal pain.
Men rarely have health problems from chlamydia. The infection can cause a fever and pain in the tubes attached to the testicles. This can, in rare cases, lead to infertility.
Untreated chlamydia may also increase your chances of getting or giving HIV.
Chlamydia trachomatis bacteria
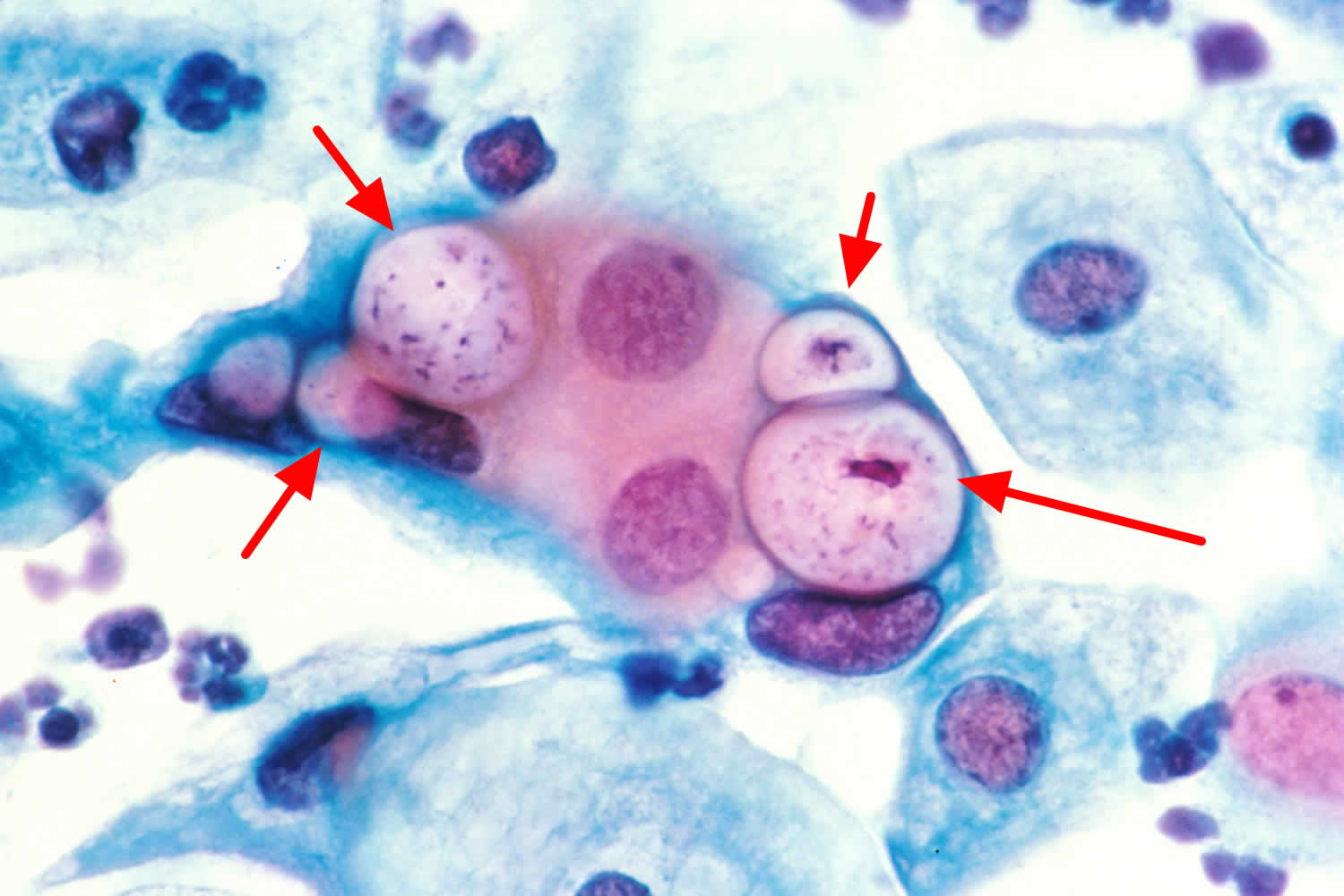
Chlamydia trachomatis is a Gram-negative anaerobic intracellular bacterium that infects the columnar epithelium of the cervix, urethra, and rectum, as well as nongenital sites such as the lungs and eyes 10, 11. Chlamydia trachomatis is a member of the Chlamydiaceae family. The genus Chlamydia includes three species that infect humans: Chlamydia trachomatis, Chlamydia pneumoniae, and Chlamydia psittaci 10, 12.
Chlamydia trachomatis differentiates into 18 serovars (serologically variant strains) based on monoclonal antibody-based typing assays. These serovars correlate with multiple medical conditions as follows 13:
- Serovars A, B, Ba, and C: Trachoma is a serious ocular illness that is endemic in Africa and Asia. It is characterized by chronic conjunctivitis and has the potential to cause blindness
- Serovars D-K: Genital tract infections, neonatal infections
- Serovars L1-L3: Lymphogranuloma venereum (LGV), which correlates with genital ulcer disease in tropical countries.
Chlamydia trachomatis bacterium is the cause of the most frequently reported sexually transmitted disease (STD) in the United States, which is responsible for more than 1.6 million infections annually 14, 15. Most people with chlamydia infection are asymptomatic. Untreated infection can result in serious complications such as pelvic inflammatory disease (PID), cervicitis, infertility, chronic pelvic pain and ectopic pregnancy in women, and epididymitis and orchitis in men and urethritis and proctitis in both men and women. Men and women can experience chlamydia-induced reactive arthritis. Lymphogranuloma venereum, another type of STD caused by different serovars of the same Chlamydia trachomatis bacterium, occurs commonly in the developing world, and has more recently emerged as a cause of outbreaks of proctitis among men who have sex with men worldwide 16. Lymphogranuloma venereum (LGV) generally presents as a unilateral, tender inguinal or femoral node, and may include a genital ulcer or papule. Anal exposure may result in proctocolitis, rectal discharge, pain, constipation, or tenesmus.If left untreated, it may lead to chronic symptoms, including fistulas and strictures. Diagnosis is based on clinical symptoms and a genital lesion swab or lymph node sample, similar to those used to diagnose the more typical C. trachomatis genitourinary infection. Molecular identification may be needed to differentiate lymphogranuloma venereum (LGV) from non-lymphogranuloma venereum (non-LGV) Chlamydia trachomatis. Doxycycline (100 mg twice daily for 21 days) is the preferred treatment. An alternative treatment regimen includes erythromycin (500 mg four times daily for 21 days); azithromycin (1 g once weekly for three weeks) may also be used 15.
Figure 1. Chlamydia trachomatis bacteria (human pap smear showing cells infected with Chlamydia trachomatis at 500x magnification, stained with haematoxylin and eosin)
Chlamydia infection causes
The Chlamydia trachomatis bacterium is most commonly spread through vaginal, oral and anal sex with a person who has chlamydia infection. Chlamydia also can spread just by touching an infected person’s genitals. It’s also possible for pregnant women to pass chlamydia to their children during delivery, causing pneumonia or a serious eye infection in the newborns.
Risk factors for chlamydia infection
Factors that increase your risk of chlamydia infection include:
- Being sexually active before age 25
- Having multiple sex partners
- Not using a condom consistently
- History of sexually transmitted infection.
Chlamydia prevention
You can get chlamydia by having vaginal, anal, or oral sex with someone who has chlamydia. Also, you can still get chlamydia even if your sex partner does not ejaculate (cum). And the only way to completely avoid chlamydia infection or other STDs is to not have vaginal, anal, or oral sex. Short of that, you can:
- Use condoms. Use a male latex condom or a female polyurethane condom during each sexual contact. Condoms used properly during every sexual encounter reduce but don’t eliminate the risk of infection.
- Limit your number of sex partners. Having multiple sex partners puts you at a high risk of contracting chlamydia and other sexually transmitted infections.
- Get regular STD tests. If you’re sexually active, particularly if you have multiple partners, talk with your doctor about how often you should be screened for chlamydia and other sexually transmitted infections.
- Avoid douching. Douching decreases the number of good bacteria in the vagina, which can increase the risk of infection.
You should always use condoms when having sex, including oral and anal sex. Latex condoms greatly reduces, but does not completely eliminate, the risk of catching or spreading STDs
If your or your partner is allergic to latex, you can use polyurethane condoms.
How to use male condoms
- Put the condom on before any contact is made.
- Unroll the condom over an erect penis to the base of the penis. (Uncircumcised men should pull back their foreskin before unrolling.) The unrolled ring should be on the outside. Leave about 1/2 inch of space in the tip so semen can collect there. Squeeze the tip to get the air out.
- Pull out after ejaculating and before the penis gets soft. To pull out, hold the rim of the condom at the base of the penis to make sure it doesn’t slip off.
- Don’t reuse condoms.
How to use female condoms
- Follow the directions on the condom package for correct placement. Be sure the inner ring goes as far into the vagina as it can. The outer ring stays outside the vagina.
- Guide the penis into the condom.
- After sex, remove the condom before standing up by gently pulling it out.
- Don’t reuse condoms.
Chlamydia signs and symptoms
Chlamydia is known as a ‘silent’ infection because most infected people are asymptomatic and lack abnormal physical examination findings. So you may not realize that you have chlamydia. But even if you don’t have symptoms, you can still pass chlamydia infection to others.
Early-stage chlamydia infections often cause few or no signs and symptoms. Even when you have signs and symptoms, they’re often mild, making them easy to overlook.
If you do have symptoms, they may not appear until 1 to 3 weeks after you have sex with someone who has chlamydia.
Signs and symptoms of chlamydia trachomatis infection can include 17, 18, 19, 20, 21, 22:
- Painful urination (a burning sensation).
- Vaginal discharge in women
- Discharge from the penis in men
- Pain in the testicles in men.
- Painful sexual intercourse in women
- Irregular periods, bleeding between periods and after sex in women
- Testicular pain in men
- Lower abdominal pain
- Rectal pain, discharge, and bleeding for men and women who engage in anal sexual activity.
- Reactive arthritis in both men and women (pain and inflammation of the joints that develops from an infection).
- Lymphogranuloma venereum. Lymphogranuloma venereum causes painful and swollen lymph nodes (buboes), which can then break down into large ulcers. Lymphogranuloma venereum symptoms include:
- Drainage through the skin from lymph nodes in the groin
- Painful bowel movements
- Small painless sore on the male genitals or in the female genital tract
- Swelling and redness of the skin in the groin area
- Swelling of the labia (in women)
- Swollen groin lymph nodes on one or both sides; it may also affect lymph nodes around the rectum in people who have anal intercourse
- Blood or pus from the rectum (blood in the stools)
Chlamydia can infect the rectum in men and women, either directly through receptive anal sex, or possibly via spread from the cervix and vagina in a woman with cervical chlamydial infection 23. Chlamydia infection of the rectum in men or women, can present with either with no signs or symptoms or with of proctitis (e.g., rectal pain, discharge, and/or bleeding) 23. You also can get chlamydial eye infections (conjunctivitis) through contact with infected body fluids.
Lymphogranuloma venereum is caused by Chlamydia trachomatis serovars L1, L2, or L3; it is an uncommon infection in the United States, but sporadic cases and outbreaks have been reported among men who have sex with men (MSM), many of whom have HIV 24, 25. Rectal manifestations with lymphogranuloma venereum can include anorectal pain, purulent rectal discharge, rectal bleeding, tenesmus, diarrhea, and constipation, which is clinically diagnosed as proctitis 24, 25. Although most cases of lymphogranuloma venereum in the United States are rectal infections, lymphogranuloma venereum can also cause enlarged inguinal lymph nodes (lymphadenopathy) characterized by multiple, unilateral, enlarged, matted, tender inguinal lymph nodes, termed “buboes” that may suppurate 24, 25. Systemic signs and symptoms, such as fever, chills, or muscle ache (myalgia), also may be present with either rectal or inguinal manifestations 26. A self-limited genital ulcer sometimes occurs at the site of inoculation. Less often, oral ulceration can occur and may be associated with cervical adenopathy. Specimens from anogenital sites and lymph nodes can be obtained in an attempt to identify Chlamydia trachomatis by a nucleic acid amplification test (NAAT).
Sexually acquired chlamydial conjunctivitis can occur in both men and women through contact with infected genital secretions 27.
While chlamydia can also be found in the throats of women and men having oral sex with an infected partner, it is typically asymptomatic and not thought to be an important cause of pharyngitis 28.
At its worst, chlamydia can damage a woman’s fertility, making it difficult to get pregnant. Also, it can cause an ectopic pregnancy (pregnancy that develops outside the womb). An extremely serious ectopic pregnancy can lead to a woman’s death.
Estimates of the proportion of chlamydia-infected people who develop symptoms vary by setting and study methodology; two published studies that incorporated modeling techniques to address limitations of point prevalence surveys estimated that only about 10% of men and 5-30% of women with laboratory-confirmed chlamydial infection develop symptoms 29. The incubation period of chlamydia is poorly defined. However, given the relatively slow replication cycle of the organism, symptoms may not appear until several weeks after exposure in those persons who develop symptoms.
Figure 2. Chlamydia infection in eye
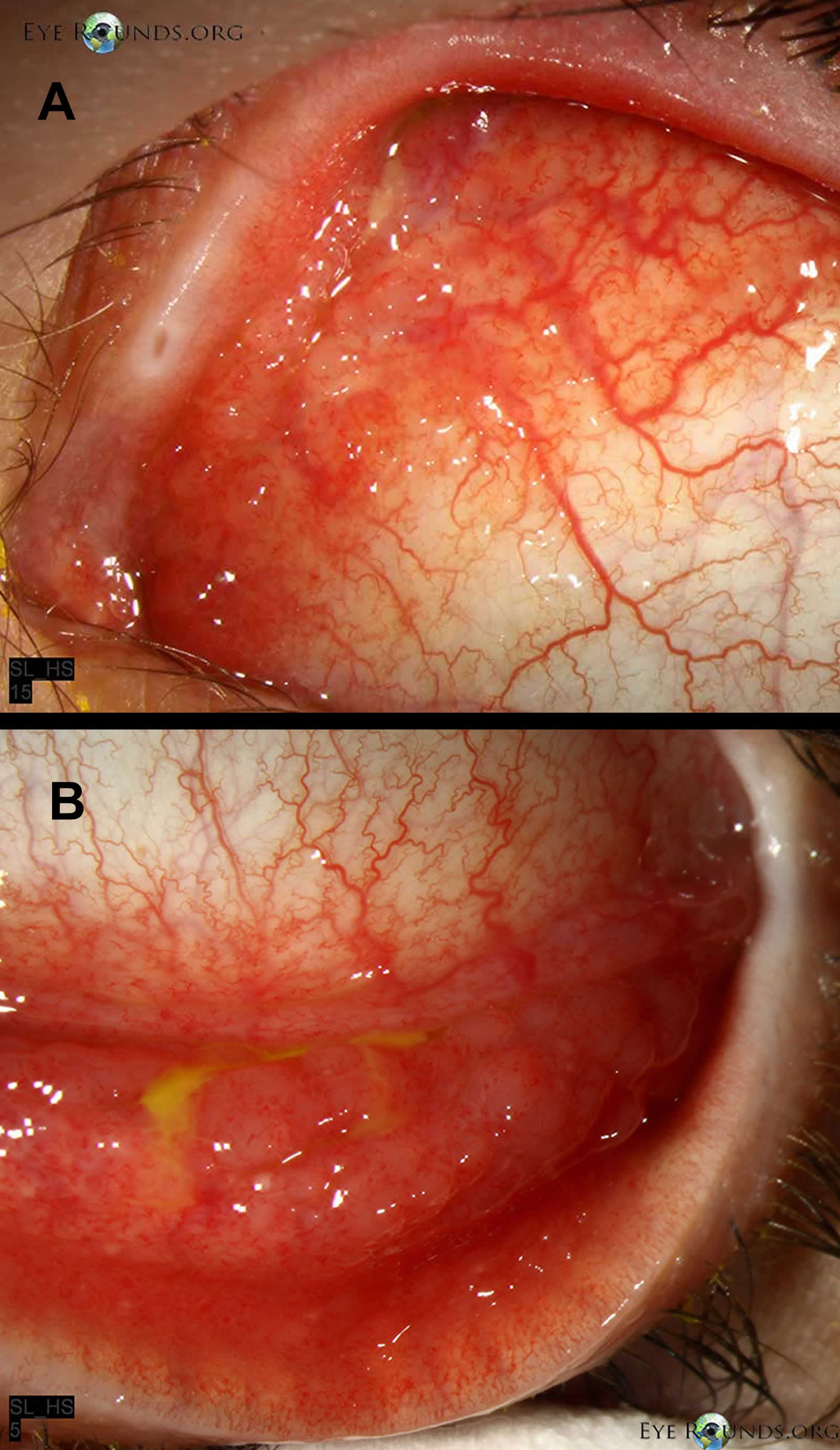
Footnote: (A) Follicles on the bulbar conjunctiva, characteristic of Chlamydia trachomatis infection. (B) Note the follicles in the inferior fornix
[Source 30 ]Chlamydia in women
Most women with urogenital chlamydia infection initially have no signs or symptoms, but may present later with a range of manifestations and complications. In women, the Chlamydia trachomatis bacteria initially infect the cervix, where the infection may cause signs and symptoms of cervicitis (e.g., mucopurulent endocervical discharge, easily induced endocervical bleeding), and sometimes the urethra, which may result in signs and symptoms of urethritis (e.g., pyuria, dysuria, urinary frequency). Infection can spread from the cervix to the upper reproductive tract (i.e., uterus, fallopian tubes), causing pelvic inflammatory disease (PID), which may be asymptomatic (“subclinical PID”) or acute, with typical symptoms of abdominal and/or pelvic pain, along with signs of cervical motion tenderness, and uterine or adnexal tenderness on examination 17, 18, 31.
Chlamydia symptoms in women include:
- Abnormal vaginal discharge, which may have a strong smell
- A burning sensation when urinating
If the infection spreads, you might get lower abdominal (belly) pain, pain during sex, nausea, and fever.
Figure 3. Female reproductive system
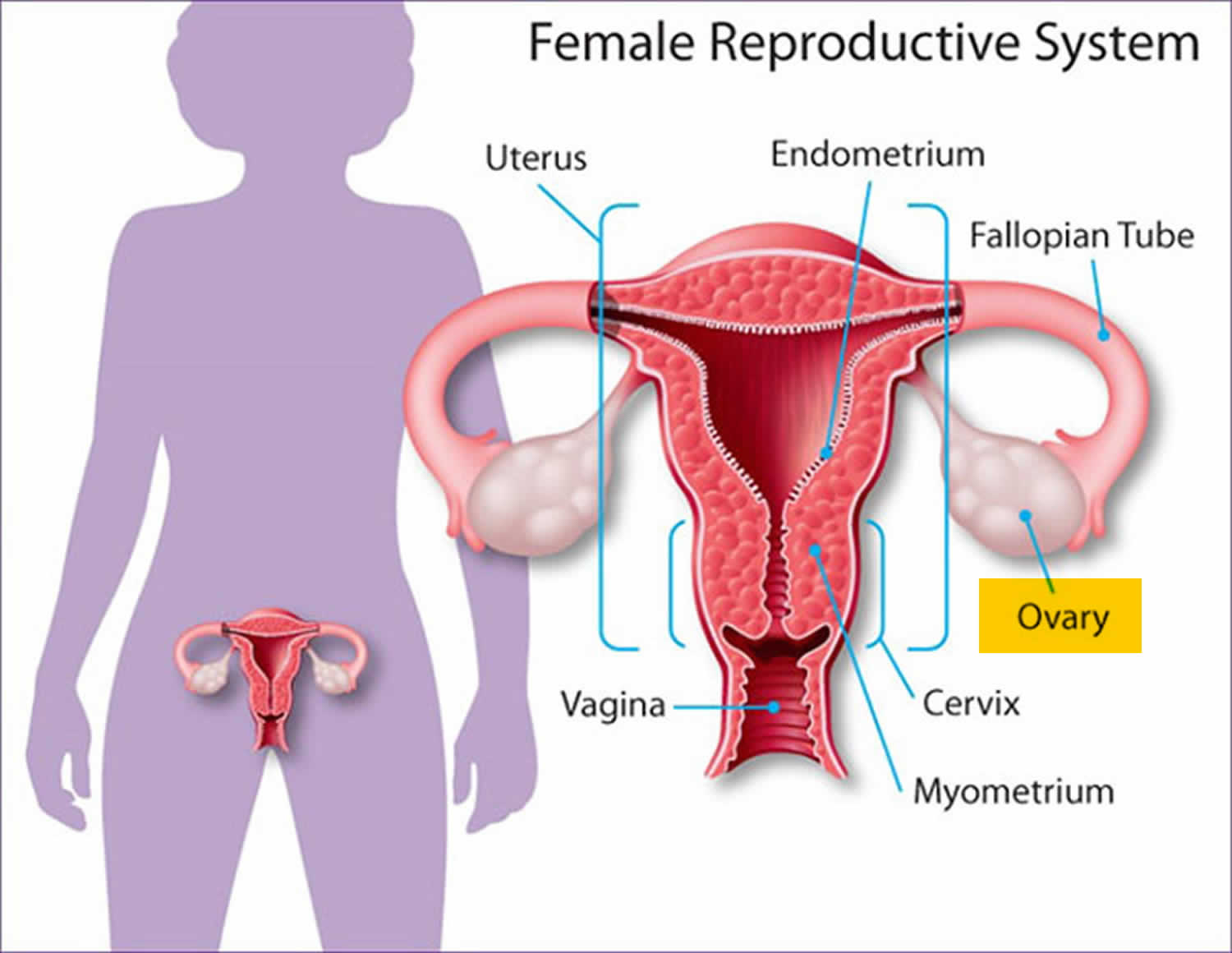
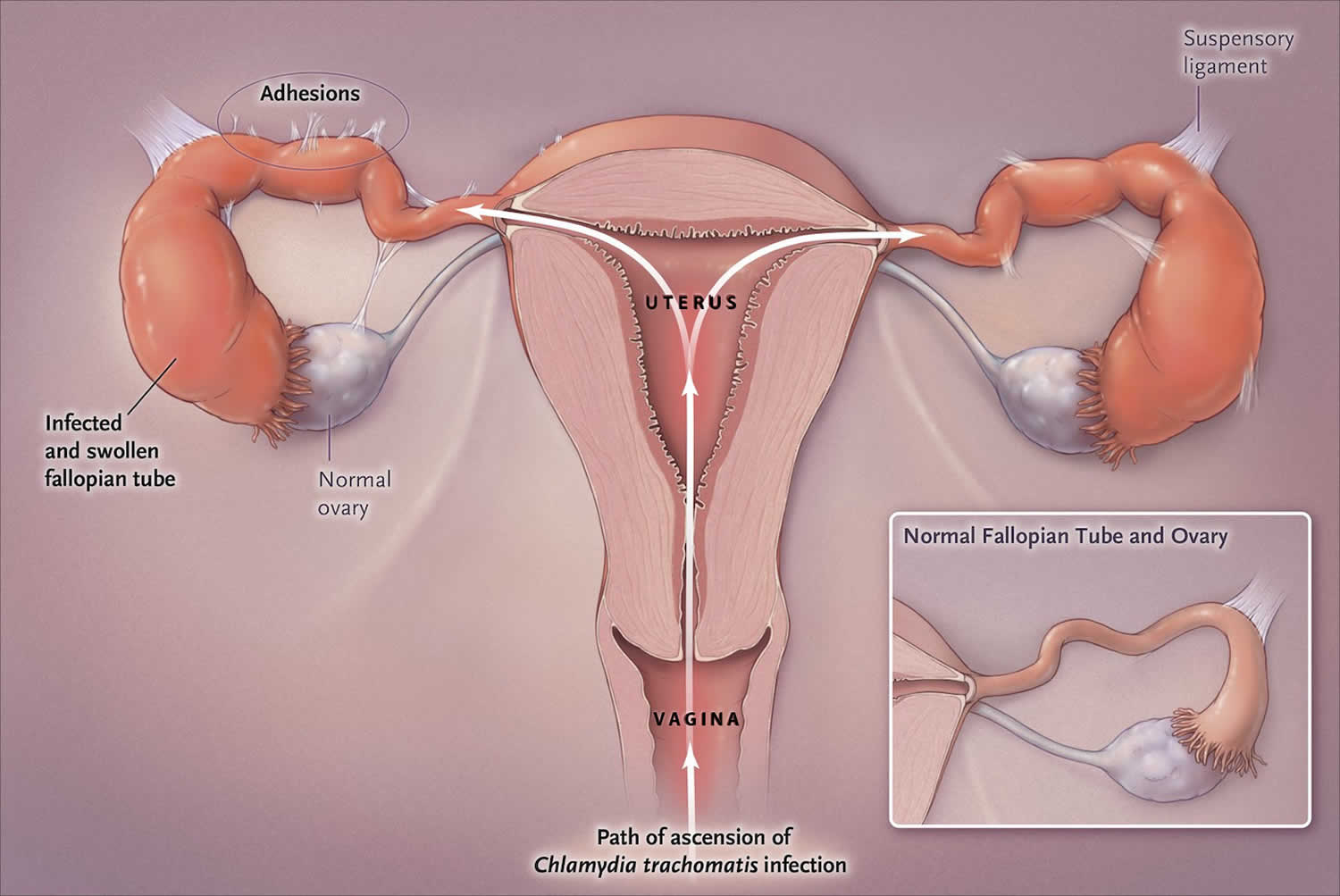
Figure 4. Chlamydia infection in the upper genital tract in women
Cervicitis
The cervix is the site of infection in 75 to 80% of women with chlamydial infection and most women with cervical chlamydial infection are asymptomatic. When symptoms are present, they are often nonspecific, such as vague abdominal discomfort or spotting. Typically, the clinical examination of the cervix is normal in women with cervical chlamydial infection, but some may have findings that suggest cervicitis, such as mucopurulent endocervical discharge and spontaneous (or easily induced) endocervical bleeding 19, 32. Causes of mucopurulent cervicitis other than Chlamydia trachomatis include Neisseria gonorrhoeae and Mycoplasma genitalium.
Urethritis
Urethral infection with chlamydia in women is usually asymptomatic, but it may cause painful urination (dysuria) and urinary frequency, which can mimic acute cystitis.[24] Nearly all women with urethral chlamydial infection also have cervical infection 33.
Pelvic inflammatory disease (PID)
Women with Chlamydia trachomatis infection can develop pelvic inflammatory disease (PID), which is a subclinical to acute clinical syndrome caused by the ascending spread of microorganisms from the cervix to the endometrium, fallopian tubes, ovaries, and contiguous structures (Figure 3) 18. Following untreated genital infection with Chlamydia trachomatis, pelvic inflammatory disease (PID) develops in approximately 3% of women within 2 weeks and in 10% of women within 1 year 34, 35. Although most women with PID caused by Chlamydia trachomatis initially have a mild or subclinical illness, some present with lower abdominal pain and may have findings of cervical motion tenderness, with or without uterine or ovary tenderness 20, 36. Chlamydia-associated pelvic inflammatory disease (PID) can result in fallopian tube scarring, which may lead to tubal factor infertility, increased risk for ectopic pregnancy, and chronic pelvic pain 18, 22. Among women treated for PID caused by chlamydia, approximately 20% become infertile, 30% develop chronic pain, and 1% have an ectopic pregnancy when they conceive 21. The extensive long-term morbidity associated with chlamydial infection underscores the importance of aggressive prevention, screening, and treatment programs 37.
Perihepatitis (Fitz-Hugh-Curtis Syndrome)
Untreated pelvic infection in women with Chlamydia trachomatis can infrequently cause inflammation of the liver capsule, which is commonly referred to as perihepatitis or the Fitz-Hugh-Curtis syndrome 38, 39. Although perihepatitis was initially attributed only to gonococcal infection, it is now known to be more often associated with chlamydial infection. Perihepatitis is characterized by right upper quadrant pain, nausea, vomiting, and fever, which are generally accompanied by evidence of pelvic inflammatory disease (PID) on physical examination 40.
Chlamydia in men
Men who are symptomatic typically have urethritis, with a mucoid or watery urethral discharge and painful urination (dysuria). A minority of infected men develop epididymitis (with or without symptomatic urethritis), presenting with unilateral testicular pain, tenderness, and swelling 41.
Chlamydia symptoms in men include:
- Discharge from your penis
- A burning sensation when urinating (peeing)
- Pain and swelling in one or both testicles (although this is less common)
If the chlamydia infects your rectum (in men or women), it can cause rectal pain, discharge, and bleeding.
Urethritis
The most common site for chlamydial infection in heterosexual men is the urethra. Although most men identified with urethral chlamydial infection have no symptoms, some will develop dysuria and urethral discharge, which is typically clear, mucoid, or mucopurulent; the clinical presentation is typically referred to as nongonococcal urethritis 42. Although attempts to distinguish gonococcal urethritis from nongonococcal urethritis on clinical examination are not reliable, the discharge caused by Chlamydia trachomatis is usually less purulent than with gonococcal urethritis.
Epididymitis
In males, epididymitis is the most common local complication of urethral Chlamydia trachomatis infection, and men with this complication typically develop unilateral scrotal pain, epididymal swelling, and tenderness 43. For men with epididymitis who have concomitant urethral discharge, most have at least 2 white blood cells per high power field on Gram’s staining of a urethral discharge specimen. Approximately 70% of sexually transmitted cases of epididymitis are due to Chlamydia trachomatis 43.
Chlamydia infections in infants and children
Although chlamydial infections are now seen infrequently among infants and children in the United States, they are still found in the cases of inadequate prenatal care. Among cases of perinatal chlamydial infection, the most common presentation is inclusion conjunctivitis, which occurs in about 25% of neonates born to mothers who have untreated cervical chlamydia infection. The second most common manifestation is neonatal pneumonia, and this occurs in only about 10 to 15% of infants of mothers who have untreated cervical chlamydia.
Conjunctivitis
For infants, conjunctivitis is the most common clinical condition resulting from perinatal transmission of chlamydia. Ocular infection with Chlamydia trachomatis results from exposure of the neonate to infected secretions from the mother’s genital tract during birth, and the exposure may also involve mucous membranes of the oropharynx, urogenital tract, and rectum. Inclusion conjunctivitis occurs 5 to 14 days after delivery. The signs range from mild scant mucoid discharge to severe copious purulent discharge, chemosis, pseudomembrane formation, erythema, friability, and edema. Neonatal ocular prophylaxis with silver nitrate solution or antibiotic ointments for prevention of gonorrhea transmission does not prevent perinatal transmission of Chlamydia trachomatis from mother to infant. A chlamydial etiology should be considered for all infants aged 30 days or younger who have conjunctivitis.
Pneumonia
Chlamydial pneumonia in infants occurs 4 to 12 weeks after delivery. Notably, infection of the nasopharynx is thought to be a precursor condition that is usually asymptomatic, but can progress to pneumonia. The signs are cough, congestion, and tachypnea. Infants are usually afebrile, and rales are apparent with auscultation of the lungs.
Trachoma
Urogenital infection
Urogenital infections in preadolescent males and females are usually asymptomatic and can be the result of vertical transmission during the perinatal period 17. Genital or rectal infection can persist for as long as 2 to 3 years, so infection in young children may be the result of perinatally-acquired infection. Sexual abuse is a major concern when chlamydia (or any STD) is detected in preadolescent males or females. STD evaluation in a case of suspected abuse should be performed by, or in consultation with, an expert in the assessment of child sexual abuse. Only tests with high specificity should be used because of the legal and psychosocial consequences of a false-positive diagnosis.
Chlamydia complications
Chlamydia infection can be associated with:
- Pelvic inflammatory disease (PID). PID is an infection of the uterus and fallopian tubes that causes pelvic pain and fever. Severe infections might require hospitalization for intravenous antibiotics. PID can damage the fallopian tubes, ovaries and uterus, including the cervix.
- Infection of the epididymis (the tube that carries sperm) also known as epididymitis. A chlamydia infection can inflame the coiled tube located beside each testicle (epididymis). The infection can result in fever, scrotal pain and swelling.
- Prostate gland infection (prostatitis). Rarely, the chlamydia organism can spread to a man’s prostate gland. Prostatitis can cause pain during or after sex, fever and chills, painful urination, and lower back pain.
- Infections in newborns. The chlamydia infection can pass from the vaginal canal to your child during delivery, causing pneumonia or a serious eye infection (conjunctivitis).
- Ectopic pregnancy. This occurs when a fertilized egg implants and grows outside of the uterus, usually in a fallopian tube. The pregnancy needs to be removed to prevent life-threatening complications, such as a burst tube. A chlamydia infection increases this risk.
- Infertility. Chlamydia infections — even those that produce no signs or symptoms — can cause scarring and obstruction in the fallopian tubes, which might make women infertile.
- Reactive arthritis also known as Reiter’s syndrome. People who have Chlamydia trachomatis are at higher risk of developing reactive arthritis. This condition typically affects the joints, eyes and urethra — the tube that carries urine from your bladder to outside of your body.
In women, an untreated chlamydia infection can spread to your uterus (womb) and fallopian tubes, causing pelvic inflammatory disease (PID). PID can cause permanent damage to your reproductive system. This can lead to long-term pelvic pain, infertility, and ectopic pregnancy. Women who have had chlamydia infections more than once are at higher risk of serious reproductive health complications.
Men often don’t have health problems from chlamydia. Sometimes it can infect the epididymis (the tube that carries sperm) causing epididymitis. This can cause pain, fever, and, rarely, infertility.
Both men and women can develop reactive arthritis because of a chlamydia infection. Reactive arthritis is a type of arthritis that happens as a “reaction” to an infection in the body.
Babies born to infected mothers can get chlamydia eye infection (conjunctivitis) and pneumonia from chlamydia 9. It may also make it more likely for your baby to be born too early (premature birth).
Untreated chlamydia may also increase your chances of getting or giving HIV.
Chlamydia diagnosis
Laboratory tests can diagnose chlamydia 47. Your doctor may ask you to provide a urine sample for testing, or they might use a cotton swab to get a vaginal sample. For women, your doctor will swab (with a long cotton swab) the inside of the vagina. For men, your doctor will swab the inside of the end of the penis. A urine test also may be required. This involves peeing in a cup provided by the doctor’s office. The urine sample is sent to a lab to be tested. If you are pregnant, your doctor may check you for chlamydia even if you have no signs of the disease. Chlamydia can be extremely dangerous to a newborn.
The Centers for Disease Control and Prevention (CDC) recommends chlamydia screening for:
- Sexually active women age 25 or younger. The rate of chlamydia infection is highest in this group, so a yearly screening test is recommended. Even if you’ve been tested in the past year, get tested when you have a new sex partner.
- Pregnant women. You should be tested for chlamydia during your first prenatal exam. If you have a high risk of infection — from changing sex partners or because your regular partner might be infected — get tested again later in your pregnancy.
- Women and men at high risk. People who have multiple sex partners, who don’t always use a condom or men who have sex with men should consider frequent chlamydia screening. Other markers of high risk are current infection with another sexually transmitted infection and possible exposure to an STD through an infected partner.
Screening and diagnosis of chlamydia is relatively simple. Tests include:
- A urine test. A sample of your urine is analyzed in the laboratory for presence of this infection.
- A swab. For women, your doctor takes a swab of the discharge from your cervix for culture or antigen testing for chlamydia. This can be done during a routine Pap test. Some women prefer to swab their vaginas themselves, which has been shown to be as diagnostic as doctor-obtained swabs.
- For men, your doctor inserts a slim swab into the end of your penis to get a sample from the urethra. In some cases, your doctor will swab the anus.
If you’ve been treated for an initial chlamydia infection, you should be retested in about three months.
Because chlamydia is usually asymptomatic, screening is necessary to identify most infections. Screening programs have been demonstrated to reduce rates of adverse sequelae in women 48. CDC recommends yearly chlamydia screening of all sexually active women younger than 25, as well as older women with risk factors such as new or multiple partners, or a sex partner who has a sexually transmitted infection 49. Pregnant women should be screened during their first prenatal care visit. Pregnant women under 25 or at increased risk for chlamydia (e.g., women who have a new or more than one sex partner) should be screened again in their third trimester 49. Women diagnosed with chlamydial infection should be retested approximately 3 months after treatment 49. Any woman who is sexually active should discuss her risk factors with a health care provider who can then determine if more frequent screening is necessary.
Routine screening is not recommended for men. However, the screening of sexually active young men should be considered in clinical settings with a high prevalence of chlamydia (e.g., adolescent clinics, correctional facilities, and STD clinics) when resources permit and do not hinder screening efforts in women 49.
Sexually active men who have sex with men who had insertive intercourse should be screened for urethral chlamydial infection and men who have sex with men who had receptive anal intercourse should be screened for rectal infection at least annually; screening for pharyngeal infection is not recommended.. More frequent chlamydia screening at 3-month intervals is indicated for men who have sex with men, including those with HIV infection, if risk behaviors persist or if they or their sexual partners have multiple partners 49.
At the initial HIV care visit, providers should test all sexually active persons with HIV infection for chlamydia and perform testing at least annually during the course of HIV care. A patient’s health care provider might determine more frequent screening is necessary, based on the patient’s risk factors.
Chlamydia test
There are a number of diagnostic tests for chlamydia, including nucleic acid amplification tests (NAATs), cell culture, and others. Nucleic acid amplification tests (NAATs) are the most sensitive tests, and can be performed on easily obtainable specimens such as vaginal swabs (either clinician- or patient-collected) or urine 50.
Vaginal swabs, either patient- or clinician-collected, are the optimal specimen to screen for genital chlamydia using NAATs in women; urine is the specimen of choice for men, and is an effective alternative specimen type for women 50. Self-collected vaginal swab specimens perform at least as well as other approved specimens using NAATs 51. In addition, patients may prefer self-collected vaginal swabs or urine-based screening to the more invasive endocervical or urethral swab specimens 52. Adolescent girls may be particularly good candidates for self-collected vaginal swab- or urine-based screening because pelvic exams are not indicated if they are asymptomatic.
Chlamydial culture can be used for rectal or pharyngeal specimens, but is not widely available. Nucleic acid amplification tests (NAATs) have demonstrated improved sensitivity and specificity compared with culture for the detection of Chlamydia trachomatis at non-genital sites 53. Most tests, including NAATs, are not FDA-cleared for use with rectal or pharyngeal swab specimens; however, NAATS have demonstrated improved sensitivity and specificity compared with culture for the detection of Chlamydia trachomatis at rectal sites 53 and however, some laboratories have met regulatory requirements and have validated NAAT testing on rectal and pharyngeal swab specimens.
Nucleic Acid Amplification Test (NAAT)
Nucleic acid amplification tests (NAATs) amplify nucleic acid sequences (either DNA or RNA) that are specific for the organism being detected. Similar to other nonculture tests, nucleic acid amplification tests (NAATs) can detect replicating or nonviable organisms. Multiple commercially available NAATs are FDA-cleared as diagnostic tests for Chlamydia trachomatis on urine specimens from men and women, urethral secretions in men, and endocervical swabs in women; some tests are cleared for vaginal swabs 17. In addition, in May 2019, the United States Food and Drug Administration (FDA) cleared two NAATs for diagnostic testing of chlamydia at extragenital sites (pharynx and rectum); the two tests are the Aptima Combo 2 Assay and the Xpert CT/NG 54. For chlamydia testing in men, NAATs are highly sensitive for detecting Chlamydia trachomatis in either urethral secretions or a first-catch urine specimen, but most experts prefer using first-catch urine samples 17. For women, vaginal swabs are preferred over urine samples since they are more sensitive than urine samples 17. Several studies have shown that self-collected vaginal swabs are preferred by women and perform equal to or better than clinician-collected vaginal swabs 55, 56. In addition, in men and women, self-collected rectal swabs for NAAT have also performed well 57. Nucleic acid amplification tests do not distinguish non-lymphogranuloma venereum (non-LGV) from lymphogranuloma venereum (LGV) strains.
Point-of-Care NAAT Testing
In March 2021, the FDA approved the first point-of-care nucleic acid amplification test (NAAT) (Binx Health IO CT/NG Assay) for the diagnosis of urogenital chlamydia and gonorrhea 58. This point-of-care test can be run on vaginal swabs obtained from women or on urine samples collected from men 58. This assay can provide a result in approximately 30 minutes 58. In a cross-sectional study, investigators evaluated this point-of-care NAAT for the diagnosis of chlamydia and gonorrhea using vaginal swabs obtained from 1,523 women and urine samples collected from 922 men 59. For chlamydia, the sensitivity estimates were 96.1% in women and 92.5% in men; the specificity estimates were 99.1% for women and 99.3% for men 59. In addition, the investigators found that self-obtained vaginal swabs in women performed equivalent to clinician-collected vaginal swabs 59.
Non-amplification molecular tests
Molecular tests that do not use nucleic acid amplification encompass a variety of antigen detection and nucleic acid hybridization methods. These tests include enzyme-immunoassays (EIA), direct fluorescent antibody tests (DFA), and nucleic acid hybridization tests—a distinct non-NAAT methodology that can detect C. trachomatis-specific DNA or RNA sequences in ribosomal RNA, genomic DNA, or plasmid DNA. All have a significantly lower sensitivity (range 50% to 75%) than NAATs 60. These non-amplification tests are rarely used in clinical practice, and they are classified as not recommended by the Centers for Disease Control and Prevention (CDC) 17.
Culture
Historically, cell culture to detect Chlamydia trachomatis was the most sensitive and specific method available to detect chlamydial infection. Cell culture, however, is technically complex, expensive, difficult to standardize, and has a lower sensitivity than amplification tests. In addition, performing Chlamydia trachomatis cell culture requires collection of Chlamydia trachomatis elementary bodies from relevant anatomical site(s) and use of stringent transport requirements. Because of their excellent sensitivity and specificity, NAATs have replaced the use of culture in most clinical situations; the use of culture for Chlamydia trachomatis is primarily limited to evaluation of suspected cases of sexual abuse in children 61.
Serology
Serologic testing is rarely used in clinical practice to diagnose genital infections caused by Chlamydia trachomatis and chlamydia serologic tests do not reliably distinguish current from prior infection. Two main types of serologic tests are used for diagnosis: (1) chlamydia complement fixation test (CFT), which measures antibody against group-specific lipopolysaccharide antigen, and (2) microimmunofluorescence (MIF) 47.
Diagnosing lymphogranuloma venereum
Since routinely used NAATs for diagnosing chlamydial infections do not distinguish non-lymphogranuloma venereum (non-LGV) strains of Chlamydia trachomatis from lymphogranuloma venereum (LGV) strains, additional diagnostic methods, such as lymphogranuloma venereum-specific molecular testing with PCR genotyping, are required to make a laboratory diagnosis of lymphogranuloma venereum (LGV). These molecular tests, however, are not widely available and results do not return within a time frame that would alter clinical management 62. In addition, chlamydia serologic testing is not recommended for diagnosing lymphogranuloma venereum (LGV) 63. Therefore, the diagnosis of lymphogranuloma venereum (LGV) should be based on epidemiologic information, compatible clinical findings, and a positive Chlamydia trachomatis NAAT at the symptomatic anatomic site 63.
Chlamydia treatment
Chlamydia can be easily cured with antibiotics. HIV-positive persons with chlamydia should receive the same treatment as those who are HIV-negative.
Recommended antibiotics for chlamydial infection among adolescents and adults 64:
- Doxycycline 100 mg orally 2 times/day for 7 days
Alternative Regimens
- Azithromycin 1 g orally in a single dose
- OR
- Levofloxacin 500 mg orally once daily for 7 days
Treatment of chlamydial infections during pregnancy
The recommended regimen for the treatment of chlamydial infections in pregnant women is azithromycin 1 gram orally in a single dose; amoxicillin is the alternative medication 17. Doxycycline and levofloxacin are not recommended for the treatment of chlamydial infections in pregnancy 17. Erythromycin is no longer recommended for the treatment of chlamydia during pregnancy due to gastrointestinal side effects that make adherence challenging for the mother during pregnancy. All pregnant women treated for chlamydial infection should have a test-of-cure performed 4 weeks after completing therapy and all should be retested 3 months after treatment for reinfection 17.
Adults with oropharyngeal chlamydial infections
The clinical significance of oropharyngeal Chlamydia trachomatis infection remains unclear, and routine screening for oropharyngeal Chlamydia trachomatis infection is not recommended. Nevertheless, since oropharyngeal C. trachomatis can be transmitted to genital sites of sex partners 65, 66, detection of Chlamydia trachomatis from an oropharyngeal sample warrants the same treatment as with urogenital chlamydial infection: doxycycline 100 mg orally twice daily for 7 days as the preferred regimen for nonpregnant adults and azithromycin 1 gram single dose orally preferred for pregnant persons 17.
Treatment for lymphogranuloma venereum
The recommended treatment for Chlamydia trachomatis infections caused by lymphogranuloma venereum strains is oral doxycycline 100 mg twice daily for 21 days; note this treatment is significantly longer than the 7-day treatment for non-lymphogranuloma venereum chlamydia strains 17. The alternative lymphogranuloma venereum treatment regimens include oral azithromycin 1 gram weekly for 3 weeks or oral erythromycin base 500 mg four times daily for 21 days 63. Since practical laboratory diagnostic methods are not available for making a timely diagnosis of lymphogranuloma venereum, the indication to provide lymphogranuloma venereum treatment (doxycycline 100 mg twice daily for 21 days) should be based on epidemiologic information, compatible clinical finding, and a positive Chlamydia trachomatis NAAT at the symptomatic anatomic site 63. In addition, empiric therapy for lymphogranuloma venereum is indicated for persons in whom (1) symptoms or signs of proctocolitis (e.g. bloody discharge, tenesmus, or ulceration), (2) those with severe inguinal lymphadenopathy with bubo formation, especially if the individual reports recently having a genital ulcer, and (3) persons with a genital ulcer and other causes for the genital ulcer have been excluded 63.
Management of sex partners
For persons diagnosed with urogenital chlamydial infection, all sex partners with whom they had sexual contact during the 60 days preceding the onset of symptoms or chlamydia diagnosis should be referred for evaluation, testing, and presumptive treatment of chlamydia 17. If no sex contacts have occurred in the 60 days before the diagnosis of chlamydia or onset of symptoms, then the most recent sex partner prior to that 60-day period should be evaluated and treated 17. All sex contacts should have testing for STDs as part of the evaluation process. The sex contacts should receive presumptive treatment for chlamydia without waiting for their STD test results to ensure the treatment does not depend on an additional follow-up visit. The empiric treatment for nonpregnant sex contacts is oral doxycycline 100 mg twice daily for 7 days and for pregnant contacts it is azithromycin 1 gram orally as a single dose. The purpose of performing an evaluation for the contact, even if they will receive presumptive treatment, is to perform counseling and screening for other STDs, which may require treatment. For neonates or infants diagnosed with chlamydial infection, it is important that mothers and their sex partners undergo diagnostic evaluation and receive empiric treatment for chlamydial infection.
Use of expedited partner therapy
Certain situations may arise in which sexual contacts are unable or unwilling to present for evaluation, testing, and treatment. In this scenario, there may be an option to provide expedited partner therapy (EPT)—a process whereby the patient diagnosed with chlamydia delivers treatment (or a prescription for treatment)—to the recent sex partner, without a medical provider examining the partner. This strategy has been demonstrated to decrease the rate of recurrent or persistent chlamydia infection 67, 68, 69. There are concerns regarding the use of expedited partner therapy for men who have sex with men, since, ideally, these individuals would get tested for other STDs, such as syphilis and HIV, during a clinic visit 17. The use of expedited partner therapy for men who have sex with men should therefore be performed on a shared-decision basis. Finally, expedited partner therapy is not legal in all states; the CDC maintains an updated information page (Legal Status of Expedited Partner Therapy) that identifies the legal status of expedited partner therapy in each state in the United States.
Infants born to mothers with chlamydial infection
When neonatal chlamydial infection occurs, it results from neonatal contact with a chlamydia-infected cervix during the birth process. Neonatal chlamydial infection most often manifests as conjunctivitis (ophthalmia neonatorum) that develops 5 to 12 days after birth or as a subacute, afebrile pneumonia with onset at ages 1 to 3 months. The erythromycin eye ointment that is routinely given to neonates at birth to prevent neonatal gonococcal ophthalmia neonatorum does not prevent neonatal chlamydial eye infection 17. The most effective strategy for preventing perinatal chlamydia transmission is to screen pregnant women for chlamydial infection and promptly treat those women who test positive. Prophylactic antibiotic treatment is not recommended for infants who are born to mothers at high risk for chlamydia or who have untreated chlamydia. In this situation, the recommended approach is to monitor the infant for signs and symptoms of chlamydial infection and promptly evaluate and treat any documented infection in the neonate 17.
Neonates with ophthalmia neonatorum
The recommended treatment regimen for the neonate with ophthalmia neonatorum is a 14-day course of oral erythromycin base or erythromycin ethylsuccinate 17. Data on oral azithromycin for the treatment of neonatal chlamydial infection are limited, but a small study suggested a short 3-day course of azithromycin may be effective.[93] The use of topical erythromycin alone is not effective for ophthalmia neonatorum, and it is not recommended for use in combination with oral antibiotics 17. The use of a recommended or alternative therapy has an efficacy of only approximately 80% and some infants require treatment with a second course of antibiotics. Treatment with oral erythromycin or oral azithromycin in infants during the first 6 weeks of life has been associated with an increased risk of infantile hypertrophic pyloric stenosis 70, 71. Thus, all infants with chlamydial ophthalmia neonatorum should have close follow-up to determine the treatment response and to evaluate signs and symptoms of infantile hypertrophic pyloric stenosis 70.
Infant pneumonia
For infants with pneumonia caused by Chlamydia trachomatis, the recommended treatment is a 14-day regimen of oral erythromycin base or erythromycin ethylsuccinate; the alternative regimen is a 3-day course of oral azithromycin 17. The treatment for chlamydial pneumonia in neonates often occurs empirically, based on the infant’s chest radiographic findings, the age of the infant, and the mother’s epidemiologic risk for chlamydial infection 17. In situations when presumptive therapy is used in a situation with a high degree of suspicion of chlamydial infection, and there is considerable concern that follow-up will not occur, the 3-day azithromycin alternative regimen can be used 17.
Chlamydial infections in infants and children
The treatment of infants and children with chlamydia is stratified into three groups: (1) younger than 8 years of age and weight less than 45 kg, (2) younger than 8 years of age and weight 45 kg or greater, and (3) age 8 or older 17. In infants and children who weigh less than 45 kg, the preferred treatment of chlamydial infections is a 14-day course of oral erythromycin base or oral erythromycin ethylsuccinate 17. For children younger than 8 years of age and weighing 45 kg or greater, the recommended regimen is single-dose oral azithromycin. Children older than 8 years of age should be treated with single-dose oral azithromycin or a 7-day course of oral doxycycline 17. A follow-up visit with chlamydia test-of-cure is recommended approximately 4 weeks after completion of treatment to evaluate for treatment effectiveness 17.
Chlamydia prognosis
Antibiotic treatment has a 95% effectiveness rate for first-time chlamydia therapy 72. The prognosis is excellent with prompt initiation of treatment early and with the completion of the entire course of antibiotics. Although treatment failures with primary therapies are quite rare, chlamydia relapse may occur. Chlamydia reinfection is common and is usually related to the nontreatment of infected sexual partners or acquisition from a new partner. Death is rare but can be caused by progression to salpingitis and tubo-ovarian abscess with rupture and peritonitis. The most significant morbidity occurs with repetitive infection with chlamydia, which leads to scarring of the fallopian tubes and subsequent infertility.
Gonorrhea
Gonorrhea also known as ‘the clap’, is a sexually transmitted disease (sexually transmitted infection) caused by the Gram-negative diplococci Neisseria gonorrhoeae (gonorrhea) bacteria (Figure 8). Gonorrhea is most common in young adults. Reported cases of gonorrhea have increased significantly in recent years, particularly among sexually active persons who are 15 to 24 years of age 73. The Neisseria gonorrhoeae bacteria or gonorrhea bacteria that cause gonorrhea can infect the genital tract, including the cervix (the opening of the uterus at the top of the vagina), uterus and fallopian tubes in women, and the urethra (the tube for urine) in women and men. Neisseria gonorrhoeae bacteria can also infect the mucous membranes of your mouth, throat, eyes, and rectum 74. You can get gonorrhea during vaginal, oral, or anal sex with an infected partner. A pregnant woman can pass gonorrhea to her baby during childbirth. In babies, gonorrhea most commonly affects the eyes.
In the United States, an estimated 1,568,000 new Neisseria gonorrhoeae infections occur each year (141,838), and gonorrhea is the second most common notifiable sexually transmitted infection (STD) in the United States and is a major public health problem 75. Infections due to gonorrhea (Neisseria gonorrhoeae), like those resulting from Chlamydia trachomatis, are a major cause of pelvic inflammatory disease (PID) in the United States. Pelvic inflammatory disease (PID) can lead to serious outcomes in women, such as tubal infertility, ectopic pregnancy, and chronic pelvic pain. In addition, epidemiologic and biologic studies provide evidence that gonococcal infections facilitate the transmission of HIV infection 76. For 2017, the rate of reported gonorrhea cases among men (202.5 cases per 100,000 males) was significantly higher than among women (141.8 cases per 100,000 females) 77. Over the 1-year period of 2016–2017, the rates of reported gonorrhea increased 19.3% among men and 17.8% among women 77. In 2017, the highest rates of gonorrhea among women were observed among those aged 20-24 years (648.8 cases per 100,000 females) and 15-19 years (557.4 cases per 100,000 females). Among men, the rate was highest among those aged 20-24 years (705.2 cases per 100,000 males) and 25–29 years (645.9 cases per 100,000 males) 77.
Gonorrhea often has no symptoms 78, 79:
- In men, gonorrhea can cause pain when urinating and thick, yellow discharge from the penis. The opening of the penis may be sore. If untreated, it can cause problems with the prostate and testicles, causing permanent damage and infertility in men.
- In women, the early symptoms of gonorrhea often are mild. Later, it can cause bleeding between periods, heavy bleeding during a period, fever, pain when urinating, and increased white, green, yellow, or bloody discharge from the vagina. If untreated, it can lead to pelvic inflammatory disease (PID), which causes problems with pregnancy and infertility.
- Both women and men can get sore throats if they’ve had oral contact with an infected person.
Gonorrhea can cause serious complications if it’s not treated.
If you think you have gonorrhea it is important to see a doctor as soon as possible. Your doctor can confirm the diagnosis with testing and start treatment. Treatment is with antibiotics. Treating gonorrhea is becoming more difficult because drug-resistant strains are increasing. Correct usage of latex condoms greatly reduces, but does not eliminate, the risk of catching or spreading gonorrhea. The most reliable way to avoid gonorrhea infection is to not have anal, vaginal, or oral sex.
Gonorrhea can be effectively treated with antibiotics. Sometimes you may need to be re-tested after your treatment to make sure the treatment has worked.
It is important to avoid having sex, even with a condom, until treatment is finished and tests show you are cured.
It is also very important to tell all your sexual partners from the past three months that you have been diagnosed with gonorrhea. They will need to be tested for gonorrhea and treated if infected.
Your doctor will help you decide who you need to tell and how you can tell them.
Figure 5. Gonorrhea eye infection
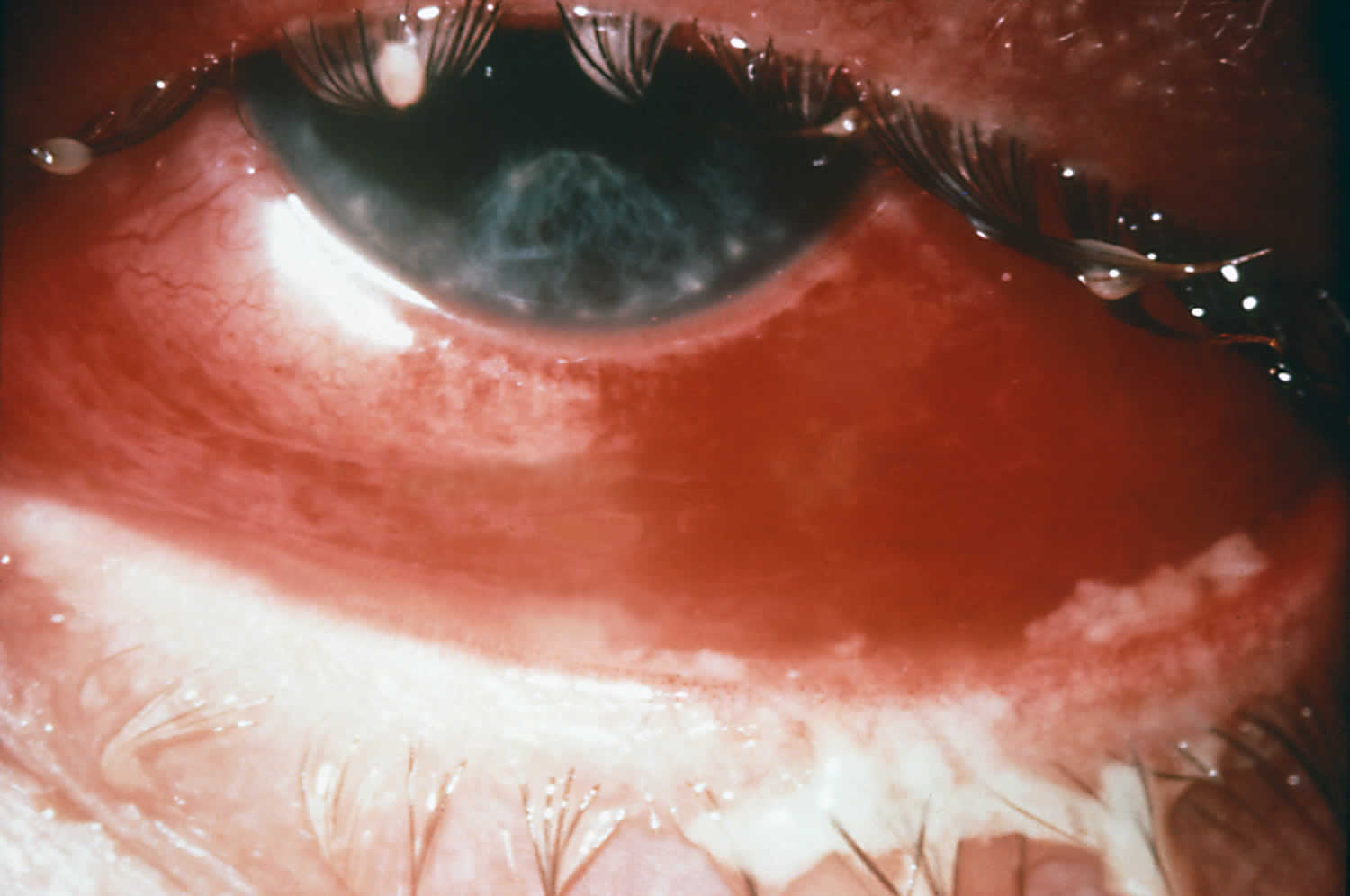
Figure 6. Gonorrhea skin rash

Figure 7. Disseminated gonococcal infection with arthritis

Figure 8. Neisseria gonorrhoeae bacteria
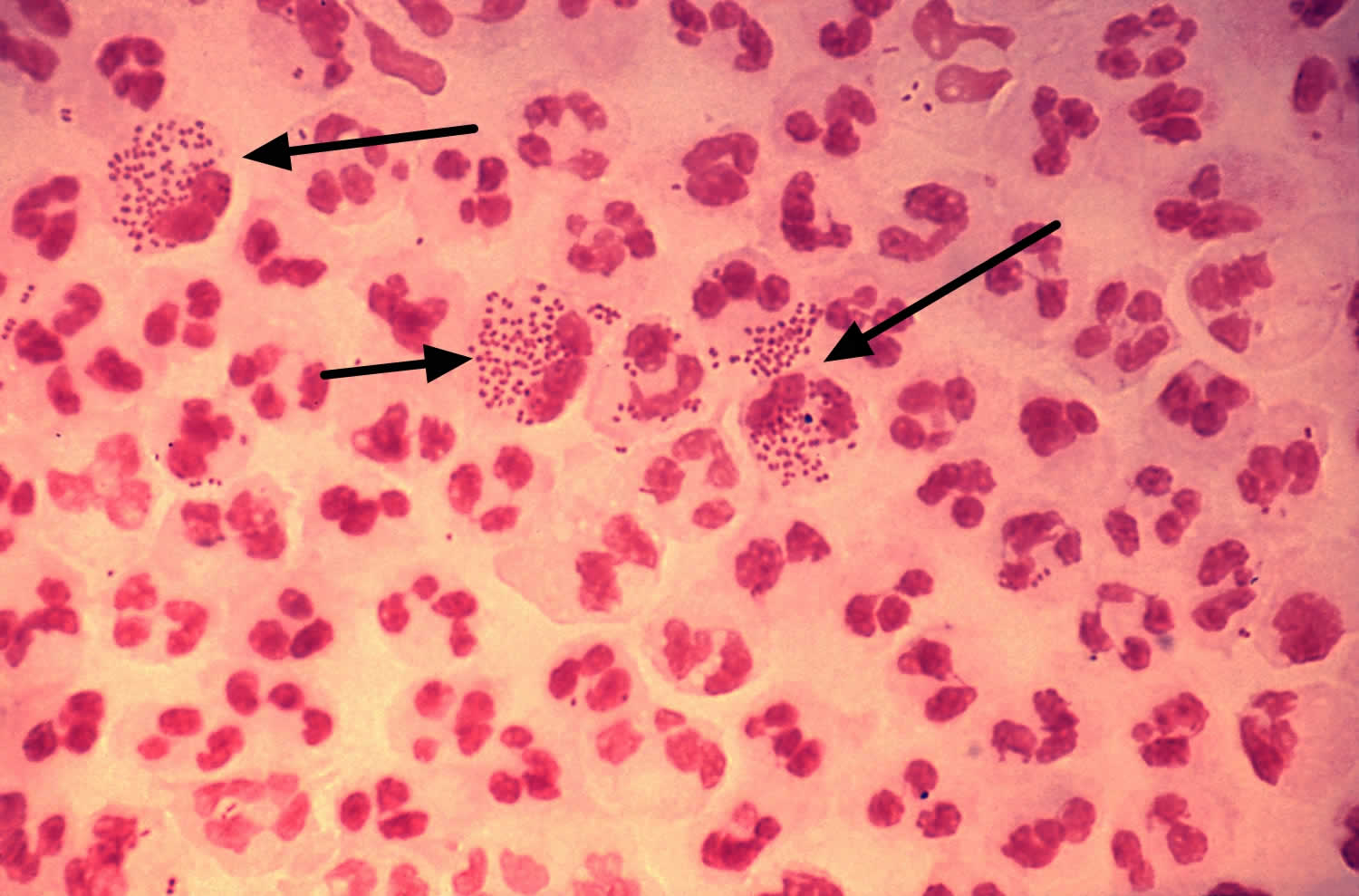
Footnotes: This low-resolution photomicrograph reveals the histopathology in an acute case of gonococcal urethritis using Gram-stain technique, demonstrated the presence of Gram-negative diplococci (black arrows). This slide is used to demonstrate the non-random distribution of Neisseria gonorrhoeae bacteria among polymorphonuclear neutrophils (a type of white blood cell). Note that there are both intracellular (inside the cell) and extracellular (outside the cell) gonorrhea bacteria in the field of view. For a presumptive diagnosis of gonorrhea to be made, additional tests would need to still be conducted.
[Source 81 ]Make an appointment with your doctor if you notice any troubling signs or symptoms, such as a burning sensation when you urinate or a pus-like discharge from your penis, vagina or rectum.
Also make an appointment with your doctor if your partner has been diagnosed with gonorrhea. You may not experience signs or symptoms that prompt you to seek medical attention. But without treatment, you can reinfect your partner even after he or she has been treated for gonorrhea.
What causes gonorrhea?
Gonorrhea is caused by infection with the bacterium Neisseria gonorrhea (Figure 8) and is spread by having unprotected vaginal, anal or oral sex with an infected person with gonorrhea. It can be passed by fingers or hands from the genitals to the eyes.
Gonorrhea can also be passed from an infected mother to her baby during birth, which can cause eye infection (neonatal conjunctivitis) and even blindness.
How does gonorrhea spread?
You can get gonorrhea by having vaginal, anal, or oral sex with someone who has gonorrhea. A pregnant person with gonorrhea can give the infection to their baby during childbirth.
How can I reduce my risk of getting gonorrhea?
The only way to completely avoid sexually transmitted diseases (STDs) is to not have vaginal, anal, or oral sex.
If you are sexually active, the following things can lower your chances of getting gonorrhea:
- Being in a long-term mutually monogamous relationship with a partner who has been tested and does not have gonorrhea.
- Using condoms the right way every time you have sex.
Am I at risk for gonorrhea?
Sexually active people can get gonorrhea through vaginal, anal, or oral sex without a condom with a partner who has gonorrhea.
If you are sexually active, have an honest and open talk with your healthcare provider. Ask them if you should get tested for gonorrhea or other STDs. If you are a sexually active gay or bisexual man, you should get tested for gonorrhea every year. If you are a sexually active woman, you should get tested for gonorrhea every year if you are:
- Younger than 25 years.
- 25 years and older with risk factors, such as new or multiple sex partners, or a sex partner who has a sexually transmitted infection.
I’m pregnant. How does gonorrhea affect my baby?
If you are pregnant and have gonorrhea, you can give the infection to your baby as your baby passes through your birth canal during delivery. This can cause cause blindness, joint infection, or a life-threatening blood infection in your baby 82. If you are pregnant, talk to your healthcare provider about getting the correct examination, testing, and treatment. Treating gonorrhea as soon as possible will make health problems for your baby less likely.
Gonorrhea infection in children
Perinatal infections most often occur during childbirth when the neonatal conjunctiva, pharynx, respiratory tract, or anal canal may become infected. Conjunctivitis (ophthalmia neonatorum) is preventable by ocular antimicrobial prophylaxis in the newborn. All cases of gonorrhea beyond the newborn period should be considered possible evidence of sexual abuse. Vulvovaginitis (not cervicitis) is the most common manifestation in prepubescent girls. Signs and symptoms may include vaginal discharge (often purulent or crusting), dysuria, odor, irritation, and pruritus. The anorectum and the pharynx are the most frequently infected sites in abused boys; urethritis is less frequently seen. If specimens are to be collected, proper guidelines for collecting forensic evidence must be followed. When evaluating a child who has potentially suffered sexual abuse, the clinician should consult individual state laws concerning reporting and counseling.
How do I know if I have gonorrhea?
Gonorrhea often has no symptoms, but it can cause serious health problems, even without symptoms.
Most women with gonorrhea do not have any symptoms. Even when a woman has symptoms, they are often mild and can be mistaken for a bladder or vaginal infection. Symptoms in women can include:
- Painful or burning sensation when peeing;
- Increased vaginal discharge; and
- Vaginal bleeding between periods.
Men who do have symptoms may have:
- A burning sensation when peeing;
- A white, yellow, or green discharge from the penis; and
- Painful or swollen testicles (although this is less common).
Rectal infections may either cause no symptoms or cause symptoms in both men and women that may include:
- Discharge;
- Anal itching;
- Soreness;
- Bleeding; and
- Painful bowel movements.
See your healthcare provider if you notice any of these symptoms. You should also see a provider if your partner has an STD or symptoms of one. Symptoms can include an unusual sore, a smelly discharge, burning when peeing, or bleeding between periods.
Is gonorrhea curable?
Yes. Gonorrhea can be cured with the right treatment. The Centers for Disease Control and Prevention (CDC) recommends either a single therapy or using two drugs, to treat gonorrhea – Ceftriaxone 250 mg IM in a single dose (for persons weighing <150 kg) with or without oral doxycycline 100 mg twice daily for 7 days depending on whether chlamydia infection has been excluded 1. If chlamydial infection has not been excluded then add doxycycline 100 mg orally 2 times/day for 7 days. For pregnant women, if chlamydia has not been excluded, oral azithromycin 1 gram should be used in place of doxycycline 1. If ceftriaxone is not available, the two options are (1) intramuscular gentamicin 240 mg plus oral azithromycin 2 grams or (2) oral cefixime 800 mg 83. It is important to take all of the medication prescribed to cure gonorrhea. Medication for gonorrhea should not be shared with anyone. Although medication will stop the infection, it will not repair any permanent damage done by the disease. Antimicrobial resistance in gonorrhea is of increasing concern, and successful treatment of gonorrhea is becoming more difficult. If a person’s symptoms continue for more than a few days after receiving treatment, he or she should return to a health care provider to be reevaluated.
Neisseria gonorrhoeae bacteria
Neisseria gonorrhoeae also known as gonococcus (singular), or gonococci (plural), is a species of Gram-negative diplococci bacteria isolated by Albert Neisser in 1879 84. Neisseria gonorrhoeae causes the sexually transmitted genitourinary infection gonorrhea as well as other forms of gonococcal disease including disseminated gonococcemia, septic arthritis, and gonococcal ophthalmia neonatorum.
Neisseria gonorrhoeae sexual transmission is through vaginal, anal, or oral sex 74. Sexual transmission may be prevented through the use of latex condoms 85. Perinatal transmission may occur during childbirth, and may be prevented by antibiotic treatment of the mother before birth and the application of antibiotic eye gel on the eyes of the newborn. After an episode of gonococcal infection, infected persons do not develop immunity to future infections. Reinfection is possible due to Neisseria gonorrhoeae’s ability to evade the immune system by varying its surface proteins 86.
Neisseria gonorrhoeae can cause infection of the genitals, throat, and eyes. Asymptomatic infection is common in males and females 87. Untreated gonococcal infection may spread to the rest of the body (disseminated gonorrhea infection), especially the joints (septic arthritis). Untreated infection in women may cause pelvic inflammatory disease (PID) and possible infertility due to the resulting scarring. Diagnosis is through gonorrhea culture or using nucleic acid amplification testing (NAAT), of a urine sample, urethral swab (for men), or endocervical or vaginal swab (for women) 1, 75. Chlamydia co-testing and testing for other STDs is recommended due to high rates of co-infection 1. FDA-cleared rectal and oral diagnostic tests for gonorrhea (as well as chlamydia) have been validated for clinical use 1.
Gonorrhea can be cured with the right treatment. The Centers for Disease Control and Prevention (CDC) now recommends a single 500 mg intramuscular (IM) dose of ceftriaxone for the treatment of gonorrhea. Alternative regimens are available when ceftriaxone cannot be used to treat urogenital or rectal gonorrhea 74.
Antibiotic resistance in Neisseria gonorrhoeae is a growing public health concern, especially given its propensity to develop resistance easily 88, 89.
How do you get gonorrhea?
Anyone who is sexually active can get gonorrhea. Gonorrhea is spread by having unprotected vaginal, anal or oral sex with an infected person.
Gonorrhea can also be passed from an infected mother to her baby during birth, which can cause eye infection (neonatal conjunctivitis) and even blindness.
The transmission of gonorrhea can occur in several ways:
- Male-to-female transmission of gonorrhea via semen occurs at a rate of approximately 50% to 70% per episode of vaginal intercourse with ejaculation; male-to-female transmission of gonorrhea can occur without ejaculation 90.
- An infected woman can transmit gonorrhea to the urethra of a male sex partner; the rate of transmission is approximately 20% per episode from vaginal intercourse, and it increases to approximately 60% to 80% after four or more intercourse exposures 91.
- Pharyngeal gonorrhea is readily acquired by fellatio; it is less efficiently acquired by cunnilingus. Gonorrhea can also be transmitted from the pharynx to the urethra during fellatio (and presumably to vagina with cunnilingus).
- Perinatal transmission (mother-to-infant) can occur during vaginal delivery, when the infected mother has not been treated during the perinatal period.
Rectal intercourse transmission rates have not been quantified, but rectal intercourse appears to be an efficient mode of transmission. - Gonorrhea is associated with increased susceptibility to HIV acquisition. It is also associated with an increase in HIV transmission, because gonococcal urethritis increases HIV shedding in men 92.
Risk factors for getting gonorrhea
Risk factors and risk markers for acquiring gonorrhea include:
- Younger age
- Being adolescent (especially female)
- Sexually active women younger than 25 and men who have sex with men
- A new sex partner
- Having more than one sex partner
- Having a sex partner who has other partners
- Inconsistent or incorrect condom use
- Living in an urban area where gonorrhea prevalence is high
- Having a lower socio-economic status
- Using drugs including alcohol (in association with higher risk sex)
- Exchanging sex for drugs or money
- African American race
- Previous gonorrhea diagnosis
- Having other sexually transmitted infections
Gonorrhea prevention
The surest way to avoid transmission of gonorrhea or other STDs is to abstain from vaginal, anal, and oral sex, or to be in a long-term mutually monogamous relationship with a partner who has been tested and is known to be uninfected. Latex condoms, when used consistently and correctly, can reduce the risk of transmission of gonorrhea 85.
Take steps to reduce your risk of gonorrhea:
- Always use condoms with a water-based lubricant if you choose to have sex. Abstaining from sex is the surest way to prevent gonorrhea. But if you choose to have sex, use a condom during any type of sexual contact, including anal sex, oral sex or vaginal sex. Use a male latex condom or a female polyurethane condom during each sexual contact. Condoms used properly during every sexual encounter reduce but don’t eliminate the risk of infection. Latex condoms greatly reduces, but does not completely eliminate, the risk of catching or spreading STDs. If your or your partner is allergic to latex, you can use polyurethane condoms.
- Always use dental dams for oral sex (a dental dam is a thin square of latex placed over the vulva or anus during oral sex).
- Limit your sex partners or have a long-term monogamous relationship where neither of you is already infected. Having multiple sex partners puts you at a high risk of contracting chlamydia and other sexually transmitted infections.
- Ask your partner to be tested for sexually transmitted infections. Find out whether your partner has been tested for sexually transmitted infections, including gonorrhea. If not, ask whether he or she would be willing to be tested.
- Don’t have sex with someone who has any unusual symptoms. If your partner has signs or symptoms of a sexually transmitted infection, such as burning during urination or a genital rash or sore, don’t have sex with that person.
- Avoid sex with someone infected with gonorrhea until after they have finished treatment and are cured.
- Have regular sexually transmitted infection (STI) check-ups. Annual screening is recommended for all sexually active women less than 25 years of age and for older women at increased risk of infection, such as those who have a new sex partner, more than one sex partner, a sex partner with concurrent partners, or a sex partner who has a sexually transmitted infection. Regular screening is also recommended for men who have sex with men, as well as their partners.
- Avoid douching. Douching decreases the number of good bacteria in the vagina, which can increase the risk of infection.
To avoid reinfection with gonorrhea, abstain from unprotected sex for seven days after you and your sex partner have completed treatment and after resolution of symptoms, if present.
How to use male condoms
- Put the condom on before any contact is made.
- Unroll the condom over an erect penis to the base of the penis. (Uncircumcised men should pull back their foreskin before unrolling.) The unrolled ring should be on the outside. Leave about 1/2 inch of space in the tip so semen can collect there. Squeeze the tip to get the air out.
- Pull out after ejaculating and before the penis gets soft. To pull out, hold the rim of the condom at the base of the penis to make sure it doesn’t slip off.
- Don’t reuse condoms.
How to use female condoms
- Follow the directions on the condom package for correct placement. Be sure the inner ring goes as far into the vagina as it can. The outer ring stays outside the vagina.
- Guide the penis into the condom.
- After sex, remove the condom before standing up by gently pulling it out.
- Don’t reuse condoms.
Screening for gonococcal infection
Routine screening for gonorrhea infection in women is recommended in order to decrease morbidity as well as to reduce the burden of disease in the community 93. Urethral infections caused by gonorrhea among men usually produce symptoms that cause them to seek curative treatment soon enough to prevent sequelae, but transmission to others may occur in this interim. Among women, gonococcal infections are commonly asymptomatic until complications (such as pelvic inflammatory disease with resultant risk for infertility and ectopic pregnancy) have occurred. The following summarizes gonorrhea screening recommendations issued by the CDC and the U.S. Preventive Services Task Force (USPSTF) for different patient populations 93, 94:
- Sexually Active Women Who Have Sex with Men: The CDC 93 and the U.S. Preventive Services Task Force 94 recommend (1) annual screening for gonorrhea in all sexually active women younger than 25 years of age, and (2) annual screening for gonorrhea in sexually active women age 25 years and older if they are considered to have increased risk for gonococcal infection. The most important identified risk factors for gonococcal infection include a new sex partner, multiple sex partners, a sex partner with concurrent partners, or a sex partner with a sexually transmitted infection; additional factors that indicate risk of gonococcal infection include inconsistent condom use in persons not in a mutually monogamous relationship, exchange of sex for money or drugs, one or more previous sexually transmitted infections, or a coexistent sexually transmitted infection. Women diagnosed with gonorrhea infection should have repeat testing approximately 3 months after completing treatment.
- Women Who Have Sex with Women: The CDC recommends gonococcal screening for women who have sex with women should occur according to the current screening guidelines for sexually active women who have sex with men 95.
- Women Who are Pregnant: The CDC recommends screening for gonorrhea should be performed at the first prenatal visit for (1) women younger than age 25 and (2) women age 25 years and older who are at increased risk for gonorrhea (e.g. women with a new sex partner, a sex partner who has a sexually transmitted infection, more than one sex partner, or a sex partner with concurrent partners 95. Additional factors associated with increased risk of gonococcal infection include inconsistent condom use in persons not in a mutually monogamous relationship, exchange of sex for money or drugs, and previous or coexisting sexually transmitted infections. A repeat test for gonococcal infection should be performed during the third trimester for those at continued risk. Pregnant women diagnosed with gonorrhea infection should have repeat testing approximately 3 months after completing treatment 95.
- Men Who Have Sex Only with Women: Routine screening for gonococcal infection is not recommended by either the CDC or the USPSTF for men who have sex only with women.[10,27]
- Men Who Have Sex with Men: The CDC 95 recommends screening for gonococcal infection in men who have sex with men at least annually, regardless of a history of condom use during sexual contact; the sites tested should correspond with sites involved in sexual activity with other men during the prior year (e.g. urethral testing if insertive intercourse, rectal testing if receptive anal intercourse, and pharyngeal testing with receptive oral intercourse). The U.S. Preventive Services Task Force 94 does not recommend routine screening for gonorrhea in men, including men who have sex with men.
- Transgender Men and Women: The CDC 95 recommends screening for gonorrhea in transgender men (“trans-men”) and transgender women (“trans-women”) should be based on age, current anatomy, and sexual practices.
- Persons with HIV Infection: The CDC 96 recommends performing routine screening for gonorrhea for persons with HIV infection who are sexually active; testing for gonorrhea should be performed at the initial evaluation and at least annually thereafter (more frequent screening may be indicated based on risk). The testing should consist of obtaining samples from the anatomic sites of sexual exposure.
- Persons in Correctional Facilities: The CDC 95 recommends performing routine gonococcal screening at the initial intake in a correctional facility for women 35 years of age and younger and men younger than age 30.
Gonorrhea signs and symptoms
Gonorrhea often has no symptoms 78, 79.
Most women with gonorrhea have no symptoms at all.
Some men, especially those with throat or anus infection, also have no symptoms.
Occasionally gonorrhea can involve the eyes, joints, heart or brain, causing permanent damage.
In women, if symptoms do occur, they usually develop within 10 days of infection. In women, symptoms may include:
- unusual vaginal discharge
- pain, discomfort or burning sensation when passing urine
- pelvic pain, especially during sex
- irregular bleeding, especially between periods or after sex
- anal discharge and discomfort
- sore, dry throat
In men, if symptoms do occur, they usually develop within 1 to 3 days. In men, symptoms may include:
- thick, yellow or white discharge from the penis
- pain, discomfort or burning sensation when passing urine
- pain in the testes (balls)
- redness around the opening of the penis
- anal discharge and discomfort
- sore, dry throat
Gonorrhea symptoms in men
In men, when symptoms do occur, they usually develop within one to three days. In men, gonorrhea symptoms may include:
- thick, yellow or white discharge from the penis
- pain, discomfort or burning sensation when passing urine
- pain or swelling in one testis (balls)
- redness around the opening of the penis
- anal discharge and discomfort
- sore, dry throat.
Urethritis
Urethritis is a common manifestation of gonorrhea in men. Most men develop overt, symptomatic urethritis, but a small percentage will develop asymptomatic (unrecognized) infection. Asymptomatic gonorrhea may act as a reservoir that perpetuates transmission in the community 97. The typical symptoms of gonococcal urethritis, when present, include a purulent or mucopurulent urethral discharge, often accompanied by dysuria. The discharge may also be clear or cloudy. The incubation period ranges from 1 to 14 days, with most men becoming symptomatic within 2 to 5 days after exposure 98.
Anorectal infections
Anorectal infection most often occurs in men who have sex with men, with acquisition of rectal gonorrhea occurring through receptive anal intercourse, but it also has been reported in women with gonococcal cervicitis who do not acknowledge rectal sexual contact. These infections may result from perineal contamination with infected cervical secretions. Most patients with anorectal infection are asymptomatic, although proctitis can occur. Symptoms of proctitis include anal irritation, painful defecation, constipation, scant rectal bleeding, painless mucopurulent discharge, anal pruritus, and tenesmus 99. When proctitis is suspected, an anoscopic examination is recommended to assess for inflammation and mucosal injury. The anorectal mucosa may appear normal, but purulent discharge, erythema, or easily induced bleeding may be observable under anoscopy.
Complications of genital infection in men
Men with untreated gonococcal genital infection can develop epididymitis, with typical symptoms of unilateral testicular pain and swelling, and epididymal tenderness. Epididymitis is infrequent following gonococcal infection, but it is the most common local complication of gonorrhea infection in men. When it does occur, epididymitis is often associated with overt or subclinical urethritis. Urethral discharge may or may not be present. Notably, up to 70% of epididymitis caused by a sexually transmitted pathogen are due to Chlamydia trachomatis. Other less common complications associated with gonococcal infection in men include inguinal lymphadenitis, penile edema, periurethral abscess or fistula, accessory gland infection (Tyson’s glands), balanitis, urethral stricture, and prostatitis, and rarely perirectal abscess.
Gonorrhea symptoms in women
In women, when symptoms do occur, they usually develop within 10 days of infection. In women, gonorrhea symptoms may include:
- unusual vaginal discharge
- pain, discomfort or burning sensation when passing urine
- pelvic pain, especially during sex
- irregular vaginal bleeding, especially between periods or after sex
- abdominal or pelvic pain
- anal discharge and discomfort
- sore, dry throat.
Cervicitis
Symptomatic gonococcal infection in women most often manifests as cervicitis and/or urethritis, but at least 50% of women with genital gonococcal infection are asymptomatic. Symptoms of cervicitis vary and may include a nonspecific vaginal discharge, intermenstrual bleeding, dysuria, lower abdominal pain, and dyspareunia. Clinically, examination of the cervix may show mucopurulent or purulent cervical discharge and easily bleed with minimal contact. The incubation period in women is variable, but symptoms, when they do occur, usually develop within 10 days of the exposure 100. Seventy to ninety percent of women with genital gonococcal infection have laboratory evidence of urethral infection (urethritis); dysuria may be present, but these women frequently do not have specific urethral symptoms.
Anorectal infections
Anorectal gonococcal infection is uncommon in women, but can occur via anal intercourse. Anorectal infection has been reported in women with gonococcal cervicitis who do not acknowledge rectal sexual contact, presumably these infections result from perineal contamination with infected cervical secretions.
Complications in genital infection in women
There are several complications associated with gonorrhea in women:
- Accessory gland (Bartholin’s glands or Skene’s glands) infections: Infection of female sex accessory glands (Bartholin’s glands or Skene’s glands) is often a unilateral infection. Occlusion of the ducts of these glands due to inflammation may result in the formation of an abscess.
- Pelvic inflammatory disease (PID): If cervical gonococcal infection ascends to the endometrium and/or fallopian tubes, PID may develop, typically causing symptoms that include lower abdominal pain, vaginal discharge, dyspareunia, intermenstrual bleeding, and fever 20. In some women, PID may also be asymptomatic. Presumptive treatment for PID should be considered if one or more of the following minimum criteria are present on pelvic examination—uterine or adnexal tenderness or cervical motion tenderness. The long-term sequelae of untreated PID can include chronic pelvic pain, tubal infertility, and increased risk for ectopic pregnancy.
- Perihepatitis (Fitz-Hugh-Curtis Syndrome): In situations where gonococcal infection ascends from the cervix, infection may produce inflammation of the liver capsule and the adjacent peritoneum. Most women with perihepatitis have associated PID, but perihepatitis can occur independently. Historically, perihepatitis was attributed only to gonococcal infection, but now it is often associated with chlamydial infection. Gonococcal perihepatitis is characterized by right upper quadrant pain, and may be accompanied by abnormal liver function tests.
Gonorrhea at other sites in the body
Gonorrhea can also affect these parts of the body:
- Rectum. Signs and symptoms include anal itching, pus-like discharge from the rectum, spots of bright red blood on toilet tissue and having to strain during bowel movements.
- Eyes. Gonorrhea that affects your eyes may cause eye pain, sensitivity to light, and pus-like discharge from one or both eyes.
- Throat. Signs and symptoms of a throat infection may include a sore throat and swollen lymph nodes in the neck.
- Joints. If one or more joints become infected by bacteria (septic arthritis), the affected joints may be warm, red, swollen and extremely painful, especially when you move an affected joint.
Gonorrhea throat infection
Gonorrhea throat infection also called gonococcal pharyngeal infection is most often asymptomatic. The pharynx may be the sole site of infection if the only exposure was receptive orogenital intercourse. Exudative pharyngitis is rare. Symptoms of pharyngeal infection may include pharyngitis, tonsillitis, fever, and cervical adenitis.
Gonorrhea eye infection
Gonococcal infection of the eye, when it does occur, typically presents as conjunctivitis. Gonococcal conjunctivitis in adults most often results from autoinoculation in persons with genital gonococcal infection. Patients may initially develop a mild non-purulent conjunctivitis, that, if untreated, typically progress to marked conjunctival redness, copious purulent discharge, and conjunctival edema 101. Less often, the manifestations include an ulcerative keratitis. Untreated gonococcal conjunctivitis can cause complications that may include corneal perforation, endophthalmitis, and blindness.
Disseminated gonococcal infection
If left untreated, gonorrhea can also spread to the blood and cause disseminated gonococcal infection (DGI) 102. Disseminated gonococcal infection, a systemic gonococcal infection, occurs infrequently and is more common in women than in men. Disseminated gonococcal infection is associated with some gonococcal strains that have a propensity to produce bacteremia without associated urogenital symptoms. In addition, patients with complement deficiency have greater risk of developing disseminated gonococcal infection. Disseminated gonococcal infection is usually characterized by arthralgia, arthritis, tenosynovitis, hepatitis, myocarditis, endocarditis, meningitis and/or dermatitis 102. This condition can be life threatening. Rates of disseminated gonococcal infection have decreased due to the declining proportion of gonococcal strains prone to disseminate 103.
Gonorrhea complications
Untreated gonorrhea can cause serious and permanent health problems in both women and men, such as:
- Infertility in women. Untreated gonorrhea can spread into the uterus and fallopian tubes, causing pelvic inflammatory disease (PID), which may result in scarring of the tubes, greater risk of pregnancy complications and infertility. Pelvic inflammatory disease (PID) is a serious infection that requires immediate treatment. Pelvic inflammatory disease (PID) symptoms may be quite mild or can be very severe and can include abdominal pain and fever 104. PID can lead to internal abscesses and chronic pelvic pain. PID can also damage the fallopian tubes enough to cause infertility or increase the risk of ectopic pregnancy.
- Infertility in men. Men with untreated gonorrhea can experience epididymitis — inflammation of a small, coiled tube in the rear portion of the testicles where the sperm ducts are located (epididymis). Epididymitis is treatable, but if left untreated, it may lead to infertility 105.
- Infection that spreads to the joints and other areas of your body. The bacterium that causes gonorrhea can spread through the bloodstream and infect other parts of your body, including your joints. Fever, rash, skin sores, joint pain, swelling and stiffness are possible results.
- Increased risk of HIV/AIDS. Having gonorrhea makes you more susceptible to infection with human immunodeficiency virus (HIV), the virus that leads to AIDS. People who have both gonorrhea and HIV are able to pass both diseases more readily to their partners.
- Complications in babies. Babies who contract gonorrhea from their mothers during birth can develop blindness, sores on the scalp and infections.
- Disseminated gonococcal infection (DGI). If left untreated, gonorrhea can also spread to the blood and cause disseminated gonococcal infection (DGI). Disseminated gonococcal infection is usually characterized by arthralgia, arthritis, tenosynovitis, hepatitis, myocarditis, endocarditis, and meningitis and/or dermatitis 102. This condition can be life threatening.
Gonorrhea diagnosis
Testing for gonorrhea involves taking a swab (sample) from the urethra in men and the cervix in women. It can also be tested by taking a urine sample.
Sometimes swabs are also be taken from the throat, urethra, vagina or anus.
It is also important to get tested for other sexually transmitted infections such as syphilis, chlamydia and HIV.
To determine whether the gonorrhea bacterium is present in your body, your doctor will analyze a sample of cells. Samples can be collected by:
- Urine test. This may help identify bacteria in your urethra.
- Swab of affected area. A swab of your throat, urethra, vagina or rectum may collect bacteria that can be identified in a laboratory.
For women, home test kits are available for gonorrhea. Home test kits include vaginal swabs for self-testing that are sent to a specified lab for testing. If you prefer, you can choose to be notified by email or text message when your results are ready. You may then view your results online or receive them by calling a toll-free hotline.
Testing for other sexually transmitted infections
Your doctor may recommend tests for other sexually transmitted infections. Gonorrhea increases your risk of these infections, particularly chlamydia, which often accompanies gonorrhea. Testing for HIV also is recommended for anyone diagnosed with a sexually transmitted infection. Depending on your risk factors, tests for additional sexually transmitted infections could be beneficial as well.
Gonorrhea test
The approach to diagnostic testing for gonorrhea has evolved from traditional cultivation to widespread use of nucleic acid amplification tests (NAAT) 106. Gram’s stain, another non-culture test, is used for the diagnosis of urethral gonorrhea in symptomatic males. Culture is still recommended if antimicrobial resistance is a concern, especially in cases of treatment failure.
Nucleic Acid Detection Tests
There are two types of nucleic acid detection tests: non-amplified tests and amplified tests:
- Amplified Tests: The nucleic acid amplification tests (NAATs) include polymerase chain reaction (PCR) (Roche Amplicor; Cepheid GeneXpert CT/NG), transcription-mediated amplification (TMA) (Gen-Probe Aptima), and strand displacement amplification (SDA) (Becton-Dickinson BDProbeTec ET) 107. Amplified tests are FDA-cleared for endocervical specimens from women, urethral specimens from men, and urine specimens from men and women. Some NAATs are also cleared for vaginal swabs. For many of the commercially available tests, the same specimen can be used to test for Chlamydia trachomatis infection. NAATs are the most sensitive test to detect gonorrhea infections. In May 2019, the FDA cleared two NAATs (Aptima Combo 2 Assay and the Xpert CT/NG) for extragenital diagnostic testing of Neisseria gonorrhoeae and Chlamydia trachomatis in rectal and pharyngeal samples 54. Multiple studies have shown NAATs are the most sensitive test to detect Neisseria gonorrhoeae infections. At present, antimicrobial susceptibility cannot be determined with NAATs, but research in this area is ongoing. In addition, the major limitation of NAATs is the potential for false-positive results due to remnant nucleic acids, either from contamination or dead organisms; this property limits the utility of NAATs for immediate post-treatment testing.
- Non-Amplified Tests: Non-amplified tests used for gonorrhea include the DNA probe (e.g. Gen-Probe PACE 2 and Digene Hybrid Capture II). A non-amplified test is less likely to be affected by transport conditions than culture, and has the potential for more timely results. These tests are FDA-cleared for endocervical specimens from women and urethral specimens from men. They are not FDA-cleared for pharyngeal, rectal, or urine specimens. The same specimen can be evaluated for Chlamydia trachomatis infection 106. Antimicrobial susceptibility cannot currently be determined with non-amplified tests.
Point-of-Care NAAT Testing
In March 2021, the FDA approved the first point-of-care nucleic acid amplification test (NAAT) (Binx Health IO CT/NG Assay) for the diagnosis of urogenital chlamydia and gonorrhea 58. This point-of-care test can be run on vaginal swabs obtained from women or on urine samples collected from men 58. This assay can provide a result in approximately 30 minutes 58. In a cross-sectional study, investigators evaluated this point-of-care NAAT for the diagnosis of chlamydia and gonorrhea using vaginal swabs obtained from 1,523 women and urine samples collected from 922 men 59. For gonorrhea, the sensitivity estimates were 100.0% in women and 97.3% in men; the specificity estimates were 99.9% for women and 100.% for men 59. In addition, the investigators found that self-obtained vaginal swabs in women performed equivalent to clinician-collected vaginal swabs 59.
Gram’s Stain
The use of Gram’s stain is a non-culture test that can make a presumptive diagnosis of gonorrhea. In the clinical setting, a Gram’s stain to detect gonorrhea is most often performed on a male with purulent urethral discharge. A Gram’s stain on a specimen positive for gonorrhea shows polymorphonuclear leukocytes (PMNs) with intracellular gram-negative diplococci. A Gram’s stain, with proper laboratory technique, has greater than 95% sensitivity and greater than 99% specificity for diagnosing symptomatic male gonococcal urethritis 106. Thus, the Gram’s stain is considered reliable both to diagnose and to exclude gonococcal urethritis in symptomatic men 93. The sensitivity of a Gram’s stain is lower for mane with asymptomatic urethral infection and thus not considered adequate to rule out infection in asymptomatic men 93. Performing a Gram’s stain is not recommended on endocervical, pharyngeal, or rectal specimens due to poor sensitivity 93.
Bacterial culture
Obtaining a bacterial culture is the historic standard for detection of gonorrhea. It has several advantages over non-culture tests, including low cost, use for a variety of specimen sites, and antimicrobial susceptibility testing can be performed if gonorrhea is isolated from the specimen. Despite having some advantages, culture is not as sensitive as NAAT and is more laboratory intensive, which has led to infrequent use in modern practice. At present, culture is primarily used for antimicrobial resistance surveillance by collecting specimens from either symptomatic urethral infections or from screen-positive sites of infection prior to treatment 1.
Disseminated Gonococcal Infection special diagnostic considerations
When evaluating persons with suspected disseminated gonococcal infection, diagnostic testing should consist of (1) obtaining and ordering NAAT and culture for specimens from all applicable urogenital and extragenital mucosal sites, (2) ordering culture for all specimens obtained from disseminated sites of infection (e.g. skin, synovial fluid, blood, or cerebrospinal fluid), and (3) performing antimicrobial susceptibility testing on all Neisseria gonorrhoeae isolates obtained in culture specimens.
Gonorrhea treatment
Adults with gonorrhea are treated with antibiotics. Due to emerging strains of drug-resistant Neisseria gonorrhoeae, the Centers for Disease Control and Prevention (CDC) recommends that uncomplicated gonorrhea be treated only with the antibiotic ceftriaxone — given as an injection — in combination with either azithromycin (Zithromax, Zmax) or doxycycline (Monodox, Vibramycin, others) — two antibiotics that are taken orally.
Some research indicates that oral gemifloxacin (Factive) or injectable gentamicin, combined with oral azithromycin, is highly successful in treating gonorrhea. This treatment may be helpful in treating people who are allergic to cephalosporin antibiotics, such as ceftriaxone.
The following summarizes several key new recommendations from the 2021 Sexually Transmitted Infections Treatment Guidelines 1, 83:
- For the treatment of uncomplicated gonococcal infection of the cervix, urethra, or rectum in persons who weigh less than 150 kg, the single intramuscular ceftriaxone dose has been increased from 250 mg to 500 mg; for persons who weigh 150 kg or greater, the dose should be increased to 1 gram. The increased dose of ceftriaxone is recommended based on pharmacokinetic and pharmacodynamic data that show ceftriaxone concentrations at 24 hours with a 500 mg dose provides more reliable eradication of Neisseria gonorrhoeae than with a 250 mg dose 108, 109.. Furthermore, because ceftriaxone produces variable levels in the pharynx, the 500 mg ceftriaxone dose should provide a more reliable treatment for pharyngeal gonorrhea.
- For persons with uncomplicated gonococcal infection of the cervix, urethra, or rectum in whom chlamydia infection has been ruled out, ceftriaxone monotherapy is recommended, which is in contrast to the prior recommendation to add azithromycin as dual therapy for all gonococcal infections 110. The rationale for eliminating the routine use of azithromycin as dual therapy for the treatment of gonorrhea is twofold: (1) the concern for azithromycin causing antimicrobial resistance in commensal organisms and concurrent pathogens, and (2) the trend of increasing Neisseria gonorrhoeae resistance to azithromycin 111, 112.
- For persons with gonococcal infection in whom chlamydia infection has not been excluded, oral doxycycline is added to ceftriaxone for the purpose of treating chlamydia (for nonpregnant persons). This new recommendation is based on emerging data suggesting better chlamydia treatment efficacy with doxycycline than with azithromycin, especially with rectal chlamydia 113, 114, 115.
- For persons with pharyngeal gonococcal infection, a test-of-cure is recommended 7 to 14 days after treatment, regardless of the treatment regimen used. The prior recommendation was to perform a test-of-cure after treatment of pharyngeal gonococcal infection only if an alternative regimen was used.
- The recommended expedited partner therapy (EPT) with a single oral dose of cefixime has increased from 400 mg to 800 mg and routine dual therapy with azithromycin is no longer recommended; if concurrent chlamydia was not excluded in the source individual who was diagnosed with gonorrhea, then the expedited partner therapy should include oral doxycycline 100 mg for 7 days (for nonpregnant persons).
Antibiotics for gonorrhea
The CDC treatment guidelines recommend using dual therapy for the treatment of gonococcal infections in adults and adolescents. Ceftriaxone is the most effective cephalosporin for treatment of gonorrhea and should be used in combination with azithromycin. The recommendation for dual therapy is based on the premise that using two antimicrobials with different mechanisms of action (e.g. a cephalosporin plus azithromycin) may improve treatment efficacy and potentially slow the emergence and spread of resistance. In addition, azithromycin and doxycycline will effectively treat concomitant C. trachomatis infection, if present. Azithromycin is preferred over doxycycline as a second agent due to convenience (single-dose therapy versus 7-day therapy) and the substantially lower prevalence of gonococcal resistance to azithromycin than with doxycycline, particularly for gonococcal strains that have an elevated cefixime MIC. In the case of azithromycin allergy or severe intolerance, doxycycline (100 mg orally twice a day for 7 days) can be used as a substitute for azithromycin, but doxycycline should only be used as an alternative, primarily because of the high prevalence of gonococcal tetracycline resistance. For details regarding these alternative regimens, refer to the section on gonococcal infections in the 2015 STD Treatment Guidelines 116. The following recommendations for treatment are based on the 2015 STD Treatment Guidelines.
Uncomplicated Gonococcal Infections of the Cervix, Urethra, and Rectum
Recommended Regimen
- Ceftriaxone 250 mg IM in a single dose (for persons weighing <150 kg)
- PLUS
- Doxycycline 100 mg orally 2 times/day for 7 days (if chlamydial infection has not been excluded)
For pregnant women, if chlamydia has not been excluded, oral azithromycin 1 gram should be used in place of doxycycline 1. If ceftriaxone is not available, the two options are (1) intramuscular gentamicin 240 mg plus oral azithromycin 2 grams or (2) oral cefixime 800 mg 83
Alternative Regimens
If cephalosporin allergy:
- Gentamicin 240 mg IM in a single dose
- PLUS
- Azithromycin 2 g orally in a single dose
If ceftriaxone is not available:
- Cefixime 800 mg* orally in a single dose
- PLUS
- * If chlamydial infection has not been excluded, treat for chlamydia with doxycycline 100 mg orally 2 times/day for 7 days.
Uncomplicated Gonococcal Infections of the throat (pharynx)
Most gonococcal infections of the pharynx are asymptomatic and can be relatively common in some populations 117. Gonococcal infections of the pharynx are more difficult to eradicate than are infections at urogenital and anorectal sites 118. Few antimicrobial regimens, including those involving oral cephalosporins, can reliably cure >90% of gonococcal pharyngeal infections 119. Doctors should ask their patients with urogenital or rectal gonorrhea about oral sexual exposure; if reported, patients should be treated with a regimen with acceptable efficacy against pharyngeal gonorrhea infection.
The recommended treatment of pharyngeal gonorrhea:
- Ceftriaxone 500 mg IM in a single dose (for persons weighing <150 kg)
- PLUS
- Doxycycline 100 mg orally 2 times/day for 7 days (if chlamydial infection has not been excluded)
Concomitant treatment for pharyngeal chlamydial infection is not indicated if testing for pharyngeal chlamydia was not performed or if the testing for chlamydia was negative 1. If treatment for chlamydia pharyngeal infection is indicated and the person is pregnant, oral azithromycin 1 gram should be used in place of doxycycline. Note there are no reliable alternative regimens for the treatment of pharyngeal gonorrhea 1. For persons with an anaphylactic or other severe reaction (e.g., Stevens Johnson syndrome) to ceftriaxone, consult an infectious disease specialist for an alternative treatment recommendation.
Gonococcal conjunctivitis
In the only published study of the treatment of gonococcal conjunctivitis among adults, all 12 study participants responded to a single 1 g intramuscular injection of ceftriaxone 120. Based on this study, the recommended treatment for gonococcal conjunctivitis is a single ceftriaxone 1 gram intramuscular dose 1. In addition, a one-time lavage of the infected eye with saline should be considered 1. Because gonococcal conjunctivitis is uncommon and data regarding treatment of gonococcal conjunctivitis among adults are limited, consultation with an infectious disease specialist should be considered.
Recommended Regimen
- Ceftriaxone 1 g IM in a single dose.
Gonococcal Infections in Pregnancy
As with other patients, pregnant women infected with gonorrhea should be treated ceftriaxone 500 mg in a single IM dose plus azithromycin if chlamydia infection was not ruled out 83. When cephalosporin allergy or other considerations preclude treatment with this regimen, consultation with an infectious disease specialist or an STD clinical expert is recommended. Gentamicin use is cautioned during pregnancy because of risk for neonatal birth defects, nephrotoxicity, or ototoxicity 121. Pregnant persons should not be treated with any fluoroquinolone or tetracycline drugs.
Gonorrhea treatment for babies
Babies born to mothers with gonorrhea receive a medication in their eyes soon after birth to prevent infection. If an eye infection develops, babies can be treated with antibiotics.
Disseminated Gonococcal Infection
Disseminated gonococcal infection frequently results in petechial or pustular acral skin lesions, asymmetric polyarthralgia, tenosynovitis, or oligoarticular septic arthritis. The infection is complicated occasionally by perihepatitis and rarely by endocarditis or meningitis. Because of the possibility of potentially severe sequelae associated with these complications, the 2021 STD Treatment Guidelines recommend hospitalization and consultation with an infectious diseases specialist for patients suspected of having disseminated gonococcal infection. Examination for clinical evidence of endocarditis and meningitis should be performed. If disseminated gonococcal infection is suspected, NAAT and culture specimens from all exposed urogenital and extragenital sites should be collected and processed, in addition to NAAT and culture specimens from disseminated sites of infection (e.g., skin, synovial fluid, blood, or CNS). All N. gonorrhoeae isolates should be tested for antimicrobial susceptibility. Risk factors for dissemination have included female sex, menstruation, pregnancy, and terminal complement deficiency 122; however, reports are increasing among men 123, 124. People receiving eculizumab, a monoclonal antibody that inhibits terminal complement activation, also might be at higher risk for disseminated gonococcal infection 125.
The recommended initial antimicrobial therapy is ceftriaxone 1 gram intramuscularly or intravenously every 24 hours; if chlamydia has not been excluded, then treatment of chlamydia with doxycycline 100 mg twice daily should be given. The first dose of ceftriaxone should be given after promptly obtaining appropriate diagnostic samples. The duration of therapy for disseminated gonococcal infection with arthritis-dermatitis syndrome is at least 7 days, and the ceftriaxone can transition to oral therapy if antimicrobial sensitivity testing shows an effective oral choice 1. For patients diagnosed with disseminated gonococcal infection and meningitis, parenteral therapy should continue for 10 to 14 days; with endocarditis, parenteral therapy should be given for at least 4 weeks 1.
Treatment of Arthritis and Arthritis-Dermatitis Syndrome
Recommended Regimen
- Ceftriaxone 1 g IM or IV every 24 hours
- PLUS
- If chlamydial infection has not been excluded, providers should treat for chlamydia with doxycycline 100 mg orally 2 times/day for 7 days.
Alternative Regimens
- Cefotaxime 1 g IV every 8 hours
- OR
- Ceftizoxime 1 g IV every 8 hours
- PLUS
- If chlamydial infection has not been excluded, providers should treat for chlamydia with doxycycline 100 mg orally 2 times/day for 7 days.
When treating for the arthritis-dermatitis syndrome, your doctor can switch to an oral agent guided by antimicrobial susceptibility testing 24–48 hours after substantial clinical improvement, for a total treatment course of at least 7 days.
Treatment of Gonococcal Meningitis and Endocarditis
Recommended Regimen
- Ceftriaxone 1–2 g IV every 12–24 hours
- PLUS
- If chlamydial infection has not been excluded, providers should treat for chlamydia with doxycycline 100 mg orally 2 times/day for 7 days.
No recent studies have been published regarding treatment of disseminated gonococcal infection involving the the brain and spinal cord (central nervous system or CNS) or cardiovascular system. The duration of treatment for disseminated gonococcal infection in these situations has not been systematically studied and should be determined in consultation with an infectious disease specialist. Treatment for disseminated gonococcal infection should be guided by the results of antimicrobial susceptibility testing. Length of treatment should be determined based on clinical presentation. Therapy for meningitis should be continued with recommended parenteral therapy for 10–14 days. Parenteral antimicrobial therapy for endocarditis should be administered for >4 weeks. Treatment of gonococcal perihepatitis should be managed in accordance with the recommendations for PID in these guidelines 1.
Management of Antibiotic-Resistant Gonorrhea
Although there are no confirmed cases of treatment failure due to cephalosporin-resistant gonorrhea in the United States, the gradual upwards trend of MICs documented by the United States Gonococcal Isolate Surveillance Project remains worrisome 126. Criteria for resistance to cefixime and ceftriaxone have not been defined by the Clinical and Laboratory Standards Institute, but isolates with cefixime or ceftriaxone MICs equal to or greater than 0.5 μg/mL are considered to have decreased susceptibility. Only five isolates with ceftriaxone MIC equal to or greater than 0.5 μg/mL have been reported during the history of the United States Gonococcal Isolate Surveillance Project. In 2019, one isolate from Nevada was reported with a ceftriaxone MIC of 1.0 μg/mL 127. Notably, isolates with high-level cefixime and ceftriaxone MICs (cefixime MICs 1.5 to 8 μg/mL and ceftriaxone MICs 1.5 to 4 μg/mL) have been identified in Japan, France, and Spain 128, 129, 130.
Allergy to Penicillins or Cephalosporin
Allergic reactions to first-generation cephalosporins occur in less than 2.5% of persons with a history of penicillin allergy and are less common with third-generation cephalosporins such as ceftriaxone and cefixime 131. Ceftriaxone is contraindicated in patients with a history of IgE-mediated anaphylaxis to penicillin. Given these considerations, expert consultation with an infectious diseases specialist (and possibly also an allergy specialist), is recommended for treating gonorrhea among persons who have documented severe cephalosporin allergy. Cephalosporin desensitization is preferred but impractical in many settings. Potential therapeutic options in this situation for adults and adolescents include (1) dual treatment with single doses of oral gemifloxacin 320 mg plus a single dose of oral azithromycin 2 g, or (2) dual treatment with single doses of intramuscular gentamicin 240 mg plus a single dose of oral azithromycin 2 g 93. Note that since May 2015, gemifloxacin has not available for use in the United States because of a legal dispute regarding the license to manufacture and distribute this drug. For patients with documented severe cephalosporin allergy, recent evidence supports superior effectiveness of dual therapy when compared with azithromycin monotherapy. In this setting, spectinomycin monotherapy has been effective in clinical trials, curing 98.2% of uncomplicated urogenital and anorectal gonococcal infections, but it has poor efficacy against pharyngeal infection and is not currently available in the United States. Although true allergic reactions to third-generation cephalosporins are uncommon among persons who report a history of penicillin allergy, use of ceftriaxone is contraindicated in persons with a history of IgE-mediated penicillin allergy.
Management of Suspected Gonococcal Treatment Failure
Clinicians who diagnose gonorrhea infection in a person with suspected cephalosporin treatment failure should (1) perform culture and susceptibility testing of all relevant clinical specimens; (2) obtain expert opinion for guidance in clinical management (through the STD Clinical Consultation Network [https://stdccn.org], a local STD/HIV Prevention Training Center clinical expert, the CDC, or an infectious diseases specialist); and (3) report the case to the CDC through state and local public health authorities 93. Isolates that grow gonorrhea should be saved and sent to the CDC through state public health laboratory mechanisms. Health departments should prioritize notification and culture evaluation for sex partner(s) of persons with gonorrhea infection suspected for cephalosporin treatment failure or persons whose isolates demonstrate decreased susceptibility to cephalosporins. In this setting, a test-of-cure at relevant clinical sites should be obtained 7 to 14 days after retreatment; culture is the recommended test, preferably with simultaneous NAAT and susceptibility testing of gonorrhea if isolated.
- Initial Approach to Suspected Treatment Failure: Persons with suspected cephalosporin treatment failure should first receive retreatment and receive a single dose of intramuscular ceftriaxone 500 mg, with doxycycline if chlamydial infection exists. This initial approach is recommended in the United States because most suspected treatment failures actually result from reinfection.
- Antimicrobial Options for Likely Treatment Failure: For individuals considered to have high likelihood of true treatment failure, especially those with a documented elevated cephalosporin MIC for N. gonorrhoeae, the suggested option to consider is single-dose oral therapy with azithromycin 2 grams plus a single intramuscular injection of a 240 mg dose of gentamicin.
- Investigational Therapy for N. gonorrhoeae: Several antimicrobials under investigation have shown promise in the treatment of gonorrhea in phase 2 trials, including single-dose oral gepotidacin and single-dose oral zoliflodacin 132, 133. These two agents are now under study in phase 3 trials, and both may have a future role in treating drug-resistant gonorrhea and gonorrhea in persons with serious penicillin or cephalosporin allergy. Two oral agents—solithromycin and delafloxacin—showed promising early results, but phase 3 studies have been disappointing, and these agents are not likely to have a clinical role in the treatment of gonorrhea 134, 135.
Follow-Up
Due to the significant risk of reinfection in persons diagnosed with gonorrhea, all persons diagnosed with gonorrhea should have repeat testing in 3 months at the anatomic site of exposure, regardless of whether they have symptoms; this is considered a test for reinfection, not a test-of-cure 1. For persons with uncomplicated gonococcal infections of the cervix, urethra, or rectum, a routine test-of-cure at 7 to 14 days post-treatment is not recommended 1. For persons with pharyngeal gonorrhea, however, a routine test-of-cure (using either culture or NAAT) is recommended 7 to 14 days after completing treatment, regardless of the treatment regimen 1. For these individuals, if the test-of-cure NAAT is positive, an effort should be made to perform a confirmatory culture before retreatment; all positive cultures for test-of-cure should undergo antimicrobial susceptibility testing 110. For persons with suspected cephalosporin-resistant gonorrhea who receive retreatment, a test-of-cure at relevant clinical sites should be obtained 7 to 14 days after retreatment; culture is the recommended test, preferably with simultaneous NAAT and susceptibility testing of N. gonorrhoeae if isolated 1.
Management of Sex Partners
Your partner also should undergo testing and treatment for gonorrhea, even if he or she has no signs or symptoms. Your partner receives the same treatment you do. Even if you’ve been treated for gonorrhea, you can be reinfected if your partner isn’t treated.
All recent sex partners (within the 60 days preceding the onset of symptoms or gonorrhea diagnosis) should be referred for evaluation, testing, and presumptive treatment of gonorrhea. If the most recent contact with a sex partner occurred more than 60 days preceding onset of symptoms or gonorrhea diagnosis, that partner should be referred for evaluation and treatment. Sex partners who are treated should also be instructed to abstain from sexual activity for 7 days after they have completed antimicrobial treatment.
Expedited partner therapy
In settings where prompt referral and treatment are unavailable or impractical, providers should consider expedited partner therapy 136. This entails provision of appropriate antibiotics as well as educational and pharmacy information for the partner. The documentation should include notification that partner(s) have been exposed, information about the importance of treatment, signs and symptoms of potential complications, as well as possible therapy-related potential allergic reactions and adverse effects 93.
The expedited partner therapy regimen for sex partners of patients with gonorrhea infection is oral cefixime 800 mg with delivery of the prescription to the partner by either the person diagnosed with gonorrhea, a disease investigation specialist, or a collaborating pharmacy as permitted by law; if concurrent chlamydia was not excluded in the source individual who was diagnosed with gonorrhea, then the expedited partner therapy should include oral doxycycline 100 mg for 7 days (for nonpregnant persons); if there is concern regarding the partner taking multidose therapy for chlamydia, then azithromycin 1 gram orally as a single dose can be given 1.
It is essential to check with one’s state health department to clarify the policies, as the use of expedited partner therapy is not legal in all states. The CDC maintains an updated information page Legal Status of Expedited Partner Therapy that identifies the legal status of expedited partner therapy in each state in the United States, as well as providing links to each state for more detailed state policies. Notably, provision of expedited partner therapy alone is not sufficient and each partner should ideally be seen in follow-up for repeat testing to confirm resolution of infection and check for reinfection. Although offering expedited partner therapy to female partners is acceptable, this approach may result in undertreatment of pelvic inflammatory disease. The use of expedited partner therapy for gonorrhea is contraindicated in a female partner who have current signs or symptoms that are suggestive of PID. Female partners who have current signs and symptoms suggestive of PID should undergo prompt evaluation by a health care provider. In addition, the use of expedited partner therapy should not be considered a routine partner management strategy in men who have sex with men with gonorrhea for several reasons, including the high risk for coexisting infections (especially HIV and syphilis infection), inadequate data regarding the efficacy of expedited partner therapy in this patient population, and concerns regarding the increased proportion of gonococcal isolates among men who have sex with men with reduced susceptibility to cefixime.
Genital herpes
Genital herpes is a sexually transmitted disease (STD) caused by two types of herpes viruses – herpes simplex virus type 1 (HSV-1) and herpes simplex virus type 2 (HSV-2) 137, 138. Genital herpes is a chronic, lifelong viral infection that causes recurrent genital ulcers and on rare occasions, disseminated and visceral disease 139. Most people with genital herpes do not know they have it or may have very mild symptoms. Other people have pain, itching and sores around their genitals, anus or mouth. People with genital herpes are able to spread the virus despite having very mild symptoms or no symptoms. Genital herpes can often be spread by skin-to-skin contact during vaginal, anal and oral sex.
Genital herpes is common in the United States. At least 50 million people in the United States—about one in six adults—are infected with HSV. More than one out of every six people aged 14 to 49 years have genital herpes. Genital herpes is more common in women than in men.
Genital herpes can cause outbreaks of blisters or sores on the genitals and anus. Once infected, you can continue to have recurrent episodes of symptoms throughout your life.
There are 2 types of herpes simplex virus (HSV), both viruses can affect either the lips, mouth, genital or anal areas, however:
- Herpes simplex virus type 1 (HSV1) commonly causes cold sores on the lips, mouth or face. However, most people do not have any symptoms. Most people with oral herpes were infected during childhood or young adulthood from non-sexual contact with saliva. Oral herpes caused by HSV-1 can be spread from the mouth to the genitals through oral sex. This is why some cases of genital herpes are caused by HSV-1.
- Herpes simplex virus type 2 (HSV2) causes most genital herpes in the United States 140.
Genital herpes is most easily spread when there are blisters or sores, but can still be passed even if a person has no current blisters or sores or other symptoms. Herpes simplex virus (HSV) also can be present on the skin even if there are no sores. If a person comes into contact with the herpes simplex virus (HSV) on an infected person’s skin, he or she can become infected.
In 2018, there were an estimated 18.6 million people age 18-49 years living with genital herpes caused by herpes simplex virus type 2 (HSV-2), plus several additional million persons living with genital herpes caused by herpes simplex virus type 1 (HSV-1) 141. In 2018 alone, approximately 572,000 persons 18-49 years of age newly acquired HSV-2 in the United States 141. Since genital herpes is not a nationally notifiable condition, the true prevalence (persons living with genital herpes) and incidence (new cases of genital herpes) are difficult to accurately determine.
There is no cure for genital herpes, once you’re infected, you have the virus for the rest of your life. Symptoms often show up again after the first outbreak. Medicine can ease symptoms. It also lowers the risk of infecting others. Condoms can help prevent the spread of a genital herpes infection.
Treatment the first time you have genital herpes
- You may be prescribed antiviral medicine to stop the symptoms getting worse, you need to start taking this within 5 days of the symptoms appearing. You doctor may also give you cream for the pain.
Treatment if the blisters come back
- Go to your doctor or STD clinic if you have been diagnosed with genital herpes and need treatment for an outbreak. Antiviral medicine may help shorten an outbreak by 1 or 2 days if you start taking it as soon as symptoms appear. But outbreaks usually settle by themselves, so you may not need treatment. Recurrent outbreaks are usually milder than the first episode of genital herpes. Over time, outbreaks tend to happen less often and be less severe. Some people never have outbreaks.
- Some people who have more than 6 outbreaks in a year may benefit from taking antiviral medicine for 6 to 12 months. If you still have outbreaks of genital herpes during this time, you may be referred to a specialist.
- If you think you have genital herpes, it is important to see a doctor as soon as possible. Your doctor can confirm the diagnosis with testing and start treatment. Anti-viral medication may help to prevent transmission. Talk to your doctor about this in more detail.
- If you have genital herpes, it is important to always use condoms and dental dams when having sex, even when you have no symptoms. A dental dam is a square of thin latex that can be placed over the vulva or anal area during oral sex. It is safest to avoid sex when you have blisters, sores or symptoms.
- It is also important to tell your sexual partners that you have genital herpes. Your doctor can help you decide who to tell and how to tell them.
- If you’re pregnant: It’s important to tell your obstetrician that you or a partner have had genital herpes, so that they can monitor you for symptoms and manage your pregnancy safely. There is a risk you can pass the virus on to your baby if you have a vaginal delivery during a first attack of genital herpes. If this happens you may be recommended to have a caesarean delivery.
Genital herpes cause
Genital herpes is a sexually transmitted disease (STD) caused by two types of herpes viruses – herpes simplex virus type 1 (HSV-1) and herpes simplex virus type 2 (HSV-2) 138. People with HSV infections can pass along the virus even when they have no visible symptoms.
First-episode genital herpes caused by HSV-1 has been identified with increased frequency among young women, college students, and men who have sex with men 142, 143, 144, 145, 146. Acquisition of genital HSV-1 can occur through genital-genital contact or via receptive oral sex 147, 148. In some settings, such as university campuses, HSV-1 has now replaced HSV-2 as the leading cause of first-episode genital herpes 143. One proposed reason for this shift is decreasing HSV-1 orolabial infection in childhood and early adolescence 145, with first exposure to HSV-1 occurring later in life with sexual activity. Changing sex practices in young adults, namely an increase in oral-genital sex, may also contribute to the changing epidemiology of genital herpes 145. General HSV-1 seroprevalence data, such as reported in the National Health and Nutrition Examination Survey (NHANES) studies, do not provide accurate information on genital herpes infections, since it is not possible to determine whether infection is oral or genital with a positive HSV-1 serologic test. Nevertheless, HSV-1 does contribute significantly to the burden of genital HSV, and there are likely at least several million prevalent genital HSV-1 infections in the United States 141.
How is genital herpes spread?
You can get genital herpes by having vaginal, anal, or oral sex with someone who has the disease, often he/she is unaware that he/she has HSV infection 149, 150, 151.
If you do not have herpes, you can get infected if you come into contact with the herpes virus in 152:
- A herpes sore;
- Saliva (if your partner has an oral herpes infection) or genital secretions (if your partner has a genital herpes infection);
- Skin in the oral area if your partner has an oral herpes infection, or skin in the genital area if your partner has a genital herpes infection.
You can get herpes from a sex partner who does not have a visible sore or who may not know he or she is infected. It is also possible to get genital herpes if you receive oral sex from a sex partner who has oral herpes.
- You will not get herpes from toilet seats, bedding, or swimming pools, or from touching objects around you such as silverware, soap, or towels. If you have additional questions about how herpes is spread, consider discussing your concerns with a healthcare provider.
Risk factors for genital herpes
A higher risk of getting genital herpes is linked to:
- Contact with genitals through oral, vaginal or anal sex. Having sexual contact without using a barrier increases your risk of genital herpes. Barriers include condoms and condom-like protectors called dental dams used during oral sex. Women are at higher risk of getting genital herpes. The virus can spread more easily from men to women than from women to men.
- Having sex with multiple partners. The number of people you have sex with is a strong risk factor. Contact with genitals through sex or sexual activity puts you at higher risk. Most people with genital herpes do not know they have it. Each additional sexual partner raises your risk of being exposed to the virus that causes genital herpes.
- Having a partner who has genital herpes but is not taking medicine to treat it. There is no cure for genital herpes, but medicine can help limit outbreaks.
- Certain groups within the population. Women, people with a history of sexually transmitted diseases, older people, Black people in in the United States and men who have sex with men diagnosed with genital herpes at a higher than average rate. Women are more likely to have genital herpes than are men. The virus is sexually transmitted more easily from men to women than it is from women to men. People in groups at higher risk may choose to talk to a health care provider about their personal risk.
Genital herpes prevention
The only way to avoid sexually transmitted diseases (STDs) is to not have vaginal, anal, or oral sex.
If you are sexually active, you can do the following things to lower your chances of getting genital herpes:
- Be in a long-term mutually monogamous relationship with a partner who is not infected with an STD (e.g., a partner who has been tested and has negative STD test results);
- Using latex condoms the right way every time you have sex.
Be aware that not all herpes sores occur in areas that are covered by a latex condom. Also, herpes virus can be released (shed) from areas of the skin that do not have a visible herpes sore. For these reasons, condoms may not fully protect you from getting herpes.
If you are in a relationship with a person known to have genital herpes, you can lower your risk of getting genital herpes if:
- Your partner takes an anti-herpes medication every day. This is something your partner should discuss with his or her doctor.
- You avoid having vaginal, anal, or oral sex when your partner has herpes symptoms (i.e., when your partner is having an outbreak).
Genital herpes signs and symptoms
The symptoms of genital herpes can vary widely, depending upon whether you are having an initial or recurrent episode. However, many people infected with genital herpes have no symptoms, or have very mild symptoms.
The first time a person has noticeable signs or symptoms of herpes may not be the initial episode. For example, it is possible to be infected for the first time, have few or no symptoms, and then have a recurrent outbreak with noticeable symptoms several years later. For this reason, it is often difficult to determine when the initial infection occurred, especially if a person has had more than one sexual partner. Thus, a current sexual partner may not be the source of the infection.
- Most people infected with HSV don’t know they have it because they don’t have any signs or symptoms or because their signs and symptoms are so mild.
When present, symptoms may begin about two to 12 days after exposure to the virus. If you experience symptoms of genital herpes, they may include:
- Pain or itching. You may experience pain and tenderness in your genital area until the infection clears.
- Small red bumps or tiny white blisters. These may appear a few days to a few weeks after infection.
- Ulcers. These may form when blisters rupture and ooze or bleed. Ulcers may make it painful to urinate.
- Scabs. Skin will crust over and form scabs as ulcers heal.
During an initial outbreak, you may have flu-like signs and symptoms such as swollen lymph nodes in your groin, headache, muscle aches and fever.
Differences in symptom location
Sores appear where the infection entered your body. You can spread the infection by touching a sore and then rubbing or scratching another area of your body, including your eyes.
Men and women can develop sores on the:
- Buttocks and thighs
- Anus
- Mouth
- Urethra (the tube that allows urine to drain from the bladder to the outside)
Women can also develop sores in or on the:
- Vaginal area
- External genitals
- Cervix
Men can also develop sores in or on the:
- Penis
- Scrotum
Genital herpes complications
Complications associated with genital herpes may include:
- Other sexually transmitted infections. Having genital sores increases your risk of transmitting or contracting other sexually transmitted infections, including HIV and AIDS.
- Newborn infection. Babies born to infected mothers can be exposed to the virus during the birthing process. Less often, the virus is passed during pregnancy or by close contact after delivery. Even with treatment, these newborns have a high risk of brain damage, blindness or death for the newborn.
- Bladder problems. In some cases, the sores associated with genital herpes can cause inflammation around the tube that delivers urine from your bladder to the outside world (urethra). The swelling can close the urethra for several days, requiring the insertion of a catheter to drain your bladder.
- Internal inflammatory disease. HSV infection can cause swelling and inflammation within the organs associated with sexual activity and urination. These include the ureter, rectum, vagina, cervix and uterus.
- Meningitis. In rare instances, HSV infection leads to inflammation of the membranes and cerebrospinal fluid surrounding your brain and spinal cord.
- Rectal inflammation (proctitis). Genital herpes can lead to inflammation of the lining of the rectum, particularly in men who have sex with men.
- Finger infection. An HSV infection can spread to a finger through a break in the skin causing discoloration, swelling and sores. The infections are called herpetic whitlow.
- Eye infection. HSV infection of the eye can cause pain, sores, blurred vision and blindness.
- Swelling of the brain. Rarely, HSV infection leads to inflammation and swelling of the brain, also called encephalitis.
- Infection of internal organs. Rarely, HSV in the bloodstream can cause infections of internal organs.
Persons with HSV-2 infection have a threefold increase in the risk of acquiring human immunodeficiency virus (HIV) infection 153. This may be related to open ulcers, or lymphocytes at the site of eruptions, facilitating HIV invasion during sexual contact 154.
Concurrent infection with HSV-2 and HIV increases the severity of HSV episodes and the likelihood of atypical presentations 155. The relationship between genital HSV-1 and HIV infections has not been well studied 156.
Genital herpes diagnosis
Your doctor usually can diagnose genital herpes based history of your sexual activity, a physical exam and the results of certain laboratory tests:
- Viral culture. This test involves taking a tissue sample or scraping of the sores for examination in the laboratory.
- Polymerase chain reaction (PCR) test also called nucleic acid amplification test (NAAT). PCR is used to copy your DNA from a sample of your blood, tissue from a sore or spinal fluid. The DNA can then be tested to establish the presence of HSV and determine which type of HSV you have.
- Antigen detection. The use of direct fluorescent antibody (DFA) testing offers lower sensitivity than viral culture or PCR and is not recommended 157.
- Cytologic examination: Cells infected with HSV will show characteristic changes, and these can be observed by obtaining a sample from the lesion and smearing it on a microscope slide (e.g. Tzanck smear). This test is not recommended due to low sensitivity (less than 80%) and lack of differentiation of HSV-1 from HSV-2.
- Blood test. This test analyzes a sample of your blood for the presence of HSV antibodies to detect a past herpes infection.
To confirm a diagnosis of genital herpes, your doctor will likely take a sample from an active sore. One or more tests of these samples are used to see if you have herpes simplex virus (HSV), infection and show whether the infection is HSV-1 or HSV-2.
Less often, a lab test of your blood may be used for confirming a diagnosis or ruling out other infections.
Your doctor will likely recommend that you get tested for other STDs. Your partner should also be tested for genital herpes and other STDs.
Genital herpes treatment
There’s no cure for genital herpes. Treatment with prescription antiviral medications may:
- Help sores heal sooner during an initial outbreak
- Lessen the severity and duration of symptoms in recurrent outbreaks
- Reduce the frequency of recurrence
- Minimize the chance of transmitting the herpes virus to another
Genital herpes anti-viral medications include 1, 139:
- Acyclovir (Zovirax) 400 mg orally 3 times/day for 7–10 days
- OR
- Valacyclovir (Valtrex) 1 gm orally 2 times/day for 7–10 days
- OR
- Famciclovir 250 mg orally 3 times/day for 7–10 days
* Treatment can be extended if healing is incomplete after 10 days of therapy.
Despite some evidence from animal models that early treatment may impact the long-term natural history of the infection, human trials have shown that oral acyclovir treatment of primary genital herpes does not influence the frequency of subsequent genital recurrences 158, 159.
These antiviral drugs will stop the herpes simplex virus multiplying once it reaches the skin or mucous membranes but cannot eradicate the virus from its resting stage within the nerve cells. They can therefore shorten and prevent episodes while the drug is being taken, but a single course cannot prevent future episodes.
Your doctor may prescribe anti-viral medication to help reduce the severity of genital herpes symptoms. This is most effective when started within 72 hours of the first symptoms.
If you have frequent or severe recurrent episodes there are medications available to help control them.
Other treatments being studied include:
- Imiquimod cream, an immune enhancer
- Human leukocyte interferon alpha cream.
Both appear less beneficial than conventional antiviral drugs.
Your doctor may recommend that you take the medicine only when you have symptoms of an outbreak or that you take a certain medication daily, even when you have no signs of an outbreak. These medications are usually well-tolerated, with few side effects.
- Different formulations of topical antiviral creams are available. They are not generally recommended for genital herpes.
Genital warts
Genital warts also called condyloma acuminata, anogenital warts or venereal warts, are a common sexually transmitted infection caused by human papillomavirus (HPV) that are passed on by vaginal and anal sex, sharing sex toys and, rarely, by oral sex. Human papillomavirus (HPV) is a small, non-enveloped, double-stranded DNA virus and there are more than 200 HPV types 160. HPVs are called papillomaviruses because some HPV types cause papillomas (warts), which are non-cancerous tumors. Each HPV virus is given a number, which is called an HPV type. Figure 1 below shows the different groups of HPV types and the problems each group can cause. About 40 of those HPV types affect the genitals. HPV subtypes number 6 and 11 cause 90% of genital warts and are considered low risk because they very rarely will cause genital or anal cancer 161, 162, 163, 164. On the other hand, HPV subtypes 16 and 18, for example, are considered high risk because, although they rarely cause genital warts, they can cause cancer, including cancers of the cervix (the base of the womb at the top of the vagina), vagina, vulva (the area around the outside of the vagina), penis, anus, and parts of the mouth and throat 165, 166. Approximately 65-70% of cervical cancers are caused by HPV types 16 or 18 167. In addition, about 10% of HPV-related cancers are caused by HPV types 31, 33, 45, 52, and 58 161. In the United States, approximately 45,000 HPV-related cancers are diagnosed each year, with cancer of the cervix the most common among women and cancer of the throat (oropharynx) the most common in men 166.
The human papillomavirus (HPV) are spread through sexual contact with an infected partner. HPV is spread by skin-to-skin contact during sexual activity; there does not need to be vaginal or anal intercourse to spread the infection. Most people who become infected with HPV will not have symptoms and will clear the infection on their own. For people who do develop genital warts, there are many options for treatment, all of which are meant to remove the visible warts. There is no cure for genital warts.
In the United States three HPV vaccines are licensed: Ceravrix, a 2-valent vaccine (2vHPV) that targets HPV types 16 and 18; Gardasil, a 4-valent vaccine (4vHPV) that targets HPV types 6, 11, 16, and 18; and Gardasil 9, a 9-valent vaccine (9vHPV) that targets HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58. Types 16 and 18 account for 65-70% of all cervical cancers, whereas the five additional types targeted by the 9-valent vaccine account for 10% 161. HPV types 6 and 11 cause >90% of genital warts. Only Gardasil 9 (9vHPV) vaccine is available in the United States 168.
- Gardasil, a 4-valent vaccine (4vHPV) that protects against the 4 strains of HPV (HPV types 6, 11, 16, and 18) that cause 70% of cervical cancers and 90% of genital warts. In the US, Gardasil is approved for girls/women and boys/men ages 9–26. In 2011, Health Canada approved the vaccine for women up to the age of 45.
- Gardasil 9, a 9-valent vaccine (9vHPV) that targets HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58, is highly effective in preventing urogenital cancers and anogenital warts.
Treatment for genital warts needs to be prescribed by a doctor. The type of treatment you’ll be offered depends on what the warts look like and where they are. Your doctor will discuss this with you.
Genital warts treatments include:
- Cream or liquid: you can usually apply this to the warts yourself a few times a week for several weeks, but in some cases you may need to go to a sexual health clinic where a doctor or nurse will apply it. These treatments can cause pain, irritation or a burning sensation.
- Surgery: a doctor or nurse may cut, burn or use a laser to remove the warts. This can cause pain, irritation or scarring.
- Freezing: a doctor or nurse freezes the warts. Sometimes the treatment is repeated several times. This can cause pain.
It may take weeks or months for treatment to work and the warts may come back. In some people, the treatment does not work.
There’s no cure for genital warts, but it’s possible for your body to fight the virus over time.
Figure 9. HPV types
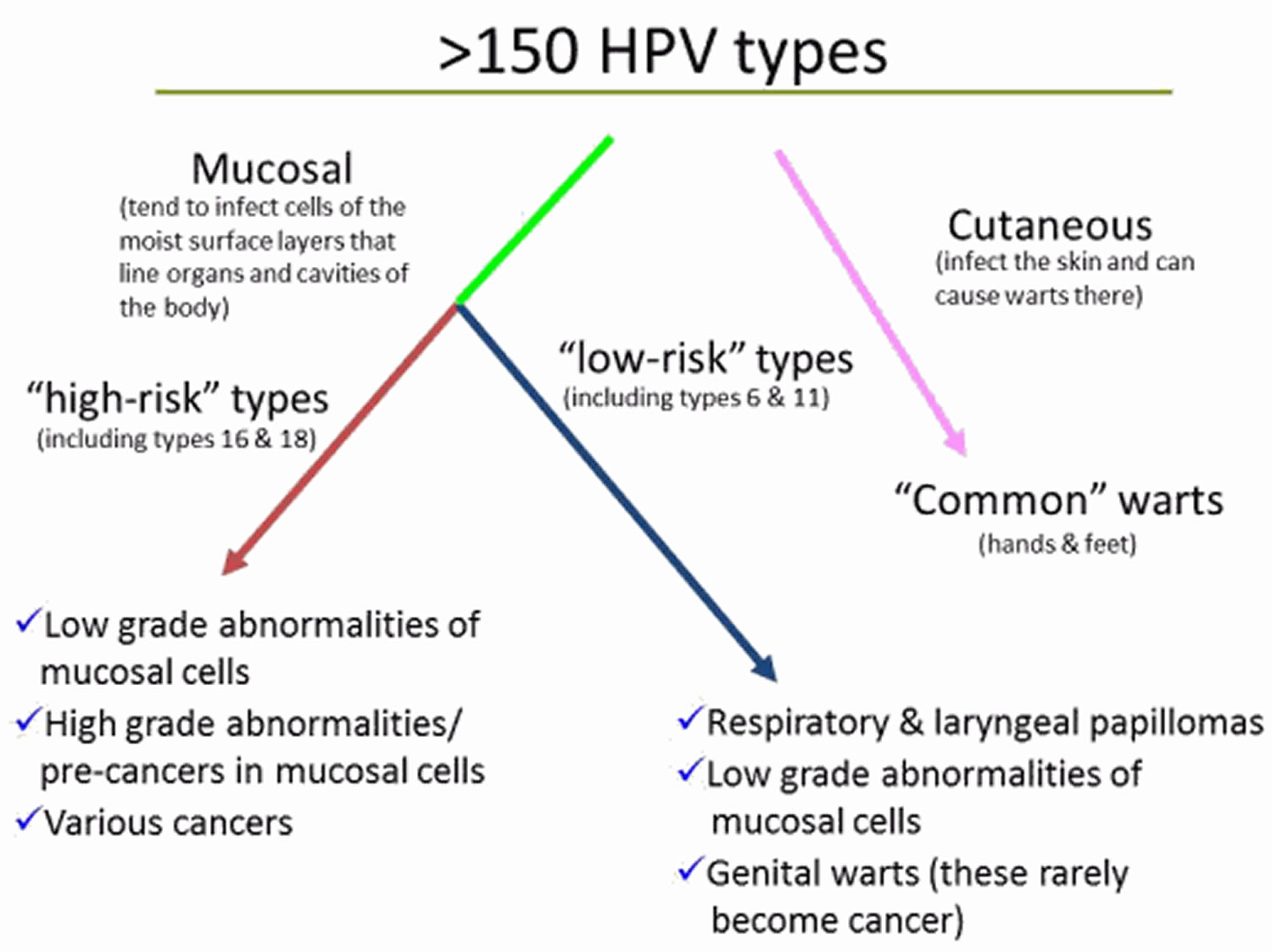
See a doctor or go to a STD clinic if you or your partner develops bumps or warts in the genital area. Genital warts affect the moist tissues of the genital area. They can look like small, flesh-colored bumps or have a cauliflower-like appearance. In many cases, the warts are too small to be visible.
- 1 or more painless growths or lumps around your vagina, penis or anus
- itching or bleeding from your genitals or anus
- a change to your normal flow of pee (for example, it’s begun to flow sideways) that does not go away
- a sexual partner who has genital warts, even if you do not have symptoms
These symptoms mean you may have genital warts. Go to a sexual health clinic to be checked.
Sexual health clinics are sometimes called STD clinics, or sexual and reproductive health services.
Treatment can help remove the warts and stop the infection being passed on.
Genital warts causes
Anogenital warts are an infection caused by specific human papillomavirus (HPV) types, most commonly HPV types 6 and 11. Anogenital warts will usually appear three to six months after infection but they may appear months or even years later. Anogenital warts are usually a sexually transmitted infection (STI) due to friction-induced microabrasions during skin-to-skin contact 162. Transmission rates of HPV between sex partners are high, and transmission often occurs from persons with HPV who are asymptomatic or have subclinical infection 169, 170. Consistent and correct use of condoms reduces the risk for genital HPV acquisition or transmission, and therefore reduces the risk for HPV-associated diseases 171. Condom use, however, does not entirely prevent transmission of HPV, since exposure to HPV can occur in areas that are not fully covered or protected by a condom 165. Treatment of warts or cervical cellular abnormalities will reduce, but not eliminate, the risk of transmission. Transmission of HPV through nonsexual routes can occur, but is uncommon 172, 173. Mothers with low-risk genital HPV types can rarely transmit HPV to their newborn during delivery, but if transmission does occur, HPV has the potential to cause recurrent respiratory papillomatosis in children 174, 175.
Genital warts are almost always spread through sexual activity. Your warts don’t have to be visible for you to spread the infection to your sexual partner.
- Sexual contact. This is the most common way amongst adults. Transmission is more likely from visible warts than from subclinical or latent HPV infection.
- Oral sex. HPV appears to prefer the genital area to the mouth.
- Vertical (mother to baby) transmission through the birth canal.
- Auto (self) inoculation from one site to another.
As anogenital warts are usually sexually acquired, they are most commonly observed in young adults between the ages of 15 and 30 years. They are highly contagious. However, anogenital warts are rare in people who have been vaccinated against the benign HPV types in childhood before beginning sexual activity. Anogenital warts have been reported in a number of studies to be more common in males than females.
Patients who are immunocompromised due to drug-induced immunosuppression or HIV infection are at particular risk of acquiring HPV and developing anogenital warts.
Anogenital warts can also affect infants and young children. The virus may be acquired during birth or from the hands of carers.
Risk factors for getting genital warts
Most people who are sexually active get infected with genital HPV at some time. Factors that can increase your risk of becoming infected include:
- Having unprotected sex with multiple partners
- Having had another sexually transmitted infection
- Having sex with a partner whose sexual history you don’t know
- Becoming sexually active at a young age
- Having a compromised immune system, such as from HIV or drugs from an organ transplant
Genital warts prevention
Limiting your number of sexual partners and being vaccinated will help prevent you from getting genital warts. Using a condom every time you have sex is a good idea, but won’t necessarily protect you from genital warts.
HPV vaccination
The Centers for Disease Control and Prevention (CDC) recommends routine HPV vaccination for girls and boys ages 11 and 12, although it can be given as early as age 9. It’s ideal for girls and boys to receive the HPV vaccine before they have sexual contact 168.
Side effects from the HPV vaccines are usually mild and include soreness at the injection site, headaches, a low-grade fever or flu-like symptoms.
The CDC now recommends that all 11- and 12-year-olds receive two doses of HPV vaccine at least six months apart, instead of the previously recommended three-dose schedule. Younger adolescents ages 9 and 10 and teens ages 13 and 14 also are able to receive vaccination on the updated two-dose schedule. Research has shown that the two-dose schedule is effective for children under 15.
Teens and young adults who begin the vaccine series later, at ages 15 through 26, should continue to receive three doses of the vaccine.
The CDC now recommends catch-up HPV vaccinations for all people through age 26 who aren’t adequately vaccinated.
The U.S. Food and Drug Administration (FDA) recently approved the use of Gardasil 9 for males and females ages 9 to 45. If you’re ages 27 to 45, discuss with your doctor whether he or she recommends that you get the HPV vaccine.
In the United States three HPV vaccines are licensed: Ceravrix, a 2-valent vaccine (2vHPV) that targets HPV types 16 and 18; Gardasil, a 4-valent vaccine (4vHPV) that targets HPV types 6, 11, 16, and 18; and Gardasil 9, a 9-valent vaccine (9vHPV) that targets HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58. Types 16 and 18 account for 65-70% of all cervical cancers, whereas the five additional types targeted by the 9-valent vaccine account for 10% 161. HPV types 6 and 11 cause >90% of genital warts. Since late 2016, only Gardasil 9 (9vHPV) vaccine is available in the United States 168.
- Gardasil, a 4-valent vaccine (4vHPV) that protects against the 4 strains of HPV (HPV types 6, 11, 16, and 18) that cause 70% of cervical cancers and 90% of genital warts. In the US, Gardasil is approved for girls/women and boys/men ages 9–26. In 2011, Health Canada approved the vaccine for women up to the age of 45.
- Gardasil 9, a 9-valent vaccine (9vHPV) that targets HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58, is highly effective in preventing urogenital cancers and anogenital warts.
HPV vaccine may be available at doctor offices, community health clinics, school-based health centers, and health departments.
Who should NOT get HPV vaccine?
Tell your doctor about any severe allergies. Some people should NOT get some HPV vaccines if:
- They have ever had a life-threatening allergic reaction to any ingredient of an HPV vaccine, or to a previous dose of HPV vaccine.
- They have an allergy to yeast (Gardasil and Gardasil 9).
- They are pregnant.
HPV vaccines are safe for children who are mildly ill, like those with a low-grade fever of less than 101 degrees, a cold, runny nose, or cough. People with a moderate or severe illness should wait until they are better.
Genital warts signs and symptoms
Genital warts affect the moist tissues of your genital area. Genital warts can look like small, flesh-colored bumps or have a cauliflower-like appearance with a folded irregular surface a few millimeters in diameter. In many cases, the warts are too small to be visible. Genital warts may join together to form plaques up to several centimeters across. A linear pattern may be seen if the HPV virus has been inoculated along a scratch or tear in the skin.
In women, genital warts can grow on the vulva, the walls of the vagina, the area between the external genitals and the anus, the anal canal, and the cervix. In men, they may occur on the tip or shaft of the penis, the scrotum, or the anus.
Genital warts can also develop in the mouth, throat, around the lips and conjunctiva of the eye of a person who has had oral sexual contact with an infected person.
The signs and symptoms of genital warts include:
- Small, flesh-colored, brown or pink swellings in your genital area
- A cauliflower-like shape caused by several warts close together
- Itching or discomfort in your genital area
- Bleeding with intercourse
Genital warts can be so small and flat as to be invisible. Rarely, however, genital warts can multiply into large clusters in someone with a suppressed immune system.
Genital warts complications
Anogenital warts are contagious and easily spread to your sexual partners. Anogenital warts can impact psychosexual functioning and quality of life.
HPV infection complications can include:
- Cancer. Cervical cancer has been closely linked with genital HPV infection. Certain types of HPV also are associated with cancers of the vulva, anus, penis, and mouth and throat. HPV infection doesn’t always lead to cancer, but it’s important for women to have regular Pap tests, particularly those who’ve been infected with higher risk types of HPV.
- Problems during pregnancy. Rarely during pregnancy, warts can enlarge and multiply, making it difficult to urinate. Warts on the vaginal wall can inhibit the stretching of vaginal tissues during childbirth. Large warts on the vulva or in the vagina can bleed when stretched during delivery. Extremely rarely, a baby born to a mother with genital warts develops warts in the throat. The baby might need surgery to keep the airway from being blocked. HPV can be transmitted to the baby resulting in recurrent respiratory papillomatosis in the infant.
Genital warts diagnosis
Anogenital warts are usually diagnosed clinically by their appearance.
Skin biopsy is sometimes necessary to confirm the diagnosis of viral wart, particularly if there is concern of anogenital cancer.
In some circumstances, researchers and clinicians may wish to confirm the presence or absence of HPV. One commercially available qualitative test for HPV is the COBAS 4800 Human Papillomavirus (HrHPV) Test, which evaluates 14 high-risk (HR oncogenic) HPV types.
Pap tests
For women, it’s important to have regular pelvic exams and Pap tests, which can help detect vaginal and cervical changes caused by genital warts or the early signs of cervical cancer.
During a Pap test, your doctor uses a device called a speculum to hold open your vagina and see the passage between your vagina and your uterus (cervix). He or she will then use a long-handled tool to collect a small sample of cells from the cervix. The cells are examined with a microscope for abnormalities.
HPV test
Only a few types of genital HPV have been linked to cervical cancer. A sample of cervical cells, taken during a Pap test, can be tested for these cancer-causing HPV strains.
This test is generally reserved for women age 30 and older. It isn’t as useful for younger women because for them, HPV usually goes away without treatment.
Genital warts treatment
There is no cure for genital warts. The goal of treatment is to remove visible warts and decrease the risk of spreading the virus 176. However, available therapies reduce but do not completely eliminate the risk of HPV transmission 177. In addition, there are no data that suggest treatment of genital warts impacts the subsequent risk of anogenital HPV-related cancer 177. Although appropriate treatment can induce wart-free periods, subsequent recurrences are common, with a 20 to 50% recurrence rate at 3 to 6 months post-treatment 178. Reappearance of genital warts within the first several months usually indicates recurrence rather than reinfection. If left untreated, visible genital warts persist with or without rapid increase in the number, but some regress spontaneously. Because spontaneous resolution of anogenital warts can occur, some individuals may choose to defer treatment and await possible spontaneous resolution 177. In addition, there are no data that suggest treatment of genital warts impacts the subsequent risk of anogenital HPV-related cancer 177.
If your warts aren’t causing discomfort, you might not need treatment. But if you have itching, burning and pain, or if you’re concerned about spreading the infection, your doctor can help you clear an outbreak with medications or surgery. However, warts often return after treatment. There is no treatment for the HPV virus itself.
Home remedies for genital warts
To be successful you must identify and reach the warts, and follow the application instructions carefully. Available treatments include:
- Podophyllotoxin 0.5% gel or solution (Condylox®). This should not be used during pregnancy.
- Imiquimod 3.75% cream (Zyclara). Imiquimod cream appears to boost your immune system’s ability to fight genital warts. Apply once daily for up to 8 weeks. Avoid sexual contact while the cream is on your skin. It might weaken condoms and diaphragms and irritate your partner’s skin. One possible side effect is skin redness. Other side effects might include blisters, body aches or pain, a cough, rashes, and fatigue.
- Imiquimod 5% cream (Aldara). Apply once daily (at bedtime) 3 times a week for up to 16 weeks.
- Sinecatechins (Veregen). Sinecatechins cream is used for treatment of external genital warts and warts in or around the anal canal. Sinecatechins 15% ointment should be administered 3 times/day using a finger to apply a 0.5 cm strand of ointment to each anogenital wart; the goal is to cover the wart entirely with a thin layer of the sinecatechins. The ointment should not be washed off after application. Genital, anal, and oral sexual contact should be avoided while sinecatechins ointment is present on the skin. This treatment can be administered for up to 16 weeks. Treatment with sinecatechins is not recommended for persons with genital herpes or for immunocompromised persons, including those with HIV. Side effects, such as reddening of the skin, itching or burning, and pain, are often mild.
Don’t try to treat genital warts with over-the-counter wart removers. These medications aren’t intended for use in the genital area.
Treatments provided at a medical clinic
Genital wart treatments that can be applied directly to your skin by a physician:
- Imiquimod (Aldara, Zyclara). This cream appears to boost your immune system’s ability to fight genital warts. Avoid sexual contact while the cream is on your skin. It might weaken condoms and diaphragms and irritate your partner’s skin. One possible side effect is skin redness. Other side effects might include blisters, body aches or pain, a cough, rashes, and fatigue.
- Podophyllin and podofilox (Condylox). Podophyllin is a plant-based resin that destroys genital wart tissue. Your doctor applies 15–25% solution. Podofilox contains the same active compound, but you can apply it at home. Never apply podofilox internally. Additionally, this medication isn’t recommended for use during pregnancy. Podophyllin resin has been associated with multiple reports of systemic toxicity when this agent was applied to large lesions or when left on for longer periods than recommended 179. Side effects can include mild skin irritation, sores or pain.
- Trichloroacetic acid (TCA) or bichloroacetic acid (BCA) 80%–90% solution: The application of trichloroacetic acid or bichloroacetic acid 80-90% solution should only be performed by an individual with training in this application and for treatment of small lesions and can be used for internal warts. These acid agents destroy wart tissue by causing chemical coagulation of proteins. Only a small amount of the solution should be applied to the wart and the solution should dry before the patient moves. If too much is applied or the patient experiences pain, sodium bicarbonate (i.e. baking soda) can be applied to neutralize the acid; the sodium bicarbonate is typically applied as a liquid soap preparation or powdered with talc. Side effects can include mild skin irritation, sores or pain.
- Freezing with liquid nitrogen (cryotherapy). Liquid nitrogen is used to freeze the warts. Freezing works by causing a blister to form around your wart. As your skin heals, the lesions slough off, allowing new skin to appear. You might need to repeat the treatment. The main side effects include pain and swelling.
- Surgical removal. This may need to be performed by a specialist with local anesthesia; usually for large amounts of warts and you might have pain afterward. You might need surgery to remove larger warts, warts that don’t respond to medications or, if you’re pregnant, warts that your baby can be exposed to during delivery.
- Laser treatment. Carbon dioxide laser treatment is useful for a large amount of urethral or vaginal warts. Side effects can include scarring and pain.
- Electrocautery. This procedure uses an electrical current to burn off warts. You might have some pain and swelling after the procedure.
Most of these treatments require multiple applications. If there is no improvement after 3 treatment cycles or if the warts are not gone after 6 treatment cycles, your doctor will usually switch you to a different medication. Common side effects of all treatments include skin irritation and redness. Some people may also develop scars at the site of the warts.
Genital warts during pregnancy
Genital warts can proliferate rapidly and become more friable during pregnancy. Watchful waiting is acceptable with smaller lesions. During pregnancy, cryotherapy, trichloroacetic acid, bichloroacetic acid, and surgical removal may be safely used 176. Cytotoxic agents (podophyllin, podofilox, imiquimod) should not be used during pregnancy 176. Although pregnant women with genital warts have a risk of transmitting HPV to their child during a vaginal birth, Cesarean section delivery should not be performed solely to prevent transmission to the neonate, since it is unclear whether Cesarean delivery prevents respiratory papillomatosis among infants 176.
Genital warts in immunocompromised patients
The general approach to the treatment of genital warts in persons with HIV is the same as for those without HIV 176. Persons with HIV, particularly those individuals with advanced immunosuppression, often have larger or more numerous warts that do not respond as well to therapy, and recurrences occur more frequently after treatment. High-grade squamous intraepithelial lesions (HSIL) and invasive cancer arising within the region of a genital wart (or resembling genital warts) are more frequent in immunocompromised patients; therefore, hyperpigmented lesions and lesions that persist despite treatment (especially in the perianal area) should be promptly evaluated by biopsy. The role of genital warts (or irritated post-treatment sites) in HIV transmission has not been well characterized.
Syphilis
Syphilis is a complex sexually transmitted disease (STD) or sexually transmitted infection (STI) caused by the bacteria Treponema pallidum. Syphilis can cause serious health problems if not adequately treated. Episodes of active disease occur, followed by latent periods, when the person remains infected but there are no signs or symptoms. Syphilis is transmitted from person to person by direct contact with a syphilitic sore, known as a chancre 180. Chancres can occur on or around the external genitals, in the vagina, around the anus or in the rectum, or in or around the mouth. Transmission of syphilis can occur during vaginal, anal, or oral sex. In addition, pregnant women with syphilis can transmit the infection to their unborn children.
The average time between acquisition of syphilis and the start of the first symptom is 21 days, but can range from 10 to 90 days.
Some people with syphilis have no symptoms, so you may not know you have it unless you get tested. The signs and symptoms of syphilis depend on the stage of disease. There are 4 stages of syphilis infection: primary, secondary, latent and tertiary.
Primary syphilis appears as a painless sore (ulcer) where the infection entered your body (usually around the penis, vagina, cervix, anus or mouth) and may go unnoticed. The sore is known as a chancre and this phase is known as primary syphilis. There may also be swollen lymph nodes.
Primary syphilis occurs 3 or 4 weeks after infection (although it can take up to 90 days for the sore to appear).
The sore, or sometimes multiple sores, can go unnoticed because it is usually painless and may be hidden from view in areas such as the back of the throat, vagina or anus.
These sores usually go away by themselves after 3 to 6 weeks, even with no treatment. However, even though the sore heals, if you haven’t been treated, you are still infectious and can pass it on to others.
Secondary syphilis can occur 7 to 10 weeks after the initial infection. Symptoms can last for 6 months or more and may include:
- a red rash on the palms, soles, chest or back
- fever
- enlarged glands in the armpits and groin
- sore throat
- hair loss
- weight loss
- headaches
- pain in the bones, muscles and joints
- tiredness
- ulcers in the mouth, nasal cavity or genitals
- neurological symptoms
After the initial infection, the syphilis bacteria, Treponema pallidum, can remain inactive in your body for decades before becoming active again, this is known as the latent (sleeping) syphilis stage. Generally the person with latent stage syphilis has no symptoms and it is only picked up on blood tests. If syphilis is not treated at this stage, it can remain latent or develop into tertiary syphilis. Latent syphilis is infectious within the first 12 to 24 months.
If the latent stage syphilis is left untreated, tertiary syphilis may develop 5 to 20 years after the primary infection. At the tertiary syphilis stage, the bacteria can damage almost any part of your body including your heart, brain, spinal cord, eyes and bones, resulting in heart disease, mental illness, blindness, deafness and neurological problems and can be life-threatening
Early syphilis can be cured, sometimes with a single shot (injection) of penicillin. If you’re allergic to penicillin, your doctor may suggest another antibiotic or recommend penicillin desensitization.
After you’ve been treated for syphilis, your doctor will ask you to:
- Have periodic blood tests and exams to make sure you’re responding to the usual dosage of penicillin. Your specific follow-up will depend on the stage of syphilis you’re diagnosed with.
- Avoid sexual contact with new partners until the treatment is completed and blood tests indicate the infection has been cured.
- Notify your sex partners so that they can be tested and get treatment if necessary.
- Be tested for HIV infection.
Figure 10. Treponema pallidum bacteria
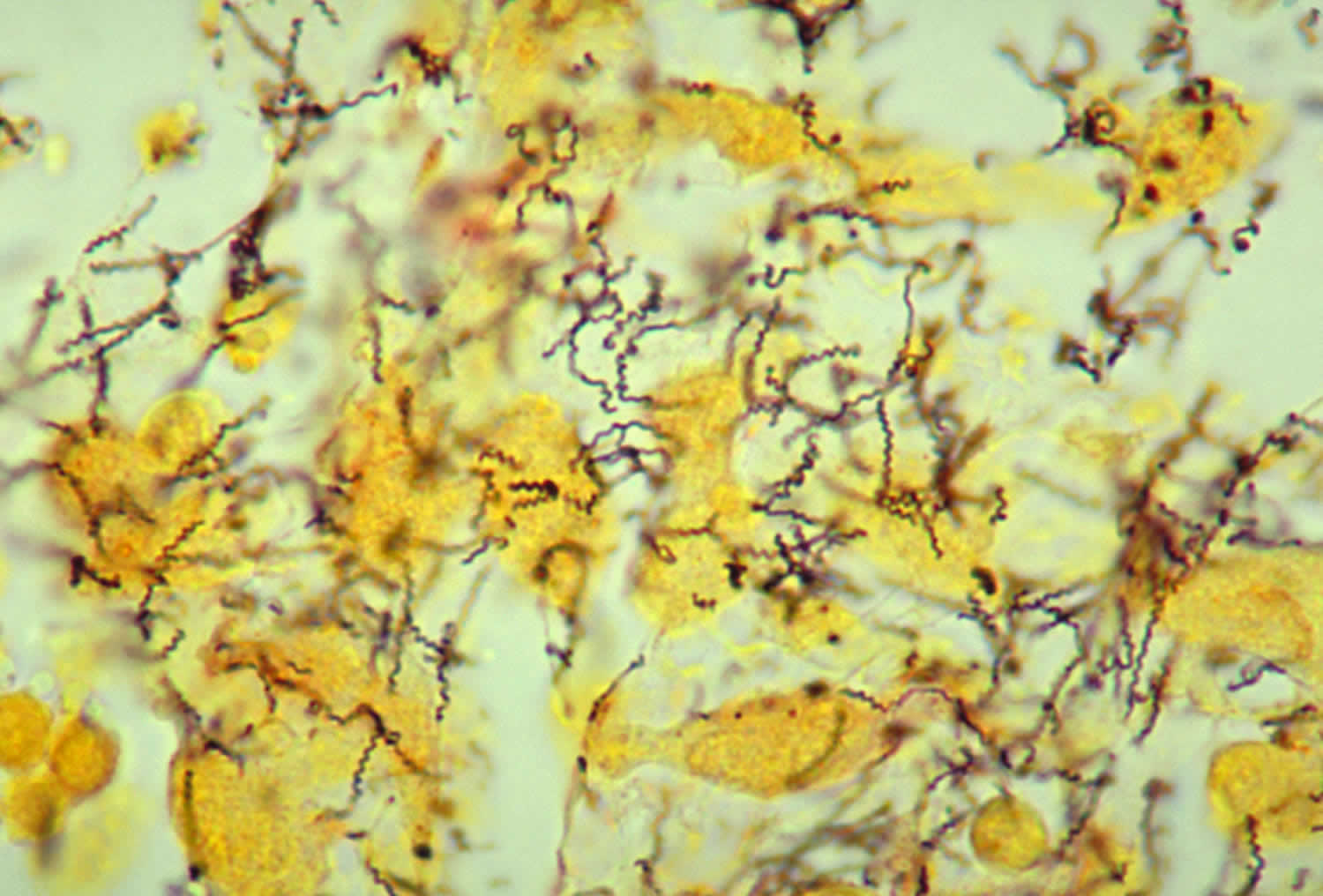
Footnote: This photomicrograph depicted a tissue sample, which had been prepared using the Steiner silver stain method. The image revealed the presence of numerous, corkscrew-shaped, darkly-stained, Treponema pallidum spirochetes. Treponema pallidum is the bacterium responsible for causing syphilis.
[Source 181 ]See your doctor if you or your child experiences any unusual discharge, sore or rash — particularly if it occurs in the groin area.
How is syphilis spread?
You can get syphilis by direct contact with a syphilis sore during vaginal, anal, or oral sex. Syphilis can also spread from a mother with syphilis to her unborn baby.
You cannot get syphilis through casual contact with objects, such as:
- toilet seats
- doorknobs
- swimming pools
- hot tubs
- bathtubs
- sharing clothing, or eating utensils
What is the treatment for syphilis?
There are no home remedies or over-the-counter drugs that will cure syphilis, but syphilis is easy to cure in its early stages. A single intramuscular injection of long acting Benzathine penicillin G (2.4 million units administered intramuscularly) will cure a person who has primary, secondary or early latent syphilis. Three doses of long acting Benzathine penicillin G (2.4 million units administered intramuscularly) at weekly intervals is recommended for individuals with late latent syphilis or latent syphilis of unknown duration. Treatment will kill the syphilis bacterium and prevent further damage, but it will not repair damage already done.
Selection of the appropriate penicillin preparation is important to properly treat and cure syphilis. Combinations of some penicillin preparations (e.g., Bicillin C-R, a combination of benzathine penicillin and procaine penicillin) are not appropriate treatments for syphilis, as these combinations provide inadequate doses of penicillin.
Although data to support the use of alternatives to penicillin is limited, options for non-pregnant patients who are allergic to penicillin may include doxycycline, tetracycline, and for neurosyphilis, ceftriaxone. These therapies should be used only in conjunction with close clinical and laboratory follow-up to ensure appropriate serological response and cure.
Persons who receive syphilis treatment must abstain from sexual contact with new partners until the syphilis sores are completely healed. Persons with syphilis must notify their sex partners so that they also can be tested and receive treatment if necessary.
Is syphilis curable?
Yes, syphilis can be cured with the right antibiotics from your health care provider. However, treatment might not undo any damage that the infection has already done.
Will syphilis recur?
After appropriate treatment, syphilis does not recur. However, having syphilis once does not protect a person from becoming infected again. Even following successful treatment, people can be reinfected. Patients with signs or symptoms that persist or recur or who have a sustained fourfold increase in nontreponemal test titer probably failed treatment or were reinfected. These patients should be retreated.
Because chancres can be hidden in the vagina, rectum, or mouth, it may not be obvious that a sex partner has syphilis. Unless a person knows that their sex partners have been tested and treated, they may be at risk of being reinfected by an untreated partner.
How common is syphilis?
During 2016, there were 88,042 reported new diagnoses of syphilis (all stages), compared to 39,513 estimated new diagnoses of HIV infection in 2015 and 468,514 cases of gonorrhea in 2016 182. Of syphilis cases, 27,814 were primary and secondary syphilis, the earliest and most transmissible stages of syphilis. In 2016, the majority of primary and secondary syphilis cases occurred among gay, bisexual, and other men who have sex with men. In 2016, men who have sex with men accounted for 80.6% of all primary and secondary syphilis cases among males in which sex of sex partner was known and 58% of all P&S syphilis cases overall. However, in recent years, the rate of primary and secondary syphilis has been increasing among men who have sex with men as well as heterosexual men and women.
Congenital syphilis (syphilis passed from pregnant women to their babies) continues to be a concern in the United States. During 2016, 628 cases of congenital syphilis were reported, compared to an estimated 86 cases of perinatal HIV infection during 2015. 1 In 2016, congenital syphilis rates were 8.0 times and 3.9 times higher among infants born to black and Hispanic mothers (43.1 and 20.5 cases per 100,000 live births, respectively) compared to white mothers (5.3 cases per 100,000 live births).
Who should be tested for syphilis?
Any person with signs or symptoms suggestive of syphilis should be tested for syphilis. Also, anyone with an oral, anal, or vaginal sex partner who has been recently diagnosed with syphilis should be tested for syphilis.
Some people should be tested (screened) for syphilis even if they do not have symptoms or know of a sex partner who has syphilis. Anyone who is sexually active should discuss his or her risk factors with a health care provider and ask whether he or she should be tested for syphilis or other STDs.
In addition, providers should routinely test for syphilis in persons who:
- are pregnant;
- are sexually active men who have sex with men (MSM);
- are living with HIV and are sexually active;
- are taking PrEP for HIV prevention.
How can I reduce my risk of getting syphilis?
The only way to avoid STDs is to not have vaginal, anal, or oral sex.
If you are sexually active, you can do the following things to lower your chances of getting syphilis:
- Being in a long-term mutually monogamous relationship with a partner who has been tested for syphilis and does not have syphilis;
- Using latex condoms the right way every time you have sex. Condoms prevent transmission of syphilis by preventing contact with a sore. Sometimes sores occur in areas not covered by a condom. Contact with these sores can still transmit syphilis.
Am I at risk for syphilis?
Any sexually active person can get syphilis through unprotected vaginal, anal, or oral sex. Have an honest and open talk with your health care provider and ask whether you should be tested for syphilis or other STDs.
- All pregnant women should be tested for syphilis at their first prenatal visit.
- You should get tested regularly for syphilis if you are sexually active and
- are a man who has sex with men;
- are living with HIV; or
- have partner(s) who have tested positive for syphilis.
I’ve been treated. Can I get syphilis again?
Having syphilis once does not protect you from getting it again. Even after you’ve been successfully treated, you can still be re-infected. Only laboratory tests can confirm whether you have syphilis. Follow-up testing by your health care provider is recommended to make sure that your treatment was successful.
It may not be obvious that a sex partner has syphilis. This is because syphilis sores can be hidden in the vagina, anus, under the foreskin of the penis, or in the mouth. Unless you know that your sex partner(s) has been tested and treated, you may be at risk of getting syphilis again from an infected sex partner.
I’m pregnant. How does syphilis affect my baby?
If you are pregnant and have syphilis, you can give the infection to your unborn baby. Having syphilis can lead to a low birth weight baby. It can also make it more likely you will deliver your baby too early or stillborn (a baby born dead) or of giving birth to a baby who dies shortly after birth. Untreated syphilis in pregnant women results in infant death in up to 40 percent of cases. To protect your baby, you should be tested for syphilis at least once during your pregnancy. Receive immediate treatment if you test positive.
An infected baby born alive may not have any signs or symptoms of disease. However, if not treated immediately, the baby may develop serious problems within a few weeks. Untreated babies may become developmentally delayed and can have health problems such as cataracts, deafness, or seizures, and can die. All babies born to mothers who test positive for syphilis during pregnancy should be screened for syphilis and examined thoroughly for evidence of congenital syphilis 183.
All pregnant women should be tested for syphilis at the first prenatal visit. For women who are at high risk for syphilis, live in areas of high syphilis morbidity, are previously untested, or had a positive screening test in the first trimester, the syphilis screening test should be repeated during the third trimester (28 to 32 weeks gestation) and again at delivery 183. Any woman who delivers a stillborn infant after 20 week’s gestation should also be tested for syphilis.
For pregnant women only penicillin therapy can be used to treat syphilis and prevent passing the disease to her baby; treatment with penicillin is extremely effective (success rate of 98%) in preventing mother-to-child transmission 184. Pregnant women who are allergic to penicillin should be referred to a specialist for desensitization to penicillin.
What causes syphilis?
Syphilis is caused by bacteria called Treponema pallidum (Figure 10). You can get syphilis by having sex with an infected person (coming into direct contact with a syphilis sore). It can also be passed from an infected mother to her baby during pregnancy.
Syphilis stages
Syphilis is divided into 4 stages: primary, secondary, latent, and tertiary. The signs and symptoms of syphilis depend on the stage of disease. A person with primary syphilis generally has a sore or sores at the original site of infection. These sores usually occur on or around the genitals, around the anus or in the rectum, or in or around the mouth. These sores are usually (but not always) firm, round, and painless. Symptoms of secondary syphilis include skin rash, swollen lymph nodes, and fever. The signs and symptoms of primary and secondary syphilis can be mild, and they might not be noticed. During the latent stage, there are no signs or symptoms. Tertiary syphilis is associated with severe medical problems. A doctor can usually diagnose tertiary syphilis with the help of multiple tests. It can affect the heart, brain, and other organs of the body.
Primary syphilis
During the first (primary) stage of syphilis, you may notice a single sore called chancre or multiple sores. The sore (chancre) is the location where syphilis entered your body. The chancres are usually (but not always) firm, round, and painless. Because the sore is painless, it can easily go unnoticed. These painless chancres can occur in locations that make them difficult to notice (e.g., the vagina or anus). The sore usually lasts 3 to 6 weeks and heals regardless of whether or not you receive treatment. Even after the sore goes away, you must still receive treatment. This will stop your infection from moving to the secondary stage. However, if the infected person does not receive adequate treatment, the infection progresses to the secondary stage.
- Single small firm red painless papule quickly ulcerates (chancre). Heals within 4-8 weeks without treatment, and within 1 to 2 weeks with appropriate treatment. Sores may be inside the vagina or anus and often go unnoticed.
- Unilateral enlargement of lymph nodes close to the ulcer develops about 5 weeks after acquiring infection. Inguinal lymphadenopathy arises in men with ulcers on the genitals and cervical lymphadenopathy in patients with ulcers in the mouth. If a syphilis ulcer is located in the vagina or rectum, the lymphadenopathy can be only detected by pelvic ultrasound examination.
Figure 11. Syphilis chancre

Secondary syphilis
During the secondary stage, you may have skin rashes and/or mucous membrane lesions. Mucous membrane lesions are sores in your mouth, vagina, or anus. This stage usually starts with a rash on one or more areas of your body. The rash can show up when your primary sore is healing or several weeks after the sore has healed. The rash can look like rough, red, or reddish brown spots on the palms of your hands and/or the bottoms of your feet. The rash usually won’t itch and it is sometimes so faint that you won’t notice it. Other symptoms you may have can include fever, swollen lymph glands, sore throat, patchy hair loss, headaches, weight loss, muscle aches, and fatigue (feeling very tired). The symptoms from this stage will go away whether or not you receive treatment. Without the right treatment, your infection will move to the latent and possibly tertiary stages of syphilis.
- Patient is very infectious during this stage.
- If left untreated or treatment has failed, about 3 weeks to 3 months after the 1st stage, a widespread skin rash occurs.
- Rash may be subtle or appear as rough, red or reddish brown papules or patches. Occurs typically on the trunk and frequently affects palms and soles. May be mistaken for other conditions. The rash does not itch. It can appear more obvious with physical activity or heat. It resolves spontaneously within several weeks but can recur during the following 2 years.
- Corymbose syphilis describes a cluster of erythematous papules around a central scaly plaque (resembling a flower).
- Patchy hair loss.
- Raw and red mucosal surfaces such as inside the mouth, throat, genital area, vagina and anus (mucous patches).
- Unilateral tonsilitis, which may be ulcerated and accompanied by cervical lymph node enlargement. Can be mistaken for common tonsilitis but does not respond to usual oral antibiotics.
- Greyish-white moist raised patches in the groin, inner thighs, armpits, umbilicus, or under breasts (condyloma lata).
- Other symptoms include fever, tiredness, muscle and joint pains, headache and swollen lymph glands.
- Other affected organs may include liver, kidneys, central nervous system (CNS), joints and eyes (resulting in visual impairment).
Figure 12. Secondary syphilis (hands rash – subtle rough, red or reddish brown papules or patches)


Figure 13. Secondary syphilis (foot rash – subtle rough, red or reddish brown papules or patches)

Latent syphilis
The latent (hidden) stage of syphilis is a period of time when there are no visible signs or symptoms of syphilis. Without treatment, the infected person will continue to have syphilis in their body even though there are no signs or symptoms. Early latent syphilis is latent syphilis where infection occurred within the past 12 months. Late latent syphilis is latent syphilis where infection occurred more than 12 months ago. Latent syphilis can last for years.
Early latent syphilis (first 2 years)
- Patient is infectious and can pass the infection on to partner.
- Usually normal,i.e. no signs on clinical examination.
- Continued infection found by positive treponemal antibody tests.
Late latent syphilis (after 2 years)
- Patient is non-infectious.
- Usually normal,i.e. no signs on clinical examination.
- Continued infection found by positive treponemal antibody tests
Tertiary syphilis
Most people with untreated syphilis do not develop tertiary syphilis. However, when it does happen it can affect many different organ systems. These include the heart and blood vessels, and the brain and nervous system. Tertiary syphilis is very serious and would occur 10–30 years after your infection began. In tertiary syphilis, the disease damages your internal organs and can result in death.
- Signs and symptoms may develop 3 to 10 years after initial infection, and corresponds with immunological response to the infection. Tertiary syphilis is very rare in developed countries.
- Solitary granulomatous lesions (gummas) may be found on the skin, in the mouth and throat or occur in bones. Small or large nodules or ulcers may persist for years. Skin lesions may be painless but gummas in long bones cause a deep boring pain that is worse at night.
- Brain involvement (neurosyphilis) may cause headaches, dizziness, blurred vision, mental disturbances, paralysis and dementia (general paresis). This occurs 10–30 years after infection.
- Spinal cord disease results in unsteady gait, bladder disturbance, impotence and sensory changes (tabes dorsalis) resulting in collapsed joints (Charcot’s joints) and foot ulcers.
- Other internal organs such as the heart, blood vessels, eyes, liver and blood may be damaged by infection.
Figure 14. Tertiary syphilis

Neurosyphilis and Ocular Syphilis
Without treatment, syphilis can spread to the brain and nervous system (neurosyphilis) or to the eye (ocular syphilis) or ear (otosyphilis). This can happen during any of the stages described above.
Symptoms of neurosyphilis include:
- severe headache;
- difficulty coordinating muscle movements;
- paralysis (not able to move certain parts of your body);
- numbness; and
- dementia (mental disorder).
Symptoms of ocular syphilis include changes in your vision and even blindness.
Congenital syphilis
- Congenital syphilis can be prevented by treatment prior to 16 weeks gestation.
- The risk to the fetus is greatest with early untreated maternal syphilis
- Miscarriage or stillbirth may occur.
- In the first few weeks of life, effects resemble secondary syphilis including blisters, scaly rash, mucous patches and condyloma latum (very infectious).
- Snuffles, inflamed bones, swollen liver and lymph glands are common.
- Blood changes include anemia, reduced platelets, and increased white cells.
- Late congenital syphilis often affects eyes (interstitial keratitis), ears, joints and CNS.
- Characteristic signs include Hutchinson’s teeth, typical facial appearance and bowed sabre shins.
Figure 15. Congenital syphilis

Figure 16. Congenital syphilis – Hutchinson’s teeth

Syphilis signs and symptoms
The signs and symptoms of syphilis depend on the stage of disease. The symptoms of syphilis are similar for men and women. Syphilis has been called “The Great Pretender”, as its symptoms can look like many other diseases. They’re often mild and difficult to recognize, so you may pass on the infection without knowing you have it.
Some people with syphilis have no symptoms.
The symptoms also tend to change over time and may come and go.
Symptoms can include:
- small, painless sores or ulcers that typically appear on the penis, vagina, or around the anus, but can occur in other places such as the mouth
- a blotchy red rash that often affects the palms of the hands or soles of the feet
- small skin growths (similar to genital warts) that may develop on the vulva in women or around the anus in both men and women
- white patches in the mouth
- tiredness, headaches, joint pains, a high temperature (fever), and swollen glands in your neck, groin or armpits
However, syphilis typically follows a progression of stages that can last for weeks, months, or even years.
Once infected there is an incubation period of anywhere from 10 to 90 days (on average 21 days) before any signs become apparent.
Initially, the first stage of syphilis or primary syphilis, a dusky red flat spot appears at the site of inoculation and is easily missed. Then, a painless ulcer (chancre) appears 18–21 days after initial infection. Genital sites in women affected are the cervix, vagina, vulva, and clitoris. Cervical and vaginal syphilis infections may not be recognized. In men, the chancre is easily seen on the penis. Other locations of infection are limited only by human ingenuity and imagination. Common sites are around the mouth (perioral) and between the buttocks (perianal) areas.
Chancres vary in size from a few millimeters to several centimeters. A chancre is usually painless, solitary, and shallow, with a sharp border and raised, hard edge. About 70–80% of patients have rubbery, non-tender, swollen lymph nodes, often on only one side of the groin, during the first week of infection.
If untreated, the chancre will remain present for 1 to 6 weeks. If treated, it heals without scarring in 1–2 weeks.
If you don’t treat syphilis early, it spreads from the sore into your blood. When syphilis gets into your blood, it can move into the secondary stage (secondary syphilis) and cause many problems. The most common sign is a rash. The rash is usually reddish-brown and can occur anywhere on the body (even on the palms of the hands and the soles of the feet). The rash appears 2 to 10 weeks after the appearance of the sores. Other signs of secondary syphilis include fever, swollen lymph nodes, sore throat, body aches, sores in the mouth, and fatigue.
After recovering from the secondary stage of syphilis, the disease can move into the latent stage (latent syphilis). Latent syphilis produces no symptoms, but the infection is still present in your body. Latent syphilis is infectious within the first 12 to 24 months. Generally the person with latent stage syphilis has no symptoms and it is only picked up on blood tests. If syphilis is not treated at this stage, it can remain latent or develop into tertiary syphilis.
After many years (5 to 20 years), people who have syphilis and don’t get treatment may develop the fourth stage of syphilis, called tertiary syphilis. At the tertiary syphilis stage, the bacteria can damage almost any part of your body including your heart, brain, spinal cord, eyes and bones, resulting in heart disease, mental illness, blindness, deafness and neurological problems and can be life-threatening.
Some people who have syphilis don’t have any signs of infection. In other people, the signs may be very mild. They might not even know they have it. But even if they have no signs or the signs go away on their own, the infection is still alive and can cause serious health problems many years later.
Primary stage symptoms
The first symptoms of syphilis usually develop around two or three weeks after infection, although they can start up to 90 days.
This stage of the infection is known as “primary syphilis”.
- the main symptom is a small, painless sore or ulcer called a chancre that you might not notice
- the sore will typically be on the penis, vagina, or around the anus, although they can sometimes appear in the mouth or on the lips, fingers or buttocks
- most people only have one sore, but some people have several
- you may also have swollen glands in your neck, groin or armpits
These symptoms usually pass within two to eight weeks. But if the infection isn’t treated, it may progress to a second stage.
Secondary stage symptoms
Symptoms of secondary syphilis include:
- a blotchy red rash that can appear anywhere on the body, but often develops on the palms of the hands or soles of the feet
- small skin growths (similar to genital warts) – on women these often appear on the vulva and for both men and women they may appear around the anus
- white patches in the mouth
- flu-like symptoms, such as tiredness, headaches, joint pains and a high temperature (fever)
- swollen glands
- occasionally, patchy hair loss
Skin rashes and/or mucous membrane lesions (sores in the mouth, vagina, or anus) mark the second stage of symptoms. This stage typically starts with the development of a rash on one or more areas of the body. Rashes associated with secondary syphilis can appear when the primary chancre is healing or several weeks after the chancre has healed. The rash usually does not cause itching. The characteristic rash of secondary syphilis may appear as rough, red, or reddish brown spots both on the palms of the hands and the bottoms of the feet. However, rashes with a different appearance may occur on other parts of the body, sometimes resembling rashes caused by other diseases. Sometimes rashes associated with secondary syphilis are so faint that they are not noticed. Large, raised, gray or white lesions, known as condyloma lata, may develop in warm, moist areas such as the mouth, underarm or groin region. In addition to rashes, symptoms of secondary syphilis may include fever, swollen lymph glands, sore throat, patchy hair loss, headaches, weight loss, muscle aches, and fatigue. The symptoms of secondary syphilis will go away with or without treatment within a few weeks, although they may come and go over several months before they disappear. However, without treatment, the infection will progress to the latent and possibly tertiary stage of disease.
Latent stage symptoms
You’ll still be infected even if you don’t have symptoms. This is known as “latent syphilis” and it can last for decades and lead to serious problems if not treated.
The latent (hidden) stage of syphilis is a period of time when there are no visible signs or symptoms of syphilis. Without treatment, the infected person will continue to have syphilis in their body even though there are no signs or symptoms. Early latent syphilis is latent syphilis where infection occurred within the past 12 months. Late latent syphilis is latent syphilis where infection occurred more than 12 months ago. Latent syphilis can last for years.
It’s still possible to pass on the infection during this stage, although this usually only happens within two years of becoming infected.
Tertiary syphilis
Without treatment, a syphilis infection can last for years or decades without causing any symptoms. Tertiary syphilis is rare and develops in a subset of untreated syphilis infections;, it can appear 10–30 years after infection was first acquired, and it can be fatal. Tertiary syphilis can affect multiple organ systems, including the brain, nerves, eyes, heart, blood vessels, liver, bones, and joints. Symptoms of tertiary syphilis vary depending on the organ system affected.
People with tertiary syphilis may experience:
- meningitis
- strokes
- dementia symptoms
- loss of co-ordination
- numbness
- vision problems or blindness
- heart problems
Syphilis is still treatable at this stage, but it’s sometimes not possible to reverse any damage that’s already been done.
Neurosyphilis
Syphilis can invade the nervous system at any stage of infection, and causes a wide range of symptoms, including headache, altered behavior, difficulty coordinating muscle movements, paralysis, sensory deficits, and dementia 185, 186. This invasion of the nervous system is called “neurosyphilis”.
- Early neurosyphilis: Cerebrospinal fluid (CSF) abnormalities can occur in 50 to 60% of persons with early syphilis and are of unknown significance in the absence of neurologic signs or symptoms 187, 188. The most common manifestation of early neurosyphilis is meningeal syphilis, which usually occurs weeks to months (and almost always within a year) after initial infection 185. Symptomatic syphilitic meningitis often resembles aseptic meningitis, and symptoms may include fever, headache, and stiff neck; with basilar involvement, cranial nerve abnormalities can develop, particularly cranial nerves 2, 6, and 8 185. Meningovascular syphilis typically develops 5 to 12 years after initial infection, but it can occur earlier. Meningovascular syphilis, which results from Treponema pallidum infection and inflammation of small and medium central nervous system blood vessels, most often manifests as a stroke-like syndrome with seizures 189.
- Late neurosyphilis: Late forms of neurosyphilis usually occur multiple years or even decades (typically at least 15 years) after infection 185, 190. In the modern era, this type of neurosyphilis is rarely seen. Clinical manifestations include general paresis and tabes dorsalis but can present with a wide variety of neurologic symptoms, including dementia 185, 186.
Ocular syphilis
Like neurosyphilis, ocular syphilis can occur at any stage of infection 190. Ocular syphilis can involve almost any part of the eye, but the most common clinical presentation is uveitis—anterior, posterior, or panuveitis 191, 192. Symptoms associated with ocular syphilis may occur with or without neurosyphilis include vision changes, decreased visual acuity, and permanent blindness 193, 191, 192. Other described ocular syphilis signs and symptoms include lid involvement, episcleritis, vitritis, papillitis, interstitial keratitis, retinitis, and optic neuritis 192. The clinical presentation of ocular syphilis can have significant overlap with other infectious and noninfectious eye diseases. People with syphilis who have ocular complaints should have a complete cranial nerve evaluation and receive a referral to an ophthalmologist for an immediate evaluation 194. In addition, if any cranial nerve abnormalities are present, a lumbar puncture should be performed with cerebrospinal fluid analysis to determine if concomitant neurosyphilis is present 194.
Clinicians should be aware of ocular syphilis and screen for visual complaints in any patient at risk for syphilis (e.g., men who have sex with men, persons living with HIV, others with risk factors and persons with multiple or anonymous partners).
Otosyphilis
Otic involvement from T. pallidum infection can occur at any stage of syphilis, and persons with otosyphilis usually present with hearing loss, tinnitus, or vertigo, or a combination of these manifestations 195, 196. The hearing loss with otosyphilis is typically sensorineural and can involve one or both ears 195, 196. Otosyphilis can develop with other syphilis manifestations, including neurosyphilis or ocular syphilis. Thus, individuals with suspected or diagnosed otosyphilis should undergo an initial screening evaluation for neurosyphilis and ocular syphilis 196. Poeple with a suspected diagnosis of otosyphilis should receive a referral for an immediate evaluation by an otolaryngologist 194. Individuals with a positive serologic test for syphilis who have isolated auditory symptoms and a normal neurologic examination do not require lumbar puncture with cerebrospinal fluid examination 194.
Congenital syphilis
Congenital syphilis occurs when Treponema pallidum is transmitted from a pregnant woman with syphilis to her fetus 197, 198. Less often, perinatal transmission of Treponema pallidum can occur at the time of the delivery if the newborn has contact with maternal genital lesions 197, 198. Transmission to the fetus in pregnancy can occur during any stage of syphilis, but the risk is much higher with primary or secondary syphilis, especially if the mother acquires Treponema pallidum in the third trimester of pregnancy 199. Fetal infection can occur during any trimester of pregnancy. For pregnant women only penicillin therapy can be used to treat syphilis and prevent passing the disease to her baby; treatment with penicillin is extremely effective (success rate of 98%) in preventing mother-to-child transmission 184. Pregnant women who are allergic to penicillin should be referred to a specialist for desensitization to penicillin.
All pregnant women should be tested for syphilis at the first prenatal visit. For women who are at high risk for syphilis, live in areas of high syphilis morbidity, are previously untested, or had a positive screening test in the first trimester, the syphilis screening test should be repeated during the third trimester (28 to 32 weeks gestation) and again at delivery 183. Any woman who delivers a stillborn infant after 20 week’s gestation should also be tested for syphilis.
Depending on how long a pregnant woman has been infected, she may have a high risk of having a stillbirth or of giving birth to a baby who dies shortly after birth. Untreated syphilis in pregnant women results in infant death in up to 40 percent of cases.
An infected baby born alive may not have any signs or symptoms of disease 199, 200, 201. However, if not treated immediately, the baby may develop serious problems within a few weeks. Untreated babies may become developmentally delayed, have seizures, or die. All babies born to mothers who test positive for syphilis during pregnancy should be screened for syphilis and examined thoroughly for evidence of congenital syphilis 183.
Congenital syphilis is traditionally classified as either early or late disease 202. Early manifestations occur within the first two years of life, and late manifestations occur after two years of age. Although infants with congenital syphilis most often display some early manifestations, some do not have clinical manifestations of active disease at the time of birth or early in life. Accordingly, regardless of symptoms, all neonates with a reactive serologic test for syphilis or who are at risk for congenital should undergo a thorough examination for signs or symptoms of congenital syphilis, as well as testing for HIV 194.
- Early congenital syphilis: Early congenital syphilis is usually defined as manifestations of syphilis in infants and children younger than 2 years of age, with more common abnormalities that include the following 197, 203:
- Rhinitis and nasal discharge
- Hepatosplenomegaly
- Jaundice
- Bone involvement (osteochondritis, diaphyseal osteomyelitis, and periostitis)
- Skin rash (begins as a maculopapular rash and may progress to form bullous or desquamating lesions)
- Ophthalmic disorders (cataracts, glaucoma, interstitial keratitis, optic neuritis, chorioretinitis, and pigmentary chorioretinopathy)
- Generalized lymphadenopathy
- Hematologic abnormalities (anemia and thrombocytopenia)
- Neurologic (pseudoparalysis of an extremity)
- Late congenital syphilis: Late congenital syphilis is generally defined as manifestations of syphilis in children older than 2 years of age, which typically result from scarring and chronic inflammatory changes from persistent infection and inflammation, and may manifest with one or more of the following disorders 197, 203, 204:
- Facial changes (frontal bossing due to periostitis, saddle deformity of the nose due to destruction of cartilage)
- Perforation of the hard palate
- Abnormal tooth development such as Hutchinson’s teeth and mulberry molars
- Bone abnormalities (shortened maxilla, tibial thickening [saber shins])
- Ophthalmic disorders (interstitial keratitis, glaucoma, optic atrophy)
- Deafness
Syphilis diagnosis
Syphilis can be diagnosed by testing samples of:
- Blood. Blood tests can confirm the presence of antibodies that the body produces to fight infection. The antibodies to the syphilis-causing bacteria remain in your body for years, so the test can be used to determine a current or past infection.
- Cerebrospinal fluid (CSF). If it’s suspected that you have nervous system complications of syphilis, your doctor may also suggest collecting a sample of cerebrospinal fluid through a lumbar puncture.
The definitive method for diagnosing syphilis is visualizing the Treponema pallidum bacterium via darkfield microscopy. This technique is rarely performed today. Diagnoses are thus more commonly made using blood tests. There are two types of blood tests available for syphilis: 1) nontreponemal blood tests and 2) treponemal blood tests. Both types of tests are needed to confirm a diagnosis of syphilis.
A presumptive diagnosis of syphilis requires use of two tests: a nontreponemal test (i.e., Venereal Disease Research Laboratory [VDRL] or Rapid Plasma Reagin [RPR]) and a treponemal test (i.e., fluorescent treponemal antibody absorbed [FTA-ABS] tests, the Treponema pallidum passive particle agglutination [TP-PA] assay, various enzyme immunoassays [EIAs], chemiluminescence immunoassays, immunoblots, or rapid treponemal assays). Although many treponemal-based tests are commercially available, only a few are approved for use in the United States. Use of only one type of serologic test is insufficient for diagnosis and can result in false-negative results in persons tested during primary syphilis and false-positive results in persons without syphilis. False-positive nontreponemal test results can be associated with various medical conditions and factors unrelated to syphilis, including other infections (e.g., HIV), autoimmune conditions, immunizations, pregnancy, injection-drug use, and older age 205. Therefore, persons with a reactive nontreponemal test should always receive a treponemal test to confirm the diagnosis of syphilis.
Nontreponemal test antibody titers might correlate with disease activity and are used to follow treatment response. Results should be reported quantitatively. A fourfold change in titer, equivalent to a change of two dilutions (e.g., from 1:16 to 1:4 or from 1:8 to 1:32), is considered necessary to demonstrate a clinically significant difference between two nontreponemal test results obtained using the same serologic test. Sequential serologic tests in individual patients should be performed using the same testing method (VDRL or RPR), preferably by the same laboratory. The VDRL and RPR are equally valid assays, but quantitative results from the two tests cannot be compared directly because RPR titers frequently are slightly higher than VDRL titers. Nontreponemal test titers usually decline after treatment and might become nonreactive with time; however, in some persons, nontreponemal antibodies can persist for a long period of time, a response referred to as the “serofast reaction.” Most patients who have reactive treponemal tests will have reactive tests for the remainder of their lives, regardless of treatment or disease activity. However, 15%–25% of patients treated during the primary stage revert to being serologically nonreactive after 2–3 years 206. Treponemal antibody titers do not predict treatment response and therefore should not be used for this purpose.
Some clinical laboratories are screening samples using treponemal tests, typically by EIA or chemiluminescence immunoassays 207. This reverse screening algorithm for syphilis testing can identify persons previously treated for syphilis, those with untreated or incompletely treated syphilis, and persons with false-positive results that can occur with a low likelihood of infection. Persons with a positive treponemal screening test should have a standard nontreponemal test with titer performed reflexively by the laboratory to guide patient management decisions. If the nontreponemal test is negative, the laboratory should perform a different treponemal test (preferably one based on different antigens than the original test) to confirm the results of the initial test. If a second treponemal test is positive, persons with a history of previous treatment will require no further management unless sexual history suggests likelihood of re-exposure. In this instance, a repeat nontreponemal test in 2–4 weeks is recommended to evaluate for early infection. Those without a history of treatment for syphilis should be offered treatment. Unless history or results of a physical examination suggest a recent infection, previously untreated persons should be treated for late latent syphilis. If the second treponemal test is negative and the epidemiologic risk and clinical probability for syphilis are low, further evaluation or treatment is not indicated. Two studies demonstrate that high quantitative index values from treponemal EIA/CIA tests correlate with TPPA positivity; however, the range of optical density values varies among different treponemal immunoassays, and the clinical significance of these findings warrant further investigation 208.
For most persons with HIV infection, serologic tests are accurate and reliable for diagnosing syphilis and following a patient’s response to treatment. However, atypical nontreponemal serologic test results (i.e., unusually high, unusually low, or fluctuating titers) might occur regardless of HIV-infection status. When serologic tests do not correspond with clinical findings suggestive of early syphilis, presumptive treatment is recommended for persons with risk factors for syphilis, and use of other tests (e.g., biopsy and PCR) should be considered.
Further testing is warranted for persons with clinical signs of neurosyphilis (e.g., cranial nerve dysfunction, auditory or ophthalmic abnormalities, meningitis, stroke, acute or chronic altered mental status, and loss of vibration sense). Laboratory testing is helpful in supporting the diagnosis of neurosyphilis; however, no single test can be used to diagnose neurosyphilis in all instances. The diagnosis of neurosyphilis depends on a combination of cerebrospinal fluid (CSF) tests (CSF cell count or protein and a reactive CSF-VDRL) in the presence of reactive serologic test results and neurologic signs and symptoms. CSF laboratory abnormalities are common in persons with early syphilis and are of unknown significance in the absence of neurologic signs or symptoms 209. CSF-VDRL is highly specific but insensitive. In a person with neurologic signs or symptoms, a reactive CSF-VDRL (in the absence of blood contamination) is considered diagnostic of neurosyphilis. When CSF-VDRL is negative despite the presence of clinical signs of neurosyphilis, reactive serologic test results, and abnormal CSF cell count and/or protein, neurosyphilis should be considered. In this instance, additional evaluation using FTA-ABS testing on CSF may be warranted. The CSF FTA-ABS test is less specific for neurosyphilis than the CSF-VDRL but is highly sensitive. Neurosyphilis is highly unlikely with a negative CSF FTA-ABS test, especially among persons with nonspecific neurologic signs and symptoms 210.
Among persons with HIV infection, CSF leukocyte count usually is elevated (>5 white blood cell count [WBC]/mm³). Using a higher cutoff (>20 WBC/ mm³) might improve the specificity of neurosyphilis diagnosis 211.
Figure 17. Standard syphilis screening algorithm
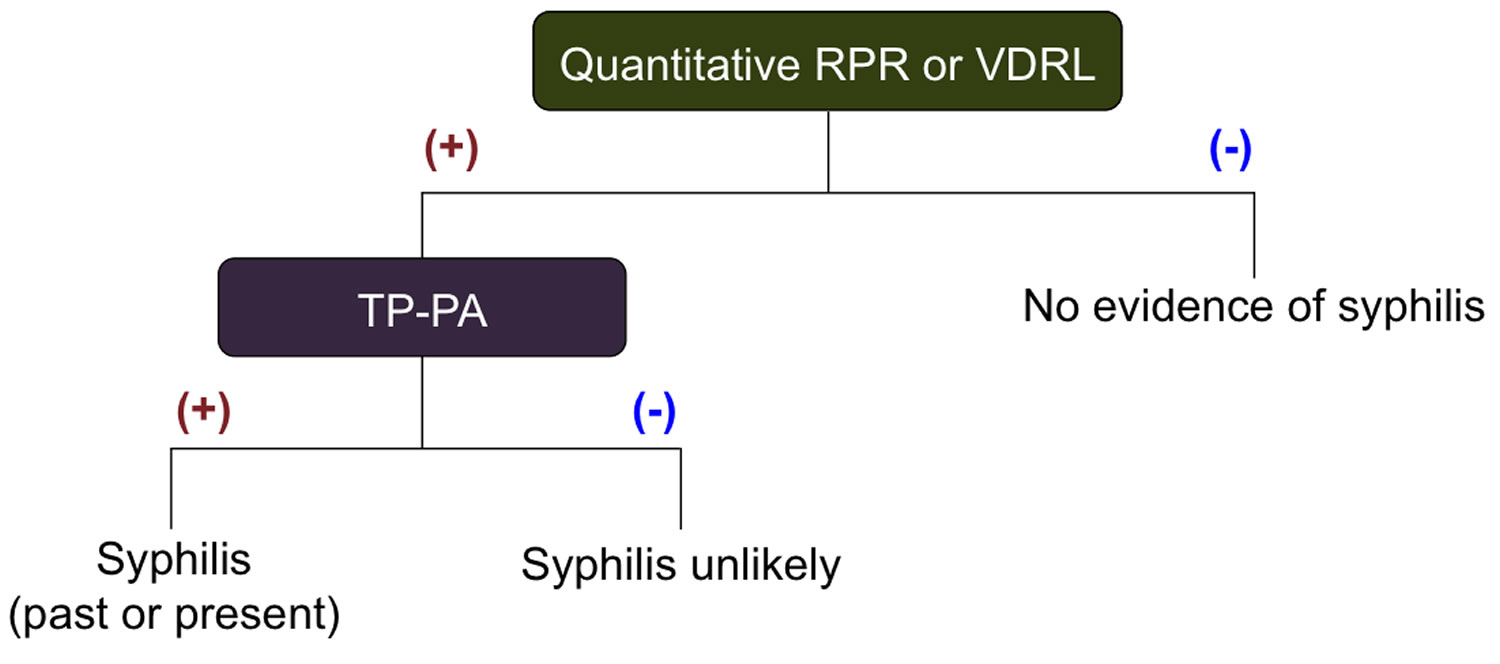
Abbreviation: TP-PA =Treponema pallidum-Particle agglutination
[Source 212 ]Figure 18. Reverse Sequence Syphilis Screening Algorithm
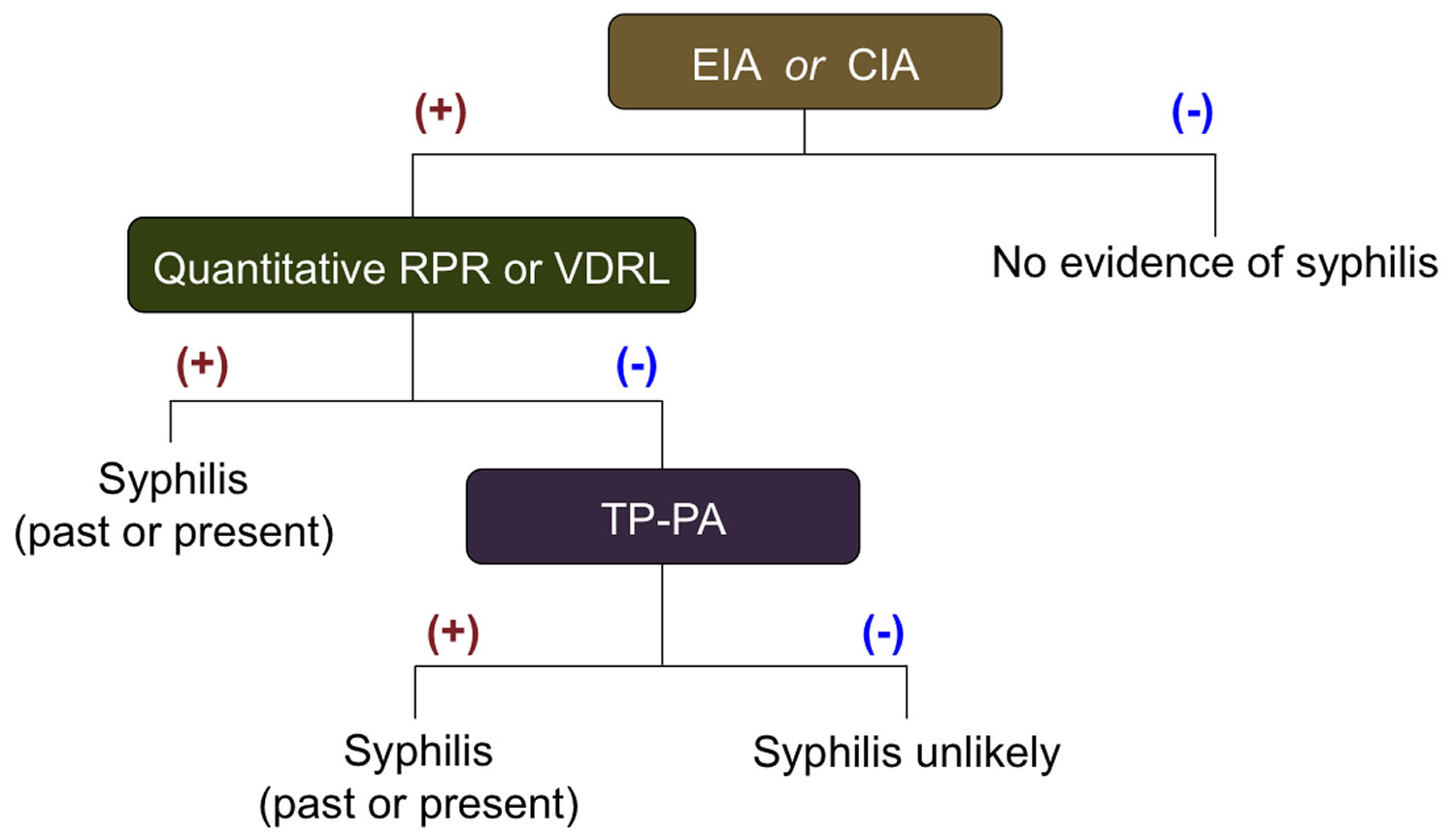
Abbreviations:
- Treponema pallidum-specific enzyme immunoassay (EIA) or chemiluminescence immunoassay (CIA)
- VDRL = Venereal Disease Research Laboratory
- RPR = Rapid Plasma Reagin
- FTA-ABS = Fluorescent Treponemal Antibody Absorbed
- TP-PA =Treponema pallidum-Particle agglutination
- ELISA= Enzyme Linked Immunoassay
Nontreponemal tests
Nontreponemal tests [e.g., Venereal Disease Research Laboratory (VDRL) and Rapid Plasma Reagin (RPR)] are simple, inexpensive, and are often used for screening. However, they are not specific for syphilis, can produce false-positive results, and, by themselves, are insufficient for diagnosis. Venereal Disease Research Laboratory (VDRL) and Rapid Plasma Reagin (RPR) tests should each have their antibody titer results reported quantitatively. Persons with a reactive nontreponemal test should always receive a treponemal test to confirm a syphilis diagnosis. This sequence of testing (nontreponemal, then treponemal test) is considered the “classical” testing algorithm.
Treponemal tests
Treponemal tests (e.g., FTA-ABS, TP-PA, various EIAs, chemiluminescence immunoassays, immunoblots, and rapid treponemal assays) detect antibodies that are specific for syphilis. Treponemal antibodies appear earlier than nontreponemal antibodies and usually remain detectable for life, even after successful treatment. If a treponemal test is used for screening and the results are positive, a nontreponemal test with titer should be performed to confirm diagnosis and guide patient management decisions. Based on the results, further treponemal testing may be indicated. This sequence of testing (treponemal, then nontreponemal test) is considered the “reverse” sequence testing algorithm. Reverse sequence testing can be more convenient for laboratories, but its clinical interpretation is problematic, as this testing sequence can identify persons previously treated for syphilis, those with untreated or incompletely treated syphilis, and persons with false-positive results that can occur with a low likelihood of infection 214.
Special note: Because untreated syphilis in a pregnant woman can infect and possibly kill her developing baby, every pregnant woman should have a blood test for syphilis. All women should be screened at their first prenatal visit. For patients who belong to communities and populations with high prevalence of syphilis and for patients at high risk, blood tests should also be performed during the third trimester (at 28–32 weeks) and at delivery.
All infants born to mothers who have reactive nontreponemal and treponemal test results should be evaluated for congenital syphilis. A quantitative nontreponemal test should be performed on infant serum and, if reactive, the infant should be examined thoroughly for evidence of congenital syphilis. Suspicious lesions, body fluids, or tissues (e.g., umbilical cord, placenta) should be examined by darkfield microscopy, PCR testing, and/or special stains. Other recommended evaluations may include analysis of cerebrospinal fluid by Venereal Disease Research Laboratory (VDRL), cell count and protein, complete blood count with differential and platelet count, and long-bone radiographs.
Latent Syphilis
Latent syphilis is defined as syphilis characterized by seroreactivity without other evidence of primary, secondary, or tertiary disease. Persons who have latent syphilis and who acquired syphilis during the preceding year are classified as having early latent syphilis, a subset of latent syphilis. Persons can receive a diagnosis of early latent syphilis if, during the year preceding the diagnosis, they had 1) a documented seroconversion or a sustained (>2 week) fourfold or greater increase in nontreponemal test titers; 2) unequivocal symptoms of primary or secondary syphilis; or 3) a sex partner documented to have primary, secondary, or early latent syphilis. In addition, for persons with reactive nontreponemal and treponemal tests whose only possible exposure occurred during the previous 12 months, early latent syphilis can be assumed. In the absence of these conditions, an asymptomatic person should be considered to have latent syphilis. Nontreponemal serologic titers usually are higher early in the course of syphilis infection. However, early latent syphilis cannot be reliably diagnosed solely on the basis of nontreponemal titers. All persons with latent syphilis should have careful examination of all accessible mucosal surfaces (i.e., the oral cavity, perianal area, perineum and vagina in women, and underneath the foreskin in uncircumcised men) to evaluate for mucosal lesions.
Congenital syphilis
The diagnosis of congenital syphilis can be difficult, as maternal nontreponemal and treponemal IgG (immunoglobulin G) antibodies can be transferred through the placenta to the fetus, complicating the interpretation of reactive serologic tests for syphilis in neonates. Therefore, treatment decisions frequently must be made on the basis of 1) identification of syphilis in the mother; 2) adequacy of maternal treatment; 3) presence of clinical, laboratory, or radiographic evidence of syphilis in the neonate; and 4) comparison of maternal (at delivery) and neonatal nontreponemal serologic titers using the same test, preferably conducted by the same laboratory. Any neonate at risk for congenital syphilis should receive a full evaluation and testing for HIV infection.
All neonates born to mothers who have reactive nontreponemal and treponemal test results should be evaluated with a quantitative nontreponemal serologic test [Rapid Plasma Reagin (RPR) or Venereal Disease Research Laboratory (VDRL)] performed on the neonate’s serum, because umbilical cord blood can become contaminated with maternal blood and yield a false-positive result, and Wharton’s jelly within the umbilical cord can yield a false-negative result. Conducting a treponemal test (i.e., TP-PA, FTA-ABS, EIA, or CIA) on neonatal serum is not recommended because it is difficult to interpret. No commercially available immunoglobulin M (IgM) test can be recommended.
All neonates born to women who have reactive serologic tests for syphilis should be examined thoroughly for evidence of congenital syphilis (e.g., nonimmune hydrops, jaundice, hepatosplenomegaly, rhinitis, skin rash, and pseudoparalysis of an extremity). Pathologic examination of the placenta or umbilical cord using specific staining (e.g., silver) or a T. pallidum PCR test using a CLIA-validated test should be considered; DFA-TP reagents are not available. Darkfield microscopic examination or PCR testing of suspicious lesions or body fluids (e.g., bullous rash and nasal discharge) also should be performed. In addition to these tests, for stillborn infants, skeletal survey demonstrating typical osseous lesions might aid in the diagnosis of congenital syphilis.
The following scenarios describe the congenital syphilis evaluation and treatment of neonates born to women who have reactive serologic tests for syphilis during pregnancy. Maternal history of infection with T. pallidum and treatment for syphilis must be considered when evaluating and treating the neonate for congenital syphilis in most scenarios, except when congenital syphilis is proven or highly probable (See Scenario 1).
Scenario 1: Proven or highly probable congenital syphilis
Any neonate with:
- an abnormal physical examination that is consistent with congenital syphilis;
OR - a serum quantitative nontreponemal serologic titer that is fourfold higher than the mother’s titer;*
OR - a positive darkfield test or PCR of lesions or body fluid(s).
* The absence of a fourfold or greater titer for a neonate does not exclude congenital syphilis.
Recommended Evaluation
- CSF analysis for VDRL, cell count, and protein **
- Complete blood count (CBC) and differential and platelet count
- Other tests as clinically indicated (e.g., long-bone radiographs, chest radiograph, liver-function tests, neuroimaging, ophthalmologic examination, and auditory brain stem response).
**CSF test results obtained during the neonatal period can be difficult to interpret; normal values differ by gestational age and are higher in preterm infants. Values as high as 25 white blood cells (WBCs) /mm3 and/or protein of 150 mg/dL might occur among normal neonates; lower values (i.e., 5 WBCs/mm³ and protein of 40 mg/dL) might be considered the upper limits of normal. Other causes of elevated values should be considered when an infant is being evaluated for congenital syphilis.
Scenario 2: Possible Congenital Syphilis
Any neonate who has a normal physical examination and a serum quantitative nontreponemal serologic titer equal to or less than fourfold the maternal titer and one of the following:
- mother was not treated, inadequately treated, or has no documentation of having received treatment;
OR - mother was treated with erythromycin or a regimen other than those recommended in these guidelines (i.e., a nonpenicillin G regimen);††
OR - mother received recommended treatment <4 weeks before delivery.
†† A women treated with a regimen other than recommended in these guidelines should be considered untreated.
Recommended Evaluation
- CSF analysis for Venereal Disease Research Laboratory (VDRL), cell count, and protein**
- CBC, differential, and platelet count
- Long-bone radiographs
A complete evaluation is not necessary if 10 days of parenteral therapy is administered, although such evaluations might be useful. For instance, a lumbar puncture might document CSF abnormalities that would prompt close follow-up. Other tests (e.g., CBC, platelet count, and bone radiographs) can be performed to further support a diagnosis of congenital syphilis.
**CSF test results obtained during the neonatal period can be difficult to interpret; normal values differ by gestational age and are higher in preterm infants. Values as high as 25 white blood cells (WBCs) /mm3 and/or protein of 150 mg/dL might occur among normal neonates; lower values (i.e., 5 WBCs/mm³ and protein of 40 mg/dL) might be considered the upper limits of normal. Other causes of elevated values should be considered when an infant is being evaluated for congenital syphilis.
Scenario 3: Congenital Syphilis less likely
Any neonate who has a normal physical examination and a serum quantitative nontreponemal serologic titer equal to or less than fourfold the maternal titer and both of the following are true:
- mother was treated during pregnancy, treatment was appropriate for the stage of infection, and treatment was administered >4 weeks before delivery and
mother has no evidence of reinfection or relapse.
Recommended Evaluation
No evaluation is recommended.
Persons with HIV Infection
Interpretation of treponemal and nontreponemal serologic tests for persons with HIV infection is the same as for the HIV-uninfected patient. Although rare, unusual serologic responses have been observed among persons with HIV infection who have syphilis; although most reports have involved post-treatment serologic titers that were higher than expected (high serofast) or fluctuated, false-negative serologic test results and delayed appearance of seroreactivity have also been reported 215.
When clinical findings are suggestive of syphilis but serologic tests are nonreactive or their interpretation is unclear, alternative tests (e.g., biopsy of a lesion, darkfield examination, and PCR of lesion material) might be useful for diagnosis. Neurosyphilis should be considered in the differential diagnosis of neurologic signs and symptoms in persons with HIV infection.
Syphilis treatment
Penicillin G, administered parenterally, is the preferred drug for treating persons in all stages of syphilis 216. The preparation used (i.e., benzathine, aqueous procaine, or aqueous crystalline), dosage, and length of treatment depend on the stage and clinical manifestations of the disease. Treatment for late latent syphilis and tertiary syphilis require a longer duration of therapy, because organisms theoretically might be dividing more slowly (the validity of this rationale has not been assessed). Longer treatment duration is required for persons with latent syphilis of unknown duration to ensure that those who did not acquire syphilis within the preceding year are adequately treated.
Selection of the appropriate penicillin preparation is important, because Treponema pallidum can reside in sequestered sites (e.g., the CNS and aqueous humor) that are poorly accessed by some forms of penicillin. Combinations of benzathine penicillin, procaine penicillin, and oral penicillin preparations are not considered appropriate for the treatment of syphilis. Reports have indicated that practitioners have inadvertently prescribed combination benzathine-procaine penicillin (Bicillin C-R) instead of the standard benzathine penicillin product (Bicillin L-A) widely used in the United States. Practitioners, pharmacists, and purchasing agents should be aware of the similar names of these two products to avoid using the inappropriate combination therapy agent for treating syphilis 217.
The effectiveness of penicillin for the treatment of syphilis was well established through clinical experience even before the value of randomized controlled clinical trials was recognized. Therefore, nearly all recommendations for the treatment of syphilis are based not only on clinical trials and observational studies, but many decades of clinical experience.
The Jarisch-Herxheimer reaction is an acute febrile reaction frequently accompanied by headache, myalgia, fever, and other symptoms that can occur within the first 24 hours after the initiation of any therapy for syphilis. Patients should be informed about this possible adverse reaction and how to manage it if it occurs. The Jarisch-Herxheimer reaction occurs most frequently among persons who have early syphilis, presumably because bacterial burdens are higher during these stages. Antipyretics can be used to manage symptoms, but they have not been proven to prevent this reaction. The Jarisch-Herxheimer reaction might induce early labor or cause fetal distress in pregnant women, but this should not prevent or delay therapy.
Primary and Secondary Syphilis Treatment
Parenteral penicillin G has been used effectively to achieve clinical resolution (i.e., the healing of lesions and prevention of sexual transmission) and to prevent late sequelae. However, no comparative trials have been conducted to guide the selection of an optimal penicillin regimen. Substantially fewer data are available for nonpenicillin regimens.
Recommended Regimen for Adults*
- Benzathine penicillin G 2.4 million units IM in a single dose
*Recommendations for treating syphilis in persons with HIV infection and pregnant women are discussed below.
Available data demonstrate that use of additional doses of benzathine penicillin G, amoxicillin, or other antibiotics do not enhance efficacy when used to treat primary and secondary syphilis, regardless of HIV status 1.
Recommended Regimen for Infants and Children
- Benzathine penicillin G 50,000 units/kg IM, up to the adult dose of 2.4 million units in a single dose
Infants and children aged >1 month who receive a diagnosis of syphilis should have birth and maternal medical records reviewed to assess whether they have congenital or acquired syphilis (see Congenital Syphilis). Infants and children aged ≥1 month with primary and secondary syphilis should be managed by a pediatric infectious-disease specialist and evaluated for sexual abuse (e.g., through consultation with child-protection services).
Other Management Considerations
All persons who have primary and secondary syphilis should be tested for HIV infection. In geographic areas in which the prevalence of HIV is high, persons who have primary or secondary syphilis should be retested for acute HIV in 3 months if the first HIV test result was negative.
Persons who have syphilis and symptoms or signs suggesting neurologic disease (e.g., cranial nerve dysfunction, meningitis, stroke, and hearing loss) or ophthalmic disease (e.g., uveitis, iritis, neuroretinitis, and optic neuritis) should have an evaluation that includes CSF analysis, ocular slit-lamp ophthalmologic examination, and otologic examination. Treatment should be guided by the results of this evaluation.
Invasion of CSF by Treponema pallidum accompanied by CSF laboratory abnormalities is common among adults who have primary or secondary syphilis 209. In the absence of clinical neurologic findings, no evidence supports variation from the recommended treatment regimen for primary and secondary syphilis. Symptomatic neurosyphilis develops in only a limited number of persons after treatment with the penicillin regimens recommended for primary and secondary syphilis. Therefore, unless clinical signs or symptoms of neurologic or ophthalmic involvement are present, routine CSF analysis is not recommended for persons who have primary or secondary syphilis.
Jarisch-Herxheimer Reaction
The Jarisch-Herxheimer reaction is a self-limited reaction associated with initiation of anti-treponemal therapy that most often occurs in persons treated for early syphilis, presumably because bacterial burdens are higher during these stages. The Jarisch-Herxheimer reaction is characterized by fever, malaise, nausea, vomiting, and less frequently, chills and exacerbation of a secondary syphilis rash 218. This reaction almost always occurs within 24 hours after initiating antimicrobial therapy and usually resolves within 24 hours. For patients who develop a Jarisch-Herxheimer reaction, the clinician should clarify this reaction is not an allergic reaction to penicillin. It occurs more frequently after treatment with penicillin and treatment of early syphilis, especially at the secondary stage. Antipyretics can be used to manage symptoms associated with the Jarisch-Herxheimer reaction, but they do not prevent this reaction.
Follow-Up
Clinical and serologic evaluation should be performed at 6 and 12 months after treatment; more frequent evaluation might be prudent if follow-up is uncertain or if repeat infection is a concern. Serologic response (i.e., titer) should be compared with the titer at the time of treatment. However, assessing serologic response to treatment can be difficult, and definitive criteria for cure or failure have not been well established. In addition, nontreponemal test titers might decline more slowly for persons previously treated for syphilis 219.
Persons who have signs or symptoms that persist or recur and those with at least a fourfold increase in nontreponemal test titer persisting for >2 weeks likely experienced treatment failure or were re-infected. These persons should be retreated and reevaluated for HIV infection. Because treatment failure usually cannot be reliably distinguished from reinfection with Treponema pallidum, a CSF analysis also should be performed; treatment should be guided by CSF findings.
Failure of nontreponemal test titers to decline fourfold within 6–12 months after therapy for primary or secondary syphilis might be indicative of treatment failure. However, clinical trial data have demonstrated that 15%–20% of persons with primary and secondary syphilis treated with the recommended therapy will not achieve the fourfold decline in nontreponemal titer used to define response at 1 year after treatment 219. Serologic response to treatment appears to be associated with several factors, including the person’s stage of syphilis (earlier stages are more likely to decline fourfold and become negative) and initial nontreponemal antibody titers (lower titers are less likely to decline fourfold than higher titers) 219. Optimal management of persons who have less than a fourfold decline in titers after treatment of syphilis is unclear. At a minimum, these persons should receive additional clinical and serologic follow-up and be evaluated for HIV infection. If additional follow-up cannot be ensured, retreatment is recommended. Because treatment failure might be the result of unrecognized CNS infection, CSF examination can be considered in such situations.
For retreatment, weekly injections of benzathine penicillin G 2.4 million units IM for 3 weeks is recommended, unless CSF examination indicates that neurosyphilis is present (see Neurosyphilis). Serologic titers might not decline despite a negative CSF examination and a repeated course of therapy 220. In these circumstances, although the need for additional therapy or repeated CSF examinations is unclear, it is not generally recommended.
Latent Syphilis Treatment
Because latent syphilis is not transmitted sexually, the objective of treating persons in this stage of disease is to prevent complications and transmission from a pregnant woman to her fetus. Although clinical experience supports the effectiveness of penicillin in achieving this goal, limited evidence is available to guide choice of specific regimens or duration.
Recommended Regimens for Adults*
Early Latent Syphilis
- Benzathine penicillin G 2.4 million units IM in a single dose
Available data demonstrate that additional doses of benzathine penicillin G, amoxicillin, or other antibiotics in early latent syphilis do not enhance efficacy, regardless of HIV infection 221
Late Latent Syphilis or Latent Syphilis of Unknown Duration
- Benzathine penicillin G 7.2 million units total, administered as 3 doses of 2.4 million units IM each at 1-week intervals
Recommended Regimens for Infants and Children
Early Latent Syphilis
- Benzathine penicillin G 50,000 units/kg IM, up to the adult dose of 2.4 million units in a single dose
Late Latent Syphilis
- Benzathine penicillin G 50,000 units/kg IM, up to the adult dose of 2.4 million units, administered as 3 doses at 1-week intervals (total 150,000 units/kg up to the adult total dose of 7.2 million units)
Infants and children aged ≥1 month diagnosed with latent syphilis should be managed by a pediatric infectious-disease specialist and receive a CSF examination. In addition, birth and maternal medical records should be reviewed to assess whether these infants and children have congenital or acquired syphilis. For those with congenital syphilis, treatment should be undertaken as described in the congenital syphilis section in this document. Those with acquired latent syphilis should be evaluated for sexual abuse (e.g., through consultation with child protection services). These regimens are for penicillin nonallergic children who have acquired syphilis and who have normal CSF examination results.
Latent Syphilis among Persons with HIV Infection
Recommended Regimen for Early Latent Syphilis
- Benzathine penicillin G, 2.4 million units IM in a single dose
Recommended Regimen for Late Latent Syphilis
- Benzathine penicillin G, at weekly doses of 2.4 million units for 3 weeks
Other Management Considerations
If a person misses a dose of penicillin in a course of weekly therapy for latent syphilis, the appropriate course of action is unclear. Clinical experience suggests that an interval of 10–14 days between doses of benzathine penicillin for latent syphilis might be acceptable before restarting the sequence of injections (i.e., if dose 1 is given on day 0, dose 2 is administered between days 10 and 14). Pharmacologic considerations suggest that an interval of 7–9 days between doses, if feasible, might be more optimal 222. Missed doses are not acceptable for pregnant women receiving therapy for latent syphilis 223. Pregnant women who miss any dose of therapy must repeat the full course of therapy.
Follow-Up
Quantitative nontreponemal serologic tests should be repeated at 6, 12, and 24 months. A CSF examination should be performed if 1) a sustained (>2 weeks) fourfold increase or greater in titer is observed, 2) an initially high titer (≥1:32) fails to decline at least fourfold within 12–24 months of therapy, or 3) signs or symptoms attributable to syphilis develop. In such circumstances, patients with CSF abnormalities should be treated for neurosyphilis. If the CSF examination is negative, retreatment for latent syphilis should be administered. Serologic titers might fail to decline despite a negative CSF examination and a repeated course of therapy, especially if the initial nontreponemal titer is low (<1:8); in these circumstances, the need for additional therapy or repeated CSF examinations is unclear but is generally not recommended. Serologic and clinical monitoring should be offered along with a reevaluation for HIV infection.
Management of Sex Partners
Sexual transmission of Treponema pallidum is thought to occur only when mucocutaneous syphilitic lesions are present. Such manifestations are uncommon after the first year of infection. Persons exposed sexually to a person who has primary, secondary, or early latent syphilis should be evaluated clinically and serologically and treated according to the following recommendations:
- Persons who have had sexual contact with a person who receives a diagnosis of primary, secondary, or early latent syphilis within 90 days preceding the diagnosis should be treated presumptively for early syphilis, even if serologic test results are negative.
- Persons who have had sexual contact with a person who receives a diagnosis of primary, secondary, or early latent syphilis >90 days before the diagnosis should be treated presumptively for early syphilis if serologic test results are not immediately available and the opportunity for follow-up is uncertain. If serologic tests are negative, no treatment is needed. If serologic tests are positive, treatment should be based on clinical and serologic evaluation and stage of syphilis.
- In some areas or populations with high rates of syphilis, health departments recommend notification and presumptive treatment of sex partners of persons with late latent syphilis who have high nontreponemal serologic test titers (i.e., >1:32), because high titers might be indicative of early syphilis. These partners should be managed as if the index case had early syphilis.
- Long-term sex partners of persons who have late latent syphilis should be evaluated clinically and serologically for syphilis and treated on the basis of the evaluation’s findings.
- The following sex partners of persons with syphilis are considered at risk for infection and should be confidentially notified of the exposure and need for evaluation: partners who have had sexual contact within 1) 3 months plus the duration of symptoms for persons who receive a diagnosis of primary syphilis, 2) 6 months plus duration of symptoms for those with secondary syphilis, and 3) 1 year for persons with early latent syphilis.
Expedited Partner Therapy
There is insufficient data to support the use of expedited partner therapy in management of syphilis contacts. Accordingly, use of expedited partner therapy is not recommended for sexual contacts of persons diagnosed with syphilis. Transmission of Treponema pallidum is highly unlikely in persons when more than 1 year has elapsed since the time of infection.
Primary and Secondary Syphilis among Persons with HIV Infection
Recommended Regimen
- Benzathine penicillin G, 2.4 million units IM in a single dose
Available data demonstrate that additional doses of benzathine penicillin G, amoxicillin, or other antibiotics in primary and secondary syphilis do not result in enhanced efficacy 221.
Persons with HIV infection who have early syphilis might be at increased risk for neurologic complications 224 and might have higher rates of serologic treatment failure with recommended regimens. The magnitude of these risks is not defined precisely, but is likely small. Although long-term (>1 year) comparative data are lacking, no treatment regimens for syphilis have been demonstrated to be more effective in preventing neurosyphilis in persons with HIV infection than the syphilis regimens recommended for persons without HIV infection 225. Careful follow-up after therapy is essential. The use of antiretroviral therapy as per current guidelines might improve clinical outcomes in persons with HIV infection and syphilis 226.
Syphilis During Pregnancy
Penicillin G is the only known effective antimicrobial for preventing maternal transmission to the fetus and treating fetal infection 227. Evidence is insufficient to determine optimal, recommended penicillin regimens 228.
Recommended Regimen
- Pregnant women should be treated with the penicillin regimen appropriate for their stage of infection.
Other Management Considerations
- Some evidence suggests that additional therapy is beneficial for pregnant women. For women who have primary, secondary, or early latent syphilis, a second dose of benzathine penicillin 2.4 million units IM can be administered 1 week after the initial dose 229.
- When syphilis is diagnosed during the second half of pregnancy, management should include a sonographic fetal evaluation for congenital syphilis. However, this evaluation should not delay therapy. Sonographic signs of fetal or placental syphilis (i.e., hepatomegaly, ascites, hydrops, fetal anemia, or a thickened placenta) indicate a greater risk for fetal treatment failure 230; cases accompanied by these signs should be managed in consultation with obstetric specialists. Evidence is insufficient to recommend specific regimens for these situations.
- Women treated for syphilis during the second half of pregnancy are at risk for premature labor and/or fetal distress if the treatment precipitates the Jarisch-Herxheimer reaction 231. These women should be advised to seek obstetric attention after treatment if they notice any fever, contractions, or decrease in fetal movements. Stillbirth is a rare complication of treatment, but concern for this complication should not delay necessary treatment. No data are available to suggest that corticosteroid treatment alters the risk for treatment-related complications in pregnancy.
- Missed doses are not acceptable for pregnant women receiving therapy for late latent syphilis 223. Pregnant women who miss any dose of therapy must repeat the full course of therapy.
- All women who have syphilis should be offered testing for HIV infection.
Follow-Up
Coordinated prenatal care and treatment are vital. At a minimum, serologic titers should be repeated at 28–32 weeks’ gestation and at delivery. Serologic titers can be checked monthly in women at high risk for reinfection or in geographic areas in which the prevalence of syphilis is high. Providers should ensure that the clinical and antibody responses are appropriate for the patient’s stage of disease, although most women will deliver before their serologic response to treatment can be assessed definitively. Inadequate maternal treatment is likely if delivery occurs within 30 days of therapy, clinical signs of infection are present at delivery, or the maternal antibody titer at delivery is fourfold higher than the pretreatment titer.
Congenital syphilis treatment
Proven or highly probable congenital syphilis Recommended Regimens
- Aqueous crystalline penicillin G 100,000–150,000 units/kg/day, administered as 50,000 units/kg/dose IV every 12 hours during the first 7 days of life and every 8 hours thereafter for a total of 10 days
OR
- Procaine penicillin G 50,000 units/kg/dose IM in a single daily dose for 10 days
If more than 1 day of therapy is missed, the entire course should be restarted. Data are insufficient regarding the use of other antimicrobial agents (e.g., ampicillin). When possible, a full 10-day course of penicillin is preferred, even if ampicillin was initially provided for possible sepsis. The use of agents other than penicillin requires close serologic follow-up to assess adequacy of therapy.
Possible Congenital Syphilis Recommended Regimens
- Aqueous crystalline penicillin G 100,000–150,000 units/kg/day, administered as 50,000 units/kg/dose IV every 12 hours during the first 7 days of life and every 8 hours thereafter for a total of 10 days
OR
- Procaine penicillin G 50,000 units/kg/dose IM in a single daily dose for 10 days
OR
- Benzathine penicillin G 50,000 units/kg/dose IM in a single dose
Before using the single-dose benzathine penicillin G regimen, the complete evaluation (i.e., CSF examination, long-bone radiographs, and CBC with platelets) must be normal, and follow-up must be certain. If any part of the infant’s evaluation is abnormal or not performed, if the CSF analysis is uninterpretable because of contamination with blood, or if follow-up is uncertain, a 10-day course of penicillin G is required. If the neonate’s nontreponemal test is nonreactive and the provider determines that the mother’s risk of untreated syphilis is low, treatment of the neonate with a single IM dose of benzathine penicillin G 50,000 units/kg for possible incubating syphilis can be considered without an evaluation.
Neonates born to mothers with untreated early syphilis at the time of delivery are at increased risk for congenital syphilis, and the 10-day course of penicillin G may be considered even if the complete evaluation is normal and follow-up is certain.
Congenital Syphilis Less Likely – Recommended Regimen
- Benzathine penicillin G 50,000 units/kg/dose IM in a single dose*
*Another approach involves not treating the infant, but rather providing close serologic follow-up every 2-3 months for 6 months for infants whose mother’s nontreponemal titers decreased at least fourfold after appropriate therapy for early syphilis or remained stable for low-titer, latent syphilis (e.g., VDRL <1:2; RPR <1:4).
Congenital Syphilis Unlikely Recommended Regimen
- No treatment is required, but infants with reactive nontreponemal tests should be followed serologically to ensure the nontreponemal test returns to negative (see Follow-Up). Benzathine penicillin G 50,000 units/kg as a single IM injection might be considered, particularly if follow-up is uncertain and the neonate has a reactive nontreponemal test.
Follow-Up
All neonates with reactive nontreponemal tests should receive careful follow-up examinations and serologic testing (i.e., a nontreponemal test) every 2–3 months until the test becomes nonreactive. In the neonate who was not treated because congenital syphilis was considered less likely or unlikely, nontreponemal antibody titers should decline by age 3 months and be nonreactive by age 6 months, indicating that the reactive test result was caused by passive transfer of maternal IgG antibody. At 6 months, if the nontreponemal test is nonreactive, no further evaluation or treatment is needed; if the nontreponemal test is still reactive, the infant is likely to be infected and should be treated. Treated neonates that exhibit persistent nontreponemal test titers by 6–12 months should be re-evaluated through CSF examination and managed in consultation with an expert. Retreatment with a 10-day course of a penicillin G regimen may be indicated. Neonates with a negative nontreponemal test at birth and whose mothers were seroreactive at delivery should be retested at 3 months to rule out serologically negative incubating congenital syphilis at the time of birth. Treponemal tests should not be used to evaluate treatment response because the results are qualitative and passive transfer of maternal IgG treponemal antibody might persist for at least 15 months.
Neonates whose initial CSF evaluations are abnormal should undergo a repeat lumbar puncture approximately every 6 months until the results are normal. A reactive CSF Venereal Disease Research Laboratory (VDRL) test or abnormal CSF indices that persist and cannot be attributed to other ongoing illness requires retreatment for possible neurosyphilis and should be managed in consultation with an expert.
Tertiary Syphilis
Tertiary syphilis refers to gummas and cardiovascular syphilis but not to neurosyphilis. Persons who are not allergic to penicillin and have no evidence of neurosyphilis should be treated with the following regimen.
Recommended Regimen
Tertiary Syphilis with Normal CSF Examination
- Benzathine penicillin G 7.2 million units total, administered as 3 doses of 2.4 million units IM each at 1-week intervals
Other Management Considerations
All persons who have tertiary syphilis should be tested for HIV infection and should receive a CSF examination before therapy is initiated. Persons with CSF abnormalities should be treated with a neurosyphilis regimen. Some providers treat all persons who have cardiovascular syphilis with a neurosyphilis regimen. These persons should be managed in consultation with an infectious-disease specialist. Limited information is available concerning clinical response and follow-up of persons who have tertiary syphilis.
Neurosyphilis Treatment
CNS involvement can occur during any stage of syphilis, and CSF laboratory abnormalities are common in persons with early syphilis, even in the absence of clinical neurologic findings. No evidence exists to support variation from recommended treatment for syphilis at any stage for persons without clinical neurologic findings, with the exception of tertiary syphilis. If clinical evidence of neurologic involvement is observed (e.g., cognitive dysfunction, motor or sensory deficits, ophthalmic or auditory symptoms, cranial nerve palsies, and symptoms or signs of meningitis or stroke), a CSF examination should be performed.
Syphilitic uveitis or other ocular manifestations (e.g., neuroretinitis and optic neuritis) can be associated with neurosyphilis. A CSF examination should be performed in all instances of ocular syphilis, even in the absence of clinical neurologic findings. Ocular syphilis should be managed in collaboration with an ophthalmologist and according to the treatment and other recommendations for neurosyphilis, even if a CSF examination is normal. In instances of ocular syphilis and abnormal CSF test results, follow-up CSF examinations should be performed to assess treatment response.
Recommended Regimen
Neurosyphilis and Ocular Syphilis
- Aqueous crystalline penicillin G 18–24 million units per day, administered as 3–4 million units IV every 4 hours or continuous infusion, for 10–14 days
If compliance with therapy can be ensured, the following alternative regimen might be considered.
Alternative Regimen
- Procaine penicillin G 2.4 million units IM once daily, PLUS Probenecid 500 mg orally four times a day, both for 10–14 days
The durations of the recommended and alternative regimens for neurosyphilis are shorter than the duration of the regimen used for latent syphilis. Therefore, benzathine penicillin, 2.4 million units IM once per week for up to 3 weeks, can be considered after completion of these neurosyphilis treatment regimens to provide a comparable total duration of therapy.
Penicillin Allergy
Limited data suggest that ceftriaxone 2 g daily either IM or IV for 10–14 days can be used as an alternative treatment for persons with neurosyphilis 232. Cross-sensitivity between ceftriaxone and penicillin can occur, but the risk for penicillin cross-reactivity between third-generation cephalosporins is negligible 233 (see Management of Persons Who Have a History of Penicillin Allergy). If concern exists regarding the safety of ceftriaxone for a patient with neurosyphilis, skin testing should be performed (if available) to confirm penicillin allergy and, if necessary, penicillin desensitization in consultation with a specialist is recommended. Other regimens have not been adequately evaluated for treatment of neurosyphilis.
Other Management Considerations
The following are other considerations in the management of persons who have neurosyphilis:
- All persons who have neurosyphilis should be tested for HIV.
- Although systemic steroids are used frequently as adjunctive therapy for otologic syphilis, such drugs have not been proven to be beneficial.
Follow-Up
If CSF pleocytosis was present initially, a CSF examination should be repeated every 6 months until the cell count is normal. Follow-up CSF examinations also can be used to evaluate changes in the CSF-Venereal Disease Research Laboratory (VDRL) or CSF protein after therapy; however, changes in these two parameters occur more slowly than cell counts, and persistent abnormalities might be less important 226. Leukocyte count is a sensitive measure of the effectiveness of therapy. If the cell count has not decreased after 6 months, or if the CSF cell count or protein is not normal after 2 years, retreatment should be considered. Limited data suggest that in immunocompetent persons and persons with HIV infection on highly active antiretroviral therapy, normalization of the serum RPR titer predicts normalization of CSF parameters following neurosyphilis treatment 226.
Penicillin Allergy
Infants and children who require treatment for congenital syphilis but who have a history of penicillin allergy or develop an allergic reaction presumed secondary to penicillin should be desensitized and then treated with penicillin (see Management of Persons with a History of Penicillin Allergy). Skin testing remains unavailable for infants and children because the procedure has not been standardized for this age group. Data are insufficient regarding the use of other antimicrobial agents (e.g., ceftriaxone) for congenital syphilis in infants and children. If a nonpenicillin G agent is used, close clinical, serologic, and CSF follow-up is required in consultation with an expert.
Management of Persons Who Have a History of Penicillin Allergy
No proven alternatives to penicillin are available for treating neurosyphilis, congenital syphilis, or syphilis in pregnant women. Penicillin also is recommended, whenever possible, for persons with HIV infection. The prevalence of reported penicillin allergy in the United States is about 8%–10% 234 and might be higher in hospitalized persons 235. The prevalence of reported penicillin allergy in developing countries is unknown; however, limited data suggest that penicillin is one of the most frequently reported allergies in some developing countries 236. Of persons reporting penicillin allergy, 10%–15% have a positive skin test suggestive of a penicillin allergy; these persons are at risk for an immunoglobulin E (IgE)-mediated allergic response to penicillin such as urticaria, angioedema, or anaphylaxis (i.e., upper airway obstruction, bronchospasm, or hypotension) 233. Re-administration of penicillin to patients with a history of IgE-mediated hypersensitivity reactions can cause severe, immediate reactions. Because anaphylactic reactions to penicillin can be fatal, every effort should be made to avoid administering penicillin to penicillin-allergic persons, unless they undergo induction of drug tolerance (also referred to as “desensitization”) to temporarily eliminate IgE-mediated hypersensitivity. However, many persons with a reported history of penicillin allergy likely have had other types of adverse drug reactions or have lost their sensitivity to penicillin over time and can safely be treated with penicillin.
Penicillin skin testing with the major and minor determinants of penicillin can reliably identify persons at high risk for IgE-mediated reactions to penicillin 237. Although the testing reagents are easily generated, only the major determinant (benzylpenicilloyl poly-L-lysine [Pre-Pen]) and penicillin G have been available commercially. These two tests identify an estimated 90%–99% of the allergic patients. However, because skin testing without the minor determinants would still fail to identify 1%–10% of allergic persons and because serious or fatal reactions can occur among these minor-determinant–positive persons, caution should be exercised when the full battery of skin-test reagents is not available (Table 1) 238. Manufacturers are working on a minor determinant mixture, but at the time of publication, no such product has been cleared by FDA for use in the United States. Penicillin skin testing has been used in a variety of settings to improve antibiotic use 239.
Table 1. Skin-test reagents for identifying persons at risk for adverse reactions to penicillin
Major Determinant
- Benzylpenicilloyl poly-L-lysine (PrePen) (AllerQuest, Plainville Connecticut) (6 x 10–5M)
Minor Determinant Precursors*
- Benzylpenicillin G (10–2M, 3.3 mg/mL, 10,000 units/mL)
- Benzylpenicilloate (10–2M, 3.3 mg/mL)
- Benzylpenicilloate (or penicilloyl propylamine) (10–2M, 3.3 mg/mL)
Positive Control
- Commercial histamine for scratch testing (1.0 mg/mL)
Negative Control
- Diluent (usually saline) or allergen diluent
Footnote: * Aged penicillin is not an adequate source of minor determinants. Penicillin G should either be freshly prepared or come from a fresh-frozen source.
[Source 240]Some studies have reported cross-reactivity rates as high as 10% among persons with a history of penicillin allergy who take cephalosporins. However, more recent studies indicate a lower rate (<2.5%) of cross reactivity between these drugs 233. Risk is highest with first-generation cephalosporins and cephalosporins that have similar R-group side chains to specific penicillins 241. The risk for penicillin cross-reactivity between most second-generation (cefoxitin) and all third generation cephalosporins (cefixime and ceftriaxone) is negligible 233; cefoxitin, cefixime, and ceftriaxone do not have an R group side chain similar to penicillin G.
Recommendations
Persons with a history of severe non-IgE-mediated reactions (e.g., Stevens-Johnson syndrome, toxic epidermal necrolysis, interstitial nephritis, and hemolytic anemia) are not candidates for skin testing or challenge and should avoid penicillins indefinitely. If the full battery of skin-test reagents is available, including both major and minor determinants (see Penicillin Allergy Skin Testing), persons who report a history of penicillin reaction and who are skin-test negative can receive conventional penicillin therapy. Persons with positive skin test results should be desensitized before initiating treatment.
If the full battery of skin-test reagents, including the minor determinants, is not available, skin testing should be conducted using the major determinant (Pre-Pen) and penicillin G. Those persons who have positive test results should be desensitized. For persons with negative skin tests, a subsequent observed challenge to the penicillin of choice is recommended. In addition, for persons with a history of severe or recent suspected IgE-mediated reactions to penicillin with negative skin testing, the penicillin of choice should be given by graded challenge. If the major determinant is not available for skin testing, all persons with a history suggesting IgE-mediated reactions to penicillin (e.g., anaphylaxis, angioedema, bronchospasm, or urticaria) should be desensitized in a hospital setting. In persons with reactions not likely to be IgE-mediated, outpatient-monitored graded challenges can be considered.
Penicillin Allergy Skin Testing
Persons at high risk for anaphylaxis, including those who 1) have a history of penicillin-related anaphylaxis or other IgE-mediated reactions, asthma, or other diseases that would make anaphylaxis more dangerous or 2) are being treated with beta-adrenergic blocking agents should be tested with 100-fold dilutions of the full-strength skin-test reagents before being tested with full-strength reagents. In these situations, testing should be performed in a monitored setting in which treatment for an anaphylactic reaction is available. If possible, antihistamines (e.g., chlorpheniramine maleate, fexofenadine, diphenhydramine HCL, and hydroxyzine) should not have been taken within the 5 days before skin testing.
Procedures
Dilute the antigens in saline either 100-fold for preliminary testing (if the patient has had a IgE- mediated reaction to penicillin) or 10-fold (if the patient has had another type of immediate, generalized reaction to penicillin within the preceding year). Pre-Pen is provided full-strength (6 x 10–5 meq penicilloyl) in a single dose ampoule. Penicillin G is diluted to 10,000 IU/ml in saline and aliquoted in sterile vials that remain stable for at least 6 months if frozen.
Epicutaneous (Prick) Tests
Duplicate drops of skin-test reagent are placed on the volar surface of the forearm. The underlying epidermis is pierced with a 26-gauge needle without drawing blood. An epicutaneous test is positive if the average wheal diameter after 15 minutes is ≥4 mm larger than that of negative controls; otherwise, the test is negative. The histamine controls should be positive to ensure that results are not falsely negative because of the effect of antihistaminic drugs.
Intradermal Test
If epicutaneous tests are negative, duplicate 0.02-mL intradermal injections of negative control and antigen solutions are made into the volar surface of the forearm by using a 26- or 27-gauge needle on a syringe. The margins of the wheals induced by the injections should be marked with a ball point pen. An intradermal test is positive if the average wheal diameter 15 minutes after injection is >2 mm larger than the initial wheal size and also is >2 mm larger than the histamine controls. Otherwise, the tests are negative. If the duplicates are discordant, a second set of duplicate tests can be used to resolve the ambiguity.
Desensitization
Persons who have a positive skin test to one of the penicillin determinants can be desensitized (Table 2). This is a straightforward, relatively safe procedure that can be performed orally or intravenously. Modified protocols might be considered based on an individual’s symptoms, drug of choice, and route of administration 242. Although the two approaches have not been compared, oral desensitization is regarded as safer and easier to perform. Desensitization should occur in a hospital setting because serious IgE-mediated allergic reactions can occur; the procedure can usually be completed in approximately 4–12 hours, after which time the first dose of penicillin is administered. After desensitization, penicillin should be maintained continuously for the duration of the course of therapy. Once the course is completed, if penicillin is required in the future, the desensitization procedure should be repeated.
Table 2. Oral desensitization protocol for persons with a positive skin test*
| Penicillin V suspension dose† | Amount§ (units/mL) | mL | Units | Cumulative dose (units) |
|---|---|---|---|---|
| 1 | 1,000 | 0.1 | 100 | 100 |
| 2 | 1,000 | 0.2 | 200 | 300 |
| 3 | 1,000 | 0.4 | 400 | 700 |
| 4 | 1,000 | 0.8 | 800 | 1,500 |
| 5 | 1,000 | 1.6 | 1,600 | 3,100 |
| 6 | 1,000 | 3.2 | 3,200 | 6,300 |
| 7 | 1,000 | 6.4 | 6,400 | 12,700 |
| 8 | 10,000 | 1.2 | 12,000 | 24,700 |
| 9 | 10,000 | 2.4 | 24,000 | 48,700 |
| 10 | 10,000 | 4.8 | 48,000 | 96,700 |
| 11 | 80,000 | 1.0 | 80,000 | 176,700 |
| 12 | 80,000 | 2.0 | 160,000 | 336,700 |
| 13 | 80,000 | 4.0 | 320,000 | 656,700 |
| 14 | 80,000 | 8.0 | 640,000 | 1,296,700 |
Footnotes:
* Observation period was 30 minutes before parenteral administration of penicillin.
† Interval between doses, 15–30 minutes; elapsed time, 4–8 hours; cumulative dose, 1.3 million units.
§ The specific amount of drug was diluted in approximately 30 mL of water and then administered orally.
[Source 243]Trichomoniasis
Trichomoniasis is a very common sexually transmitted disease (STD) caused by a tiny protozoan parasite called Trichomonas vaginalis. Trichomoniasis is usually spreads during sex, but can also be spread by sharing wet towels or washers. Trichomoniasis mostly affects women, but men can get it too. Most people who have trichomoniasis do not have any symptoms.
Trichomoniasis is the most common curable STD (sexually transmitted disease). In the United States, an estimated 3.7 million people have the infection 244. However, only about 30% develop any symptoms of trichomoniasis. Trichomoniasis is more common in women than in men. Older women are more likely than younger women to have been infected with trichomoniasis.
Although symptoms of trichomoniasis vary, most people who have the Trichomonas vaginalis parasite cannot tell they are infected. Your doctor or sexual health clinic can test for and treat trichomoniasis.
Clinical manifestations in symptomatic pubertal or postpubertal females may include a diffuse foul-smelling (smelly fishy odor) vaginal discharge and vulvovaginal itch and irritation. Pain with urination or sexual intercourse and, less often, lower abdominal pain can occur. Vaginal discharge may be any color, but classically is yellow-green, frothy, and malodorous. The vulva and vaginal mucosa can be reddish and swollen. The cervix can be inflamed and sometimes is covered with numerous punctate cervical hemorrhages and swollen papillae, referred to as “strawberry” cervix. This finding occurs in less than 5% of infected females but is highly suggestive of trichomoniasis. Clinical manifestations in symptomatic men include urethritis (urethra inflammation) and, rarely, epididymitis or prostatitis. Reinfection is common, and resistance to treatment is rare but increasing. Rectal infections are uncommon, and oral infections have not been described.
The prevalence of Trichomonas vaginalis infection in the United States is estimated to be 2.3 million (3.1%) among women ages 14-49, based on a nationally representative sample of women who participated in National Health and Examination Survey (NHANES) 2001–2004. The following are other findings from this study 245:
- An estimated 3.7 million women and men are infected with Trichomonas vaginalis in the United States 246
- Most women found to have trichomoniasis (85%) reported no symptoms.
- Women with no history of sexual intercourse can still be affected by trichomoniasis (1.0%), as can pregnant women (3.2%), and women who have ever been pregnant (4.1%).
- African American women had a prevalence of 13.3%, white women prevalence of 1.3%, and Mexican American women prevalence of 1.8%.
- Prevalence of trichomoniasis increases with age and lifetime number of sexual partners among African American women.
It is not possible to diagnose trichomoniasis based on your symptoms alone. For both men and women, your doctor or sexual health care provider can examine you and get a laboratory test to diagnose trichomoniasis.
Trichomoniasis can be cured with a single dose of prescription antibiotic medication (either metronidazole or tinidazole or or secnidazole), pills which can be taken by mouth. It is okay for pregnant women to take this medication. Some people who drink alcohol within 24 hours after taking this kind of antibiotic can have uncomfortable side effects.
People who have been treated for trichomoniasis can get it again. About 1 in 5 people get infected again within 3 months after treatment. To avoid getting reinfected, make sure that all of your sex partners get treated too, and wait to have sex again until all of your symptoms go away (about a week). Get checked again if your symptoms come back. You can reduce your risk of infection by using condoms correctly every time you have sex.
If your symptoms don’t go away after treatment, talk to your doctor or sexual health worker.
Without treatment, trichomoniasis can last months, or even years. Trichomoniasis can cause premature labor, low birth weight, or increase your risk of getting HIV, the virus that causes AIDS.
Trichomoniasis key facts
- Trichomoniasis can be asymptomatic in men and women, and may persist silently for years.
- Untreated trichomoniasis is associated with adverse pregnancy outcomes such as premature rupture of the membranes, preterm delivery, and low birthweight infants.
- Douching may worsen vaginal discharge in patients with trichomoniasis.
- Alcohol consumption is contraindicated with metronidazole and tinidazole.
- Transmission Issues:
- Trichomoniasis is almost always sexually transmitted.
- Sex partners should be treated.
- Patients should abstain from intercourse until they and their sex partners are cured (about 7 days).
- Trichomoniasis has been associated with increased susceptibility to HIV acquisition and transmission.
- Risk Reduction:
- Individualize risk-reduction plans with each patient.
- Prevention strategies include abstinence, mutual monogamy with an uninfected partner, use of condoms, and limiting the number of sex partners.
- Latex condoms, when used consistently and correctly, can reduce the risk of transmission of Trichomonas vaginalis.
- Douching should be avoided since it increases the risk for trichomoniasis.
- Male circumcision reduces the risk of trichomoniasis.
Figure 19. Trichomonas vaginalis
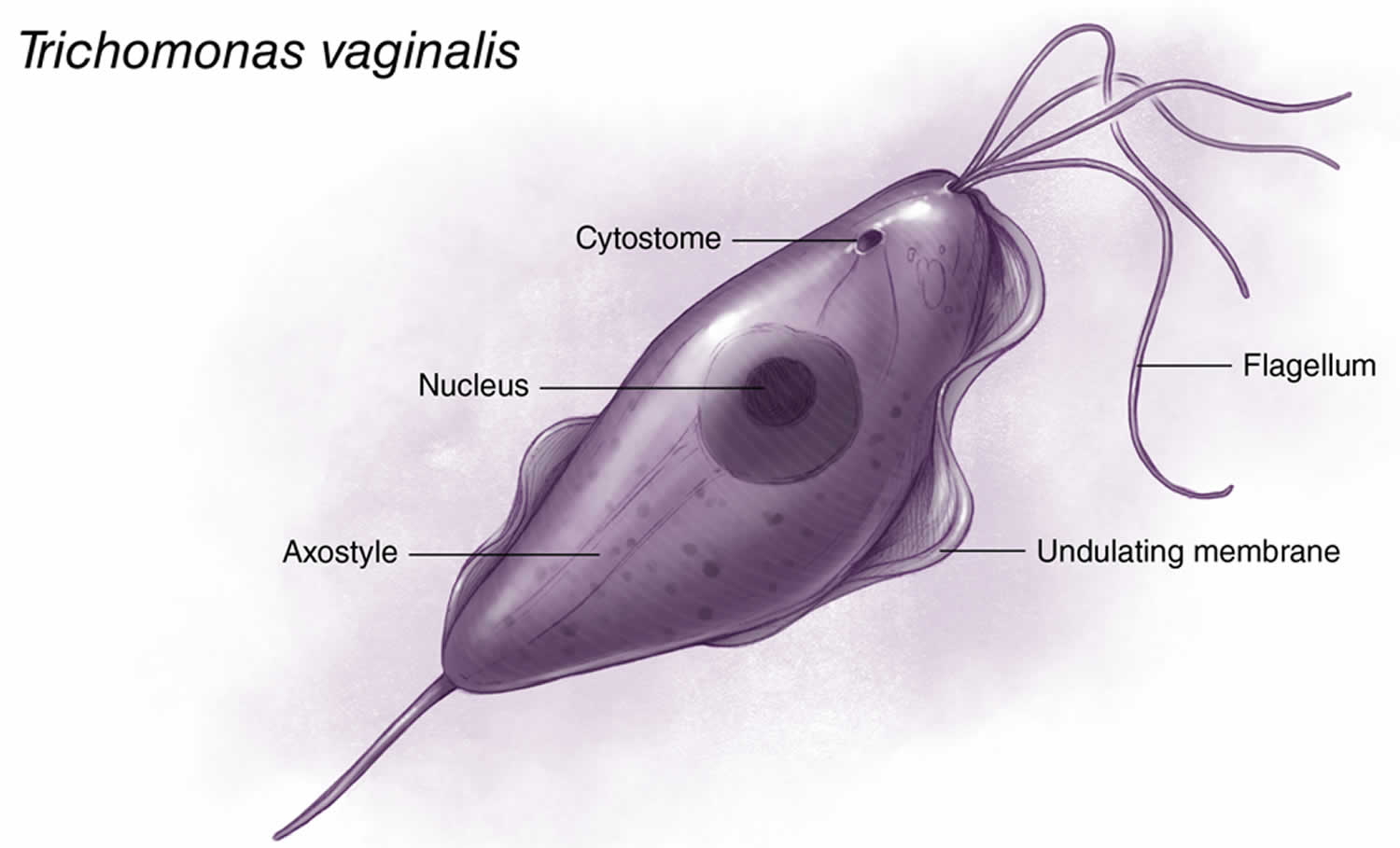
Footnote: Trichomonas vaginalis is a pear-shaped flagellated protozoan parasitic organism that is approximately 10 by 7 micrometers. The organism achieves a quivering motion via the anterior flagella and the undulating membrane. After attaching to vaginal epithelial cells, the organism takes on a more ameboid-like appearance.
[Source 247]Trichomoniasis in men
Trichomonas vaginalis may cause up to 11% to 13% of nongonococcal urethritis (NGU) in males, but urethral infection in males is frequently asymptomatic 248. Men with Trichomonas vaginalis infection may also present with prostatitis or epididymitis 249.
Trichomoniasis rarely causes symptoms in men. When men do have signs and symptoms, however, they might include:
- Irritation inside the penis
- Burning with urination or after ejaculation
- Discharge from the penis
How does trichomoniasis affect a pregnant woman and her baby?
Pregnant women with trichomoniasis are more likely to have their babies too early (preterm delivery) 250. Also, babies born to infected mothers are more likely to have a low birth weight (less than 5.5 pounds) 251.
How do you get trichomoniasis?
The Trichomonas vaginalis parasite passes from an infected person to an uninfected person during sex. In women, the most commonly infected part of the body is the lower genital tract (vulva, vagina, cervix, or urethra). In men, the most commonly infected body part is the inside of the penis (urethra). During sex, the parasite usually spreads from a penis to a vagina, or from a vagina to a penis. Trichomoniasis can also spread from a vagina to another vagina. It is not common for the Trichomonas vaginalis parasite to infect other body parts, like the hands, mouth, or anus. It is unclear why some people with the trichomoniasis infection get symptoms while others do not. It probably depends on factors like a person’s age and overall health. Infected people without symptoms can still pass the infection on to others.
Resumption of Sexual Activity
Patients should be instructed to avoid sex until they and their sex partners have been treated, and until they no longer have any symptoms of trichomoniasis. This usually takes about 7 days.
Post-Treatment Follow-Up
All sexually active women who are diagnosed and treated for Trichomonas vaginalis infection (including pregnant women and women with HIV infection) should be retested 3 months after initial treatment to evaluate the possibility of reinfection. Retesting in men is not routinely recommended.
Trichomoniasis symptoms
About 70% of infected people with trichomoniasis do not have any signs or symptoms. When trichomoniasis does cause symptoms, they can range from mild irritation to severe inflammation. Some people with symptoms get them within 5 to 28 days after being infected. Others do not develop symptoms until much later. Symptoms can come and go.
Trichomoniasis symptoms in men
Men don’t usually get symptoms from trichomoniasis, but there may be a discharge from the penis, or pain when urinating 252.
Men with trichomoniasis may notice:
- Itching or irritation inside the penis;
- Burning after urination or ejaculation;
- Discharge from the penis.
Trichomoniasis in women
Women with trichomoniasis may notice:
- Itching, burning, redness or soreness of the genitals;
- Vaginal itching or burning;
- Pain during sex;
- Discomfort with urination;
- Pain low in the tummy;
- A change in their vaginal discharge (i.e., thin discharge or increased volume) that can be clear, frothy, white, yellowish, greyish or greenish with an unusual fishy smell.
Having trichomoniasis can make it feel unpleasant to have sex, but many women are asymptomatic 253. Without treatment, the infection can last for months or even years.
Chronic Trichomonas vaginalis infection may be associated with minimal vaginal discharge, mild itch and/or pain during sex (dyspareunia) 253. The presence of cervical punctate hemorrhages (Figure 2), often referred to as a “strawberry cervix,” strongly suggests a diagnosis of trichomoniasis, but this occurs in fewer than 5% of women with trichomoniasis 253, 254.
Figure 20. Trichomoniasis and Cervical Petechiae (“strawberry cervix”)
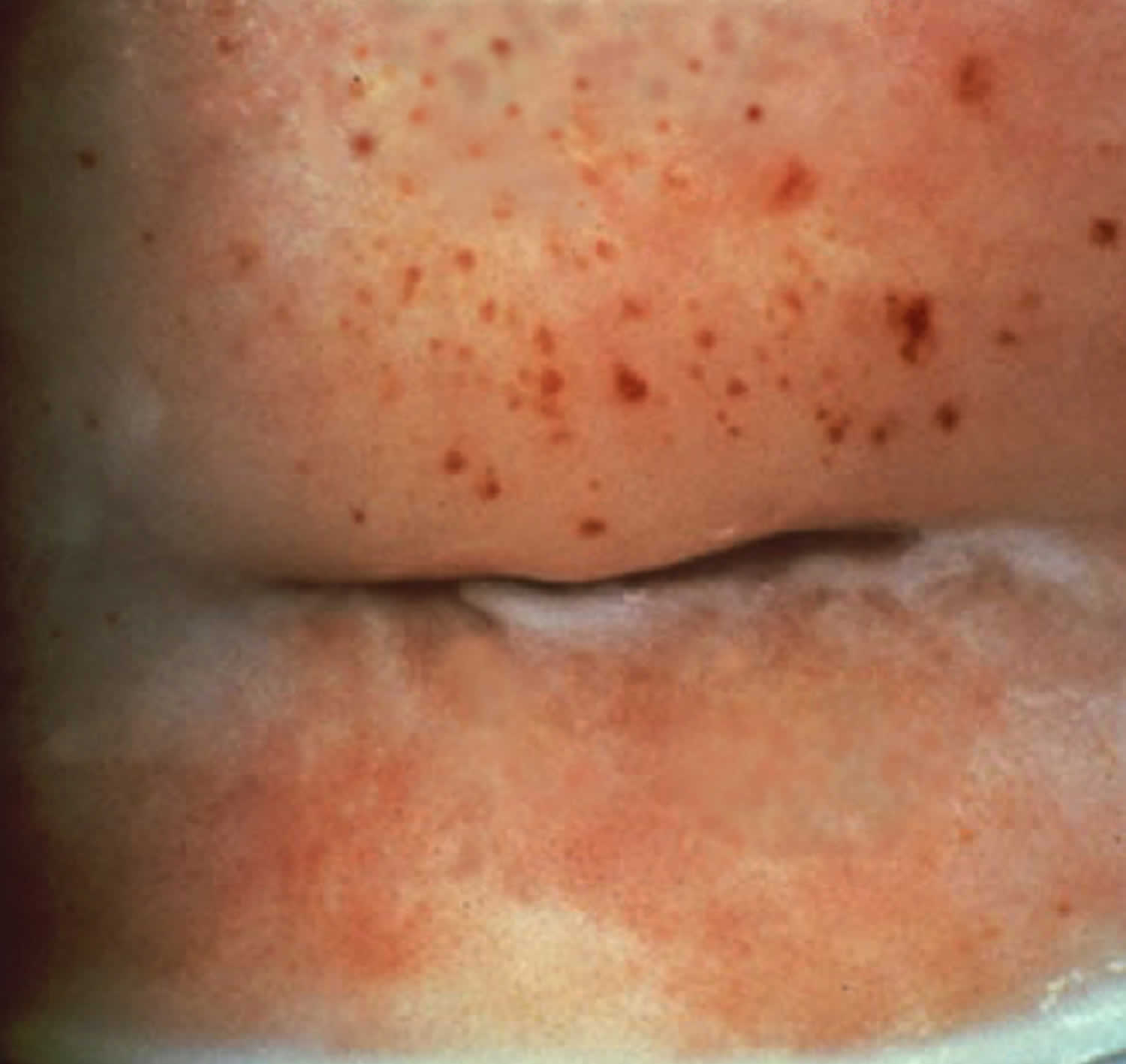
Footnote: This photograph shows multiple petechiae on the cervix of a women with trichomoniasis. This manifestation in a woman with vaginal discharge strongly suggests a diagnosis of trichomoniasis and is often referred to as a ‘strawberry cervix‘.
[Source 247 ]Trichomoniasis in pregnancy
Infection with Trichomonas vaginalis in pregnant women is associated with both obstetrical and gynecologic adverse outcomes, including low birth weight, premature rupture of membranes (PPROM) and preterm labor; trichomoniasis in pregnancy increases the risk of preterm birth by about 30% 255, 256, 257. Neonatal trichomoniasis is unusual but can occur 258, 259.
Trichomoniasis in people with HIV
Among women with HIV, more than half are coinfected with Trichomonas vaginalis, and they have been shown to have an increased risk for pelvic inflammatory disease (PID) and for shedding of HIV in the genital tract 260, 261. Antiretroviral therapy appears to lessen the potentiating effects of trichomoniasis infections on HIV transmission risk 260. Infection with HIV does not make a woman more likely to have persistent or recurrent trichomoniasis 262.
Trichomoniasis causes
Trichomoniasis is caused by Trichomonas vaginalis, which is a single-celled flagellated anaerobic protozoan parasite, a type of tiny parasite that travels between people during sexual intercourse. The incubation period between exposure and infection is unknown, but it’s thought to range from five to 28 days.
Trichomonas vaginalis is the only known protozoan parasite that infects the genital tract. Trichomonas vaginalis has four anterior flagella and one flagellum embedded in an undulating membrane (Figure 1) 263. The flagella are responsible for the jerky motility of this organism that is seen under a microscope. After attaching to vaginal epithelial cells, this globular, pear-shaped organism transforms into a thin, flat, ameboid shape 264. Trichomoniasis is almost always sexually transmitted; fomite transmission is extremely rare. T. vaginalis may persist for months to years in epithelial crypts and periglandular areas of the genital tract 263. Distinguishing persistent, subclinical infection from remote sexual acquisition is not always possible.
Risk factors for trichomoniasis
Investigators have identified multiple risk factors associated with trichomoniasis that include the following 265:
- Older age
- Multiple sex partners
- Drug use (marijuana, crack cocaine, alcohol, cigarettes)
- Sex without a condom
- Presence of sexually transmitted infections (STIs) at baseline
- Low socioeconomic status
- Douching
- Black race.
Trichomoniasis complications
Trichomoniasis can increase the risk of getting or spreading other sexually transmitted infections (STIs). For example, trichomoniasis can cause genital inflammation that makes it easier to get infected with human immunodeficiency virus (HIV), the virus that causes acquired immunodeficiency syndrome (AIDS), or to pass the HIV virus on to a sex partner 266.
Pregnant women who have trichomoniasis might:
- Deliver too early (prematurely)
- Have a baby with a low birth weight
- Give the infection to the baby as the baby passes through the birth canal
Trichomoniasis is also associated with an increased risk of cervical or prostate cancer.
Untreated, trichomoniasis infection can last for months to years.
Trichomoniasis prevention
The only way to avoid STDs (sexually transmitted diseases) is to not have vaginal, anal, or oral sex. The best way to avoid trichomoniasis is by using condoms every time you have sex. Safe sex also helps stop the spread of other sexually transmitted diseases (STDs).
To prevent re-infection with trichomoniasis, make sure any partner is treated too. It is best to avoid having sex for seven days after your or your partner’s treatment to lower the chance of you both getting the infection again.
If you are sexually active, you can do the following things to lower your chances of getting trichomoniasis:
- Be in a long-term mutually monogamous relationship with a partner who has been tested and has negative STD test results;
- Use latex condoms the right way every time you have sex. This can lower your chances of getting trichomoniasis. But the parasite can infect areas that are not covered by a condom – so condoms may not fully protect you from getting trichomoniasis.
Another approach is to talk about the potential risk of STDs before you have sex with a new partner. That way you can make informed choices about the level of risk you are comfortable taking with your sex life.
If you or someone you know has questions about trichomoniasis or any other STD, talk to a health care provider.
Trichomoniasis diagnosis
Your doctor is likely to take a sample from inside the vagina to test for trichomoniasis. Men can be checked with a urine test or a swab from the opening of the penis.
If the Trichomonas vaginalis parasite can be seen under the microscope, no further tests are needed.
If the test doesn’t show the parasite, but your doctor thinks you may have trichomoniasis, other tests may be done. Your doctor may order tests done on a sample of vaginal fluid, a penis uretheral swab or sometimes urine. Tests include a rapid antigen test and nucleic acid amplification test (NAAT).
If you have trichomoniasis, your doctor may also want to test you for other sexually transmitted infections (STIs) so they can also be treated.
Trichomoniasis test
In clinical practice, wet mount preparation has been the most commonly used method for diagnosing trichomoniasis, primarily because of the low cost, convenience, and point-of-care diagnosis 267, 268. The wet mount preparation however has a sensitivity (44 to 68%) that is significantly lower than with newer molecular nucleic acid amplification tests (NAATs) 269. Papanicolaou (PAP) testing is not considered an appropriate diagnostic tool for trichomoniasis; if Trichomonas vaginalis infection is identified on routine Papanicolaou (PAP) testing, a standard trichomonas diagnostic test should be used to verify infection 270. The following summarizes the major methods used to diagnose trichomoniasis.
Wet Mount Preparation
The traditional diagnostic method for trichomoniasis has been wet mount with microscopic visualization of motile Trichomonas vaginalis parasites on slide preparations from vaginal or urethral secretions. Ideally, specimens should be examined within 10 minutes to observe motile parasites, which are diagnostic. Wet mount is an inexpensive diagnostic test; however, sensitivity is estimated at 51-65%, and varies based on the individual performing the test and how promptly the slide is interpreted 271.
Figure 21. Trichomonas vaginalis on Wet Mount preparation
Footnote: This photomicrograph taken of a vaginal discharge wet mount sample shows numerous oval Trichomonas vaginalis protozoan parasites; the black arrow on left indicates two characteristic Trichomonas vaginalis organisms (the thin flagellum can be faintly seen).
[Source 272 ]Culture
Obtaining a culture using modified Diamond’s medium was the previous gold standard for diagnosis of trichomoniasis prior to the availability of highly sensitive NAATs. Culture has been considered the gold standard for diagnosis of trichomoniasis with a specificity approaching 100%, but it is not widely used and its sensitivity can be as low as 75–96% 271. Culture is a more sensitive diagnostic tool than wet mount alone, but results are not immediately available. Clinical specimens can be inoculated into transport systems such as Amies gel medium to maintain viability for up to 24 hours at room temperature 273. Specialized culture systems (i.e. InPouch System [Biomed Diagnostics]) are available to allow for transport of cultures when shipping to an off-site laboratory. Additionally, these systems can be used to transport specimens after inoculation. Such systems are useful when immediate transportation of specimens to the laboratory is not available. The specimen should be inoculated as soon as possible (within an hour of collection) to maintain viability of the organism.
Culture may be used for diagnosing Trichomonas vaginalis in both men and women. Culture in men may be performed on samples of urethral secretions, urine sediment, or semen, but testing in women requires sampling of vaginal secretions, as the sensitivity is low in urine culture 1. Trichomonas vaginalis culture is categorized by the Clinical Laboratory Improvement Amendments (CLIA) as moderately complex as it is time-consuming and requires incubation 269. If Trichomonas vaginalis is isolated in culture, drug susceptibility testing can be performed, particularly in cases of persistent infection.
Nucleic Acid Amplification Testing (NAAT)
Several NAAT-based methods are available for diagnosis of Trichomonas vaginalis, including transcription-mediated amplification and polymerase chain reaction (PCR). There are no data to suggest Trichomonas vaginalis causes anorectal infection, and therefore use of NAAT to detect Trichomonas vaginalis anorectal infection is not recommended 1, 274, 275.
- Aptima Trichomonas vaginalis Assay (Becton Dickinson): This assay uses transcription-mediated amplification for detection of Trichomonas vaginalis RNA 252. This test is FDA-cleared for detection of Trichomonas vaginalis in symptomatic and asymptomatic women 276. The test can be performed on clinician-collected vaginal swabs, clinician-collected endocervical swabs, female urine specimens, or liquid endocervical Pap smear specimens collected in PreservCyt Solution 277. The Aptima Trichomonas vaginalis assay has a sensitivity of 95.3 to 100% and specificity of 95.2 to 100%, which are considerably higher than wet mount or culture 278, 252, 279. The Aptima Trichomonas vaginalis assay is not FDA-cleared for use in men, but it may be used to test urine or urethral swabs from men if the assay is internally validated in accordance with CLIA regulations 276.
- Probe Tec TV Qx Amplified DNA Assay (Becton-Dickinson): This assay uses Strand Displacement Amplification technology and is FDA-cleared for detection of Trichomonas vaginalis from vaginal swabs (clinician-collected or self-collected), endocervical swabs (clinician-collected), and female urine specimens 276. This assay can be used to detect Trichomonas vaginalis in symptomatic and asymptomatic females. The Probe Tec TV Qx Amplified DNA assay has a sensitivity of 98.3% and specificity of 99.6% for detecting Trichomonas vaginalis 280.
- GeneXpert TV (Cepheid): This PCR-based NAAT is FDA-cleared for detection of Trichomonas vaginalis genomic DNA using self-collected or clinician-collected vaginal specimens, female urine specimens, clinician-collected endocervical swab specimens, and male urine specimens 276, 281. With this assay, the results are available within 63 minutes; for samples that have a clear positive result after 45 PCR cycles have been completed, the Early Assay Termination function will provide the positive result earlier, typically within 40 minutes 281. The GeneXpert TV has a sensitivity of 99.5 to 100% and a specificity of 99.4 to 99.9% 282.
- Max CTGCTV2 Assay (Becton Dickinson): This FDA-cleared PCR assay for gonorrhea and chlamydia has been modified to test concurrently for Trichomonas vaginalis 283. This test is FDA-cleared for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis from vaginal specimens (self-collected or clinician-collected), female urine specimens, and male urine specimens 276. The Max CTGCTV2 Assay has a sensitivity of 96.2 to 100% and specificity of 99.1 to 100% for detecting Trichomonas vaginalis 282.
- Cobas TV/MG (Roche Diagnostics): This PCR-based NAAT is FDA-cleared for detection of Trichomonas vaginalis and M. genitalium using vaginal specimens (self-collected or clinician-collected), clinician-collected endocervical swab specimens, female urine specimens, male urine specimens, and clinician-collected meatal specimens 284. This assay is FDA-cleared for both symptomatic and asymptomatic patients. The Cobas TV/MG has a sensitivity and specificity greater than 99.5% 284, 285.
Point-of-Care Testing
There are multiple point-of-care tests available for diagnosing trichomoniasis in women 286:
- Osom Trichomonas Rapid Test (Sekisui Diagnostics): This is an antigen-detection point-of-care test for use with clinician-collected vaginal samples. The test requires about 10 to 15 minutes for test results to become available; this test has a sensitivity of 82 to 95% and a specificity of 97 to 100% 287. The Osom Trichomonas Rapid Test is not FDA-cleared for use in men.
- Solana Trichomonas Assay (Quidel): This point-of-care test uses isothermal Helicase-Dependent Amplification technology to detect Trichomonas vaginalis DNA from asymptomatic and symptomatic female urine specimens or clinician-collected vaginal specimens, with a sensitivity greater than 92% for urine specimens and greater than 98% for vaginal samples 288. Results are available within 40 minutes. This test is not FDA-cleared for use in men.
- Sexual Health Click Test (Visby Medical): This point-of-care PCR test is a single-use, disposable test that can detect chlamydia, gonorrhea, and trichomonas using self-collected vaginal swabs 289. The compact test device provides results within 30 minutes. In an analysis of self-collected vaginal swabs obtained in 1,449 women, this test had a sensitivity of 99.2% and specificity of 96.9% for detection of Trichomonas vaginalis 289. This assay received FDA clearance and a CLIA waiver in August 2021.
Trichomoniasis treatment
Trichomoniasis can be treated with oral antibiotic (either metronidazole or tinidazole or secnidazole). These pills are taken by mouth. It is safe for pregnant women to take this medication. Don’t drink alcohol for 24 hours after taking metronidazole, 48 hours after taking secnidazole or 72 hours after taking tinidazole. Drinking alcohol during and for a few days after treatment can cause severe nausea and vomiting.
Oral antibiotic options may include:
- Megadose. Your doctor may recommend one large dose (megadose) of either metronidazole (Flagyl), tinidazole (Tindamax) or secnidazole (Solosec). You only take these oral medications one time.
- Multiple doses. Your provider might recommend several lower doses of metronidazole or tinidazole. You take the pills two times a day for seven days. To help clear up the infection completely, keep taking this medicine for the full time your provider prescribed the drug, even if you begin to feel better after a few days. If you stop using this medicine too soon, your infection may not go away completely.
Recommended oral antibiotic regimen for Women 276:
- Metronidazole 500 mg orally twice a day for 7 days
Recommended oral antibiotic regimen for Men 276:
- Metronidazole 2 g orally in a single dose
Alternative oral antibiotic regimen for Women and Men 276:
- Tinidazole2 g orally in a single dose
People who have been treated for trichomoniasis can get it again. About 1 in 5 people get infected again within 3 months after receiving treatment. To avoid getting reinfected, make sure that all of your sex partners get treated. Also, wait 7- 10 days after you and your partner have been treated to have sex again. This usually takes about a week after finishing the last antibiotic dose. Get checked again if your symptoms come back.
Your doctor will typically retest you for trichomoniasis after treatment. A retest two weeks to three months after treatment can check to be sure the infection is gone and that you haven’t been reinfected.
Even if you’ve had treatment that gets rid of trichomoniasis, it’s possible to get it again if you’re exposed to someone with the infection.
Trichomoniasis cure
Recommended oral antibiotic regimen for Women 276:
- Metronidazole 500 mg orally twice a day for 7 days
Recommended oral antibiotic regimen for Men 276:
- Metronidazole 2 g orally in a single dose
Alternative oral antibiotic regimen for Women and Men 276:
- Tinidazole2 g orally in a single dose
The nitroimidazoles are the only class of antimicrobial medications known to be effective against Trichomonas vaginalis infections. Of these drugs, metronidazole and tinidazole have been cleared by FDA for the oral or parenteral treatment of trichomoniasis 290. Tinidazole is generally more expensive, reaches higher levels in serum and the genitourinary tract, has a longer half-life than metronidazole (12.5 hours versus 7.3 hours), and has fewer gastrointestinal side effects 291. In randomized clinical trials, recommended metronidazole regimens have resulted in cure rates of approximately 84%–98% 291, and the recommended tinidazole regimen has resulted in cure rates of approximately 92%–100% 292. Randomized controlled trials comparing single 2 g doses of metronidazole and tinidazole suggest that tinidazole is equivalent or superior to metronidazole in achieving parasitologic cure and resolution of symptoms 293.
Metronidazole gel does not reach therapeutic levels in the urethra and perivaginal glands. Because it is less efficacious than oral metronidazole, it is not recommended.
Treatment of persistent or recurrent trichomoniasis
The most likely reasons for persistent or recurrent trichomoniasis are reinfection from an untreated partner or lack of adherence with treatment, but in some individuals, antimicrobial-resistant Trichomonas vaginalis infection can occur. Currently, rates of metronidazole resistance range from 4 to 10%, and the rate of tinidazole resistance is about 1% 294, 295. Tinidazole retains activity against many metronidazole-refractory strains. The following summarizes the approach to treatment in persons with persistent or recurrent trichomoniasis 276.
- Treatment Failure with Reexposure: For women and men who received standard treatment for trichomoniasis and have treatment failure due to reexposure from an untreated partner, retreatment should consist of the same regimen they initially received 276.
- Treatment Failure without Reexposure: For men who have treatment failure after receiving an initial single-dose therapy of metronidazole 2 grams orally (and reexposure has not occurred), the recommended retreatment is metronidazole 500 mg orally twice daily for 7 days 276. For women who have failed the initial regimen of metronidazole 500 mg twice daily for 7 days and have not been reexposed, repeat treatment should be given with a 7-day regimen of either metronidazole 2 grams given once per day or tinidazole 2 grams once per day 276. Tinidazole should not be used in pregnant women.
- Treatment Failure after Second-Line Treatment without Reexposure: If an individual experiences persistent infection after receiving treatment with a second-line regimen (and reexposure to a partner with trichomoniasis has not occurred), the clinician should request a special kit from the Centers for Disease Control and Prevention for 5-nitroimidazole drug-resistance testing (Trichomonas Susceptibility Testing) 276.
- Treatment of 5-Nitroimidazole-Resistant Trichomonas: If drug-resistance testing reveals nitroimidazole resistance and treatment with a 7-day regimen of either metronidazole 2 grams given once per day or tinidazole 2 grams once per day has been unsuccessful, then the next option is oral tinidazole 2 grams daily plus intravaginal tinidazole 500 mg twice daily for 14 days 276. If this option fails, then consider using high-dose oral tinidazole (1 gram 3 times daily) plus intravaginal paromomycin (4 grams of 6.25% intravaginal paromomycin cream nightly) for 14 days 276. Note that tinidazole should not be used in pregnant women. Intravaginal boric acid has been used to treat trichomoniasis in women allergic to nitroimidazole and thus could be considered as an option for women with treatment-refractory nitroimidazole-resistant trichomoniasis 276.
Other Management Considerations
You should abstain from sex until you and your sex partners are treated and until you and your partners no longer have any symptoms of trichomoniasis. This usually takes about 7 days after completion of treatment 276.
Testing for other STDs including HIV should be performed in people infected with Trichomonas vaginalis.
Follow-up
Because of the high rate of reinfection among women treated for trichomoniasis (17% within 3 months in one study) 296, retesting for T. vaginalis is recommended for all sexually active women within 3 months following initial treatment regardless of whether they believe their sex partners were treated. Testing by nucleic acid amplification can be conducted as soon as 2 weeks after treatment 297. Data are insufficient to support retesting men 276.
Management of Sex Partners
Concurrent treatment of all sex partners is critical for symptomatic relief, microbiologic cure, and prevention of transmission and reinfections. Current partners should be referred for presumptive therapy to avoid reinfection. Partners should be advised to abstain from intercourse until they and their sex partners have been adequately treated and any symptoms have resolved. EPT might have a role in partner management for trichomoniasis 298 and can be used in states where permissible by law; however, no one partner management intervention has been shown to be superior in reducing reinfection rates. Though no definitive data exist to guide treatment for partners of persons with persistent or recurrent trichomoniasis in whom nonadherance and reinfection are unlikely, partners benefit from undergoing evaluation and receiving the same regimen as the patient (see Persistent or Recurrent Trichomoniasis).
Treatment of women during pregnancy
Trichomonas vaginalis infection in pregnant women is associated with adverse pregnancy outcomes, particularly premature rupture of membranes, preterm delivery, and delivery of a low birthweight infant 299. Pregnant women with symptomatic trichomoniasis, in any trimester, should receive treatment with metronidazole 500 mg orally twice daily for 7 days 276. Treatment of asymptomatic trichomoniasis in pregnancy, however, has not been shown to reduce preterm birth 300. One trial suggested the possibility of increased preterm delivery in women with Trichomonas vaginalis infection who received metronidazole treatment 300, yet study limitations prevented definitive conclusions regarding the risks of treatment. More recent, larger studies have shown no positive or negative association between metronidazole use during pregnancy and adverse outcomes of pregnancy 301. Symptomatic pregnant women, regardless of pregnancy stage, should be tested and considered for treatment. Treatment of Trichomonas vaginalis infection can relieve symptoms of vaginal discharge in pregnant women and reduce sexual transmission to partners. Although perinatal transmission of trichomoniasis is uncommon, treatment also might prevent respiratory or genital infection of the newborn 302. Clinicians should counsel symptomatic pregnant women with trichomoniasis regarding the potential risks for and benefits of treatment and about the importance of partner treatment and condom use in the prevention of sexual transmission.
Although metronidazole crosses the placenta, data suggest that it poses a low risk to pregnant women 303. No evidence of teratogenicity or mutagenic effects in infants has been found in multiple cross-sectional and cohort studies of pregnant women 304.
Both metronidazole and tinidazole are secreted in breast milk (https://www.ncbi.nlm.nih.gov/books/NBK501922). Metronidazole is secreted in breast milk. With maternal oral therapy, breastfed infants receive metronidazole in doses that are lower than those used to treat infections in infants, although the active metabolite adds to the total infant exposure. Plasma levels of the drug and metabolite are measurable, but remain less than maternal plasma levels. Although several reported case series found no evidence of adverse effects in infants exposed to metronidazole in breast milk, some clinicians advise deferring breastfeeding for 12–24 hours after taking a dose of metronidazole 276, 305. Tinidazole is not recommended during pregnancy due to limited animal studies suggesting fetal risk; women who are breastfeeding should wait 72 hours after taking tinidazole before breastfeeding 276.
Treatment of women with HIV
Up to 53% of women with HIV infection also are infected with Trichomonas vaginalis 306. Trichomonas vaginalis infection in these women is significantly associated with pelvic inflammatory disease 307, and treatment of trichomoniasis is associated with significant decreases in genital-tract HIV viral load and viral shedding 308. For these reasons, routine screening and prompt treatment are recommended for all women with HIV infection; screening should occur at entry to care and then at least annually thereafter. A randomized clinical trial involving women with HIV infection and Trichomonas vaginalis infection demonstrated that a single dose of metronidazole 2 g orally was less effective than 500 mg twice daily for 7 days 309. Thus, to improve cure rates, women with HIV infection who receive a diagnosis of Trichomonas vaginalis infection should be treated with a 7-day treatment course of metronidazole 500 mg twice daily (rather than with a 2-g single dose of metronidazole) 276. This longer course of therapy has been shown to have higher cure rates than single-dose metronidazole therapy in women with HIV 261, 310, 311.
Factors that might interfere with standard single-dose treatment for trichomoniasis in these women include high rates of asymptomatic bacterial vaginosis co-infections, use of antiretroviral therapy, changes in vaginal ecology, and impaired immunity 312.
In women with HIV infection who receive a diagnosis of T. vaginalis infection, retesting is recommended within 3 months following initial treatment; NAAT is encouraged because of higher sensitivity of these tests. Data are insufficient to recommend routine screening, alternative treatment regimens of longer duration, or retesting in men.
Pregnant women with HIV who are treated for Trichomonas vaginalis infection should be retested 3 months after treatment.
Allergy, Intolerance, and Adverse Reactions
Metronidazole and tinidazole are both nitroimidazoles. Patients with an IgE mediated-type allergy to a nitroimidazole can be managed by metronidazole desensitization according to a published regimen 313 and in consultation with a specialist.
- Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Centers for Disease Control and Prevention. STD trends in the United States: 2010 national data for gonorrhea, chlamydia, and syphilis Snapshot sexually transmitted diseases in 2010. https://www.cdc.gov/std/stats10/tables/trends-snapshot.htm[↩]
- 2016 Sexually Transmitted Diseases Surveillance. https://www.cdc.gov/std/stats16/default.htm[↩][↩]
- Satterwhite CL et al, Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008. STD 2013 Mar;40(30):187-93[↩][↩]
- Centers for Disease Control and Prevention. STD trends in the United States: 2010 national data for gonorrhea, chlamydia, and syphilis. https://www.cdc.gov/std/stats10/tables/trends-table.htm[↩]
- Torrone E, Papp J, Weinstock H. Prevalence of Chlamydia trachomatis Genital Infection Among Persons Aged 14–39 Years — United States, 2007–2012. MMWR 2014;63:834-8.[↩]
- Pinsky L, Chiarilli DB, Klausner JD, et al. Rates of asymptomatic nonurethral gonorrhea and chlamydia in a population of university men who have sex with men. Journal of American college health : J of ACH 2012;60:481-4.[↩]
- Park J, Marcus JL, Pandori M, Snell A, Philip SS, Bernstein KT. Sentinel surveillance for pharyngeal chlamydia and gonorrhea among men who have sex with men–San Francisco, 2010. Sexually transmitted diseases 2012;39:482-4.[↩]
- Chlamydia – CDC Basic Fact Sheet. https://www.cdc.gov/std/chlamydia/stdfact-chlamydia.htm[↩][↩]
- Darville T, Hiltke TJ. Pathogenesis of genital tract disease due to Chlamydia trachomatis. J Infect Dis. 2010 Jun 15;201 Suppl 2(Suppl 2):S114-25. doi: 10.1086/652397[↩][↩]
- William M. Geisler, Duration of Untreated, Uncomplicated Chlamydia trachomatis Genital Infection and Factors Associated with Chlamydia Resolution: A Review of Human Studies, The Journal of Infectious Diseases, Volume 201, Issue Supplement_2, June 2010, Pages S104–S113, https://doi.org/10.1086/652402[↩]
- Elwell C, Mirrashidi K, Engel J. Chlamydia cell biology and pathogenesis. Nat Rev Microbiol. 2016 Jun;14(6):385-400. doi: 10.1038/nrmicro.2016.30[↩]
- Morré SA, Rozendaal L, van Valkengoed IG, Boeke AJ, van Voorst Vader PC, Schirm J, de Blok S, van Den Hoek JA, van Doornum GJ, Meijer CJ, van Den Brule AJ. Urogenital Chlamydia trachomatis serovars in men and women with a symptomatic or asymptomatic infection: an association with clinical manifestations? J Clin Microbiol. 2000 Jun;38(6):2292-6. doi: 10.1128/JCM.38.6.2292-2296.2000[↩]
- Sexually Transmitted Disease Surveillance 2020. https://www.cdc.gov/std/statistics/2020/overview.htm#Chlamydia[↩]
- Workowski KA, Berman S; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2010 [published correction appears in MMWR Recomm Rep. 2011;60(1):18]. MMWR Recomm Rep. 2010;59(RR-12):1–110.[↩][↩]
- O’Farrell N, Morison L, Moodley P, et al. Genital ulcers and concomitant complaints in men attending a sexually transmitted infections clinic: implications for sexually transmitted infections management. Sexually transmitted diseases 2008;35:545-9.[↩]
- Chlamydial Infections. https://www.cdc.gov/std/treatment-guidelines/chlamydia.htm[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Wiesenfeld HC. Screening for Chlamydia trachomatis Infections in Women. N Engl J Med. 2017 Feb 23;376(8):765-773. doi: 10.1056/NEJMcp1412935[↩][↩][↩][↩][↩]
- Jeanne M. Marrazzo, David H. Martin, Management of Women with Cervicitis, Clinical Infectious Diseases, Volume 44, Issue Supplement_3, April 2007, Pages S102–S110, https://doi.org/10.1086/511423[↩][↩]
- Brunham RC, Gottlieb SL, Paavonen J. Pelvic inflammatory disease. N Engl J Med. 2015 May 21;372(21):2039-48. doi: 10.1056/NEJMra1411426[↩][↩][↩]
- Ness RB, Soper DE, Holley RL, Peipert J, Randall H, Sweet RL, Sondheimer SJ, Hendrix SL, Amortegui A, Trucco G, Songer T, Lave JR, Hillier SL, Bass DC, Kelsey SF. Effectiveness of inpatient and outpatient treatment strategies for women with pelvic inflammatory disease: results from the Pelvic Inflammatory Disease Evaluation and Clinical Health (PEACH) Randomized Trial. Am J Obstet Gynecol. 2002 May;186(5):929-37. doi: 10.1067/mob.2002.121625[↩][↩]
- Brunham RC, Binns B, McDowell J, Paraskevas M. Chlamydia trachomatis infection in women with ectopic pregnancy. Obstet Gynecol. 1986 May;67(5):722-6. doi: 10.1097/00006250-198605000-00022[↩][↩]
- Barry PM, Kent CK, Philip SS, Klausner JD. Results of a program to test women for rectal chlamydia and gonorrhea. Obstetrics and gynecology 2010;115:753-9.[↩][↩]
- Handsfield HH. Lymphogranuloma Venereum Treatment and Terminology. Sex Transm Dis. 2018 Jun;45(6):409-411. doi: 10.1097/OLQ.0000000000000853[↩][↩][↩]
- Bradley P. Stoner, Stephanie E. Cohen, Lymphogranuloma Venereum 2015: Clinical Presentation, Diagnosis, and Treatment, Clinical Infectious Diseases, Volume 61, Issue suppl_8, December 2015, Pages S865–S873, https://doi.org/10.1093/cid/civ756[↩][↩][↩]
- Schachter J, Moncada J. Lymphogranuloma venereum: how to turn an endemic disease into an outbreak of a new disease? Start looking. Sex Transm Dis. 2005 Jun;32(6):331-2. doi: 10.1097/01.olq.0000168429.13282.c8[↩]
- Kalayoglu MV. Ocular chlamydial infections: pathogenesis and emerging treatment strategies. Current drug targets Infectious disorders 2002;2:85-91.[↩]
- Jones RB, Rabinovitch RA, Katz BP, et al. Chlamydia trachomatis in the pharynx and rectum of heterosexual patients at risk for genital infection. Annals of internal medicine 1985;102:757-62.[↩]
- Farley TA, Cohen DA, Elkins W. Asymptomatic sexually transmitted diseases: the case for screening. Preventive medicine 2003;36:502-9.[↩]
- Chlamydia Trachomatis Infection. https://webeye.ophth.uiowa.edu/eyeforum/atlas/pages/chlamydia-trachomatis-infection.htm[↩]
- Wiesenfeld HC, Sweet RL, Ness RB, Krohn MA, Amortegui AJ, Hillier SL. Comparison of acute and subclinical pelvic inflammatory disease. Sexually transmitted diseases 2005;32:400-5.[↩]
- Taylor SN. Cervicitis of unknown etiology. Curr Infect Dis Rep. 2014 Jul;16(7):409. doi: 10.1007/s11908-014-0409-x[↩]
- Bradley MG, Hobson D, Lee N, Tait IA, Rees E. Chlamydial infections of the urethra in women. Genitourin Med. 1985 Dec;61(6):371-5. doi: 10.1136/sti.61.6.371[↩]
- Hook EW, Spitters C, Reichart CA, Neumann TM, Quinn TC. Use of Cell Culture and a Rapid Diagnostic Assay for Chlamydia trachomatis Screening. JAMA. 1994;272(11):867–870. doi:10.1001/jama.1994.03520110047027[↩]
- Oakeshott P, Kerry S, Aghaizu A, Atherton H, Hay S, Taylor-Robinson D, Simms I, Hay P. Randomised controlled trial of screening for Chlamydia trachomatis to prevent pelvic inflammatory disease: the POPI (prevention of pelvic infection) trial. BMJ. 2010 Apr 8;340:c1642. doi: 10.1136/bmj.c1642[↩]
- Ross JD. Pelvic inflammatory disease. BMJ Clin Evid. 2013 Dec 11;2013:1606[↩]
- LeFevre ML; U.S. Preventive Services Task Force. Screening for Chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014 Dec 16;161(12):902-10. doi: 10.7326/M14-1981[↩]
- Money DM, Hawes SE, Eschenbach DA, Peeling RW, Brunham R, Wölner-Hanssen P, Stamm WE. Antibodies to the chlamydial 60 kd heat-shock protein are associated with laparoscopically confirmed perihepatitis. Am J Obstet Gynecol. 1997 Apr;176(4):870-7. doi: 10.1016/s0002-9378(97)70613-6[↩]
- Wang SP, Eschenbach DA, Holmes KK, Wager G, Grayston JT. Chlamydia trachomatis infection in Fitz-Hugh-Curtis syndrome. Am J Obstet Gynecol. 1980 Dec 1;138(7 Pt 2):1034-8. doi: 10.1016/0002-9378(80)91103-5[↩]
- Ris HW. Perihepatitis (Fitz-Hugh–Curtis syndrome). A review and case presentation. J Adolesc Health Care. 1984 Oct;5(4):272-6. doi: 10.1016/s0197-0070(84)80131-x[↩]
- Berger RE, Alexander ER, Monda GD, Ansell J, McCormick G, Holmes KK. Chlamydia trachomatis as a cause of acute “idiopathic” epididymitis. The New England journal of medicine 1978;298:301-4.[↩]
- Moi H, Blee K, Horner PJ. Management of non-gonococcal urethritis. BMC Infect Dis. 2015 Jul 29;15:294. doi: 10.1186/s12879-015-1043-4[↩]
- Stephanie N. Taylor, Epididymitis, Clinical Infectious Diseases, Volume 61, Issue suppl_8, December 2015, Pages S770–S773, https://doi.org/10.1093/cid/civ812[↩][↩]
- Trachoma. https://eyewiki.org/Trachoma[↩]
- Cook JA. Eliminating blinding trachoma. N Engl J Med. 2008 Apr 24;358(17):1777-9. doi: 10.1056/NEJMp0708546[↩]
- Taylor HR, Burton MJ, Haddad D, West S, Wright H. Trachoma. Lancet. 2014 Dec 13;384(9960):2142-52. doi: 10.1016/S0140-6736(13)62182-0[↩]
- Centers for Disease Control and Prevention. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae–2014. MMWR Recomm Rep. 2014 Mar 14;63(RR-02):1-19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047970[↩][↩]
- Cates W, Jr., Wasserheit JN. Genital chlamydial infections: epidemiology and reproductive sequelae. American journal of obstetrics and gynecology 1991;164:1771-81.[↩]
- Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines, 2015. MMWR, 64(RR-3) (2015). https://www.cdc.gov/std/tg2015/default.htm[↩][↩][↩][↩][↩]
- APHL. Laboratory Diagnostic Testing for Chlamydia trachomatis and Neisseria gonorrhoeae. Expert Consultation Meeting Summary Report. January 13-15, 2009. Atlanta, GA.[↩][↩]
- Schachter J, Chernesky MA, Willis DE, et al. Vaginal swabs are the specimens of choice when screening for Chlamydia trachomatis and Neisseria gonorrhoeae: results from a multicenter evaluation of the APTIMA assays for both infections. Sexually transmitted diseases 2005;32:725-8.[↩]
- Doshi JS, Power J, Allen E. Acceptability of chlamydia screening using self-taken vaginal swabs. International journal of STD & AIDS 2008;19:507-9.[↩]
- Bachmann LH, Johnson RE, Cheng H, et al. Nucleic acid amplification tests for diagnosis of Neisseria gonorrhoeae and Chlamydia trachomatis rectal infections. Journal of clinical microbiology 2010;48:1827-32.[↩][↩]
- FDA clears first diagnostic tests for extragenital testing for chlamydia and gonorrhea. https://www.fda.gov/news-events/press-announcements/fda-clears-first-diagnostic-tests-extragenital-testing-chlamydia-and-gonorrhea[↩][↩]
- Lunny C, Taylor D, Hoang L, Wong T, Gilbert M, Lester R, Krajden M, Ogilvie G. Self-Collected versus Clinician-Collected Sampling for Chlamydia and Gonorrhea Screening: A Systemic Review and Meta-Analysis. PLoS One. 2015 Jul 13;10(7):e0132776. doi: 10.1371/journal.pone.0132776[↩]
- Masek BJ, Arora N, Quinn N, Aumakhan B, Holden J, Hardick A, Agreda P, Barnes M, Gaydos CA. Performance of three nucleic acid amplification tests for detection of Chlamydia trachomatis and Neisseria gonorrhoeae by use of self-collected vaginal swabs obtained via an Internet-based screening program. J Clin Microbiol. 2009 Jun;47(6):1663-7. doi: 10.1128/JCM.02387-08[↩]
- van der Helm JJ, Hoebe CJ, van Rooijen MS, Brouwers EE, Fennema HS, Thiesbrummel HF, Dukers-Muijrers NH. High performance and acceptability of self-collected rectal swabs for diagnosis of Chlamydia trachomatis and Neisseria gonorrhoeae in men who have sex with men and women. Sex Transm Dis. 2009 Aug;36(8):493-7. doi: 10.1097/OLQ.0b013e3181a44b8c[↩]
- FDA Allows for First Point-of-Care Chlamydia and Gonorrhea Test to be Used in More Near-Patient Care Settings. https://www.fda.gov/news-events/press-announcements/fda-allows-first-point-care-chlamydia-and-gonorrhea-test-be-used-more-near-patient-care-settings[↩][↩][↩][↩][↩][↩]
- Van Der Pol B, Taylor SN, Mena L, Lebed J, McNeil CJ, Crane L, Ermel A, Sukhija-Cohen A, Gaydos CA. Evaluation of the Performance of a Point-of-Care Test for Chlamydia and Gonorrhea. JAMA Netw Open. 2020 May 1;3(5):e204819. doi: 10.1001/jamanetworkopen.2020.4819[↩][↩][↩][↩][↩][↩]
- Jensen IP, Fogh H, Prag J. Diagnosis of Chlamydia trachomatis infections in a sexually transmitted disease clinic: evaluation of a urine sample tested by enzyme immunoassay and polymerase chain reaction in comparison with a cervical and/or a urethral swab tested by culture and polymerase chain reaction. Clin Microbiol Infect. 2003 Mar;9(3):194-201. doi: 10.1046/j.1469-0691.2003.00483.x[↩]
- Chlamydial Infections. https://www.std.uw.edu/go/comprehensive-study/chlamydial-infections/core-concept/all[↩]
- Centers for Disease Control and Prevention. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae–2014. MMWR Recomm Rep. 2014 Mar 14;63(RR-02):1-19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047970/[↩]
- Lymphogranuloma Venereum (LGV). https://www.cdc.gov/std/treatment-guidelines/lgv.htm[↩][↩][↩][↩][↩]
- Chlamydial Infections. Sexually Transmitted Infections Treatment Guidelines, 2021. https://www.cdc.gov/std/treatment-guidelines/chlamydia.htm[↩]
- Marcus JL, Kohn RP, Barry PM, Philip SS, Bernstein KT. Chlamydia trachomatis and Neisseria gonorrhoeae transmission from the female oropharynx to the male urethra. Sex Transm Dis. 2011 May;38(5):372-3. doi: 10.1097/OLQ.0b013e3182029008[↩]
- Kyle T. Bernstein, Sally C. Stephens, Pennan M. Barry, Robert Kohn, Susan S. Philip, Sally Liska, Jeffrey D. Klausner, Chlamydia trachomatis and Neisseria gonorrhoeae Transmission from the Oropharynx to the Urethra among Men who have Sex with Men, Clinical Infectious Diseases, Volume 49, Issue 12, 15 December 2009, Pages 1793–1797, https://doi.org/10.1086/648427[↩]
- Golden MR, Whittington WL, Handsfield HH, Hughes JP, Stamm WE, Hogben M, Clark A, Malinski C, Helmers JR, Thomas KK, Holmes KK. Effect of expedited treatment of sex partners on recurrent or persistent gonorrhea or chlamydial infection. N Engl J Med. 2005 Feb 17;352(7):676-85. doi: 10.1056/NEJMoa041681[↩]
- Schillinger JA, Kissinger P, Calvet H, Whittington WL, Ransom RL, Sternberg MR, Berman SM, Kent CK, Martin DH, Oh MK, Handsfield HH, Bolan G, Markowitz LE, Fortenberry JD. Patient-delivered partner treatment with azithromycin to prevent repeated Chlamydia trachomatis infection among women: a randomized, controlled trial. Sex Transm Dis. 2003 Jan;30(1):49-56. doi: 10.1097/00007435-200301000-00011[↩]
- Klausner JD, Chaw JK. Patient-delivered therapy for chlamydia: putting research into practice. Sex Transm Dis. 2003 Jun;30(6):509-11. doi: 10.1097/00007435-200306000-00007[↩]
- Eberly MD, Eide MB, Thompson JL, Nylund CM. Azithromycin in early infancy and pyloric stenosis. Pediatrics. 2015 Mar;135(3):483-8. doi: 10.1542/peds.2014-2026[↩][↩]
- Smith C, Egunsola O, Choonara I, Kotecha S, Jacqz-Aigrain E, Sammons H. Use and safety of azithromycin in neonates: a systematic review. BMJ Open. 2015 Dec 9;5(12):e008194. doi: 10.1136/bmjopen-2015-008194[↩]
- Mohseni M, Sung S, Takov V. Chlamydia. [Updated 2023 Jan 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537286[↩]
- Gonorrhea – CDC Basic Fact Sheet. https://www.cdc.gov/std/gonorrhea/stdfact-gonorrhea.htm[↩]
- Gonorrhea – CDC Detailed Fact Sheet. https://www.cdc.gov/std/gonorrhea/stdfact-gonorrhea-detailed.htm[↩][↩][↩]
- Gonococcal Infections Among Adolescents and Adults. https://www.cdc.gov/std/treatment-guidelines/gonorrhea-adults.htm[↩][↩]
- Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice: The contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sex Transm Infect 1999; 75(1):3–17.[↩]
- Sexually Transmitted Disease Surveillance 2017. https://www.cdc.gov/std/stats17/gonorrhea.htm [↩][↩][↩]
- Handsfield HH, Lipman TO, Harnisch JP, Tronca E, Holmes KK. Asymptomatic gonorrhea in men. Diagnosis, natural course, prevalence and significance. N Engl J Med. 1974 Jan 17;290(3):117-23. doi: 10.1056/NEJM197401172900301[↩][↩]
- Peterman TA, Tian LH, Metcalf CA, Satterwhite CL, Malotte CK, DeAugustine N, Paul SM, Cross H, Rietmeijer CA, Douglas JM Jr; RESPECT-2 Study Group. High incidence of new sexually transmitted infections in the year following a sexually transmitted infection: a case for rescreening. Ann Intern Med. 2006 Oct 17;145(8):564-72. doi: 10.7326/0003-4819-145-8-200610170-00005[↩][↩]
- Gonococcal Infections. https://www.std.uw.edu/go/comprehensive-study/gonococcal-infections/core-concept/all[↩][↩][↩]
- https://phil.cdc.gov/details.aspx?pid=4085[↩]
- Thadepalli H, Rambhatla K, Maidman JE, Arce JJ, Davidson EC Jr. Gonococcal sepsis secondary to fetal monitoring. Am J Obstet Gynecol. 1976 Oct 15;126(4):510-2. doi: 10.1016/0002-9378(76)90650-5[↩]
- St Cyr S, Barbee L, Workowski KA, Bachmann LH, Pham C, Schlanger K, Torrone E, Weinstock H, Kersh EN, Thorpe P. Update to CDC’s Treatment Guidelines for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep. 2020 Dec 18;69(50):1911-1916. doi: 10.15585/mmwr.mm6950a6[↩][↩][↩][↩]
- O’Donnell, Judith A.; Gelone, Steven P. (2009). Pelvic Inflammatory Disease. Infobase Publishing. ISBN 9781438101590.[↩]
- Holmes KK, Levine R, Weaver M. Effectiveness of condoms in preventing sexually transmitted infections. Bull World Health Organ. 2004 Jun;82(6):454-61. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2622864[↩][↩]
- Hill SA, Masters TL, Wachter J. Gonorrhea – an evolving disease of the new millennium. Microb Cell. 2016 Sep 5;3(9):371-389. doi: 10.15698/mic2016.09.524[↩]
- Chlamydia and Gonorrhea: Screening. https://www.uspreventiveservicestaskforce.org/uspstf/document/RecommendationStatementFinal/chlamydia-and-gonorrhea-screening[↩]
- Hook EW 3rd, Kirkcaldy RD. A brief history of evolving diagnostics and therapy for gonorrhea: lessons learned. Clin Infect Dis 2018;67:1294–9. 10.1093/cid/ciy271[↩]
- Sánchez-Busó L, Golparian D, Corander J, et al. The impact of antimicrobials on gonococcal evolution. Nat Microbiol 2019;4:1941–50. 10.1038/s41564-019-0501-y[↩]
- Hooper RR, Reynolds GH, Jones OG, et al. Cohort study of venereal disease. I: the risk of gonorrhea transmission from infected women to men. Am J Epidemiol. 1978;108:136-44.[↩]
- Lin JS, Donegan SP, Heeren TC, et al. Transmission of Chlamydia trachomatis and Neisseria gonorrhoeae among men with urethritis and their female sex partners. J Infect Dis. 1998;178:1707-12.[↩]
- Cohen MS, Hoffman IF, Royce RA, et al. Reduction of concentration of HIV-1 in semen after treatment of urethritis: implications for prevention of sexual transmission of HIV-1. AIDSCAP Malawi Research Group. Lancet. 1997;349:1868-73.[↩]
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. Gonococcal infections. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- LeFevre ML; U.S. Preventive Services Task Force. Screening for Chlamydia and gonorrhea: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161:902-10.[↩][↩][↩]
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. Special populations. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.[↩][↩][↩][↩][↩][↩]
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. HIV infection: detection, counseling, and referral. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.[↩]
- Handsfield HH, Lipman TO, Harnisch JP, Tronca E, Holmes KK. Asymptomatic gonorrhea in men. Diagnosis, natural course, prevalence and significance. N Engl J Med. 1974;290:117-23.[↩]
- Harrison WO, Hooper RR, Wiesner PJ, et al. A trial of minocycline given after exposure to prevent gonorrhea. N Engl J Med. 1979;300:1074-8.[↩]
- Jeffrey D. Klausner, Robert Kohn, Charlotte Kent, Etiology of Clinical Proctitis among Men Who Have Sex with Men, Clinical Infectious Diseases, Volume 38, Issue 2, 15 January 2004, Pages 300–302, https://doi.org/10.1086/380838[↩]
- McCormack WM, Stumacher RJ, Johnson K, Donner A. Clinical spectrum of gonococcal infection in women. Lancet. 1977 Jun 4;1(8023):1182-5. doi: 10.1016/s0140-6736(77)92720-9[↩]
- Wan WL, Farkas GC, May WN, Robin JB. The clinical characteristics and course of adult gonococcal conjunctivitis. Am J Ophthalmol. 1986;102:575-83.[↩]
- Holmes KK, Counts GW, Beaty HN. Disseminated gonococcal infection. Ann Intern Med. 1971 Jun;74(6):979-93. doi: 10.7326/0003-4819-74-6-979[↩][↩][↩]
- Bleich AT, Sheffield JS, Wendel GD Jr, Sigman A, Cunningham FG. Disseminated gonococcal infection in women. Obstet Gynecol. 2012;119:597-602.[↩]
- Svensson L, Weström L, Ripa KT, Mårdh PA. Differences in some clinical and laboratory parameters in acute salpingitis related to culture and serologic findings. Am J Obstet Gynecol. 1980 Dec 1;138(7 Pt 2):1017-21. doi: 10.1016/0002-9378(80)91099-6[↩]
- Berger RE, Alexander ER, Harnisch JP, Paulsen CA, Monda GD, Ansell J, Holmes KK. Etiology, manifestations and therapy of acute epididymitis: prospective study of 50 cases. J Urol. 1979 Jun;121(6):750-4. doi: 10.1016/s0022-5347(17)56978-5[↩]
- Centers for Disease Control and Prevention. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae–2014. MMWR Recomm Rep. 2014;63:1-19.[↩][↩][↩]
- Centers for Disease Control and Prevention. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae–2014. MMWR Recomm Rep. 2014;63:1-19. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047970[↩]
- Connolly KL, Eakin AE, Gomez C, Osborn BL, Unemo M, Jerse AE. Pharmacokinetic Data Are Predictive of In Vivo Efficacy for Cefixime and Ceftriaxone against Susceptible and Resistant Neisseria gonorrhoeae Strains in the Gonorrhea Mouse Model. Antimicrob Agents Chemother. 2019 Feb 26;63(3):e01644-18. doi: 10.1128/AAC.01644-18[↩]
- Stephanie A. Chisholm, Johan W. Mouton, David A. Lewis, Tom Nichols, Catherine A. Ison, David M. Livermore, Cephalosporin MIC creep among gonococci: time for a pharmacodynamic rethink?, Journal of Antimicrobial Chemotherapy, Volume 65, Issue 10, October 2010, Pages 2141–2148, https://doi.org/10.1093/jac/dkq289[↩]
- Screening Recommendations and Considerations Referenced in Treatment Guidelines and Original Sources. https://www.cdc.gov/std/treatment-guidelines/screening-recommendations.htm[↩][↩]
- Sexually Transmitted Disease Surveillance 2020. https://www.cdc.gov/std/statistics/2020/overview.htm#Gonorrhea[↩]
- Gernert KM, Seby S, Schmerer MW, Thomas JC 4th, Pham CD, Cyr SS, Schlanger K, Weinstock H, Shafer WM, Raphael BH, Kersh EN; Antimicrobial-Resistant Neisseria gonorrhoeae Working Group *. Azithromycin susceptibility of Neisseria gonorrhoeae in the USA in 2017: a genomic analysis of surveillance data. Lancet Microbe. 2020 Aug;1(4):e154-e164. doi: 10.1016/S2666-5247(20)30059-8[↩]
- Khosropour CM, Dombrowski JC, Barbee LA, Manhart LE, Golden MR. Comparing azithromycin and doxycycline for the treatment of rectal chlamydial infection: a retrospective cohort study. Sex Transm Dis. 2014 Feb;41(2):79-85. doi: 10.1097/OLQ.0000000000000088[↩]
- Fabian Yuh Shiong Kong, Sepehr N. Tabrizi, Christopher Kincaid Fairley, Lenka A. Vodstrcil, Wilhelmina M. Huston, Marcus Chen, Catriona Bradshaw, Jane S. Hocking, The efficacy of azithromycin and doxycycline for the treatment of rectal chlamydia infection: a systematic review and meta-analysis, Journal of Antimicrobial Chemotherapy, Volume 70, Issue 5, May 2015, Pages 1290–1297, https://doi.org/10.1093/jac/dku574[↩]
- F. Y. S. Kong, S. N. Tabrizi, M. Law, L. A. Vodstrcil, M. Chen, C. K. Fairley, R. Guy, C. Bradshaw, J. S. Hocking, Azithromycin Versus Doxycycline for the Treatment of Genital Chlamydia Infection: A Meta-analysis of Randomized Controlled Trials, Clinical Infectious Diseases, Volume 59, Issue 2, 15 July 2014, Pages 193–205, https://doi.org/10.1093/cid/ciu220[↩]
- 2015 Sexually Transmitted Diseases Treatment Guidelines. Gonococcal Infections. https://www.cdc.gov/std/tg2015/gonorrhea.htm[↩]
- Schachter J, Moncada J, Liska S, et al. Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sex Transm Dis 2008;35:637–42.[↩]
- Ota KV, Fisman DN, Tamari IE, et al. Incidence and treatment outcomes of pharyngeal Neisseria gonorrhoeae and Chlamydia trachomatis infections in men who have sex with men: a 13-year retrospective cohort study. Clin Infect Dis 2009;48:1237–43.[↩]
- Newman LM, Moran JS, Workowski KA. Update on the management of gonorrhea in adults in the United States. Clin Infect Dis 2007;44(Suppl 3):S84–101.[↩]
- Haimovici R, Roussel TJ. Treatment of gonococcal conjunctivitis with single-dose intramuscular ceftriaxone. Am J Ophthalmol. 1989 May 15;107(5):511-4. doi: 10.1016/0002-9394(89)90495-9[↩]
- American College of Obstetricians and Gynecologists’ Committee on Obstetric Practice. Committee opinion No. 717: sulfonamides, nitrofurantoin, and risk of birth defects. Obstet Gynecol 2017;130:e150–2. 10.1097/AOG.0000000000002300[↩]
- Bleich AT, Sheffield JS, Wendel GD Jr, Sigman A, Cunningham FG. Disseminated gonococcal infection in women. Obstet Gynecol 2012;119:597–602. 10.1097/AOG.0b013e318244eda9[↩]
- Belkacem A, Caumes E, Ouanich J, et al.; Working Group FRA-DGI. Changing patterns of disseminated gonococcal infection in France: cross-sectional data 2009–2011. Sex Transm Infect 2013;89:613–5. 10.1136/sextrans-2013-051119[↩]
- Birrell JM, Gunathilake M, Singleton S, Williams S, Krause V. Characteristics and impact of disseminated gonococcal infection in the “Top End” of Australia. Am J Trop Med Hyg 2019;101:753–60. 10.4269/ajtmh.19-0288[↩]
- Crew PE, Abara WE, McCulley L, et al. Disseminated gonococcal infections in patients receiving eculizumab: a case series. Clin Infect Dis 2019;69:596–600. 10.1093/cid/ciy958[↩]
- Centers for Disease Control and Prevention (CDC). Update to CDC’s sexually transmitted diseases treatment guidelines, 2006: fluoroquinolones no longer recommended for treatment of gonococcal infections. MMWR Morb Mortal Wkly Rep. 2007;56:332-6.[↩]
- Picker MA, Knoblock RJ, Hansen H, Bautista I, Griego R, Barber L, Bendik W, Lam K, Adelman E, Qiu-Shultz Z, Raphael BH, Pham CD, Kersh EN, Weinstock H, St Cyr SB. Notes from the Field: First Case in the United States of Neisseria gonorrhoeae Harboring Emerging Mosaic penA60 Allele, Conferring Reduced Susceptibility to Cefixime and Ceftriaxone. MMWR Morb Mortal Wkly Rep. 2020 Dec 11;69(49):1876-1877. doi: 10.15585/mmwr.mm6949a5[↩]
- Deguchi T, Yasuda M, Hatazaki K, et al. New Clinical Strain of Neisseria gonorrhoeae with Decreased Susceptibility to Ceftriaxone, Japan. Emerg Infect Dis. 2016;22:142-4.[↩]
- Ohnishi M, Golparian D, Shimuta K, Saika T, Hoshina S, Iwasaku K, Nakayama S, Kitawaki J, Unemo M. Is Neisseria gonorrhoeae initiating a future era of untreatable gonorrhea?: detailed characterization of the first strain with high-level resistance to ceftriaxone. Antimicrob Agents Chemother. 2011 Jul;55(7):3538-45. doi: 10.1128/AAC.00325-11[↩]
- Jordi Cámara, Judit Serra, Josefina Ayats, Teresa Bastida, Dolors Carnicer-Pont, Antònia Andreu, Carmen Ardanuy, Molecular characterization of two high-level ceftriaxone-resistant Neisseria gonorrhoeae isolates detected in Catalonia, Spain, Journal of Antimicrobial Chemotherapy, Volume 67, Issue 8, August 2012, Pages 1858–1860, https://doi.org/10.1093/jac/dks162[↩]
- Novalbos A, Sastre J, Cuesta J, et al. Lack of allergic cross-reactivity to cephalosporins among patients allergic to penicillins. Clin Exp Allergy. 2001;31:438-43.[↩]
- Taylor SN, Marrazzo J, Batteiger BE, Hook EW 3rd, Seña AC, Long J, Wierzbicki MR, Kwak H, Johnson SM, Lawrence K, Mueller J. Single-Dose Zoliflodacin (ETX0914) for Treatment of Urogenital Gonorrhea. N Engl J Med. 2018 Nov 8;379(19):1835-1845. doi: 10.1056/NEJMoa1706988[↩]
- Taylor SN, Morris DH, Avery AK, Workowski KA, Batteiger BE, Tiffany CA, Perry CR, Raychaudhuri A, Scangarella-Oman NE, Hossain M, Dumont EF. Gepotidacin for the Treatment of Uncomplicated Urogenital Gonorrhea: A Phase 2, Randomized, Dose-Ranging, Single-Oral Dose Evaluation. Clin Infect Dis. 2018 Aug 1;67(4):504-512. doi: 10.1093/cid/ciy145[↩]
- Chen MY, McNulty A, Avery A, Whiley D, Tabrizi SN, Hardy D, Das AF, Nenninger A, Fairley CK, Hocking JS, Bradshaw CS, Donovan B, Howden BP, Oldach D; Solitaire-U Team. Solithromycin versus ceftriaxone plus azithromycin for the treatment of uncomplicated genital gonorrhoea (SOLITAIRE-U): a randomised phase 3 non-inferiority trial. Lancet Infect Dis. 2019 Aug;19(8):833-842. doi: 10.1016/S1473-3099(19)30116-1[↩]
- Hook EW 3rd, Golden MR, Taylor SN, Henry E, Tseng C, Workowski KA, Swerdlow J, Nenninger A, Cammarata S. Efficacy and Safety of Single-Dose Oral Delafloxacin Compared With Intramuscular Ceftriaxone for Uncomplicated Gonorrhea Treatment: An Open-Label, Noninferiority, Phase 3, Multicenter, Randomized Study. Sex Transm Dis. 2019 May;46(5):279-286. doi: 10.1097/OLQ.0000000000000971[↩]
- Golden MR, Whittington WL, Handsfield HH, et al. Effect of expedited treatment of sex partners on recurrent or persistent gonorrhea or chlamydial infection. N Engl J Med. 2005;352:676-85.[↩]
- Schiffer JT, Corey L. New concepts in understanding genital herpes. Curr Infect Dis Rep. 2009 Nov;11(6):457-64. doi: 10.1007/s11908-009-0066-7[↩]
- Genital Herpes – CDC Detailed Fact Sheet. https://www.cdc.gov/std/herpes/stdfact-herpes-detailed.htm[↩][↩]
- Genital Herpes. https://www.cdc.gov/std/treatment-guidelines/herpes.htm[↩][↩]
- Gnann JW Jr, Whitley RJ. CLINICAL PRACTICE. Genital Herpes. N Engl J Med. 2016 Aug 18;375(7):666-74. doi: 10.1056/NEJMcp1603178[↩]
- Spicknall IH, Flagg EW, Torrone EA. Estimates of the Prevalence and Incidence of Genital Herpes, United States, 2018. Sex Transm Dis. 2021 Apr 1;48(4):260-265. doi: 10.1097/OLQ.0000000000001375[↩][↩][↩]
- Ryder N, Jin F, McNulty AM, Grulich AE, Donovan B. Increasing role of herpes simplex virus type 1 in first-episode anogenital herpes in heterosexual women and younger men who have sex with men, 1992-2006. Sex Transm Infect. 2009 Oct;85(6):416-9. doi: 10.1136/sti.2008.033902[↩]
- Roberts CM, Pfister JR, Spear SJ. Increasing proportion of herpes simplex virus type 1 as a cause of genital herpes infection in college students. Sex Transm Dis. 2003 Oct;30(10):797-800. doi: 10.1097/01.OLQ.0000092387.58746.C7[↩][↩]
- James M. Sizemore, Jr, Fred Lakeman, Richard Whitley, Annalee Hughes, Edward W. Hook III, The Spectrum of Genital Herpes Simplex Virus Infection in Men Attending a Sexually Transmitted Disease Clinic, The Journal of Infectious Diseases, Volume 193, Issue 7, 1 April 2006, Pages 905–911, https://doi.org/10.1086/500841[↩]
- Heather Bradley, Lauri E. Markowitz, Theda Gibson, Geraldine M. McQuillan, Seroprevalence of Herpes Simplex Virus Types 1 and 2—United States, 1999–2010, The Journal of Infectious Diseases, Volume 209, Issue 3, 1 February 2014, Pages 325–333, https://doi.org/10.1093/infdis/jit458[↩][↩][↩]
- Bernstein DI, Bellamy AR, Hook EW 3rd, Levin MJ, Wald A, Ewell MG, Wolff PA, Deal CD, Heineman TC, Dubin G, Belshe RB. Epidemiology, clinical presentation, and antibody response to primary infection with herpes simplex virus type 1 and type 2 in young women. Clin Infect Dis. 2013 Feb;56(3):344-51. doi: 10.1093/cid/cis891[↩]
- Cherpes TL, Meyn LA, Hillier SL. Cunnilingus and vaginal intercourse are risk factors for herpes simplex virus type 1 acquisition in women. Sex Transm Dis. 2005 Feb;32(2):84-9. doi: 10.1097/01.olq.0000151414.64297.46[↩]
- William E. Lafferty, Lois Downey, Connie Celum, Anna Wald, Herpes Simplex Virus Type 1 as a Cause of Genital Herpes: Impact on Surveillance and Prevention, The Journal of Infectious Diseases, Volume 181, Issue 4, April 2000, Pages 1454–1457, https://doi.org/10.1086/315395[↩]
- Gregory J. Mertz, Asymptomatic Shedding of Herpes Simplex Virus 1 and 2: Implications for Prevention of Transmission, The Journal of Infectious Diseases, Volume 198, Issue 8, 15 October 2008, Pages 1098–1100, https://doi.org/10.1086/591914[↩]
- Mertz GJ, Benedetti J, Ashley R, Selke SA, Corey L. Risk factors for the sexual transmission of genital herpes. Ann Intern Med. 1992 Feb 1;116(3):197-202. doi: 10.7326/0003-4819-116-3-197[↩]
- Mertz GJ, Schmidt O, Jourden JL, Guinan ME, Remington ML, Fahnlander A, Winter C, Holmes KK, Corey L. Frequency of acquisition of first-episode genital infection with herpes simplex virus from symptomatic and asymptomatic source contacts. Sex Transm Dis. 1985 Jan-Mar;12(1):33-9. doi: 10.1097/00007435-198501000-00007[↩]
- Ribes JA, Steele AD, Seabolt JP, Baker DJ. Six-year study of the incidence of herpes in genital and nongenital cultures in a central Kentucky medical center patient population. J Clin Microbiol. 2001 Sep;39(9):3321-5. doi: 10.1128/JCM.39.9.3321-3325.2001[↩]
- Freeman EE, Weiss HA, Glynn JR, Cross PL, Whitworth JA, Hayes RJ. Herpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and meta-analysis of longitudinal studies. AIDS. 2006 Jan 2;20(1):73-83. doi: 10.1097/01.aids.0000198081.09337.a7[↩]
- Corey L. Synergistic copathogens–HIV-1 and HSV-2. N Engl J Med. 2007 Feb 22;356(8):854-6. doi: 10.1056/NEJMe068302. Erratum in: N Engl J Med. 2007 Apr 5;356(14):1487.[↩]
- Leeyaphan C, Surawan TM, Chirachanakul P, Prasertworonun N, Punyaratabandhu P, Omcharoen V, Jiamton S. Clinical characteristics of hypertrophic herpes simplex genitalis and treatment outcomes of imiquimod: a retrospective observational study. Int J Infect Dis. 2015 Apr;33:165-70. doi: 10.1016/j.ijid.2015.02.002[↩]
- Tan DH, Kaul R, Walsmley S. Left out but not forgotten: Should closer attention be paid to coinfection with herpes simplex virus type 1 and HIV? Can J Infect Dis Med Microbiol. 2009 Spring;20(1):e1-7. doi: 10.1155/2009/965263[↩]
- Johnston C, Corey L. Current Concepts for Genital Herpes Simplex Virus Infection: Diagnostics and Pathogenesis of Genital Tract Shedding. Clin Microbiol Rev. 2016 Jan;29(1):149-61. doi: 10.1128/CMR.00043-15[↩]
- Efstathiou S, Field HJ, Griffiths PD, Kern ER, Sacks SL, Sawtell NM, Stanberry LR. Herpes simplex virus latency and nucleoside analogues. Antiviral Res. 1999 Apr;41(3):85-100. doi: 10.1016/s0166-3542(99)00003-0[↩]
- Simmons A, Field HJ. Can HSV latency be conquered by current antiviral therapies? Sex Transm Infect. 1998 Feb;74(1):1-2.[↩]
- Doorbar J, Quint W, Banks L, Bravo IG, Stoler M, Broker TR, Stanley MA. The biology and life-cycle of human papillomaviruses. Vaccine. 2012 Nov 20;30 Suppl 5:F55-70. doi: 10.1016/j.vaccine.2012.06.083[↩]
- Schiffman M, Doorbar J, Wentzensen N, de Sanjosé S, Fakhry C, Monk BJ, Stanley MA, Franceschi S. Carcinogenic human papillomavirus infection. Nat Rev Dis Primers. 2016 Dec 1;2:16086. doi: 10.1038/nrdp.2016.86[↩][↩][↩][↩]
- Wangu Z, Hsu KK. Impact of HPV vaccination on anogenital warts and respiratory papillomatosis. Hum Vaccin Immunother. 2016 Jun 2;12(6):1357-62. doi: 10.1080/21645515.2016.1172754[↩][↩]
- Suzanne M. Garland, Marc Steben, Heather L. Sings, Margaret James, Shuang Lu, Radha Railkar, Eliav Barr, Richard M. Haupt, Elmar A. Joura, Natural History of Genital Warts: Analysis of the Placebo Arm of 2 Randomized Phase III Trials of a Quadrivalent Human Papillomavirus (Types 6, 11, 16, and 18) Vaccine, The Journal of Infectious Diseases, Volume 199, Issue 6, 15 March 2009, Pages 805–814, https://doi.org/10.1086/597071[↩]
- Ball, S.L.R., Winder, D.M., Vaughan, K., Hanna, N., Levy, J., Sterling, J.C., Stanley, M.A. and Goon, P.K.C. (2011), Analyses of human papillomavirus genotypes and viral loads in anogenital warts. J. Med. Virol., 83: 1345-1350. https://doi.org/10.1002/jmv.22111[↩]
- Human Papillomavirus (HPV) Infection. https://www.cdc.gov/std/treatment-guidelines/hpv.htm[↩][↩]
- Cancers Associated with Human Papillomavirus, United States—2013–2017. https://www.cdc.gov/cancer/uscs/about/data-briefs/no18-hpv-assoc-cancers-UnitedStates-2013-2017.htm[↩][↩]
- Saraiya M, Unger ER, Thompson TD, Lynch CF, Hernandez BY, Lyu CW, Steinau M, Watson M, Wilkinson EJ, Hopenhayn C, Copeland G, Cozen W, Peters ES, Huang Y, Saber MS, Altekruse S, Goodman MT; HPV Typing of Cancers Workgroup. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst. 2015 Apr 29;107(6):djv086. doi: 10.1093/jnci/djv086[↩]
- Human Papillomavirus (HPV) Vaccination: What Everyone Should Know. https://www.cdc.gov/vaccines/vpd/hpv/public[↩][↩][↩]
- Burchell AN, Tellier PP, Hanley J, Coutlée F, Franco EL. Human papillomavirus infections among couples in new sexual relationships. Epidemiology. 2010 Jan;21(1):31-7. doi: 10.1097/EDE.0b013e3181c1e70b[↩]
- Burchell AN, Coutlée F, Tellier PP, Hanley J, Franco EL. Genital transmission of human papillomavirus in recently formed heterosexual couples. J Infect Dis. 2011 Dec 1;204(11):1723-9. doi: 10.1093/infdis/jir644[↩]
- Lam JU, Rebolj M, Dugué PA, Bonde J, von Euler-Chelpin M, Lynge E. Condom use in prevention of Human Papillomavirus infections and cervical neoplasia: systematic review of longitudinal studies. J Med Screen. 2014 Mar;21(1):38-50. doi: 10.1177/0969141314522454[↩]
- Ryndock EJ, Meyers C. A risk for non-sexual transmission of human papillomavirus? Expert Rev Anti Infect Ther. 2014 Oct;12(10):1165-70. doi: 10.1586/14787210.2014.959497[↩]
- Sabeena, S., Bhat, P., Kamath, V., and Arunkumar, G. (2017) Possible non-sexual modes of transmission of human papilloma virus. J. Obstet. Gynaecol. Res., 43: 429– 435. doi: 10.1111/jog.13248[↩]
- Maturo SC, Hartnick CJ. Juvenile-onset recurrent respiratory papillomatosis. Adv Otorhinolaryngol. 2012;73:105-8. doi: 10.1159/000334457[↩]
- Derkay CS, Bluher AE. Update on Recurrent Respiratory Papillomatosis. Otolaryngol Clin North Am. 2019 Aug;52(4):669-679. doi: 10.1016/j.otc.2019.03.011[↩]
- Anogenital Warts. https://www.cdc.gov/std/treatment-guidelines/anogenital-warts.htm[↩][↩][↩][↩][↩]
- Human Papillomavirus Infection. https://www.std.uw.edu/go/comprehensive-study/hpv/core-concept/all[↩][↩][↩][↩]
- D’Ambrogio A, Yerly S, Sahli R, Bouzourene H, Demartines N, Cotton M, Givel JC. Human papilloma virus type and recurrence rate after surgical clearance of anal condylomata acuminata. Sex Transm Dis. 2009 Sep;36(9):536-40. doi: 10.1097/OLQ.0b013e3181a866a3[↩]
- Filley CM, Graff-Richard NR, Lacy JR, Heitner MA, Earnest MP. Neurologic manifestations of podophyllin toxicity. Neurology. 1982 Mar;32(3):308-11. doi: 10.1212/wnl.32.3.308[↩]
- Syphilis – CDC Fact Sheet (Detailed). https://www.cdc.gov/std/syphilis/stdfact-syphilis-detailed.htm[↩]
- https://phil.cdc.gov/Details.aspx?pid=21621[↩]
- Centers for Disease Control and Prevention.Sexually Transmitted Disease Surveillance, 2016. Atlanta, GA: Department of Health and Human Services; September 2017. https://www.cdc.gov/std/stats16/default.htm[↩]
- Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines, 2015 MMWR, 64(RR-3) (2015) https://www.cdc.gov/std/tg2015/default.htm[↩][↩][↩][↩]
- Alexander, J.M., et al., Efficacy of treatment for syphilis in pregnancy. Obstet Gynecol, 1999. 93(1): p. 5-8.[↩][↩]
- Marra CM. Neurosyphilis. Continuum (Minneap Minn). 2015 Dec;21(6 Neuroinfectious Disease):1714-28. doi: 10.1212/CON.0000000000000250[↩][↩][↩][↩][↩]
- Ho EL, Lukehart SA. Syphilis: using modern approaches to understand an old disease. J Clin Invest. 2011 Dec;121(12):4584-92. doi: 10.1172/JCI57173[↩][↩]
- Rolfs RT, Joesoef MR, Hendershot EF, Rompalo AM, Augenbraun MH, Chiu M, Bolan G, Johnson SC, French P, Steen E, Radolf JD, Larsen S. A randomized trial of enhanced therapy for early syphilis in patients with and without human immunodeficiency virus infection. The Syphilis and HIV Study Group. N Engl J Med. 1997 Jul 31;337(5):307-14. doi: 10.1056/NEJM199707313370504[↩]
- Lukehart SA, Hook EW 3rd, Baker-Zander SA, Collier AC, Critchlow CW, Handsfield HH. Invasion of the central nervous system by Treponema pallidum: implications for diagnosis and treatment. Ann Intern Med. 1988 Dec 1;109(11):855-62. doi: 10.7326/0003-4819-109-11-855[↩]
- Hook EW 3rd, Marra CM. Acquired syphilis in adults. N Engl J Med. 1992 Apr 16;326(16):1060-9. doi: 10.1056/NEJM199204163261606[↩]
- Ghanem KG, Ram S, Rice PA. The Modern Epidemic of Syphilis. N Engl J Med. 2020 Feb 27;382(9):845-854. doi: 10.1056/NEJMra1901593[↩][↩]
- Woolston SL, Dhanireddy S, Marrazzo J. Ocular Syphilis: a Clinical Review. Curr Infect Dis Rep. 2016 Nov;18(11):36. doi: 10.1007/s11908-016-0542-9[↩][↩]
- Spoor TC, Wynn P, Hartel WC, Bryan CS. Ocular syphilis. Acute and chronic. J Clin Neuroophthalmol. 1983 Sep;3(3):197-203.[↩][↩][↩]
- Moradi A, Salek S, Daniel E, Gangaputra S, Ostheimer TA, Burkholder BM, Leung TG, Butler NJ, Dunn JP, Thorne JE. Clinical features and incidence rates of ocular complications in patients with ocular syphilis. Am J Ophthalmol. 2015 Feb;159(2):334-43.e1. doi: 10.1016/j.ajo.2014.10.030[↩]
- Syphilis. https://www.cdc.gov/std/treatment-guidelines/syphilis.htm[↩][↩][↩][↩][↩]
- Ramchandani MS, Litvack JR, Marra CM. Otosyphilis: A Review of the Literature. Sex Transm Dis. 2020 May;47(5):296-300. doi: 10.1097/OLQ.0000000000001155[↩][↩]
- Theeuwen, H., Whipple, M. and Litvack, J.R. (2019), Otosyphilis: Resurgence of an Old Disease. The Laryngoscope, 129: 1680-1684. https://doi.org/10.1002/lary.27635[↩][↩][↩]
- Medoro AK, Sánchez PJ. Syphilis in Neonates and Infants. Clin Perinatol. 2021 Jun;48(2):293-309. doi: 10.1016/j.clp.2021.03.005[↩][↩][↩][↩]
- Peeling RW, Mabey D, Kamb ML, Chen XS, Radolf JD, Benzaken AS. Syphilis. Nat Rev Dis Primers. 2017 Oct 12;3:17073. doi: 10.1038/nrdp.2017.73[↩][↩]
- Syphilis. https://www.cdc.gov/std/statistics/2020/overview.htm#Syphilis[↩][↩]
- Rac MW, Revell PA, Eppes CS. Syphilis during pregnancy: a preventable threat to maternal-fetal health. Am J Obstet Gynecol. 2017 Apr;216(4):352-363. doi: 10.1016/j.ajog.2016.11.1052[↩]
- Rathbun KC. Congenital syphilis. Sex Transm Dis. 1983 Apr-Jun;10(2):93-9. doi: 10.1097/00007435-198304000-00009[↩]
- Lafond RE, Lukehart SA. Biological basis for syphilis. Clin Microbiol Rev. 2006 Jan;19(1):29-49. doi: 10.1128/CMR.19.1.29-49.2006[↩]
- Cremin BJ, Fisher RM. The lesions of congenital syphilis. Br J Radiol. 1970 May;43(509):333-41. doi: 10.1259/0007-1285-43-509-333[↩][↩]
- Fiumara NJ, Lessell S. Manifestations of Late Congenital Syphilis: An Analysis of 271 Patients. Arch Dermatol. 1970;102(1):78–83. doi:10.1001/archderm.1970.04000070080012[↩]
- CDC, Association of Public Health Laboratories. Laboratory diagnostic testing for Treponema pallidum, Expert Consultation Meeting Summary Report, January 13-15, 2009, Atlanta, GA. https://www.aphl.org/programs/infectious_disease/std/Documents/ID_2009Jan_Laboratory-Guidelines-Treponema-pallidum-Meeting-Report.pdf[↩]
- Romanowski B, Sutherland R, Fick GH, et al. Serologic response to treatment of infectious syphilis. Ann Intern Med 1991;114:1005–9.[↩]
- CDC. Discordant results from reverse sequence syphilis screening–five laboratories, United States, 2006-2010. MMWR Morbid Mortal Wkly Rep 2011;60:133–7.[↩]
- Park IU, Chow JM, Bolan G, et al. Screening for syphilis with the treponemal immunoassay: analysis of discordant serology results and implications for clinical management. J Infect Dis 2011;204:1297–304.[↩]
- Lukehart SA, Hook EW, III, Baker-Zander SA, et al. Invasion of the central nervous system by Treponema pallidum: implications for diagnosis and treatment. Ann Intern Med 1988;109:855–62.[↩][↩]
- Jaffe HW, Larsen SA, Peters M, et al. Tests for treponemal antibody in CSF. Arch Intern Med 1978;138:252–5.[↩]
- Marra CM, Maxwell CL, Smith SL, et al. Cerebrospinal fluid abnormalities in patients with syphilis: association with clinical and laboratory features. J Infect Dis 2004;189:369–76.[↩]
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. Syphilis. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.[↩]
- Centers for Disease Control and Prevention (CDC). Discordant results from reverse sequence syphilis screening–five laboratories, United States, 2006-2010. MMWR Morb Mortal Wkly Rep. 2011;60:133-7.[↩]
- Centers for Disease Control and Prevention. Discordant results from reverse sequence syphilis screening–five laboratories, United States, 2006-2010. MMWR Morb Mortal Wkly Rep, 2011. 60(5): p. 133-7. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6005a1.htm[↩]
- Kingston AA, Vujevich J, Shapiro M, et al. Seronegative secondary syphilis in 2 patients coinfected with human immunodeficiency virus. Arch Dermatol 2005;141:431–3.[↩]
- Syphilis. 2015 Sexually Transmitted Diseases Treatment Guidelines. https://www.cdc.gov/std/tg2015/syphilis.htm[↩]
- CDC. Inadvertent use of Bicillin® C-R to treat syphilis infection-Los Angeles, California, 1999-2004. MMWR Morbid Mortal Wkly Rep 2005;54:217–9.[↩]
- Brown ST. Adverse reactions in syphilis therapy. J Am Vener Dis Assoc. 1976;3:172-6.[↩]
- Sena AC, Wolff M, Martin DH, et al. Predictors of serological cure and Serofast State after treatment in HIV-negative persons with early syphilis. Clin Infect Dis 2011;53:1092–9.[↩][↩][↩]
- Sena AC, Wolff M, Behets F, et al. Response to therapy following retreatment of serofast early syphilis patients with benzathine penicillin. Clin Infect Dis 2013;56:420–2.[↩]
- Taiwan HIV and Syphilis Study Group. Comparison of effectiveness of 1 dose versus 3 doses of benzathine penicillin in treatment of early syphilis in HIV-infected patients: multicenter, prospective observational study in Taiwan [Abstract# S-119]. Presented at: the 20th Conference on Retroviruses and Opportunistic Infections (CROI 2013); March 3-6, 2013; Atlanta, GA.[↩][↩]
- Hagdrup HK, Lange Wantzin G, Secher L, et al. Penicillin concentrations in serum following weekly injections of benzathine penicillin G. Chemotherapy 1986;32:99–101.[↩]
- Nathan L, Bawdon RE, Sidawi JE, et al. Penicillin levels following the administration of benzathine penicillin G in pregnancy. Obstet Gynecol 1993;82:338–42.[↩][↩]
- CDC. Symptomatic early neurosyphilis among HIV-positive men who have sex with men–four cities, United States, January 2002-June 2004. MMWR Morb Mortal Wkly Rep 2007;56:625–8.[↩]
- Rolfs RT, Joesoef MR, Hendershot EF, et al. The Syphilis and HIV Study Group. A randomized trial of enhanced therapy for early syphilis in patients with and without human immunodeficiency virus infection. N Engl J Med 1997;337:307–14.[↩]
- Marra CM, Maxwell CL, Tantalo LC, et al. Normalization of serum rapid plasma reagin titer predicts normalization of cerebrospinal fluid and clinical abnormalities after treatment of neurosyphilis. Clin Infect Dis 2008;47:893–9.[↩][↩][↩]
- Alexander JM, Sheffield JS, Sanchez PJ, et al. Efficacy of treatment for syphilis in pregnancy. Obstet Gynecol 1999;93:5–8.[↩]
- Walker GJ. Antibiotics for syphilis diagnosed during pregnancy. Cochrane Database Syst Rev 2001:CD001143.[↩]
- Hawkes S, Matin N, Broutet N, et al. Effectiveness of interventions to improve screening for syphilis in pregnancy: a systematic review and meta-analysis. Lancet Infect Dis 2011;11:684–91.[↩]
- Hollier LM, Harstad TW, Sanchez PJ, et al. Fetal syphilis: clinical and laboratory characteristics. Obstet Gynecol 2001;97:947–53.[↩]
- Klein VR, Cox SM, Mitchell MD, et al. The Jarisch-Herxheimer reaction complicating syphilotherapy in pregnancy. Obstet Gynecol 1990;75(3 Pt 1):375–80.[↩]
- Shann S, Wilson J. Treatment of neurosyphilis with ceftriaxone. Sex Transm Infect 2003;79:415–6.[↩]
- Ahmed KA, Fox SJ, Frigas E, et al. Clinical outcome in the use of cephalosporins in pediatric patients with a history of penicillin allergy. International Arch Allergy Immunol 2012;158:405–10.[↩][↩][↩][↩]
- Albin S, Agarwal S. Prevalence and characteristics of reported penicillin allergy in an urban outpatient adult population. Allergy Asthma Proc 2014;35:489–94.[↩]
- Lee CE, Zembower TR, Fotis MA, et al. The incidence of antimicrobial allergies in hospitalized patients: implications regarding prescribing patterns and emerging bacterial resistance. Arch Intern Med 2000;160:2819–22.[↩]
- Jares EJ, Sanchez-Borges M, Cardona-Villa R, et al. Multinational experience with hypersensitivity drug reactions in Latin America. Ann Allergy Asthma Immunol 2014;113:282–9.[↩]
- Wong BB, Keith PK, Waserman S. Clinical history as a predictor of penicillin skin test outcome. Annals Asthma Allergy Immunol 2006;97:169–74.[↩]
- Macy E, Ngor EW. Safely diagnosing clinically significant penicillin allergy using only penicilloyl-poly-lysine, penicillin, and oral amoxicillin. J Allergy Clin Immunol Pract 2013;1:258–63.[↩]
- Raja AS, Lindsell CJ, Bernstein JA, et al. The use of penicillin skin testing to assess the prevalence of penicillin allergy in an emergency department setting. Annals Emerg Med 2009;54:72–7.[↩]
- Saxon A, Beall GN, Rohr AS, Adelman DC. Immediate hypersensitivity reactions to beta-lactam antibiotics. Ann Intern Med 1987;107:204–15.[↩]
- Vega JM, Blanca M, Garcia JJ, et al. Immediate allergic reactions to amoxicillin. Allergy 1994;49:317–22.[↩]
- Legere HJ, 3rd, Palis RI, Rodriguez Bouza T, et al. A safe protocol for rapid desensitization in patients with cystic fibrosis and antibiotic hypersensitivity. Journal of Cystic Fibrosis 2009;8:418–24.[↩]
- Wendel GO, Jr, Stark BJ, Jamison RB, Melina RD, Sullivan TJ. Penicillin allergy and desensitization in serious infections during pregnancy. N Engl J Med 1985;312:1229–32.[↩]
- Trichomoniasis – CDC Fact Sheet. https://www.cdc.gov/std/trichomonas/stdfact-trichomoniasis.htm[↩]
- Madeline Sutton, Maya Sternberg, Emilia H. Koumans, Geraldine McQuillan, Stuart Berman, Lauri Markowitz; The Prevalence of Trichomonas vaginalis Infection among Reproductive-Age Women in the United States, 2001–2004, Clinical Infectious Diseases, Volume 45, Issue 10, 15 November 2007, Pages 1319–1326, https://doi.org/10.1086/522532[↩]
- Sutton MY, Sternberg M, Nsuami M, Behets F, Nelson AM, St Louis ME. Trichomoniasis in pregnant human immunodeficiency virus-infected and human immunodeficiency virus-uninfected Congolese women: prevalence, risk factors, and association with low birth weight, Am J Obstet Gynecol , 1999, vol. 181, pg. 656-62[↩]
- Vaginitis. https://www.std.uw.edu/go/syndrome-based/vaginal-discharge/core-concept/all#trichomoniasis[↩][↩]
- Schwebke JR, Hobbs MM, Taylor SN, et al. Molecular Testing for Trichomonas vaginalis in Women: Results from a Prospective U.S. Clinical Trial . Journal of Clinical Microbiology. 2011;49(12):4106-4111. doi:10.1128/JCM.01291-11. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3232944/[↩]
- Trichomoniasis. https://www.cdc.gov/std/tg2015/trichomoniasis.htm[↩]
- Cotch MF, Pastorek JG2nd, Nugent RP, et al. Trichomonas vaginalis associated with low birth weight and preterm delivery. The Vaginal Infections and Prematurity Study Group, Sex Transm Dis , 1997, vol. 24, pg. 353-60[↩]
- French JI, McGregor JA, Parker R. Readily treatable reproductive tract infections and preterm birth among black women, Am J Obstet Gynecol , 2006, vol. 194 (pg. 1717-26) discussion 1726-7[↩]
- Schwebke JR, Hobbs MM, Taylor SN, Sena AC, Catania MG, Weinbaum BS, Johnson AD, Getman DK, Gaydos CA. Molecular testing for Trichomonas vaginalis in women: results from a prospective U.S. clinical trial. J Clin Microbiol. 2011 Dec;49(12):4106-11. doi: 10.1128/JCM.01291-11[↩][↩][↩]
- Petrin D, Delgaty K, Bhatt R, Garber G. Clinical and microbiological aspects of Trichomonas vaginalis. Clin Microbiol Rev. 1998 Apr;11(2):300-17. doi: 10.1128/CMR.11.2.300[↩][↩][↩]
- Anthony C. Fouts, Stephen J. Kraus, Trichomonas vaginalis: Reevaluation of Its Clinical Presentation and Laboratory Diagnosis, The Journal of Infectious Diseases, Volume 141, Issue 2, February 1980, Pages 137–143, https://doi.org/10.1093/infdis/141.2.137[↩]
- Van Gerwen OT, Craig-Kuhn MC, Jones AT, Schroeder JA, Deaver J, Buekens P, Kissinger PJ, Muzny CA. Trichomoniasis and adverse birth outcomes: a systematic review and meta-analysis. BJOG. 2021 Nov;128(12):1907-1915. doi: 10.1111/1471-0528.16774[↩]
- Mann JR, McDermott S, Gill T. Sexually transmitted infection is associated with increased risk of preterm birth in South Carolina women insured by Medicaid. J Matern Fetal Neonatal Med. 2010 Jun;23(6):563-8. doi: 10.3109/14767050903214574[↩]
- Mann JR, McDermott S, Zhou L, Barnes TL, Hardin J. Treatment of trichomoniasis in pregnancy and preterm birth: an observational study. J Womens Health (Larchmt). 2009 Apr;18(4):493-7. doi: 10.1089/jwh.2008.0964[↩]
- Carter JE, Whithaus KC. Neonatal respiratory tract involvement by Trichomonas vaginalis: a case report and review of the literature. Am J Trop Med Hyg. 2008 Jan;78(1):17-9.[↩]
- Trintis J, Epie N, Boss R, Riedel S. Neonatal Trichomonas vaginalis infection: a case report and review of literature. Int J STD AIDS. 2010 Aug;21(8):606-7. doi: 10.1258/ijsa.2010.010174[↩]
- Masese LN, Graham SM, Gitau R, Peshu N, Jaoko W, Ndinya-Achola JO, Mandaliya K, Richardson BA, Overbaugh J, McClelland RS. A prospective study of vaginal trichomoniasis and HIV-1 shedding in women on antiretroviral therapy. BMC Infect Dis. 2011 Nov 3;11:307. doi: 10.1186/1471-2334-11-307[↩][↩]
- Kissinger P, Adamski A. Trichomoniasis and HIV interactions: a review. Sex Transm Infect. 2013 Sep;89(6):426-33. doi: 10.1136/sextrans-2012-051005[↩][↩]
- Susan Cu-Uvin, Ko Hyejin, Denise J. Jamieson, Joseph W. Hogan, Paula Schuman, Jean Anderson, S. Klein Robert, HIV Epidemiology Research Study (HERS) Group, Prevalence, Incidence, and Persistence or Recurrence of Trichomoniasis among Human Immunodeficiency Virus (HIV)–Positive Women and among HIV-Negative Women at High Risk for HIV Infection, Clinical Infectious Diseases, Volume 34, Issue 10, 15 May 2002, Pages 1406–1411, https://doi.org/10.1086/340264[↩]
- Petrin D, Delgaty K, Bhatt R, Garber G. Clinical and Microbiological Aspects of Trichomonas vaginalis. Clinical Microbiology Reviews. 1998;11(2):300-317. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC106834/[↩][↩]
- Signalling of Trichomonas vaginalis for amoeboid transformation and adhesion synthesis follows cytoadherence. Mol Microbiol. 1993 Jan;7(2):299-309. https://www.ncbi.nlm.nih.gov/pubmed/8446032[↩]
- Swartzendruber A, Sales JM, Brown JL, DiClemente RJ, Rose ES. Correlates of Incident Trichomonas vaginalis Infections Among African American Female Adolescents. Sexually transmitted diseases. 2014;41(4):240-245. doi:10.1097/OLQ.0000000000000094. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4313569/[↩]
- Guenthner PC, Secor WE, Dezzutti CS. Trichomonas vaginalis-induced epithelial monolayer disruption and human immunodeficiency virus type 1 (HIV-1) replication: implications for the sexual transmission of HIV-1, Infect Immun , 2005, vol. 73, pg. 4155-60[↩]
- Kingston MA, Bansal D, Carlin EM. ‘Shelf life’ of Trichomonas vaginalis. Int J STD AIDS. 2003 Jan;14(1):28-9. doi: 10.1258/095646203321043228[↩]
- Bachmann LH, Hobbs MM, Seña AC, Sobel JD, Schwebke JR, Krieger JN, McClelland RS, Workowski KA. Trichomonas vaginalis genital infections: progress and challenges. Clin Infect Dis. 2011 Dec;53 Suppl 3(Suppl 3):S160-72. doi: 10.1093/cid/cir705[↩]
- Van Gerwen OT, Muzny CA. Recent advances in the epidemiology, diagnosis, and management of Trichomonas vaginalis infection. F1000Res. 2019 Sep 20;8:F1000 Faculty Rev-1666. doi: 10.12688/f1000research.19972.1[↩][↩]
- Lobo TT, Feijo G, Carvalho SE, Costa PL, Chagas C, Xavier J, et al. A comparative evaluation of the Papanicolaou test for the diagnosis of trichomoniasis. Sex Transm Dis 2003;30(9):694-9.[↩]
- Nye MB, Schwebke JR, Body BA. Comparison of APTIMA Trichomonas vaginalis transcription-mediated amplification to wet mount microscopy, culture, and polymerase chain reaction for diagnosis of trichomoniasis in men and women. Am J Obstet Gynecol 2009;200(2):188 e1-7.[↩][↩]
- Centers for Disease Control and Prevention Public Health Image Library (Joe Miller, 1975).[↩]
- Beverly AL, Venglarik M, Cotton B, Schwebke JR. Viability of Trichomonas vaginalis in transport medium. J Clin Microbiol 1999;37(11):3749-50.[↩]
- Cosentino LA, Campbell T, Jett A, Macio I, Zamborsky T, Cranston RD, Hillier SL. Use of nucleic acid amplification testing for diagnosis of anorectal sexually transmitted infections. J Clin Microbiol. 2012 Jun;50(6):2005-8. doi: 10.1128/JCM.00185-12[↩]
- Francis SC, Kent CK, Klausner JD, Rauch L, Kohn R, Hardick A, Gaydos CA. Prevalence of rectal Trichomonas vaginalis and Mycoplasma genitalium in male patients at the San Francisco STD clinic, 2005-2006. Sex Transm Dis. 2008 Sep;35(9):797-800. doi: 10.1097/OLQ.0b013e318177ec39[↩]
- Trichomoniasis. https://www.cdc.gov/std/treatment-guidelines/trichomoniasis.htm[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- https://www.aphl.org/AboutAPHL/publications/Documents/ID_2013August_Advances-in-Laboratory-Detection-of-Trichomonas-vaginalis.pdf[↩]
- Hollman D, Coupey SM, Fox AS, Herold BC. Screening for Trichomonas vaginalis in high-risk adolescent females with a new transcription-mediated nucleic acid amplification test (NAAT): associations with ethnicity, symptoms, and prior and current STIs. J Pediatr Adolesc Gynecol. 2010 Oct;23(5):312-6. doi: 10.1016/j.jpag.2010.03.004[↩]
- Andrea SB, Chapin KC. Comparison of Aptima Trichomonas vaginalis transcription-mediated amplification assay and BD affirm VPIII for detection of T. vaginalis in symptomatic women: performance parameters and epidemiological implications. J Clin Microbiol. 2011 Mar;49(3):866-9. doi: 10.1128/JCM.02367-10[↩]
- Van Der Pol B, Williams JA, Taylor SN, Cammarata CL, Rivers CA, Body BA, Nye M, Fuller D, Schwebke JR, Barnes M, Gaydos CA. Detection of Trichomonas vaginalis DNA by use of self-obtained vaginal swabs with the BD ProbeTec Qx assay on the BD Viper system. J Clin Microbiol. 2014 Mar;52(3):885-9. doi: 10.1128/JCM.02966-13[↩]
- Schwebke JR, Gaydos CA, Davis T, Marrazzo J, Furgerson D, Taylor SN, Smith B, Bachmann LH, Ackerman R, Spurrell T, Ferris D, Burnham CA, Reno H, Lebed J, Eisenberg D, Kerndt P, Philip S, Jordan J, Quigley N. Clinical Evaluation of the Cepheid Xpert TV Assay for Detection of Trichomonas vaginalis with Prospectively Collected Specimens from Men and Women. J Clin Microbiol. 2018 Jan 24;56(2):e01091-17. doi: 10.1128/JCM.01091-17[↩][↩]
- Gaydos CA, Beqaj S, Schwebke JR, Lebed J, Smith B, Davis TE, Fife KH, Nyirjesy P, Spurrell T, Furgerson D, Coleman J, Paradis S, Cooper CK. Clinical Validation of a Test for the Diagnosis of Vaginitis. Obstet Gynecol. 2017 Jul;130(1):181-189. doi: 10.1097/AOG.0000000000002090[↩][↩]
- Van Der Pol B, Torres-Chavolla E, Kodsi S, Cooper CK, Davis TE, Fife KH, Taylor SN, Augenbraun MH, Gaydos CA. Clinical Performance of the BD CTGCTV2 Assay for the BD MAX System for Detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis Infections. Sex Transm Dis. 2021 Feb 1;48(2):134-140. doi: 10.1097/OLQ.0000000000001280[↩]
- Van Der Pol B. A profile of the cobas® TV/ MG test for the detection of Trichomonas vaginalis and Mycoplasma genitalium. Expert Rev Mol Diagn. 2020 Apr;20(4):381-386. doi: 10.1080/14737159.2020.1714440[↩][↩]
- Van Der Pol B, Rao A, Nye MB, Chavoustie S, Ermel A, Kaplan C, Eisenberg D, Chan PA, Mena L, Pacheco S, Waites KB, Xiao L, Krishnamurthy S, Mohan R, Bertuzis R, McGowin CL, Arcenas R, Marlowe EM, Taylor SN. Trichomonas vaginalis Detection in Urogenital Specimens from Symptomatic and Asymptomatic Men and Women by Use of the cobas TV/MG Test. J Clin Microbiol. 2021 Sep 20;59(10):e0026421. doi: 10.1128/JCM.00264-21[↩]
- Gaydos CA, Manabe YC, Melendez JH. A Narrative Review of Where We Are With Point-of-Care Sexually Transmitted Infection Testing in the United States. Sex Transm Dis. 2021 Aug 1;48(8S):S71-S77. doi: 10.1097/OLQ.0000000000001457[↩]
- Sheele JM, Crandall CJ, Arko BL, Vallabhaneni M, Dunn CT, Chang BF, Fann P, Bigach M. The OSOM® Trichomonas Test is unable to accurately diagnose Trichomonas vaginalis from urine in men. Am J Emerg Med. 2019 May;37(5):1002-1003. doi: 10.1016/j.ajem.2018.10.022[↩]
- Gaydos CA, Schwebke J, Dombrowski J, Marrazzo J, Coleman J, Silver B, Barnes M, Crane L, Fine P. Clinical performance of the Solana® Point-of-Care Trichomonas Assay from clinician-collected vaginal swabs and urine specimens from symptomatic and asymptomatic women. Expert Rev Mol Diagn. 2017 Mar;17(3):303-306. doi: 10.1080/14737159.2017.1282823[↩]
- Morris SR, Bristow CC, Wierzbicki MR, Sarno M, Asbel L, French A, Gaydos CA, Hazan L, Mena L, Madhivanan P, Philip S, Schwartz S, Brown C, Styers D, Waymer T, Klausner JD. Performance of a single-use, rapid, point-of-care PCR device for the detection of Neisseria gonorrhoeae, Chlamydia trachomatis, and Trichomonas vaginalis: a cross-sectional study. Lancet Infect Dis. 2021 May;21(5):668-676. doi: 10.1016/S1473-3099(20)30734-9[↩][↩]
- Trichomoniasis. 2015 Sexually Transmitted Diseases Treatment Guidelines. https://www.cdc.gov/std/tg2015/trichomoniasis.htm[↩]
- Spence MR, Harwell TS, Davies MC, et al. The minimum single oral metronidazole dose for treating trichomoniasis: a randomized, blinded study. Obstet Gynecol 1997;89(5 Pt 1):699–703.[↩][↩]
- Prasertsawat PO, Jetsawangsri T. Split-dose metronidazole or single-dose tinidazole for the treatment of vaginal trichomoniasis. Sex Transm Dis 1992;19:295–7.[↩]
- Forna F, Gulmezoglu AM. Interventions for treating trichomoniasis in women. Cochrane Database Syst Rev 2003;2:CD000218.[↩]
- Kirkcaldy RD, Augostini P, Asbel LE, Bernstein KT, Kerani RP, Mettenbrink CJ, Pathela P, Schwebke JR, Secor WE, Workowski KA, Davis D, Braxton J, Weinstock HS. Trichomonas vaginalis antimicrobial drug resistance in 6 US cities, STD Surveillance Network, 2009-2010. Emerg Infect Dis. 2012 Jun;18(6):939-43. doi: 10.3201/eid1806.111590[↩]
- Schwebke JR, Barrientes FJ. Prevalence of Trichomonas vaginalis isolates with resistance to metronidazole and tinidazole. Antimicrob Agents Chemother. 2006 Dec;50(12):4209-10. doi: 10.1128/AAC.00814-06[↩]
- Peterman TA, Tian LH, Metcalf CA, et al. High incidence of new sexually transmitted infections in the year following a sexually transmitted infection: a case for rescreening. Ann Intern Med 2006;145:564–72.[↩]
- Williams JA, Van Der Pol B, Ofner S, et al. Time from treatment to negative PCR results for C. trachomatis, N. gonorrhoeae and T. vaginalis. National STD Prevention Conference; March 10-13, 2008, 2008; Chicago, IL.[↩]
- Schwebke JR, Desmond RA. A randomized controlled trial of partner notification methods for prevention of trichomoniasis in women. Sex Transm Dis 2010;37:392–6.[↩]
- Mann JR, McDermott S. Are maternal genitourinary infection and pre-eclampsia associated with ADHD in school-aged children? J Atten Disord 2011;15:667–73.[↩]
- Klebanoff MA, Carey JC, Hauth JC, Hillier SL, Nugent RP, Thom EA, Ernest JM, Heine RP, Wapner RJ, Trout W, Moawad A, Leveno KJ, Miodovnik M, Sibai BM, Van Dorsten JP, Dombrowski MP, O’Sullivan MJ, Varner M, Langer O, McNellis D, Roberts JM; National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection. N Engl J Med. 2001 Aug 16;345(7):487-93. doi: 10.1056/NEJMoa003329[↩][↩]
- Stringer E, Read JS, Hoffman I, et al. Treatment of trichomoniasis in pregnancy in sub-Saharan Africa does not appear to be associated with low birth weight or preterm birth. South African Medical Journal 2010;100:58–64.[↩]
- Trintis J, Epie N, Boss R, et al. Neonatal Trichomonas vaginalis infection: a case report and review of literature. International journal of STD and AIDS 2010;21:606–7.[↩]
- Briggs GC, Freeman RK, Yaffe SJ. Drugs in Pregnancy and Lactation, 9th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2011.[↩]
- Goldenberg RL, Mwatha A, Read JS, et al. The HPTN 024 Study: the efficacy of antibiotics to prevent chorioamnionitis and preterm birth. Am J Obstet Gynecol 2006;194:650–61.[↩]
- Erickson SH, Oppenheim GL, Smith GH. Metronidazole in breast milk. Obstet Gynecol 1981;57:48–50.[↩]
- Miller M, Liao Y, Wagner M, et al. HIV, the clustering of sexually transmitted infections, and sex risk among African American women who use drugs. Sex Transm Dis 2008;35:696–702.[↩]
- Moodley P, Wilkinson D, Connolly C, et al. Trichomonas vaginalis is associated with pelvic inflammatory disease in women infected with human immunodeficiency virus. Clin Infect Dis 2002;34:519–22.[↩]
- Anderson BL, Firnhaber C, Liu T, et al. Effect of trichomoniasis therapy on genital HIV viral burden among African women. Sex Transm Dis 2012;39:638–42.[↩]
- Kissinger P, Mena L, Levison J, et al. A randomized treatment trial: single versus 7-day dose of metronidazole for the treatment of Trichomonas vaginalis among HIV-infected women. J Acquir Immune Defic Syndr 2010;55:565–71.[↩]
- Kissinger P, Adamski A, Clark RA, Mena L, Levison J, Martin DH. Does Antiretroviral Therapy Interfere With the Treatment of Trichomonas vaginalis Among HIV+ Women? Sex Transm Dis. 2013 Jun;40(6):506-7. doi: 10.1097/OLQ.0b013e31829335fe[↩]
- Balkus JE, Richardson BA, Mochache V, Chohan V, Chan JD, Masese L, Shafi J, Marrazzo J, Farquhar C, McClelland RS. A prospective cohort study comparing the effect of single-dose 2 g metronidazole on Trichomonas vaginalis infection in HIV-seropositive versus HIV-seronegative women. Sex Transm Dis. 2013 Jun;40(6):499-505. doi: 10.1097/OLQ.0b013e31828fce34[↩]
- Kissinger P, Adamski A. Trichomoniasis and HIV interactions: a review. Sex Transm Infect 2013;89:426–33.[↩]
- Helms DJ, Mosure DJ, Secor WE, et al. Management of Trichomonas vaginalis in women with suspected metronidazole hypersensitivity. Am J Obstet Gynecol 2008;198:e371–7.[↩]





{kind=link}