
Contents
Stiff Person syndrome
Stiff-Person syndrome (SPS) is an extremely rare progressive neurological disorder with features of an autoimmune disease, that affects the nervous system, specifically the brain and spinal cord. Stiff-Person syndrome symptoms may include extreme muscle stiffness, rigidity and involuntary painful spasms in the trunk and limbs, severely impairing mobility. Stiff-Person syndrome is characterized by progressive rigidity and muscle spasms affecting the axial and limb muscles 1. Persistent muscle spasms affecting the axial and limb muscles can lead to abnormal posturing of the spine, such as being hunched over. Stiff-Person syndrome patients typically present with muscle spasms and stiffness, concurrently in the thoracolumbar paraspinal and abdominal muscles, resulting in difficulty turning and bending (see Figure 1). This results in a typical clinical picture of stiff-legged gait with exaggerated lumbar hyperlordosis. When stiffness is severe, the patients’ walking resembles a “statue” or exhibits a “freezing-like” appearance; some patients mention that they walk like a “tin-man” with hyperlordotic posture 2, 3. Spasms are frequent in the trunk or any arms or legs and can be painful 4. Spasms can generate enough force to fracture bone. Spasms can be also seen in the face and if limited exclusively to the facial muscles, often referred to as “stiff-face syndrome” 4. People with stiff person syndrome often have heightened sensitivity to noise, sudden movements, and emotional distress. Muscle spasms and stiffness can be precipitated by unexpected stimuli, including sounds, like a phone ring or a siren, sudden touches or conditions triggering anxiety and emotional upset which, when severe, are misdiagnosed as a primary anxiety disorder 4. The episodic nature of spasms, often emphasized by the patients, is important to acknowledge because at times it may not be obvious when a patient is first examined but may become apparent even 30 minutes later as the patient becomes more anxious even while waiting in the examining room 4. Task-specific phobias, especially fear of walking, crossing a street or a green light and fear of falling, are quite common 2, 5, 6. In some cases, these or similar events can cause severe and continuous painful spasms, along with stiffness in the thoracic muscles with breathing difficulties, tachycardia and hyperhidrosis, a condition we have labeled “status spasticus,” requiring emergency admission for intravenous diazepam 2, 5, 6. Electrophysiological studies reveal continuous activity of motor unit firing at rest, confirming that stiffness is caused by co-contractions of agonists and antagonists muscles 2, 7, 8.
The exact incidence and prevalence of stiff person syndrome is unknown, although one estimate places the incidence at approximately 1 in 1,000,000 individuals in the general population 9. The distribution of stiff person syndrome between men and women indicates a female predominance. Stiff person syndrome affects twice as many women as men above the age of 20 years 10. Stiff person syndrome usually becomes apparent sometime between 30-60 years of age. However, stiff person syndrome has been reported to occur in children and older adults as well.
Stiff-Person syndrome was first described in the medical literature by doctors Moersch and Woltman in 1956 as stiff-man syndrome 11. The disorder is now known as Stiff-Person syndrome to reflect that the disorder affects individuals of any age and both genders. Onset is usually in the third to fifth decades of life. Investigations reveal a characteristic abnormality on electromyography (EMG) recordings with continuous motor unit activity of the paraspinal axial muscles.
Stiff-Person syndrome can be classified according to the clinical presentation into 12:
- Classic Stiff-Person syndrome
- Classic Stiff-Person syndrome is the most common clinical form, present in 70 to 80% of Stiff-Person syndrome patients 13. It is associated with anti-glutamic acid decarboxylase (anti-GAD) antibodies 14. Classic Stiff-Person syndrome has an insidious onset with gradual worsening over few months and often leads to permanent disability and, in some cases, death. Stiff-Person syndrome may coexist with other autoimmune disorders, including type 1 diabetes, autoimmune thyroid disease, pernicious anemia, celiac disease, and vitiligo 15. Classic Stiff-Person syndrome usually starts with rigidity and stiffness of the trunk muscles, specifically in the thoracolumbar region, due to continuous contraction of both abdominal and paraspinal muscles. Patients describe difficulties bending and turning, feeling that they walk like a “tin-man.” Later, the rigidity spreads to proximal upper and lower extremities 2. Eventually, it leads to multiple chronic orthopedic abnormalities such as increased lumbar lordosis, joint deformities, and abnormal posturing, which results in a “statue-like” appearance and is accompanied by gait disturbances and multiple falls. In addition, patients develop painful generalized muscle spasms and exaggerated startle responses precipitated by unexpected tactile, visual, or acoustic stimuli and strong emotions. Patients often develop depression, task-specific phobias, fear of open spaces, anticipatory anxiety due to triggered spasms, and pathological startling 16. Due to common psychiatric comorbidities, Stiff-Person syndrome is being misdiagnosed for a functional neurological disorder or a primary psychiatric condition. Patients usually have diurnal fluctuations of symptoms, worse with physical and emotional stress, cold weather, and infection. Distal and facial muscles are spared until later in the disease course. The frequency and duration of painful spasms vary. In some cases, severe spasms can last for hours (“status spasticus”), often requiring an emergency room visit for treatment intravenous muscle relaxants. In rare cases, respiratory muscles can be involved17.
- Partial Stiff-Person syndrome variants
- Several clinical variants of Stiff-Person syndrome have been described and include Stiff-Limb syndrome, Jerky Stiff-Person syndrome, cerebellar variant Stiff-Person syndrome, Stiff-Person syndrome with epilepsy, and dystonia 12, 15. Stiff-Limb syndrome presents with isolated limb spasms and mostly spared trunk muscles. Abnormal posturing of the distal limb can resemble dystonia. Stiffness can eventually involve other muscles, but it remains most severe in one limb. In Stiff-Trunk syndrome, spasms involve only axial musculature, sparing extremities. Rarely extraocular abnormalities with oscillopsia (a visual disturbance in which objects in the visual field appear to jump, jiggle, or vibrate when they’re actually still), opsoclonus, and nystagmus were reported 17. Patients with cerebellar variant Stiff-Person syndrome (Stiff-Person syndrome-Cer) present with dysmetria (inability to control the distance, speed, and range of motion necessary to perform smoothly coordinated movements), gait ataxia, and nystagmus superimposed on stiffness 18.
- Stiff-Person syndrome plus Progressive Encephalomyelitis with Rigidity and Myoclonus (PERM)
- Progressive Encephalomyelitis with Rigidity and Myoclonus (PERM) was first described in 1956, is known as Stiff-Person syndrome-plus syndrome. Progressive Encephalomyelitis with Rigidity and Myoclonus (PERM) is a more severe variant of Stiff-Person syndrome and it is characterized by relapsing-remitting course and more extensive involvement of different parts of the central nervous system (brain and spinal cord), including the brainstem. This results in decreased consciousness or altered mentation, extraocular muscle dysfunction, ataxia, and autonomic failure 19, 16. Patients have the rigidity of axial and limb muscles, diffuse myoclonus in addition to prominent autonomic instability 15.
- Paraneoplastic Stiff-Person syndrome
- The paraneoplastic Stiff-Person syndrome is associated with breast cancer, colon cancer, thyroid cancer, lung cancer, Hodgkin lymphoma and non-Hodgkin lymphoma and tends to clinically manifest before cancer itself 14. Paraneoplastic Stiff-Person syndrome was described by some authors that paraneoplastic Stiff-Person syndrome demonstrates more significant stiffness in the neck and upper extremities. These patients usually show a faster response to therapy and significant clinical improvement once their malignancy is removed 19.
In a longitudinal study of 57 anti-GAD-positive Stiff-Person syndrome patients 2, which represents the largest clinical series of personally examined patients every 6 months for a two-year period to assess disease progression, the most common initial symptom was the insidious onset of proximal leg stiffness followed by rigidity in the lumbosacral paraspinals, thoracic and abdominal muscles. Axial muscle stiffness (truncal and proximal legs), lumbar hyperlordosis and impaired gait were first signs in 68% of these patients with 28% of them also having various degrees of facial muscle stiffness 20. About 15% of the patients with typical Stiff-Person syndrome symptomatology also had ataxia, dysarthria and dysphagia, overlapping with the cerebellar variant Stiff-Person syndrome, an important distinction because these patient subsets do not fully respond to immunotherapies 17. Exaggerated reaction to various external stimuli and “startle response” were present in all patients except two 2. Marked anxiety related to unprotected falls or in anticipation of physically challenging situations was seen in 52 of 57 patients; 21 patients experienced chronic anxiety combined with intermittently depressed mood 2. Simple phobias, such as fear of walking in open and crowded places, crossing a street or taking escalators, were reported by more than 10% of patients with several also having task-related phobias, such as fear of public speaking. Most patients had been misdiagnosed with conversion or functional disorder because their falls were attributed to avoidant behavior and heightened mental anticipation 2. Other common misdiagnoses were myelopathies, dystonias or Parkinsonism. Many patients reported muscle pain along with painful spasms and some had been on narcotics.
Stiff person syndrome is caused by increased muscle activity due to decreased inhibition of the central nervous system. It is thought to have an autoimmune component as in most cases antibodies against glutamic acid decarboxylase (GAD) are observed and is often associated with diabetes, as well as other autoimmune diseases such as thyroiditis, vitiligo, and pernicious anemia. Similarly, paraneoplastic stiff person syndrome is usually linked to anti-amphiphysin antibodies and anti-GAD and anti-Ri antibodies may also be present 21. Paraneoplastic stiff person syndrome is commonly associated with breast cancer but may also occur in patients with lung, renal, thyroid, colon cancer, malignant thymoma or lymphoma or Hodgkin’s disease.
Structural MRIs of brain and spine are usually normal. The exact cause of classic stiff person syndrome remains unknown but automimmune mechanisms are suspected to have a role. Antibodies to the enzyme glutamic acid decarboxylase (GAD), have been detected and other autoimmune disorders such as diabetes, pernicious anemia, and thyroiditis occur more frequently in patients with stiff person syndrome. 60-90% of classic stiff person syndrome patients have very high anti-GAD titres, (usually over 20 nmol/l). Another important association is that of stiff person syndrome with paraneoplastic syndromes. Mutations of the GLRA1 (glycine receptor) gene have also been identified to account for some cases of startle and limb stiffness.
Stiff person syndrome may be diagnosed after having various tests including blood tests (including a test showing elevated glutamic acid decarboxylase (GAD) antibodies), a lumbar puncture, and electromyography (EMG). Most patients with stiff person syndrome have antibodies directed against the glutamic acid decarboxylase (GAD antibodies), the rate-limiting enzyme for the production of the inhibitory neurotransmitter gamma-aminobutyric acid (GABA). Antibodies directed against GABAA receptor-associated protein (anti-GABARAP), and the glycine-α1 receptor can also be observed. Paraneoplastic stiff person syndrome is commonly associated with antiamphiphysin antibodies and breast cancer.
The diagnostic criteria for Stiff-Person Syndrome (SPS) include stiffness of the limbs and axial muscles, particularly abdominal and thoracolumbar paraspinals; superimposed painful spasms precipitated by emotional distress or unexpected tactile or auditory stimuli; and high (>1: 10,000 by ELISA) serum antiglutamic acid decarboxylase-65 (GAD-65) antibody titers in up to 80% of the patients 22, 4.
Stiff person syndrome treatment aims to control symptoms and improve mobility, and may involve benzodiazepines, muscle relaxants with GABAergic action, and/or immunosuppressive therapies that include plasmapheresis or intravenous immunoglobulin (IVIG) infusion. Detailed follow-up data from 53 sequentially studied patients have shown that without immunotherapy, Stiff-Person syndrome is a progressive disease leading to cumulative physical disability over time even with the use of antispasmodic medications such as baclofen, diazepam, and gabapentin 17. Among the immunotherapeutic agents, high-dose intravenous immunoglobulin (IVIg) is currently the preferred treatment for patients with Stiff-Person syndrome who do not achieve symptom control with muscle relaxants and benzodiazepines, based on a placebo-controlled randomized trial that had shown that high-dose intravenous immunoglobulin (IVIg) significantly improves stiffness, spasms, and gait, over a 3-month study period 23. Because Stiff-Person syndrome is a progressive disease, intravenous immunoglobulin (IVIg) is currently used as a chronic monthly treatment. This 2022 study 24 demonstrated that maintenance therapy with intravenous immunoglobulin (IVIG) continues to be effective over a median of 3.3 years in 67% of patients with typical Stiff-Person syndrome, improving daily functioning, gait, balance, painful spasms, posture, and facial expression with a demonstrable effect in decreasing stiffness, spasms and startle response. Although it’s an uncontrolled study due to disease rarity and the clinical ethics to give placebo over 2–3 years, this is a long-term study in a large group of patients with Stiff-Person syndrome seen over time by the same experienced clinicians that documents continued IVIg efficacy based on a combination of modified Rankin Scale scores, dependency tests, and objective clinical observations 24. The results complement the conclusions from the original short-term 3-month controlled study that the same investigators conducted 20 years ago with a much smaller number of enrolled patients 23.
While some people with stiff person syndrome may maintain reasonable levels of activity with treatment, the majority become disabled over time 25. No reliable predictor of the disease course has been identified. The prognosis for patients with Stiff-Person syndrome depends on multiple factors, including clinical presentation, the duration of symptoms, co-existing neoplastic process, and a response to therapy 13. It is critical to timely initiate therapy to prevent or lessen progression and avoid long-term complications 13. Most of Stiff-Person syndrome patients improve with medications, however fluctuations precipitated by physical and emotional stressors still occur. Despite the availability of multiple treatment options, some patients with Stiff-Person syndrome show disease progression over time, leading to permanent orthopedic abnormalities, inability to walk, and disability 19, 16. In one longitudinal study, only 19% of patients could work after 4 years of follow-up 17. Patients report markedly reduced quality of life due to physical and social limitations 13.
Figure 1. Stiff person syndrome
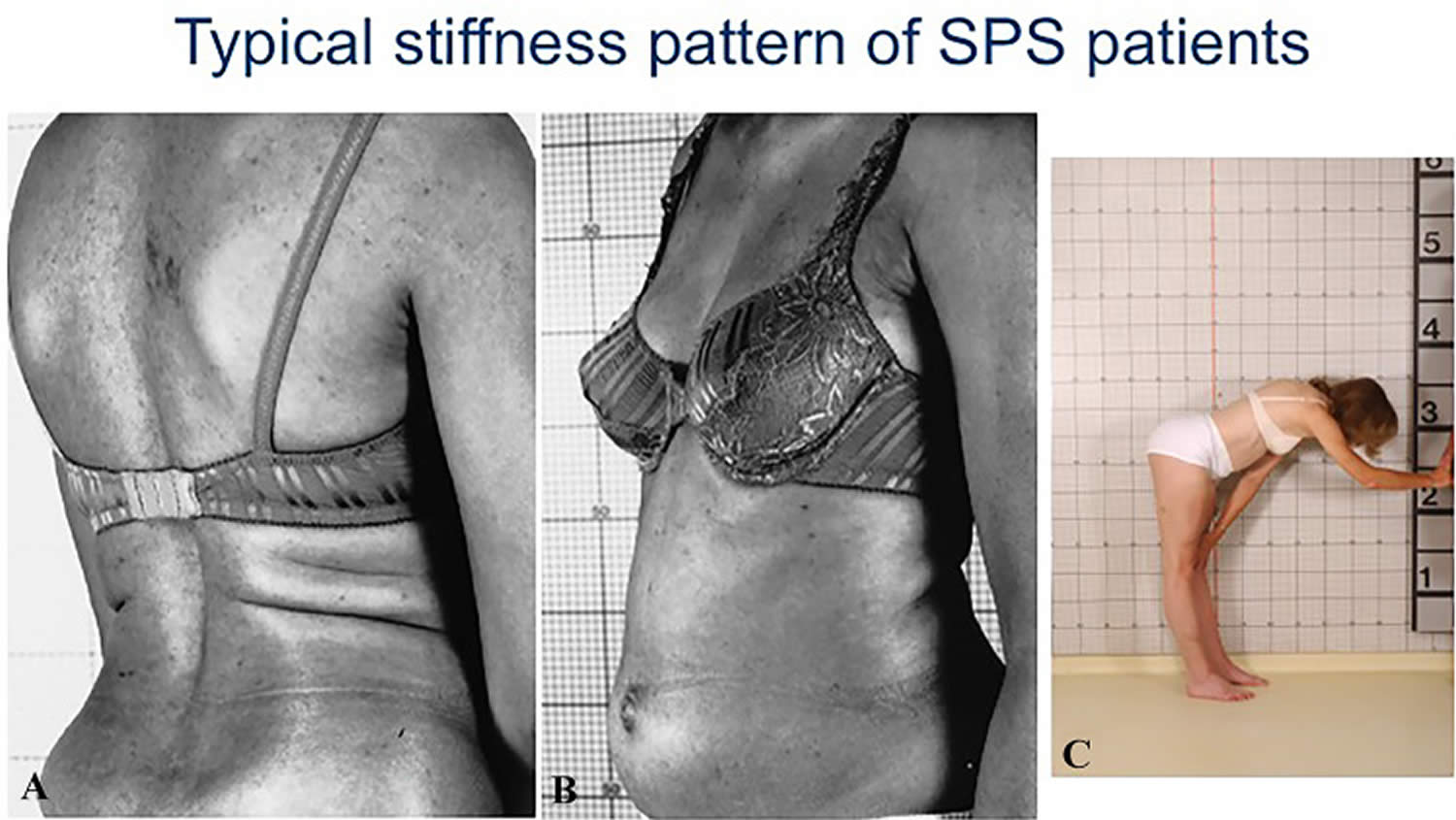
Footnotes: Typical stiffness pattern in Stiff-Person Syndrome (SPS) patients. (A-C) Concurrent stiffness of thoracolumbar (A) and abdominal muscles (B) due to lack of reciprocal inhibition in a patient with typical Stiff-Person Syndrome. Another patient (C) shows significant stiffness with inability to bend forwards.
[Source 22, 4 ]Stiff person syndrome causes
Scientists don’t yet understand what causes stiff person syndrome, but research indicates that it is the result of an autoimmune response gone awry in the brain and spinal cord. Autoimmune disorders are caused when the body’s natural defenses (e.g., antibodies) against “foreign” or invading organisms begin to attack healthy tissue for unknown reasons. Stiff person syndrome is frequently associated with other autoimmune diseases such as diabetes, thyroiditis, vitiligo, and pernicious anemia.
Up to 80% of Stiff-Person syndrome patients have antibodies to glutamic acid decarboxylase (GAD), a protein in inhibitory nerve cells that is involved in the creation (synthesis) of the main inhibitory neurotransmitter called gamma-aminobutyric acid (GABA) 5. GABA helps control muscle movement and prevent hyperexcitibility within the brain and spine. The symptoms of Stiff-Person syndrome may develop when the immune system mistakenly attacks certain nerve cells (neurons) that produce glutamic acid decarboxylase (GAD) leading to a deficiency of GABA in the body 26, 27. Since glutamic acid decarboxylase (GAD) is also expressed in pancreatic cells and patients with type-1 diabetes have low-titer anti-GAD antibodies, up to 35% of Stiff-Person syndrome patients may also have type-1 diabetes along with and other autoimmune diseases, such as vitiligo, pernicious anemia, celiac disease or thyroiditis 28, 29, 30.
There are classically two isoforms of anti-glutamic acid decarboxylase (GAD): GAD65 and GAD67. Most patients have antibodies to glutamic acid decarboxylase 65 (GAD65) enzyme, which has an unclear role in the disease pathogenesis 31. In some studies, up to 20% of patients with Stiff-Person Syndrome did not have these autoantibodies 32. Anti-GAD67 is associated to Stiff-Person Syndrome, diabetes mellitus, cerebellar ataxia, and limbic encephalitis 33.
The exact role that deficiency of glutamic acid decarboxylase (GAD) plays in the development of stiff person syndrome is not fully understood. Antibodies to GAD-65 are associated with several other disorders including diabetes. In fact, GAD-65 is the most common antibody produced by people with autoimmune diabetes and many people have these antibodies in that context. In some individuals with stiff person syndrome no antibodies to glutamic acid decarboxylase (GAD) are detectable. The cause of stiff person syndrome in these individuals may ultimately be unknown (idiopathic), but testing for other causes (e.g. amphiphysin antibodies) is usually appropriate. More research is necessary to determine the exact, underlying mechanisms that ultimately cause stiff person syndrome and the exact role that anti-glutamic acid decarboxylase (GAD) antibodies play in the development and progression of the disorder.
Less commonly, individuals with Stiff-Person syndrome will have antibodies to amphiphysin (anti-amphiphysin), a protein involved in the transmission of signals from one nerve cell to another. The paraneoplastic form accounts for 5% to 10% of all cases and is characterized by the presence of antibodies to amphiphysin and less frequently to gephyrin. The most common malignancy associated with paraneoplastic variant includes breast adenocarcinoma followed by adenocarcinoma of the colon, small-cell lung carcinoma, malignancies of thymus and thyroid gland cancer and Hodgkin’s lymphoma 15.
Genetic predisposition has been determined by the presence of DQB1 and DRB1 MHC-II alleles which increase the risk of idiopathic and paraneoplastic variants of SPS 5.
Stiff-Person syndrome pathophysiology
The pathogenesis of Stiff-Person syndrome has been explained by B-cell-mediated autoimmune inflammation that affects different components of inhibitory GABAergic neurons and their synapses 13. Production of autoantibodies against antigens involved in GABA synthesis and release within the central nervous system results in a dysfunction of major inhibitory pathways leading to impaired truncal and axial muscles’ impaired relaxation due to hyperexcitability the motor cortex. Glutamic acid decarboxylase (GAD) is an intracellular enzyme that transforms glutamate into GABA and is a primary target and the most common antigen identified in classic Stiff-Person syndrome 34. GAD exists in 2 isoforms: GAD67 and GAD65. The baseline production of GABA is regulated by GAD67, while the second isoform provides additional GABA when there is an increased demand 19, 5.
Primarily, the production of anti-GAD65 antibodies is a hallmark of a pathological process in classic Stiff-Person syndrome and is found in 70-80% of cases. In addition to classic Stiff-Person syndrome, anti-GAD antibodies have been associated with other autoimmune neurological disorders, including limbic encephalitis, autoimmune epilepsy, cerebellar ataxia, myoclonus, and nystagmus. They now comprise GAD antibody-spectrum disorders (GAD-SD) 35. It is currently unclear if different epitope binding patterns can cause diverse clinical presentations of GAD antibody-spectrum disorders. Low titers of anti-GAD antibodies also are seen in patients with type 1 diabetes, and up to 30% of patients with GAD antibody-spectrum disorders, including Stiff-Person syndrome, have type-1 diabetes. However, high titers of anti-GAD antibodies are seen only in GAD antibody-spectrum disorders 2.
Additional antigens described with Stiff-Person syndrome include GABA-A Receptor Associated Protein (GABARAP), dipeptidyl-peptidase-like protein-6 (DPPX) as well as glycine receptor (GlyR), which is associated with Progressive Encephalomyelitis with Rigidity and Myoclonus (PERM) 36.
A paraneoplastic variant of Stiff-Person syndrome is associated with antibodies against amphiphysin or gephyrin. Amphiphysin is an intracellular presynaptic protein involved in the endocytosis of the vesicle membrane and regulates the expression of GABA receptors at the axon membrane. It is demonstrated that antibodies against amphiphysin can decrease the amount of GABA receptors by reducing the endocytosis of the GABA-containing vesicles. Therefore, this diminishes the presynaptic vesicle pool and leads to impaired GABA transmission 37.
Figure 2. Stiff-Person syndrome pathophysiology
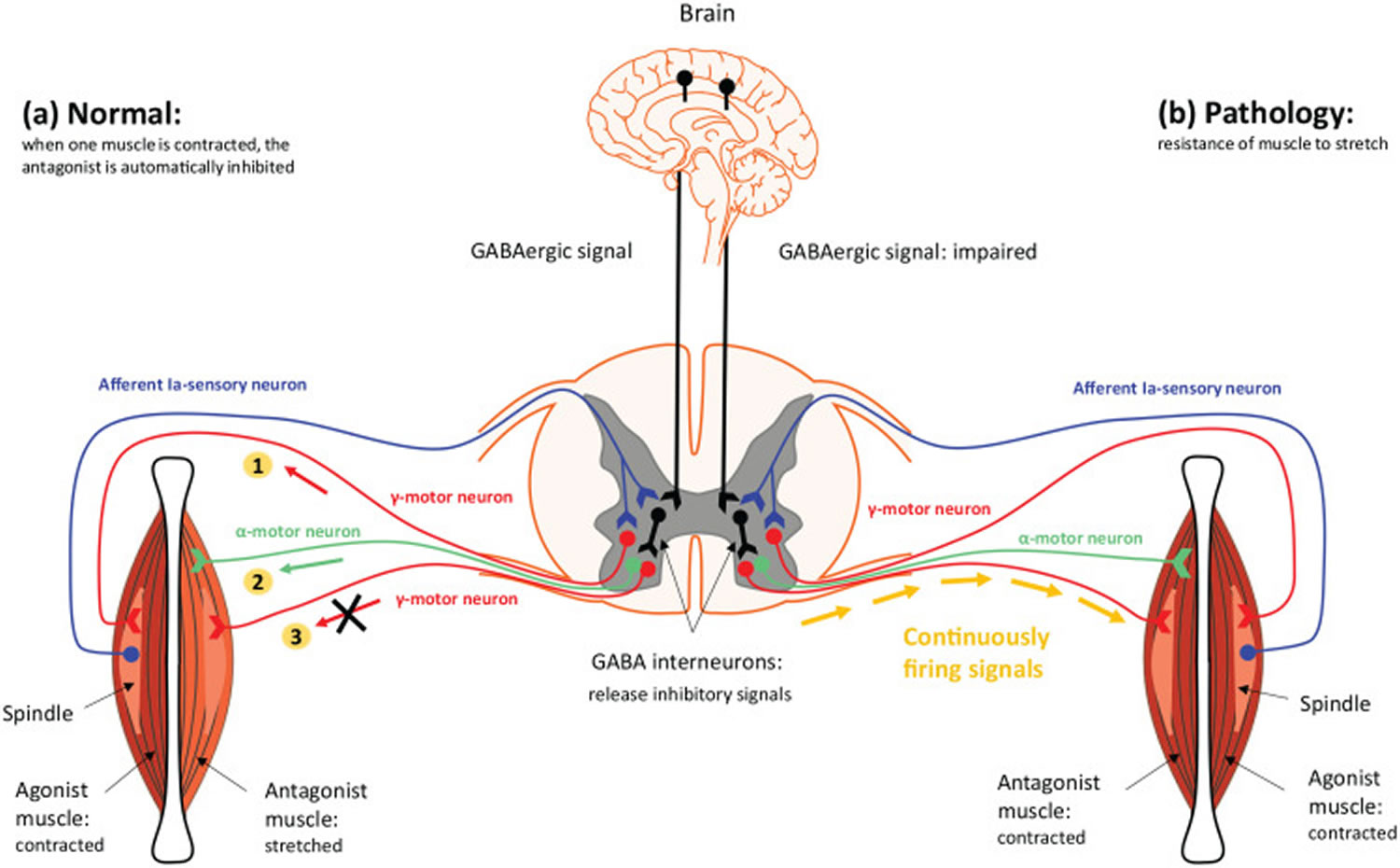
Footnotes: (a) Normal function: when one muscle is contracted, its antagonist is automatically inhibited. Afferent 1a sensory neuron fires, bringing information to the spinal cord, and stimulates the gamma neurons. Then, the γ-motor neuron (gamma-motor neurons) of the agonist muscle send signals to the spindle to contract [1], while the gamma motor neurons (γ-motor neurons) of the antagonist muscle do not discharge (X) due to inhibition of GABA interneuron [3]. As a result, the α-motor neuron (alpha-motor neuron) of antagonist stretches (relaxes) the muscle [2] (interneuron: releases inhibitory mediators). (b) Pathology: if the motor neuron is continuously firing signals, while there is no inhibition of the GABA interneuron to the antagonist muscle, the whole muscle will continuously be stimulated and will become hypertonic (spastic), without the ability to stretch (relax), due to concurrent contraction of the agonist and the antagonist muscles, as happens in stiff person syndrome that presents with stiffness and hyperexcitability.
[Source 2 ]Stiff-Person syndrome antibodies
Apart from the antibodies against glutamic acid decarboxylase (GAD), other antibodies may also be positive in patients with Stiff-Person syndrome (SPS) and hyperexcitability syndromes. Antibodies against GABA-A receptor-associated protein in about 70% of the patients, but these findings have not been replicated 20. Another autoantibody found in 10–15% of SPS patients is against glycine-a1 receptor (GlyR), a key inhibitory neurotransmitter. Anti-GlyRa1 antibodies, first described in progressive encephalomyelitis with rigidity and myoclonus (PERM), may be pathogenic as they recognize extracellular epitopes of the receptor expressed in the spinal cord, brainstem and cerebellum 38, 39. Low-titer autoantibodies against GABA-A receptor are also found in 10% of patients with SPS, cerebellar ataxia, epilepsy or encephalitis 40. In about 5% of patients, SPS can be paraneoplastic, associated with antibodies against amphiphysin 41, 42 and in a single case against gephyrin 43. Apart from glycine-a1 receptor (GlyR) all targeted antigens are predominantly cytoplasmic and it remains to be determined whether they can transiently exhibit an extracellular domain during neurotransmission and exocytosis that may account for pathogenicity 6.
Figure 3. Stiff-Person syndrome antibodies
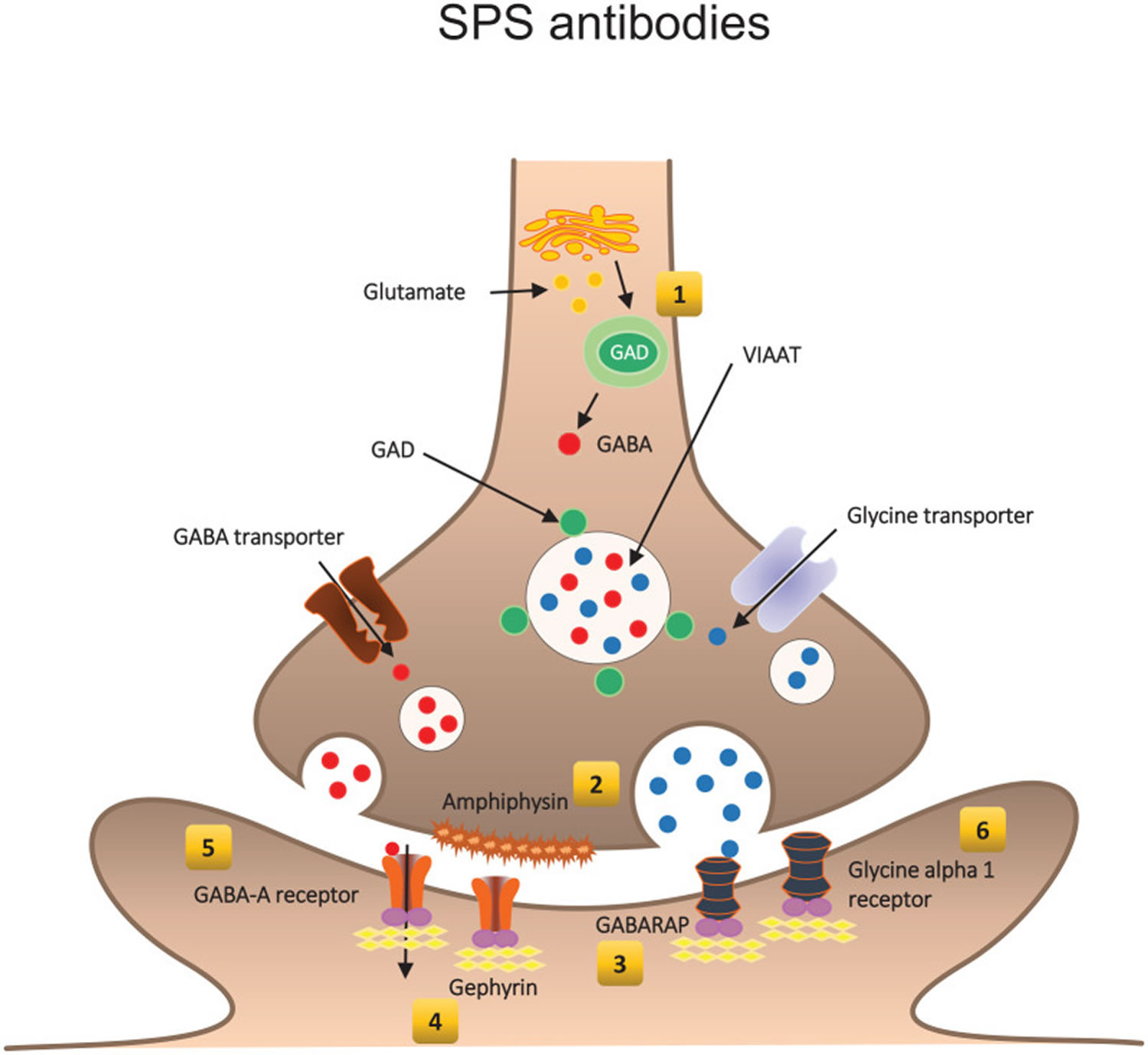
Footnotes: The pre-synaptic antigens are GAD (1), the enzyme that synthesizes GABA, the main inhibitory neurotransmitter, and amphiphysin (2), a synaptic vesicle protein responsible for endocytosis of plasma membranes following GABA release. Post-synaptically, the main targets are GABA-A Receptor Associated Protein (GABARAP) (3), gephyrin (4), a tubulin-binding protein needed for clustering both GABA-A (5) and glycine receptors (6). The most common antigen in stiff person syndrome is GAD followed by glycine receptor (vesicular inhibitory amino acid transporter; VIAAT).
Abbreviations: GABA = gamma-aminobutyric acid; GAD = glutamic acid decarboxylase; GABA-A Receptor Associated Protein = GABARAP
[Source 2 ]Stiff person syndrome symptoms
Stiff-Person syndrome is characterized by fluctuating muscle rigidity in the trunk and limbs and a heightened sensitivity to stimuli such as noise, touch, and emotional distress, which can set off muscle spasms. Abnormal postures, often hunched over and stiffened, are characteristic of the disorder. People with stiff person syndrome can be too disabled to walk or move, or they are afraid to leave the house because street noises, such as the sound of a horn, can trigger spasms and falls.
The characteristic findings associated with Stiff-Person syndrome are progressive, fluctuating muscular rigidity that occurs along with muscle spasms. The severity and progression of stiff person syndrome can vary from one person to another. The symptoms usually develop over a period of months and may remain stable for many years or slowly worsen. In some people, symptoms can be stabilized through medication. Affected individuals should talk to their physician and medical team about their specific case, associated symptoms and overall prognosis.
Signs and symptoms in 57 patients with Stiff-Person syndrome 17:
Increased tone in:
- Axial (diffuse paraspinal and proximal limb muscles) 68%
- Combined lumbosacral paraspinal and proximal leg muscles 58%
- Spasms 88%
- Proximal leg muscles 30%
- Face 28%
- Lumbosacral paraspinal muscles 28%
- Thoracic paraspinal and abdominal wall muscles 24%
- Cervical paraspinal and shoulder girdle muscles 19%
- Asymmetry with one limb predominant (stiff-limb) 10%
- Distal limb stiffness 7%
Other associated symptoms:
- Ocular symptoms 23%
- Cerebellar symptoms and signs 12%
Functional impairment resulting in the following:
- Stiff or impaired gait 94%
- Startle response 96%
- Anxiety and task-specific phobias 91%
- Hyperlordosis 84%
- Inability to work 84%
- Need for cane 45%
- Need for walker 24%
- Shortness of breath 19%
- Need for wheelchair 15%
- Depressed mood 5%
In many cases, stiff person syndrome begins slowly over several months or a few years. Affected individuals may initially experience aching discomfort, stiffness, or pain, especially in the lower back or legs (predominantly classic type). Early on, stiffness may come and go, but it gradually becomes fixed. The shoulders, neck, and hips may also be affected. As the disease progresses, stiffness of the leg muscles develops, and is often more pronounced on one side than the other (asymmetrical). This leads to a slow, stiff manner of walking. As stiffness increases, affected individuals may develop a hunched or slouched posture due to outward curving of the upper spine (kyphosis) or an arched back due to inward curving of the lower spine (hyperlordosis). In some individuals, stiffness may progress to involve the arms or face.
In addition to muscular rigidity/stiffness, individuals with stiff person syndrome also develop muscle spasms, which may occur for no apparent reason (spontaneously) or in response to various triggering events (i.e., stimuli). Spasms can be triggered by unexpected or loud noises, minor physical contact, cold environments, stress or situations that cause a heightened emotional response. Muscle spasms are often very painful and usually worsen existing stiffness. The spasms may involve the entire body or only a specific region. The legs are often involved, which may lead to falls. Spasms of abdominal muscles may lead to individuals feeling full faster than normal (early satiety) leading to unintended weight loss. Spasms involving the chest and respiratory muscles can be serious, potentially requiring emergency medical treatment with ventilatory support. Spasms may last several minutes, but occasionally last for hours. Sudden withdrawal of medication in individuals with stiff person syndrome may result in a life-threatening situation with overwhelmingly severe muscle spasms. Sleep usually suppresses the frequency of contractions.
In some cases, stiff person syndrome becomes severe enough to affect an individual’s ability to perform daily activities and routines. Some individuals may need to use an assist device such as a cane, walker or wheelchair. Some affected individuals experience uncontrollable anxiety when they need to cross large, open areas unassisted (agoraphobia) and become reluctant to go outside. If left untreated, stiff person syndrome can potentially progress to cause significant disability or life-threatening complications such as respiratory compromise.
Stiff person syndrome may be associated with other autoimmune disorders more frequently than would be regularly expected to occur in the general population. The most common associated condition is diabetes. Less commonly, affected individuals may also develop inflammation of the thyroid (thyroiditis), pernicious anemia and vitiligo. Pernicious anemia is characterized by low levels of red bloods cells due to the body’s inability to absorb vitamin B12 from the gastrointestinal tract. Vitiligo is a skin condition in which loss of color (pigmentation) of areas of skin results in the development of abnormal white patches. Clinical reports indicate that individuals with stiff person syndrome also have an increased incidence of epilepsy.
Several variants of stiff person syndrome have been reported in the medical literature suggesting that Stiff-Person syndrome represents a spectrum of disease ranging from the involvement of one specific, localized area to widespread involvement. These variants include Stiff-Limb syndrome, Jerking Stiff-Person syndrome, Progressive Encephalomyelitis with Rigidity and Myoclonus (PERM) and paraneoplastic-related Stiff-Person syndrome. These variants are sometimes collectively referred to as “stiff-person plus syndromes”.
Stiff-limb syndrome is characterized by the localized involvement of one limb, usually a leg. The stiffness and muscle spasms are extremely similar to those found in classic stiff-person syndrome. Stiff-limb syndrome may progress to eventually affect both legs and may cause difficulty walking. Some individuals may eventually develop classic stiff-person syndrome or variant stiff person syndrome. When stiff person syndrome affects only one specific area of the body, it may also be referred to as focal or partial stiff-person syndrome.
Jerking stiff-person syndrome is characterized by muscles stiffness and spasms usually affecting the legs. Affected individuals also develop involvement of the brainstem, which can cause myoclonus. Myoclonus is a general term used to describe the sudden, involuntary jerking of a muscle or group of muscles caused by muscle contractions (positive myoclonus) or muscle relaxation (negative myoclonus). The twitching or jerking of muscles cannot be controlled by the person experiencing it. Only a handful of cases of jerking stiff-person syndrome have been described in the medical literature.
Progressive encephalomyelitis with rigidity and myoclonus (PERM) is characterized by stiffness and painful muscles that are similar to those seen in individuals with classic stiff-person syndrome. Progressive encephalomyelitis with rigidity and myoclonus (PERM) is more rapidly progressive than other forms of stiff person syndrome; onset of symptoms usually occurs over several weeks. Stiffness and spasms may occur along with, before or after the development of other symptoms including vertigo, a lack of coordination of voluntary muscles (ataxia), and difficulty speaking (dysarthria). In some cases, the cranial nerves may also become involved causing paralysis of certain eye muscles (ophthalmoplegia), rapid, involuntary eye movements (nystagmus), difficulty swallowing (dysphagia), and hearing loss. Progressive encephalomyelitis with rigidity and myoclonus (PERM) is considered a distinct disorder from classic stiff person syndrome and some feel that it is a distinct condition all together. There is no evidence that stiff person syndrome will inevitably evolve into progressive encephalomyelitis with rigidity and myoclonus (PERM).
Paraneoplastic-related stiff-person syndrome is a rare disorder that affects the nervous system in some individuals with cancer, especially individuals with cancer of the lungs or breast. The disorder is characterized by stiffness and rigidity, along with painful spasms. Symptoms usually begin in the muscles of the lower back and legs, although some individuals experience neck and upper torso symptoms first. The disorder may grow progressively worse eventually affecting the arms and other parts of the body. Painful muscle spasms can be worsened or triggered by a variety of events including anxiety, loud or unexpected noises or light physical contact. Paraneoplastic stiff-person syndrome is thought to be immune-mediated and is typically associated with a different auto-antibody (called anti-amphiphysin) than is found in individuals with classic stiff-person syndrome. This antibody is usually found in the blood and spinal fluid of affected individuals.
Stiff baby syndrome
The clinical presentation of stiff baby syndrome is somewhat different. Babies and young children are less rigid between attacks. Involvement of the distal muscles is often more evident, particularly during paroxysms. Opisthotonic posturing is more prominent. Startle or stress is a frequent and prominent precipitant of the attacks.
Its clinical characteristics are within a broader descriptive category known as hyperekplexia. Differentiation of a particular case as stiff baby syndrome sometimes is considered dependent upon the presence of anti-GAD antibodies. In addition, stiff baby syndrome may be more persistent or more frequently recurrent, although this is not invariable.
Diagnosis can also be more complex because other etiologies (eg, other neuromuscular disorders, seizures, withdrawal or intoxication from maternal drug abuse) need to be excluded.
Associated diseases
- Diabetes mellitus: Although different epitopes for the GAD antibodies in diabetes have been identified, stiff person syndrome and diabetes have demonstrated comorbidity. This comorbidity occurs in association with a finding of positive GAD antibodies. Early distal involvement and involvement of a single limb is more frequent in patients with diabetes mellitus. Stiff person syndrome has also been associated with diabetes mellitus and ICA 105 pancreatic autoantigen with and without the presence of anti-GAD antibodies. About 35 percent of stiff person syndrome patients have type 1 diabetes.
- Thyroiditis: An association with thyroiditis has been described. This may be due to comorbidity of multiple autoimmune entities or may be a more direct association. At least one group has suggested a link due to neuromuscular hyperactivity.
- Breast cancer: A variant of stiff person syndrome occurs rarely in patients with breast cancer. The antibodies involved are to a synaptic protein, amphiphysin. Anti-GAD antibodies are absent.
- Epilepsy: Anti-GAD antibodies have been described in patients with medication-resistant focal epilepsies. In one series, 4 of 19 patients with anti-GAD–positive stiff person syndrome were also found to have localization-related epilepsy.
- Cerebellar ataxia: A number of case studies report the presence of cerebellar ataxia (with or without stiff person syndrome) associated with anti-GAD antibodies.
- A form of familial spastic cerebral palsy has been described with a missense mutation in the GAD-67 gene. This is a different isoform of glutamic decarboxylase; however, it demonstrates that the pathophysiology of stiff person syndrome is likely due to abnormalities in the function of glutamic acid decarboxylase.
Stiff person syndrome complications
Complications of Stiff-Person syndrome are multifaceted and may occur at any stage of the disease. In general, complications are responsible for the illness and death. The earliest and most common complications of Stiff-Person syndrome are anxiety and depression. Patients with Stiff-Person syndrome are at higher risk of developing orthopedic problems such as lumbar hyperlordosis, joint deformities, and muscle atrophies, leading to abnormal posturing and gait abnormalities with increased fall risk. As the disease progresses, unexpected tactile and auditory stimuli could trigger the occurrence of autonomic failure with tachycardia, hypertension, and hyperthermia 19, 16.
The function of glutamic acid decarboxylase (GAD) is to convert glutamate to GABA. Although this is not the only source of GABA for the CNS (central nervous system), it is a significant source; depending on the situation, GABA can be depleted rapidly. GABA serves as a natural antianxiety compound. The most potent antianxiety medications are based on augmentation of the GABA-A receptor. Because a significant portion of patients with stiff person syndrome have antibodies to GAD, not surprisingly patients also have anxiety. Tragically, anxiety worsens the spasms.
In the early stages, signs of stiff-person syndrome are often subtle to physicians and other health care workers. The patient feels uncomfortable and is aware of the stiffness, but his or her daily life is not disrupted significantly. Unfortunately, the failure of physicians and family to respond to the problem may result in increased anxiety and lead to dysphoria on the part of the patient. Ironically, the anxiety and dysphoria may become more disruptive to the patient’s quality of life than the disease, and the patient may be diagnosed with a somatization disorder.
In the late stages of stiff-person syndrome, patients may experience spasm of the pharyngeal muscles, making swallowing difficult and necessitating alternative methods of feeding. Severe paroxysms of spasms may result in skeletal fractures, particularly of the vertebral elements. They also have been reported in long bones. Muscle rupture has been reported in severe cases during spasms.
Infants with stiff baby syndrome are at particularly high risk of sudden infant death and require monitoring.
Complications of baclofen pump failure can occur. Cataclysmic exacerbations of the disease have been reported due to baclofen pump failure. At least one death has been reported. In addition, rare malfunctions of the baclofen pump have been associated with excessive release of baclofen intrathecally also resulting in death or permanent disability.
Psychiatric morbidity from this disease is common. The unpredictability of symptoms and the linkage to stressful events only serve to exacerbate the situation. In addition, GABA mechanisms subserve many of the brain’s emotional centers, which may contribute significantly to the psychiatric symptomatology.
Musculoskeletal complications are common, particularly in later stages of the disease. Joint deformity, joint dislocation, joint contracture, skeletal fracture, and muscle rupture have been reported.
Stiff person syndrome diagnosis
A diagnosis of Stiff-Person syndrome is made based upon identification of characteristic symptoms, a detailed patient history, and a thorough clinical evaluation 19. Stiff-Person syndrome is often misdiagnosed as Parkinson’s disease, multiple sclerosis, fibromyalgia, psychosomatic illness, or anxiety and phobia. A definitive diagnosis can be made with a blood test that measures the level of glutamic acid decarboxylase (GAD) antibodies in the blood. People with stiff person syndrome have elevated levels of glutamic acid decarboxylase (GAD) antibody that works against an enzyme involved in the synthesis of an important neurotransmitter in the brain.
Additional tests can be used to support a diagnosis and to rule out other conditions. Such tests include screening tests to detect the presence of antibodies against GAD-65, antibodies against amphiphysin (which are associated with paraneoplastic stiff person syndrome) and an electromyography (EMG), a test that records electrical activity in skeletal (voluntary) muscles at rest and during muscle contraction. Electrodiagnostic testing is useful to rule out other nerve and muscle pathologies and to confirm the clinical diagnosis. Routine nerve conduction studies in Stiff-Person syndrome are usually normal. Needle electromyography (EMG) in Stiff-Person syndrome shows continuous involuntary motor unit activity even at rest, despite volitional effort to relax, which is characteristic of Stiff-Person syndrome. Continuous motor unit activity and co-activation of agonists-antagonists muscles are key diagnostic features and are mostly detected in trunk muscles, especially paraspinal and abdominal muscles and proximal limb muscles 14. High doses of diazepam will suppress the characteristic EMG results.
Continuous muscle fiber activity on electromyography (EMG) and anti-GAD-65 are pathognomic of Stiff-Person syndrome. Anti-amphiphysin, anti-GABARAP, and anti-gephyrin may be present in the patient’s serum or CSF in GAD-negative patients.
The level of anti-GAD antibodies in serum higher than 10,000IU/mL supports a clinical impression of Stiff-Person syndrome 2. CSF analysis is usually unremarkable. In patients with PERM, a mild increase in CSF cell count with elevated protein and positive oligoclonal bands has been demonstrated as well as positive autoantibodies against glycine receptors 16.
MRI brain and spinal cord are usually non-diagnostic in classic Stiff-Person syndrome, but they are often performed to rule out other causes of rigidity and stiffness.
Magnetic resonance spectroscopy can show a focal change in GABA levels in the motor area of the brain in Stiff-Person syndrome 26. In patients with Progressive Encephalomyelitis with Rigidity and Myoclonus (PERM), MRI might show hyperintense signals in the spinal cord and the brainstem 19.
To diagnose a Paraneoplastic Stiff-Person syndrome, it is important to check for antibodies against amphiphysin and gephyrin and initiate a prompt neoplastic workup.
Since around 35% of patients diagnosed with Stiff-Person syndrome have type-1 diabetes and about 5% have associated autoimmune thyroid disease, a search for coexisting autoimmune conditions is commonly performed.
Stiff-Person syndrome diagnostic criteria
The diagnostic criteria for Stiff-Person syndrome have evolved over the years, and most accepted are criteria revised by Dalakas in 2009 29.
The current diagnostic criteria for classic Stiff-Person syndrome include 29:
- Stiffness of the limb and axial muscles, particularly the abdominal and thoraco-lumbar paraspinals, leading to hyperlordosis;
- Painful spasms triggered by unexpected tactile or auditory stimuli;
- Severe anxiety with task-specific phobias especially in anticipation of physically challenging tasks;
- Electromyographic evidence of continuous motor unit activity of agonist and antagonist muscles;
- Absence of other neurological impairments that may suggest an alternative diagnosis; and
- Highly positive GAD-antibody titers (anti-GAD65 or anti-amphiphysin autoantibodies) by immunocytochemistry, Western blot, enzyme linked immunosorbent assay (ELISA) or radioimmunoassay
- Clinical response to therapy with benzodiazepines.
Although these criteria best describe “classic or typical Stiff-Person syndrome”, some patients with positive anti-GAD antibodies may not exhibit all the above mentioned symptomatology 2.
Stiff person syndrome differential diagnosis
The differential diagnosis for Stiff-Person syndrome is broad, and it includes disorders of the brain, spinal cord, and muscles 13:
- Spinal cord diseases: spinal cord compression, spinal cord inflammation, spinal cord infectious, spinal cord ischemia
- Congenital myopathies and muscular dystrophies
- Metabolic myopathies
- Idiopathic Parkinson disease and Parkinson-plus syndromes
- Autoimmune encephalitis
- Stiff encephalomyelitis
- Primary lateral sclerosis
- Painful tonic spasms of multiple sclerosis
- Generalized or focal dystonia
- Axial torsion dystonia
- Myoclonic seizures
- Neuromyotonia
- Neuromyotonia (Isaac syndrome)
- Ankylosing spondylitis
- Hereditary spastic paraplegia
- Hereditary hyperekplexia
- Idiopathic hyperekplexia
- Leukodystrophies
- Neuroleptic malignant syndrome, serotonin syndrome, or malignant hyperthermia
- Tetanus
- Cocaine-addicted infant
- Startle syndrome
- Hereditary startle disease
- Paraneoplastic hypertonic syndrome
- Functional neurological disorder
- Somatoform disorder
- Schwartz-Jampel syndrome
Stiff person syndrome treatment
Treatment options for Stiff-Person syndrome can be divided into two main categories: symptomatic and and disease-modifying or immunotherapy 15. These lines of therapy are commonly used in combinations, depending on the severity of the disease.
Symptomatic management is a standard of initial therapy and focuses on decreasing stiffness, rigidity, and painful muscle spasms. Symptomatic management often requires a multifaceted approach including using medications and non-medication interventions (stretching, heat therapy, aqua therapy, massage therapy, acupuncture, etc). Symptomatic management is achieved using medications that promote GABA effects, such as benzodiazepines, specifically high doses of diazepam and clonazepam, are used to treat muscle stiffness and episodic spasms. Diazepam is known to be a first-line symptomatic agent for patients with SPS. Affected individuals may also benefit from baclofen, usually given in addition to benzodiazepines. Still, it is not uncommon to develop a tolerance and addiction to benzodiazepines over time, resulting in a loss of its beneficial effects.
Other medications reported to have benefit in a small number of individuals include anti-epileptic (anticonvulsant) drugs including vigabatrin, valproate, pregabalin, tiagabine and gabapentin. Intrathecal baclofen is also effectively used in some patients. Other commonly used muscle relaxants include dantrolene and tizanidine 14. Symptom management also includes treatment of co-existing seizures and psychiatric comorbidities with and antidepressant medications, respectively.
Disease-modifying therapy is a specific immune-modulating treatment that aims at reducing or removing autoantibodies. Intravenous immunoglobulin (IVIG) is proven to be the most effective immunotherapy in SPS, promoting a clinical improvement for up to 1 year after a standard course of five sessions. Unlike intravenous immunoglobulin (IVIG), the benefit of plasma exchange is not yet fully established, and most patients only demonstrate temporary or no improvement in symptoms 44. Peer-reviewed clinical studies have shown that intravenous immunoglobulin (IVIG) is effective and well-tolerated in reducing stiffness and lowering sensitivity to noise, touch, and stress in people with Stiff-Person syndrome. Intravenous immunoglobulin (IVIG) is commonly used as a therapy for immune-mediated disorders as Stiff-Person syndrome is believed to be. Intravenous immunoglobulin (IVIG), under certain conditions, has been associated with increased risks for stroke and heart attacks and can rarely cause kidney injury and meningitis. Treatment should be prescribed only after a discussion of the attendant risks and benefits. More research is necessary to determine the long-term safety and effectiveness of IVIG for the treatment of individuals with Stiff-Person syndrome.
This 2022 study 24 demonstrated that maintenance therapy with intravenous immunoglobulin (IVIG) continues to be effective over a median of 3.3 years in 67% of patients with typical Stiff-Person syndrome, improving daily functioning, gait, balance, painful spasms, posture, and facial expression with a demonstrable effect in decreasing stiffness, spasms and startle response. Although it’s an uncontrolled study due to disease rarity and the clinical ethics to give placebo over 2–3 years, this is a long-term study in a large group of patients with Stiff-Person syndrome seen over time by the same experienced clinicians that documents continued IVIg efficacy based on a combination of modified Rankin Scale scores, dependency tests, and objective clinical observations 24. The results complement the conclusions from the original short-term 3-month controlled study that the same investigators conducted 20 years ago with a much smaller number of enrolled patients 23.
Corticosteroid effectiveness is controversial in Stiff-Person Syndrome. Rituximab, a monoclonal antibody against CD20 antigen on B-cells, has provided a long-lasting benefit in non-randomized trials 45. Use of other immunomodulating agents including mycophenolate mofetil, azathioprine, cyclophosphamide, cyclosporine, tacrolimus, and sirolimus is reported with variable effects 16.
There are classes of medications that should be avoided in Stiff-Person syndrome, including serotonin-norepinephrine reuptake inhibitors (SNRIs; i.e, tricyclic antidepressants and duloxetine) and opioids. Serotonin-norepinephrine reuptake inhibitors (SNRIs) have previously been shown to worsen the electromyography (EMG) activity and clinical symptoms in stiff person syndrome. Opioids are not recommended for pain control because most individuals with stiff person syndrome are on benzodiazepines. Mixing these two classes of medications can lead to severe respiratory depression and death.
Ongoing physical therapy and occupational therapy
Physical and occupational therapists can help with long-term muscle control and also serve as an adjunct to clinical observation for worsening signs and symptoms. They can also use passive muscle relaxation techniques that can help to relieve symptoms of long-term muscle spasm and to avoid loss of range of motion.
Cognitive behavioral therapy
Muscle stiffness gets exaggerated due to anxiety as it is an autonomic physiological symptom. A study conducted have showed that about 44% of the patients develop severe motor symptoms due to their anxiety 46. A case study was conducted on an Stiff-Person syndrome patient who underwent five weeks of cognitive behavioral therapy (CBT). The results were promising as evidenced by the substantial decrease in anxiety, upliftment of the self-confidence, and lessening stiffness and rigidity 47.
Investigational Therapies
Several different immune therapies have been used to treat individuals with Stiff-Person syndrome beyond IVIG including plasmapheresis, corticosteroids, rituximab, and oral immunosuppressive drugs. Other therapies are being evaluated including non-myeloablative and myeloablative stem cell therapies.
Plasmapheresis may be of benefit in individuals with Stiff-Person syndrome. This procedure is a method for removing unwanted substances (toxins, bad antibodies, metabolic substances, plasma parts) from the blood. Blood is removed from an affected individual and blood cells are separated from plasma. The plasma is then replaced with other human plasma or albumin. This therapy remains under investigation to analyze side effects and effectiveness. More research is needed to determine what role plasmapheresis may play in the treatment of individuals with Stiff-Person syndrome.
Stiff person syndrome prognosis
The prognosis for patients with Stiff-Person syndrome depends on multiple factors, including clinical presentation, the duration of symptoms, co-existing neoplastic process, and a response to therapy 13. Many patients have an indolent course that is primarily asymptomatic and is punctuated by occasional episodes of stiffness. Other patients may have a much more aggressive course, rapidly progressing to the late stages of disease.
Treatment with intravenous immunoglobulin (IVIG), anti-anxiety drugs, muscle relaxants, anti-convulsants, and pain relievers will improve the symptoms of stiff person syndrome, but will not cure the disorder. Most individuals with Stiff-Person syndrome have frequent falls and because they lack the normal defensive reflexes; injuries can be severe. With appropriate treatment, the symptoms are usually well controlled.
It is critical to timely initiate therapy to prevent or lessen progression and avoid long-term complications 13. Most of Stiff-Person syndrome patients improve with medications, however fluctuations precipitated by physical and emotional stressors still occur. Despite the availability of multiple treatment options, some patients with Stiff-Person syndrome show disease progression over time, leading to permanent orthopedic abnormalities, inability to walk, and disability 19, 16. In one longitudinal study, only 19% of patients could work after 4 years of follow-up 17. Patients report markedly reduced quality of life due to physical and social limitations 13.
Prognosis for stiff baby syndrome is perhaps better. It is generally believed to be self-limiting and resolves with maturation of the CNS. Unfortunately, long-term follow-up studies are lacking.
- Baizabal-Carvallo JF, Jankovic J. Stiff-person syndrome: insights into a complex autoimmune disorder. Journal of Neurology, Neurosurgery & Psychiatry 2015;86:840-848. http://dx.doi.org/10.1136/jnnp-2014-309201[↩]
- Tsiortou P, Alexopoulos H, Dalakas MC. GAD antibody-spectrum disorders: progress in clinical phenotypes, immunopathogenesis and therapeutic interventions. Ther Adv Neurol Disord. 2021 Mar 30;14:17562864211003486. doi: 10.1177/17562864211003486[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Levy LM, Dalakas MC, Floeter MK. The stiff-person syndrome: an autoimmune disorder affecting neurotransmission of gamma-aminobutyric acid. Ann Intern Med. 1999 Oct 5;131(7):522-30. doi: 10.7326/0003-4819-131-7-199910050-00008[↩]
- Dalakas MC. Stiff-person Syndrome and GAD Antibody-spectrum Disorders: GABAergic Neuronal Excitability, Immunopathogenesis and Update on Antibody Therapies. Neurotherapeutics. 2022 Apr;19(3):832-847. doi: 10.1007/s13311-022-01188-w[↩][↩][↩][↩][↩][↩]
- Alexopoulos H, Dalakas MC. Immunology of stiff person syndrome and other GAD-associated neurological disorders. Expert Rev Clin Immunol. 2013 Nov;9(11):1043-53. doi: 10.1586/1744666X.2013.845527[↩][↩][↩][↩][↩]
- Dalakas MC. Progress and stiff challenges in understanding the role of GAD-antibodies in stiff-person syndrome. Exp Neurol. 2013 Sep;247:303-7. doi: 10.1016/j.expneurol.2013.02.010[↩][↩][↩]
- Molloy FM, Dalakas MC, Floeter MK. Increased brainstem excitability in stiff-person syndrome. Neurology. 2002 Aug 13;59(3):449-51. doi: 10.1212/wnl.59.3.449[↩]
- Friedhelm Sandbrink, Nadir Ali Syed, Mavis D. Fujii, Marinos C. Dalakas, Mary Kay Floeter, Motor cortex excitability in stiff-person syndrome, Brain, Volume 123, Issue 11, November 2000, Pages 2231–2239, https://doi.org/10.1093/brain/123.11.2231[↩]
- Meinck, H.-M. and Thompson, P.D. (2002), Stiff man syndrome and related conditions. Mov. Disord., 17: 853-866. https://doi.org/10.1002/mds.10279[↩]
- McKeon, A. and Tracy, J.A. (2017), GAD65 neurological autoimmunity. Muscle Nerve, 56: 15-27. https://doi.org/10.1002/mus.25565[↩]
- Moersch FP, Woltman HW. Progressive fluctuating muscular rigidity and spasm (‘stiff-man syndrome’): report of a case and some observations in 13 other cases. Mayo Clin Proc. 1956. 31:421-7.[↩]
- McKeon A, Robinson MT, McEvoy KM, Matsumoto JY, Lennon VA, Ahlskog JE, Pittock SJ. Stiff-man syndrome and variants: clinical course, treatments, and outcomes. Arch Neurol. 2012 Feb;69(2):230-8. doi: 10.1001/archneurol.2011.991[↩][↩]
- Muranova A, Shanina E. Stiff Person Syndrome. [Updated 2022 Jul 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK573078[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Rakocevic G, Floeter MK. Autoimmune stiff person syndrome and related myelopathies: understanding of electrophysiological and immunological processes. Muscle Nerve. 2012 May;45(5):623-34. doi: 10.1002/mus.23234[↩][↩][↩][↩]
- Baizabal-Carvallo JF, Jankovic J. Stiff-person syndrome: insights into a complex autoimmune disorder. J Neurol Neurosurg Psychiatry. 2015 Aug;86(8):840-8. doi: 10.1136/jnnp-2014-309201[↩][↩][↩][↩][↩]
- Hadavi S, Noyce AJ, Leslie RD, Giovannoni G. Stiff person syndrome. Pract Neurol. 2011 Oct;11(5):272-82. doi: 10.1136/practneurol-2011-000071[↩][↩][↩][↩][↩][↩][↩]
- Rakocevic G, Alexopoulos H, Dalakas MC. Quantitative clinical and autoimmune assessments in stiff person syndrome: evidence for a progressive disorder. BMC Neurol. 2019 Jan 3;19(1):1. doi: 10.1186/s12883-018-1232-z[↩][↩][↩][↩][↩][↩][↩]
- Rakocevic G, Raju R, Semino-Mora C, Dalakas MC. Stiff person syndrome with cerebellar disease and high-titer anti-GAD antibodies. Neurology. 2006 Sep 26;67(6):1068-70. doi: 10.1212/01.wnl.0000237558.83349.d0[↩]
- El-Abassi R, Soliman MY, Villemarette-Pittman N, England JD. SPS: Understanding the complexity. J Neurol Sci. 2019 Sep 15;404:137-149. doi: 10.1016/j.jns.2019.06.021[↩][↩][↩][↩][↩][↩][↩][↩]
- Raghavan Raju, Goran Rakocevic, Ziwei Chen, Gerard Hoehn, Cristina Semino-Mora, Wei Shi, Richard Olsen, Marinos C. Dalakas, Autoimmunity to GABAA-receptor-associated protein in stiff-person syndrome, Brain, Volume 129, Issue 12, December 2006, Pages 3270–3276, https://doi.org/10.1093/brain/awl245[↩][↩]
- Buechner S, Florio I, Capone L. Stiff Person Syndrome: A Rare Neurological Disorder, Heterogeneous in Clinical Presentation and Not Easy to Treat. Case Rep Neurol Med. 2015;2015:278065. doi:10.1155/2015/278065 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4461724[↩]
- The clinical spectrum of anti-GAD antibody-positive patients with stiff-person syndrome. Marinos C. Dalakas, Mavis Fujii, Mian Li, Beverly McElroy. Neurology Nov 2000, 55 (10) 1531-1535; https://doi.org/10.1212/WNL.55.10.1531[↩][↩]
- Dalakas MC, Fujii M, Li M, Lutfi B, Kyhos J, McElroy B. High-dose intravenous immune globulin for stiff-person syndrome. N Engl J Med. 2001 Dec 27;345(26):1870-6. doi: 10.1056/NEJMoa01167[↩][↩][↩]
- Yi J, Dalakas MC. Long-term Effectiveness of IVIg Maintenance Therapy in 36 Patients With GAD Antibody-Positive Stiff-Person Syndrome. Neurol Neuroimmunol Neuroinflamm. 2022 Jul 7;9(5):e200011. doi: 10.1212/NXI.0000000000200011[↩][↩][↩][↩]
- Stiff-person syndrome. https://www.uptodate.com/contents/stiff-person-syndrome[↩]
- Levy LM, Levy-Reis I, Fujii M, Dalakas MC. Brain gamma-aminobutyric acid changes in stiff-person syndrome. Arch Neurol. 2005 Jun;62(6):970-4. doi: 10.1001/archneur.62.6.970[↩][↩]
- Dinkel, K., Meinck, H.-M., Jury, K.M., Karges, W. and Richter, W. (1998), Inhibition of γ-aminobutyric acid synthesis by glutamic acid decarboxylase autoantibodies in stiff-man syndrome. Ann Neurol., 44: 194-201. https://doi.org/10.1002/ana.410440209[↩]
- Ali F, Rowley M, Jayakrishnan B, Teuber S, Gershwin ME, Mackay IR. Stiff-person syndrome (SPS) and anti-GAD-related CNS degenerations: protean additions to the autoimmune central neuropathies. J Autoimmun. 2011 Sep;37(2):79-87. doi: 10.1016/j.jaut.2011.05.005[↩]
- Dalakas MC. Stiff person syndrome: advances in pathogenesis and therapeutic interventions. Curr Treat Options Neurol. 2009 Mar;11(2):102-10. doi: 10.1007/s11940-009-0013-9[↩][↩][↩]
- Ehler E, Latta J, Mandysová P, Havlasová J, Mrklovský M. Stiff-person syndrome following tick-borne meningoencephalitis. Acta Medica (Hradec Kralove). 2011;54(4):170-4. doi: 10.14712/18059694.2016.44[↩]
- Rizzi M, Knoth R, Hampe CS, Lorenz P, Gougeon ML, Lemercier B, Venhoff N, Ferrera F, Salzer U, Thiesen HJ, Peter HH, Walker UA, Eibel H. Long-lived plasma cells and memory B cells produce pathogenic anti-GAD65 autoantibodies in Stiff Person Syndrome. PLoS One. 2010 May 26;5(5):e10838. doi: 10.1371/journal.pone.0010838[↩]
- Holmøy T, Geis C. The immunological basis for treatment of stiff person syndrome. J Neuroimmunol. 2011 Feb;231(1-2):55-60. doi: 10.1016/j.jneuroim.2010.09.014[↩]
- Matà S, Muscas GC, Cincotta M, Bartolozzi ML, Ambrosini S, Sorbi S: GAD antibodies associated neurological disorders: incidence and phenotype distribution among neurological inflammatory diseases. J Neuroimmunol. 2010, 227:175–77. 10.1016/j.jneuroim.2010.07.011[↩]
- Ciccotto G, Blaya M, Kelley RE. Stiff person syndrome. Neurol Clin. 2013 Feb;31(1):319-328. doi: 10.1016/j.ncl.2012.09.005[↩]
- Baizabal-Carvallo JF. The neurological syndromes associated with glutamic acid decarboxylase antibodies. J Autoimmun. 2019 Jul;101:35-47. doi: 10.1016/j.jaut.2019.04.007[↩]
- Balint B, Bhatia KP. Stiff person syndrome and other immune-mediated movement disorders – new insights. Curr Opin Neurol. 2016 Aug;29(4):496-506. doi: 10.1097/WCO.0000000000000351[↩]
- Christian Werner, Martin Pauli, Sören Doose, Andreas Weishaupt, Holger Haselmann, Benedikt Grünewald, Markus Sauer, Manfred Heckmann, Klaus V. Toyka, Esther Asan, Claudia Sommer, Christian Geis, Human autoantibodies to amphiphysin induce defective presynaptic vesicle dynamics and composition, Brain, Volume 139, Issue 2, February 2016, Pages 365–379, https://doi.org/10.1093/brain/awv324[↩]
- Mas N, Saiz A, Leite MI, Waters P, Baron M, Castaño D, Sabater L, Vincent A, Graus F. Antiglycine-receptor encephalomyelitis with rigidity. J Neurol Neurosurg Psychiatry. 2011 Dec;82(12):1399-401. doi: 10.1136/jnnp.2010.229104[↩]
- Iizuka T, Leite MI, Lang B, Waters P, Urano Y, Miyakawa S, Hamada J, Sakai F, Mochizuki H, Vincent A. Glycine receptor antibodies are detected in progressive encephalomyelitis with rigidity and myoclonus (PERM) but not in saccadic oscillations. J Neurol. 2012 Aug;259(8):1566-73. doi: 10.1007/s00415-011-6377-2[↩]
- Gresa-Arribas N, Ariño H, Martínez-Hernández E, Petit-Pedrol M, Sabater L, Saiz A, Dalmau J, Graus F. Antibodies to inhibitory synaptic proteins in neurological syndromes associated with glutamic acid decarboxylase autoimmunity. PLoS One. 2015 Mar 16;10(3):e0121364. doi: 10.1371/journal.pone.0121364[↩]
- De Camilli P, Thomas A, Cofiell R, Folli F, Lichte B, Piccolo G, Meinck HM, Austoni M, Fassetta G, Bottazzo G, Bates D, Cartlidge N, Solimena M, Kilimann MW, et al. The synaptic vesicle-associated protein amphiphysin is the 128-kD autoantigen of Stiff-Man syndrome with breast cancer. J Exp Med. 1993 Dec 1;178(6):2219-23. doi: 10.1084/jem.178.6.2219[↩]
- Folli F, Solimena M, Cofiell R, Austoni M, Tallini G, Fassetta G, Bates D, Cartlidge N, Bottazzo GF, Piccolo G, De Camilli P, et al. Autoantibodies to a 128-kd synaptic protein in three women with the stiff-man syndrome and breast cancer. N Engl J Med. 1993 Feb 25;328(8):546-51. doi: 10.1056/NEJM199302253280805[↩]
- Butler MH, Hayashi A, Ohkoshi N, Villmann C, Becker CM, Feng G, De Camilli P, Solimena M. Autoimmunity to gephyrin in Stiff-Man syndrome. Neuron. 2000 May;26(2):307-12. doi: 10.1016/s0896-6273(00)81165-4[↩]
- Ortiz JF, Ghani MR, Morillo Cox Á, Tambo W, Bashir F, Wirth M, Moya G. Stiff-Person Syndrome: A Treatment Update and New Directions. Cureus. 2020 Dec 9;12(12):e11995. doi: 10.7759/cureus.11995[↩]
- Baker MR, Das M, Isaacs J, Fawcett PR, Bates D. Treatment of stiff person syndrome with rituximab. J Neurol Neurosurg Psychiatry. 2005 Jul;76(7):999-1001. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1739691/pdf/v076p00999.pdf[↩]
- Henningsten P, Meinck H-M: Specific phobia is a frequent non-motor feature in stiff man syndrome. J Neurol Neurosurg Psychiatry. 2003, 74:462–65. 10.1136/jnnp.74.4.462[↩]
- Morrisa LL, Dysch L, Salkovskisa PM, Giffin N: Reducing excess stiffness in Stiff Person Syndrome using CBT: A case study. NeuroRehabilitation. 2014, 35:627–31. 10.3233/NRE-141147[↩]





{kind=link}