Contents
What is tongue cancer
Tongue cancer is a form of cancer that begins in the cells of the tongue. Several types of cancer can affect the tongue, but tongue cancer most often begins in the thin, flat squamous cells that line the surface of the tongue. The type of cells involved in your tongue cancer helps determine your prognosis and treatment.
Where your tongue cancer occurs also affects your treatment.
The most common type of tongue cancer is squamous cell carcinoma (SCC). Squamous cells are the flat, skin like cells that cover the lining of the mouth, nose, larynx, thyroid and throat. Squamous cell carcinoma is the name for a cancer that starts in these cells.
Tongue cancer can occur:
- In the mouth, where it may be more likely to be seen and felt (oral tongue cancer). This type of tongue cancer tends to be diagnosed when the cancer is small and more easily removed through surgery.
- In the throat, at the base of the tongue, where tongue cancer may develop with few signs and symptoms (hypopharyngeal tongue cancer). Cancer at the base of the tongue is usually diagnosed at an advanced stage, when the tumor is larger and the cancer has spread into the lymph nodes in the neck.
Symptoms can include a patch, spot or lump on your tongue that doesn’t go away. The main risk factors are smoking, drinking a lot of alcohol and infection with the human papillomavirus (HPV) virus. Increasingly, cancers at the base of the tongue are associated with human papillomavirus (HPV), which has a profound effect on the prognosis and treatment of the cancer.
Treatment for tongue cancer typically involves surgery to remove the cancer. Chemotherapy, radiation therapy and targeted drug therapy also may be recommended.
Treatment for advanced tongue cancers can impact your ability to speak and eat. Working with a skilled rehabilitation team can help you cope with changes that result from tongue cancer treatment.
Tongue anatomy
The tongue is a highly mobile structure that is vital to digestive functions such as chewing, detection of taste, and swallowing. It is also important in speech. The tongue’s mobility is greatly aided by its attachment to the mandible, styloid process of the temporal bone, and hyoid bone.
There are two parts to your tongue:
- the oral tongue
- the base of the tongue
Cancer can develop in either part.
The oral tongue is the part you see when you poke your tongue out at someone. This is the front two thirds of your tongue. Cancers that develop in this part of the tongue come under a group of cancers called mouth (oral) cancer.
The base of the tongue is the back third of the tongue (see Figure 2). This part is very near your throat (pharynx). Cancers that develop in this part are called oropharyngeal cancers.
Figure 1. Tongue anatomy
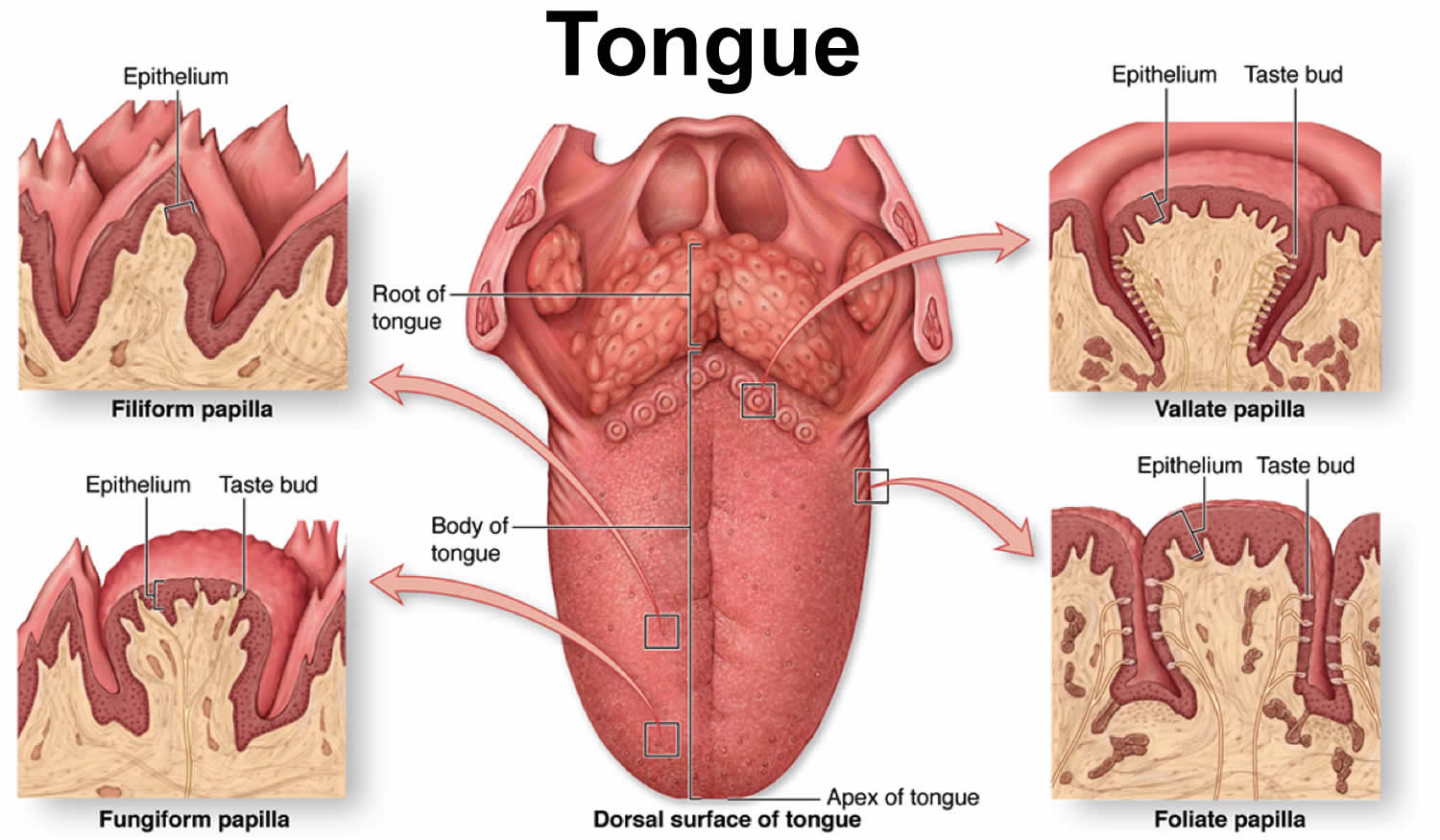
Figure 2. Base of tongue (Oropharynx)

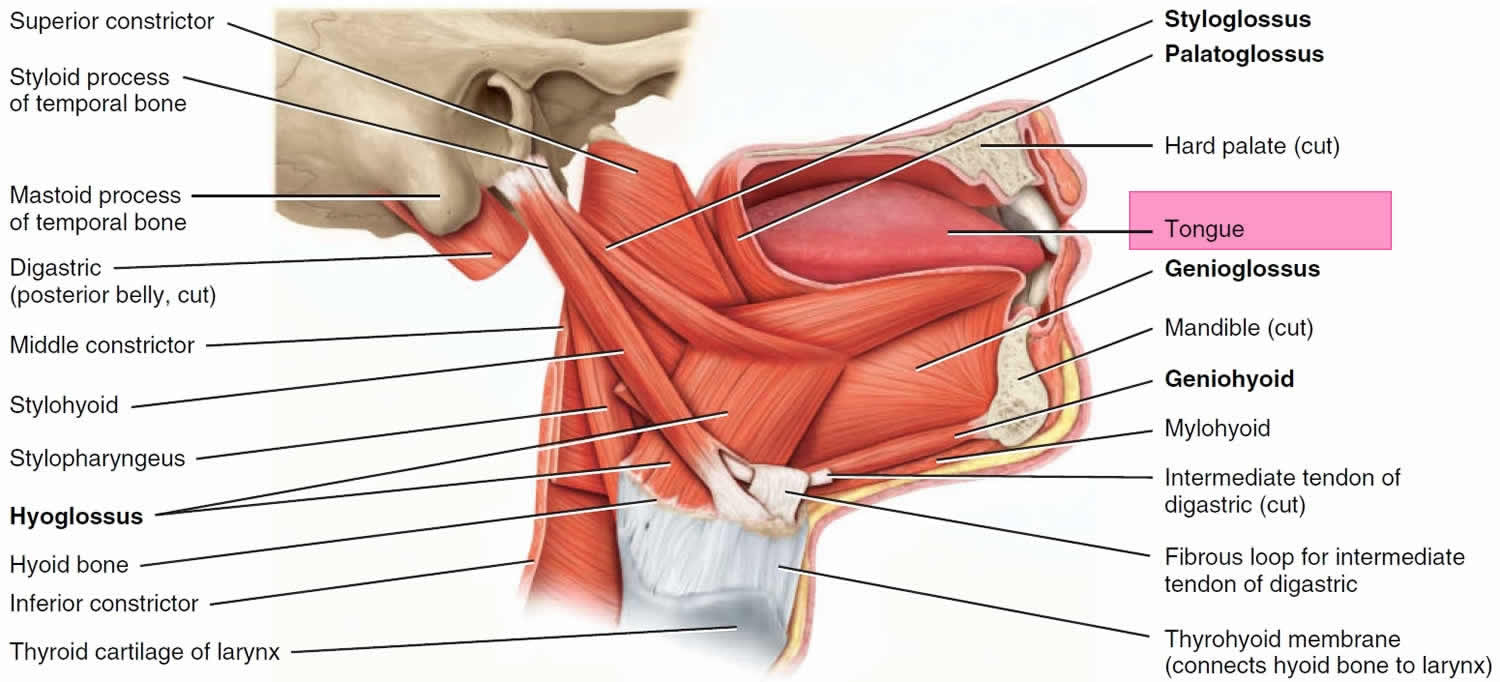
Figure 3. Muscles that move the tongue
Tongue cancer signs and symptoms
The symptoms of tongue cancer might include:
- a red or white patch on the tongue that won’t go away
- a sore throat that doesn’t go away
- a sore spot (ulcer) or lump on the tongue that doesn’t go away
- pain when swallowing
- numbness in the mouth that won’t go away
- unexplained bleeding from the tongue (that’s not caused by biting your tongue or other injury)
- pain in the ear (rare)
It’s important to remember that these symptoms might be due to a less serious medical condition. But it’s best to check symptoms with your doctor just to make sure.
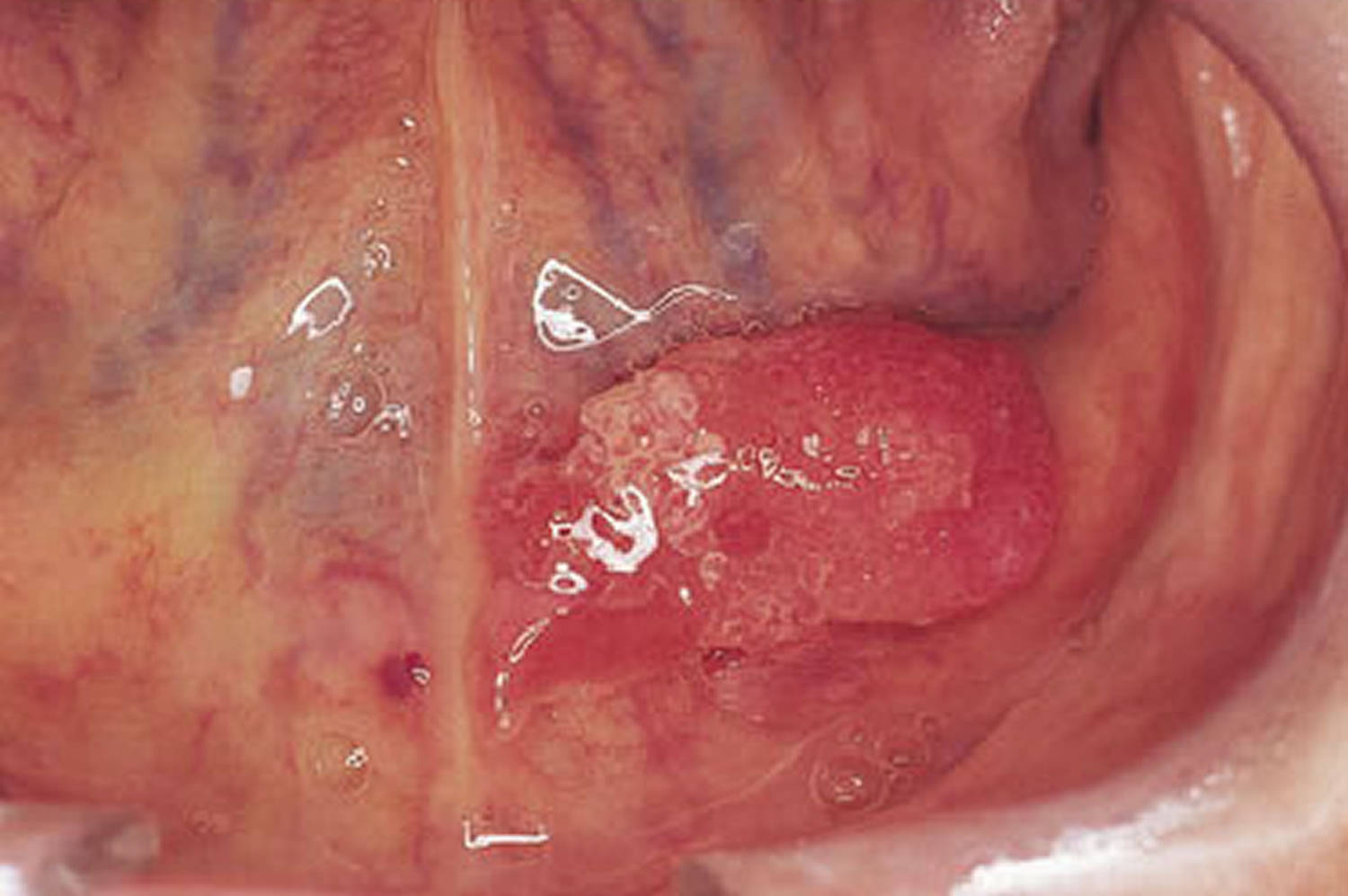
The photos below give you an idea of what tongue cancers can look like, but remember that they might appear differently from this. Contact your doctor or dentist if you notice anything abnormal.
What does tongue cancer look like
Figure 4. Tongue cancer

Figure 5. Tongue cancer

Figure 6. Tongue cancer – a red patch underneath the tongue
What causes tongue cancer
Researchers don’t know the exact causes of most head and neck cancers, but several risk factors have been identified.
Smoking tobacco (cigarettes, cigars and pipes) and drinking a lot of alcohol are the main risk factors for cancers of the head and neck in the western world. The human papillomavirus (HPV) virus transmitted through sexual contact is another risk factor.
Having a risk factors means that your risk is increased. But it does not mean that you will definitely develop cancer.
Smoking
Smoking tobacco (cigarettes, pipes, cigars) increases your risk of developing mouth and oropharyngeal cancer. Research suggests that more than 60 out of 100 (more than 60%) of mouth and oropharyngeal cancers in the US are caused by smoking.
There is some evidence that people exposed to second hand smoke (passive smoking) at home or in the workplace may have a small increase in their risk of mouth and oropharyngeal cancer.
Alcohol
Drinking alcohol increases your risk of mouth and oropharyngeal cancer. Research shows around 30 out of 100 (30%) of mouth and oropharyngeal cancers are caused by drinking alcohol.
Smoking and drinking together further increases the risk of cancer more than either by itself.
Chewing tobacco or betel quid
Smokeless tobacco, including chewing tobacco, such as betel quid (gutkha) or paan is known to cause mouth and orpharyngeal cancer. It is not a safe alternative to cigarettes. In the US, it is often popular with South Asian communities.
Diet
A diet low in fruit and vegetables may increase your risk of mouth and orpharyngeal cancer. This might be due to a lack of vitamins and minerals. A balanced diet usually means you are getting enough vitamins and minerals.
Human papilloma virus (HPV)
The human papilloma virus (HPV) is a type of virus that infects the skin and the cells lining body cavities. For most people, HPV causes no harm and gets better on it’s own. You don’t catch cancers like an infection. But the virus can cause changes in the mouth and throat making them more likely to become cancerous in the future.
HPV spreads through close skin to skin contact, usually during sexual activity. It is very common. Only a very small percentage of people with HPV develop mouth or oropharyngeal cancer.
The risk of HPV in the mouth and throat is linked to certain sexual behaviours, such as oral sex, and having a higher number of sexual partners.
Weak immune system
Your body’s immune system fights infection. Some illnesses and medication can weaken your immune system. Research shows an increased risk of mouth cancer if you are:
- having treatment for HIV or AIDS
- taking medicines to suppress your immune system after an organ transplant
Tongue cancer stages
The staging system most often used for oral cavity or oropharyngeal cancers is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
- The extent of the tumor (T): How large is the main (primary) tumor and which, if any, tissues of the oral cavity or oropharynx it has spread to?
- The spread to nearby lymph nodes (N): Has the cancer spread to nearby lymph nodes?
- The spread (metastasis) to distant sites (M): Has the cancer spread to distant organs such as the lungs?
Numbers or letters after T, N, and M provide more details about each of these factors. Higher numbers mean the cancer is more advanced. Once a person’s T, N, and M categories have been determined, this information is combined in a process called stage grouping to assign an overall stage.
The staging system in the table below is based on the most recent American Joint Committee on Cancer (AJCC) system, effective January 2018. It uses the pathologic stage (also called the surgical stage). It’s determined by examining the tissue removed during an operation. Sometimes, if surgery isn’t possible right away or at all, the cancer will be given a clinical stage instead (which is not shown below). This is based on the results of a physical exam, endoscopy exam, biopsy, and imaging tests. The clinical stage will be used to help plan treatment. Sometimes, though, the cancer has spread further than the clinical stage estimates, and it may not predict the patient’s outlook as accurately as a pathologic stage.
The earliest stage oral cavity or oropharyngeal cancers are called stage 0 (carcinoma in situ), and then range from stages I (1) through IV (4). As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means cancer has spread more. And within a stage, an earlier letter means a lower stage. Although each person’s cancer experience is unique, cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
Oropharyngeal cancers that contain human papillomavirus (HPV) virus DNA (called p16 positive) tend to have a better outlook than those without human papillomavirus (HPV) virus (p16 negative). Because p16 positive cancers have a better prognosis than p16 negative oropharyngeal cancers, separate staging systems are used. Both systems are described below.
Cancer staging can be complex, so ask your doctor to explain it to you in a way you understand.
Table 1. Lip, oral cavity, and p16 negative oropharynx stages
| AJCC stage | Stage grouping | Lip, oral cavity and p16 negative oropharynx stage description* |
| 0 | Tis N0 M0 | The cancer is still within the epithelium (the top layer of cells lining the oral cavity and oropharynx) and has not yet grown into deeper layers. It has not spread to nearby lymph nodes (N0) or distant sites (M0). This stage is also known as carcinoma in situ (Tis). |
| I | T1 N0 M0 | The cancer is 2 cm (about ¾ inch) or smaller. It’s not growing into nearby tissues (T1). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| II | T2 N0 M0 | The cancer is larger than 2 cm but no larger than 4 cm (about 1½ inch). It’s not growing into nearby tissues (T2). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| III
| T3 N0 M0 | The cancer is larger than 4 cm (T3). For cancers of the oropharynx, T3 also includes tumors that are growing into the epiglottis (the base of the tongue). It has not spread to nearby lymph nodes (N0) or to distant sites (M0). |
| OR | ||
| T1, T2, T3 N1 M0 | The cancer is any size and may have grown into nearby structures if oropharynx cancer(T1-T3) AND has spread to 1 lymph node on the same side as the primary tumor. The cancer has not grown outside of the lymph node and the lymph node is no larger than 3 cm (about 1¼ inch) (N1). It has not spread to distant sites (M0). | |
| IVA | T4a N0 or N1 M0 | The cancer is any size and is growing into nearby structures such as:
This is known as moderately advanced local disease (T4a). AND either of the following:
It has not spread to distant sites (M0). |
| OR | ||
| T1, T2, T3 or T4a N2 M0 | The cancer is any size and may have grown into nearby structures (T0-T4a). It has not spread to distant organs (M0). It has spread to one of the following:
| |
| IVB | Any T N3 M0 | The cancer is any size and may have grown into nearby soft tissues or structures (Any T) AND any of the following:
It has not spread to distant organs (M0). |
| OR | ||
| T4b Any N M0 | The cancer is any size and is growing into nearby structures such as the base of the skull or other bones nearby, or it surrounds the carotid artery. This is known as very advanced local disease (T4b). It might or might not have spread to nearby lymph nodes (Any N). It has not spread to distant organs (M0). | |
| IVC | Any T Any N M1 | The cancer is any size and may have grown into nearby soft tissues or structures (Any T) AND it might or might not have spread to nearby lymph nodes (Any N). It has spread to distant sites such as the lungs (M1). |
Footnotes:
* The following additional categories are not described in the table above:
TX: Main tumor cannot be assessed due to lack of information.
T0: No evidence of a primary tumor.
NX: Regional lymph nodes cannot be assessed due to lack of information.
Table 2. p16 positive oropharynx stages (cancers that contain human papillomavirus (HPV) virus DNA)
| AJCC stage | Stage grouping | p16 positive oropharynx stage description* |
| I | T0, T1 or T2 N0 or N1 M0 | The cancer is no larger than 4 cm (about 1 1/2 inches) (T0 to T2) AND any of the following:
It has not spread to distant sites (M0). |
| II | T0, T1 or T2 N2 M0 | The cancer is no larger than 4 cm (about 1 1/2 inches) (T0 to T2) AND it has spread to 1 or more lymph nodes on the opposite side of the primary cancer or both sides of the neck, and none are larger than 6 cm (N2). It has not spread to distant sites (M0). |
| OR | ||
| T3 or T4 N0 or N1 M0 | The cancer is larger than 4 cm (about 1 1/2 inches) (T3) OR is growing into the epiglottis (the base of the tongue) (T3) OR is growing into the larynx (voice box), the tongue muscle, or bones such as the medial pterygoid plate, the hard palate, or the jaw (T4) AND any of the following:
It has not spread to distant sites (M0). | |
| III
| T3 or T4 N2 M0 | The cancer is larger than 4 cm (about 1 1/2 inches) (T3) OR is growing into the epiglottis (the base of the tongue) (T3) OR is growing into the larynx (voice box), the tongue muscle, or bones such as the medial pterygoid plate, the hard palate, or the jaw (T4) AND it has spread to 1 or more lymph nodes on the opposite side of the primary cancer or both sides of the neck, and none are larger than 6 cm (N2). It has not spread to distant sites (M0). |
| IV | Any T Any N M1 | The cancer is any size and may have grown into nearby structures (Any T) AND it might or might not have spread to nearby lymph nodes (Any N). It has spread to distant sites such as the lungs or bones (M1). |
Footnotes:
* The following additional categories are not described in the table above:
TX: Main tumor cannot be assessed due to lack of information.
T0: No evidence of a primary tumor.
NX: Regional lymph nodes cannot be assessed due to lack of information.
Tongue cancer prognosis
Survival rates are often used by doctors as a standard way of discussing a person’s prognosis (outlook).
The 5-year survival rate refers to the percentage of patients who live at least 5 years after their cancer is diagnosed. Of course, many of these people live much longer than 5 years.
Five-year relative survival rates, such as the numbers below, assume that some people will die of other causes and compares the observed survival of people with cancer with that expected for people without cancer. This is a more accurate way to describe the impact that a particular type and stage of cancer may have on survival.
To get 5-year survival rates, doctors have to look at people who were treated at least 5 years ago. Improvements in treatment since then may result in a more favorable outlook for people now being diagnosed with these cancers.
Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they cannot predict what will happen in any individual’s case. Many other factors may affect a person’s outlook, such as the patient’s age and health, the treatment received, and how well the cancer responds to treatment. Your doctor can tell you how the numbers below may apply to you, because they are familiar with the aspects of your particular situation.
The following survival statistics come from the National Cancer Institute’s SEER program. They are based on large numbers of patients diagnosed between 2000 and 2014. SEER doesn’t provide recent statistics by American Joint Committee on Cancer (AJCC) stage. Instead, cancers are divided into the summary stages:
- Local: the cancer is only in the area where it started. This includes stages I and II, as well as some stage III cancers that haven’t spread to any lymph nodes.
- Regional: the cancer has spread to nearby tissues and/or lymph nodes. This includes some stage III cancers, as well as stage IV cancers that haven’t spread to distant sites
- Distant: the cancer has spread to distant sites
Also, these statistics are based on the stage of the cancer when it was first diagnosed. They do not apply to cancers that have come back or spread, for example.
For cancers of the oropharynx (including the base of tongue cancer) and tonsil, the relative 5-year survival rate was 66%, but survival by stage is not available 2.
Table 3. Tongue cancer 5 year survival rate
| Stage | 5-Year Relative Survival Rate |
| Local | 78% |
| Regional | 63% |
| Distant | 36% |
Table 4. Floor of the mouth cancer 5 year survival rate
| Stage | 5-Year Relative Survival Rate |
| Local | 75% |
| Regional | 38% |
| Distant | 20% |
Tongue cancer treatment
The main treatments for tongue cancer are surgery, radiotherapy and chemotherapy, either combined or on their own. Your treatment depends on how far your cancer has grown and whether it has spread (the stage). It also depends on which part of the tongue is affected.
Treating the oral tongue cancer
The front two thirds of the tongue (oral tongue) are treated like a mouth cancer.
Early stage
Early cancer means your cancer is smaller than 4cm and is contained within the tongue.
The most common treatment is surgery to remove the affected area. You might also have surgery to remove lymph nodes in your neck.
Advanced stage
Advanced cancer means your cancer is larger than 4cm. Or it has grown outside the tongue, invading other tissues or lymph nodes. You are most likely to have a combination of all of these treatments:
- surgery to remove the cancer from your tongue and the lymph nodes in your neck
- reconstructive surgery
- radiotherapy after surgery – this might be combined with chemotherapy (chemoradiotherapy)
You might have chemotherapy if your cancer has come back. Or if your cancer has spread into surrounding tissues or to other parts of the body.
Treating the base of the tongue cancer
The back third of the tongue (base of the tongue) is treated like oropharyngeal cancer. Oropharyngeal cancer starts in the part of the throat just behind the mouth.
Early cancer
Early cancer means your cancer is smaller than 4cm and is contained within the tongue.
You might have either:
- surgery to remove the cancer and some of the lymph nodes in your neck
- radiotherapy to the throat and neck
You might need radiotherapy or chemoradiotherapy after surgery if your doctor thinks there is a high risk that your cancer will come back. Chemoradiotherapy means you have chemotherapy and radiotherapy together.
Advanced cancer
Advanced cancer means your cancer is larger than 4cm. Or it has grown outside the tongue, invading other tissues or lymph nodes.
You might have one of the following:
- chemotherapy and radiotherapy together (chemoradiotherapy) to your throat and neck
- surgery to remove part of the throat (including all or part of the tongue) and some of the lymph nodes in your neck, followed by radiotherapy or chemoradiotherapy
- radiotherapy on its own
You might have radiotherapy, chemotherapy or surgery to control symptoms of advanced cancer.
Tongue cancer surgery
Your surgeon removes the cancer and an area (margin) of normal tissue around it. This helps to make sure that they have removed all the cancer. The operation is called a primary tumor resection.
There are different types of primary tumor resection. It depends on the location of your cancer.
You might only need a simple operation if the cancer is very small. This can be done using local anaesthetic or with laser surgery, and you don’t need to stay overnight in hospital.
For larger cancers, you might need a more complicated operation and stay in hospital for a while. You might have an operation to remove part or all of your tongue (a glossectomy). This is quite a big operation. Your surgeon rebuilds (reconstructs) your tongue.
The surgeon usually removes the lymph nodes from one or both sides of your neck. This operation is called a neck dissection. It lowers the risk of your cancer coming back in the future.
Surgery to your tongue
Surgery to remove the tongue is called a glossectomy. Having your tongue removed sounds frightening and you will probably feel shocked if you need this operation. Surgeons only ever perform this type of surgery if it is absolutely necessary.
There are 2 types of glossectomy:
- partial glossectomy
- total glossectomy
Partial glossectomy
The surgeon removes less than half of your tongue. You may have changes to your speech after this operation. Your surgeon will explain the possible effects of a partial glossectomy.
Total glossectomy
This means removing more than half or all of your tongue. Your surgeon will rebuild (reconstruct) your tongue. But your speech and swallowing will change after the surgery. You will have a lot of support to help you cope afterwards.
Radiotherapy
Radiotherapy uses high energy waves similar to x-rays to kill cancer cells. You might have radiotherapy:
- on its own as your main treatment or after surgery
- combined with chemotherapy (chemoradiotherapy) as your main treatment or after surgery
- to help relieve the symptoms of advanced tongue cancer
You have radiotherapy to the part of the tongue affected by cancer. And the doctor might also treat the lymph nodes in your neck.
You usually have radiotherapy treatment once a day for a few weeks.
Chemotherapy
Chemotherapy uses anti cancer (cytotoxic) drugs to destroy cancer.
You might have chemotherapy combined with radiotherapy (chemoradiotherapy). The chemotherapy helps the radiotherapy work better. You might have this:
- after surgery if there is a high risk of your cancer coming back
- as your main treatment
You usually have a PET-CT scan a few months after chemoradiotherapy. This is to check if your lymph nodes contain cancer. If there are signs of cancer, you usually have surgery to remove the lymph nodes.
Some people have chemotherapy to shrink the cancer before the main treatment, although this isn’t very common. This is called neo adjuvant treatment.
The most commonly used drug is cisplatin. You might have this with fluoracil (5FU). Some people have carboplatin instead of cispatin.
Targeted cancer drugs
Cetuximab (Erbitux) is a type of targeted cancer drug called a monoclonal antibody. You might have cetuximab together with radiotherapy if you can’t have chemotherapy for any reason.
Nivolumab is a type of immunotherapy. This type of treatment stimulates the body’s immune system to fight cancer cells. You might be able to have nivolumab if your cancer has started to grow again within 6 months of stopping chemotherapy.
Treatment side effects
All treatments have side effects. Some are temporary but some might be permanent.
Surgery to the tongue can cause problems with your speech, and changes in eating and drinking. These could be permanent changes for some people.
This can be very hard to cope with and you’re likely to need a lot of support and help following your operation. Talk to your doctor or specialist nurse before your operation. You can ask them about how it will affect you.
Radiotherapy to the head and neck area can cause several side effects including a dry, sore mouth and taste changes.
Common chemotherapy side effects include:
- feeling sick
- loss of appetite
- losing weight
- feeling very tired
- a lower resistance to infections
- bleeding and bruising easily
Follow-up care
After you have completed treatment, your doctors will still want to watch you closely. It’s very important to go to all of your follow-up appointments. During these visits, your doctors will ask questions about any problems you are having and will examine you. Your doctor may also order lab tests or imaging tests (such as MRI or CT scans) to look for signs of cancer return (called cancer recurrence). Your health care team will discuss which tests should be done and how often based on the type and stage of your cancer, the type of treatment you had, and the response to that treatment.
People with cancer of the oral cavity or oropharynx may develop recurrences or new cancers in the head and neck area or the lungs. With improvements in surgery and radiation therapy, the ability to control the main (primary) cancer has greatly improved. But development of second cancers in the head and neck or lungs remains an important risk. Because of this, you will be followed closely after treatment. Recurrences happen most often in the first 2 years after treatment, so you will be examined every few months during the first 2 years and then less often after that.
If you were treated with radiation to the neck, blood tests to look at thyroid function may be needed about every 6 months.
Many studies have found that some people’s quality of life tends to get worse in the first few months after treatment. But after that, for people who have given up smoking and drinking alcohol, things tend to get better. Within a year, many people are feeling reasonably well and happy.
Almost any cancer treatment can have side effects. Some may last for a few weeks to several months, but others can last the rest of your life. Don’t hesitate to tell your cancer care team about any symptoms or side effects that bother you so they can help you manage them. Keep in mind that it’s very important to report any new symptoms to your doctor right away, because they may prompt your doctor to do tests that could help find recurrent cancer as early as possible, when the likelihood of successful treatment is greatest.
Problems with eating and nutrition
Cancers of the mouth and throat and their treatments can sometimes cause problems such as loss or change in taste, dry mouth, or even loss of teeth. This can make it hard to eat, which can lead to weight loss and weakness due to poor nutrition.
Some people may need to adjust what they eat during and after treatment. Some may even need a feeding tube placed into the stomach, at least for a short time during and after treatment. You may want to consult with a nutritionist to help find ways to meet your nutritional needs. If a dry mouth is making it hard to eat, your doctor may recommend a saliva substitute. This can help you maintain your weight and nutritional intake. Again, talk to your doctor about any problems you’re having. There are often ways to help.
Speech and swallowing therapy
Oral cavity or oropharyngeal cancers and their treatments may affect a person’s speech and ability to swallow. A speech therapist can often help with these. These experts are knowledgeable about speech and swallowing problems. They can help you learn to manage these problems and do the things you want and need to do.
Dietary supplements
So far, no dietary supplements (including vitamins, minerals, and herbal products) have been shown to clearly help lower the risk of oral cavity or oropharyngeal cancer progressing or coming back. This doesn’t mean that no supplements will help, but it’s important to know that none have been proven to do so.
Dietary supplements are not regulated like medicines in the United States – they do not have to be proven effective (or even safe) before being sold, although there are limits on what they’re allowed to claim they can do. If you’re thinking about taking any type of nutritional supplement, talk to your health care team. They can help you decide which ones you can use safely while avoiding those that might be harmful.
Get support
Emotional support can be a powerful tool for both cancer survivors and their families. Talking with others who are in situations like yours can help ease loneliness. You can also get useful ideas from others that might help you.
There are many kinds of support programs, including individual or group counseling and support groups.
Support in any form allows you to express your feelings and develop coping skills. Studies have found that people who take part in support groups have an improved quality of life, including better sleep and appetite. Contact your American Cancer Society to find out about available sources of support where you live (https://www.cancer.org/treatment/support-programs-and-services.html) or call the National Cancer Information Center toll-free number, 1-800-227-2345. They’re there to help you any time, day or night.
Online support groups may be another option for support. The Cancer Survivors Network, an online support community supported by your American Cancer Society is just one example. You can visit this community at https://csn.cancer.org/. There are many other good communities on the Internet that you can join as well, although you’ll want to check them out before joining.
- Oral Cavity and Oropharyngeal Cancer Stages. https://www.cancer.org/cancer/oral-cavity-and-oropharyngeal-cancer/detection-diagnosis-staging/staging.html[↩][↩]
- Survival Rates for Oral Cavity and Oropharyngeal Cancer. https://www.cancer.org/cancer/oral-cavity-and-oropharyngeal-cancer/detection-diagnosis-staging/survival-rates.html[↩][↩][↩]





{kind=link}