What is torticollis
Torticollis also called twisted neck or wry neck, is a stiff and painful neck that’s twisted to one side. When the symptoms of a twisted (or wry) neck appear suddenly (such as overnight), it is called acute torticollis. Torticollis is the most common cause of neck pain in young people and it’s not generally associated with a previous neck injury or neck pain.
Torticollis usually causes pain on one side of your neck but you may feel pain in the middle of the neck and in the shoulders and head. Your neck may be very tender and if you try to massage the area, to provide some relief, it’s possible your neck muscles will spasm. You may also find it difficult to straighten your neck or turn your head a particular way.
Symptoms of a torticollis neck (twisted neck) will usually disappear completely within a week, and they usually ease considerably within one or two days. Sometimes torticollis neck symptoms last longer, but this is not common.
Diagnosis is usually confirmed by history and physical exam.
Torticollis symptoms
The following are the most common symptoms of torticollis. However, each person may experience symptoms differently. Symptoms may include:
- Neck muscle pain or pain down the spine
- Inability to turn the head, usually holding it twisted to one side
- Spasm of the neck muscles
- Awkward position of the chin
The symptoms of torticollis may resemble other conditions and medical problems. Always consult your healthcare provider for a diagnosis.
Torticollis in adults causes
The exact cause of torticollis is unknown.
Torticollis may be caused by:
- sitting or sleeping awkwardly, without sufficient support for your head
- poor posture, such as at a workstation that is not ergonomically suited to you
- carrying bags with unequal amounts of weight that cause your neck to strain, for example, a handbag on one side and heavy shopping bags on the other
- sleeping or sitting in a draughty room, where the neck is exposed to the cold.
Congenital muscular torticollis is more likely to happen in firstborn children. This may also be accompanied by a congenital hip dislocation. The cause is likely from the fetus’s position in the uterus resulting in injury to the neck muscles.
Acquired torticollis may be caused by irritation to the cervical ligaments from a viral infection, injury, or vigorous movement. Additional causes may include:
- Sleeping in an awkward position
- Neck muscle injury at birth
- Burn injury
- Any injury that causes heavy scarring and skin or muscle shrinkage
- Neck muscle spasm
Torticollis may also be a secondary condition that results from the following:
- Slipped facets (two small joints on the side of the spine)
- Herniated disk
- Viral or bacterial infection
You should see a doctor if:
- the pain is getting worse
- the pain doesn’t ease up in a week or so
- you have numbness, tingling or pins and needles in your arms or legs
- you start having difficulties with your bladder or bowel you have a fever as well as neck pain.
Torticollis in adults treatments
If you have torticollis (twisted, stiff neck) you can do a number of things to help manage the condition. Some of these measures include:
- Keep active and move your neck as normally as possible. You should try not to make sudden movements for a day or so, but then you try to carry on with your normal routines and move your head and neck to prevent it stiffening up.
- Try gently moving your neck in circles and moving it backwards, forwards and to either side to loosen the muscles and keep your neck supple.
- Get advice on suitable pain relief medicines.
- Apply a heat pad or ice pack, which may relieve neck stiffness and pain.
And to reduce your chances of future episodes of neck pain, you can:
- Improve your posture with gentle stretching exercises, such as those popular in activities such as yoga or Pilates.
- Arrange your work space so that your desk and chair are suitable for your needs. Ask for a footrest if you find that your knees and hips are not level and your feet do not sit flat on the ground. You may also need to move items that you use regularly closer to you, so that you don’t twist or reach too far to find items you need.
- Support your neck while sleeping with a support pillow, and sleep with just one pillow.
- Make sure your neck is supported in the car by adjusting the headrest so that it is at least at eye level and as close to the back of your head as possible. You can see images of the correct position on the Royal Society for the Prevention of Accidents website. Don’t drive if you can’t turn your head properly.
You should see a doctor if:
- the pain is getting worse
- the pain doesn’t ease up in a week or so
- you have numbness, tingling or pins and needles in your arms or legs
- you start having difficulties with your bladder or bowel you have a fever as well as neck pain.
Torticollis exercises
You should use the suggested exercises for at least 6–8 weeks to help prevent symptoms returning. If you have severe neck pain or weakness in your arms/hands, see your doctor.
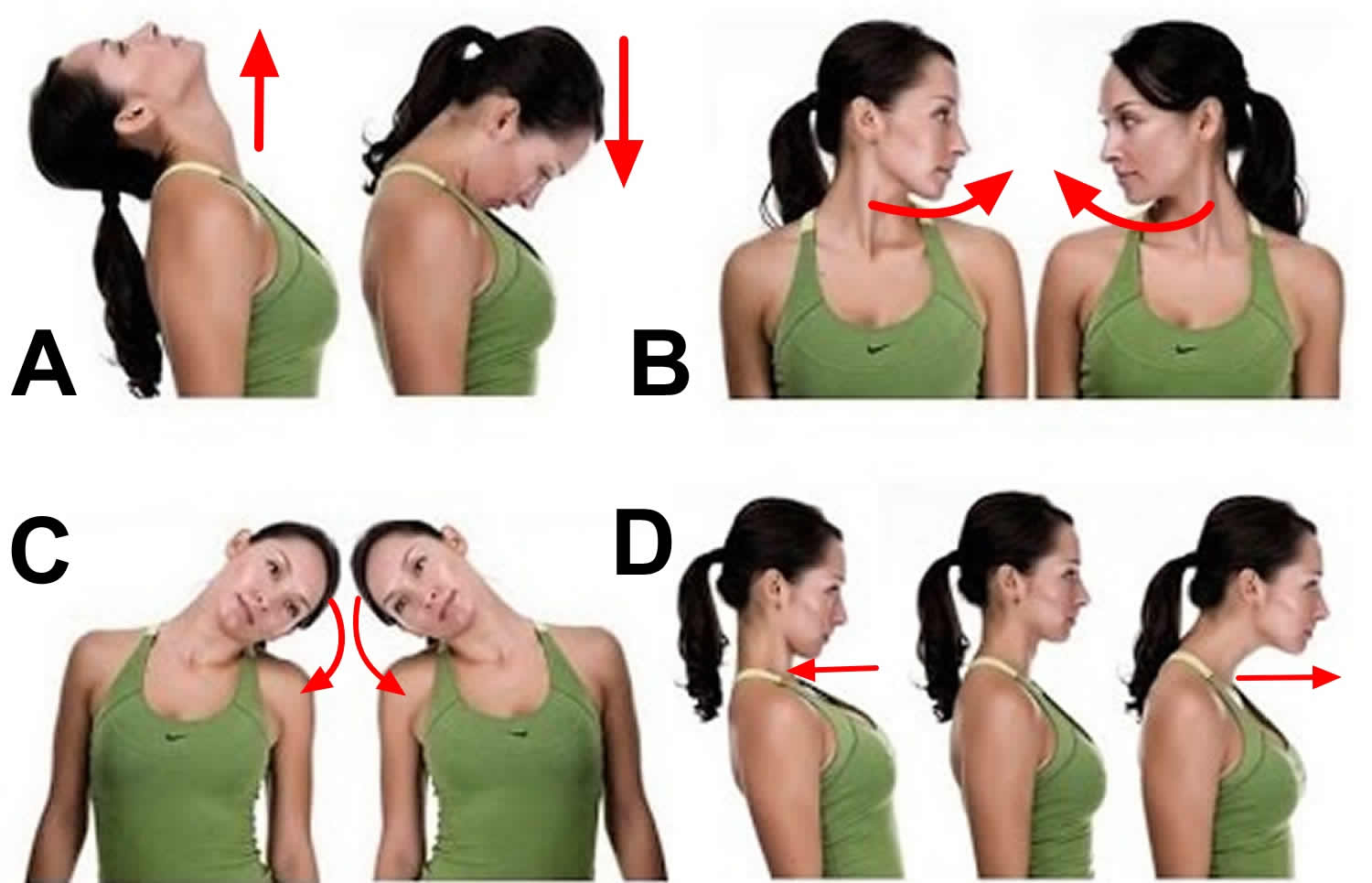
A. Neck tilt
Tilt your head down to rest your chin on your chest. Gently tense your neck muscles and hold for 5 seconds. Return to a neutral position and repeat 5 times.
B. Neck turn
Turn your head towards one side, keeping your chin at the same height and moving within comfortable limits. Gently tense your neck muscles and hold for 5 seconds. Return your head to the center and repeat on the opposite side. Repeat 5 times on each side.
C. Neck tilt (side to side)
Tilt your head down towards your shoulder, leading with your ear. Gently tense your neck muscles and hold for 5 seconds. Return your head to center and repeat on the opposite side. Repeat 5 times on each side.
D. Neck stretch
Keeping the rest of the body straight, push your chin forward so your throat is stretched. Gently tense your neck muscles and hold for 5 seconds. Return your head to the center and push it backwards, keeping your chin up. Hold for 5 seconds. Repeat 5 times.
Figure 1. Torticollis exercises
Spasmodic torticollis
Spasmodic torticollis also called cervical dystonia, is a painful and debilitating neurological movement disorder in which your neck muscles contract involuntarily, causing your head to twist or turn to one side. Spasmodic torticollis (cervical dystonia) can also cause your head to uncontrollably tilt forward or backward.
Spasmodic torticollis (cervical dystonia) is rare disorder that can occur at any age, cervical dystonia most often occurs in middle-aged people, women more than men. Approximately 3 in every 10,000 people – about 90,000 people in the United States – are known to suffer from spasmodic torticollis 1.
The exact cause of spasmodic torticollis (cervical dystonia) is unknown. Spasmodic torticollis can occur any time in life, although the symptoms most frequently occur between 25 and 55 years of age. Spasmodic torticollis is more common in women than men.
Onset sometimes comes after an injury to the head or neck, following an infection, or after taking certain medications. There also seems to be a genetic link, with 5 percent of patients reporting at least one relative with spasmodic torticollis and 50 percent demonstrating a family history of tremors in the head or hands.
First symptoms generally occur slowly or intermittently and are usually noticed when a person tried to keep his or her head straight, for example, while driving. Family or friends are often the first to see the sign, asking questions like, “Why does your head look like it’s on crooked?” Within two to five years, progression of the disease reaches a plateau without further worsening. The pain associated with spasmodic torticollis is almost always focused in one place, frequently the side of the neck or the back of the shoulders.
Spasmodic torticollis symptoms generally begin gradually and then reach a point where they don’t get substantially worse. Spasmodic torticollis is different in every person.
Spasmodic torticollis is caused by a dysfunction of the brain. The symptoms are caused by intermittent or sustained contractions of the muscles around the neck which control the position of your head. This causes your head to lean to one side, or be pulled forward or backward. The shoulders may also be uneven and some patients experience tremors in the head or arms. Spasmodic torticollis is usually accompanied by constant and extreme pain.
Spasmodic torticollis can resemble other disorders including Parkinson’s disease, epilepsy, muscular dystrophy and wry neck (acute torticollis – an acute episode of pain and spasm in the neck that resolves itself in days or weeks).
There are three distinct varieties of spasmodic torticollis:
- Tonic, in which the head turns to one side,
- Clonic, which involves the shaking of the head, and
- Mixed which involves both turning and shaking.
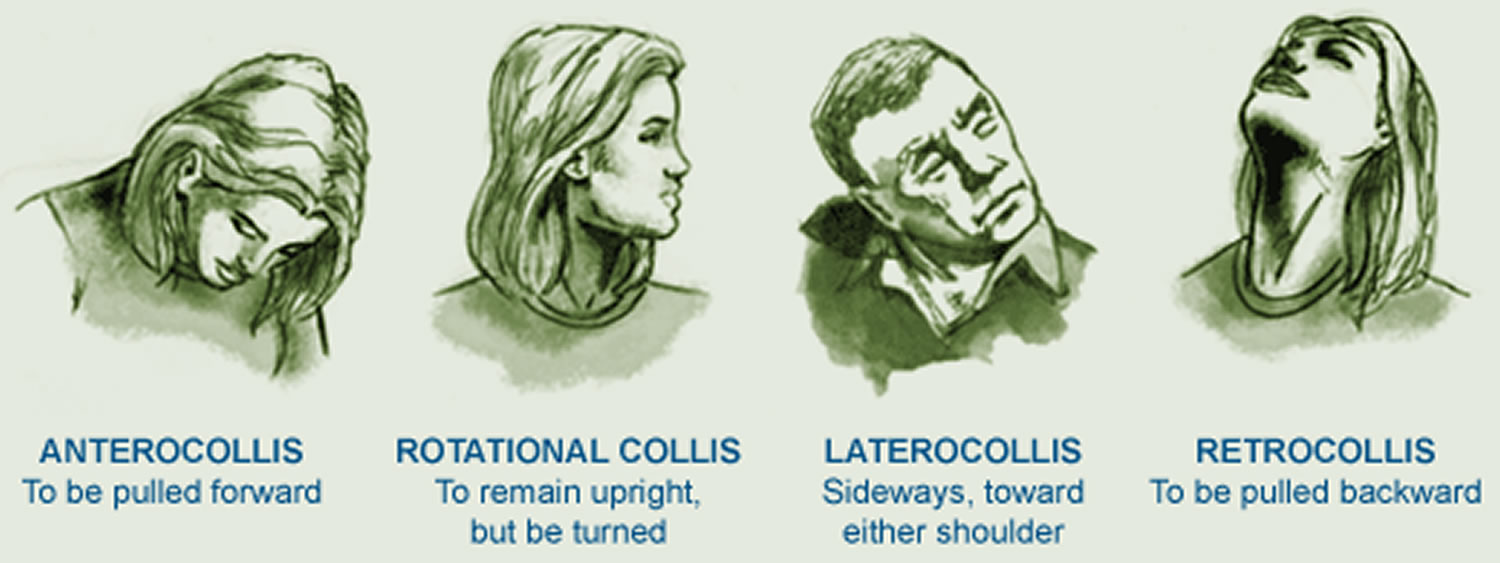
The turning of the head is generally considered to fall into one of four categories:
- Rotational, in which the head turns to one side or the other
- Laterocollis in which the head is pulled toward the shoulder
- Retrocollis in which the head is pulled to the back, or
- Anterocollis in which the head is pulled forward.
In fact, most people’s spasmodic torticollis is more complex, having a combination of “pulling” from among these four categories.
Spasmodic torticollis
Spasmodic torticollis can limit a person’s ability to function. As a localized disability this disorder does not directly affect other body systems. Because it can be more severe during times of anxiety or stress, spasmodic torticollis was once thought to be a psychiatric disorder. Research has shown, however, that while spasmodic torticollis does indeed seem to originate in the brain, it is clearly a neurological disorder rather than a psychiatric one.
Spasmodic torticollis (cervical dystonia) movements often disappear in sleep and may not reappear for a short time, any where between 10 minutes and 4 hours after waking. Because of this, many people find relief by taking breaks during the day to lie on their backs. Touching the opposite side of the face or chin may also cause spasms to cease temporarily.
Spontaneous recovery can be found in up to 20 percent of people within five years of the onset of symptoms, however this is more common in those whose symptoms begin before age 40 and/or who have a relatively mild case of spasmodic torticollis (cervical dystonia).
There is no cure for spasmodic torticollis (cervical dystonia). Spasmodic torticollis sometimes resolves without treatment, but sustained remissions are uncommon. Injecting botulinum toxin (Botox) into the affected muscles often reduces the signs and symptoms of spasmodic torticollis (cervical dystonia). Physical therapy, “alternative” treatments and stress reduction techniques may also help relief from the pain and disability. If none of those methods work for you, as a last resort, there are two surgical procedures called Denervation Surgery and Deep Brain Stimulation that may help. Surgery may be appropriate in a few cases.
Spasmodic torticollis signs and symptoms
The muscle contractions involved in spasmodic torticollis (cervical dystonia) can cause your head to twist in a variety of directions, including:
- Chin toward shoulder
- Ear toward shoulder
- Chin straight up
- Chin straight down
The most common type of twisting associated with spasmodic torticollis (cervical dystonia) is when your chin is pulled toward your shoulder. Some people experience a combination of abnormal head postures. A jerking motion of the head also may occur.
Many people who have spasmodic torticollis (cervical dystonia) also experience neck pain that can radiate into the shoulders. The disorder also can cause headaches. In some people, the pain from cervical dystonia can be exhausting and disabling.
Spasmodic torticollis complications
In some cases, the involuntary muscle contractions associated with spasmodic torticollis (cervical dystonia) can spread to nearby areas of your body. The most common locations include the face, jaw, arms and trunk.
People who have spasmodic torticollis (cervical dystonia) also may develop bone spurs that may reduce the amount of space in the spinal canal. This can cause tingling, numbness and weakness in your arms, hands, legs or feet.
Spasmodic torticollis causes
In most cases of spasmodic torticollis (cervical dystonia), the cause is unknown. Some people who have cervical dystonia have a family history of the disorder, so a genetic component may be a factor. Spasmodic torticollis (cervical dystonia) is sometimes linked to head, neck or shoulder injuries.
Risk factors for spasmodic torticollis
Risk factors for cervical dystonia include:
- Age. While the disorder can occur in people of any age, it most commonly begins after age 30.
- Your sex. Women are more likely to develop cervical dystonia than are men.
- Family history. If a close family member has cervical dystonia or some other type of dystonia, you are at higher risk of developing the disorder.
Spasmodic torticollis diagnosis
While the physical examination alone can often confirm a diagnosis of spasmodic torticollis (cervical dystonia), your doctor might suggest blood tests or magnetic resonance imaging (MRI) to rule out any underlying conditions causing your signs and symptoms.
Spasmodic torticollis treatment
There is no cure for spasmodic torticollis (cervical dystonia). In some people, signs and symptoms may disappear without treatment, but recurrence is common. Treatment focuses on relieving the signs and symptoms.
There are essentially three treatment options: botulinum toxin injections, oral medications, and, in some cases, surgery. These treatments may be used alone or in combination. In addition, physical therapy may provide a helpful complement to medical treatment. In some cases, if there is a trick such as touching the chin, a soft cervical collar may be beneficial.
Medications
Currently, there are no oral medications that are Food and Drug Administration (FDA) approved for use in dystonia. Among the oral medications used, dopaminergic agents (levodopa), anticholinergic agents (benztropine, trihexyphenidyl), baclofen and clonazepam are the most frequently used. These drugs are usually most effective in children with generalized dystonia. In adults, the side effects of these agents, including memory problems and sedation, often occur before an effective dose can be reached.
Botulinum toxin injections are the treatment of choice for cervical dystonia.
Botulinum toxin, a paralyzing agent (a neurotoxin) often used to smooth facial wrinkles, can be injected directly into the neck muscles affected by spasmodic torticollis (cervical dystonia). Botulinum toxin works by preventing the nerve from releasing a messenger, called acetylcholine, that tells the muscle to contract. This causes weakness of the muscle. The effect of botulinum toxin on the muscle begins approximately 2-3 days following injection, peaks at around 4 weeks, and provides relief for approximately 2-6 months. Botulinum toxin treatment is not a cure, but rather a symptom treatment. When the effect of botulinum toxin wears off, the symptoms of cervical dystonia recur and another injection is needed to sustain benefit. In order for botulinum toxin injections to be successful, it is critical that the injecting physician be well-versed in spasmodic torticollis (cervical dystonia), the functional anatomy of the neck muscles, and the type and doses of botulinum toxin to use.
There are now four brands of Botulinum toxin that have been approved by the Food and Drug Administration (FDA) for the treatment of individuals with cervical dystonia. There are three brands of botulinum toxin serotype A, including onabotulinumtoxinA (BOTOX, Allergan Inc.) abobotulinumtoxinA (Dysport, Tercica Inc) and incobotulinumtoxinA (Xeomin, Merz Pharmaceuticals). There is one formulation of botulinum toxin type B called rimabotulinumtoxinB (Myobloc, Solstice, US World Meds). These brands are not interchangeable, and each should be administered as a unique drug. At this time, there is no clinical data that supports the use of one over the other. The most frequent side effects from the injection are swallowing difficulties, pain and sometimes neck weakness. These side effects are usually mild and transient, lasting a few weeks. The FDA has a “black box” warning concerning the use of any of these toxins that indicates that the toxin can spread from the injection site. However, with the doses used for cervical dystonia the clinical effects of spread of toxin are rare.
Most people with spasmodic torticollis (cervical dystonia) see an improvement with these injections, which usually must be repeated every three to four months.
To improve results or to help reduce the dosage and frequency of botulinum toxin injections, your doctor might also suggest oral medications that have a muscle-relaxing effect.
Physical Therapy
Sensory tricks, such as touching the opposite side of your face or the back of your head, may cause spasms to stop temporarily. Different sensory tricks work for different people, but they often lose effectiveness as the disease progresses.
Heat packs and massage can help relax your neck and shoulder muscles. Exercises that improve neck strength and flexibility may also be helpful.
The signs and symptoms of spasmodic torticollis (cervical dystonia) tend to worsen when you’re stressed, so learning stress management techniques is also important.
Surgical and other procedures
If less invasive treatments don’t help, your doctor might suggest surgery. Procedures may include:
- Deep brain stimulation. In this procedure, a thin wire is guided into the brain through a small hole cut into the skull. The tip of the wire is placed in the portion of the brain that controls movement called the globus pallidus on both sides. Electrical pulses are sent through the wire to interrupt the nerve signals making your head twist. Deep brain stimulation surgery is effective for cervical dystonia and may be appropriate for patients who lose their response to botulinum toxin, or have a form of cervical dystonia that is difficult to treat with the injections, in particular anterocollis. Although the precise mechanism is not clear, the electrical impulses seem to “reset” the brain and improve the dystonic movements. After the deep brain stimulation is placed, the stimulators are programmed for the optimal outcome.
- Cutting the nerves (denervation surgery). Another option is to surgically sever the nerves carrying the contraction signals to the affected muscles.
Coping and support
Severe cases of cervical dystonia may make you feel uncomfortable in social situations or even limit your abilities to accomplish everyday tasks such as driving. Many people with cervical dystonia feel isolated and depressed.
Remember that you’re not alone. A number of organizations and support groups are dedicated to providing information and support for you and your family — whether you have the disorder or you have a friend or family member who does.
Your doctor may be able to suggest support groups available in your area, or there are a number of good sites on the internet with information about local support groups.
- National Spasmodic Torticollis Association: http://www.torticollis.org/
- Dystonia Europe: https://dystonia-europe.org/
- Dystonia Medical Research Foundation: https://www.dystonia-foundation.org/
- Dystonia Society UK: https://www.dystonia.org.uk/
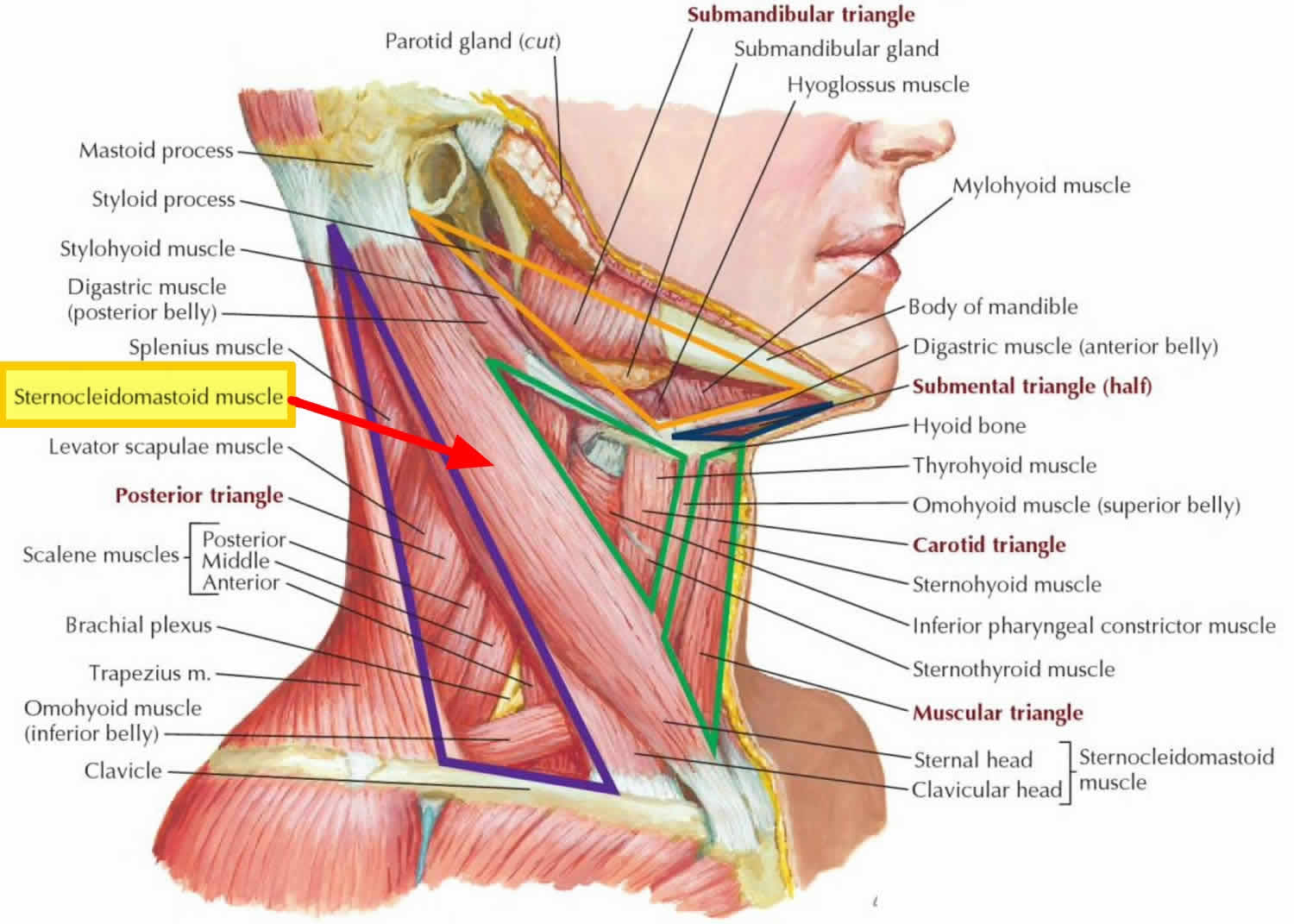
Figure 2. Sternocleidomastoid muscle
Torticollis in baby and children
In general, torticollis is classified as either congenital (present at birth) or acquired (occurring later in infancy or childhood). By far the most common type is congenital muscular torticollis. Although children have this when they are born, parents may not notice it until children are several weeks old, as they start to gain more control of their head movement.
- Congenital muscular torticollis responds very well to physical therapy, especially when it’s started early. Sometimes it is associated with plagiocephaly, a common and treatable condition in which there is asymmetry in the shape of the head and face. This happens because the forces of gravity pull unevenly on a baby’s tilted head, causing a flattened appearance on one side of the skull or face.
- Acquired torticollis typically occurs in the first 4 to 6 months of childhood or later. It may come on quickly or slowly. In contrast to congenital muscular torticollis, there is usually no facial asymmetry with acquired torticollis. Acquired torticollis can be benign (not serious) or a sign of more serious health issues. Because the causes can be so different, it is very important to act quickly so that your child can get the proper care and treatment.
Note: Pediatric torticollis is different from another condition, called spasmodic torticollis, that affects adults.
Associated anomalies 2:
- 6% of children will have associated musculoskeletal abnormalities: hip dysplasia, metatarsus adductus, talipes equinovarus, C1-C2 subluxation
- Facial asymmetry
- Skull deformities (plagiocephaly) can result because the baby will repeatedly rest his/her head on one side
Check your child’s bed if he or she first complained of torticollis after waking up. A lumpy pillow or toys in the bed can create an uncomfortable night of sleep. (Remember, to help prevent SIDS (sudden infant death syndrome), never let babies younger than 12 months old sleep with pillows, blankets, crib bumpers, or toys.) Making sure the sleep space is safe and comfortable may help the torticollis go — and stay — away.
Torticollis in baby and children causes
Because there are different types of torticollis, it is important to know the root cause so that your child can get the proper care and treatment as quickly as possible 3.
Congenital muscular torticollis
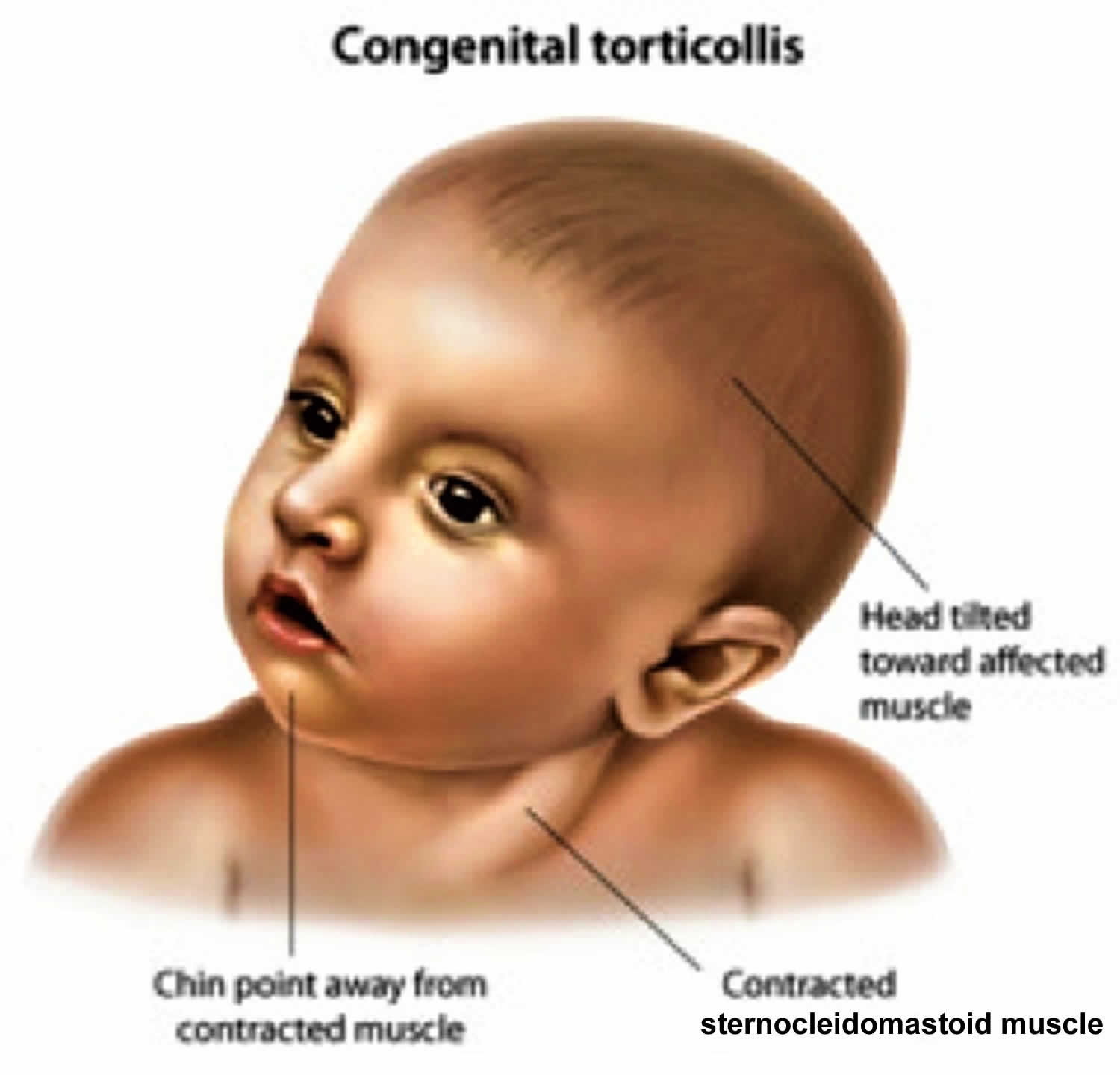
For children with congenital muscular torticollis, the most common form of pediatric torticollis, the sternocleidomastoid muscle muscle becomes shortened and contracted 4. The sternocleidomastoid muscle muscle runs along each side of the neck and controls how the head moves — side to side, and up and down. Congenital muscular torticollis presents in newborn infants or young children with reported incidence ranging from 0.3% to 2%. Owing to effective shortening of sternocleidomastoid muscle on the involved side there is ipsilateral head tilt and contralateral rotation of the face and chin (see Figure 3).
There are a few common reasons why the sternocleidomastoid muscle muscle may have become contracted and cause your child’s head to tilt to one side:
- The way your baby was positioned in the womb before birth
- Abnormal development of the sternocleidomastoid muscle muscle
- Trauma or damage to the muscle during birth
In far less common cases, congenital muscular torticollis may occur as a symptom of other underlying conditions, including:
- congenital bony abnormalities of the upper cervical spine, with subluxation (abnormal rotation) of the C1 vertebrae over the C2 vertebrae in the cervical spine (the part of the spine that encompasses the neck).
- congenital bony abnormalities of the upper cervical spine, which are most often associated with other congenital skeletal anomalies, such as:
- shortened neck
- short limbs (arms and legs)
- dwarfism
- congenital webs of skin running along the side of the neck
- Klippel-Feil syndrome, a rare birth defect that causes some of the neck vertebrae to fuse together
- Achondroplasia, a bone growth disorder
- Multiple epiphyseal dysplasia, a disease that affects the development of bone and cartilage in the long bones of the arms and legs
- Morquio’s syndrome, an inherited metabolic disorder that prevents the body from breaking down sugar molecules
Figure 3. Congenital muscular torticollis
Acquired torticollis
For children who have acquired torticollis, the causes vary widely and range in severity from benign (not serious) to very serious. Some causes of acquired torticollis include:
- a mild (usually viral) infection
- minor trauma to the head and neck
- gastroesophageal reflux (GERD)
- respiratory and soft-tissue infections of the neck
- abnormalities in the cervical spine (such as atlantoaxial subluxation)
- vision problems (called ocular torticollis)
- abnormal reaction to certain medications (called a dystonic reaction)
- spasmus nutans (a usually benign condition that causes head bobbing along with uncontrolled eye movements)
- Sandifer syndrome (a rare condition combining gastroesophageal reflux with spasms in the neck)
Torticollis in baby and children can stems from a musculoskeletal problem or an underlying non-musculoskeletal pathology 5. Musculoskeletal reasons for infantile torticollis include a tumor in the sternocleidomastoid muscle, an imbalance in the neck musculature or a dysfunction in the craniocervical junction 6. In addition, abnormalities of the cervical spine, like the Klippel-Feil syndrome, can cause torticollis 7. The non-musculoskeletal reasons for infantile torticollis could be ocular, neurological or due to auditory problems 7.
The most common ocular causes of torticollis in all population ages are a congenital paralytic squint and congenital nystagmus 8. Kuschner 9 stated that the underactivity of the superior oblique muscle is the most common ocular cause of torticollis in all ages. It is also stated by Kekunnaya 10 that 74% of all patients with unilateral paresis of the superior oblique muscles have torticollis. In a patient with true ocular torticollis, the condition results from the body trying to assist its vision in one or more ways 8: to improve vision, to bring the field of vision into a central area, to reduce eye discomfort, to strengthen binocular vision and to protect and relieve the eye from pain. With unilateral paresis of the superior oblique muscle the eye looks up and in slight adduction when looking straight ahead; a child will usually flex its neck laterally to the opposite side to compensate, but variations can occur 8,
The reported prevalence of congenital muscular torticollis with a tumor in the sternocleidomastoid muscle has ranged from 0.3% to 2% 11. The prevalence of muscular imbalance and dysfunction in the craniocervical junction causing torticollis is unknown.
The prevalence of the non-musculoskeletal causes of torticollis in children is unknown. Ballock 12 studied 288 subjects with a mean age of 22.7 months and found that non-musculoskeletal causes of torticollis accounted for 18.4% of the total. Of all the non-musculoskeletal causes 22.6% had ocular cause. Another study, a prospective consecutive case series from 2005 13, investigated the prevalence of different causes of torticollis in children presenting to primary care pediatricians. Of the 29 patients below the age of one year, 19 had orthopedic etiology, 4 ocular and 6 unknown problems. This is a small number of patients, but is, however, the only prospective study done on the prevalence of torticollis in infants 14.
Musculoskeletal and non-musculoskeletal torticollis can cause secondary functional deficits like unilateral breastfeeding problems and asymmetrical use of their hands 15. In addition, changes in form can develop because of torticollis, such as deformational plagiocephlay, facial scoliosis and infantile scoliosis 7.
Figure 4. Torticollis baby

Torticollis in baby and children signs and symptoms
Congenital muscular torticollis
- The child has a limited range of motion in the head and neck.
- The head tilts to one side while the chin tilts to the other.
- A small, pea-sized lump (or “pseudo tumor”) is sometimes found on the sternocleidomastoid muscle.
- Asymmetries of the head and face, indicating plagiocephaly, may also be present.
- Musculoskeletal problems, such as hip dysplasia, are sometimes present.
Acquired torticollis
- There is limited range of motion in the head and neck.
- The head tilts to one side while the chin tilts to the other.
- With a condition called benign paroxysmal torticollis, there may be recurrent episodes, or “attacks,” of head tilting; often these attacks are accompanied by other symptoms, such as vomiting, irritability and/or drowsiness.
- Additional symptoms vary according to the cause of the torticollis.
Note: Children who develop torticollis that is associated with neck pain after trauma (even minor trauma) should be evaluated right away to make sure they do not have any subluxation of the C1 or C2 vertebrae. In addition, children who develop painful torticollis at the same time as a fever that is caused by an infection in the pharynx (cavity behind the nose, mouth and larynx) or retropharyngeal space (the area behind the pharynx) need to see a doctor immediately. If left untreated, these complications can lead to a rare disorder called Grisel’s syndrome.
Long term effects of torticollis in baby
If the baby suffers sustained torticollis then the following collateral problems may emerge:
Plagiocephaly: Torticollis may cause positional plagiocephaly, where an infant’s head flattens because of repeated sleeping on one side due to neck tilt 16. The condition needs to be managed along with torticollis. For plagiocephaly, a baby will have to undergo a helmet therapy where a helmet-shaped head brace gently squeezes the skull bone back to shape (see Figure 6).
Facial asymmetry: Facial asymmetry happens when one side of a face is excessively dissimilar to the other side. Since the infant will tend to tilt the head in one direction, the facial muscles and attributes slowly align the wrong way. Asymmetry can happen with any type of torticollis but is most common in ocular torticollis. Correction of torticollis helps improve the condition.
Skeletal disorders: Infants suffering from torticollis have a significantly higher risk of developing other skeletal problems (Torticollis. https://pedclerk.bsd.uchicago.edu/page/torticollis()). A baby with torticollis will tend to align other parts of the body the wrong way to counterbalance the effects of tilted head. The voluntary skeletal misalignment causes bones to fuse incorrectly thus leading to skeletal complications like hip dysplasia (hip dislocation), metatarsus adductus (deformed foot), and talipes equinovarus (bent foot).
Timely initiation of torticollis treatment is all you need to do to prevent the above conditions. Parents can always play a part in helping the baby come out of the problem.
How is torticollis in baby and children diagnosed?
Your doctor will obtain a full medical history and perform a comprehensive physical exam of your child. When an infant is believed to have torticollis along with an underlying skeletal abnormality, x-ray imaging or magnetic resonance imaging (MRI) may be necessary to confirm the diagnosis.
Medical history
Your child’s doctor will begin by asking you a series of questions that will help determine the type of torticollis your child has. Questions may include:
- How old is your child?
- When did the torticollis develop?
- Did the torticollis happen suddenly or slowly?
- Was there any trauma to the head or neck?
- Does your child have a fever?
- Does your child have an infection?
- Has your child had any surgeries in the head and/or neck?
- Have you noticed any other symptoms?
- Has your child been exposed to any medications or drugs?
Physical examination
Your child’s doctor will perform a complete physical and neurological exam to determine the type of torticollis she has. This exam involves:
- checking the range of motion of the head and neck
- palpating (examining by touch) the sternocleidomastoid muscle muscle in the neck to see if there is a small lump, or “pseudo tumor,” that happens in about one in three cases of congenital muscular torticollis
- looking for the presence or absence of asymmetry or unevenness of the face and head to check for a condition called plagiocephaly (it’s important to check for this because the child’s head and face may develop unevenly due to the pull of gravity upon the tilted head)
- checking your baby’s hips and how they rotate (this is because there is a slightly higher chance that babies with congenital muscular torticollis may develop hip dysplasia)
Your doctor may also request other imaging studies, such as ultrasound, to look for certain abnormalities in the spine that may be a sign of rare but serious health problems.
How is torticollis in baby and children treated?
Congenital muscular torticollis
Once your doctor has determined that your child has congenital muscular torticollis, you and your child will begin a program of physical therapy designed to lengthen the shortened sternocleidomastoid muscle.
The treatment works best when initiated before the age of six months when the baby has a flexible musculoskeletal system. Whereas physical exercises can take six months or more to show positive results, surgical intervention shows immediate results, but in the latter case, the baby will have to undergo physical therapy for more than three months to reinforce the muscle’s position. In either case, it can take months before the infant holds his head straight. It is worth the wait because if left untreated, torticollis can lead to other complications.
Torticollis can be helped with physical therapy. Your physical therapist will give you specific home program activities in addition to these general recommendations. The home program will include:
- stretches
- active strengthening exercises
- developmental activities
Physical therapy programs will include specific exercises you can do at home on a set schedule, such as during diaper changes. In addition, you will learn how to hold your baby and tailor his environment to encourage him to turn his head and stretch the sternocleidomastoid muscle.
If home therapy doesn’t resolve the limited range of movement in 4-6 weeks, outpatient physical therapy is recommended
The majority of cases resolve after a few months of stretching therapy and careful positioning:
- Positioning
- Hold the child so he/she must rotate the chin towards the affected side while feeding
- Position the child so that he/she must rotate the chin toward the affected side to see his/her toys or to view the room
- Stretching exercises: for young babies, parents can do passive stretching exercises to gently stretch the shortened sternocleidomastoid muscle; older babies (> 6-8 months) are treated with active stretching exercises
- More tummy time. Tummy time promotes strengthening of the neck, shoulder, arm, and back muscles, in addition to preventing flattening of the back of your baby’s head. Tummy time is recommended for at least 15 minutes, 4 times a day. If your baby is unable to tolerate this position for the full time, use shorter intervals of tummy time, with increased frequency throughout the day. Supporting your child on your chest, across your lap, or propped on a pillow helps your baby tolerate tummy time more easily. It is important that your baby is always awake and supervised during tummy time.
- Engage your child in play activities that promote the use of both hands and both legs. Babies commonly play by bringing hands together and bringing their feet up to their hands. You can help your baby bring both hands to midline and then reach for both feet. Encourage your baby to reach for toys and rattles equally with either hand.
- Encourage your child to turn his/her head to look to both sides. Toy placement influences the direction in which your baby looks. You want to place toys on both sides of your baby so that they are able to actively look to both sides. Perform this activity with your baby on his/her belly and back. Toys with sounds and lights are especially helpful. Your baby should be able to actively turn his or her head from side to side without limitations. When you place your baby on his/her back to sleep, alternate the side to which the head turns.
- A soft “TOT collar” can be used as an adjunctive therapy once the child is 4-5 months old
- The age at which children are referred to therapy correlates with successful conservative treatment (children who are referred earlier do better)
- Most children require < 6 months of physical therapy
- Infants should be re-evaluated every 2-4 weeks.
Your child’s physical therapist may recommend using a simple device called a “TOT collar.” TOT stands for Tubular Orthosis for Torticollis, which is really just a small piece of plastic tubing that fits around your baby’s neck. The TOT collar is designed to help babies straighten their heads and strengthen their neck muscles. Your physical therapist will teach you the proper way to use a TOT collar.
Figure 5. TOT collar

Children who have torticollis with asymmetry of the face and head, known as plagiocephaly, usually respond very well to non-surgical, minimally invasive interventions like:
- customized, corrective helmets and molding cups
- sleep position changes
- special exercises
Sometimes other measures, such as surgery, are required to correct the shortened sternocleidomastoid muscle in torticollis and any asymmetry that may happen with plagiocephaly.
Figure 6. Baby helmet therapy for plagiocephaly

Chiropractic treatment or spinal manipulative therapy that focuses on bone adjustment to relieve tension on muscles and nerves. The alternative medicine works well with other forms of non-invasive treatments such as physiotherapy. In a chiropractic adjustment, the chiropractor (musculoskeletal health practitioner) uses his hands to adjust the baby’s spine with calculated and precise moves 14. It is not a standard bone setting as the practitioner will conduct a detailed assessment before doing the adjustment. Chiropractic adjustments have been found to be effective at curing musculoskeletal torticollis, and some experts believe it should be considered an option for torticollis treatment in infants 14.
Botox: Botulinum injections, also known as Botox, can help relieve the tautness of sternocleidomastoid muscle muscle and reduce the head tilt 17. Botox injections are formulated using botulinum toxin secreted by the bacteria called Clostridium botulinum. The dose is directly administered to the sternocleidomastoid muscle muscle to release its tension. An infant may have to undergo more than one injection depending on the intensity of torticollis.
Botox is considered a midway between physical therapy and surgery since it is suitable for infants, who do not respond to physiotherapy but the condition is not severe enough for surgery. Botox is used for the treatment of spasmodic torticollis in adults, and researchers find botulinum injections effective even for babies with torticollis 17. However, the treatment is ideal for infants above six months of age.
Surgery: Surgery is the last option if the baby does not respond to any other interventions. The severity of initial presentation is not a predictor of whether a child will develop persistent torticollis and need surgical intervention. Surgery is recommended when children have persistently limited range of motion (loss of > 30 degrees of movement) of the neck, significant plagiocephaly, or facial asymmetry after 6 to 12 months of age. The surgery for torticollis in infants aims to reduce the sternocleidomastoid muscle tension and achieve a complete neck extension without any tilt. The exact surgical process depends on the severity of the torticollis. A standard operating procedure involves making an incision at the lower attachment point of sternocleidomastoid muscle on the chest. Here, the muscle is stripped from the bone, allowed to relax, and reattached with the corrected neck position 18. Surgical outcomes are excellent overall.
Surgical procedures are followed by intensive physiotherapy sessions that help reinforce the stretchiness of the muscle. The infant will also have to wear a brace to maintain the correct position of the head. Once the muscle heals and sets into place, the infant can be free of torticollis.
Acquired torticollis
Your child’s treatment plan will vary based on the cause of the torticollis. Some common therapies include:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) to relieve pain and discomfort related to musculoskeletal injury e.g., ibuprofen
- Use warm compresses over the part of the neck that hurts when moved. (Never apply heat packs directly to the skin. Instead, keep a towel or cloth between the heat and the skin.) Only use heat for 20 minutes at a time. You can apply warm compresses every 3–4 hours.
- If the pain does not ease with ibuprofen, the doctor may prescribe a muscle relaxant for a few days.
- For older kids, a soft neck collar may help to keep the neck from moving too quickly.
- Antibiotic therapy for children whose torticollis is caused by infection
- Medications to stop gastroesophageal reflux for children whose primary cause of torticollis is reflux
Infant torticollis
A bad night’s sleep can mean waking up with a stiff neck, which makes it hard or painful to turn your head. This is called torticollis (twisted neck or wry neck).
In newborns, torticollis can happen due to positioning in the womb or after a difficult childbirth. This is called infant torticollis or congenital muscular torticollis 19.
It can be upsetting to see that your baby has a tilted head or trouble turning his or her neck. But most with babies don’t feel any pain from torticollis. And the problem usually gets better with simple position changes or stretching exercises done at home.
What causes infant torticollis?
Torticollis is relatively common in newborns. Boys and girls are equally likely to develop the head tilt. It can be present at birth or take up to 3 months to develop.
No one knows why some babies get torticollis and others don’t. Most doctors believe it could be related to the cramping of a fetus inside the uterus or abnormal positioning (such as being in the breech position, where the baby’s buttocks face the birth canal). The use of forceps or vacuum devices to deliver a baby during childbirth also makes a baby more likely to develop it.
These things put pressure on a baby’s sternocleidomastoid muscle (see Figure 2 above). This large, rope-like muscle runs on both sides of the neck from the back of the ears to the collarbone. Extra pressure on one side of the sternocleidomastoid muscle can cause it to tighten, making it hard for a baby to turn his or her neck.
Some babies with torticollis also have developmental dysplasia of the hip, another condition caused by abnormal positioning in the womb or a difficult childbirth.
Infant torticollis signs and symptoms
Babies with torticollis will act like most other babies except when it comes to activities that involve turning. A baby with torticollis might:
- tilt the head in one direction (this can be hard to notice in very young infants)
- prefer looking at you over one shoulder instead of turning to follow you with his or her eyes
- if breastfed, have trouble breastfeeding on one side (or prefers one breast only)
- work hard to turn toward you and get frustrated when unable turn his or her head completely
Some babies with torticollis develop a flat head (positional plagiocephaly) on one or both sides from lying in one direction all the time. Some might develop a small neck lump or bump, which is similar to a “knot” in a tense muscle. Both of these conditions tend to go away as the torticollis gets better.
How is infant torticollis diagnosed?
Your doctor will do a physical exam to see how far your baby can turn his or her head.
Infant torticollis treatment
If your baby does have torticollis, the doctor might teach you neck stretching exercises to practice at home. These help loosen the tight sternocleidomastoid muscle and strengthen the weaker one on the opposite side (which has weakened due to underuse). This will help to straighten out your baby’s neck.
Sometimes, doctors suggest taking a baby to a physical therapist for further treatment.
After treatment has started, the doctor may examine your baby every 2 to 4 weeks to see if the torticollis is getting better.
Helping your baby at home
Encourage your baby to turn his or her head in both directions. This helps loosen tense neck muscles and tighten the loose ones. Babies cannot hurt themselves by turning their heads on their own.
- Positioning
- Hold the child so he/she must rotate the chin towards the affected side while feeding
- Position the child so that he/she must rotate the chin toward the affected side to see his/her toys or to view the room
Here are some exercises to try:
- When your baby wants to eat, offer the bottle or your breast in a way that encourages your baby to turn away from the favored side.
- One way to rectify the baby’s neck tilt is to encourage them to turn in the opposite direction. Use food or toys to lure the infant to turn in order to stimulate the natural and voluntary extension of the neck muscle. During feeds, the mother can place the bottle or feed the baby on the breast on the opposite direction of torticollis. Such stimulation relaxes and conditions the sternocleidomastoid muscle muscle thus providing relief from torticollis in the long run 20.
- When putting your baby down to sleep, position him or her to face the wall. Since babies prefer to look out onto the room, your baby will actively turn away from the wall and this will stretch the tightened muscles of the neck. Remember — always put your baby to sleep on his or her back to help prevent SIDS (sudden infant death syndrome).
- During play, draw your baby’s attention with toys and sounds to make him or her turn in both directions.
Don’t forget “Tummy Time”
Laying your baby on the stomach for brief periods while awake (known as “tummy time”) is an important exercise because it helps strengthen neck and shoulder muscles and prepares your baby for crawling.
This exercise is especially useful for a baby with torticollis and a flat head — and can actually help treat both problems at once.
Here’s how to do it:
- Lay your baby on your lap for tummy time. Position your baby so that his or her head is turned away from you. Then, talk or sing to your baby and encourage him or her to turn and face you. Practice this exercise for 10 to 15 minutes.
Looking ahead
Most babies with torticollis get better through position changes and stretching exercises. It might take up to 6 months to go away completely, and in some cases can take a year or longer.
Stretching exercises to treat torticollis are most likely to work well if started when a baby is between 3 to 6 months old. If you find that your baby’s torticollis is not improving with stretching, talk to your doctor. Your baby may be a candidate for muscle-release surgery, a procedure that cures most cases of torticollis that don’t improve.
- What is Spasmodic Torticollis. http://www.torticollis.org/spasmodic-torticollis/[↩]
- Torticollis. https://pedclerk.bsd.uchicago.edu/page/torticollis[↩]
- Torticollis Symptoms and Causes. http://www.childrenshospital.org/conditions-and-treatments/conditions/t/torticollis/symptoms-and-causes[↩]
- Nilesh K, Mukherji S. Congenital muscular torticollis. Annals of Maxillofacial Surgery. 2013;3(2):198-200. doi:10.4103/2231-0746.119222. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3814673/ [↩]
- Ballock R.T., Song K.M. The prevalence of nonmuscular causes of torticollis in children. J Pediatr Orthop. 1996;16(4):500–504.[↩]
- Hüter-Becker A., Dölken M. Thieme; Stuttgard: 2005. Physiotherapie in der Pädiatrie; pp. 429–430.[↩]
- Hefti F. 2nd ed. Springer International Publishing AG; Heidelberg: 2006. Kinderorthopädie in der Praxis; pp. 117–120.[↩][↩][↩]
- Mitchell P.R. Ocular torticollis. Trans Am Ophthalmol Soc. 1999;97:697–769.[↩][↩][↩]
- Williams C.R.P., O`Flynn E., Clarce N.M.P., Morris R.J. Torticollis secondary to ocular pathology. J Bone Joint Surg (Br) 1996;78(4):620–624.[↩]
- Kekunnaya R., Isenberg S.J. Effect of strabismus surgery on torticollis caused by congenital superior oblique palsy in young children. Indian J Ophthalmol. 2014;62(3):322–326[↩]
- Cheng J.C.Y., Wong M.W.N., Tang S.P., Chen T.M., Shum S.L.F., Wong E.M.S. Clinical determination of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants: A prospective study of eight hundred and twenty-one cases. J Bone Joint Surg Am. 2001;83(5):679–687.[↩]
- Ballock R.T., Song K.M. The prevalence of nonmuscular causes of torticollis in children. J Pediatr Orthop. 1996;16(4):500–504. https://www.ncbi.nlm.nih.gov/pubmed/8784706[↩]
- Nucci P., Kushner B.J., Serafino M., Orzalesi N. A multi-disciplinary study of the ocular, orthopaedic and neurologic causes of abnormal head postures in children. Am J Ophthalmol. 2005;140(1):65–68.[↩]
- Hobaek Siegenthaler M. Chiropractic Management of Infantile Torticollis With Associated Abnormal Fixation of One Eye: A Case Report. Journal of Chiropractic Medicine. 2015;14(1):51-56. doi:10.1016/j.jcm.2014.12.003. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4371108/[↩][↩][↩]
- Biedermann H. Elsevier Urban und Fischer; München: 2006. Manuelle Therapie bei Kindern; pp. 253–254.[↩]
- Torticollis and plagiocephaly in infancy: Therapeutic strategies. Pediatric Rehabilitation, January 2006; 9(1): 40–46. http://regispthomeexerciseprograms.pbworks.com/f/torticollis%20tx-systematic%20review.pdf[↩]
- Botulinum Toxin Type A in the Treatment of Children with Congenital Muscular Torticollis. Am J Phys Med Rehabil 2005;84:813–816. http://regispthomeexerciseprograms.pbworks.com/f/botox+for+torticollis.pdf[↩][↩]
- Nilesh K, Mukherji S. Congenital muscular torticollis. Annals of Maxillofacial Surgery. 2013;3(2):198-200. doi:10.4103/2231-0746.119222. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3814673/[↩]
- Infant Torticollis. https://www.childrensmn.org/educationmaterials/parents/article/13011/infant-torticollis[↩]
- Top 5 Tips for Helping a Baby Who has Torticollis at Home. https://www.hss.edu/playbook/top-5-tips-for-helping-a-baby-who-has-torticollis-at-home/[↩]





{kind=link}