What is a trochanter
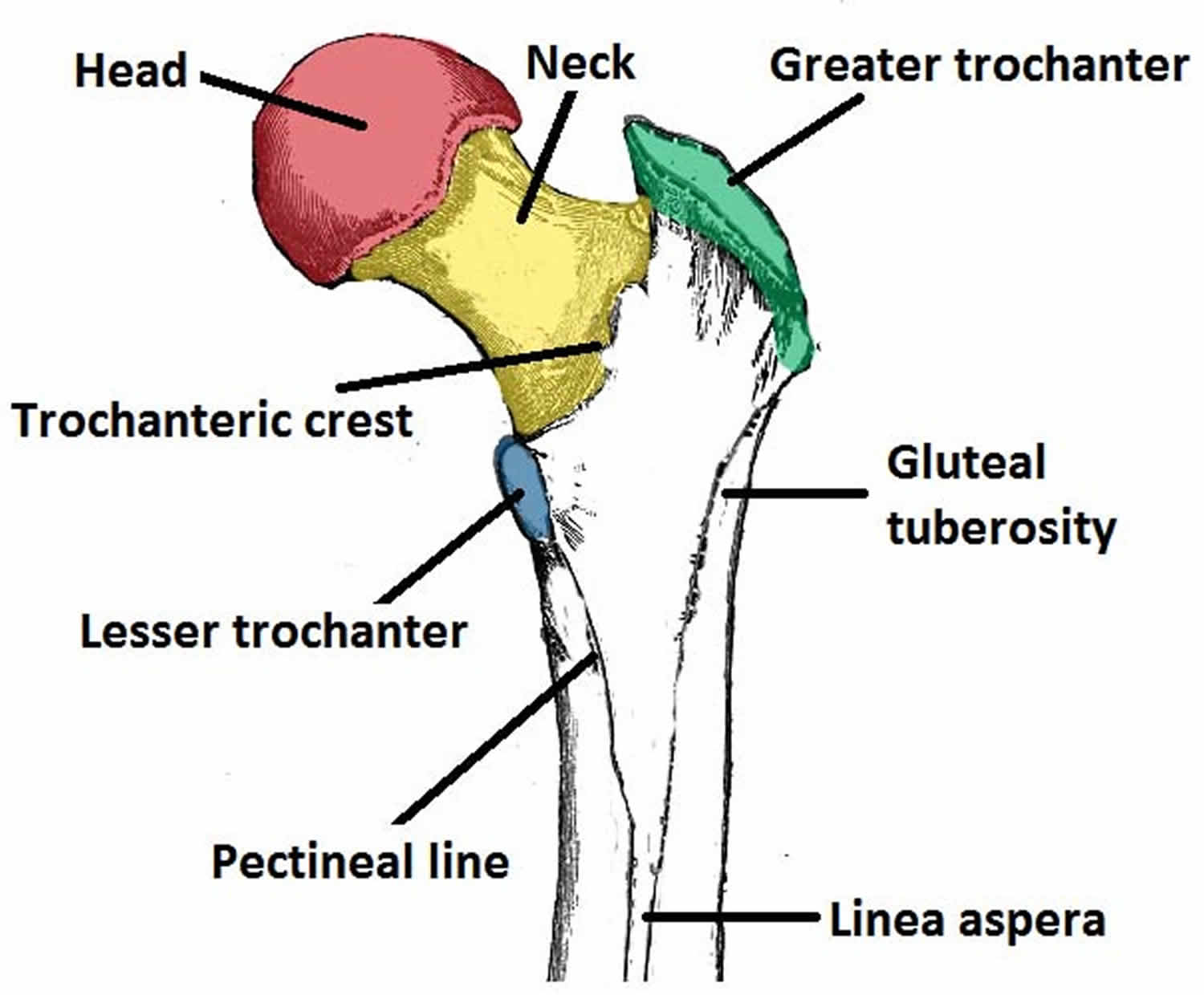
Trochanter is a very large, blunt, irregularly shaped process or projection, the only examples are the greater trochanter and lesser trochanter of femur. The greater trochanter and lesser trochanter are projections from the junction of the neck and shaft of femur that serve as points of attachment for the tendons of some of the thigh and buttock muscles (see Figure 1). The greater trochanter is the most lateral palpable projection of bone that originates from the anterior aspect, just lateral to the neck of femur and seen anterior to the hollow on the side of the hip. The greater trochanter is a landmark commonly used to locate the site for intramuscular injections into the lateral surface of the thigh. Greater trochanter is the site of attachment for many of the muscles in the gluteal region, such as gluteus medius, gluteus minimus and piriformis. The vastus lateralis originates from this site. An avulsion fracture of the greater trochanter can occur as a result of forceful contraction of the gluteus medius.
The lesser trochanter (smaller than the greater trochanter) is inferior and medial to the greater trochanter. Lesser trochanter projects from the posteromedial side of the femur, just inferior to the neck-shaft junction. Lesser trochanter is the site of attachment for iliopsoas (forceful contraction of which can cause an avulsion fracture of the lesser trochanter).
Between the anterior surfaces of the trochanters is a narrow intertrochanteric line (Figure 1). Intertrochanteric line is a ridge of bone that runs in an inferomedial direction on the anterior surface of the femur, spanning between the two trochanters. After intertrochanteric line passes the lesser trochanter on the posterior surface, it is known as the pectineal line. Intertrochanteric line is the site of attachment for the iliofemoral ligament (the strongest ligament of the hip joint). It also serves as the anterior attachment of the hip joint capsule.
Intertrochanteric crest is a ridge of bone that connects the two trochanters. Intertrochanteric crest is located on the between the posterior surfaces of the trochanters. There is a rounded tubercle on its superior half called the quadrate tubercle; where quadratus femoris attaches.
Figure 1. Greater trochanter and lesser trochanter of femur
Greater trochanter pain
Greater trochanteric pain syndrome also called trochanteric bursitis or hip bursitis (inflammation of bursa), is pain that occurs on the outside of your hip over the greater trochanter. Bursa, is small, jelly-like sac that is located throughout your body, including around the shoulder, elbow, hip, knee, and heel. Bursa contains a small amount of fluid, and are positioned between bones and soft tissues, acting as cushions to help reduce friction.
Bursitis is inflammation of the bursa. There are two major bursae in the hip that typically become irritated and inflamed. One bursa covers the bony point of the hip bone called the greater trochanter. Inflammation of this bursa is called trochanteric bursitis.
The main symptom of trochanteric bursitis is pain at the point of the hip. The pain usually extends to the outside of the thigh area. In the early stages, the pain is usually described as sharp and intense. Later, the pain may become more of an ache and spread across a larger area of the hip. Typically, the pain is worse at night, when lying on the affected hip, and when getting up from a chair after being seated for a while. It also may get worse with prolonged walking, stair climbing, or squatting.
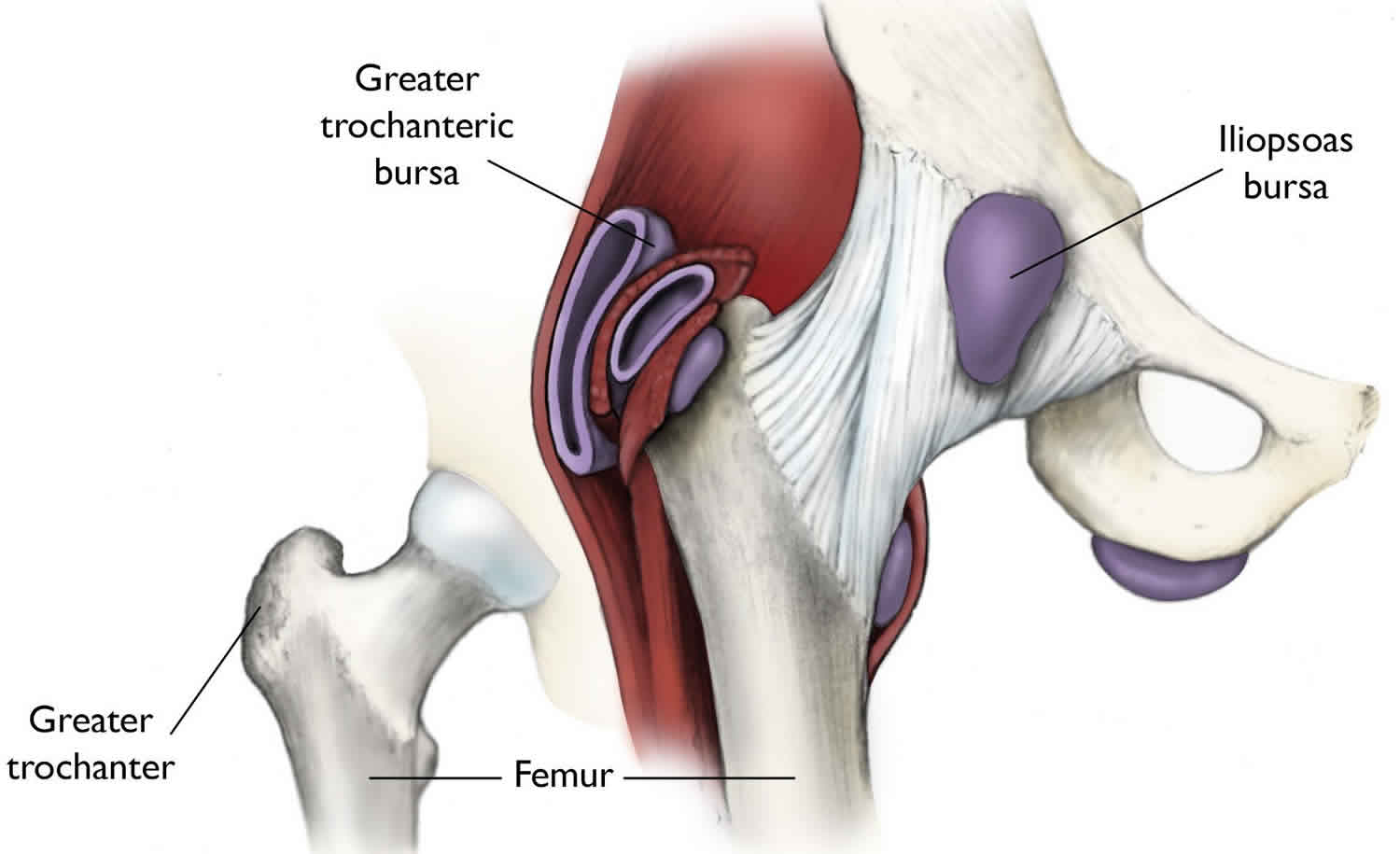
Another bursa — the iliopsoas bursa — is located on the inside (groin side) of the hip (see Figure 2). When this bursa becomes inflamed, the condition is also sometimes referred to as hip bursitis, but the pain is located in the groin area. This condition is not as common as trochanteric bursitis, but is treated in a similar manner.
Figure 2. Greater trochanteric pain syndrome (hip bursitis most often involves the bursa that covers the greater trochanter of the femur, although the iliopsoas bursa can also become inflamed)
Greater trochanteric pain syndrome causes
Greater trochanteric pain syndrome can be caused by:
- Overuse or stress on the hip from exercising or standing for long periods
- Hip injury, such as from a fall
- Being overweight
- Having one leg that is longer than the other
- Bone spurs on the hip
- Arthritis of the hip, knee, or foot
- Painful problems of the foot, such as a bunion, callas, plantar fasciitis, or Achilles tendon pain
- Spine problems, including scoliosis and arthritis of the spine
- Muscle imbalance that puts more stress around the hip muscles
- Tear in a buttocks muscle
- Infection (rare)
Greater trochanteric pain syndrome is more common in older adults. Being out of shape or overweight may put you at greater risk for hip bursitis. Women are more affected than men.
Risk factors for greater trochanteric pain syndrome
Greater trochanteric pain syndrome or hip bursitis can affect anyone, but is more common in women and middle-aged or elderly people. It is less common in younger people and in men.
The following risk factors have been associated with the development of hip bursitis.
- Repetitive stress (overuse) injury. This can occur when running, stair climbing, bicycling, or standing for long periods of time.
- Hip injury. An injury to the point of your hip can occur when you fall onto your hip, bump your hip, or lie on one side of your body for an extended period of time.
- Spine disease. This includes scoliosis, arthritis of the lumbar (lower) spine, and other spine problems.
- Leg-length inequality. When one leg is significantly shorter than the other, it affects the way you walk, and can lead to irritation of a hip bursa.
- Rheumatoid arthritis. This makes the bursa more likely to become inflamed.
- Previous surgery. Surgery around the hip or prosthetic implants in the hip can irritate the bursa and cause bursitis.
- Bone spurs or calcium deposits. These can develop within the tendons that attach muscles to the trochanter. They can irritate the bursa and cause inflammation.
Greater trochanteric pain syndrome prevention
Although hip bursitis cannot always be prevented, there are things you can do to prevent the inflammation from getting worse.
To help prevent hip pain:
- Always warm up and stretch before exercising and cool down afterward. Stretch your quadriceps and hamstrings.
- Avoid repetitive activities that put stress on the hips.
- Don’t increase the distance, intensity, and amount of time you exercise all at the same time.
- Avoid running straight down hills. Walk down instead.
- Swim instead of running or cycling.
- Run on a smooth, soft surface, such as a track. Avoid running on cement.
- If you have flat feet, try special shoe inserts and arch supports (orthotics).
- Make sure your running shoes fit well and have good cushioning.
- Lose weight if you need to.
- Get a properly fitting shoe insert for leg-length differences.
- Maintain strength and flexibility of the hip muscles.
Greater trochanteric pain syndrome symptoms
Common symptoms include:
- Pain at the side of the hip, which may also be felt on the outside of the thigh
- Pain that is sharp or intense at first, but may become more of an ache
- Difficulty walking
- Joint stiffness
- Swelling and warmth of the hip joint
- Catching and clicking sensation
You may notice the pain more when:
- Getting out of a chair or bed
- Sitting for a long time
- Walking up stairs
- Sleeping or lying on the affected side
Greater trochanteric pain syndrome diagnosis
To diagnose hip bursitis or greater trochanteric pain syndrome, the doctor will perform a comprehensive physical examination, looking for tenderness in the area of the point of the hip. He or she may also perform additional tests to rule out other possible injuries or conditions. These tests can include imaging studies, such as x-rays, bone scanning, and magnetic resonance imaging (MRI).
Your health care provider will do a physical exam and ask about your symptoms. Your doctor may do the following during the exam:
- Ask you to point to the location of the pain
- Feel and press on your hip area
- Move your hip and leg as you lie on the exam table
- Ask you to stand, walk, sit down and stand up
- Measure the length of each leg
To rule out other conditions that could be causing your symptoms, you may have tests such as:
- X-rays
- Ultrasound
- MRI
Greater trochanteric pain syndrome treatment
Nonsurgical treatment
Many cases of greater trochanteric pain syndrome go away with rest and self-care. The initial treatment for hip bursitis does not involve surgery. Your doctor may recommend that you try the following:
- Use an ice pack 3 to 4 times a day for the first 2 or 3 days.
- Take pain relievers such as nonsteroidal anti-inflammatory drugs (NSAIDs), ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), piroxicam, celecoxib, and others, may relieve pain, reduce swelling and control inflammation. Use NSAIDs cautiously and for limited periods. Talk with your doctor about the NSAIDs you use. NSAIDs may have adverse side effects if you have certain medical conditions or take certain medications.
- Activity modification. Avoid the activities that worsen symptoms.
- When sleeping, do not lie on the side that has bursitis.
- Avoid standing for long periods of time.
- When standing, stand on a soft, cushioned surface. Put an equal amount of weight on each leg.
- Placing a pillow between your knees when lying on your side can help decrease your pain.
- Wear comfortable, well-cushioned shoes with a low heel.
- Lose weight if you are overweight.
- Strengthen your core muscles.
- Assistive devices. Use of a walking cane or crutches for a week or more when needed.
- Physical therapy. Your doctor may prescribe exercises to increase hip strength and flexibility. You may do these exercises on your own, or a physical therapist may teach you how to stretch your hip muscles and use other treatments such as rolling therapy (massage), ice, heat, or ultrasound.
As the pain goes away, your doctor may suggest exercises to build strength and prevent muscle atrophy. You may need physical therapy if you have trouble moving the joint.
Other treatments include:
- Removing fluid from the bursa
- Steroid injection into the bursa. Injection of a corticosteroid along with a local anesthetic may also be helpful in relieving symptoms of hip bursitis. This is a simple and effective treatment that can be done in the doctor’s office. It involves a single injection into the bursa. The injection may provide temporary (months) or permanent relief. If pain and inflammation return, another injection or two, given a few months apart, may be needed. It is important to limit the number of injections, as prolonged corticosteroid injections may damage the surrounding tissues.
Call your doctor if symptoms come back or do not improve after 2 weeks of treatment.
Get medical help right away if you have any of the following:
- Your hip pain is caused by a serious fall or other injury
- Your leg is deformed, badly bruised, or bleeding
- You are unable to move your hip or bear any weight on your leg
Surgical treatment
Surgery is rarely needed for hip bursitis. If the bursa remains inflamed and painful after all nonsurgical treatments have been tried, your doctor may recommend surgical removal of the bursa. Removal of the bursa does not hurt the hip, and the hip can function normally without it.
A newer technique that is gaining popularity is arthroscopic removal of the bursa. In this technique, the bursa is removed through a small (1/4-inch) incision over the hip. A small camera, or arthroscope, is placed in a second incision so the doctor can guide miniature surgical instruments and cut out the bursa. This surgery is less invasive, and recovery is quicker and less painful.
Both types of surgeries are done on an outpatient (same-day) basis, so an overnight stay in the hospital is not usually necessary. Early research shows arthroscopic removal of the bursa to be quite effective, but this is still being studied.
Rehabilitation
Following surgery, a short rehabilitation period can be expected. Most patients find that using a cane or crutches for a couple of days is helpful. It is reasonable to be up and walking around the evening after surgery. The soreness from surgery usually goes away after a few days.
Snapping hip
Snapping hip can occur in different areas of the hip where tendons and muscles slide over knobs in the hip bones. The most common site of snapping hip is at the outer side where the iliotibial band passes over the portion of the thighbone known as the greater trochanter.
When the hip is straight, the iliotibial band is behind the trochanter. When the hip bends, the band moves over the trochanter so that it is in front of it. The iliotibial band is always tight, like a stretched rubber band. Because the trochanter juts out slightly, the movement of the band across it creates the snap you hear.
Eventually, snapping hip may lead to hip bursitis. Bursitis is thickening and inflammation of the bursa, a fluid-filled sac that allows the muscle to move smoothly over bone.
Another tendon that could cause a snapping hip runs from the front of the thigh up to the pelvis (rectus femoris tendon). Snapping of the rectus femoris tendon is felt in the front of the hip. As you bend the hip, the tendon shifts across the head of the thighbone, and when you straighten the hip, the tendon moves back to the side of the thighbone. This back-and-forth motion across the head of the thighbone causes the snapping.
In addition to the rectus femoris tendon at the front of the hip, the iliopsoas tendon can catch on bony prominences at the front of the pelvis bone.
Snapping in the back of the hip can involve the hamstring tendon. This tendon attaches to the sitting bone, called the ischial tuberosity. When it moves across the ischial tuberosity, the tendon may catch, causing a snapping sensation in the buttock region.
The labrum that lines the socket of the hip can tear and cause a snapping sensation. Damaged cartilage can loosen and float in the joint causing the hip to catch or “lock up.” This type of snapping hip usually causes pain and may be disabling.
Snapping hip causes
Snapping hip is most often the result of tightness in the muscles and tendons surrounding the hip. People who are involved in sports and activities that require repeated bending at the hip are more likely to experience snapping hip. Dancers are especially vulnerable.
Young athletes are also more likely to have snapping hip. This is because tightness in the muscle structures of the hip is common during adolescent growth spurts.
Snapping hip diagnosis
Your doctor will first determine the exact cause of the snapping by discussing you medical history and symptoms, and conducting a physical examination. He or she may ask you where it hurts, what kinds of activities bring on the snapping, whether you can demonstrate the snapping, or whether you have experienced any injury to the hip area.
You may also be asked to stand and move your hip in various directions to reproduce the snapping. Your doctor may even be able to feel the tendon moving as you bend or extend your hip.
Imaging Tests
X-rays create clear pictures of dense structures, like bone. Although x-rays of people with snapping hip do not typically show anything abnormal, your doctor may order x-rays along with other tests to rule out any problems with the bones or joint.
Snapping hip treatment
Initial treatment typically involves a period of rest and modification of activities. Depending upon the cause of your snapping hip, your doctor may also recommend other conservative treatment options.
Home remedies
Most people do not see a doctor for snapping hip unless they experience some pain. If the snapping hip bothers you — but not to the point of seeing a doctor — try the following conservative home treatment options:
- Reduce your activity levels and apply ice to the affected area.
- Use nonsteroidal anti-inflammatory drugs (NSAIDs), such as aspirin or ibuprofen, to reduce discomfort.
- Modify your sport or exercise activities to avoid repetitive movement of the hip. For example, reduce time spent on a bicycle, and swim using your arms only.
If you are still experiencing discomfort after trying these conservative methods, consult your doctor for professional treatment.
Physical therapy
Your doctor may prescribe exercises to stretch and strengthen the musculature surrounding the hip. Guidance from a physical therapist may also be recommended.
Iliotibial band stretch:
- Stand next to a wall for support
- Cross the leg that is closest to the wall behind your other leg.
- Lean your hip toward the wall until you feel a stretch at the outside of your hip. Hold the stretch for 30 seconds.
- Repeat on the opposite side.
- Perform 2 to 3 sets of 4 repetitions each side.
Piriformis stretch:
- Lie on your back with bent knees and feet flat on the floor.
- Cross the foot of the affected hip over the opposite knee and clasp your hands behind your thigh.
- Pull your thigh toward you until you feel the stretch in your hip and buttocks. Hold the stretch for 30 seconds.
- Repeat on the opposite side.
- Perform 2 to 3 sets of 4 repetitions each side.
Corticosteroid injection
If you have hip bursitis, your doctor may recommend an injection of a corticosteroid into the bursa to reduce painful inflammation.
Surgical treatment
In the rare instances that snapping hip does not respond to conservative treatment, your doctor may recommend surgery. The type of surgery will depend on the cause of the snapping hip.
- Hip arthroscopy. During hip arthroscopy, your surgeon inserts a small camera, called an arthroscope, into your hip joint. The camera displays pictures on a television screen, and your surgeon uses these images to guide miniature surgical instruments. Because the arthroscope and surgical instruments are thin, the surgeon can use very small incisions (cuts), rather than the larger incision needed for standard, open surgery. Hip arthroscopy is most often used to remove or repair fragments of a torn labrum.
- Open procedure. A traditional open surgical incision (several centimeters long) may be required to address the cause of the snapping hip. An open incision can help your surgeon to better see and gain access to the problem in the hip.
Your orthopaedic surgeon will discuss with you the best procedure to meet your individual health needs.
Trochanter fracture
Intertrochanteric fracture
This fracture occurs between the neck of the femur and a lower bony prominence called the lesser trochanter. This occurs further down the bone and tends to have better blood supply to the fracture pieces. The lesser trochanter is an attachment point for one of the major muscles of the hip. Intertrochanteric fractures generally cross in the area between the lesser trochanter and the greater trochanter. The greater trochanter is the bump you can feel under the skin on the outside of the hip. It acts as another muscle attachment point.
Subtrochanteric fracture
Subtrochanteric fracture occurs below the lesser trochanter, in a region that is between the lesser trochanter and an area approximately 2 1/2 inches below. Subtrochanteric femur fractures are difficult to treat due to strong deforming forces at the fracture site, tenuous blood supply, and the immense load-bearing forces exerted through the peri-trochanteric region 1. Adequate reduction and stable fixation are paramount when treating these fractures to optimize patient outcomes 2.
Trochanter fracture treatment
Once the diagnosis of the hip fracture has been made, the patient’s overall health and medical condition will be evaluated. In very rare cases, the patient may be so ill that surgery would not be recommended. In these cases, the patient’s overall comfort and level of pain must be weighed against the risks of anesthesia and surgery.
Most surgeons agree that patients do better if they are operated on fairly quickly. It is, however, important to insure patients’ safety and maximize their overall medical health before surgery. This may mean taking time to do cardiac and other diagnostic studies.
Nonsurgical treatment
Patients who might be considered for nonsurgical treatment include those who are too ill to undergo any form of anesthesia and people who were unable to walk before their injury and may have been confined to a bed or a wheelchair.
Certain types of fractures may be considered stable enough to be managed with nonsurgical treatment. Because there is some risk that these “stable” fractures may instead prove unstable and displace (change position), the doctor will need to follow with periodic X-rays of the area. If patients are confined to bed rest as part of the management for these fractures, they will need to be closely monitored for complications that can occur from prolonged immobilization. These include infections, bed sores, pneumonia, the formation of blood clots, and nutritional wasting.
Surgical treatment
Before surgery
Anesthesia for surgery could be either general anesthesia with a breathing tube or spinal anesthesia. In very rare circumstances, where only a few screws are planned for fixation, local anesthesia with heavy sedation can be considered. All patients will receive antibiotics during surgery and for the 24-hours afterward.
Appropriate blood tests, chest X-rays, electrocardiograms, and urine samples will be obtained before surgery. Many elderly patients may have undiagnosed urinary tract infections that could lead to an infection of the hip after surgery.
The surgeon’s decision as to how to best fix a fracture will be based on the area of the hip that is broken and the surgeon’s familiarity with the different systems that are available to manage these injuries.
Intracapsular fracture
If the head of the femur (“ball”) alone is broken, management will be aimed at fixing the cartilage on the ball that has been injured or displaced. Frequently with these injuries, the socket, or acetabulum, may also be broken. The surgeon will need to take this into consideration as well.
These injuries may be approached either from either the front or back of the hip. In some cases, both approaches are required in order to clearly see and fix the injured bone.
For true intracapsular hip fractures, the surgeon may decide either to fix the fracture with individual screws (percutaneous pinning) or a single larger screw that slides within the barrel of a plate. This compression hip screw will allow the fracture to become more stable by having the broken area impact on itself. Occasionally, a secondary screw may be added for stability.
If the intracapsular hip fracture is displaced in a younger patient, a surgical attempt will be made to reduce, or realign, the fracture through a larger incision. The fracture will be held together with either individual screws or with the larger compression hip screw.
In these cases, the blood supply to the ball, or head of the femur, may have been damaged at the time of injury (avascular necrosis). Even though the fracture is realigned and fixed into place, the cartilage and underlying supporting bone may not receive adequate blood. Over a period of time, this may cause the femoral head to flatten out. When this occurs, the joint surface becomes irregular. Ultimately, the hip joint may develop a painful arthritis, despite the surgical repair.
In the older patient, the chance that the head of the femur is damaged in this way is higher. It is generally felt that for these displaced fractures, patients will do better if some of the components of the hip are replaced. In some cases, this can mean a replacement of the ball, or head of the femur (hemiarthroplasty). In other cases, this can mean the replacement of both the ball and socket, or head of the femur and acetabulum (total hip replacement).
Intertrochanteric fracture
Most intertrochanteric fractures are managed with either a compression hip screw or an intramedullary nail, which also allows for impaction at the fracture site.
The compression hip screw is fixed to the outer side of the bone with bone screws and has a large secondary screw (lag screw) that is placed through the plate into the neck and head of the hip (see compression hip screw figure above). The design of the device allows for impaction and compression at the fracture site. This may increase the stability of the area and promote healing.
The intramedullary nail is placed directly into the marrow canal of the bone through an opening made at the top of the greater trochanter. A lag screw is then placed through the nail and up into the neck and head of the hip. As with the compression hip screw, sliding of the lag screw and impaction of the fracture take place.
There are no definitive studies to show that one device is superior to another. The decision as to which to use is based on the surgeon’s preference and experience.
Subtrochanteric fracture
At the subtrochanteric level, most fractures are managed with a long intramedullary nail together with a large lag screw or they are managed with screws that capture the neck and head of the femur or the area immediately underneath it, if it has remained intact.
In order to keep the bones from rotating around the nail or from shortening (“telescoping”) on the nail, additional screws may be placed at the lower end of the nail in the area of the knee. These are called interlocking screws.
In certain cases, the surgeon may choose to use a plate rather than a nail. The plate will have screws that go into the bone from the lateral, or outer, side of the femur. A single large screw goes into the neck and the head of the femur and appears similar to the compression hip screw, but at a different angle. Secondary screws are then placed through the plate into the bone to hold the fracture in place.
Trochanter fracture recovery
Patients may be discharged from the hospital to their home or find that a stay in a rehabilitation facility is necessary to assist them in regaining their ability to walk.
Pain management
Pain after an injury or surgery is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover faster.
Medications are often prescribed for short-term pain relief after surgery or an injury. Many types of medicines are available to help manage pain, including opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery or an injury, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your treatment.
Rehabilitation
Patients may be encouraged to get out of bed on the day following surgery with the assistance of a physical therapist. The amount of weight that is allowed to be placed on the injured leg will be determined by the surgeon and is generally a function of the type of fracture and repair (fixation).
The physical therapist will work with the patient to help regain strength and the ability to walk. This process may take up to three months.
Medical care
Occasionally, a blood transfusion may be required after surgery, but longer term antibiotics are generally not necessary.
Most patients will be placed on medicine to thin their blood to reduce the chances of developing blood clots for up to 6 weeks. These medicines may be in the form of pills or injections. Elastic compression stockings or inflatable compression boots may also be used.
Follow-Up care
During the appointments that take place after surgery, the surgeon will want to check the wound, remove sutures, follow the healing process using X-rays, and prescribe additional physical therapy, if necessary.
Following hip fracture surgery, most patients will regain much, if not all, of the mobility and independence they had before the injury.
- Medda S, Pilson H. Subtrochanteric Femur Fractures. [Updated 2019 May 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507803[↩]
- Lo YC, Su YP, Hsieh CP, Huang CH. Augmentation Plate Fixation for Treating Subtrochanteric Fracture Nonunion. Indian J Orthop. 2019 Mar-Apr;53(2):246-250.[↩]

{kind=link}