
Contents
- What is a verruca
- What is the human papillomavirus?
- Which types of HPV are most likely to cause disease?
- How common is human papillomavirus (HPV) infection?
- How serious is disease caused by HPV?
- How is human papillomavirus transmitted?
- Can HPV be transmitted by non-sexual transmission routes, such as clothing, undergarments, sex toys, or surfaces?
- If a person has been infected with a wild-type strain of HPV can they be reinfected with the same strain?
- Who gets verruca?
- Are verrucas contagious?
- What causes verruca?
- How can verruca be prevented?
- HPV vaccination
- Who should NOT get HPV vaccine?
- If I have been sexually active for a number of years, is it still recommended that I get HPV vaccine or to complete the HPV vaccine series?
- Are catch-up recommendations for the use of HPV vaccine different for males and females?
- Should transgender persons receive HPV vaccine?
- What are the recommendations for use of HPV vaccine in people age 27 through 45 years?
- Why is HPV vaccination not routinely recommended for all adults age 27 through 45 years?
- Do I need revaccination with 9-valent HPV vaccine if I previously received a 3-dose series of 2-valent HPV vaccine or 4-valent HPV vaccine?
- Are additional 9-valent HPV vaccine doses recommended for a person who started a 3-dose series with 2-valent HPV vaccine or 4-valent HPV vaccine and completed the series with one or two doses of 9-valent HPV vaccine?
- We have several males in our health clinics whose records indicate that they received doses of Cervarix. Can we count these doses as valid?
- Preventing verruca warts from spreading
- HPV vaccination
- Verruca signs and symptoms
- Complications of verruca
- Verruca diagnosis
- Verruca treatment
- Living with warts
- What is the human papillomavirus?
What is a verruca
Verruca is commonly called a wart, viral wart or papilloma and warty lesions may be described as verrucous. Verruca is a very common growth on the skin and mucous membranes (the mouth or genitals) that are caused by infection with human papillomavirus (HPV). There are over 200 types of the human papillomavirus (HPV). Verruca (warts) appear as circular raised flesh-colored growths that have a roughened, irregular surface. Common warts (verruca vulgaris) occur most frequently on areas of the body prone to trauma, such as on the fingers, backs of the hands, face, knees, and elbows. They are usually not painful and are harmless. The human papillomavirus (HPV) causes thickening of the top skin layer.
Verrucas (warts) are usually acquired from person-to-person contact. The human papillomavirus (HPV) is not highly contagious but can cause an infection by entering through a small break in the skin. In the same way, warts can be spread to other places on your own body. The human papillomavirus (HPV) is rarely transferred by touching an object used by an infected person.
Verrucas (warts) can affect people of any age, but they are most common between the ages 12–16. It is estimated that 20% of school children and about 10% of the general population have verruca (warts). Those with HIV, organ transplants, or on chemotherapy have a higher incidence of verruca (warts) due to their weakened immune system.
Verruca infection can be described as:
- Mild – just one or a few painless lesions
- Moderate – 10–20 lesions that are painless
- Severe – pain that limits normal life activities, bleeding, or over 20 lesions, except for flat warts, which can be numerous, yet not bothersome
Verruca are usually painless and go away on their own, sometimes taking a few months to resolve, but can take up to two years. No treatment is universally effective at eradicating viral warts. In children, even without treatment, 50% of verrucas disappear within six months, and 90% are gone in 2 years. They are more persistent in adults, but they clear up eventually. Verrucas are likely to recur in patients that are immune suppressed, for example, organ transplant recipients. Recurrence is more frequent in tobacco smokers.
See a doctor if:
- you’re worried about a growth on your skin
- you aren’t sure whether the growths are warts
- the growths are bothersome and interfere with activities
- you also have a weakened immune system because of immune-suppressing drugs, HIV/AIDS or other immune system disorders
- you have a wart or verruca that keeps coming back
- you have a very large or painful wart or verruca
- a wart bleeds or changes in how it looks
- you have a wart on your face or genitals
- the growths are painful or change in appearance or color
- you’ve tried treating the warts, but they persist, spread or recur
Figure 1. Warts on hands

Figure 2. Wart on finger


Figure 3. Warts on face


Figure 4. Filiform warts


Figure 5. Flat warts

Figure 6. Periungual warts are warts about the nails. They are particularly common in children who bite their nails or pick at their cuticles.

What is the human papillomavirus?
Human papillomaviruses (HPV) are a large family of species-specific related double-stranded DNA viruses. There are more than 200 different HPV types; at least 40 can infect the anogenital area. Other types cause warts on other areas of skin. HPV types are often referred to as “non-oncogenic” (wart-causing) or “oncogenic” (cancer-causing), based on whether they put a person at risk for cancer. The International Agency for Research on Cancer found that 13 HPV types can cause cervical cancer, and at least one of these types can cause cancers of the vulva, vagina, penis, anus, and certain head and neck cancers (specifically, the oropharynx, which includes the back of the throat, base of the tongue and tonsils) 1. The types of HPV that can cause genital warts are not the same as the types that can cause cancer.
Human papillomavirus (HPV) transmission is from direct skin-to-skin contact with apparent or subclinical lesions and contact with genital secretions. Micro-abrasions in the recipient’s skin allow viral access to the basal cells of the epithelium. HPV infects keratinocytes in the skin and epithelial cells in mucosa and stimulates them to proliferate, causing a visible lesion. Most HPV infections are asymptomatic and latent, not developing into visible warts. Subclinical infection may show up on a cervical smear. However some HPV types cause anogenital cancer. These types are also contagious.
Most people who become infected with HPV do not know they have it. Usually, the body’s immune system gets rid of the HPV infection naturally within two years. This is true of both oncogenic (cancer-causing) and non-oncogenic (wart-causing) HPV types. By age 50, at least 4 out of every 5 women will have been infected with HPV at one point in their lives. HPV is also very common in men, and often has no symptoms.
At least 75% of sexually active adults have been infected with at least one type of anogenital HPV at some time in their life.
Every year in the United States, 36,500 people (including women and men) are estimated to be diagnosed with a cancer caused by HPV infection (see Table 1 below). Although cervical cancer is the most well-known of the cancers caused by HPV, there are other types of cancer caused by HPV. HPV vaccination could prevent more than 90% of cancers caused by HPV from ever developing. This is an estimated 33,700 cases in the United States every year 2.
Cervical cancer is the only type of cancer caused by HPV with a recommended screening test for detection at an early stage. The other cancers may not be detected until they cause health problems.
Even with screening, HPV causes 11,000 cases of cervical cancer each year in the United States. Every year, 4,000 women die of cervical cancer.
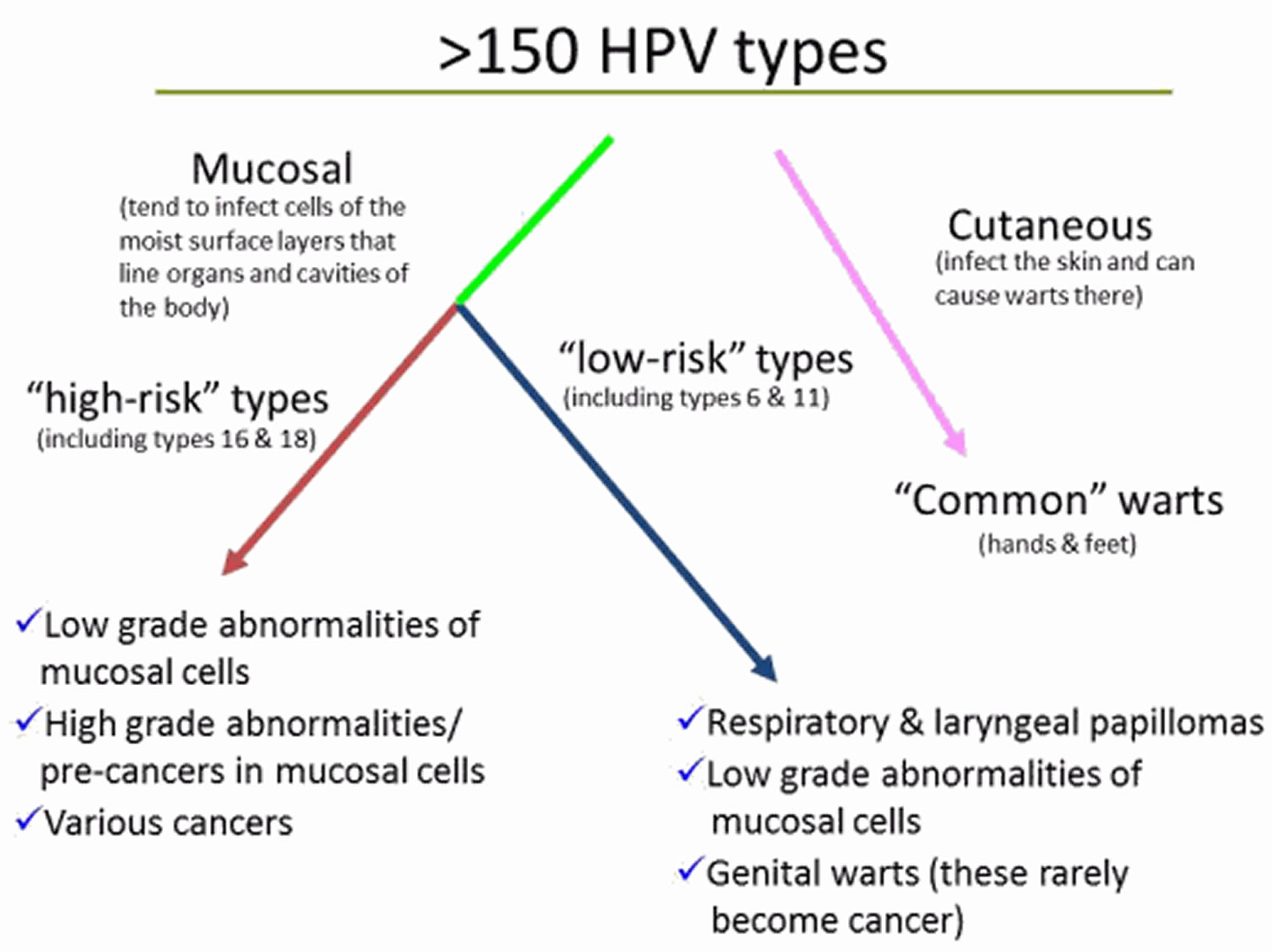
Figure 7. Human papillomavirus (HPV) types and the problems each group can cause (this diagram shows the different groups of human papillomavirus (HPV) types and the problems each group can cause)
Which types of HPV are most likely to cause disease?
In the United States, approximately 80% of HPV-related cancers are attributable to HPV 16 or 18 which are included in all three HPV vaccines that have been available in the U.S. Approximately 12% are attributable to HPV types 31, 33, 45, 52, and 58 (16% of all HPV-attributable cancers for females; 6% for males; approximately 3,800 cases annually), which are included in the 9-valent HPV vaccine. HPV types 16, 18, 31, 33, 45, 52, or 58 account for about 81% of cervical cancers in the United States. HPV types 6 or 11 cause 90% of anogenital warts (condylomata) and most cases of recurrent respiratory papillomatosis.
How common is human papillomavirus (HPV) infection?
HPV is the most common sexually transmitted infection in the United States. In the United States, an estimated 79 million persons are infected, and an estimated 14 million new HPV infections occur every year among persons age 15 through 59 years. Approximately half of new infections occur among persons age 15 through 24 years. First HPV infection occurs within a few months to years of becoming sexually active.
How serious is disease caused by HPV?
Most HPV infections are asymptomatic and go away completely on their own within 2 years after infection without causing clinical disease. Some infections are persistent and can lead to precancerous lesions or cancer. HPV infection caused by certain HPV types cause almost all cases of anogenital warts in women and men and recurrent respiratory papillomatosis.
From 2014 through 2018, approximately 46,143 new cases of HPV-associated cancers occurred each year in the United States (25,719 among women and 20,424 among men). Cervical cancer, the most widely known HPV-associated cancer, caused an average of 12,200 cases in the U.S. each year during that time. HPV is also associated with vulvar, and vaginal cancer in females, penile cancer in males, and anal and oropharyngeal cancer in both females and males. Between 2014 and 2018, oropharyngeal cancers were the most commonly occurring HPV-associated cancers, with an average of 20,236 reported cases each year (16,680 among men and 3,556 among women).
Table 1. Number of HPV-attributable cancer cases per year in United States
| Cancer site | Average number of cancers per year in sites where HPV is often found (HPV-associated cancers) | Percentage probably caused by any HPV type a | Estimated number probably caused by any HPV type a |
|---|---|---|---|
| Cervix | 12293 | 91% | 11100 |
| Vagina | 879 | 75% | 700 |
| Vulva | 4282 | 69% | 2900 |
| Penis | 1375 | 63% | 900 |
| Anus b | 7531 | 91% | 6900 |
| Female | 5106 | 93% | 4700 |
| Male | 2425 | 89% | 2200 |
| Oropharynx | 20839 | 70% | 14800 |
| Female | 3617 | 63% | 2300 |
| Male | 17222 | 72% | 12500 |
| TOTAL | 47199 | 79% | 37300 |
| Female | 26177 | 83% | 21700 |
| Male | 21022 | 74% | 15600 |
Footnotes: Data are from population-based cancer registries participating in the Centers for Disease Control and Prevention (CDC) National Program of Cancer Registries (NPCR) and/or the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program for 2015 to 2019, covering 99% of the U.S. population.
a HPV types detected in genotyping study; most were high-risk HPV types known to cause cancer 3. Estimates were rounded to the nearest 100. Estimated counts might not sum to total because of rounding.
b Includes anal and rectal squamous cell carcinomas.
[Source 4 ]How is human papillomavirus transmitted?
Visible anogenital warts and subclinical HPV infection nearly always arise from direct skin to skin contact. Transmission is more likely from visible warts than from subclinical or latent HPV infection. Most new HPV infections occur in adolescents and young adults after their first sexual activity 5. Although most sexually active adults have been exposed to HPV 6, new infections can occur with a new sex partner 7.
- Sexual contact. This is the most common way amongst adults 5.
- Oral sex. HPV appears to prefer the genital area to the mouth.
- Vertical (mother to baby) transmission through the birth canal.
- Auto (self) inoculation from one site to another.
- Fomites (ie from objects like bath towels). It remains very controversial whether warts can spread this way.
Visible genital warts and subclinical human papillomavirus (HPV) infection nearly always arise from direct skin to skin contact.
Often, warts will appear three to six months after infection but they may appear months or even years later.
Can HPV be transmitted by non-sexual transmission routes, such as clothing, undergarments, sex toys, or surfaces?
Nonsexual HPV transmission is theoretically possible but has not been definitely demonstrated. This is mainly because HPV can’t be cultured and DNA detection from the environment is difficult and likely prone to false negative results.
If a person has been infected with a wild-type strain of HPV can they be reinfected with the same strain?
- If a person is infected with an HPV strain that does not clear (that is, the person becomes persistently infected) the person cannot be reinfected because they are continuously infected.
- If a person is infected with an HPV strain that clears, some but not all persons will have a lower chance of reinfection with the same strain. Data suggest that females are more likely than males to develop immunity after clearance of natural infection.
- Prior infection with an HPV strain does not lessen the chance of infection with a different HPV strain.
Who gets verruca?
Verruca (warts) are particularly common in:
- School-aged children, but they may arise at any age
- Eczema, due to a defective skin barrier
- People who are immune suppressed with medications such as azathioprine or ciclosporin, or with human immunodeficiency virus (HIV) infection. In these patients, verruca may never disappear — despite treatment.
Are verrucas contagious?
Yes. Warts are caused by a virus known as the human papilloma virus (HPV) and warts can be spread to other people from contaminated surfaces or through close skin contact. You’re more likely to spread a wart or verruca if your skin is wet or damaged.
It can take months for a wart or verruca to appear after contact with the virus.
Mucosal HPV is spread mainly by direct skin-to-skin contact during vaginal, oral, or anal sexual activity. It’s not spread through blood or body fluids. It can be spread even when an infected person has no visible signs or symptoms.
Anyone who has had sexual contact can get HPV, even if it was only with only one person, but infections are more likely in people who have had many sex partners.
The virus can also be spread by genital contact without sex, but this is not common. Oral-genital and hand-genital spread of some genital HPV types have been reported. And there may be other ways to become infected with HPV that aren’t yet clear.
You DO NOT get HPV from:
- Toilet seats
- Hugging or holding hands
- Swimming in pools or hot tubs
- Sharing food or utensils
- Being unclean
Transmission from mother to newborn during birth is rare, but it can happen, too. When it does, it can cause warts (papillomas) in the infant’s breathing tubes (trachea and bronchi) and lungs, which is called respiratory papillomatosis. These papillomas can also grow in the voice box, which is called laryngeal papillomatosis. Both of these infections can cause life-long problems.
DO
- wash your hands after touching a wart or verruca
- change your socks daily if you have a verruca
- cover warts and verrucas with a plaster when swimming
- take care not to cut a wart when shaving
DON’T
- share towels, flannels, socks or shoes if you have a wart or verruca
- bite your nails or suck fingers with warts on
- walk barefoot in public places if you have a verruca
- scratch or pick a wart
What causes verruca?
Verruca are due to infection by the human papillomavirus (HPV), a DNA virus. More than 100 HPV subtypes are known, giving rise to a variety of presentations. Infection occurs in the superficial layers of the epidermis, causing proliferation of the keratinocytes (skin cells) and hyperkeratosis — the wart. The most common subtypes of HPV are types 2, 3, 4, 27, 29, and 57.
HPV is spread by direct skin-to-skin contact or autoinoculation. This means if a verruca is scratched or picked, the viral particles may be spread to another area of skin. The incubation period can be as long as twelve months.
How can verruca be prevented?
HPV vaccines are available to prevent anogenital warts. HPV vaccination is recommended for preteen girls and boys at age 11 or 12 years. Anecdotally, these have been reported to result in the clearance of non-genital warts in some people without definite evidence that the vaccine is the cause of remission.
HPV vaccination
The Centers for Disease Control and Prevention (CDC) recommends routine HPV vaccination for girls and boys ages 11 and 12, although it can be given as early as age 9. It’s ideal for girls and boys to receive the HPV vaccine before they have sexual contact 8.
Side effects from the HPV vaccines are usually mild and include soreness at the injection site, headaches, a low-grade fever or flu-like symptoms.
The CDC now recommends that all 11- and 12-year-olds receive two doses of HPV vaccine at least six months apart, instead of the previously recommended three-dose schedule. Younger adolescents ages 9 and 10 and teens ages 13 and 14 also are able to receive vaccination on the updated two-dose schedule. Research has shown that the two-dose schedule is effective for children under 15.
Teens and young adults who begin the vaccine series later, at ages 15 through 26, should continue to receive three doses of the vaccine.
The CDC now recommends catch-up HPV vaccinations for all people through age 26 who aren’t adequately vaccinated.
The U.S. Food and Drug Administration (FDA) recently approved the use of Gardasil 9 for males and females ages 9 to 45. If you’re ages 27 to 45, discuss with your doctor whether he or she recommends that you get the HPV vaccine.
In the United States three HPV vaccines are licensed: Ceravrix, a 2-valent vaccine (2vHPV) that targets HPV types 16 and 18; Gardasil, a 4-valent vaccine (4vHPV) that targets HPV types 6, 11, 16, and 18; and Gardasil 9, a 9-valent vaccine (9vHPV) that targets HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58. Types 16 and 18 account for 65-70% of all cervical cancers, whereas the five additional types targeted by the 9-valent vaccine account for 10% 9. HPV types 6 and 11 cause >90% of genital warts. Since late 2016, only Gardasil 9 (9vHPV) vaccine is available in the United States 8.
- Gardasil, a 4-valent vaccine (4vHPV) that protects against the 4 strains of HPV (HPV types 6, 11, 16, and 18) that cause 70% of cervical cancers and 90% of genital warts. In the US, Gardasil is approved for girls/women and boys/men ages 9–26. In 2011, Health Canada approved the vaccine for women up to the age of 45.
- Gardasil 9, a 9-valent vaccine (9vHPV) that targets HPV types 6, 11, 16, 18, 31, 33, 45, 52, and 58, is highly effective in preventing urogenital cancers and anogenital warts.
HPV vaccine may be available at doctor offices, community health clinics, school-based health centers, and health departments.
Who should NOT get HPV vaccine?
Tell your doctor about any severe allergies. Some people should NOT get some HPV vaccines if:
- They have ever had a life-threatening allergic reaction to any ingredient of an HPV vaccine, or to a previous dose of HPV vaccine.
- They have an allergy to yeast (Gardasil and Gardasil 9).
- They are pregnant.
HPV vaccines are safe for children who are mildly ill, like those with a low-grade fever of less than 101 degrees, a cold, runny nose, or cough. People with a moderate or severe illness should wait until they are better.
If I have been sexually active for a number of years, is it still recommended that I get HPV vaccine or to complete the HPV vaccine series?
Yes. HPV vaccine should be administered to people who are already sexually active. Ideally, patients should be vaccinated before onset of sexual activity; however, people who have already been infected with one or more HPV types will still be protected from other HPV types in the vaccine that have not been acquired.
Are catch-up recommendations for the use of HPV vaccine different for males and females?
No. In June 2019, the Advisory Committee on Immunization Practices (ACIP) voted to recommend routine catch-up HPV vaccination of all previously unvaccinated or incompletely vaccinated males age 22 through 26, the same as the recommendation for females 10. HPV vaccination recommendations differ by age group. There is one recommendation for people 9 through 26 years of age and another recommendation for people 27 through 45 years of age.
Should transgender persons receive HPV vaccine?
Yes. The Advisory Committee on Immunization Practices (ACIP) recommends routine HPV vaccination for transgender persons as for all adolescents and young adults through age 26 years. Clinicians should discuss the risks of HPV disease and benefits of HPV vaccination with unvaccinated or incompletely vaccinated transgender persons age 27 through 45 years.
What are the recommendations for use of HPV vaccine in people age 27 through 45 years?
Catch-up HPV vaccination is not recommended for all adults older than 26 years of age 11. Instead, shared clinical decision-making (a discussion between the provider and the patient) regarding HPV vaccination is recommended for some adults aged 27 through 45 years who are not adequately vaccinated. Ideally, HPV vaccine should be administered before potential exposure to HPV through sexual contact.
Why is HPV vaccination not routinely recommended for all adults age 27 through 45 years?
Because HPV acquisition generally occurs soon after first sexual activity, HPV vaccine effectiveness will be lower in older age groups as the result of prior infections. In general, exposure to HPV also decreases among individuals in older age groups. Evidence suggests that although HPV vaccination is safe for adults 27 through 45 years, population benefit would be minimal; nevertheless, some adults who are unvaccinated or incompletely vaccinated might be at risk for new HPV infection and might benefit from vaccination in this age range.
Do I need revaccination with 9-valent HPV vaccine if I previously received a 3-dose series of 2-valent HPV vaccine or 4-valent HPV vaccine?
The Advisory Committee on Immunization Practices (ACIP) has not recommended routine revaccination with 9-valent HPV vaccine (Gardasil-9) for persons who have completed a 3-dose series of another HPV vaccine. There are data that indicate revaccination with 9-valent HPV vaccine (Gardasil) after a 3-dose series of 4-valent HPV vaccine (quadrivalent Gardasil) is safe. Clinicians should decide if the benefit of immunity against 5 additional oncogenic strains of HPV (which cause 12% of HPV-attributable cancers) is justified for their patients.
Are additional 9-valent HPV vaccine doses recommended for a person who started a 3-dose series with 2-valent HPV vaccine or 4-valent HPV vaccine and completed the series with one or two doses of 9-valent HPV vaccine?
There is no Advisory Committee on Immunization Practices (ACIP) recommendation for additional doses of 9-valent HPV vaccine (Gardasil 9) for persons who started the 3-dose series with 2-valent HPV vaccine (Cervarix) or 4-valent HPV vaccine (quadrivalent Gardasil) and completed the series with 9-valent HPV vaccine (Gardasil 9).
We have several males in our health clinics whose records indicate that they received doses of Cervarix. Can we count these doses as valid?
No. Cervarix (2-valent HPV vaccine) was not approved or recommended for use in males. Doses of Cervarix administered to males should not be counted and need to be repeated using 9-valent HPV vaccine (Gardasil-9).
Preventing verruca warts from spreading
There are steps you can take to prevent spreading warts and verrucas to others if you have them:
- if you have a plantar (on the bottom of the feet) wart, you need to change your socks daily
- don’t share towels with another person. If you have a plantar wart you should avoid sharing any footwear including socks
- if you have a plantar wart make sure you clean out the bottom of your shower or bath after use
- wash your hands if they come into direct contact with your wart, such as when you apply any treatments
- never pick, scratch or bite a wart
- don’t share any medicines or remedies used to treat your wart. This includes emery boards and pumice stones
- if you go swimming and you have a plantar wart you should cover it up and wear thongs in communal areas. Don’t go barefoot in public areas.
Verruca signs and symptoms
Cutaneous verruca (warts) have a hard, keratinous surface. Verruca (warts) may occur singly or in multiples and often have multiple small black “dots” at the surface from tiny blood vessels, due to an intracorneal hemorrhage.
Verruca vulgaris
Verruca vulgaris also called common warts are rough, thick, skin-colored, pink, or white bumps from 1 mm to over 10 mm in size. Verruca vulgaris (common warts) arise most often on the backs of fingers or toes, your hands, around the nails—where they can distort nail growth, face, elbows and on the knees. Sometimes verruca vulgaris resemble a cauliflower; these are known as butcher’s warts.
Verruca plantaris
Verruca plantaris also called plantar warts are thick, rough, callus-like, often tender areas of the soles of the feet, usually on the weight-bearing areas. Since verruca plantaris are painful, they are often thought to be corns. Verruca plantaris include tender inwardly growing and painful ‘myrmecia’ on the sole, and clusters of less painful mosaic warts. Plantar epidermoid cysts are associated with warts. Persistent plantar warts may rarely be complicated by the development of verrucous carcinoma.
Verruca plana
Verruca plana also called plane warts have a flat surface and are very slightly raised, smooth, 1–5 mm, skin-colored bumps that may appear in a line from self-inoculation from scratching or widely from shaving. Verruca plana are often seen on the face, hands and shins. Verruca plana are often numerous. They may be inoculated by shaving or scratching so that they appear in a linear distribution (pseudo-Koebner response). Verruca plana (plane warts) are mostly caused by HPV types 3 and 10.
Filiform wart
Filiform warts are finger like long and narrow, like tufts of thread, and usually small at the base (1–3 mm); they often affect the face, eyelids, nose area, armpits or neck. Filiform warts are also described as digitate warts (like a finger).
Mucosal wart
Oral warts can affect the lips and even inside the cheeks, where they may be called squamous cell papillomas. They are softer than cutaneous warts.
Genital warts
Genital warts are a sexually transmitted disease (STD) caused by the human papillomavirus (HPV). The warts usually appear as a small bump or group of bumps in the genital area. They are flesh-colored and can be flat or look bumpy like cauliflower. Some genital warts are so small you cannot see them. In women, the warts usually occur in or around the vagina, on the cervix, or around the anus. In men, genital warts are less common. They may have warts on the tip of the penis, around the anus, or on the scrotum, thigh, or groin.
You can get genital warts during oral, vaginal, or anal sex with an infected partner. Correct usage of latex condoms greatly reduces, but does not completely eliminate, the risk of catching or spreading HPV. The most reliable way to avoid infection is to not have anal, vaginal, or oral sex. HPV vaccines may help prevent some of the HPV infections that cause genital warts.
Mosaic warts
Mosaic warts these grow in clusters and are most common on your hands and feet.
Complications of verruca
Verrucas (viral warts) are very widespread in people with the rare inherited disorder epidermodysplasia verruciformis.
Malignant change is rare in verruca vulgaris (common warts) and causes verrucous carcinoma.
Oncogenic strains of HPV, the cause of some anogenital warts and warts arising in the oropharynx, are responsible for intraepithelial and invasive neoplastic lesions including cervical, anal, penile and vulval cancer.
Verruca diagnosis
Tests are rarely needed to diagnose a verruca, as they are so common and have a characteristic appearance.
- Pinpoint dots (clotted capillaries) are revealed when the top of the wart is removed.
- A dermatoscopic examination is sometimes helpful to distinguish viral warts from other verrucous lesions such as seborrhoeic keratosis and skin cancer.
- Sometimes, viral warts are diagnosed on skin biopsy. The histopathological features of verruca vulgaris differ from that of verruca plana.
Verruca treatment
Many people don’t bother to treat verruca because treatment can be more uncomfortable than verrucas —they are hardly ever a serious problem. Moreover, because verruca can resolve on their own, it is not necessary to treat all verrucas (warts). Warts that are very small and not troublesome can be left alone, and in some cases, they will regress on its own. Additionally, treating verruca may not always destroy them, nor will it necessarily keep other verruca (warts) from appearing. Treatments can be painful and cause scars and need to be repeated, so it should only be done in cases where the warts are highly bothersome or interfere with daily life.
To get rid of verrucas (warts), you have to stimulate your body’s immune system to attack the wart virus. Persistence with the treatment and patience is essential.
- Over-the-counter wart removers have a high percentage of salicylic acid and work by dissolving away the layer of skin infected with the virus. This treatment needs to be used daily and can sometimes be irritating if it touches unaffected skin around the wart. You can treat warts on places such as the hands, feet, or knees by putting salicylic acid (one brand name: Compound W) on the warts. After you take a bath or shower, pat your skin dry with a towel. Then apply the salicylic acid. The acid sinks in deeper and works better when it is applied to damp skin. Before you take a shower or a bath the next day, use an emery board or pumice stone to file away the dead surface of the warts. Apply the acid every day for many weeks as directed.
- Duct tape applied daily to the affected area seems to work for unknown reasons. The tape should be very sticky and kept on for a few days.
- Over-the-counter freezing medications are available but have not been found to be very effective.
- Coupled with the above therapies, the wart should be soaked in warm water, and any loose skin should be removed every few days with a mild abrasive, like a pumice stone.
- Family members should avoid sharing personal items such as towels.
Treatments your doctor may prescribe
- Destruction with freezing (cryosurgery); burning (electrocautery); laser; or cantharidin, podophyllin, tretinoin, or acid application
- Applying cantharidin. Your doctor may “paint” the chemical cantharidin on your warts. Most people don’t feel any pain when the chemical is applied. However, you may experience some pain and blistering of the wart about 3 to 8 hours later. Follow your doctor’s instructions for at-home care. When you return to your doctor for your follow-up visit, they will remove the dead skin of the wart. If the wart isn’t gone after one treatment, your doctor may suggest another treatment.
- Applying liquid nitrogen. Your doctor may use liquid nitrogen to freeze the wart. This treatment is called cryotherapy or cryosurgery. This is a two-step process that does not hurt the skin around the wart. Applying liquid nitrogen to the wart causes a little discomfort. To completely remove a wart, the treatments may be needed every 1 to 3 weeks for a total of 2 to 4 times. If no improvement is noted, your doctor may recommend another type of treatment.
- Injection of chemotherapy drugs e.g., Bleomycin injections
- Application of imiquimod, an immunotherapy agent, or other chemicals that induce an allergic reaction to destroy the wart. Imiquimod cream – is approved for treating anogenital warts but is usually ineffective for cutaneous warts.
- Pulsed dye laser destruction of feeding blood vessels
- Photodynamic therapy
- Laser vaporisation
- Diphencyprone, dinitrochlorobenzene, or squaric acid to cause localized allergic contact dermatitis over the wart.
Your doctor may choose to burn the wart, cut it out, or remove it with a laser. These treatments are effective, but they may leave a scar. They are normally reserved for warts that have not cleared up with other treatments.
Topical treatment
Topical treatment includes wart paints containing salicylic acid or similar compounds, which work by removing the dead surface skin cells.
The paint is applied once daily. Treatment with wart paint usually makes the wart smaller and less uncomfortable; 70% of warts resolve within twelve weeks of daily applications.
- Soften the wart by soaking in a bath or bowl of hot soapy water.
- Rub the wart surface with a piece of pumice stone or emery board.
- Apply wart paint or gel accurately, allowing it to dry.
- Cover with plaster or duct tape.
- If the wart paint makes the skin sore, stop treatment until the discomfort has settled, then recommence as above. Take care to keep the chemical off normal skin.
Verruca freeze
Cryotherapy is repeated at one to two–week intervals. It is uncomfortable and may result in blistering for several day or weeks. Success is in the order of 70% after 3–4 months of regular freezing.
A hard freeze using liquid nitrogen might cause a permanent white mark or scar. It can also cause temporary numbness.
An aerosol spray with a mixture of dimethyl ether and propane (DMEP) can be purchased over the counter to freeze common and plantar warts. Read and follow the instructions carefully.
Combining immunotherapy with cryotherapy reduces the number of cryotherapy sessions.
Electrosurgery
Electrosurgery (curettage and cautery) is used for large and resistant warts. Under local anaesthetic, the growth is pared away and the base burned. The wound heals in two weeks or longer; even then 20% of warts can be expected to recur within a few months. This treatment leaves a permanent scar.
Other treatments
Other experimental treatments for recurrent, resistant or extensive warts include:
- Topical retinoids, such as tretinoin cream or adapalene gel
- The immune modulator, imiquimod cream
- Fluorouracil cream
- Bleomycin injections
- Oral retinoids
- Pulsed dye laser destruction of feeding blood vessels
- Photodynamic therapy
- Laser vaporisation
- H2 receptor antagonists
- Oral zinc oxide and zinc sulfate
- Applications of raw garlic or tea tree oil
- Immune stimulation using diphencyprone, or squaric acid
- Immunotherapy with Candida albicans or tuberculin PPD
- Hypnosis
- Hyperthermia
- Occlusion with duct tape.
Living with warts
No treatment is universally effective at eradicating viral warts. However, most of the time, treatment of warts on the skin is successful and the warts are gone for good.
In children, even without treatment, 50% of warts disappear within six months, and 90% are gone in 2 years.
Viral warts are more persistent in adults, but they clear up eventually. Viral warts are likely to recur in patients that are immunosuppressed, for example, organ transplant recipients. Recurrence is more frequent in tobacco smokers.
Immunity to HPV is likely to be type-specific.
- Human Papillomaviruses. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Volume 90. https://publications.iarc.fr/108[↩]
- Cancers Caused by HPV Are Preventable. https://www.cdc.gov/hpv/hcp/protecting-patients.html[↩]
- Saraiya M, Unger ER, Thompson TD, Lynch CF, Hernandez BY, Lyu CW, Steinau M, Watson M, Wilkinson EJ, Hopenhayn C, Copeland G, Cozen W, Peters ES, Huang Y, Saber MS, Altekruse S, Goodman MT; HPV Typing of Cancers Workgroup. US assessment of HPV types in cancers: implications for current and 9-valent HPV vaccines. J Natl Cancer Inst. 2015 Apr 29;107(6):djv086. doi: 10.1093/jnci/djv086[↩]
- How Many Cancers Are Linked with HPV Each Year? https://www.cdc.gov/cancer/hpv/statistics/cases.htm[↩]
- Human papillomavirus vaccination: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2014;63. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6305a1.htm[↩][↩]
- Chesson HW, Dunne EF, Hariri S, Markowitz LE. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex Transm Dis 2014;41:660–4. 10.1097/OLQ.0000000000000193[↩]
- Winer RL, Hughes JP, Feng Q, Stern JE, Xi LF, Koutsky LA. Incident detection of high-risk human papillomavirus infections in a cohort of high-risk women aged 25–65 years. J Infect Dis 2016;214:665–75. 10.1093/infdis/jiw074[↩]
- Human Papillomavirus (HPV) Vaccination: What Everyone Should Know. https://www.cdc.gov/vaccines/vpd/hpv/public[↩][↩]
- Schiffman M, Doorbar J, Wentzensen N, de Sanjosé S, Fakhry C, Monk BJ, Stanley MA, Franceschi S. Carcinogenic human papillomavirus infection. Nat Rev Dis Primers. 2016 Dec 1;2:16086. doi: 10.1038/nrdp.2016.86[↩]
- Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, Markowitz LE. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. 2019 Aug 16;68(32):698-702. doi: 10.15585/mmwr.mm6832a3[↩]
- Human Papillomavirus (HPV). https://www.immunize.org/askexperts/experts_hpv.asp[↩]





{kind=link}