Contents
What is Waldenstrom macroglobulinemia
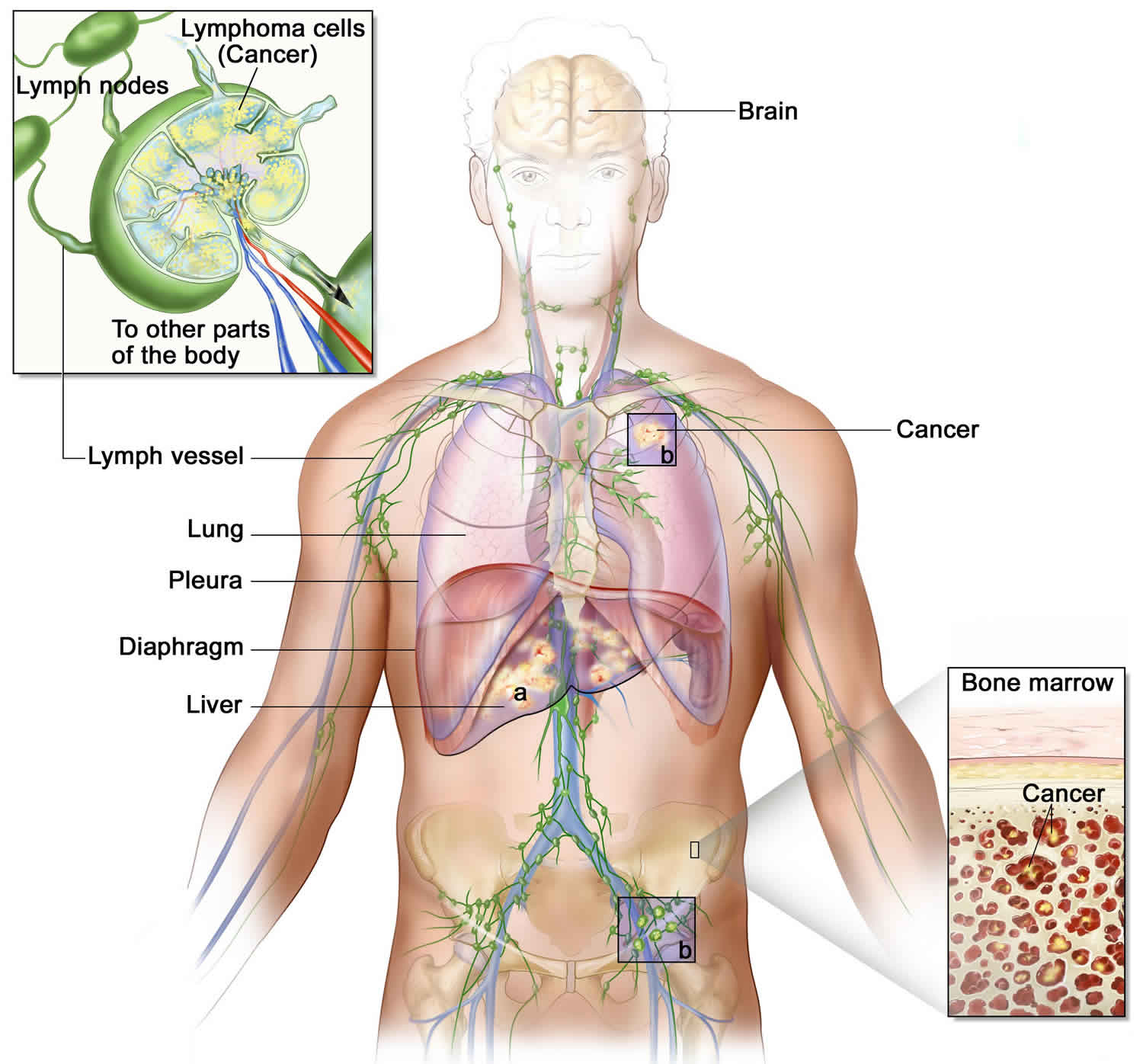
Waldenstrom macroglobulinemia is a type of non-Hodgkin lymphoma 1. Waldenstrom macroglobulinemia is a rare blood cell cancer that starts in B cells (B lymphocytes) that is characterized by an excess of abnormal white blood cells called lymphoplasmacytic cells in the bone marrow. The cancer cells make large amounts of an abnormal protein (called a macroglobulin). Another name for Waldenstrom macroglobulinemia is lymphoplasmacytic lymphoma. This condition used to be called Waldenstrom’s macroglobulinemia, so some people refer to it as Waldenstrom’s.
Waldenstrom macroglobulinemia affects an estimated 3 per million people each year in the United States. Approximately 1,500 new cases of the condition are diagnosed each year in this country, and whites are more commonly affected than African Americans. For unknown reasons, the condition occurs twice as often in men than women.
Waldenstrom macroglobulinemia usually begins in a person’s sixties and is a slow-growing (indolent) cancer. Some affected individuals have elevated levels of IgM and lymphoplasmacytic cells but no symptoms of the condition; in these cases, the disease is usually found incidentally by a blood test taken for another reason. These individuals are diagnosed with smoldering (or asymptomatic) Waldenström macroglobulinemia. It can be several years before this form of the condition progresses to the symptomatic form.
To understand Waldenstrom macroglobulinemia, it helps to know about the functions of lymphoid tissue in the body.
Lymphoid tissue and the immune system
Lymphoid tissue is made up several types of immune system cells that work together to help the body resist infections. Lymphoid tissue is found in many places in the body:
- Lymph nodes, which are pea-sized collections of immune system cells throughout the body, including in the underarm area, in the groin, on the sides of the neck, and inside the chest and abdomen
- Bone marrow, the soft inner part of certain bones where new blood cells are made
- The thymus, a small organ behind the chest bone and in front of the heart
- The spleen, an organ on the left side of the abdomen next to the stomach
- The tonsils and adenoids in the throat
- Throughout body systems like the digestive system and respiratory system
Lymphocytes (lymph cells) are the main cells of lymphoid tissue. The 2 main types of lymphocytes are:
- B lymphocytes (B cells) respond to an infection by changing into a different type of cell called a plasma cell. Plasma cells make proteins called antibodies (also called immunoglobulins) that help the body attack and kill disease-causing germs like bacteria.
- T lymphocytes (T cells) help direct immune responses, but they also can kill invading germs directly.
Figure 1. Locations of major lymph nodes
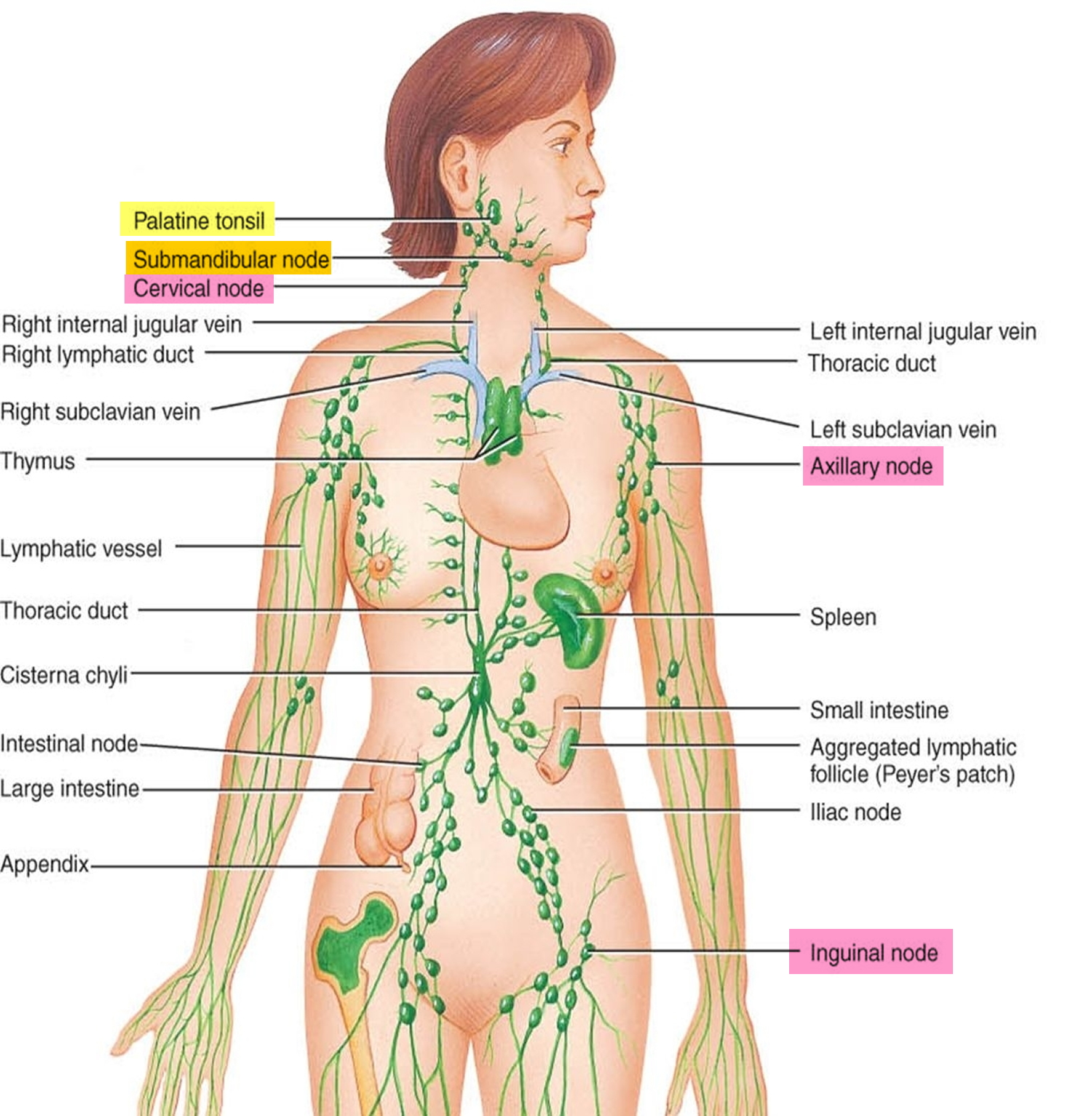
Figure 2. Functions of lymph nodes in the lymphatic system
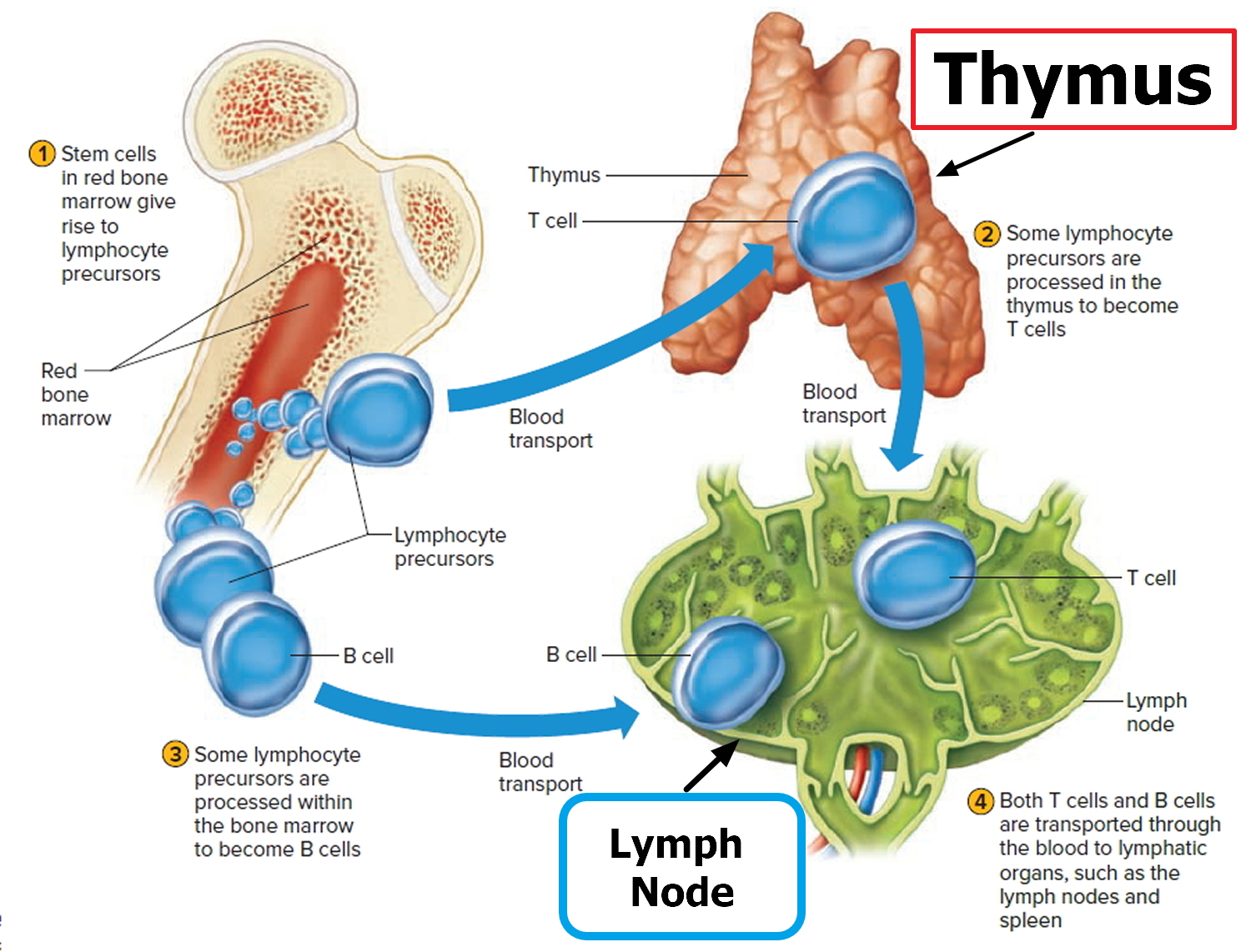
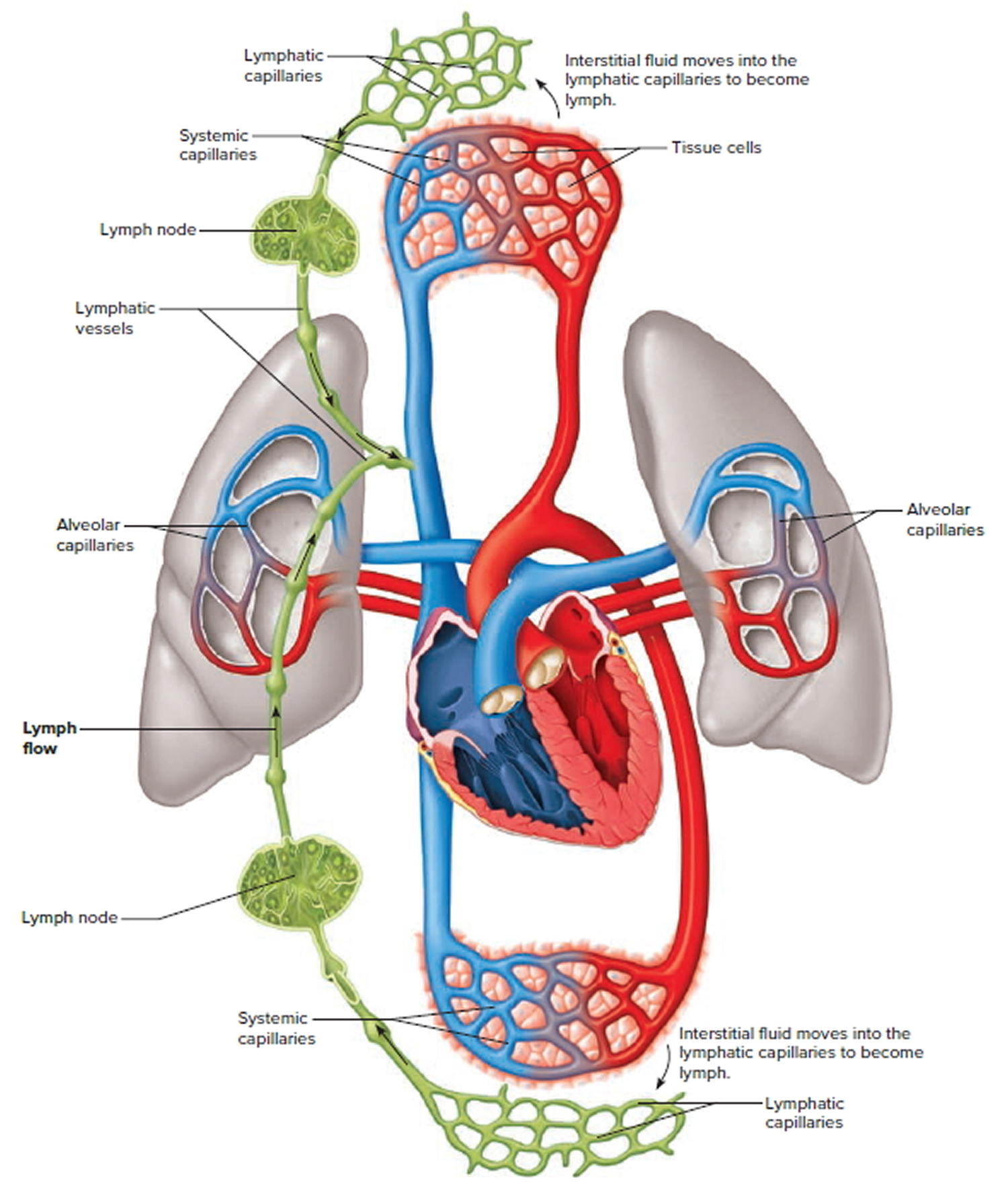
Figure 3. Schematic representation of lymphatic vessels transporting fluid from interstitial spaces to the bloodstream. Depending on its origin, lymph enters the right or left subclavian vein.
Waldenstrom macroglobulinemia is a cancer that starts in B cells. The cancer cells in people with Waldenstrom macroglobulinemia are similar to those of 2 other types of cancer: multiple myeloma and non-Hodgkin lymphoma. Multiple myeloma is considered a cancer of plasma cells, and non-Hodgkin lymphoma is a cancer of lymphocytes. Waldenstrom macroglobulinemia cells have features of both plasma cells and lymphocytes and are called lymphoplasmacytoid.
Waldenstrom macroglobulinemia cells make large amounts of a certain type of antibody (immunoglobulin M, or IgM), which is known as a macroglobulin. Each antibody (protein) made by the Waldenstrom macroglobulinemia cells is the same, so it is called a monoclonal protein, or just an M protein. The buildup of this M protein in the body can lead to many of the symptoms of Waldenstrom macroglobulinemia, including excess bleeding, problems with vision, and nervous system problems.
The Waldenstrom macroglobulinemia cells grow mainly in the bone marrow, where they can crowd out the normal cells that make the different types of blood cells. This can lead to low levels of red blood cells (called anemia), which can make people feel tired and weak. It can also cause low numbers of white blood cells, which makes it hard for the body to fight infection. The numbers of platelets in the blood can also drop, leading to increased bleeding and bruising.
Individuals with symptomatic Waldenstrom macroglobulinemia can experience general symptoms such as fever, night sweats, and weight loss. Several other signs and symptoms of the condition are related to the excess IgM, which can thicken blood and impair circulation, causing a condition known as hyperviscosity syndrome. Features related to hyperviscosity syndrome include bleeding in the nose or mouth, blurring or loss of vision, headache, dizziness, and difficulty coordinating movements (ataxia). In some affected individuals, the IgM proteins clump together in the hands and feet, where the body temperature is cooler than at the center of the body. These proteins are then referred to as cryoglobulins, and their clumping causes a condition known as cryoglobulinemia. Cryoglobulinemia can lead to pain in the hands and feet or episodes of Raynaud phenomenon, in which the fingers and toes turn white or blue in response to cold temperatures. The IgM protein can also build up in organs such as the heart and kidneys, causing a condition called amyloidosis, which can lead to heart and kidney problems. Some people with Waldenström macroglobulinemia develop a loss of sensation and weakness in the limbs (peripheral neuropathy). Doctors are unsure why this feature occurs, although they speculate that the IgM protein attaches to the protective covering of nerve cells (myelin) and breaks it down. The damaged nerves cannot carry signals normally, leading to neuropathy.
Lymphoma cells can also grow in organs like the liver and spleen, causing these organs to swell and leading to abdominal pain.
Other features of Waldenstrom macroglobulinemia are due to the accumulation of lymphoplasmacytic cells in different tissues. For example, accumulation of these cells can lead to an enlarged liver (hepatomegaly), spleen (splenomegaly), or lymph nodes (lymphadenopathy). In the bone marrow, the lymphoplasmacytic cells interfere with normal blood cell development, causing a shortage of normal blood cells (pancytopenia). Excessive tiredness (fatigue) due to a reduction in red blood cells (anemia) is common in affected individuals.
People with Waldenstrom macroglobulinemia have an increased risk of developing other cancers of the blood or other tissues.
Waldenstrom macroglobulinemia is generally not considered to be curable, but it is treatable. Many different medicines can help keep Waldenstrom macroglobulinemia under control, often for long periods of time.
Not everyone with Waldenstrom macroglobulinemia needs treatment right away. In fact, some people are diagnosed with Waldenstrom macroglobulinemia before they even have symptoms from it. Most experts recommend that people with Waldenstrom macroglobulinemia should not usually be treated until the disease is causing problems. This lets people avoid the side effects of chemotherapy (chemo), targeted therapy, or immunotherapy drugs until they really need these medicines. In fact, studies suggest that patients who delay treatment until their Waldenstrom macroglobulinemia is causing problems do not live any less time than those who start treatment as soon as they are diagnosed.
Waldenstrom macroglobulinemia survival rate
Survival rates are often used by doctors as a way of discussing a person’s outlook. Survival rates tell you what percentage of people with the same type and stage of cancer are still alive a certain length of time (usually 5 years) after they were diagnosed. These numbers can’t tell you how long you will live, but they may help give you a better understanding about how likely it is that your treatment will be successful.
Cancer survival rates don’t tell the whole story. Survival rates are often based on previous outcomes of large numbers of people who had the disease, but they can’t predict what will happen in any particular person’s case. There are a number of limitations to remember:
- The numbers below are among the most current available. But to get 5-year survival rates, doctors look at people who were treated at least 5 years ago. As treatments are improving over time, people who are now being diagnosed with ovarian cancer may have a better outlook than these statistics show.
- The statistics below are based on the stage of the cancer when it was first diagnosed. They do not apply to cancers that come back later or spread, for example.
- Besides the cancer stage, many other factors can affect a person’s outlook, such as age and overall health, and how well the cancer responds to treatment.
Your doctor can tell you how these numbers may apply to you, as he or she is familiar with the aspects of your particular situation.
Experts have used these factors to develop a system that helps predict prognosis (outlook) for patients with WM. It is called the International Prognostic Scoring System for Waldenstrom Macroglobulinemia (ISSWM). This system takes into account the factors that seem to predict a poorer outcome, such as:
- Older than 65
- Blood hemoglobin level 11.5 g/dL or less
- Platelet count 100,000/mcL or less
- Beta-2 microglobulin more than 3 mg/L
- Monoclonal IgM level more than 7 g/dL
Except for age, each of these factors is worth a single point. The points are added to make a score, which is used to divide patients into 3 risk groups:
- The low-risk group includes patients 65 or younger who have no more than 1 point.
- The intermediate-risk group includes those who are older than 65 with 2 or fewer points, and those younger than 65 who have 2 points.
- The high-risk group includes those of any age who have at least 3 points.
These groups can be used to help predict survival.
According to the National Cancer Institute’s SEER database (based on people diagnosed between 2001 and 2010), the overall relative 5-year survival of people with Waldenstrom macroglobulinemia is about 78% 2.
The group that created the International Prognostic Scoring System for Waldenstrom Macroglobulinemia (ISSWM) used data from about 600 patients with Waldenstrom macroglobulinemia who were diagnosed and treated before January 2002 to develop their risk groups:
| ISSWM risk group | 5-year survival rate |
| Low | 87% |
| Intermediate | 68% |
| High | 36% |
Median survival
Median survival is another way to look at survival. It is the length of time at which half of the patients in a group are still alive, and half have died. By definition, half of the patients live longer than the median survival. The group that developed the International Prognostic Scoring System for Waldenstrom Macroglobulinemia used data from Waldenstrom macroglobulinemia patients diagnosed and treated before January 2002 and found the following:
| ISSWM risk group | Median survival* |
| Low | 12 years |
| Intermediate | 8 years |
| High | 3.5 years |
*Median survival is measured from the point that treatment is started.
In the last decade (2001-2010), the median overall survival for all Waldenstrom macroglobulinemia groups has improved to just over 8 years compared to 6 years in the previous decade (1991-2000).
[Source 2]Waldenstrom macroglobulinemia signs and symptoms
Waldenstrom macroglobulinemia is slow growing and may not cause signs and symptoms for many years.
When Waldenstrom macroglobulinemia does cause symptoms, some of them can be like those seen with other types of non-Hodgkin lymphoma (NHL). For example, weight loss, fever, night sweats, and swollen lymph nodes can be seen in many types of non-Hodgkin lymphoma.
Waldenstrom macroglobulinemia signs and symptoms may include:
- Easy bruising
- Bleeding from the nose or the gums
- Fatigue
- Weight loss
- Numbness in your hands or feet
- Fever
- Headache
- Shortness of breath
- Changes in vision
- Confusion
Other Waldenstrom macroglobulinemia symptoms are caused by the large amounts of abnormal IgM antibody (M protein) made by the cancer cells:
- In hyperviscosity syndrome, too much of the M protein in the blood can cause it to become too “thick.” (This is not the kind of thickness that can be treated with drugs known as blood thinners.) When the blood gets too thick, it has trouble moving through blood vessels. This can cause problems such as poor circulation to the brain, which can lead to symptoms like those from a stroke.
- If the M protein only thickens the blood in cooler parts of the body (like in the tip of the nose, ears, fingers, and toes), it is called a cryoglobulin. Cryoglobulins can cause pain or other problems in these areas if a person is exposed to cooler temperatures.
- A condition called amyloidosis can occur when a part of the IgM antibody (called the light chain) builds up in organs like the heart and kidneys. This buildup can lead to heart and kidney problems.
Not all people with Waldenstrom macroglobulinemia develop hyperviscosity, cryoglobulins, or amyloidosis.
Common symptoms of Waldenstrom macroglobulinemia
Weakness: This is one of the most common symptoms of Waldenstrom macroglobulinemia. It can be caused by anemia (too few red blood cells), which can happen when the Waldenstrom macroglobulinemia cells crowd out normal cells in the bone marrow. Some people also feel weak when the blood thickens from the buildup of the abnormal protein.
Loss of appetite: Some people with Waldenstrom macroglobulinemia lose their appetite.
Fever, sweats, weight loss: Waldenstrom macroglobulinemia, like other lymphomas, can cause fevers (without an infection), drenching night sweats, and weight loss (without trying). These are called B symptoms.
Neuropathy: In some people with Waldenstrom macroglobulinemia, the abnormal antibody can attack and damage nerves outside the brain. This can lead to numbness or a painful “pins and needles” sensation in the feet and legs, which is called neuropathy.
Less common signs and symptoms of Waldenstrom macroglobulinemia
Enlarged lymph nodes: These usually appear as lumps under the skin around the neck, in the groin, or in the armpits. Enlarged lymph nodes are usually about 1 or 2 inches (2.5-5 cm) across. They are seen less often in Waldenstrom macroglobulinemia than in most other lymphomas.
Swollen abdomen (belly): Waldenstrom macroglobulinemia can sometimes make the spleen or liver bigger, making the belly look swollen. In the upper part of the abdomen, the liver is on the right and the spleen on the left. When the spleen gets larger, it can press on the stomach, which makes people feel full when they eat even a small amount.
Circulation system symptoms: In hyperviscosity syndrome, the thickened blood causes poor brain circulation, leading to problems like headache, confusion, and dizziness. It can also cause symptoms like those seen with a stroke, including slurred speech and weakness on one side of the body. Patients with these symptoms should contact their doctor right away.
Abnormal bleeding: High levels of abnormal antibody can damage blood vessels, which can lead to problems like nosebleeds and bleeding gums.
Vision problems: Bleeding around the small blood vessels inside the eyes or poor circulation in these vessels caused by thickened blood might lead to blurred vision or blind spots.
Kidney problems: High levels of the M protein can damage the kidneys directly or through the development of amyloidosis. When the kidneys don’t work well, excess salt, fluid, and body waste products stay in the blood. This can cause symptoms like weakness, trouble breathing, and fluid buildup in body tissues.
Heart problems: High levels of the M protein can damage heart tissue directly or through the development of amyloidosis, in which the protein builds up in the heart muscle. This weakens the heart, affecting its ability to pump blood. In addition, because the blood of people with Waldenstrom macroglobulinemia is thicker than normal, their hearts have to work harder to pump blood throughout the body. This strain can wear down the heart muscle, leading to a condition called congestive heart failure. Symptoms can include heart palpitations, feeling tired and weak, cough, shortness of breath, rapid weight gain, and swelling in the feet and legs.
Infections: The high levels of abnormal antibody in Waldenstrom macroglobulinemia can slow the body’s normal antibody production. This makes it harder for the body to fight infections.
Digestive symptoms: In some people with Waldenstrom macroglobulinemia, the buildup of the M protein in the intestines can lead to problems such as diarrhea, poor absorption of vitamins, or gastrointestinal bleeding (seen as blood in the stools or dark stools).
Sensitivity to cold: In people with cryoglobulins, exposure to cold temperatures can lead to pain, itching, a bluish color, or even sores on the tip of the nose, ears, fingers, or toes due to reduced blood flow to these areas.
Waldenstrom macroglobulinemia causes
It’s not clear what causes Waldenstrom macroglobulinemia.
Doctors know that the disease begins with one abnormal white blood cell that develops errors (mutations) in its genetic code. The errors tell the cell to continue multiplying rapidly.
Because cancer cells don’t mature and then die as normal cells do, they accumulate, eventually overwhelming production of healthy cells. In the bone marrow — the soft, blood-producing tissue that fills in the center of most of your bones — Waldenstrom macroglobulinemia cells crowd out healthy blood cells.
Waldenstrom macroglobulinemia cells continue trying to produce antibodies, as healthy white blood cells do, but instead they produce abnormal proteins that the body can’t use. The protein immunoglobulin M (IgM) accumulates in the blood, impairs circulation and causes complications.
Risk factors for developing Waldenstrom macroglobulinemia
Researchers have found a few risk factors that make a person more likely to develop Waldenstrom macroglobulinemia (Waldenstrom macroglobulinemia). But most people with these risk factors never develop Waldenstrom macroglobulinemia.
Factors that may increase your risk of Waldenstrom macroglobulinemia include:
- Being older. Waldenstrom macroglobulinemia can occur at any age, but it’s most often diagnosed in adults 65 and older.
- Being male. Males are more likely to be diagnosed with Waldenstrom macroglobulinemia.
- Being white. White people are more likely to develop the disease, compared with people of other races.
- Having a family history of lymphoma. If you have a relative who has been diagnosed with Waldenstrom macroglobulinemia or another type of B-cell lymphoma, you may have an increased risk.
- Hepatitis C. Hepatitis C is caused by infection with a virus (known as the hepatitis C virus, or HCV). Some studies have found that people with chronic hepatitis C infection might be more likely to develop Waldenstrom macroglobulinemia than people without the virus. But not all studies have found such a link.
- Certain autoimmune diseases. Some research has suggested that people with certain types of autoimmune disease, such as Sjögren (Sjogren) syndrome, might be at higher risk for Waldenstrom macroglobulinemia.
- Monoclonal gammopathy of undetermined significance (MGUS). Monoclonal gammopathy of undetermined significance (MGUS) is an abnormality of antibody-making cells that is related to multiple myeloma and Waldenstrom macroglobulinemia. In MGUS, like Waldenstrom macroglobulinemia and multiple myeloma, abnormal cells in the bone marrow make large amounts of one particular antibody. This antibody is called a monoclonal (or M) protein, and the condition is called a monoclonal gammopathy. MGUS itself does not cause health problems, but each year about 1% to 2% of people with MGUS go on to develop a related cancer (like multiple myeloma, Waldenstrom macroglobulinemia, or lymphoma) or another serious health problem (like amyloidosis).
Can Waldenstrom macroglobulinemia be prevented?
Most of the risk factors for Waldenstrom macroglobulinemia (Waldenstrom macroglobulinemia), such as older age or monoclonal gammopathy of undetermined significance (MGUS), can’t be changed or controlled, so there is no way to prevent cancers that might be related to these risk factors.
Some research suggests that people with hepatitis C might be more likely to develop Waldenstrom macroglobulinemia. There is currently no vaccine to prevent hepatitis C, but there are ways to lower your risk of getting it, such as avoiding known risk factors like injection drug use or unprotected sex with many partners. Hepatitis C can also be treated effectively in many cases, although it’s not known how this might affect a person’s risk of Waldenstrom macroglobulinemia.
Waldenstrom macroglobulinemia diagnosis
Waldenstrom macroglobulinemia (Waldenstrom macroglobulinemia) is often found when a person goes to see their doctor because of symptoms they are having, or because they just don’t feel well and go in for a checkup. Sometimes it’s found in people without symptoms when they have blood tests done for some other reason.
If signs or symptoms suggest that a person might have Waldenstrom macroglobulinemia, exams and tests will be done to be sure. The most important tests will look for abnormal proteins in the blood and abnormal cells in the bone marrow. Because Waldenstrom macroglobulinemia is a type of lymphoma, like other lymphomas it can invade the bone marrow, lymph nodes, and other organs.
Tests and procedures used to diagnose Waldenstrom macroglobulinemia include:
Lab tests
Waldenstrom macroglobulinemia might be suspected if your doctor finds you have low blood cell counts or unusual protein levels on blood tests. If so, your doctor may order a blood test called serum protein electrophoresis to find out what the abnormal proteins are. It is usually only after these tests are done that a biopsy of either the bone marrow or a lymph node is considered.
Blood cell counts
The complete blood count (CBC) is a test that measures the levels of red blood cells, white blood cells, and platelets. If lymphoma cells occupy too much of the bone marrow, these blood levels may be low.
Immunoglobulin levels
This test measures the levels of the different antibodies (immunoglobulins) in the blood – IgA, IgE, IgG, and IgM – to see if any are abnormally high or low. In Waldenstrom macroglobulinemia the level of IgM is high but the IgG level is often low.
Electrophoresis
The abnormal immunoglobulin made in Waldenstrom macroglobulinemia is an IgM antibody. This antibody is monoclonal, meaning that it is many copies of the exact same antibody. Serum protein electrophoresis (or SPEP) is a test that measures the total amount of immunoglobulins in the blood and finds any monoclonal immunoglobulin. Another test, such as immunofixation electrophoresis, is then used to determine the type of antibody that is abnormal (IgM or some other type).
Finding a monoclonal IgM antibody in the blood is needed to diagnose Waldenstrom macroglobulinemia. This abnormal protein in Waldenstrom macroglobulinemia is known by many different names, including monoclonal immunoglobulin M, IgM protein, IgM spike, IgM paraprotein, M protein, and M-spike. High levels of other types of monoclonal immunoglobulins, like IgA or IgG, are seen in different disorders (like multiple myeloma and some other lymphomas).
Sometimes pieces of the IgM protein are excreted by the kidneys into the urine. These proteins can be detected with a test called urine protein electrophoresis.
Viscosity
Viscosity is a measure of how thick the blood is. If the IgM level is too high, the blood will become thick (viscous) and can’t flow freely (think about pouring honey compared to pouring water).
Cryocrit
This test measures the blood levels of cryoglobulins (proteins that clump together in cool temperatures and can block blood vessels).
Cold agglutinins
Cold agglutinins are antibodies that attack and kill red blood cells, especially at cooler temperatures. These dead cells can then build up and block blood vessels. A blood test can be used to detect these antibodies.
Beta-2 microglobulin (β2M)
This test measures another protein made by the cancer cells in Waldenstrom macroglobulinemia. This protein itself doesn’t cause any problems, but it’s a useful indicator of a patient’s prognosis (outlook). High levels of β2M are linked with a worse outlook.
Biopsies
The symptoms of Waldenstrom macroglobulinemia and non-Hodgkin lymphoma (NHL) are not distinctive enough for a doctor to know for certain if a person has one of them, based on symptoms alone. Most symptoms can also be caused by non-cancerous problems like infections or by other kinds of cancers. Blood tests can help point to the correct diagnosis, but a biopsy (removing samples of affected tissue to look at under a microscope) is the only way to be sure. Several types of biopsies might be used.
Bone marrow aspiration and biopsy
This is the most important type of biopsy for Waldenstrom macroglobulinemia, and is needed to confirm the diagnosis. It can be done at the doctor’s office or at the hospital.
The bone marrow aspiration and biopsy are usually done at the same time. The samples are taken from the back of the pelvic (hip) bone, although in some cases they may be taken from the sternum (breast bone) or other bones.
- In bone marrow aspiration, you lie on a table (either on your side or on your belly). The doctor cleans the skin over the hip and then numbs the area and the surface of the bone by injecting a local anesthetic. This may briefly sting or burn. A thin, hollow needle is then inserted into the bone, and a syringe is used to suck out a small amount of liquid bone marrow. Even with the anesthetic, most patients still have some brief pain when the marrow is removed.
- A bone marrow biopsy is usually done just after the aspiration. A small piece of bone and marrow is removed with a slightly larger needle that is pushed down into the bone. This may also cause some brief pain.
Once the biopsy is done, pressure is applied to the site to help stop any bleeding. There will be some soreness in the biopsy area when the numbing medicine wears off. Most patients can go home right after the procedure.
The bone marrow samples are then sent to a lab, where they are tested to see if they have lymphoma cells (see below). For a diagnosis of Waldenstrom macroglobulinemia, at least 10% of the cells in the bone marrow must be lymphoplasmacytoid lymphoma cells.
Fine needle aspiration (FNA) biopsy
In an FNA biopsy, the doctor uses a very thin, hollow needle with a syringe to withdraw a small amount of tissue from a tumor or lymph node. This type of biopsy is useful for sampling lymph nodes to see if they are enlarged because of cancer or an infection. FNA can help diagnose some lymphomas, but Waldenstrom macroglobulinemia is usually diagnosed with a bone marrow biopsy.
For an FNA on an enlarged node near the surface of the body, the doctor can aim the needle while feeling the node. If the enlarged node (or tumor) is deep inside the body, the needle can be guided while it is seen on a computed tomography (CT) scan or ultrasound (see the descriptions of imaging tests later in this section).
The main advantage of FNA is that it does not require surgery and can often be done in a doctor’s office. The main drawback is that in some cases it might not get enough tissue to make a definite diagnosis of lymphoma. However, advances in lab tests (discussed later in this section) and the growing experience of many doctors with FNA have improved the accuracy of this procedure.
Excisional or incisional biopsy
For these types of biopsies, a surgeon cuts through the skin to remove an entire lymph node or tumor (excisional biopsy) or just a small part of a large tumor or lymph node (incisional biopsy). These biopsies are rarely needed in people with Waldenstrom macroglobulinemia because the diagnosis is usually made with a bone marrow biopsy. They are used more often for other types of lymphoma.
If the area to be biopsied is near the skin surface, this can be done using local anesthesia (numbing medicine). If the area is inside the chest or abdomen, general anesthesia or deep sedation is used (where the patient is asleep). These types of biopsies almost always provide enough tissue to diagnose the exact type of lymphoma.
Fat pad fine needle aspiration
This type of biopsy may be used in some people with Waldenstrom macroglobulinemia to check for amyloid. In this procedure, a thin, hollow needle with a syringe attached is inserted into an area of fat (usually under the skin of the abdomen/belly). A small amount of fat is removed and sent to the lab for testing.
Lab tests on biopsy specimens
All biopsy specimens are looked at in the lab by a pathologist – a doctor with special training in using lab tests to diagnose diseases. In some cases, a hematopathologist, a doctor with further training in diagnosing blood and lymph node diseases, might also look at the biopsy. The doctors look at the size and shape of the cells and how they are arranged. Sometimes just looking at the cells doesn’t provide a clear answer, so other lab tests are needed.
Immunohistochemistry
In this test, a part of the biopsy sample is treated with special man-made antibodies that attach to cells only if they contain specific proteins. These antibodies cause color changes in the cells, which can be seen with a microscope. This test may help tell different types of lymphoma from one another and from other diseases.
Flow cytometry
In this test, cells are treated with special man-made antibodies. Each antibody sticks only to certain types of cells. The cells are then passed in front of a laser beam. If the cells now have antibodies attached to them, the laser will make them give off light, which is measured and analyzed by a computer.
This is the most common test for immunophenotyping – classifying lymphoma cells according to the proteins (antigens) on their surfaces. Different types of lymphocytes have different antigens on their surface. These antigens also change as each cell matures.
This test can help show if a lymph node is swollen because of lymphoma, some other cancer, or a non-cancerous disease. It has become very important in helping doctors determine the exact type of lymphoma so they can select the best treatment.
Cytogenetics
Doctors use this technique to look at the chromosomes (long strands of DNA) inside lymphoma cells. Cells (usually from the bone marrow) are first grown in the lab. Then the chromosomes are stained and looked at closely. Because it takes time for the cells to start dividing, this test can take a few weeks.
In some lymphomas, the cells may have too many chromosomes, too few chromosomes, missing parts of chromosomes (called deletions), or other abnormalities. These changes can help identify the type of lymphoma.
Molecular genetic tests
Molecular tests such as fluorescent in situ hybridization (FISH) and polymerase chain reaction (PCR) are not usually needed to diagnose Waldenstrom macroglobulinemia, but they are sometimes used to diagnose other types of non-Hodgkin lymphoma. These tests look at the cells’ DNA without having to grow the cells in the lab first. The tests can give results in less time than cytogenetics and can be done on cells from different sources (like lymph nodes, blood, and bone marrow). They are generally used to look for specific chromosome or gene changes, not just any change.
Imaging tests
Imaging tests use x-rays, magnetic fields, sound waves, or radioactive particles to produce pictures of the inside of the body. These tests are not needed to diagnose Waldenstrom macroglobulinemia, but one or more of them might be done to help show how much disease and where it is in the body.
Chest x-ray
An x-ray might be done to look at the chest for enlarged lymph nodes.
Computed tomography (CT) scan
The CT scan is an x-ray that makes detailed cross-sectional images of your body. Unlike a regular x-ray, CT scans can show the detail in soft tissues (such as internal organs). This scan can help show if any lymph nodes or organs in your body are enlarged. CT scans are useful for looking for signs of lymphoma in the chest, abdomen, and pelvis.
CT-guided needle biopsy: CT scans can also be used to guide a biopsy needle into a suspicious area. For this procedure, the patient lies on the CT scanning table while the doctor moves a biopsy needle through the skin and toward the area. CT scans are repeated until the needle is in the right place. A biopsy sample is then removed and sent to the lab.
Magnetic resonance imaging (MRI) scan
This test is rarely used in Waldenstrom macroglobulinemia, but if your doctor is concerned about the brain or spinal cord, MRI is very useful for looking at these areas.
Ultrasound
Ultrasound can be used to look at lymph nodes near the surface of the body or to look inside your abdomen for enlarged lymph nodes or organs such as the liver, spleen, and kidneys. (It can’t be used to look at organs or lymph nodes in the chest because the ribs block the sound waves.) It is sometimes used to help guide a biopsy needle into an enlarged lymph node.
Positron emission tomography (PET) scan
A PET scan can be helpful in spotting small collections of cancer cells. It is even more valuable when combined with a CT scan (PET/CT scan).
PET scans also can help tell if an enlarged lymph node contains lymphoma or not. It can help spot small areas that might be lymphoma, even if the area looks normal on a CT scan. These tests can be used to tell if a lymphoma is responding to treatment. They can also be used after treatment to help decide whether an enlarged lymph node still contains lymphoma or is merely scar tissue.
Waldenstrom macroglobulinemia treatment
Waldenstrom macroglobulinemia is generally not considered to be curable, but it is treatable. Many different medicines can help keep Waldenstrom macroglobulinemia under control, often for long periods of time.
Not everyone with Waldenstrom macroglobulinemia needs treatment right away. In fact, some people are diagnosed with Waldenstrom macroglobulinemia before they even have symptoms from it. Most experts recommend that people with Waldenstrom macroglobulinemia should not usually be treated until the disease is causing problems. This lets people avoid the side effects of chemotherapy (chemo), targeted therapy, or immunotherapy drugs until they really need these medicines. In fact, studies suggest that patients who delay treatment until their Waldenstrom macroglobulinemia is causing problems do not live any less time than those who start treatment as soon as they are diagnosed.
Treatment options for Waldenstrom macroglobulinemia may include:
- Observation. If IgM proteins are found in your blood, but you don’t have any signs or symptoms, you may choose to wait before beginning treatment. Your doctor may recommend blood tests every few months to monitor your condition. You may go years without needing further treatment.
- Plasma exchange. If you experience signs and symptoms related to having too many IgM proteins in your blood, your doctor may recommend plasma exchange (plasmapheresis) to remove the proteins and replace them with healthy blood plasma.
- Chemotherapy. Chemotherapy is a drug treatment that kills quickly growing cells, such as the abnormal blood cells produced by Waldenstrom macroglobulinemia. Chemotherapy may be used alone or combined with other drug treatments as an initial treatment for people who experience signs and symptoms of Waldenstrom macroglobulinemia. High-dose chemotherapy may also be used to suppress your bone marrow production in preparation for a bone marrow transplant.
- Targeted therapy. Targeted therapy drugs kill cancer cells by focusing on the specific abnormalities present in the cancer cells that allow them to survive. Targeted therapy drugs may be used alone or combined with other medications, such as chemotherapy or biological therapy, as an initial treatment for Waldenstrom macroglobulinemia or in cases where the cancer returns despite treatment.
- Biological therapy. Biological therapy drugs use your immune system to kill cancer cells. Biological therapy drugs can be used alone or in combination with other medications as an initial treatment or as a treatment for recurrent Waldenstrom macroglobulinemia.
- Bone marrow transplant. In certain highly selected situations, a bone marrow transplant, also known as a stem cell transplant, may be used to treat Waldenstrom macroglobulinemia. During this procedure, high doses of chemotherapy are used to wipe out your diseased bone marrow. Healthy blood stem cells are infused into your body where they can rebuild healthy bone marrow.
- Clinical trials. Clinical trials give you a chance to try the latest in Waldenstrom macroglobulinemia treatment.
Doctors agree that hyperviscosity syndrome is a reason to treat with plasmapheresis right away, because it can be life threatening. Other reasons to start treatment include problems from amyloidosis or cryoglobulins, as well as anemia (too few red blood cells), kidney or heart problems, nerve damage, or any severe symptom from the Waldenstrom macroglobulinemia.
Once a decision has been made to start treatment, there are several options, depending on the patient’s age, general health, and symptoms. Treatment is also based on whether or not the patient might have a stem cell transplant in the future.
The drugs used to treat Waldenstrom macroglobulinemia can be given in a variety of combinations and schedules depending on the situation. Some doctors like to combine drugs (often some type of chemotherapy plus rituximab), while others prefer to start with a single drug. The patient’s age, overall health, and symptoms can also affect which treatments are recommended.
In general, rituximab is not usually given when the IgM level is very high because it can make the IgM level temporarily go up even higher. Plasmapheresis may be used first to lower the IgM level before starting rituximab. Another option is to give rituximab along with ibrutinib because the combination can rapidly reduce the level of IgM.
If a stem cell transplant might be used later on, many experts recommend not giving certain chemo drugs (chlorambucil, bendamustine, cladribine, or fludarabine) because they might affect the stem cells in the body.
Some of the drugs and combinations that might be used as the first treatment for Waldenstrom macroglobulinemia include:
- Ibrutinib, with or without rituximab
- Bendamustine, with or without rituximab
- Bortezomib, with or without dexamethasone and/or rituximab
- Chlorambucil
- Cladribine, with or without rituximab
- Cyclophosphamide, doxorubicin, vincristine, prednisone, and rituximab (CHOP-R)
- Cyclophosphamide, prednisone, and rituximab (CPR)
- Fludarabine, with or without rituximab
- Fludarabine, cyclophosphamide, and rituximab (FCR)
- Rituximab
- Rituximab, cyclophosphamide, and dexamethasone (RCD)
- Thalidomide, with or without rituximab
Other drugs and drug combinations can also be used. Talk to your doctor about which regimen might be best for you based on your situation.
During treatment, you’ll have regular visits with your doctor, who will ask you about your symptoms, do physical exams, and test your blood to see how well the treatment is working. In most people with Waldenstrom macroglobulinemia, the disease will respond to treatment (IgM levels will go down and symptoms will get better) within a few months, although this may take longer in people getting only rituximab . If the Waldenstrom macroglobulinemia responds, options include close monitoring for signs of disease progression or giving rituximab on a regular schedule to help keep the disease in check.
If treatment doesn’t work or if the disease comes back after treatment
No single treatment for Waldenstrom macroglobulinemia works for all patients. If the first drug or set of drugs doesn’t work, other drugs may be helpful.
Most people with Waldenstrom macroglobulinemia will require treatment with different drugs at some point. Often, a certain drug or combination of drugs will work at first, but over time it might stop working. Or a person might stop treatment if the Waldenstrom macroglobulinemia is under control, only to have it come back some time later. If the Waldenstrom macroglobulinemia remained under control for at least a year after the first treatment, then giving the same drug(s) again can often help bring the cancer back under control.
If the cancer comes back sooner, or if the initial treatment was not effective, then switching to another drug or drug combination is likely to be a better option. Many of the same drugs and combinations listed above as first-line treatments might be helpful here. Other drugs that might also be tried include alemtuzumab (Campath), ofatumumab (Arzerra), or everolimus (Afinitor). High-dose chemotherapy with stem cell transplant might also be an option for some patients.
If chemotherapy or other drugs are no longer slowing the growth of the Waldenstrom macroglobulinemia, some patients can still get relief from symptoms by getting plasmapheresis at regular intervals to lower the levels of the abnormal IgM protein in their blood.
Sometimes Waldenstrom macroglobulinemia can turn into an aggressive lymphoma. When this happens, the cancer grows much more quickly and causes symptoms that can soon become life threatening. These lymphomas are usually treated with a combination of several chemo drugs like those used for patients who are first diagnosed with an aggressive non-Hodgkin lymphoma. If combination chemo is not successful, high-dose chemo with a stem cell transplant may be an option.
New treatment for Waldenstrom macroglobulinemia
Many new drugs to treat Waldenstrom macroglobulinemia are being studied in clinical trials, as well as ways to use drugs already known to be effective by combining them in new ways, using different doses, or different sequences of drugs, one after another.
Some of the newer types of drugs that have shown promise or are being tested in Waldenstrom macroglobulinemia include 3:
- mTOR inhibitors, such as temsirolimus (Torisel)
- Proteasome inhibitors, such as ixazomib , carfilzomib (Kyprolis), and oprozomib
- Histone deacetylase (HDAC) inhibitors, such as panobinostat, romidepsin (Istodax), and belinostat (Beleodaq)
- Bruton tyrosine kinase (BTK) inhibitors, such as ACP-196, and AVL-292
- PI3K inhibitors, such as idelalisib (Zydelig) and buparlisib (BKM120)
- Aurora kinase inhibitors, such as alisertib
- BCL-2 inhibitor such as ABT-199
- A CXCR4 antibody such as ulocuplumab
Biological therapy
Another newer approach to Waldenstrom macroglobulinemia treatment is the use of biological response modifiers that stimulate the patient’s immune system to attack and destroy the lymphoma cells.
For example, it has recently been found that the bone marrow support tissues (stromal cells) make a substance called interleukin 6 (IL-6). IL-6 is a strong growth factor for multiple myeloma cells. IL-6 also helps cause the bone destruction seen in myeloma. Some current research efforts are trying to develop ways to block these functions of IL-6.
Bone marrow and peripheral blood stem cell transplant
Researchers are continually improving bone marrow and peripheral blood stem cell transplant methods, as well as trying to determine how helpful this type of treatment can be for people with Waldenstrom macroglobulinemia.
Vaccines
Doctors know it is possible for people with cancer to develop immune responses to their cancer. In rare instances, people’s immune systems have rejected their cancers, and they have been cured. Scientists are now studying ways to boost this immune reaction by using vaccines.
Unlike vaccines used to prevent infections, these vaccines create an immune reaction against the lymphoma cells in patients who have very early disease or whose disease is in remission but could come back or relapse. This is a major area of research in treating lymphomas (including Waldenstrom macroglobulinemia), but it is still being tested in clinical trials. You might want to consider enrolling in one of these studies.
- What Is Waldenstrom Macroglobulinemia? https://www.cancer.org/cancer/waldenstrom-macroglobulinemia/about/what-is-wm.html[↩]
- Survival Rates for Waldenstrom Macroglobulinemia. https://www.cancer.org/cancer/waldenstrom-macroglobulinemia/detection-diagnosis-staging/survival-rates.html[↩][↩][↩]
- What’s New in Waldenstrom Macroglobulinemia Research and Treatment? https://www.cancer.org/cancer/waldenstrom-macroglobulinemia/about/new-research.html[↩]





{kind=link}