
Contents
What is xanthoma
A xanthoma is a skin lesion caused by the accumulation of fat in macrophage immune cells in your skin and more rarely in the layer of fat under your skin. A xanthoma looks like a yellow to orange bump (papule) with defined borders. There may be several individual ones or they may form clusters. The growth is noncancerous and painless, but may be a sign of another medical condition.
Some types of xanthoma are indicative of lipid metabolism disorders (e.g. hyperlipidemia or high blood fats), where they may be associated with increased risk of coronary artery heart disease and occasionally with pancreatitis.
Xanthomas may be a sign of a medical condition that involves an increase in blood lipids. Such conditions include:
- Certain cancers
- Diabetes
- High blood cholesterol levels
- Inherited metabolic disorders, such as familial hypercholesterolemia
- Scarring of the liver due to blocked bile ducts (primary biliary cirrhosis)
- Inflammation and swelling of the pancreas (pancreatitis)
- Underactive thyroid (hypothyroidism)
Xanthelasma palpebra is a common type of xanthoma that appears on the eyelids (Figure 1). It usually occurs without any underlying medical condition.
Xanthomas are classified into the following types based on where they are found on the body and how they develop.
Xanthelasma palpebrarum
- Most common type of xanthoma
- Lesions arise symmetrically on upper and lower eyelids and the medial canthus
- Lesions are soft, velvety, yellow, flat papules or plaques
- Lesions start off as small bump and gradually grow larger over several months
- May or may not be associated with hyperlipidemia
The medical term xanthelasma palpebrarum is composed of two words. Xanthelasma, derived from ancient Greece where “xanthos” means yellow and “elesma” means plate. Palpebrarum is a Latin word that means “near or related to the eyelid” 1. Xanthelasma palpebrarum is a lipid-rich deposition, mainly cholesterol. Xanthelasma palpebrarum is mostly semisolid yellowish deposits that are commonly found on the medial aspect of the eyes. It is often seen along the corners of the upper and lower eyelids. Xanthelasma palpebrarum is the commonest cutaneous presentation of xanthoma which occurs over the eyelids, even with the absence of any other cutaneous or mucosal lesions. It is characterized by soft, yellowish papules and plaques that occur more commonly near the inner canthus of the eyelid more often at the upper eyelid. Lesions are usually symmetrical. There might be one or multiples.
Xanthelasma palpebrarum is a benign condition that never leads to serious consequences, but it is cosmetically bothersome, and most of the patients are unhappy about their image, and they seek medical advice. The patients visit dermatology offices, Reconstructive surgery clinics, and ophthalmology clinics looking for permanent solutions.
Xanthelasma palpebrarum is an uncommon skin lesion in the general population with a crude incidence of 1.2%. It is more common in women than in men. The age of onset ranges from 20 to 70 years, but it is most commonly seen between the age of 35 and 55 years.
About 50% of patients who develop xanthelasma have lipid disorder. It is commonly seen in patients with:
- Type 2 hyperlipidemia that includes type 2a, also known as familial hypercholesterolemia, and type 2b, which is commonly referred to as familial combined hyperlipidemia
- Type 4 hyperlipidemia, which is also known as familial hypertriglyceridemia
- Diabetes mellitus
- Hypothyroidism
- Those with low levels of HDL “good” cholesterol
Xanthelasma palpebrarum are observed also in patients who had previous erythroderma, generalized cutaneous inflammatory dermatosis, and in cases who had previous contact dermatitis. It may be a predictor of ischemic heart disease, myocardial infarction, or systemic atherosclerosis.
Management
- If LDL cholesterol levels are raised, treatment to reduce levels may improve the size of the lesions
- It is important to treat the underlying medical conditions like hyperlipidemia, liver diseases, diabetes, and thyroid disorders 1.
- Physical treatments such as curettage, laser and chemical peels using trichloroacetic acid can all help, but lesions often recur
- Invasive procedures should be the last option. Liquid nitrogen sessions are the first to be offered for the patients.
The treatment of xanthelasma involves changes in lifestyle and taking medications to lower serum lipids. Even though a low-fat diet and statins are often recommended, they have a limited effect on xanthelasmas once they have developed. If the lesions are a cosmetic concern, they can be excised by simple surgical procedure, cauterized, or removed with liquid nitrogen sessions. Surgery around the eyelids is fraught with complications and can result in ectropion, eyelid retraction, and injury to the eye itself. Use of cryotherapy and chemical cauterization can lead to severe scarring and skin discoloration.
Other methods include chemical peels utilizing trichloroacetic acid (TCA) in a high percentage of 50% or above to reach to the optimum depth for the cholesterol deposits in the reticular dermis; similar substances like salicylic acid might be used as well. Deep peels may be complicated by hyperpigmentation, especially in dark-skin individuals, so the treating physician should pay attention to this point very well.
Lasers can be used to treat selected cases of xanthelasma palpebrarum using carbon dioxide, erbium, pulsed dye, argon, and Nd:YAG lasers. Most of the patients might accept laser treatments since they are not associated with tissue destructions or loss, and its better alternative for surgery. Complications of laser therapy include pain, erythema, pigmentations, scars, and eyes injuries. Fractionated Er:YAG and/ or fractionated CO2 lasers are the most commonly used machines to treat xanthelasmas.
Radiofrequency machines can be used to treat some cases of xanthelasma because it is a very safe method compared to other modalities but it is less effective, and it might be expensive.
Even after removal, recurrence of xanthelasma is common especially due to genetics and high cholesterol levels. Lipid-lowering medications can be used in patients with high cholesterol and triglyceride levels to prevent ischemic attacks and further deposits.
Figure 1. Xanthoma eye (xanthelasma palpebrum)

Tuberous xanthoma
- Firm, painless, red-yellow nodules that develop around the pressure areas such as the knees, elbows, heels and buttocks
- Lesions can join together to form multilobated masses
- Morphology – firm, painless, red-yellow papules and nodules. The diameter can vary from 0.5 cm papules to 2.5 cm multilobulated nodules
- Usually associated with hypercholesterolemia (increased cholesterol levels in blood) and increased LDL “bad” cholesterol levels
Figure 2. Tuberous xanthoma

Figure 3. Tuberous xanthoma

Footnote: A 10-years-old boy presents as an outpatient in a rural hospital complaining of slow and multiple mass growth on extensor surface of right elbow and both knees since the age of 8 years old. He has no remarkable past medical history. On physical exam, the patient does not reveal any signs of distress, focused examination shows an arrange of small solitary masses of approximately 3×3 cm located at the extensor surfaces of right elbow (Figure 2), left and right knee. On palpation they present as a firm, mobile and non-painful nodules, smaller multiple lesions of approximately 5 mm were seen on the inferior and superior pole adjacent to the patellar region of the right and left knee respectively (Figure 3). Laboratory studies revealed a high low-density lipoprotein level measured at 623 mg/dL, a 12 lead EKG was found to have no apparent cardiac abnormalities. With biochemical results and a typical clinical presentation of tuberous xanthomas, a diagnosis of familial hypercholesterolemia was established. The patient was offered initial medical treatment with high dose statins, ezetimibe and elective surgical resection of xanthomas which occurred without any complication with surgical findings of one firm yellowish nodule located at the extensor surface of right elbow of 3×3 cm, one firm yellowish round nodule of 3×3 located on the anterolateral surface of the patella and two firm nodules at the left and inferior borders of the left patella of 3×3 cm and 2×2 cm respectively without any compromise of surrounding structures. After his surgical intervention the patient underwent an uneventful recovery and it was discharged after 16 hours of in hospital surveillance.
[Source 2 ]Tendinous xanthoma
- Appears as slowly enlarging subcutaneous nodules related to a tendon or ligament
- Most commonly found on the hands, feet, and Achilles tendon
- Morphology – slowly enlarging subcutaneous nodules related to the tendons or ligaments. As the lipid deposition is deep within the tendons, the skin is not yellow. Generally mobile, occasionally tethered
- Associated with severe hypercholesterolaemia and elevated LDL “bad” cholesterol levels
Figure 4. Tendinous xanthoma

Eruptive xanthoma
- Lesions typically erupt as crops of small, red-yellow papules
- Most commonly arise over the buttocks, shoulders, arms and legs but may occur all over the body, although facial involvement is rare
- Rarely the face and inside of the mouth may be affected
- Lesions may be tender and usually itchy
- Lesions may resolve spontaneously over a few weeks
- Associated with hypertriglyceridemia (increased triglyceride levels in blood) often in patients with diabetes mellitus (sugar diabetes)
Eruptive xanthomas are characterized by the sudden appearance of grouped, yellow–red papules scattered over the trunk, arms, legs and buttocks 3. The condition is associated with the markedly elevated serum triglyceride levels that occur with hyperlipidemia syndromes (i.e., Fredrickson–Levy types 1, 4 and 5) or with diabetes mellitus, hypothyroidism, obesity, pancreatitis, nephrotic syndrome, cholestatic liver disease, dysglobulinemia and as an adverse effect of using certain medications (e.g., estrogens, corticosteroids, systemic retinoid agents) 4. Treatment involves management of the underlying condition, whereby lesions resolve within weeks to months 5. Patients should also be counseled on lifestyle changes, including weight control, adopting a low-fat diet, exercising and quitting smoking 5.
Figure 5. Eruptive xanthoma

Footnote: A 46-year-old man with obesity, hypertension, hyperlipidemia and bipolar disorder presented with a rash accompanied by ongoing excessive urine production, excessive thirst and blurred vision. The lesions had appeared on his arms 1 month earlier and had spread to his neck, buttocks and legs. He was taking quetiapine and metoprolol. Both of the patient’s parents had type 2 diabetes mellitus. A physical examination showed crops of firm yellow–red papules (diameter 1–3 mm) distributed on the patient’s neck, bilateral extremities and buttocks, suggestive of eruptive xanthomas. Laboratory investigations showed elevated levels of triglycerides (64.2 [normal 0.6–2.8] mmol/L), cholesterol (18.2 [normal 3.1–5.2] mmol/L), acetylated hemoglobin (139.3 [normal 25.6–42.0] mmol/mol) and glucose (31.2 [normal 3.3–6.1] mmol/L). Results of kidney and liver function tests were normal, as were the results of tests for thyroid stimulating hormone, triiodothyronin, thyroxin, amylase and lipase. He was admitted to the intensive care unit, and his condition responded well to treatment with insulin, metformin and gemfibrozil. The patient’s quetiapine was stopped, and he was transitioned to topiramate without complications. The patient’s triglyceride levels improved to 13.8 mmol/L after 8 days of treatment, and his skin lesions improved after 8 weeks.
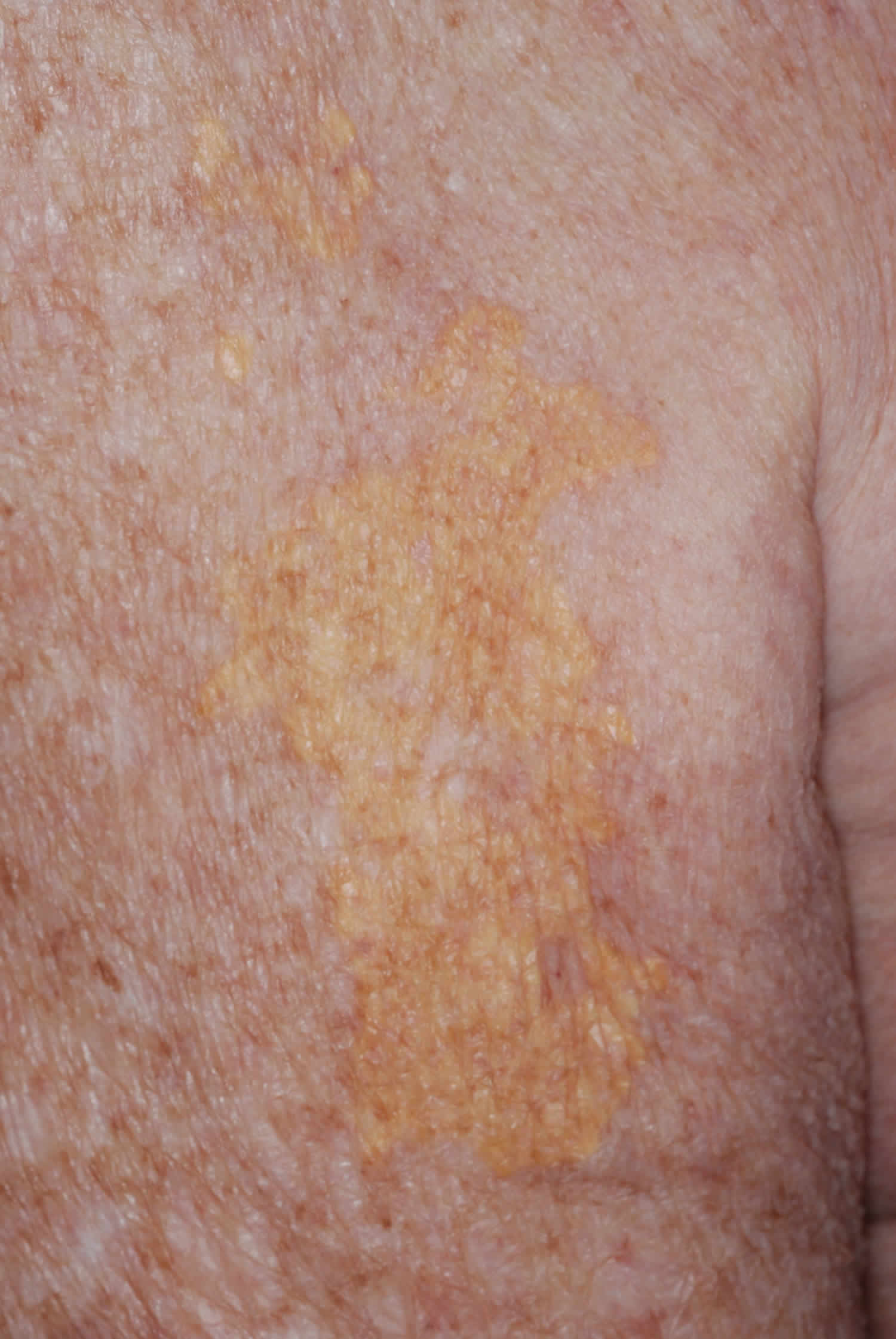
[Source 6 ]Plane xanthoma
- Lesions are multiple yellow / orange flat papules or patches that can occur anywhere on the body
- Lesions on the creases of the palms are indicative of a specific pattern of increased lipids in blood called type 3 dysbetalipoproteinemia
- May be associated with hyperlipidemia and hypertriglyceridemia
Figure 6. Plane xanthoma

Palmar xanthoma
- These have a similar appearance to plane xanthoma, but are found on the palmar creases
- Pathognomonic of type 3 / familial dysbetalipoproteinaemia
Figure 7. Palmar xanthoma

Diffuse normolipemic plane xanthomas
- A rare form of histiocytosis.
- Associated with an abnormal antibody in the blood called a paraprotein.
- Lipid levels are normal.
- About 50% will have a malignancy of the blood; usually multiple myeloma or leukaemia.
- Presents with large flat reddish-yellow plaques over the face, neck, chest, buttocks and in skin folds (such as the armpits and groin).
Diffuse normolipemic plane xanthomas are an uncommon occurrence mainly affecting adults and are associated with blood dyscrasias especially monoclonal gammopathy 7. Since the original description in 1965 a strong association of diffuse normolipemic plane xanthoma with systemic disorders, especially multiple myeloma and monoclonal gammopathy, has been established. Other disorders have also been reported in association with diffuse normolipemic plane xanthoma, including leukemia and Castleman disease 8.
The first xanthomatous plaques typically appear on the face or palpebral area and exhibit the potential for slow cutaneous progression. Hallmarks of diffuse normolipemic plane xanthomas are sheet-like xanthomas, also known as plane xanthomas, of the head, neck, trunk, and extremities. They usually present symmetrically on the body surface. Palpebral xanthelasma may also be present, but lipid levels and cholesterol are characteristically normal. On histopathology, the characteristic findings are foam cells, which are lipid-laden macrophages. There is typically no family history of significant lipid or cholesterol abnormalities. Additional cholesterol studies can be performed, such as lipoprotein A or cholesterol receptor analyses; however, these are normal.
The pathogenesis of diffuse normolipemic plane xanthomas has been attributed to the formation of complexes of monoclonal IgG and low-density lipoprotein with deposition in the skin and subsequent phagocytosis by histiocytes 9. Complement level abnormalities have also been attributed to the development of diffuse normolipemic plane xanthoma 10. Purpura and petechiae may present if immune complex aggregates lead to vasculitis. For limited cutaneous involvement, cosmetic excision, dermabrasion, or ablative laser therapy are options 11. For diffuse disease, treatment options are limited.
Diffuse normolipemic plane xanthoma is important to consider in rare cases of cutaneous xanthomatous plaques in which lipid profiles are unremarkable and there is no family history of lipid profile abnormalities or cardiovascular events occurring at young ages. Such a patient may require further evaluation for hematologic malignancies 8.
Figure 8. Diffuse normolipemic plane xanthoma

Footnote: An 80-year-old white male presented for evaluation of a six-year history of slowly increasing yellow skin lesions. He had no significant past medical history nor a family history of hypercholesterolemia or early cardiac deaths. He denied systemic complaints such as shortness of breath or chest pain. On skin examination, a yellow papule near the lateral epicanthus and a yellow macule near the temple were present (Figure 8). Multiple, well-demarcated yellow skin plaques in sheets were noted on the arms and back (see Figure 9 below). There was no involvement of his palms, tendon areas, or other parts of his skin.
[Source 8 ]Figure 9. Diffuse normolipemic plane xanthoma
Xanthoma disseminatum
- Xanthoma-like lesions due to a rare form of histiocytosis.
- Lipid metabolism is normal.
- The skin lesions usually consist of hundreds of small yellowish-brown or reddish-brown bumps, which are usually evenly spread on both sides of the face and trunk. They may particularly affect the armpits and groins.
- The small bumps may join together to form sheets of thickened skin.
- 30% of affected people have involvement of the lining of the mouth, airways or eyes (mucosal surfaces). Warty plaques in the mouth are called verruciform xanthomas.
- 40% of affected people develop diabetes insipidus, a condition that results in inability to control water loss (resulting in continual thirst and excessive urine production). This is due to histiocyte overgrowth on the lining of the brain (meninges).
- May affect internal organs (such as liver, lungs, kidneys etc.)
- Self-limiting and eventually improves by itself but may persist for many years.
Xanthoma disseminatum is a rare normolipidaemic mucocutaneous xanthomatosis, characterized by proliferation of histiocytic cells and secondary deposition of lipid in the dermis, which can affect people of any age 12. The male to female ratio is 2·4:1. The mucous membranes are also affected in 40–60% of cases, most frequently the upper digestive and respiratory tracts, which can cause hoarseness, dysphagia, or dyspnea. Lower respiratory tract involvement leading to respiratory failure and death has also been reported. The most common form of CNS disease (occurring in about 40% of patients) is pituitary involvement leading to diabetes insipidus, which is often mild or transient and can be well controlled by vasopressin. In contrast to patients with other xanthomatous lesions, those with xanthoma disseminatum are usually normolipidaemic. The differential diagnosis includes Langerhans cell histiocytosis, juvenile xanthogranuloma, papular xanthoma, generalised eruptive histiocytosis, progressive nodular histiocytosis, multicentric reticulohistiocytosis, and eruptive xanthoma.
Treatment of xanthoma disseminatum is challenging. Carbon dioxide (CO2) laser therapy has reportedly shown good results in treatment of cutaneous lesions. Surgical excision of cutaneous and internal lesions does not stop disease progression, and the large extent of system involvement limits its use. Several systemic treatments, including lipid-lowering agents, systemic corticosteroids and immunosuppressants, and chemotherapies have shown mixed or disappointing results. Prognosis is poorly understood, but three clinical patterns have been suggested: a common persistent form, a less common progressive form with systemic involvement, and a rare self-healing form with spontaneous resolution.
Figure 10. Xanthoma disseminatum
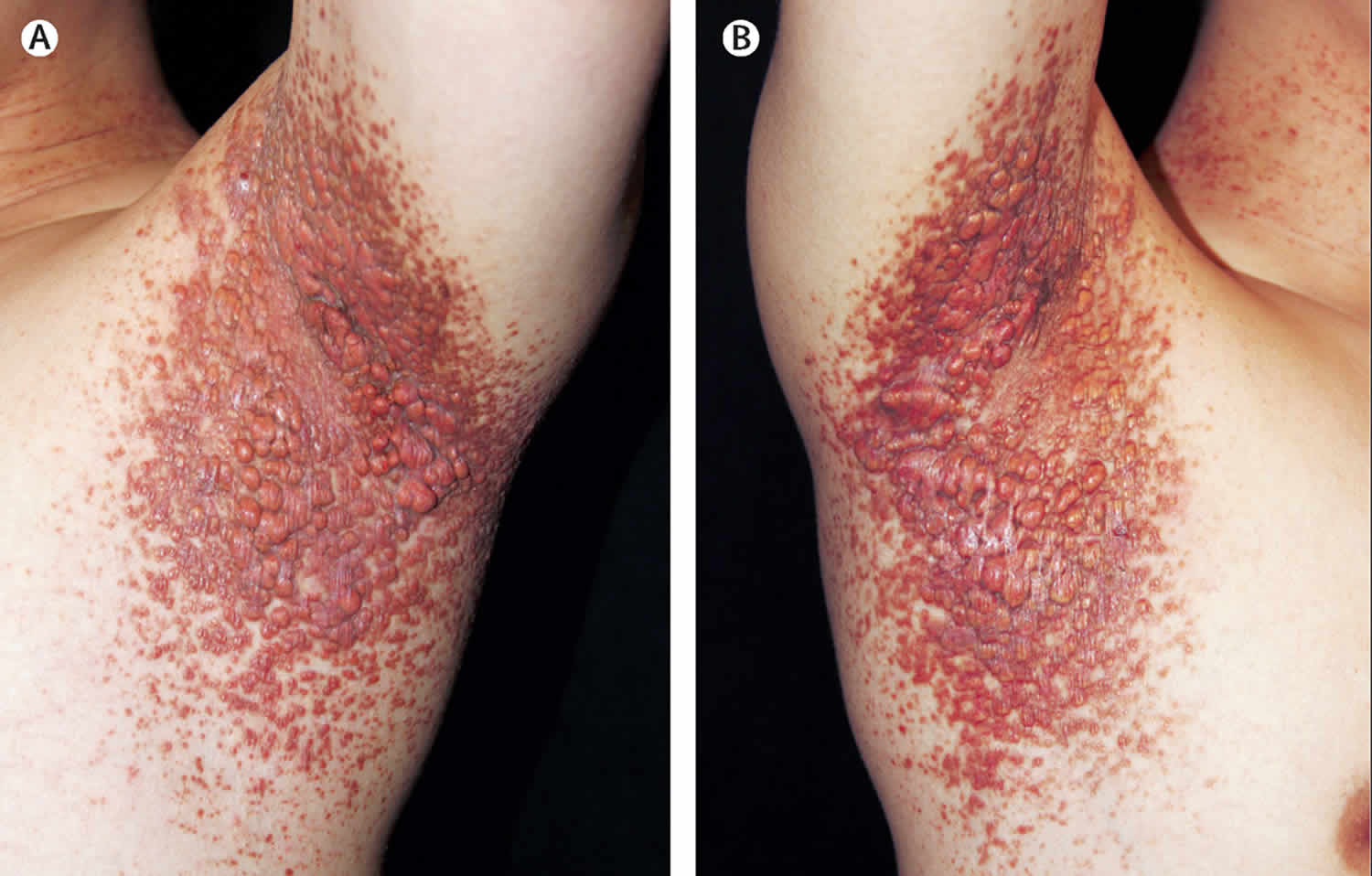
Footnote: (A, B) Hundreds of red to brown papules and nodules distributed symmetrically in the axillae. A 20-year-old man presented to the dermatology department with a 5-year history of multiple brownish-yellow xanthoma-like papules and nodules affecting the face, flexures of the trunk, and limbs, with no systemic symptoms. The lesions had initially appeared as discrete or grouped papules, which then coalesced into plaques and nodules, especially in the axillae, over a period of 2 years. They were painless and asymptomatic, and the patient sought medical help only for cosmetic resions, particularly regarding the lesions on his face. He had no family history of cutaneous disorders. On examination he had numerous papules and nodules scattered over his eyelids, cheeks, oral commissure, neck, axillae (Figure 10), cubital fossae, palms, abdomen, flank, and popliteal fossa. The lesions were discrete and confluent, shiny, and ranged in tone from skin coloured to yellow and brown. The papules were arranged linearly in a few places on the oral commissure and abdomen, suggestive of koebnerisation. The patient’s lesions progressed slowly, with no mucous membrane involvement or diabetes insipidus, over 4 years of follow-up.
[Source 12 ]Xanthoma causes
Xanthomas are common, especially among older adults and people with high blood lipids (fats). Xanthomas vary in size. Some are very small. Others are bigger than 3 inches (7.5 centimeters) in diameter. They appear anywhere on the body. But, they are most often seen on the elbows, joints, tendons, knees, hands, feet, or buttocks.
There are several underlying disorders in which xanthoma is caused by a disturbance in lipid (fat) metabolism. Because lipids are insoluble in water they combine with proteins to form compounds called lipoproteins. Lipoproteins transport lipids and cholesterol in the blood to different parts of the body. Depending on their size and weight, the common lipoproteins are classified as chylomicrons, very-low-density lipoproteins (VLDL), low-density-lipoproteins (LDL), and high-density-lipoproteins (HDL) (Fredrickson classification). They all have a role to play in maintaining metabolic functioning of the body.
Alterations in lipoproteins may be a result of a genetic defect (e.g. primary hyperlipoprotenaemia) or from some underlying systemic disorder such as diabetes mellitus, hypothyroidism, or nephrotic syndrome. These underlying diseases can cause elevated levels of certain lipids and lipoproteins, which then manifest as cutaneous xanthoma.
Monogenic familial hypercholesterolemia: Type 2a
- Mutation in LDL receptor
- High levels of LDL
- Total cholesterol in heterozygotes 9–14 mmol/L
- Total cholesterol in homozygotes 15–30 mmol/L
Polygenic familial hypercholesterolemia: Type 2a
- Mixed genetic and lifestyle causes
- Wide range of results
Polygenic familial combined hyperlipidemia: Type 2b
- Mixed genetic and lifestyle causes
- Raised total cholesterol
- Raised triglyceride
- Low HDL cholesterol
- Increased VLDL cholesterol
- LDL may be normal level but denser and more likely to cause atheroma
Moderate hypertriglyceridemia
- Often also associated with high blood pressure, obesity, diabetes mellitus, high insulin levels, high uric acid levels
- Can be due to alcohol, or medications such as systemic steroids, isotretinoin, acitretin
- Triglycerides 2_10 mmol/L
- Often associated with low HDL cholesterol
Severe hypertriglyceridemia: Type 1 and 5
- Mixed genetic and lifestyle causes
- Diabetes mellitus
- Familial LPL deficiency
- Triglycerides > 10 mmol/L
- Raised total cholesterol
- Raised chylomicrons
- Raised VLDL cholesterol
Broad beta hyperliproteinemia: Type 3
- Rare apo E gene mutation
- Triglycerides 5–20 mmol/L
- Total cholesterol 7–12 mmol/L
The reason for the appearance of xanthoma when the blood fats are normal is not understood at this time.
Xanthoma diagnosis
Your health care provider will examine the skin. Usually, a diagnosis can be made by looking at the xanthoma. If needed, a skin biopsy may be necessary to confirm a clinical diagnosis of xanthoma. Appropriate blood and urine tests and X-rays are performed to determine the cause of disturbed lipoprotein levels if they are present. The risk of cardiovascular disease, including heart attacks, peripheral vascular disease and stroke, is increased with elevated levels of certain lipoproteins. It is essential to identify the contributing factors so that appropriate therapy can be established.
Xanthoma treatment
The main aim of treatment for xanthoma that is associated with an underlying lipid disorder is to identify and treat the lipid disorder. In many cases, treating the underlying disorder will reduce or resolve the xanthoma. In addition, treating hyperlipidaemia will reduce the risk of heart disease, and treating hypertriglyceridaemia will prevent pancreatitis. Dietary and lifestyle modifications with or without medication are used to treat lipid disorders.
Dietary measures should include:
- Prepare most meals from vegetables, salads, cereals and fish
- Minimize saturated fats (found in meat, butter, other dairy produce, coconut oil, palm oil)
- Minimize intake of simple, refined sugars found in fizzy drinks, sweets, biscuits and cakes
- If obese or overweight, aim to slowly reduce weight by reducing caloric intake and increasing exercise.
Very effective medications may also be prescribed. These may include:
- Statins (HMG CoA reductase inhibitors), such as simvastatin and atorvastatin, reduce cholesterol production by the liver, resulting in lower LDL cholesterol levels, increase HDL cholesterol and mildly reduce triglycerides. Treatment should be monitored by regular blood tests to check the lipid levels and ensure liver and muscle enzymes are normal, as statins sometimes cause abnormalities especially when prescribed in higher doses.
- Fibrates, such as bezafibrate, may be added to reduce triglyceride production by the liver, lowering triglycerids and increasing HDL cholesterol. They may cause gastrointestinal side effects.
- Ezetimibe may be added in high risk patients or if higher doses of statins are poorly tolerated. It reduces cholesterol absorption from the gut, lowering total and LDL cholesterol.
- Nicotinic acid lowers cholesterol, LDL cholesterol and triglycerides, and increases HDL cholesterol. At therapeutic doses of at least one gram daily, it causes flushing. An analogue, acipimox, is better tolerated.
- Cholestyramine and colestipol are rarely used as they are not as effective as the medications listed above and they are poorly tolerated.
Surgery or locally destructive modalities can be used to remove xanthomas that do not resolve spontaneously or with treatment of the underlying cause. Xanthoma disseminatum affecting vital organ functions may be treated by chemotherapy drugs or radiotherapy.
Treatments for xanthelasma include:
- Topical trichloroacetic acid
- Electrodesiccation
- Laser vaporisation
- Excision.
- Al Aboud AM, Al Aboud DM. Xanthelasma Palpebrarum. [Updated 2018 Oct 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531501[↩][↩]
- Tuberous Xanthomatosis as a Presentation of Familial Hypercholesterolemia. JSM Clin Case Rep 4(5): 1114. https://www.jscimedcentral.com/CaseReports/casereports-4-1114.php[↩]
- Parker F. Xanthomas and hyperlipidemias. J Am Acad Dermatol 1985;13:1–30.[↩]
- Robson KJ, Piette WW. Cutaneous manifestations of systemic diseases. Med Clin North Am 1998;82:1359–79.[↩]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002;106:3143–421.[↩][↩]
- Eruptive xanthomas in a patient with severe hypertriglyceridemia and type 2 diabetes. Barry Ladizinski, Kachiu C. Lee. CMAJ Dec 2013, 185 (18) 1600; DOI: 10.1503/cmaj.130148 http://www.cmaj.ca/content/185/18/1600[↩]
- Bayer-Garner IB, Smoller BR, Jones RR, et al. The spectrum of cutaneous disease in multiple myeloma. J Am Acad Dermatol. 2003;48(4):497-507.[↩]
- Unknown: Yellow plaques on the chest and arms present for more than 6 years in an 80-year-old male. Dermatology Online Journal 17 (5): 11 https://escholarship.org/content/qt74t0s0kw/inner/article2.html[↩][↩][↩]
- Stockman A, Delanghe J, Geerts ML, Naeyaert JM. Diffuse plane normolipaemic xanthomatosis in a patient with chronic lymphatic leukaemia and monoclonal gammopathy. Dermatology. 2002;204(4):351-354.[↩]
- Malbran A, Parra LS, Casas JG, et al. Case report: diffuse plane xanthoma with low C4 and systemic inflammatory symptoms. Dermatol Online J. 2009;15(4):5.[↩]
- Marcoval J, Moreno A, Bordas X, Gallardo F, Peyri J. Diffuse plane xanthoma: clinicopathologic study of 8 cases. J Am Acad Dermatol. Sep 1998;39(3):439-442.[↩]
- Xanthoma disseminatum. www.thelancet.com Vol 391, January 20, 2018 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)31934-7/fulltext[↩][↩]





{kind=link}