Contents
- Yolk sac carcinoma
Yolk sac carcinoma
Yolk sac carcinoma also known as malignant yolk-sac tumors or endodermal sinus tumors, is a rare aggressive malignant cancer that forms in the germ cells (cells that form sperm or eggs) that line the yolk sac of the embryo 1, 2, 3, 4, 5. Germ cells (cells that form sperm or eggs) normally develop into ovaries or testes. Yolk sac carcinoma occur most often in the ovary or testicle forming testicular and ovarian cancer 6. Sometimes, yolk sac carcinoma form in places outside of your reproductive system (extragonadal germ cell tumors), like your brain, chest and abdomen 7, 8. It has also been reported that yolk sac tumor occurred in penile shaft, urachus, stomach, liver, lungs, heart, thyroid, nasal region, cranial base, vulva, retroperitoneum, prostate, pericardium, diaphragm, mesentery, mouth, ears, omentum, eyes, and subcutaneous region 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22.
Extragonadal germ-cell tumors represent only 1% to 5% of all germ-cell tumors, making them relatively uncommon 23. Yolk sac carcinomas are most common in children before the ages of 1 to 2, which account for about 3.5% of all childhood cancers, but can occur at any age 24. They tend to grow quickly and spread to other parts of the body, such as the lung, liver, lymph nodes, and brain, if not treated 25, 26. They’re potentially fatal without treatment. Treatment for these highly aggressive tumors usually involves surgery and chemotherapy. Radiation therapy can play a supportive role in managing specific clinical scenarios to control disease progression and improve patient outcomes. The decision to use radiotherapy is typically made on a case-by-case basis, taking into consideration factors such as the location and extent of the tumor, the patient’s overall health, and response to the initial treatment 27. With the introduction of new chemotherapeutic regimens in the end of 1970s, the 5-year survival rates of yolk sac tumor significantly improved from 14% to nearly 90% 28. Adding cisplatin to combination therapies, prognosis of the patients reached excellent values, even for patients with advanced stages 29.
Childhood and adolescent cancer survivors require close monitoring because late effects of cancer therapy may persist or develop months or years after treatment.
Yolk sac tumor diagnosis involves a physical examination to check for signs of the tumor, like unusual lumps or swelling in your abdomen or testicles. Your doctor will also ask about your symptoms. However, yolk sac carcinoma present significant diagnostic and therapeutic challenges due to their diverse signs and symptoms and aggressive growth. Yolk sac carcinoma cells secrete specific hormones, two of which are alpha-fetoprotein (AFP) and human chorionic gonadotropin (beta-hCG). A blood test which shows an increase in alpha-fetoprotein (AFP) and human chorionic gonadotropin (beta-hCG) hormones can help with the diagnosis. Your doctor may also check for an elevated lactate dehydrogenase (LDH). Other studies may include an ultrasound, CT scan, or MRI. A biopsy will be needed for final diagnosis. The biopsy, surgical removal of part of the mass is done in surgery under general anesthesia so the child is not conscious and will not feel any pain.
Germ cell tumors can also be diagnosed in utero. Sacrococcygeal teratomas are the most common germ cell tumor of childhood and the most frequently recognized neoplasm of the fetus. Approximately 25–50% of sacrococcygeal teratomas are diagnosed in utero before birth (i.e., true congenital neoplasms) during routine ultrasonographic surveillance 30, 31. In utero diagnosis of sacrococcygeal teratoma warrants vigilant fetal monitoring because of the higher risks of polyhydroamniosis, fetal hydrops, or placentomegaly, which may lead to premature delivery or fetal demise. The diagnosis of sacrococcygeal teratoma prior to a gestational age of 30 weeks is especially hazardous 32.
Figure 1. Extracranial germ cell tumors
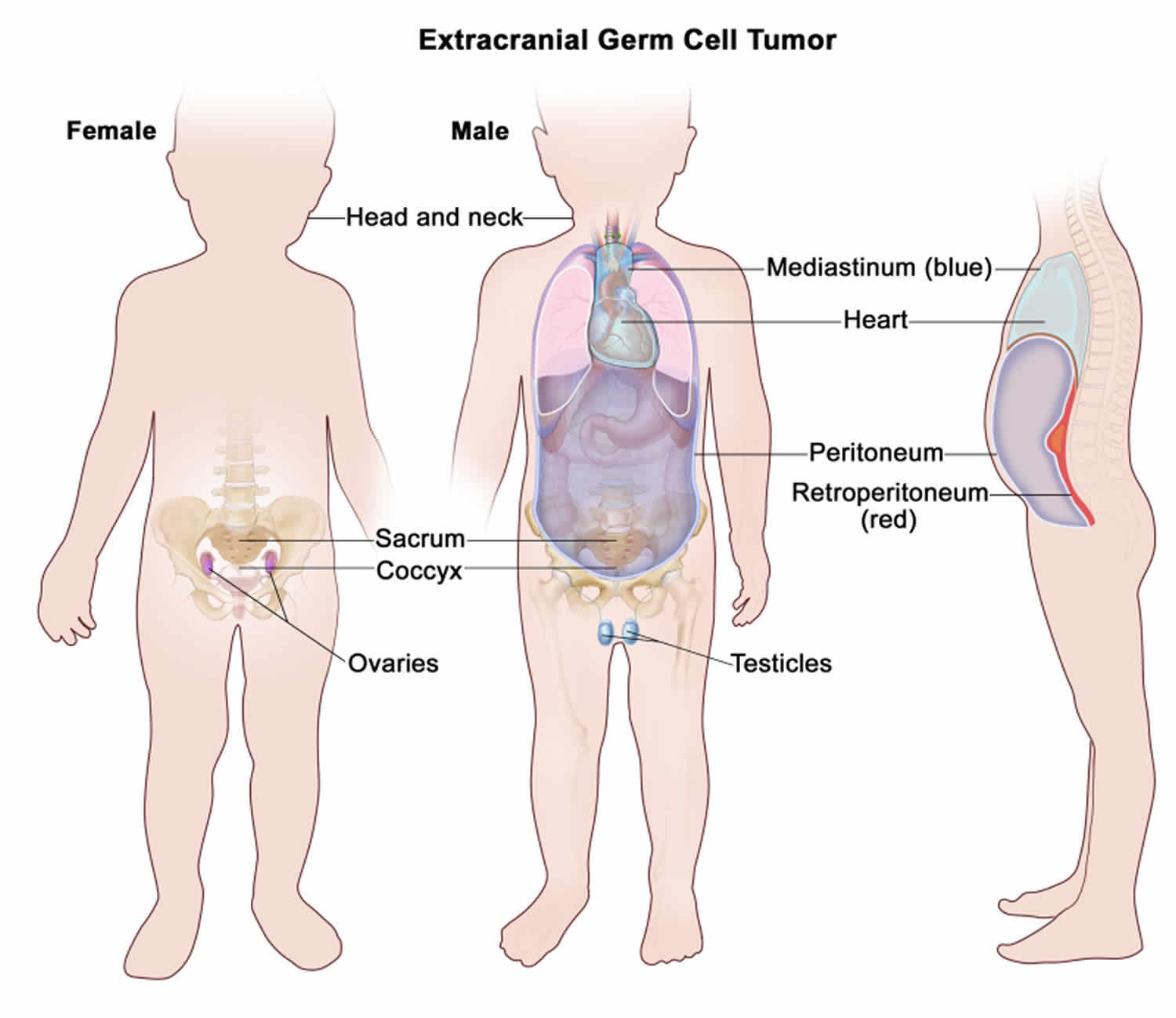
Footnotes: Extracranial germ cell tumors form in parts of the body other than the brain. This includes the testicles, ovaries, sacrococcyx (usually originating from the coccyx and including the sacrum), mediastinum, and retroperitoneum.
[Source 33 ]Figure 2. Yolk sac tumor
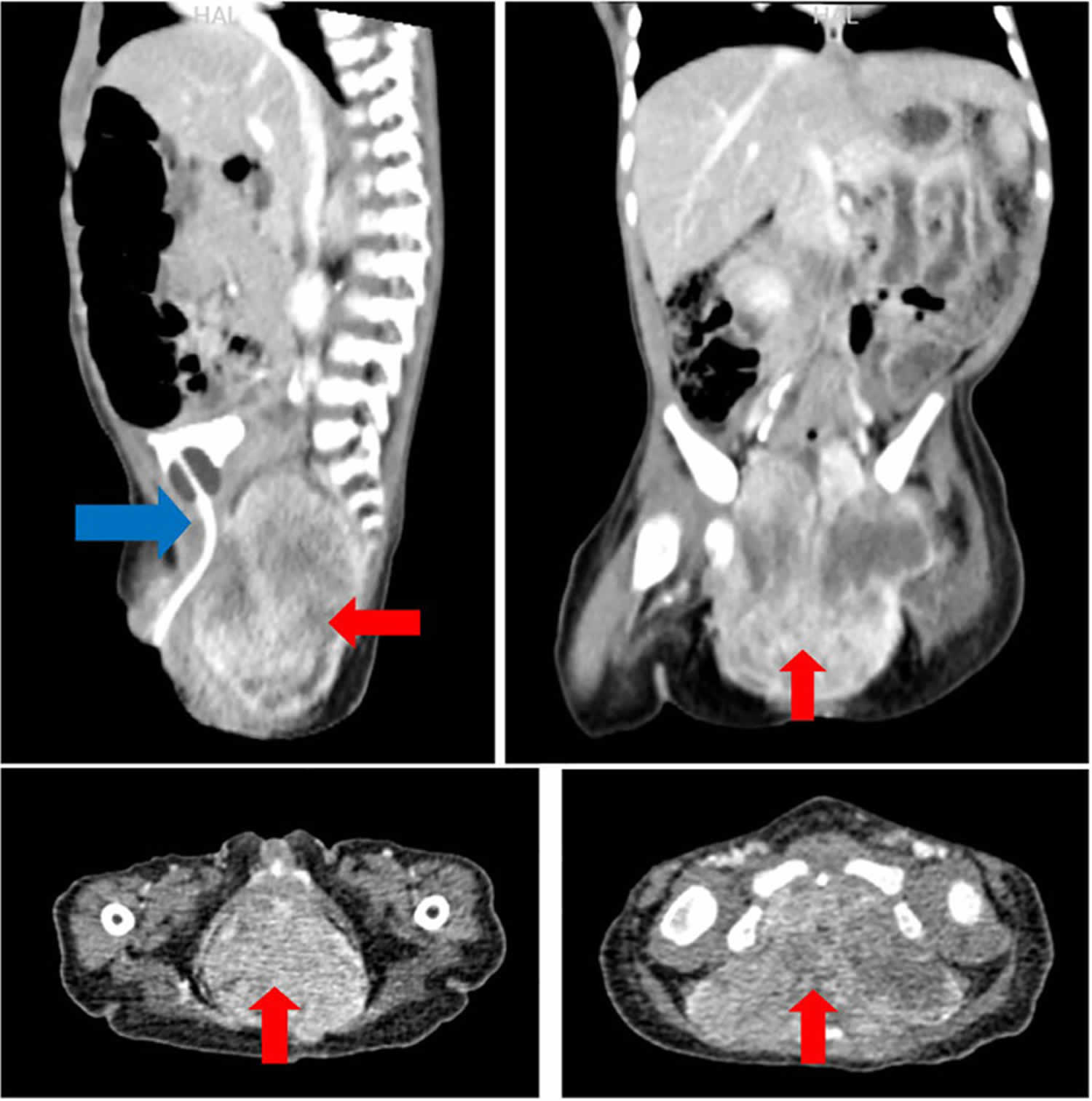
Footnotes: An 8-month-old female was referred with a 3-week history of progressively worsening abdominal distension and an inability to pass urine. CT-scan chest-abdomen-pelvis showed a large heterogeneous enhancing mass (7.6 × 5.3 × 8.4 cm in size) (red) within the pelvis, arising from the sacrococcygeal region, pushing the urinary bladder, rectum and large bowels anteriorly (blue). She then had an elective wide local excision. Histopathological examination displayed malignant primitive germ cell tumor composed of loose mesh-work of anastomosing channels or cysts lined by primitive cells with abundant clear to eosinophilic cytoplasm. These features were suggestive of malignant yolk sac tumor (see Figure 3 below).
[Source 2 ]Figure 3. Yolk sac carcinoma histopathology
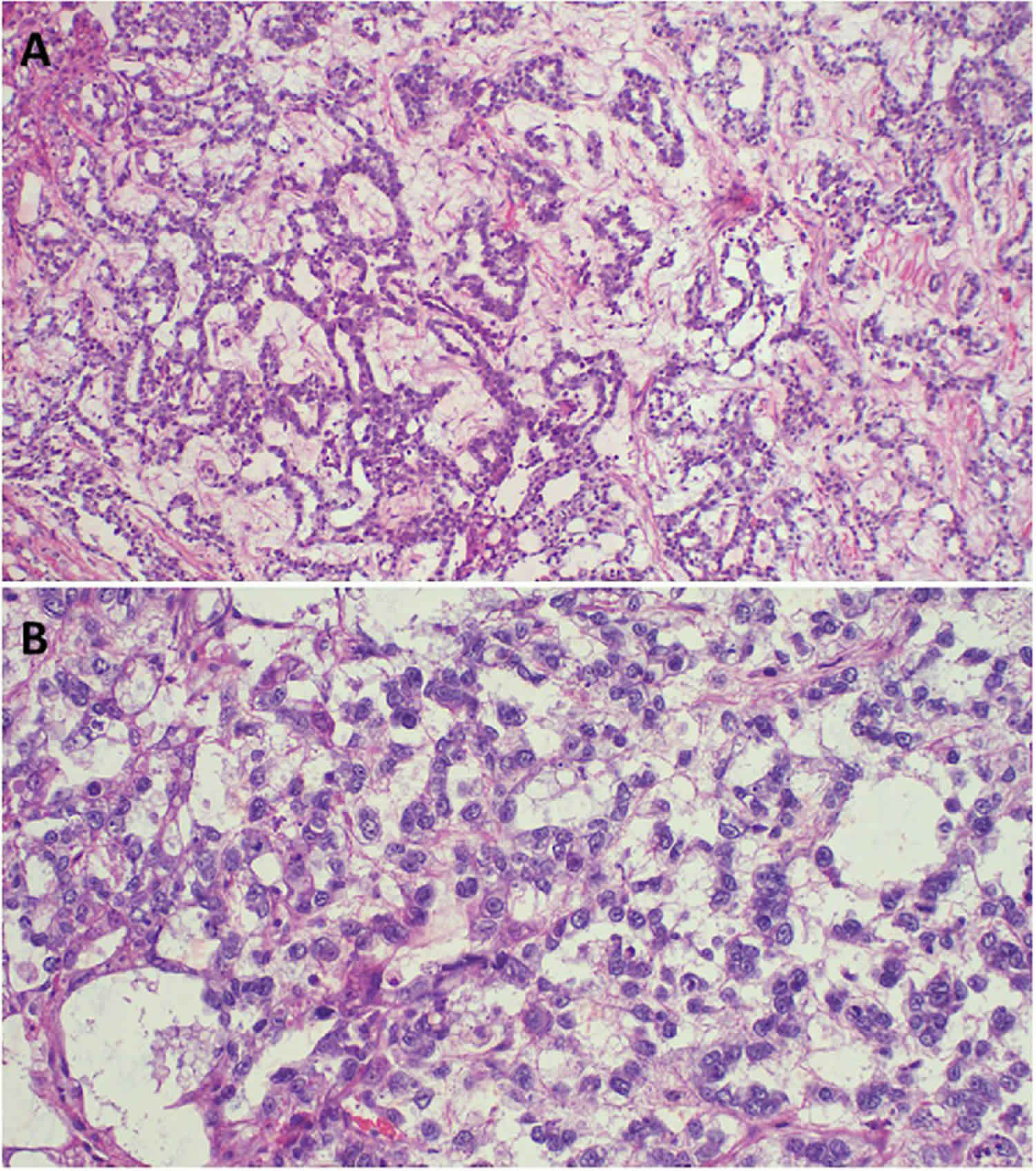
Footnotes: (A) Microscopic image of Yolk sac carcinoma demonstrating loose meshwork of anastomosing channels and variably sized cysts (macro or microcysts) lined by primitive tumor cells with varying amounts of clear to eosinophilic cytoplasm; H&E staining 10 x original magnification. (B) Histopathology of Germ cell carcinoma displaying infiltrative tumor with Microscopic image of Yolk sac carcinoma demonstrating loose meshwork of anastomosing channels and variably sized cysts (macro or microcysts) lined by primitive tumor cells with varying amounts of clear to eosinophilic cytoplasm; H&E staining 20 x original magnification.
[Source 2 ]What are germ cell tumors?
Germ cell tumors develop in germ cells. Germ cells are reproductive cells in your body that develop into sperm inside testicles in males and into eggs inside ovaries in females. Germ cell tumors most often develop in the ovary or testicle (reproductive organs) because this is where most germ cells are. However, germ cell tumors can also occur in other places within your body where there are germ cells, including:
- Abdomen called retroperitoneal tumor
- Pelvis
- Central chest area (mediastinum) called mediastinal tumor
- Brain called pineal region tumor
- Lower back/tailbone area (sacrococcygeal) called sacrococcygeal tumor
Germ cell tumors that grow outside the ovary or testicle are very rare. Doctors call them extragonadal germ cell tumors (EGCTs). Extragonadal germ cell tumors form from developing sperm or egg cells that travel from the gonads to other parts of your body. Extragonadal germ cell tumors (EGCTs) represent 1–5% of all germ cell tumors and are usually seen in children or young male adults 34, 7.
“Extragonadal” means outside of the gonads (sex organs). When germ cells that are meant to form sperm in the testicles or eggs in the ovaries travel to other parts of the body, they may grow into extragonadal germ cell tumors. These tumors may begin to grow anywhere in the body but usually begin in organs such as the pineal gland in your brain, in the mediastinum (area between the lungs), or in the retroperitoneum (the back wall of the abdomen).
Germ cell tumors can be malignant (fast-growing and have a tendency to spread) or benign (slow-growing and do not spread).
- Benign germ cell tumors include benign teratomas or mature teratomas. These are more common than malignant extragonadal germ cell tumors and often are very large.
- Malignant germ cell tumors are split into 2 main groups:
- Seminoma germ cell tumors in males (in females these are called dysgerminomas)
- Non-seminoma germ cell tumors in males (in females these are called non dysgerminomas). Nonseminomas tend to grow and spread more quickly than seminomas. They usually are large and cause signs and symptoms. If untreated, malignant extragonadal germ cell tumors may spread to the lungs, lymph nodes, bones, liver, or other parts of the body.
- Malignant nonseminoma tumors include:
- immature teratomas
- yolk sac tumors
- choriocarcinomas
- embryonal carcinomas
- Malignant nonseminoma tumors include:
Some nonseminomas develop from just one type of cell. And some develop from a mixture of cell types. So, for example, a tumor can contain a mix of some teratoma cells and some embryonal carcinoma cells.
Seminomas are sometimes called pure seminomas. They only contain one type of cell. Some germ cell tumor contain both seminoma cells and non-seminoma cells. Doctors usually class and treat these as non-seminoma tumors.
Doctors use different names to describe the different types of germ cell tumors. The name describes:
- whereabouts in the body it started – such as ovarian or testicular
- what the tumor looks like under the microscope
The main treatments are surgery and chemotherapy. Your treatment depends on your type of germ cell tumor and whereabouts it is in your body.
What are yolk sac tumors?
Yolk sac tumors also known as primitive endodermal tumors or endodermal sinus tumors are primitive germ cell cancers. They are histologically similar to the mesenchyme of the primitive yolk sac 35, 36
Types of yolk sac tumors include:
- Testicular yolk sac tumors. A form of testicular cancer, these tumors are most common in children under 3 and people in their 20s and 30s. Testicular yolk sac tumors are usually diagnosed before they spread, while they’re curable.
- Ovarian yolk sac tumors. This aggressive form of ovarian cancer is most common in people 20 years old or younger. One-third of diagnoses involve children too young to have gotten their periods.
Like other types of germ cell tumors, yolk sac tumors sometimes form in places outside of your reproductive organs, in places like your brain, chest, abdomen or tailbone. These are called extragonadal germ cell tumors.
Yolk Sac Tumors in Males
Yolk sac tumors of the testis have a bimodal age distribution, young children under the age of 3 and post-pubertal adults 37.
In children, the yolk sac tumor is the most common testicular tumor. It makes up about 30% of the germ cell tumors in this age group, with a median age of diagnosis at 18 months. Usually, children have pure yolk sac tumors, and their prognosis is good. In adults, yolk sac tumors typically present mixed germ cell tumors and present in the second to third decades of life 38, 39.
Yolk Sac Tumors in Females
Yolk sac tumors are uncommon tumors in the ovary, and they account for 15% of all ovarian germ cell tumors; they present in early life and rarely after the age of 40. The median age of diagnosis is 19 years, and 40% of patients are diagnosed in the prepubertal period. About 60% of ovarian yolk sac tumors present in a pure form, while 40% present with mixed germ cell tumors 40.
Yolk sac carcinoma causes
Scientists don’t know what causes yolk sac tumors 41. Like all cancers, yolk sac tumors form when changes to the genes in cell DNA (mutations) cause cells to multiply too fast. But experts are still researching what starts this process in the first place. Some studies suggest that RUNX3 gene hypermethylation and GATA-4 overexpression may be involved in the pathogenesis of yolk sac tumors 42, 43.
Yolk sac carcinoma signs and symptoms
Yolk sac carcinoma signs and symptoms depend on the location of the cancer and may include:
- A firm, painless lump in a testicle
- Swelling in your abdomen or a mass (ovaries)
- Abdominal pain or back pain (ovaries)
- Changes in your bowel habits (ovaries)
- Irregular periods, including heavy period bleeding (ovaries)
- Headaches or vision issues (brain)
- Cough and shortness of breath (chest)
- A swollen area resembling a bruise or infected bump (in your tailbone)
Within the testes, the tumor is a visible, painless, firm swelling or may lead to precocious puberty. Children with testicular yolk sac tumors are generally present with testicular masses; the mass is painless and solid. Metastasis is not common in the presentation of the disease. It occurs in less than one-tenth of cases. In adults, testicular yolk sac tumors are mixed with other germ cell components such as embryonal carcinoma, choriocarcinoma, teratoma, and seminoma 44.
In the ovary it is not as visible and the tumor may grow very large before being noticed; this tumor is described by very rapid growth and the duration of the symptoms in most of the patients is seven days or less 45. This can lead to abdominal pain, abdominal swelling. Other symptoms can lead to abnormal vaginal bleeding or precocious puberty. Most patients with ovarian yolk sac tumors have symptoms of abdominal distention and sudden onset of pain at presentation. A pelvic mass may be palpable on examination of the patient. Metastasis develops quickly in ovarian yolk sac tumors and invades the structures around the ovaries. Metastasis can also spread through the lymph nodes 46.
In the sacrococcygeal area, it may be seen as a swelling of the buttocks often mistaken for a bruise or infection.
Tumors in the chest can present with chest pain, cough or shortness of breath.
In adults, most common sites of primary extragonadal germ cell tumors (EGCTs) are, in descending order, the mediastinum (15%), retroperitoneum (10% of all primary malignant retroperitoneal tumors), and cranium. In children, the skull and sacrococcygeal region are common sites 47. Abdominal and low back pain are the most frequent symptoms, as pain can simulate a kidney stone. Other clinical symptoms and signs include a palpable mass, weight loss, constipation, hip and back pain, shortness of breath, leg swelling, fever, varicocele (veins in the scrotum become enlarged and twisted), and urinary retention 48, 49.
Malignant yolk sac tumors may cause signs and symptoms as they grow into nearby areas. Other conditions may cause the same signs and symptoms. Check with your doctor if you have any of the following:
- Chest pain.
- Breathing problems.
- Cough.
- Fever.
- Headache.
- Change in bowel habits.
- Fatigue
- Upset stomach (dyspepsia)
- Back pain
- Pain during sex (dyspareunia)
- Constipation
- Changes in the period, such as more massive bleeding (menorrhagia) or irregular bleeding (metrorrhagia)
- Abdominal swelling with weight loss
- Feeling very tired.
- Trouble walking.
- Trouble in seeing or moving the eyes.
Yolk sac carcinoma complications
The complications of the yolk sac tumors can be related to the tumor itself or the treatment. Tumor mass effect complications depend on the location and the size of the mass; another tumor complication is metastasis; even if cancer has spread to other parts of the body, many patients might not have symptoms until very late stages. Treatment complications include chemotherapy side effects, operative complications, and postoperative complications.
Yolk sac carcinoma diagnosis
Doctors use the following tests and procedures to diagnose yolk sac tumors.
Physical exam and health history
An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. The testicles may be checked for lumps, swelling, or pain. A history of the patient’s health habits and past illnesses and treatments will also be taken.
Chest x-ray
An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
CT scan (CAT scan)
A CT scan is also called computed tomography, computerized tomography, or computerized axial tomography, is a noninvasive imaging procedure that uses X-rays to create detailed pictures of the inside of your body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly.
Sometimes a CT scan and a PET scan are done at the same time. A PET scan is a procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. When a PET scan and CT scan are done at the same time, it is called a PET-CT.
Serum tumor marker test
A procedure in which a sample of blood is examined to measure the amounts of certain substances released into the blood by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the blood. These are called tumor markers. The following three tumor markers are used to detect extragonadal germ cell tumor:
- Alpha-fetoprotein (AFP). Alpha-fetoprotein (AFP) is specific in the yolk sac tumor, but it is not sensitive (overall sensitivity as low as 60%) because it can be seen in other cancers like liver cancer (hepatocellular carcinoma) 50.
- Beta-human chorionic gonadotropin (beta-hCG).
- Lactate dehydrogenase (LDH).
Yolk sac carcinoma cells secrete specific hormones, two of which are alpha-fetoprotein (AFP) and human chorionic gonadotropin (beta-hCG). A blood test which shows an increase in alpha-fetoprotein (AFP) and human chorionic gonadotropin (HCG) hormones can help with the diagnosis. Your doctor may also check for an elevated lactate dehydrogenase (LDH). Other studies may include an ultrasound, CT scan, or MRI. A biopsy will be needed for final diagnosis. The biopsy, surgical removal of part of the mass is done in surgery under general anesthesia so the child is not conscious and will not feel any pain.
Biopsy
In a biopsy, a small piece of tissue is taken out of the body and tested for cancer cells. The removal of cells or tissues can be viewed under a microscope by a pathologist to check for signs of cancer. The type of biopsy used depends on where the tumor is found.
- Excisional biopsy: The removal of an entire lump of tissue.
- Incisional biopsy: The removal of part of a lump or sample of tissue.
- Core biopsy: The removal of tissue using a wide needle.
- Fine-needle aspiration (FNA) biopsy: The removal of tissue or fluid using a thin needle.
Histopathology
On gross examination, yolk sac tumors are soft, solid masses, and tan to yellow or grey with a mucoid appearance; notable necrosis, cystic changes, and hemorrhages are commonly present 51.
On microscopic examination, the tumors consist of primitive tumor cells and have many histological types, including microcystic/reticular, papillary, solid, festoon, poly vesicular-vitelline, glandular, intestinal, endometroid, parietal, tubular, and hepatoid. The reticular microcystic pattern is the most common type formed by vacuolated cytoplasm of tumor cells; it appears like a honeycomb under a microscope 52.
Schiller-Duval body is pathognomonic for yolk sac tumors, and it appears like a glomerulus in structure with a fibrovascular core. However, Schiller-Duvall bodies are usually present only in two to three-quarters of yolk sac tumors and are only seen in papillary type 53.
Immunohistochemical staining can support the diagnosis of yolk sac tumors because almost all cases stain positive for alpha-fetoprotein (AFP) 50.
In mixed germ cell tumors with small foci of the yolk sac tumors, the biopsy findings may be negative for yolk sac tumors because yolk sac tumors are usually limited to small malignant foci within a larger tumor, staining positive for alpha-fetoprotein (AFP) will confirm the presence of yolk sac tumors within other germ cell tumors, (e.g., in teratoma the biopsy of cancer may reveal teratoma alone, whereas elevated AFP reveals that yolk sac tumor is also present) 43.
When yolk sac tumor arises in a small focus only, it may be hard to detect alpha-fetoprotein (AFP) in immunohistochemical staining because staining for alpha-fetoprotein is unequable and often varies throughout the tissue; strong staining is not seen in every tumor; in this situation, yolk sac tumors may be marked with cytokeratin or glypican-3, cytokeratin is present in almost all cases, another immunostaining which is frequently positive in yolk sac tumors is placental alkaline phosphatase (ALP) 54, 55.
Yolk sac carcinoma staging
After the tumor type has been diagnosed, tests are done to find out if cancer cells have spread to other parts of the body. The extent or spread of cancer is usually described as stages. Doctors stage yolk sac tumors to determine how advanced the cancer is and find the best treatment options. Using information like tumor size and the extent of cancer spread, they assign a number or “stage.” Lower numbers mean that cancer is in the early stages. Higher numbers mean more advanced cancer. Staging systems are essential to decide the next step in the management of any patient because each stage has a unique treatment plan.
There are three ways that cancer spreads in the body. Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of tumor as the primary tumor. For example, if an extragonadal germ cell tumor spreads to the lung, the tumor cells in the lung are actually cancerous germ cells. The disease is metastatic extragonadal germ cell tumor, not lung cancer.
Testicular yolk sac tumors range from stages 1 to 3:
- Stage 1: The cancer is only in your testicle.
- Stage 2: Cancer has spread to your lymph nodes.
- Stage 3: Cancer cells have spread to other organs.
Ovarian yolk sac tumors range from stages 1 to 4:
- Stage 1: The cancer hasn’t spread beyond one or both ovaries.
- Stage 2: Cancer cells have spread below your pelvis, but they’re not in your lymph nodes.
- Stage 3: The cancer has spread to your lymph nodes and the layer of tissue lining your abdomen (peritoneum) that’s outside your pelvis.
- Stage 4: Cancer has spread to tissues and organs other than your peritoneum.
However, for extragonadal germ cell tumors, prognostic groups are used instead of stages. The tumors are grouped according to how well the cancer is expected to respond to treatment. It is important to know the prognostic group in order to plan treatment.
The following prognostic groups are used for extragonadal germ cell tumors 56:
Good prognosis
A nonseminoma extragonadal germ cell tumor is in the good prognosis group if:
- the tumor is in the back of the abdomen; and
- the tumor has not spread to organs other than the lungs; and
- the levels of tumor markers AFP and beta-hCG are normal and LDH is slightly above normal.
A seminoma extragonadal germ cell tumor is in the good prognosis group if:
- the tumor has not spread to organs other than the lungs; and
- the level of AFP is normal; beta-hCG and LDH may be at any level.
Intermediate prognosis
A nonseminoma extragonadal germ cell tumor is in the intermediate prognosis group if:
- the tumor is in the back of the abdomen; and
- the tumor has not spread to organs other than the lungs; and
- the level of any one of the tumor markers (AFP, beta-hCG, or LDH) is more than slightly above normal.
A seminoma extragonadal germ cell tumor is in the intermediate prognosis group if:
- the tumor has spread to organs other than the lungs; and
- the level of AFP is normal; beta-hCG and LDH may be at any level.
Poor prognosis
A nonseminoma extragonadal germ cell tumor is in the poor prognosis group if:
- the tumor is in the chest; or
- the tumor has spread to organs other than the lungs; or
- the level of any one of the tumor markers (AFP, beta-hCG, or LDH) is high.
Seminoma extragonadal germ cell tumor does not have a poor prognosis group.
Testicular tumors staging
Stage 0 is the earliest stage of testicular cancer it is also known as neoplasia in situ. Stage 4 is not applicable to testicular cancer.
The TNM system is the most popular system for staging testicular cancer, and the system is based on four elements:
- Tumor (T): size and location of the tumor.
- Node (N): lymph node involvement.
- Metastasis (M): number and site of spread of the tumor.
- Serum tumor marker (S): Are the serum tumor markers AFP, beta-hCG, and LDH elevated? If so, how high are they?
Stage 1
There is no evidence of metastasis or lymph node involvement. It is divided into 1A and 1B depending on the tumor size and 1S when tumor markers are elevated.
Stage 2
The cancer cells have spread to the lymph nodes, but there is no metastasis to other body parts. It is divided into 2A, 2B, and 2C depending on the number and size of lymph nodes involved.
Stage 3
The cancer has metastasized to other organs, and this stage is divided into 3A, 3B, and 3C depending on metastasis location and level of tumor markers.
Ovarian Cancer staging
The FIGO (International Federation of Gynecology and Obstetrics) system and the AJCC (American Joint Committee on Cancer) TNM staging system are the same, and they are the most used systems for staging ovarian cancers.
Both of the FIGO (International Federation of Gynecology and Obstetrics) system and the AJCC (American Joint Committee on Cancer) systems contain three elements:
- Tumor (T): size and location of the tumor.
- Node (N): lymph node involvement.
- Metastasis (M): number and site of spread of the tumor.
Stage 1
The cancer is only in the ovary (IA) or both ovaries (IB).
Stage 2
The cancer has spread to the pelvis (below pelvic brim) without lymph node involvement, and this stage is divided into 2A (spread to the uterus or the fallopian tubes) and 2B (other pelvic tissues).
Stage 3
The cancer has spread to the lymph nodes and/or peritoneum outside the pelvis, and this stage is divided into 3A, 3B, and 3C, depending on metastasis location and size.
Stage 4
The cancer has spread to other tissues (distant metastasis excluding peritoneal metastasis), and this stage is divided into stages 4A (pleural effusion) and 4B (extra-abdominal metastasis).
Yolk sac carcinoma treatment
The present-day treatment for yolk sac tumors is surgery and chemotherapy. Treatment with cisplatin, etoposide, and bleomycin has shown a good response in most patients 57, 58. Furthermore, yolk sac tumor spreads through the blood route in >50% of the children patients in comparison with only 4–6% of the adult patients 59. This fact modifies the therapeutic strategy. Therefore, Retroperitoneal Lymph Node Dissection (RPLND) would not be the appropriate treatment for children patients and complications such as wound infection, atelectasis, pulmonary insufficiency secondary to bleomycin-induced interstitial fibrosis, chylous ascities, small bowel obstruction, and subsequently ejaculatory dysfunction could occur 60.
The general treatment for yolk sac tumor is surgery to remove the primary tumor including all traces of the yolk sac tumor 61. This typically means removing the entire affected testicle (orchiectomy) or ovary (oophorectomy). Your surgeon may also remove lymph nodes if the cancer has spread there.
Chemotherapy treatment (chemo) usually follows. This treatment uses chemotherapy drugs to kill any cancer cells that may remain. If a yolk sac tumor is so large that surgery may pose risks, you may need chemotherapy before surgery to shrink the tumor.
The treatment regimen of testicular yolk sac tumors depends on the stage of cancer and age of the patient at the presentation; most children with yolk sac tumors present with stage 1 disease. Orchiectomy and chemotherapy +/- dissection of retroperitoneal lymph nodes with the careful post-orchiectomy measuring of serum AFP values is indicated in most cases. Most pediatric patients with metastasis or recurrence can be treated with a chemotherapy regimen successfully 62.
Ovarian yolk sac tumors, specifically in post-menopausal patients, need more intensive treatment, and surgical resection of cancer with chemotherapy is indicated in the early stages of the disease 63.
In patients with yolk sac tumors of the ovary, fertility-sparing surgery with a postoperative Cisplatin-based combination chemotherapy should be the selected mode of treatment 28, 64. The treatment of ovarian germ cell tumors in the advanced stage generally involves debulking surgery of tumors followed by adjuvant chemotherapy 65. Several studies support the regimen of BEP (bleomycin, etoposide and platinum) for primary treatment of the ovarian germ cell tumor patients 66. They demonstrated a significantly high 5-year survival rate of 94%, even for the patients with residual cancers 67, 68, 69. The national comprehensive cancer network recommends 3–4 BEP cycles after surgical resection 66. Furthermore, it was reported that platinum-based chemotherapy should be used for the more malignant tumors such as endodermal sinus tumor and mixed germ cell tumor 70, 71. Neoadjuvant chemotherapy (a type of cancer treatment that involves administering chemotherapy drugs before surgery) could be considered for the patients having extensive intra-abdominal disorders when initial surgical debulking is not preferred 72. Chemotherapy is suggested for treating recurrence 60. Bleomycin, etoposide and platinum (BEP) chemotherapy is considered as a gold-standard first-line treatment for germ cell tumors at all stages 73. Adding cisplatin to combination therapies, prognosis of the patients reached excellent values, even for patients with advanced stages 29.
Rudaitis et al. 72 applied neoadjuvant chemotherapy (a type of cancer treatment that involves administering chemotherapy drugs before surgery) of four BEP cycles to decrease the tumor size in order to minimize the extent of surgery and thus the impact on the patient’s fertility. In spite of the risks of damaging the reproductive function of female patients involved in chemotherapy, previous investigations have revealed that most of the women could recover their normal menstrual and reproductive functions post treatment 74, 75.
Follow-up After Treatment
After treatment, follow-ups are required such as abdominal and pelvic examination, CT, chest X-ray and AFP levels 76.
- AFP and beta-hCG. Monitor AFP and beta-hCG levels monthly for 6 months (period of highest risk) and then every 3 months, for a total of 2 years (3 years for sacrococcygeal teratoma).
A COG trial of patients with low-risk and intermediate-risk germ cell tumors reported the following results 77:- Forty-eight patients with elevated tumor markers at diagnosis relapsed during the surveillance phase.
- At the time of relapse (after central review), 47 of 48 (98%) relapses were detected by tumor marker elevation.
- Imaging tests.
- MRI/CT may be performed at the completion of therapy. When tumor markers are normal at diagnosis, ultrasonography or CT/MRI may be performed every 3 months for 2 years and then annually for 5 years for germinomas.
- Guided imaging of the primary site may be performed every 3 months for the first year and every six months for the second year. Seminomas and dysgerminomas may recur later, so the imaging schedule may need to be extended.
- Chest x-ray annually.
Testicular Yolk Sac Tumors Treatment by Stage
Stage 1
Stage 1 disease can be cured in almost all cases, and radical inguinal orchiectomy is performed in all patients.
Choices for Stage 1A
- Careful observation (surveillance): this management includes visits every two months during the first year, with computed tomography scans (CT scans) every four to six months. Then, in the second year, the appointments will be every three months, with computed tomography scans (CT scans) every six to twelve months. If cancer relapses, chemotherapy is indicated to treat the patient.
- Nerve-sparing retroperitoneal lymph node dissection (RPLND)
- Chemotherapy: giving the BEP regimen (bleomycin, etoposide, and cisplatin) for one cycle. Chemotherapy decreases the rate of relapse.
Stage 1S
- Chemotherapy with three cycles of BEP or four cycles of EP (etoposide and cisplatin) is indicated if the alpha-fetoprotein is still elevated after the surgery with no evidence of mass on CT scan.
Stage 2
Surgery must be done first for all the cases.
Stage 2A
Tumor marker values after performing the surgery and the involvement of the retroperitoneal lymph nodes will decide the next step of management in those patients.
Normal tumor marker levels:
- Retroperitoneal lymph node dissection (RPLND): If the lymph nodes contain cancer, then give two cycles of chemotherapy (BEP or EP). If no lymph nodes are involved, watch and monitor closely for signs of relapse.
- Chemotherapy: 4 cycles of EP (etoposide and cisplatin) or three cycles of BEP (bleomycin, etoposide, and cisplatin).
High tumor markers after the surgery should be treated using chemotherapy (EP or BEP). The number of cycles is determined after the risk stratification (good, intermediate, or poor).
Stage 2B
Normal tumor marker levels:
- Chemotherapy: Four cycles of EP or three cycles of BEP should be given to treat the patients.
- Retroperitoneal lymph node dissection (RPLND)
High tumor markers after the surgery should be treated using chemotherapy (EP or BEP). The number of cycles is determined by the risk stratification (good, intermediate, or poor).
Stage 3
Patients with stage 3 disease should be treated with radical inguinal orchiectomy, followed by 3 to 4 cycles of the following chemotherapy regimens:
- EP 4 cycles
- BEP 3 or 4 cycles
- VIP (etoposide, ifosfamide, and cisplatin) 4 cycles
High-dose chemotherapy and bone marrow transplant might be indicated in cancer resistance to usual dose chemotherapy.
Ovarian Yolk Sac Tumors Treatment
Usually, treating ovarian cancer is the same for all stages and types. Surgery should be performed, and a chemotherapy regimen must be given after the surgery.
- Surgery: deciding between radical surgery or conservative surgery depends on the patient’s wish to have more children and the involvement of one side or both sides of the ovaries. Debulking surgery is indicated in patients with cancer metastasis to other organs.
- Chemotherapy: most patients will need at least three cycles of chemotherapy. The BEP regimen is the best choice. Reduction in tumor marker levels after chemotherapy is an indication of an excellent response to chemotherapy.
Yolk sac carcinoma prognosis
Without any treatment, yolk sac tumors can be very dangerous and lead to death. This is why early diagnosis and treatment are so important. As with most cancers, the earlier you get treatment, the better your prognosis (outcome).
Yolk sac tumor was universally life-threatening before the development of combination chemotherapy. With the introduction of new chemotherapeutic regimens in the end of 1970s, the 5-year survival rates of yolk sac tumor significantly improved from 14% to nearly 90% 28, 78. Adding cisplatin to combination therapies, prognosis of the patients reached excellent values, even for patients with advanced stages 29.
To better identify prognostic factors, data from five U.S. trials and two U.K. trials for malignant extracranial germ cell tumors in children and adolescents were merged by the Malignant Germ Cell Tumor International Collaborative. The goal was to ascertain the important prognostic factors in 519 young patients who received chemotherapy, incorporating age at diagnosis, stage, and site of primary tumor, along with pretreatment AFP level and histology 79. In this age-focused investigation of these factors in young children and adolescents, outcomes included the following 79:
- Patients aged 11 years and older with stage 3 or stage 4 extragonadal disease or stage 4 ovarian disease had a less than 70% likelihood of long-term disease-free survival, ranging from 40% (extragonadal stage 4) to 67% (ovarian stage 4).
- Boys (aged 11 years and older) with International Germ Cell Consensus Classification intermediate-risk or poor-risk features also had inferior outcomes 80.
- Presence of a yolk sac tumor predicted better outcome, but it did not achieve statistical significance at the .05 level.
- Preoperative AFP levels were not prognostic. Postoperative AFP levels were prognostic in adult men 80.
A subsequent study used a database of 11 germ cell tumor trials and identified 593 patients with metastatic testicular, mediastinal, or retroperitoneal germ cell tumors. The distribution of patients by age groups included 90 children (aged 0 to <11 years), 109 adolescents (aged 11 to <18 years), and 394 young adults (aged 18 to ≤30 years) 81:
- The 5-year event-free survival (EFS) rate was lower for adolescents (72%) than it was for children (90%) or young adults (88%).
- After adjusting for the International Germ Cell Consensus Classification risk group 80, only the difference in event-free survival (EFS) between adolescents and children remained significant 81.
Although few pediatric data exist, adult studies have shown that an unsatisfactory decline of elevated tumor markers after the first cycle of chemotherapy is a poor prognostic finding 82, 83.
The presence of gonadal dysgenesis in patients with ovarian nondysgerminomas is associated with worse outcomes. In a report from the Children’s Oncology Group AGCT 0132 study 84, seven patients with gonadal dysgenesis and ovarian nondysgerminomas had an estimated 3-year event-free survival (EFS) rate of 67%, compared with 89% for 100 patients with nondysgerminoma ovarian tumors who did not have gonadal dysgenesis. These dysgenetic gonads contain Y-chromosome material, and intra-abdominal gonads with Y-chromosome material are at increased risk of tumor development 85, 86. In contrast to nondysgerminomas, gonadal dysgenesis was identified in 7 of 48 patients with ovarian dysgerminomas in a report from the French Society of Pediatric Oncology. With a medium follow-up of 14 years, all patients survived 87.
Yolk sac tumor survival rates
Yolk sac tumor was universally life-threatening before the development of combination chemotherapy. The good news is that treatments like surgery and BEP (bleomycin, etoposide and platinum) chemotherapy improve the survival rate of people diagnosed with yolk sac tumors. Adding cisplatin to combination therapies, prognosis of the patients reached excellent values, even for patients with advanced stages 29. For example, nearly all stage 1 testicular yolk sac tumors are curable with this treatment. A recent study tracking the survival of people treated for ovarian yolk cell tumors showed that 91.5% with early-stage cancer were alive five years later. That number was 74.8% for people who had cancer spread beyond their ovaries.
- Chen LH, Yip K-C, Wu H-J, Yong S-B. Yolk sac tumor in an eight-year-old girl: a case report and literature review. Front Pediatr. 2019;7:169. doi: 10.3389/fped.2019.00169[↩]
- Rwomurushaka ES, Mremi A, Lodhia J. Yolk-sac carcinoma mimicking sacrococcygeal teratoma in an infant. Radiol Case Rep. 2024 Oct 4;20(1):34-41. doi: 10.1016/j.radcr.2024.09.106[↩][↩][↩]
- Quirk JT, Natarajan N. Ovarian cancer incidence in the United States, 1992-1999. Gynecol Oncol. (2005) 97:519–23. 10.1016/j.ygyno.2005.02.007[↩]
- Merchant A, Stewart RW. Sacrococcygeal yolk sac tumor presenting as subcutaneous fluid collection initially treated as abscess. South Med J. 2010;103:1068–1070. doi: 10.1097/SMJ.0b013e3181efb572[↩]
- Khanchel-Lakhoua F, Koubâa-Mahjoub W, Jouini R, Bel Haj Salah M, Kaabar N, Chadli-Debbiche A. Sacrococcygeal yolk sac tumor: an uncommon site. APSP J Case Rep. 2012 Sep;3(3):17. https://pmc.ncbi.nlm.nih.gov/articles/PMC3468336[↩]
- Ulbright TM. Germ cell tumors of the gonads: a selective review emphasizing problems in differential diagnosis, newly appreciated, and controversial issues. Mod Pathol. 2005 Feb;18 Suppl 2:S61-79. doi: 10.1038/modpathol.3800310[↩]
- Dell’Aversana S, Coppola M, Romeo V, Ugga L, Piccin L, Sirignano C, D’Amico A, Soscia E, Matano E, D’Armiento FP, Del Basso De Caro M, Camera L, Maurea S. Germ cell tumors in male patients without gonadal involvement: computed tomography/magnetic resonance imaging findings and diagnostic workflow. Quant Imaging Med Surg. 2019 Dec;9(12):2000-2007. doi: 10.21037/qims.2019.11.01[↩][↩]
- Phi JH. Sacrococcygeal Teratoma : A Tumor at the Center of Embryogenesis. J Korean Neurosurg Soc. 2021 May;64(3):406-413. doi: 10.3340/jkns.2021.0015[↩]
- Chen LH, Yip KC, Wu HJ, Yong SB. Yolk Sac Tumor in an Eight-Year-Old Girl: A Case Report and Literature Review. Front Pediatr. 2019 Apr 30;7:169. doi: 10.3389/fped.2019.00169[↩]
- Mandelia A, Mutt N, Lal R, Prasad R. Yolk Sac tumor of stomach: case report and review of literature. J Indian Assoc Pediatr Surg. (2018) 23:232–3. 10.4103/jiaps.JIAPS_17_18[↩]
- Imaniar R, Syahruddin E, Soepandi PZ, Putra AC, Nurwidya F. Mediastinal yolk sac tumor infiltrating the heart. Exp Oncol. (2018) 40:82–4. 10.31768/2312-8852.2018[↩]
- Mondal K, Mandal R. Bilateral lung metastases unveils an asymptomatic sacrococcygeal yolk sac tumor. Indian J Pathol Microbiol. (2017) 60:565–7. 10.4103/IJPM.IJPM_385_16[↩]
- Chen Z, Zheng P, Huang S, Zhang D. Yolk sac tumor of upper lip: a case report. Oncol Lett. (2017) 14:6238–42. 10.3892/ol.2017.6918[↩]
- Kamal S, Kaliki S, Sreedhar A, Mishra DK. Primary orbital yolk sac tumor: report of a case and review of literature. Int Ophthalmol. (2016) 36:435–44. 10.1007/s10792-015-0142-y[↩]
- Pasricha S, Gupta A, Shah M, Vadodaria H. Extragonadal yolk sac tumor of face in a female infant: a case report. Indian J Pathol Microbiol. (2010) 53:592–3. 10.4103/0377-4929.68269[↩]
- Tekgunduz SA, Bozkurt C, Sahin G, Apaydin S, Oren AC, Balkaya E, et al. A subcutaneous paraspinal yolk sac tumor in a child. J Pediatr Hematol Oncol. (2014) 36:e115–7. 10.1097/MPH.0b013e31829d140a[↩]
- Zhang Q, Huang Y, Bao CY, Li LJ. Yolk sac tumour involving floor of mouth: case report. Br J Oral Maxillofac Surg. (2013) 51:e67–9. 10.1016/j.bjoms.2012.04.074[↩]
- Filho BC, McHugh JB, Carrau RL, Kassam AB. Yolk sac tumor in the nasal cavity. Am J Otolaryngol. (2008) 29:250–4. 10.1016/j.amjoto.2007.09.001[↩]
- Liang TC, Lu MY, Chen SJ, Lu FL, Lin KH. Cardiac tamponade caused by intrapericardial yolk sac tumor in a boy. J Formos Med Assoc. 2002 May;101(5):355-8.[↩]
- Alkatan HM, Al-Kofide A, Al-Hussain H. Yolk sac tumor: histopathologic report of 2 cases. Can J Ophthalmol. 2008 Feb;43(1):125-6. doi: 10.3129/i07-198[↩]
- Samaila MO, Maitama HY, Abdullahi K, Mbibu H, Waziri GD. Yolk sac tumour of the penile shaft: a rare primary extra-gonadal presentation. Afr J Paediatr Surg. 2011 May-Aug;8(2):241-3. doi: 10.4103/0189-6725.86074[↩]
- Magni E, Sonzogni A, Zampino MG. Primary pure gastric yolk sac tumor. Rare Tumors. 2010 Mar 31;2(1):e10. doi: 10.4081/rt.2010.e10[↩]
- Pawar NP, Mahajan S V, Chaudhari RA, Chavan SD. Extragonadal GCT: a rare case report of sacrococcygeal pure yolk sac tumor. Indian J Pathol Microbiol. 2013;56:329–331. doi: 10.4103/0377-4929.120421[↩]
- Bernstein L, Smith ML. Germ cell trophoblastic and other gonadal neoplasms ICCC X 1975–2004. In: Ries L, Melbert D, Krapcho M, editors. SEER Cancer Statistics Review. Bethesda, MD: National Cancer Institute; (2007). p. 125–37.[↩]
- Children’s Oncology Group Family Handbook 2nd Edition. https://www.childrensoncologygroup.org/docs/default-source/pdf/english_cog_family_handbook.pdf[↩]
- Dell’Aversana S, Coppola M, Romeo V, Ugga L, Piccin L, Sirignano C, et al. Germ cell tumors in male patients without gonadal involvement: computed tomography/magnetic resonance imaging findings and diagnostic workflow. Quant Imaging Med Surg. 2019;9:2000–2007. doi: 10.21037/qims.2019.11.01[↩]
- Cheng X, Yu H, Li J, Han X, Meng E, Zhou H, et al. Dramatic response to local radiotherapy in a refractory metastatic mediastinal yolk sac tumor patient harboring a germline BRCA2 frameshift mutation: a case report. Cancer Biol Ther. 2022;23:393–400. doi: 10.1080/15384047.2022.2072635[↩]
- Nawa A, Obata N, Kikkawa F, Kawai M, Nagasaka T, Goto S, Nishimori K, Nakashima N. Prognostic factors of patients with yolk sac tumors of the ovary. Am J Obstet Gynecol. 2001 May;184(6):1182-8. doi: 10.1067/mob.2001.113323[↩][↩][↩]
- Umezu T, Kajiyama H, Terauchi M, Shibata K, Ino K, Nawa A, Kikkawa F. Long-term outcome and prognostic factors for yolk sac tumor of the ovary. Nagoya J Med Sci. 2008 Mar;70(1-2):29-34.[↩][↩][↩][↩]
- Gabra HO, Jesudason EC, McDowell HP, Pizer BL, Losty PD. Sacrococcygeal teratoma–a 25-year experience in a UK regional center. J Pediatr Surg. 2006;41:1513–1516. doi: 10.1016/j.jpedsurg.2006.05.019[↩]
- Masahata K, Ichikawa C, Makino K, Abe T, Kim K, Yamamichi T, et al. Long-term functional outcome of sacrococcygeal teratoma after resection in neonates and infants: a single-center experience. Pediatr Surg Int. 2020;36:1327–1332. doi: 10.1007/s00383-020-04752-7[↩]
- Barksdale EM, Jr, Obokhare I. Teratomas in infants and children. Curr Opin Pediatr. 2009;21:344–349. doi: 10.1097/MOP.0b013e32832b41ee[↩]
- PDQ Pediatric Treatment Editorial Board. Childhood Extracranial Germ Cell Tumors Treatment (PDQ®): Health Professional Version. 2024 Nov 5. In: PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK65877[↩]
- McKenney JK, Heerema-McKenney A, Rouse RV. Extragonadal germ cell tumors: a review with emphasis on pathologic features, clinical prognostic variables, and differential diagnostic considerations. Adv Anat Pathol 2007;14:69-92. 10.1097/PAP.0b013e31803240e6[↩]
- Arumugam D, Thandavarayan P, Chidambaram L, Boj S, Marudasalam S. Primary Nasopharngeal Yolk Sac Tumor: A Case Report. J Clin Diagn Res. 2016 May;10(5):ED06-7. doi: 10.7860/JCDR/2016/17620.7760[↩]
- Futagami M, Yokoyama Y, Shigeto T, Mizunuma H. A case of recurrent yolk sac tumor as spindle cell sarcoma of the abdominal wall. Eur J Gynaecol Oncol. 2010;31(6):690-3.[↩]
- Shah JP, Kumar S, Bryant CS, Ali-Fehmi R, Malone JM Jr, Deppe G, Morris RT. A population-based analysis of 788 cases of yolk sac tumors: A comparison of males and females. Int J Cancer. 2008 Dec 1;123(11):2671-5. doi: 10.1002/ijc.23792[↩]
- Maizlin II, Dellinger M, Gow KW, Goldin AB, Goldfarb M, Nuchtern JG, Langer M, Vasudevan SA, Doski JJ, Raval MV, Beierle EA. Testicular tumors in prepubescent patients. J Pediatr Surg. 2018 Sep;53(9):1748-1752. doi: 10.1016/j.jpedsurg.2017.09.020[↩]
- Kruslin B, Turcić M, Cupić H, Novosel I, Reljić A, Ruzić B, Belicza M. Vaznost odredivanja razlicitih histoloskih sastavnica tumora zametnih stanica testisa [Importance of determination of various histologic components in testicular germ cell tumors]. Lijec Vjesn. 2003 Sep-Oct;125(9-10):242-5. Croatian.[↩]
- Hannan A, Malik MA, Fasih S, Badar F, Siddiqui N. MALIGNANT OVARIAN GERM CELL TUMORS AT A TERTIARY CARE SETTING IN PAKISTAN. J Ayub Med Coll Abbottabad. 2015 Jul-Sep;27(3):624-7.[↩]
- Kattuoa Ml, Dunton CJ. Yolk Sac Tumors. [Updated 2023 Feb 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK563163[↩]
- Kato N, Tamura G, Fukase M, Shibuya H, Motoyama T. Hypermethylation of the RUNX3 gene promoter in testicular yolk sac tumor of infants. Am J Pathol. 2003 Aug;163(2):387-91. doi: 10.1016/S0002-9440(10)63668-1[↩]
- Siltanen S, Anttonen M, Heikkilä P, Narita N, Laitinen M, Ritvos O, Wilson DB, Heikinheimo M. Transcription factor GATA-4 is expressed in pediatric yolk sac tumors. Am J Pathol. 1999 Dec;155(6):1823-9. doi: 10.1016/S0002-9440(10)65500-9[↩][↩]
- Wei Y, Wu S, Lin T, He D, Li X, Liu J, Liu X, Hua Y, Lu P, Wei G. Testicular yolk sac tumors in children: a review of 61 patients over 19 years. World J Surg Oncol. 2014 Dec 29;12:400. doi: 10.1186/1477-7819-12-400[↩]
- Cicin I, Saip P, Guney N, Eralp Y, Ayan I, Kebudi R, Topuz E. Yolk sac tumours of the ovary: evaluation of clinicopathological features and prognostic factors. Eur J Obstet Gynecol Reprod Biol. 2009 Oct;146(2):210-4. doi: 10.1016/j.ejogrb.2009.02.052[↩]
- Stefanelli E, Talarico V, Scavone M, Carboni E, Stranieri G, Galati MC, Salerno D, Raiola G. Acute abdominal pain in an adolescent girl with an ovarian yolk sac tumor. Acta Biomed. 2019 Dec 23;90(4):599-602. doi: 10.23750/abm.v90i4.9017[↩]
- Ueno T, Tanaka YO, Nagata M, Tsunoda H, Anno I, Ishikawa S, Kawai K, Itai Y. Spectrum of germ cell tumors: from head to toe. Radiographics. 2004 Mar-Apr;24(2):387-404. doi: 10.1148/rg.242035082[↩]
- Rosado-de-Christenson ML, Templeton PA, Moran CA. Mediastinal germ cell tumors: radiologic and pathologic correlation. RadioGraphics 1992;12:1013-30. 10.1148/radiographics.12.5.1326777[↩]
- Nichols CR. Mediastinal germ cell tumors: clinical features and biologic correlates. Chest 1991;99:472-9. 10.1378/chest.99.2.472[↩]
- Gong W, Su Y, Liu A, Liu J, Sun D, Jiang T, Xiang J, Chi C, Sun P. Clinical characteristics and treatments of patients with alpha-fetoprotein producing gastric carcinoma. Neoplasma. 2018 Mar 14;65(3):326-330. doi: 10.4149/neo_2018_170207N84[↩][↩]
- Cornejo KM, Frazier L, Lee RS, Kozakewich HP, Young RH. Yolk Sac Tumor of the Testis in Infants and Children: A Clinicopathologic Analysis of 33 Cases. Am J Surg Pathol. 2015 Aug;39(8):1121-31. doi: 10.1097/PAS.0000000000000432[↩]
- Kim CY, Choi JW, Lee JY, Kim SK, Wang KC, Park SH, Choe G, Ahn HS, Kim IH, Cho BK. Intracranial growing teratoma syndrome: clinical characteristics and treatment strategy. J Neurooncol. 2011 Jan;101(1):109-15. doi: 10.1007/s11060-010-0238-1[↩]
- Schindewolffs L, Dierks C, Heppelmann M, Gähle M, Piechotta M, Beineke A, Brehm R, Distl O. Testicular yolk sac tumor and impaired spermatogenesis in a Holstein Friesian calf. Syst Biol Reprod Med. 2015;61(5):314-9. doi: 10.3109/19396368.2015.1066901[↩]
- Cao D, Li J, Guo CC, Allan RW, Humphrey PA. SALL4 is a novel diagnostic marker for testicular germ cell tumors. Am J Surg Pathol. 2009 Jul;33(7):1065-77. doi: 10.1097/PAS.0b013e3181a13eef[↩]
- Kao CS, Idrees MT, Young RH, Ulbright TM. Solid pattern yolk sac tumor: a morphologic and immunohistochemical study of 52 cases. Am J Surg Pathol. 2012 Mar;36(3):360-7. doi: 10.1097/PAS.0b013e31823c510b[↩]
- Extragonadal Germ Cell Tumors Treatment (PDQ®)–Patient Version. https://www.cancer.gov/types/extragonadal-germ-cell/patient/extragonadal-treatment-pdq[↩]
- de La Motte Rouge T, Pautier P, Duvillard P, Rey A, Morice P, Haie-Meder C, Kerbrat P, Culine S, Troalen F, Lhommé C. Survival and reproductive function of 52 women treated with surgery and bleomycin, etoposide, cisplatin (BEP) chemotherapy for ovarian yolk sac tumor. Ann Oncol. 2008 Aug;19(8):1435-1441. doi: 10.1093/annonc/mdn162[↩]
- Zhang GY, Zhang R, Wu LY, Li B, Li SM. Neoadjuvant Bleomycin, Etoposide, and Cisplatin (BEP) Chemotherapy in the Treatment of Extensively Advanced Yolk Sac Tumors: A Single Center Experience. Int J Gynecol Cancer. 2018 May;28(4):713-720. doi: 10.1097/IGC.0000000000001209[↩]
- Ahmed HU, Arya M, Muneer A, Mushtaq I, Sebire NJ. Testicular and paratesticular tumours in the prepubertal population. Lancet Oncol. (2010) 11:476–83. 10.1016/S1470-2045(10)70012-7[↩]
- Khan IU, Jose J, Fawazy T, Hadi WA, Sharma PK. Testicular yolk sac tumor in an eight-month old child: a case report. Gulf Med. J. (2012) 1:37–40.[↩][↩]
- Guida M, Pignata S, Palumbo AR, Miele G, Marra ML, Visconti F, Zullo F. Laparoscopic treatment of a Yolk Sac Tumor: case report and literature review. Transl Med UniSa. 2013 Sep 2;7:1-5. https://pmc.ncbi.nlm.nih.gov/articles/PMC3829784[↩]
- Liu HC, Liang DC, Chen SH, Liu FL, Chang PY, Sheu JC, Wang NL. The stage I yolk sac tumor of testis in children younger than 2 years, chemotherapy or not? Pediatr Hematol Oncol. 1998 May-Jun;15(3):223-8. doi: 10.3109/08880019809028788[↩]
- Wang Y, Yang J, Yu M, Cao D, Zhang Y, Zong X, Shen K. Ovarian yolk sac tumor in postmenopausal females: A case series and a literature review. Medicine (Baltimore). 2018 Aug;97(33):e11838. doi: 10.1097/MD.0000000000011838[↩]
- Ayhan A, Taskiran C, Bozdag G, Altinbas S, Altinbas A, Yuce K. Endodermal sinus tumor of the ovary: the Hacettepe University experience. Eur J Obstet Gynecol Reprod Biol. 2005 Dec 1;123(2):230-4. doi: 10.1016/j.ejogrb.2005.04.021[↩]
- McBee WC, Jr, Brainard J, Sawady J, Rose PG. Yolk sac tumor of the ovary associated with endometrioid carcinoma with metastasis to the vagina: a case report. Gynecol Oncol. (2007) 105:244–7. 10.1016/j.ygyno.2006.07.042[↩]
- Eddaoualline H, Sami H, Rais H, Belbaraka R, El Omrani A, Khouchani M. Ovarian Yolk sac tumor: a case report and literature review. Clin Case Rep Int. (2018) 2:1057.[↩][↩]
- Ayhan A, Taskiran C, Bozdag G, Altinbas S, Altinbas A, Yuce K. Endodermal sinus tumor of the ovary: the Hacettepe University experience. Eur J Obstet Gynecol Reprod Biol. (2005) 123:230–4. 10.1016/j.ejogrb.2005.04.021[↩]
- Curtin JP, Morrow CP, D’Ablaing G, Schlaerth JB. Malignant germ cell tumors of the ovary: 20-year report of LAC-USC Women’s Hospital. Int J Gynecol Cancer. 1994 Jan;4(1):29-35. doi: 10.1046/j.1525-1438.1994.04010029.x[↩]
- Williams SD, Birch R, Einhorn LH, Irwin L, Greco FA, Loehrer PJ. Treatment of disseminated germ-cell tumors with cisplatin, bleomycin, and either vinblastine or etoposide. N Engl J Med. 1987 Jun 4;316(23):1435-40. doi: 10.1056/NEJM198706043162302[↩]
- Gobel U, Calaminus G, Schneider DT, Schmidt P, Haas RJ, Makei, et al. Management of germ cell tumors in children: approaches to cure. Onkologie. (2002) 25:14–22. 10.1159/000055197[↩]
- Chang FH, Lai CH, Chu KK, Chang TC, Hsueh S, Hung IJ. Treatment of malignant germ cell tumors of the ovary. J Formos Med Assoc. 1994 May;93(5):411-6.[↩]
- Rudaitis V, Mickys U, Katinaite J, Dulko J. Successful treatment of advanced stage yolk sac tumour of extragonadal origin: a case report and review of literature. Acta Med Litu. (2016) 23:110–6. 10.6001/actamedica.v23i2.3327[↩][↩]
- Williams S, Blessing JA, Liao SY, Ball H, Hanjani P. Adjuvant therapy of ovarian germ cell tumors with cisplatin, etoposide, and bleomycin: a trial of the Gynecologic Oncology Group. J Clin Oncol. 1994 Apr;12(4):701-6. doi: 10.1200/JCO.1994.12.4.701[↩]
- Zanetta G, Bonazzi C, Cantu M, Binidagger S, Locatelli A, Bratina G, et al. Survival and reproductive function after treatment of malignant germ cell ovarian tumors. J Clin Oncol. (2001) 19:1015–20. 10.1200/JCO.2001.19.4.1015[↩]
- Byrne J, Mulvihill JJ, Myers MH, Connelly RR, Naughton MD, Krauss MR, Steinhorn SC, Hassinger DD, Austin DF, Bragg K, et al. Effects of treatment on fertility in long-term survivors of childhood or adolescent cancer. N Engl J Med. 1987 Nov 19;317(21):1315-21. doi: 10.1056/NEJM198711193172104[↩]
- Kawai M, Kano T, Furuhashi Y, Mizuno K, Nakashima N, Hattori SE, Kazeto S, Iida S, Ohta M, Arii Y, et al. Prognostic factors in yolk sac tumors of the ovary. A clinicopathologic analysis of 29 cases. Cancer. 1991 Jan 1;67(1):184-92. doi: 10.1002/1097-0142(19910101)67:1<184::aid-cncr2820670131>3.0.co;2-c[↩]
- Fonseca A, Xia C, Lorenzo AJ, Krailo M, Olson TA, Pashankar F, Malogolowkin MH, Amatruda JF, Billmire DF, Rodriguez-Galindo C, Frazier AL, Shaikh F. Detection of Relapse by Tumor Markers Versus Imaging in Children and Adolescents With Nongerminomatous Malignant Germ Cell Tumors: A Report From the Children’s Oncology Group. J Clin Oncol. 2019 Feb 10;37(5):396-402. doi: 10.1200/JCO.18.00790[↩]
- Smith MA, Altekruse SF, Adamson PC, Reaman GH, Seibel NL. Declining childhood and adolescent cancer mortality. Cancer. 2014 Aug 15;120(16):2497-506. doi: 10.1002/cncr.28748[↩]
- Frazier AL, Hale JP, Rodriguez-Galindo C, Dang H, Olson T, Murray MJ, Amatruda JF, Thornton C, Arul GS, Billmire D, Shaikh F, Pashankar F, Stoneham S, Krailo M, Nicholson JC. Revised risk classification for pediatric extracranial germ cell tumors based on 25 years of clinical trial data from the United Kingdom and United States. J Clin Oncol. 2015 Jan 10;33(2):195-201. doi: 10.1200/JCO.2014.58.3369[↩][↩]
- International Germ Cell Consensus Classification: a prognostic factor-based staging system for metastatic germ cell cancers. International Germ Cell Cancer Collaborative Group. J Clin Oncol. 1997 Feb;15(2):594-603. doi: 10.1200/JCO.1997.15.2.594[↩][↩][↩]
- Shaikh F, Stark D, Fonseca A, Dang H, Xia C, Krailo M, Pashankar F, Rodriguez-Galindo C, Olson TA, Nicholson JC, Murray MJ, Amatruda JF, Billmire D, Stoneham S, Frazier AL. Outcomes of adolescent males with extracranial metastatic germ cell tumors: A report from the Malignant Germ Cell Tumor International Consortium. Cancer. 2021 Jan 15;127(2):193-202. doi: 10.1002/cncr.33273[↩][↩]
- Motzer RJ, Nichols CJ, Margolin KA, Bacik J, Richardson PG, Vogelzang NJ, Bajorin DF, Lara PN Jr, Einhorn L, Mazumdar M, Bosl GJ. Phase III randomized trial of conventional-dose chemotherapy with or without high-dose chemotherapy and autologous hematopoietic stem-cell rescue as first-line treatment for patients with poor-prognosis metastatic germ cell tumors. J Clin Oncol. 2007 Jan 20;25(3):247-56. doi: 10.1200/JCO.2005.05.4528[↩]
- Fizazi K, Pagliaro L, Laplanche A, Fléchon A, Mardiak J, Geoffrois L, Kerbrat P, Chevreau C, Delva R, Rolland F, Theodore C, Roubaud G, Gravis G, Eymard JC, Malhaire JP, Linassier C, Habibian M, Martin AL, Journeau F, Reckova M, Logothetis C, Culine S. Personalised chemotherapy based on tumour marker decline in poor prognosis germ-cell tumours (GETUG 13): a phase 3, multicentre, randomised trial. Lancet Oncol. 2014 Dec;15(13):1442-1450. doi: 10.1016/S1470-2045(14)70490-5[↩]
- Dicken BJ, Billmire DF, Krailo M, Xia C, Shaikh F, Cullen JW, Olson TA, Pashankar F, Malogolowkin MH, Amatruda JF, Rescorla FJ, Egler RA, Ross JH, Rodriguez-Galindo C, Frazier AL. Gonadal dysgenesis is associated with worse outcomes in patients with ovarian nondysgerminomatous tumors: A report of the Children’s Oncology Group AGCT 0132 study. Pediatr Blood Cancer. 2018 Apr;65(4):10.1002/pbc.26913. doi: 10.1002/pbc.26913[↩]
- Huang H, Wang C, Tian Q. Gonadal tumour risk in 292 phenotypic female patients with disorders of sex development containing Y chromosome or Y-derived sequence. Clin Endocrinol (Oxf). 2017 Apr;86(4):621-627. doi: 10.1111/cen.13255[↩]
- Thorup J, McLachlan R, Cortes D, Nation TR, Balic A, Southwell BR, Hutson JM. What is new in cryptorchidism and hypospadias–a critical review on the testicular dysgenesis hypothesis. J Pediatr Surg. 2010 Oct;45(10):2074-86. doi: 10.1016/j.jpedsurg.2010.07.030[↩]
- Duhil de Bénazé G, Pacquement H, Faure-Conter C, Patte C, Orbach D, Corradini N, Berger C, Sudour-Bonnange H, Vérité C, Martelli H, Fresneau B. Paediatric dysgerminoma: Results of three consecutive French germ cell tumours clinical studies (TGM-85/90/95) with late effects study. Eur J Cancer. 2018 Mar;91:30-37. doi: 10.1016/j.ejca.2017.11.030[↩]





{kind=link}