Contents
What is a root canal
A root canal is a dental procedure that involves drilling a hole into a decayed tooth and removing the soft center, known as the dental pulp, to remove dead or dying nerve tissue and bacteria from inside a tooth – the space in a tooth containing the dental pulp. The portion of the cavity within the crown of the tooth is the pulp chamber; the portion within the root is the pulp canal or root canal. A root canal is done if you have an infection that affects the pulp of a tooth. Generally, there is pain and swelling in the area. The infection can be the result of a tooth crack, cavity, or injury. It may also be the result of a deep pocket in the gum area around a tooth. If this is the case, a dental specialist known as a periodontist should examine the area.
A root canal can save your tooth. Without a root canal treatment, the tooth may become so damaged that it must be removed.
The dental pulp is made up of connective tissue, nerves and blood supply, and extends into the roots of the tooth. The crown, or surface of the tooth that is used for chewing, may also be replaced if necessary.
If your tooth pulp becomes infected, the infection may spread through the root canal system of the tooth (see “What is tooth cavity” below). This may eventually lead to an abscess. An abscess is an inflamed area in which pus collects and can cause swelling of the tissues around the tooth. The symptoms of a tooth abscess can range from a dull ache to severe pain, and the tooth may be tender when you bite. If root canal treatment is not done, the infection will spread and the tooth may need to be taken out.
You may not feel any pain in the early stages of the root canal infection. In some cases your tooth could darken in color, which may mean that the nerve of the tooth has died (or is dying). This would need root canal treatment.
Root canal symptoms – symptoms of tooth pulp damage or disease
A diseased tooth pulp may cause inflammation or infection. The symptoms of a damaged or diseased tooth pulp may include:
- unprovoked or spontaneous pain
- sensitivity to hot and cold drinks and foods
- pain when biting or chewing
- loosening of the tooth
- swelling of the gum near the affected tooth
- oozing of pus surrounding the affected tooth
- facial swelling.
Sometimes, tooth pulp may become damaged or diseased without presenting any symptoms. In these cases, the problem is usually diagnosed by special tests or x-rays during a dental check-up or treatment for other dental concerns.
A root canal treatment is a dental procedure in which a hole is drilled into the decayed tooth, cleaned and filled with medicine, and capped with a crown. Root canal filings is any material that is used to seal the root canal and protect against re-infection.
A root canal treatment is a sequence of treatments involving root canal cleaning, shaping, decontamination and obturation 1. A root canal treatment is conventionally performed through a hole drilled into the crown of the affected tooth, namely orthograde root canal therapy. For teeth that cannot be treated with orthograde root canal therapy, or for which it has failed, retrograde root filling, which seals the root canal from the root apex, is a good alternative. Many materials, such as amalgam, zinc oxide eugenol and mineral trioxide aggregate, are generally used. Since none meets all the criteria an ideal material should possess, selecting the most efficacious material is of utmost importance.
Although root canal results are generally good, a small number of failures do occur. This may be attributed to the complexity of the root canal system, which has many small additional pathways communicating with each other, making it difficult to completely eliminate all of the toxins and irritants. These can spread, causing the infection around the root to last indefinitely. When root canal therapy fails, a retreatment called retrograde filling is a good alternative to save the tooth. During retrograde filling the dentist cuts a flap in the gum and creates a hole in the bone to get access to the bottom tip of the root 2. After cutting off the tip, then thorough preparation, the apex is sealed (the apical seal) and the hole made by the dentist filled with a dental material. This sealing process is thought to be the single most important factor in achieving success in a retrograde root filling. Many materials have been developed to seal the root tip, mineral trioxide aggregate is the material of interest at present, but there is no consensus about which material is best 1.
Tooth anatomy
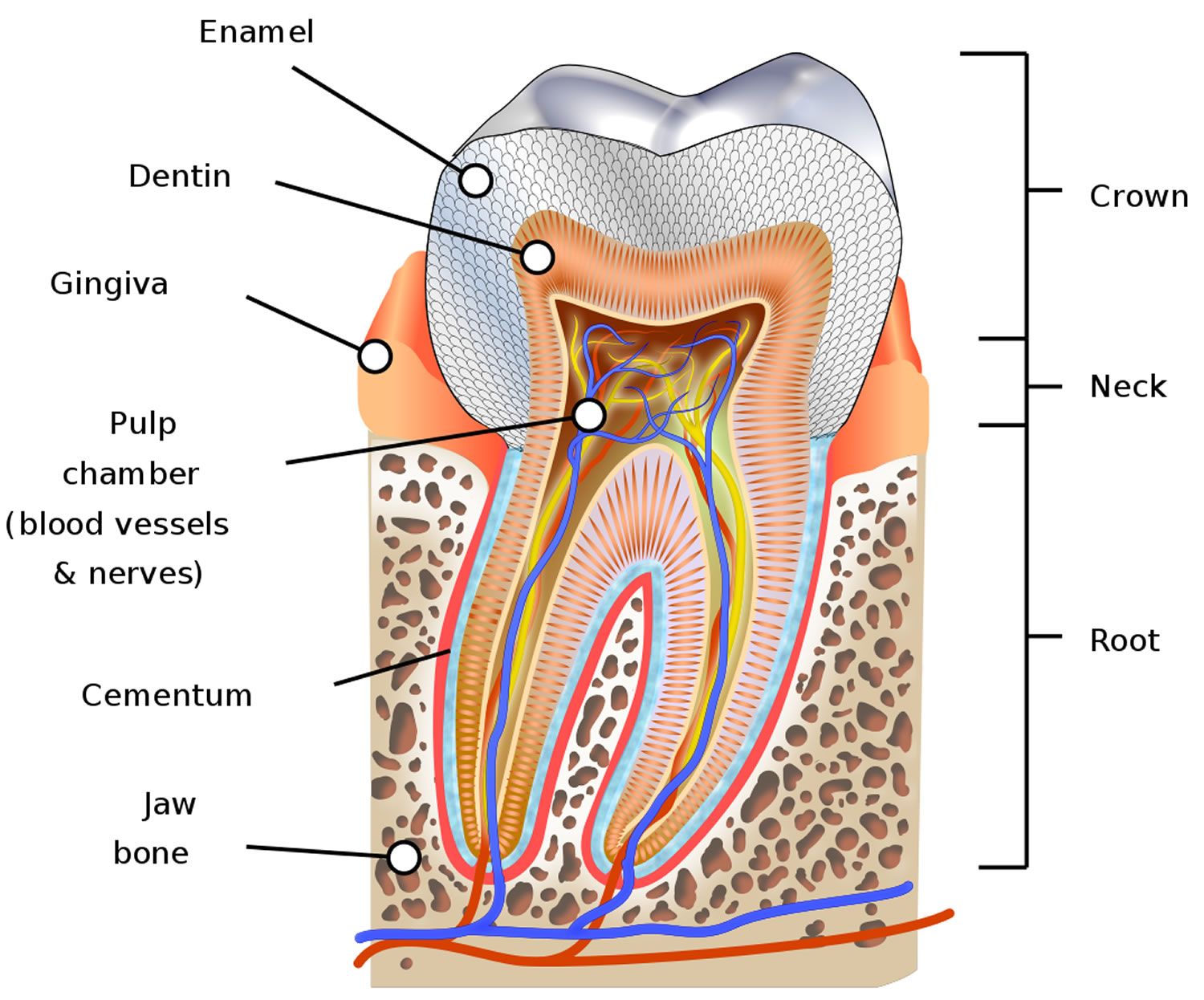
A tooth is mainly made of a hard material called dentine. Enamel is the surface layer that protects the visible part of the tooth (crown). The part of the tooth that sits beneath the gum line is called the root. The root is the ‘prong’ that helps anchor the tooth into the jaw. Generally, front teeth have only one root, while molars have several. There may be several root canals in one root.
The hollow center of a tooth is called the pulp chamber. This area contains the blood vessels, nerves and pulp. The pulp is a sensitive tissue that provides oxygen, nutrients and feeling to the tooth. The main function of the dental pulp is to regulate the growth and development of the tooth during childhood. The pulp extends from the roof of the pulp chamber down into the bottom of each root canal.Once the tooth is fully formed, nutrition for the tooth comes from the tissues surrounding the root. Therefore, a tooth can function without its pulp and, in the majority of cases, can be kept indefinitely. After endodontic treatment, the tooth is ‘pulpless’, but it is not a dead tooth.
Figure 1. Human tooth
Root canal causes
The tooth may have become infected or damaged by decay, repeated dental work, cracked fillings or an injury to the tooth.
There are many events that can lead to disease or damage to dental pulp. Some of these include:
- deep-seated and untreated dental decay
- decay beneath a deep filling
- trauma that damages a tooth
- habitual tooth grinding (bruxism)
- long-standing cracks in the teeth
- advanced gum disease
When the dental pulp is damaged, bacteria can start to multiply inside the tooth. This can lead to an infection or abscess, which is a pocket of pus that forms at the end of the tooth’s root.
What are the symptoms you might need a root canal treatment?
Sometimes there are no symptoms that a tooth needs root canal therapy. More commonly, the signs include:
- severe toothache when chewing
- sensitivity to hot or cold that lasts after the heat or cold has been removed
- darkening of the tooth
- swollen and tender gums
- a persistent pimple on the gums or a hole in the tooth
- swelling of the face or neck.
What is a tooth cavity
Tooth cavity is permanently damaged area in the hard surface (enamel) of your tooth that develop into tiny openings or holes 3. Cavities are also called tooth decay or dental caries, are caused by plaque which is a sticky, slimy substance made up mostly of the bacteria that cause tooth decay. Tooth decay can occur when acid is produced from plaque, which builds up on your teeth. If plaque is allowed to build up, it can lead to further problems, such as dental caries (holes in the teeth), gum disease or dental abscesses, which are collections of pus at the end of the teeth or in the gums. Bacteria that live in your mouth thrive on the sugars and starches in the food you eat. Plaque builds up due to frequent snacking, sipping sugary drinks and not cleaning your teeth well. When plaque clings to your teeth the bacteria in your mouth make acids that can eat away at the outermost layer of the tooth, called the enamel. The result is a cavity or a hole that can grow bigger and deeper over time. Once cavities have formed in the enamel, the plaque and bacteria can reach the dentine (the softer, bone-like material underneath the enamel). As the dentine is softer than the enamel, the process of tooth decay speeds up. If you have a tooth cavity it’s important to get it repaired as soon as possible.
Without treatment, bacteria will enter the pulp (the soft center of the tooth that contains nerves and blood vessels). At this stage, your nerves will be exposed to bacteria, usually making your tooth painful. The bacteria can cause a dental abscess in the pulp and the infection could spread into the bone, causing another type of abscess.
Plaque also causes gingivitis, which is gum disease that can make your gums red, swollen, and sore. Your gums are those soft pink tissues in your mouth that hold your teeth in place. If you don’t take care of your teeth, cavities and unhealthy gums will make your mouth very, very sore. Eating meals will be difficult.
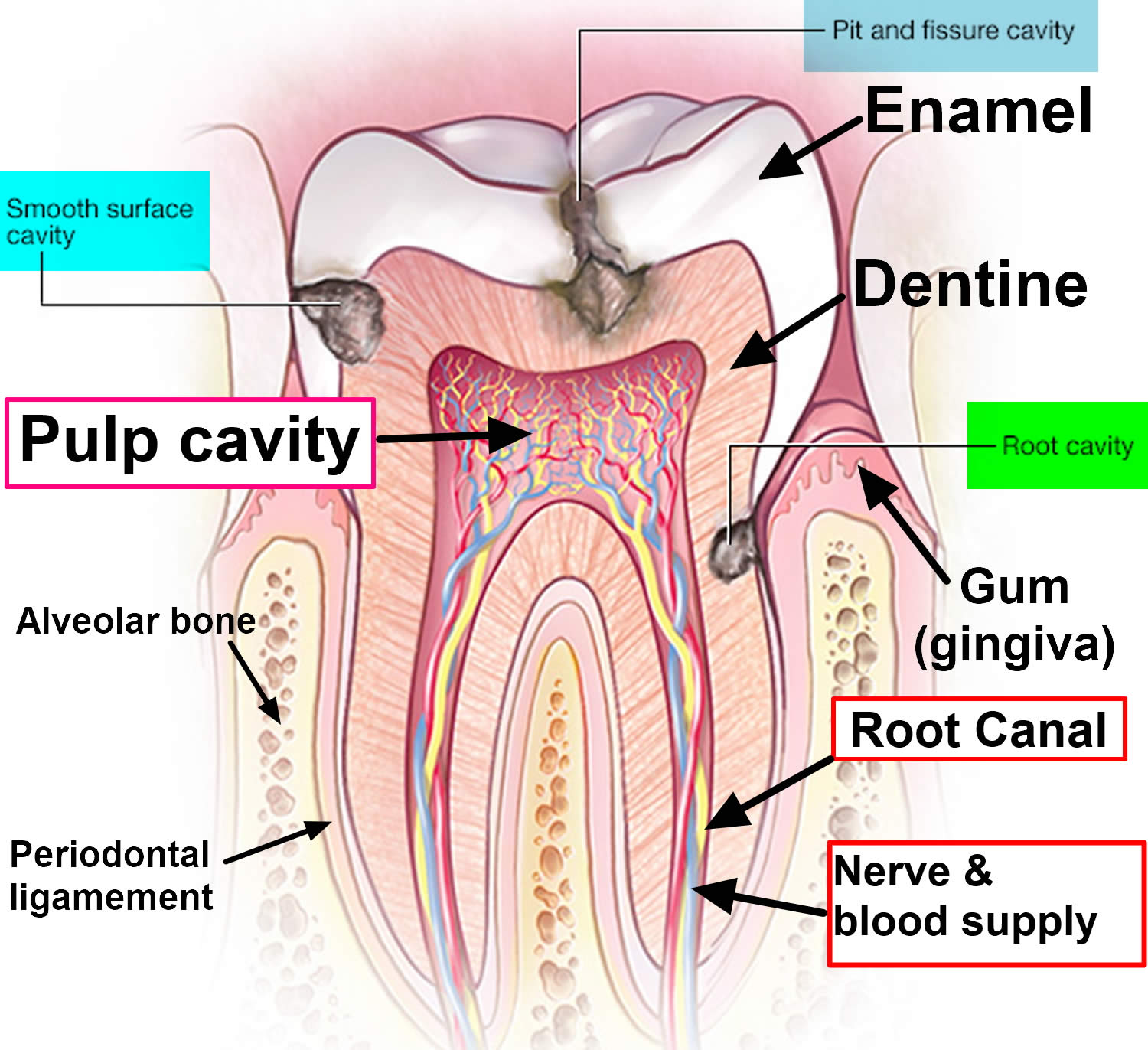
Cavities are decayed areas of your teeth that develop into tiny openings or holes. The three types of cavities are shown here in Figure 1. Smooth surface cavities occur on the smooth sides of your teeth, while root cavities develop on the surface over the roots. Pit and fissure cavities occur on the chewing surface of your teeth. Remember, not cleaning your teeth well, frequent snacking and sipping sugary drinks are the main culprits behind cavities. The first sign of tooth cavity or decay may be a sensation of pain when you eat something sweet, very cold or very hot. Sometimes decay will show as a brown or white spot on the tooth.
Tooth decay may not cause any pain. However, if you have dental caries you might have:
- toothache – either continuous pain keeping you awake or occasional sharp pain without an obvious cause
- tooth sensitivity – you may feel tenderness or pain when eating or drinking something hot, cold or sweet
- grey, brown or black spots appearing on your teeth
- bad breath
- an unpleasant taste in your mouth
Dental caries (tooth decay) remains the world’s most common chronic disease in both children and adults, even though it is largely preventable. They’re especially common in children, teenagers and older adults. But anyone who has teeth can get cavities, including infants.
If you don’t go to the dentist to have the cavities treated, the acids can continue to make their way through the enamel, the cavity will get larger and affect deeper layers of your teeth and the inside parts of your tooth where the nerve endings are can begin to decay. They can lead to a severe toothache, infection and tooth loss. Regular dental visits and good brushing and flossing habits are your best protection against cavities and tooth decay.
Although tooth decay is a common problem, it’s often entirely preventable. The best way to avoid tooth decay is to keep your teeth and gums as healthy as possible.
Complications of root canal infection
If tooth pulp infection is left untreated, complications could include:
- spreading infection – once the pulp becomes infected, it loses its ability to fight the spread of the infection. If bacteria find their way into the pulp chamber, the bacteria will multiply unchecked. This can cause a severe infection or an endodontic abscess (a pocket or ‘blister’ of pus) when it spreads into the surrounding bone
- localized bone loss – the infection may spread around the ends of the infected root canal and erode surrounding jaw bone
- loss of tooth – the tooth may have to be removed, which interferes with the person’s ability to bite and chew. Subsequent tooth replacement with dentures, bridges or dental implants are costly and may not be possible or tolerated, especially if the infection has already caused advanced bone loss.
When to see a dentist
You may not be aware that a cavity is forming. That’s why it’s important to have regular dental checkups and cleanings, even when your mouth feels fine. However, if you experience a toothache or mouth pain, see your dentist as soon as possible, so early tooth decay can be treated as soon as possible and the prevention of decay can begin. Tooth decay is much easier and cheaper to treat in its early stages. Dentists can usually identify tooth decay and further problems with a simple examination or X-ray.
It’s also important to have regular dental check-ups. Adults should have a check-up at least once every two years and children under the age of 18 should have a check-up at least once a year.
Figure 2. Tooth cavity
Tooth Cavity Prevention Tips
Though cavities can be repaired, try to avoid them by taking care of your teeth. Ask your dentist which tips are best for you.
Good oral and dental hygiene can help you avoid cavities and tooth decay. Here’s how:
- Floss your teeth at least once a day to remove plaque and food that’s stuck between your teeth after eating. Bedtime is an important time to floss.
- Brush your teeth with fluoride toothpaste after eating or drinking or at least twice a day. The American Dental Association recommends brushing your teeth twice a day with fluoride toothpaste. Bedtime is an important time to brush.
- Brush up and down in a circular motion. When you brush your teeth, you help remove food and plaque — a sticky white film that forms on your teeth and contains bacteria. After you eat a meal or snack that contains sugar, the bacteria in plaque produce acids that attack tooth enamel. Repeated attacks can break down tooth enamel and lead to cavities. Plaque that isn’t removed can also harden into tartar, making it harder to keep teeth clean.
- Gently brush your gums as well to keep them healthy.
- Limit or avoid sweets and sugary drinks, like soda or juice. Whenever you eat or drink beverages other than water, you help your mouth bacteria create acids that can destroy tooth enamel. If you snack or drink throughout the day, your teeth are under constant attack.
- Drink some tap water. Most public water supplies have added fluoride, which can help reduce tooth decay significantly. If you drink only bottled water that doesn’t contain fluoride, you’ll miss out on fluoride benefits.
- Consider dental sealants. A sealant is a protective plastic coating applied to the chewing surface of back teeth. It seals off grooves and crannies that tend to collect food, protecting tooth enamel from plaque and acid. The Centers for Disease Control and Prevention (CDC) recommends sealants for all school-age children. Sealants may last for several years before they need to be replaced, but they need to be checked regularly.
- Consider fluoride treatments. Your dentist may recommend periodic fluoride treatments, especially if you aren’t getting enough fluoride through fluoridated drinking water and other sources. He or she may also recommend custom trays that fit over your teeth for application of prescription fluoride if your risk of tooth decay is very high.
- See your dentist twice a year for regular checkups.
- Ask about antibacterial treatments. If you’re especially vulnerable to tooth decay — for example, because of a medical condition — your dentist may recommend special antibacterial mouth rinses or other treatments to help cut down on harmful bacteria in your mouth.
- Combined treatments. Chewing xylitol-based gum along with prescription fluoride and an antibacterial rinse can help reduce the risk of cavities.
What type of toothpaste should I use?
It’s important to use a toothpaste with the right concentration of fluoride. Check the packaging to find out how much fluoride each brand contains.
- Adults should use a toothpaste that contains at least 1,350 parts per million (ppm) fluoride.
- Children don’t need to use special “children’s toothpaste”. Children of all ages can use family toothpaste, as long as it contains 1,350-1,500ppm fluoride.
- Children aged six and under who don’t have tooth decay can use a lower-strength children’s toothpaste, but make sure it contains at least 1,000ppm fluoride.
- Below the age of three, children should use just a smear of toothpaste. Children aged three to six years should use a pea-sized blob of toothpaste. Make sure children don’t lick or eat toothpaste from the tube.
Your dentist may advise you or your child to use a toothpaste with a higher concentration of fluoride, if you need it.
Root canal treatment
Root canal treatment (also called ‘endodontics’) is needed when the blood or nerve supply of the tooth (called the ‘pulp’) is infected through decay or injury.
The living part of the tooth, also known as the tooth pulp, can become irreversibly inflamed as a result of damage or bacterial infection due to tooth decay. To deal with this problem, the dentist has to drill a hole to access the inner space of the tooth or root canal system, and remove the infected tissue and toxic irritants by a combination of mechanical cleaning and irrigation. After this is done, the dentist fills the space with an inert packing material and seals the opening. This procedure is known as root canal treatment.
The aim of the root canal treatment is to remove all the infection from the root canal. The root is then cleaned and filled to prevent any further infection.
Root canal treatment is a skilled and time-consuming procedure. Most courses of treatment will involve two or more visits to your dentist.
At the first appointment, the infected pulp is removed and any abscesses can be drained. The root canal is then cleaned and shaped ready for the filling. A temporary filling is put in and the tooth is left to settle.
The tooth is checked at a later visit and when all the infection has cleared, the tooth is permanently filled.
In the past, a root-filled tooth would often darken after a root canal treatment. However, with modern techniques this does not usually happen. If there is any discolouration, there are several treatments that will restore the natural appearance.
Does a root canal treatment hurt?
No. Usually, a local anaesthetic is used and it should feel no different to having an ordinary filling done. There may be some tenderness afterwards but this should gradually get less over time.
What if a root canal infection happens again?
Root canal treatment is usually very successful. However, if the infection comes back, the treatment can sometimes be repeated.
What if I don’t have the root canal treatment?
The alternative is to have the tooth out. Once the tooth pulp is destroyed it can’t heal, and it is not recommended to leave an infected tooth in the mouth.
Although some people would prefer to have the tooth out, it is usually best to keep as many natural teeth as possible.
Will the tooth be safe after a root canal treatment?
Yes. However, because a ‘dead’ tooth is more brittle, you may need to have a crown to provide extra support and strength to the tooth.
Where is root canal treatment carried out?
Root canal treatment is a routine dental procedure, which your dentist will be happy to do for you. However, sometimes your dentist may refer you to an endodontist, who is a specialist in this type of treatment.
How do I care for my tooth afterwards?
Root-treated teeth should be looked after just the same as any other tooth. Remember to clean your teeth last thing at night and at least one other time during the day, with a fluoride toothpaste. Cut down on sugary foods and drinks, and have them only at mealtimes if possible. See your dental team as often as they recommend for regular check-ups.
Root canal procedure
You may need one or more visits to complete the endodontic treatment, depending on the complexity of the case. The exact procedure chosen by your dentist may differ from the procedure outlined here. Ask your dentist for further information.
Root canal treatment has four main aims:
- Removing active decay and infection – any old or leaky fillings, tooth decay, infected nerve tissue, pus and debris are removed
- Shaping the root canals – in order to be filled well, the canals within the tooth root need to be shaped into smooth, hollow tunnels that are free of irregularities where residual bacteria may have been harboured. This shaping process involves small instruments, special disinfectants and medication. It may take a few weeks to months for these solutions to take maximum effect against stubborn bacteria within the tooth, and this step may have to be repeated several times.
- Filling the root canals – to prevent bacteria from re-infecting the empty canals in your tooth, they are permanently sealed with a long-lasting barrier material.
- Making the tooth functional again – to make sure no bacteria from the oral environment can leak back into the tooth, a large, well-sealed restoration is put on the tooth (such as a crown). Teeth that require root canal treatment have sometimes lost considerable tooth structure due to previous decay or cracks, and may require further protection in the form of porcelain, gold alloy crowns or other similar materials.
First, the dentist takes an X-ray of the tooth to see the shape of the root canals and determine whether there is any infection in the bone around the tooth.
A dentist will use a needle to place numbing medicine (local anesthetic) around the bad tooth. You may feel a slight prick when the needle is being inserted.
Next, your dentist uses a tiny drill to remove a small portion of the top part of your tooth to expose the tooth pulp. This is typically called access.
Pulp is made up of nerves, blood vessels, and connective tissue. It is found inside the tooth and runs to the jaw bone. Pulp supplies blood to a tooth and allows you to feel sensations such as temperature.
The infected pulp is removed with special tools called files. The canals (tiny pathways inside the tooth) are cleaned. Medicines may be placed into the area to make sure all the germs are removed and to prevent further infection.
The cleaned tooth area is sealed with a soft, temporary material. Once the tooth is filled, a permanent crown may be placed on top.
A pulpless tooth is more brittle than a non-treated tooth and great care should be taken to avoid fracture and chipping. The tooth is restored with a crown to prevent fracture.
You may be given antibiotics to treat and prevent infection.
It can take several appointments for the dentist to clean and shape the hole inside the tooth before placing a sterile filling inside. They may also insert a small support into the root canals to strengthen the tooth. They may cap the tooth with an artificial crown if necessary.
Root canal therapy can be more uncomfortable than a normal filling, because it takes longer, but it is often no more painful.
The root canal procedure
Root canal procedure involves the removal of the infected pulp, the subsequent shaping, cleaning, decontamination of the hollow tooth core and obturation. Traditionally, treatment is carried out through a hole drilled on the top of the crown of the tooth, and it is known as orthograde root canal therapy [Figure 3 (A and B)]. With the development of new materials and techniques, orthograde root canal therapy has been demonstrated to provide satisfactory results for patients in most cases. However, because of the well-known complexity of the root canal system and the acknowledged difficulty of completely eliminating all bacteria, their by-products and toxins, from the canal system, failures occur at a reported rate of 4% to 15% 4. There are many causes for such failures, such as untreated canals, ledges formation, perforations, and overextensions of root-filling materials 5. To plan treatment effectively, the clinician may place the causal factors into four groups 6:
- Persistent or reintroduced intraradicular micro-organisms;
- Extraradicular infection;
- Foreign body reaction;
- True cysts.
For root canal treatment failures, conventional orthograde endodontic retreatment is always the first choice. Although it is a highly predictable option in most cases, periradicular surgery may be indicated for teeth with persistent periradicular pathosis that have not responded to non-surgical approaches 7. Sometimes, apical surgery is preferred to orthograde treatment for expediency or if a tight-fitting post, especially a fiber post, is present. At this circumstance, conventional retreatment needs to remove more dentine to acquire a pathway into the original root canal, which may cause root perforation or root fracture.
Periradicular surgery should be considered as an extension to non-surgical treatment, because the underlying aetiology of the disease process and the treatment objectives are the same: the prevention or elimination of apical periodontitis 8. Periradicular surgery, also called retrograde filling, always requires root-end preparation and obturation (Figure 3 (D and E)). The former aims to expose the apical root via flap elevation and bone removal prior to cavity preparation on the apical root where the apical foramina is located. Following that, materials are placed in the cavity for apical sealing. Harty reported that the apical seal was the single most important factor in achieving success in such surgery 9. This apical seal is established by retrograde filling materials obturated between the root canal system and the surrounding tissues 10. Thus, subsequent studies have evaluated many retrograde materials so as to determine which is most efficacious.
Amalgam has been used as a retrograde filling material for many years. Its earliest use as a root-end filling following resection has been reported in 1884 11. It has the advantages of being easily available, inexpensive and easy to handle. Therefore, for many years, amalgam was accepted as the material of choice for root-end filling, and the clinical application of amalgam was well documented in several clinical studies with a reported success rate of 50% to 80% 12. However, in recent years, the efficacy of amalgam has been questioned due to initial marginal leakage, corrosion, moisture sensitivity, mercury contamination of periapical tissue and the potential hazards associated with mercury-containing materials 13. The disadvantages associated with amalgam and the potential long-term damage to the environment has led to the research and development of alternative materials.
In the past decades, amalgam has slowly given way to zinc oxide eugenol containing materials, such as intermediate restorative material, which has 20%, by weight, polymethacrylate added to the base zinc oxide powder and super ethoxybenzoic acid (Super-EBA), which contains ethoxybenzoic acid. In vitro leakage studies, animal studies, and retrospective in vivo studies indicate that these zinc oxide eugenol-containing materials are superior to amalgam in terms of sealability and biocompatibility 14. Shortcomings of the currently available zinc oxide eugenol-containing cements are their mild to moderate toxicity, when freshly mixed, and their radiopacity, which is similar to that of gutta-percha 15.
In recent years a promising new root-end filling material, mineral trioxide aggregate, developed at Loma Linda University, California, USA 16 has received widespread attention 17. Its major components are similar to Portland cement, a mixture of dicalcium silicate, tricalcium silicate, tricalcium aluminate, gypsum, and tetracalcium aluminoferrite 18. Although it is an expensive material and requires additional skill and equipment to use satisfactorily, the clinician can handle it satisfactorily after suitable training 19. Mineral trioxide aggregate has major advantages, including excellent biocompatibility 20, ideal adherence to cavity walls, low solubility 21, and the ability of inducing cementogenesis at the root surface, with deposition of new cementum onto the exposed dentine and mineral trioxide aggregate surfaces 22. Mineral trioxide aggregate is an excellent bioactive material. When it is placed in direct contact with human tissues, it will form calcium hydroxide that releases calcium ions for cell attachment and proliferation 23; modulates cytokine production 24, and encourages proliferation and migration of progenitors followed by their differentiation into odontoblast-like cells 25. However, the mean setting time of mineral trioxide aggregate is 165 ± 5 minutes, which is longer than amalgam, super ethoxybenzoic acid (Super-EBA), and intermediate restorative material 26, which is potentially problematic in endodontic surgery.
In addition to polymers, glass ionomer cements, polycarboxylate cements, zinc phosphate cements, calcium phosphate cements and composite resins have all been employed and several cases reported 27. A new material, Biodentine, which is reported to have reparative dentine synthesis properties 28, is awaiting clinical evaluation as a possible retrograde filling material. All these materials have different characteristics and are potential alternatives to traditional materials, although potential harm should be carefully considered before widespread use is considered.
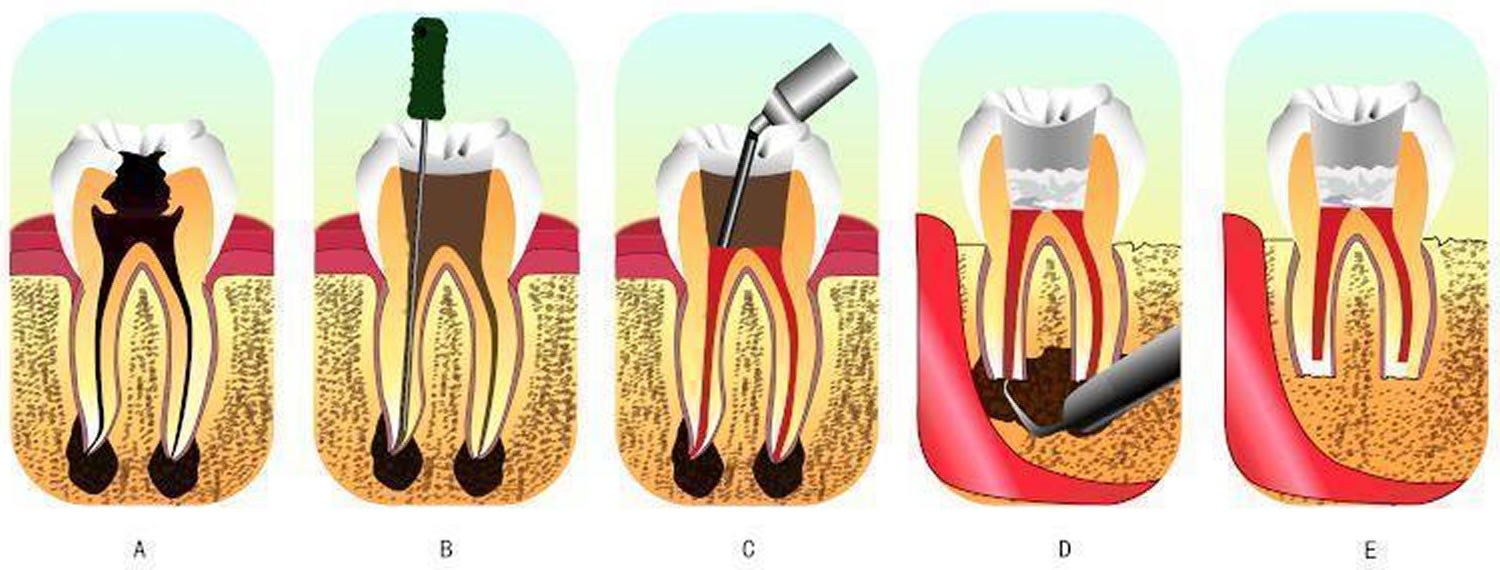
Figure 3. Root canal procedure
 Footnotes:
Footnotes:
A: an infected tooth. The inner space of the tooth is the root canal system, where the pulp is located. The pulp of this tooth is irreversibly inflamed from bacterial infection due to decay.
B and C: the process of root canal therapy. B: a hole has been drilled from the top of the crown of the tooth. The dentist could then remove the infected tissues and toxic irritants by a combination of mechanical cleaning and irrigation in the root canal system through the hole. C: after cleaning and irrigation, the dentist fills the space with an inert packing material and seals the opening.
D and E: the process of retrograde filling. D: when retrograde filling is indicated, the dentist needs to cut a flap in the gum and creates a hole in the bone to get access to the bottom tip of the root. E: after cutting off the tip, then thorough preparation, the apex is sealed (the apical seal) and the hole made by the dentist filled with a dental material.
Root canal risks
Possible risks of root canal procedure are:
- Abscess
- Loss of tooth
- Nerve damage
- Tooth fracture
Studies have proved that the main contributory factor in root canal failure is persistent microbial infection in the root canal system and periapical region 29. Chemical and mechanical preparation may not reach every corner of the complex root canal system. Bacteria in isthmuses, ramifications, irregularities and dentinal tubules may persist and some necrotic tissue debris may also remain. Bacteria may gain access to the periapical region if complete sealing is not achieved, leading to pathological lesions 30.
To control microbial infection is always a high priority in periradicular surgery. The surgery removes the pathogenic agents and establishes an environment facilitating the regeneration of damaged tissue first. Then the procedure usually involves root-end exposure and resection, in addition to preparing a Class I cavity and retrofilling with packing materials 31. Hence, these materials can form a proper seal of the internal root canal contents from the external periradicular tissues and therefore repair root defects 32.
After the root canal procedure
You will need to see your dentist after the root canal procedure to make sure the infection is gone. A dental x-ray may be taken. Regular dental checkups are necessary. For adults, this usually means a visit twice a year.
Pain after root canal procedure
You may have some pain or soreness after the procedure. An over-the-counter anti-inflammatory drug, such as ibuprofen or naproxen, can help relieve discomfort.
Root canal recovery
Most people can return to their normal routine the next day. Until the tooth is permanently filled or covered with a crown, you should avoid rough chewing in the area.
Cosmetic issues after root canal treatment
A normal tooth with a healthy pulp is yellowish-white in color. A pulp-free tooth may eventually turn grey. The dentist can advise you on appropriate aesthetic (cosmetic dentistry) procedures.
- Ma X, Li C, Jia L, Wang Y, Liu W, Zhou X, Johnson TM, Huang D. Materials for retrograde filling in root canal therapy. Cochrane Database of Systematic Reviews 2016, Issue 12. Art. No.: CD005517. DOI: 10.1002/14651858.CD005517.pub2. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD005517.pub2/full[↩][↩]
- Materials for retrograde filling in root canal therapy. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0090254[↩]
- Cavities/tooth decay. https://www.mayoclinic.org/diseases-conditions/cavities/symptoms-causes/syc-20352892[↩]
- Wong R. Conventional endodontic failure and retreatment. Dental Clinics of North America 2004;48(1):265-89. https://www.ncbi.nlm.nih.gov/pubmed/15066516[↩]
- Eriksen HM. Endodontology: epidemiologic considerations. Endodontics and Dental Traumatology 1991;7(5):189-95. https://www.ncbi.nlm.nih.gov/pubmed/1687387[↩]
- Sundqvist G, Figdor D. Endodontic treatment of apical periodontitis. In: Orstavik D, Pitt Ford TR editor(s). Essential Endodontology: Prevention and Treatment of Apical Periodontitis. London: Wiley-Blackwell, 1998:242.[↩]
- Lee YL, Lee BS, Lin FH, Yun Lin A, Lan WH, Lin CP. Effects of physiological environments on the hydration behavior of mineral trioxide aggregate. Biomaterials 2004;25(5):787-93. https://www.ncbi.nlm.nih.gov/pubmed/14609667[↩]
- Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. 11th Edition. Mosby, 2015.[↩]
- Harty FJ, Parkins BJ, Wengraf AM. The success rate of apicectomy. A retrospective study of 1016 cases. British Dental Journal 1970;129(9):407-13.[↩]
- Gutmann JL, Harrison JW. Surgical Endodontics. Boston: Blackwell Scientific Publications, 1991.[↩]
- Vasudev SK, Goel BR, Tyagi S. Root end filling materials – A review. Endodontology 2003;15:12-8.[↩]
- Grung B, Molven O, Halse A. Periapical surgery in a Norwegian county hospital: follow-up findings of 477 teeth. Journal of Endodontics 1990;16(9):411-7.[↩]
- Eley BM, Cox SW. The release, absorption and possible health effects of mercury from dental amalgam: a review of recent findings. British Dental Journal 1993;175(10):355-62. https://www.ncbi.nlm.nih.gov/pubmed/8257645[↩]
- Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. Journal of Endodontics 2006;32(7):601-23.[↩]
- Johnson BR. Considerations in the selection of a root-end filling material. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 1999;87(4):398-404.[↩]
- Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. Journal of Endodontics 1993;19(12):591-5. https://www.ncbi.nlm.nih.gov/pubmed/8151252[↩]
- Lee SJ, Monsef M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. Journal of Endodontics 1993;19(11):541-4.[↩]
- Camilleri J, Montesin FE, Brady K, Sweeney R, Curtis RV, Ford TR. The constitution of mineral trioxide aggregate. Dental Materials 2005;21(4):297-303.[↩]
- Wang WH, Wang CY, Shyu YC, Liu CM, Lin CM, Lin CP. Compositional characteristics and hydration behavior of mineral trioxide aggregates. Journal of Dental Science 2010;5(2):53-9.[↩]
- Camilleri J, Pitt Ford TR. Mineral trioxide aggregate: a review of the constituents and biological properties of the material. International Endodontic Journal 2006;39(10):747-54.[↩]
- Poggio C, Lombardini M, Conti A, Rindi S. Solubility of root-end filling materials: a comparative study. Journal of Endodontics 2007;33(9):1094-7.[↩]
- Baek SH, Plenk H Jr, Kim S. Periapical tissue responses and cementum regeneration with amalgam, SuperEBA, and MTA as root-end filling materials. Journal of Endodontics 2005;31(6):444-9.[↩]
- Takita T, Hayashi M, Takeichi O, Ogiso B, Suzuki N, Otsuka K, et al. Effect of mineral trioxide aggregate on proliferation of cultured human dental pulp cells. International Endodontic Journal 2006;39(5):415-22.[↩]
- Koh ET, McDonald F, Pitt Ford TR, Torabinejad M. Cellular response to Mineral Trioxide Aggregate. Journal of Endodontics 1998;24(8):543-7.[↩]
- Kuratate M, Yoshiba K, Shigetani Y, Yoshiba N, Ohshima H, Okiji T. Immunohistochemical analysis of nestin, osteopontin, and proliferating cells in the reparative process of exposed dental pulp capped with mineral trioxide aggregate. Journal of Endodontics 2008;34:970-4.[↩]
- Torabinejad M, Hong CU, McDonald F, Pitt Ford TR. Physical and chemical properties of a new root-end filling material. Journal of Endodontics 1995;21(7):349-53.[↩]
- Hauman CH, Love RM. Biocompatibility of dental materials used in contemporary endodontic therapy: a review. Part 2: Root-canal filling materials. International Endodontic Journal 2003;36(3):147-60.[↩]
- Laurent P, Camps J, About I. Biodentine(TM) induces TGF-beta1 release from human pulp cells and early dental pulp mineralization. International Endodontic Journal 2012;45(5):439-48.[↩]
- Siqueira JF Jr. Microbial causes of endodontic fare-ups. International Endodontic Journal 2003;36(7):453-63. https://www.ncbi.nlm.nih.gov/pubmed/12823700[↩]
- Siqueira J. Aetiology of root canal treatment failure: why well-treated teeth can fail. International Endodontic Journal 2001;34(1):1-10. https://www.ncbi.nlm.nih.gov/pubmed/11307374[↩]
- Torabinejad M, Hong CU, McDonald F, Pitt Ford TR. Physical and chemical properties of a new root-end filling material. Journal of Endodontics 1995;21(7):349-53. https://www.ncbi.nlm.nih.gov/pubmed/7499973[↩]
- Chong BS. Chapter 8. A surgical alternative. In: Chong BS editor(s). Managing Endodontic Failure in Practice. Chicago: Quintessence Publishing Co Ltd, 2004:123-47.[↩]





{kind=link}