Contents
Thrombolysis
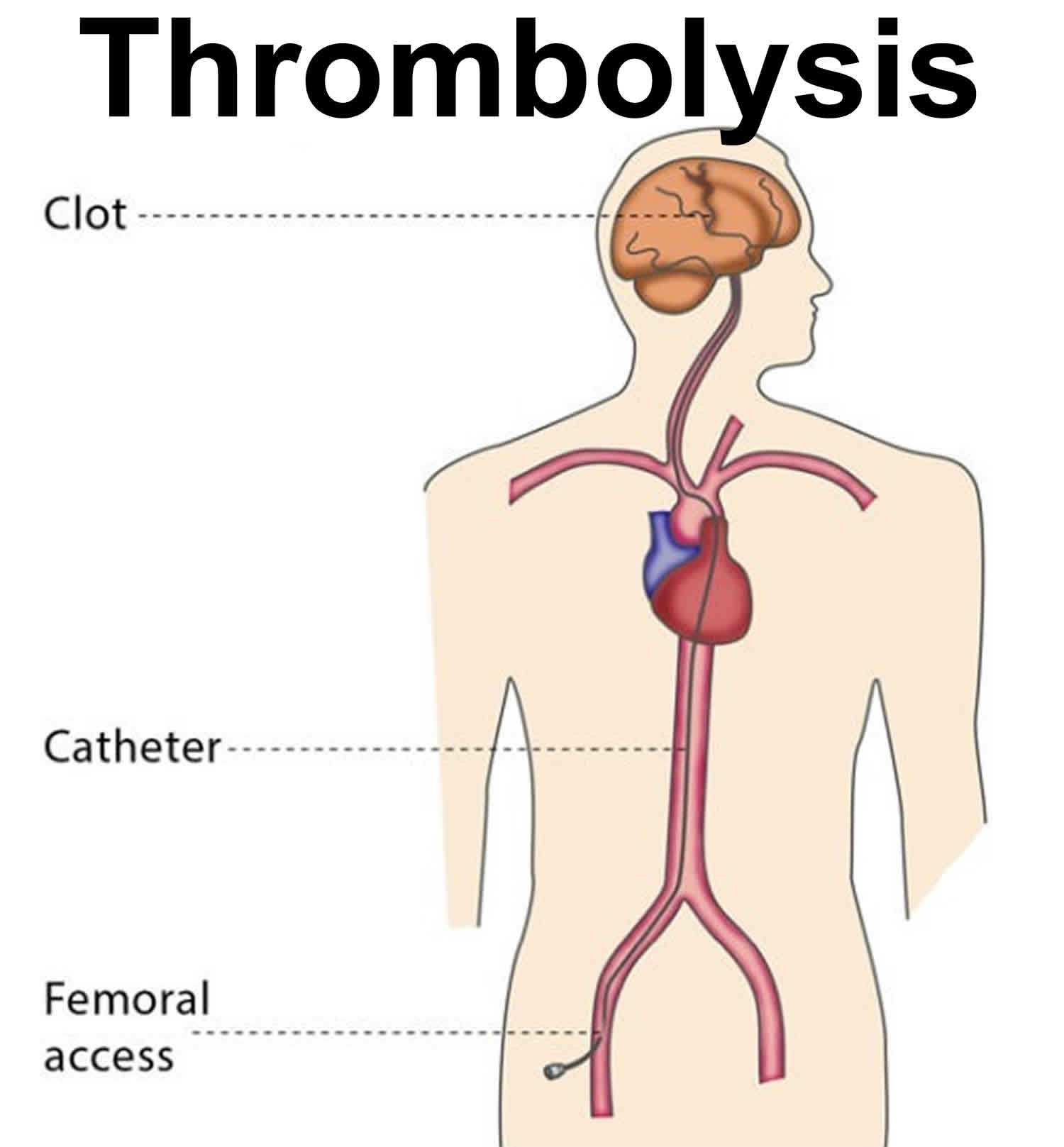
Thrombolysis is a procedure which uses drugs to break up or dissolve blood clots. The medications used in thrombolysis are called thrombolytic agents. Thrombolysis is most commonly performed to treat a blood clot in the lower limbs, which causes acute limb ischemia (restricted blood flow in the affected limb), leading to pain in affected area. Thrombolysis can also be used to treat blood clots in organs such as the liver or kidney, as well as treating restricted blood flow in the small intestine due to inflammation or an injury, massive pulmonary embolism (a blood clot in main artery of a lung) or stroke. Thrombolytic medicines are approved for the emergency treatment of stroke and heart attack. The most commonly used drug for thrombolytic therapy is tissue plasminogen activator (tPA), but other drugs can do the same thing. Heart attacks and strokes are medical emergencies. The sooner treatment with thrombolytics begins, the better the chance for a good outcome.
Ideally, you should receive thrombolytic medicines within the first 30 minutes after arriving at the hospital for treatment.
Thrombolysis is performed to remove the blood clot and to prevent the vein or artery from becoming permanently blocked and restricting blood flow to a limb or organ. Restricted blood flow leads to acute symptoms of pain, a lack of pulse, paleness, paresthesia (when a limb ‘falls asleep’) and paralysis, as well as the possibility of permanent complications such as tissue necrosis (the death of tissue cells in your body).
You will probably also need medication to prevent blood clots forming as well as a thrombectomy, for which you will be under strict observation for a 24-48 hours with several angiographic follow ups.
You will also be treated for the underlying condition which caused the thrombus (blood clot), which may be a heart rhythm disorder or a small blood clot caused by deep venous thrombosis (DVT).
Tissue plasminogen activator (tPA) is classified as a serine protease (enzymes that cleave peptide bonds in proteins) and is thus one of the essential components of the dissolution of blood clots. Tissue plasminogen activator (tPA) primary function includes catalyzing the conversion of plasminogen to plasmin, the primary enzyme involved in dissolving blood clots.
Recombinant biotechnology has allowed tissue plasminogen activator to be manufactured in labs, and these synthetic products are called recombinant tissue plasminogen activator (rtPA). Examples of these drugs include alteplase, reteplase, and tenecteplase. These drugs have undergone various modifications to amplify their pharmacokinetic and pharmacodynamic properties, especially to prolong their short half-life in the circulation and further increase their fibrin specificity, to prevent an unwanted fibrinolytic state.
Heart attacks
A blood clot can block the arteries to your heart. This can cause a heart attack, when part of the heart muscle dies due to a lack of oxygen being delivered by the blood. Thrombolytics work by dissolving a major clot quickly. This helps restart blood flow to the heart and helps prevent damage to the heart muscle. Thrombolytics can stop a heart attack that would otherwise be larger or potentially deadly. Outcomes are better if you receive a thrombolytic drug within 12 hours after the heart attack starts. But the sooner treatment begins, the better the results.
The drug restores some blood flow to the heart in most people. However, the blood flow may not be completely normal and there may still be a small amount of muscle damaged. Further therapy, such as cardiac catheterization with angioplasty and stenting, may be needed.
Your health care provider will base the decisions about whether to give you a thrombolytic medicine for a heart attack on many factors. These factors include your history of chest pain and the results of an ECG test.
Other factors used to determine if you are a good candidate for thrombolysis include:
- Age (older people are at increased risk of complications)
- Gender
- Medical history (including your history of a previous heart attack, diabetes, low blood pressure, or increased heart rate)
Generally, thrombolytics may not be given if you have:
- A recent head injury
- Bleeding problems
- Bleeding ulcers
- Pregnancy
- Recent surgery
- Taken blood thinning medicines such as Coumadin
- Trauma
- Uncontrolled (severe) high blood pressure
Strokes
Most strokes are caused when blood clots move to a blood vessel in the brain and block blood flow to that area. For such strokes (ischemic strokes), thrombolytics can be used to help dissolve the clot quickly. Giving thrombolytics within 3 hours of the first stroke symptoms can help limit stroke damage and disability.
The decision to give the thrombolytic drug is based upon:
- A brain CT scan to make sure there has not been any bleeding
- A physical exam that shows a significant stroke
- Your medical history
As in heart attacks, a clot-dissolving drug isn’t usually given if you have one of the other medical problems listed above.
How does the thrombolysis procedure work?
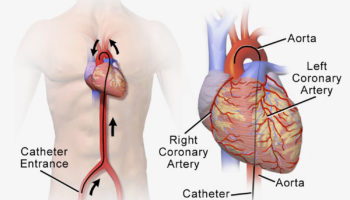
The interventional radiologist will insert a 3 mm plastic tube (called a sheath) into the base of your skull or your groin and will guide the sheath to the blood clot.
Thrombolysis is performed using medications which prevent blood clots from growing (known as lytic substances), which are administered via a catheter into the thrombus. Catheters designed to be used in this treatment have lots of tiny holes. This means that the distribution of lytic substances can be spread out across the catheter and have maximum effect.
Tissue plasminogen activator
Tissue plasminogen activator (tPA) is a thrombolytic (i.e., it breaks up blood clots) formed by aggregation of activated platelets into fibrin meshes by activating plasminogen. More specifically, it cleaves the zymogen plasminogen at its Arg561-Val562 peptide bond to form the serine protease, plasmin 1. Plasmin, an endogenous fibrinolytic enzyme, breaks the cross-links between fibrin molecules, which are the structural support of the blood clot, and its activity is extremely short-lived. This is because alpha 2-antiplasmin, an abundant inhibitor of plasmin, quickly inactivates it and restricts the action of plasmin to the vicinity of the clot.
The following sequence summarizes the action of tissue plasminogen activator (tPA):
- Tissue plasminogen activator attaches to the fibrin on the clot surface.
- It activates the fibrin-bound plasminogen.
- Plasmin is subsequently cleaved from the plasminogen affiliated with the fibrin.
- The molecules of fibrin are broken up by the plasmin, and the clot dissolves.
Plasminogen activator inhibitor 1 (PAI 1) eventually terminates the catalytic activity of tissue plasminogen activator by binding to it, and this inactive complex (PAI 1-bound tissue plasminogen activator) is removed from the circulation by the liver, more specifically via the scavenger receptor, LDL receptor-related protein 1 (LRRP1). In the nervous system, a neuronal-specific inhibitor of Tissue plasminogen activator, neuroserpin, acts similarly to plasminogen activator inhibitor 1 (PAI 1), and the inactive Tissue plasminogen activator-neuroserpin complexes are internalized by the LDL receptor-related protein 1 (LRRP1) for removal from circulation 2.
Indications for the use of tissue plasminogen activator (tPA) include the following:
- Ischemic stroke (most common) in patients presenting to treating facility within 3 hours (4.5 hours in certain, eligible people) after the onset of symptoms 3.
- Myocardial Infarction (heart attack) if there would be a delay of more than 1 to 2 hours before percutaneous transluminal coronary angioplasty 4.
- Pulmonary embolism in massive pulmonary embolisms, causing severe instability due to high pressure on the heart 5.
- Thrombolysis (e.g., deep vein thrombosis or DVT) 6.
Alteplase
Alteplase is the normal, human plasminogen activator and is FDA-approved for the management of patients with ischemic stroke, myocardial infarction with ST-elevation (STEMI), acute massive pulmonary embolism, and those with central venous access devices (CVAD) 7.
Reteplase
Reteplase is a modified form of human tissue plasminogen activator with similar effects but a faster onset and longer duration of action. It is currently FDA-approved for the management of acute myocardial infarction. Preferred over alteplase due to its longer half-life, which allows it to be given as a bolus injection rather than through an infusion like Alteplase 8.
Tenecteplase
Tenecteplase is another modified version of Tissue plasminogen activator with a longer half-life. It is indicated for the management of acute myocardial infarction 9.
Tissue plasminogen activator side effects
- Alteplase: Adverse effects are seen in 1% to 10% of the people who are administered alteplase. The most common adverse effect is bleeding, and the most serious is a stroke. Other side effects include bruising, pulmonary edema, arterial embolism, deep vein thrombosis, orolingual angioedema, intracranial hemorrhage, shock, hypersensitivity, nausea/vomiting, seizure, ischemic stroke, thromboembolism, and sepsis 10.
- Tenecteplase: Adverse effects are seen in greater than 10% of the patients who are administered tenecteplase. The most common is minor bleeding. Other adverse effects include fever, myocardial infarction, reperfusion arrhythmias, nausea/vomiting, edema, allergic reaction, and cholesterol embolization 10.
- Reteplase: As with other tPAs, the most common adverse effect seen with reteplase is bleeding. Other observed adverse effects include reperfusion arrhythmias, hypotension, nausea/vomiting, cardiogenic shock, muscle pain, allergic reaction, a reaction at injection site, anemia, gastrointestinal/urogenital bleed, intracranial hemorrhage, cholesterol embolization 11.
Tissue plasminogen activator contraindications
- Do not administer tissue plasminogen activator (tPA) for the treatment of acute ischemic stroke in the following scenarios:
- If the risk of bleeding and serious complications are greater than the potential benefit of tPA therapy. These include patients with current intracranial hemorrhage (ICH), subarachnoid hemorrhage, and those who have active internal bleeding.
- If the patient underwent recent (less than 3 months) intracranial or intraspinal surgery or suffered a serious head trauma.
- Evidence of intracranial conditions that may possibly increase the risk of bleeding.
- Bleeding diathesis (hemorrhagic diathesis).
- Patients with severe uncontrolled hypertension 12.
- Do not administer tissue plasminogen activator (tPA) in the management of acute myocardial infarction or pulmonary embolism in the following:
- If the risk of bleeding is greater than any potential benefit. This includes active internal bleeding; patients with a recent history of stroke.
- Recent (within three months) intracranial or intraspinal surgery or serious head trauma.
- Presence of intracranial pathologies that may increase the risk of bleeding.
- Bleeding diathesis (hemorrhagic diathesis).
- Current severe uncontrolled hypertension 12.
- Do not administer tPA in any patient who had a hypersensitivity reaction to a previous dose of tPA (urticarial or anaphylactic reactions) 12.
Monitoring During Therapy with tPA
- Perform regular neurologic assessment on the patient.
- Check thoroughly for major or minor bleeding.
- Continuously monitor the blood pressure of the patient.
- Check for the signs and symptoms of ICH.
- Check for the signs of orolingual angioedema.
- Discontinue tPA infusion and order an emergency CT scan if the patient develops a severe headache, severe hypertension, nausea/vomiting, or has a worsening neurologic examination.
- If a hypersensitivity reaction occurs in the patient, stop the tPA administration and immediately initiate supportive therapy with antihistamines and corticosteroids 13.
Drug Interactions
Monitor closely with any drug that causes anticoagulation as there is an increased risk of bleeding.
- Defibrotide: Through pharmacodynamic synergism, defibrotide increases the effects of tPA drugs and is thus contraindicated.
- Prothrombin complex concentrate, human: This can cause pharmacodynamic antagonism of the tPA drugs.
- Apixaban: Apixaban and tPA drugs increase anticoagulation and can lead to an increased bleeding risk.
- Nitroglycerin: This could decrease the serum concentration of tPA drugs.
- Salicylates: These could enhance the toxic effects of thrombolytic drugs. Monitor therapy as there is an increased risk of bleeding.
Monitoring After Therapy with tPA
- Follow up the patient to monitor for any neurologic deterioration.
- Check for any major or minor bleeding.
- Monitor and strictly control blood pressure.
- Order a follow-up CT scan or MRI at least 24 hours before initiating anticoagulants or antiplatelet agents.
- Continue to monitor for hypersensitivity and signs of orolingual angioedema
- 13.
Reversing tPA toxicity
The drug used to reverse tPA toxicity is aminocaproic acid, an FDA-approved drug for the management of acute bleeding caused by increased fibrinolytic activity. It acts as an effective inhibitor for proteolytic enzymes like plasmin, which is the primary enzyme responsible for fibrinolysis 14.
Thrombolysis contraindications
Thrombolytics are not given to someone who is having a stroke that involves bleeding in the brain. They could worsen the stroke by causing increased bleeding.
Generally, thrombolytics may not be given if you have:
- Any source of active hemorrhage
- A recent head injury
- Cerebral bleed
- Cerebral mass
- Bleeding problems
- Bleeding ulcers
- Prior ischemic stroke
- Pregnancy
- Recent ulcer in the gastrointestinal tract
- Recent surgery
- Major abdominal or pelvic surgery
- Recent brain/spine surgery
- Taken blood thinning medicines such as Coumadin
- Trauma
- Uncontrolled (severe) high blood pressure
- Vascular deformation
Thrombolysis complications
Minor risks of thrombolysis include the risk of bruising at the puncture site in your neck or groin, or in the affected limb.
The major risks tend to be due to the devices used in the procedure, such as the risk of the blood clot travelling deeper into the artery or vein or an injury to the affected area during the treatment.
In rare cases, the patient experiences bleeding in the skull due to the thrombolysis – if this occurs, the treatment will be stopped immediately.
Bleeding is the most common complication of thrombolysis. It can be life threatening.
Minor bleeding from the gums or nose can occur in approximately 25% of people who receive the drug. Bleeding into the brain occurs approximately 1% of the time. This risk is the same for both stroke and heart attack patients.
If thrombolysis are felt to be too dangerous, other possible treatments for clots causing a stroke or heart attack include:
- Removal of the clot (thrombectomy)
- A procedure to open narrowed or blocked blood vessels that supply blood to the heart or the brain
Catheter directed thrombolysis
Pulmonary embolism (PE) is the third most common cause of cardiovascular death in the United States of America 15. Pulmonary embolism is one of the most common causes of death worldwide. Most patients die within the first few hours of presentation, making an early diagnosis and treatment paramount to survival. Pulmonary embolism is categorized as small (low risk), sub-massive (intermediate risk) and massive (high risk). Catheter-directed thrombolysis is one of the newest treatment options for pulmonary embolism 16. The SEATLE II study was a prospective multicenter study which revealed that ultrasound-guided catheter-directed, low-dose thrombolysis decreased right ventricular dilation, lessened pulmonary hypertension, reduced clot burden, and minimized intracranial bleeding in acute massive and submassive pulmonary embolism 17.
Pulmonary embolism usually arises from deep veins of the lower extremities and/or pelvis. Dislodgement of the DVT or parts of the DVT can result in the blood clot traveling up the venous system through the right heart and lodging in the pulmonary vasculature. The pulmonary trunk, main pulmonary artery, segmental or sub-segmental branches are all common locations for a pulmonary embolus to lodge. Once lodged in the pulmonary vasculature depending on the size and location of the pulmonary embolism, this can cause heart strain and decreased oxygenation. The most serious consequence of pulmonary embolus is when the clot blocks the right and left pulmonary artery, blocking the right heart outflow tract. This is called a saddle embolus. Saddle embolus usually results in death, but in the event of survival immediate medical therapy should be administered to reduce adverse events. catheter directed thrombolysis was developed to provide direct thrombolytic therapy to the site of the pulmonary embolus.
Catheter directed thrombolysis indications
Currently catheter directed thrombolysis for the management of pulmonary embolism is only suggested for massive pulmonary embolism as a class IIa and level B recommendation according to the American College of Cardiology and American Heart Association. While the use of systemic thrombolytic therapy in patients with submassive pulmonary embolism is not recommended by the guidelines, cardiopulmonary collapse or the development of critical hypotension is the only case exemption 18. Catheter directed thrombolysis has a considerable advantage over systemic thrombolytic therapy due to the lower the risk of bleeding. Some centers divide the category of submassive pulmonary embolism into intermediate high risk and intermediate low risk. At these facilities, those patients who fall into the intermediate high risk are considered for catheter directed thrombolysis. Those patients determined to be in the intermediate low risk are not considered for thrombolytic therapy. All patients considered for thrombolytic therapy should have a low bleeding risk.
Catheter directed thrombolysis contraindications
Though thrombolysis is administered locally during catheter directed thrombolysis for pulmonary embolism, the thrombolysis disperses systemically. Systemic dispersion of thrombolytic therapy is the cause for many of the severe complications of catheter directed thrombolysis. Therefore, contraindications to catheter directed thrombolysis are a prior ischemic stroke, cerebral bleed, cerebral mass, vascular deformation, recent ulcer in the gastrointestinal tract, recent brain/spine surgery, major abdominal or pelvic surgery, or any source of active hemorrhage 18. Those with contraindications to catheter directed thrombolysis therapy are usually contraindicated for systemic thrombolytic. These patient are treated with anticoagulant therapy, antiplatelet therapy, or supportive care.
Thrombolysis procedure
The current guidelines recommend all hospitals treating pulmonary embolisms to setup a pulmonary embolism response team 19. The pulmonary embolism response team team is a multidisciplinary team made up of cardiologist and pulmonologist specialized. They work together to treat pulmonary embolism and to determine the best treatment plan and achieve the best outcomes. Once catheter directed thrombolysis is chosen as a management course, the practitioners should counsel the patient regarding the risk and benefits of the procedure. A trained physician knowledgeable in the risk and benefits should have this discussion. The patient should give consent. An anesthesiologist should evaluate the patient to determine the need, mode, and safety of anesthetic delivery. An imaging specialist or structuralist may consult for further recommendations on the size and burden of pulmonary embolism. It is a level I recommendation to utilize this multidisciplinary approach. Studies have shown the pulmonary embolism response team team can reduce adverse events 20. A swift and early diagnosis followed by early treatment is the key to successful thrombolysis of pulmonary embolism.
Before initiation of the thrombolysis procedure, the practitioner should inspect the thrombolysis catheter delivery system thoroughly to ensure all pieces are present. They may administer intravenous antibiotics before the procedure to prevent infection. Thrombolysis procedure requires a fully operating catheterization laboratory. Healthcare professionals should use proper sterile techniques including sterile drapes, gloves, and gowns.
Technique
Catheter directed thrombolysis procedure begins by obtaining vascular access. Insertion of the introducer needle into the desired venous system is the first step. Then one threads a guide-wire through the needle and up through the right heart into the pulmonary system close to the thrombus. Using fluoroscopic guidance, the infusion catheter is passed over the guide-wire and across the treatment site. Note that radiopaque marker bands can be found at each end of the catheter to enhance catheter placement. Once positioned correctly, remove the guide-wire. Gently insert the ultrasonic core into the catheter until the fittings lock into place. Thrombolysis can now be administered. The thrombolysis exits the catheter through side holes while saline exits through the distal tip. Activating the ultrasonic waves enhances the dispersion of the thrombolysis medication. When the therapy is complete, remove the ultrasonic core and replace the guide-wire inside the catheter. Next, remove the catheter leaving the guide-wire in place. Finally, remove the guide-wire and apply a compression device to the access site.
Catheter directed thrombolysis complications
There are several possible complications from catheter directed thrombolysis for pulmonary embolus. One of the most common and most feared complications being hemorrhagic stroke which can be debilitating 21. Other common complications include vascular access related injury, pulmonary hemorrhage, retroperitoneal hemorrhage, cardiogenic shock, perforation or dissection of the pulmonary artery, arrhythmias, right-sided valvular regurgitation, pericardial tamponade, and contrast-induced nephropathy 22.
- Jilani TN, Siddiqui AH. Tissue Plasminogen Activator. [Updated 2019 Mar 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507917[↩]
- Collen D. Molecular mechanism of action of newer thrombolytic agents. J. Am. Coll. Cardiol. 1987 Nov;10(5 Suppl B):11B-15B[↩]
- Gravanis I, Tsirka SE. Tissue-type plasminogen activator as a therapeutic target in stroke. Expert Opin. Ther. Targets. 2008 Feb;12(2):159-70[↩]
- Rogers SD, Riemersma LB, Clements SD. Tissue plasminogen activator: an evaluation of clinical efficacy in acute myocardial infarction. Pharmacotherapy. 1987;7(4):111-21[↩]
- Niedermeyer J, Meissner E, Fabel H. [Thrombolytic therapy in pulmonary embolism. Indications and therapeutic strategies]. Z Gesamte Inn Med. 1993 Jun-Jul;48(6-7):332-43[↩]
- Sharifi M, Bay C, Nowroozi S, Bentz S, Valeros G, Memari S. Catheter-directed thrombolysis with argatroban and tPA for massive iliac and femoropopliteal vein thrombosis. Cardiovasc Intervent Radiol. 2013 Dec;36(6):1586-1590[↩]
- Demaerschalk BM, Kleindorfer DO, Adeoye OM, Demchuk AM, Fugate JE, Grotta JC, Khalessi AA, Levy EI, Palesch YY, Prabhakaran S, Saposnik G, Saver JL, Smith EE., American Heart Association Stroke Council and Council on Epidemiology and Prevention. Scientific Rationale for the Inclusion and Exclusion Criteria for Intravenous Alteplase in Acute Ischemic Stroke: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2016 Feb;47(2):581-641[↩]
- Wang W, Zhao X, Ren Y, Qiao P. Therapeutic effect evaluation of reteplase on acute pulmonary embolism. Pak J Pharm Sci. 2018 May;31(3):899-905[↩]
- Saran RK, Sethi R, Nagori M. “Tenecteplase–the best among the equals.”. Indian Heart J. 2009 Sep-Oct;61(5):454-8[↩]
- Logallo N, Novotny V, Assmus J, Kvistad CE, Alteheld L, Rønning OM, Thommessen B, Amthor KF, Ihle-Hansen H, Kurz M, Tobro H, Kaur K, Stankiewicz M, Carlsson M, Morsund Å, Idicula T, Aamodt AH, Lund C, Næss H, Waje-Andreassen U, Thomassen L. Tenecteplase versus alteplase for management of acute ischaemic stroke (NOR-TEST): a phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol. 2017 Oct;16(10):781-788[↩][↩]
- Rosenberg G, Steiner I. And why not thrombolysis in the ambulance (at least for some)? Neurology. 2016 Jul 12;87(2):214-9[↩]
- Parker S, Ali Y. Changing contraindications for t-PA in acute stroke: review of 20 years since NINDS. Curr Cardiol Rep. 2015 Oct;17(10):81[↩][↩][↩]
- Cheng JW, Zhang XJ, Cheng LS, Li GY, Zhang LJ, Ji KX, Zhao Q, Bai Y. Low-Dose Tissue Plasminogen Activator in Acute Ischemic Stroke: A Systematic Review and Meta-Analysis. J Stroke Cerebrovasc Dis. 2018 Feb;27(2):381-390.[↩][↩]
- Golembiewski J. Antifibrinolytic Use in the Perioperative Setting: Aminocaproic Acid and Tranexamic Acid. J. Perianesth. Nurs. 2015 Dec;30(6):560-563[↩]
- Brown KN, Gupta N. Catheter Directed Thrombolysis Of Pulmonary Embolism. [Updated 2019 Jan 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536918[↩]
- Dilektasli AG, Demirdogen Cetinoglu E, Acet NA, Erdogan C, Ursavas A, Ozkaya G, Coskun F, Karadag M, Ege E. Catheter-Directed Therapy in Acute Pulmonary Embolism with Right Ventricular Dysfunction: A Promising Modality to Provide Early Hemodynamic Recovery. Med. Sci. Monit. 2016 Apr 15;22:1265-73[↩]
- Piazza G, Hohlfelder B, Jaff MR, Ouriel K, Engelhardt TC, Sterling KM, Jones NJ, Gurley JC, Bhatheja R, Kennedy RJ, Goswami N, Natarajan K, Rundback J, Sadiq IR, Liu SK, Bhalla N, Raja ML, Weinstock BS, Cynamon J, Elmasri FF, Garcia MJ, Kumar M, Ayerdi J, Soukas P, Kuo W, Liu PY, Goldhaber SZ., SEATTLE II Investigators. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv. 2015 Aug 24;8(10):1382-92[↩]
- Furfaro D, Stephens RS, Streiff MB, Brower R. Catheter-directed Thrombolysis for Intermediate-Risk Pulmonary Embolism. Ann Am Thorac Soc. 2018 Feb;15(2):134-144[↩][↩]
- Giri JS, Piazza G. A midterm report card for pulmonary embolism response teams. Vasc Med. 2018 Feb;23(1):72-74[↩]
- Porres-Aguilar M, Anaya-Ayala JE, Heresi GA, Rivera-Lebron BN. Pulmonary Embolism Response Teams: A Novel Approach for the Care of Complex Patients With Pulmonary Embolism. Clin. Appl. Thromb. Hemost. 2018 Nov 19;:1076029618812954[↩]
- Bloomer TL, El-Hayek GE, McDaniel MC, Sandvall BC, Liberman HA, Devireddy CM, Kumar G, Fong PP, Jaber WA. Safety of catheter-directed thrombolysis for massive and submassive pulmonary embolism: Results of a multicenter registry and meta-analysis. Catheter Cardiovasc Interv. 2017 Mar 01;89(4):754-760[↩]
- Mostafa A, Briasoulis A, Telila T, Belgrave K, Grines C. Treatment of Massive or Submassive Acute Pulmonary Embolism With Catheter-Directed Thrombolysis. Am. J. Cardiol. 2016 Mar 15;117(6):1014-20.[↩]




{kind=link}