Contents
What is ALT test
ALT is short for alanine aminotransferase is also called SGPT (Serum Glutamic-Pyruvic Transaminase) or GPT (Glutamic-Pyruvic Transaminase) or alanine transaminase, which is an enzyme found mostly in the cells of the liver and kidney. Much smaller amounts of ALT are also found in the heart and muscles. ALT blood test measures the level of ALT (alanine aminotransferase) in the blood. Normal ALT are less than 36U/L [7 to 55 units per liter (U/L)]. This result is typical for adult men. Normal results vary from laboratory to laboratory and might be slightly different for women and children (neonate < 50 U/L).
The function of ALT (alanine aminotransferase) is to convert alanine, an amino acid found in proteins, into pyruvate, an important intermediate in cellular energy production. In healthy individuals, ALT levels in the blood are low. When the liver is damaged, ALT is released into the blood, usually before more obvious signs of liver damage occur, such as jaundice. This makes ALT (alanine aminotransferase) a useful test for early detection of liver damage.
A number of conditions can cause damage to liver cells, resulting in an increase in ALT. The ALT (alanine aminotransferase) test is most useful in detecting damage due to hepatitis or as a result of drugs or other substances that are toxic to the liver. ALT (alanine aminotransferase) is more specific for hepatocellular damage than is AST (aspartate aminotransferase) or LD (lactate dehydrogenase) and remains elevated for longer, due to its longer half-life.
ALT is commonly tested in conjunction with aspartate aminotransferase (AST), another liver enzyme, as part of a liver panel. Both ALT and AST levels usually rise whenever the liver is being damaged, although ALT is more specific for the liver and, in some cases, may be the only one of the two to be increased. An AST/ALT ratio may be calculated to aid in distinguishing between different causes and severity of liver injury and to help distinguish liver injury from damage to heart or muscles. The AST/ALT ratio is typically > 1 in alcoholic liver disease and AST/ALT < 1 in non-alcoholic liver disease.
ALT may be elevated in skeletal muscle disease but the degree of elevation is much less than for AST (aspartate aminotransferase) and CK (creatine kinase).
The Liver
Your liver is the largest organ inside your body, weighing about 1.4 kg (3 pounds) in an average adult. Your liver is a vital organ located in the upper right-hand side of the abdominal cavity, just inferior to the diaphragm in the right superior part of the abdominal cavity and under your right ribs just beneath your right lung – filling much of the right hypochondriac and epigastric regions and extending into the left hypochondriac region.
Your liver is partially surrounded by the ribs, and extends from the level of the fifth intercostal space to the lower margin of the right rib cage, which protects this highly vascular organ from blows that could rupture it. Your liver is shaped like a wedge, the wide base of which faces right and the narrow apex of which lies just inferior to the level of the left nipple. The reddish-brown liver is well supplied with blood vessels.
Your liver is involved in many important functions in the body. Your liver helps to process your body’s nutrients, manufactures bile to help digest fats, produces many important proteins such as blood clotting factors, and breaks down potentially toxic substances into harmless ones that the body can use or excrete.
Figure 1. Location of the human liver
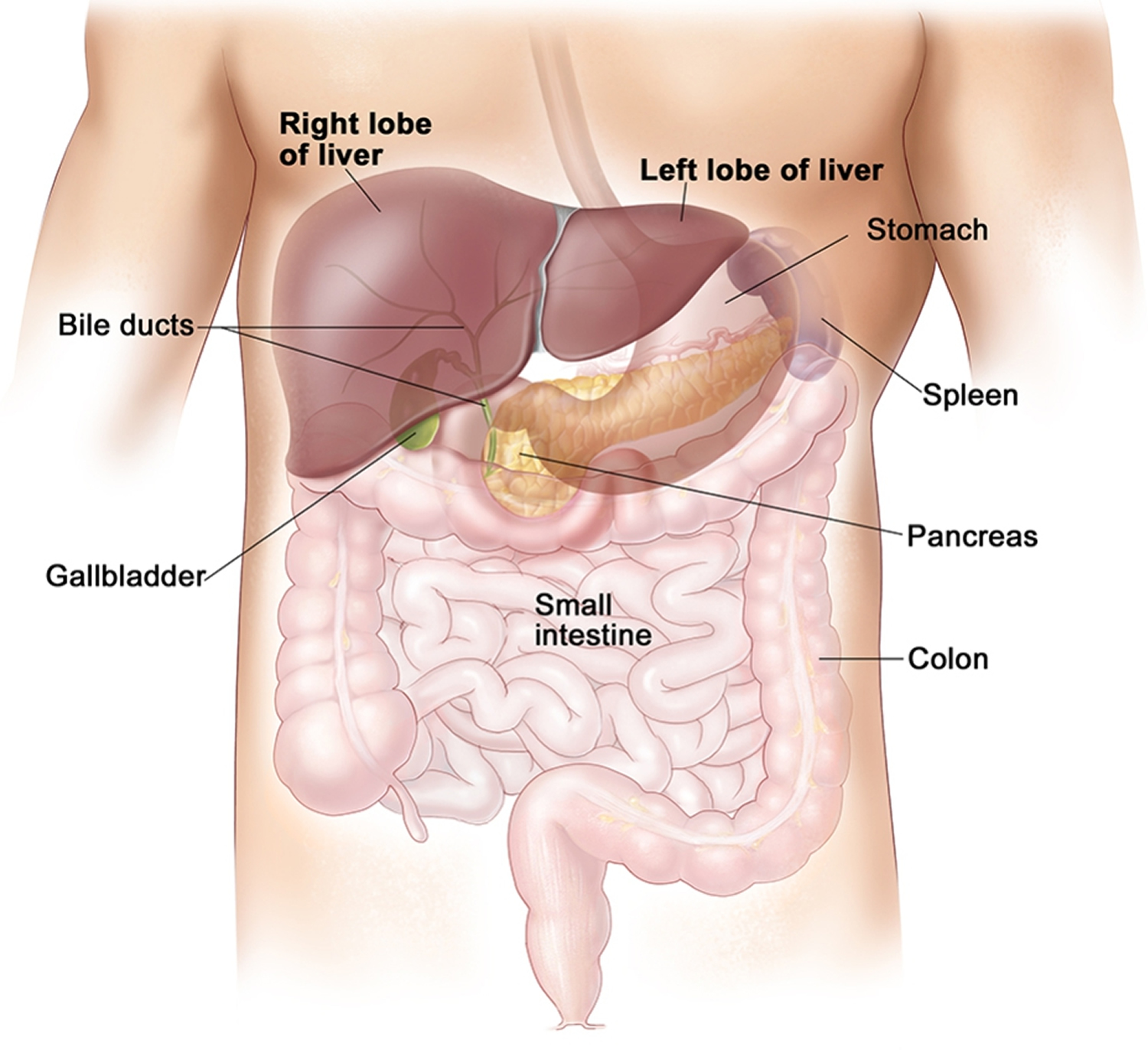
Figure 2. Liver lobule
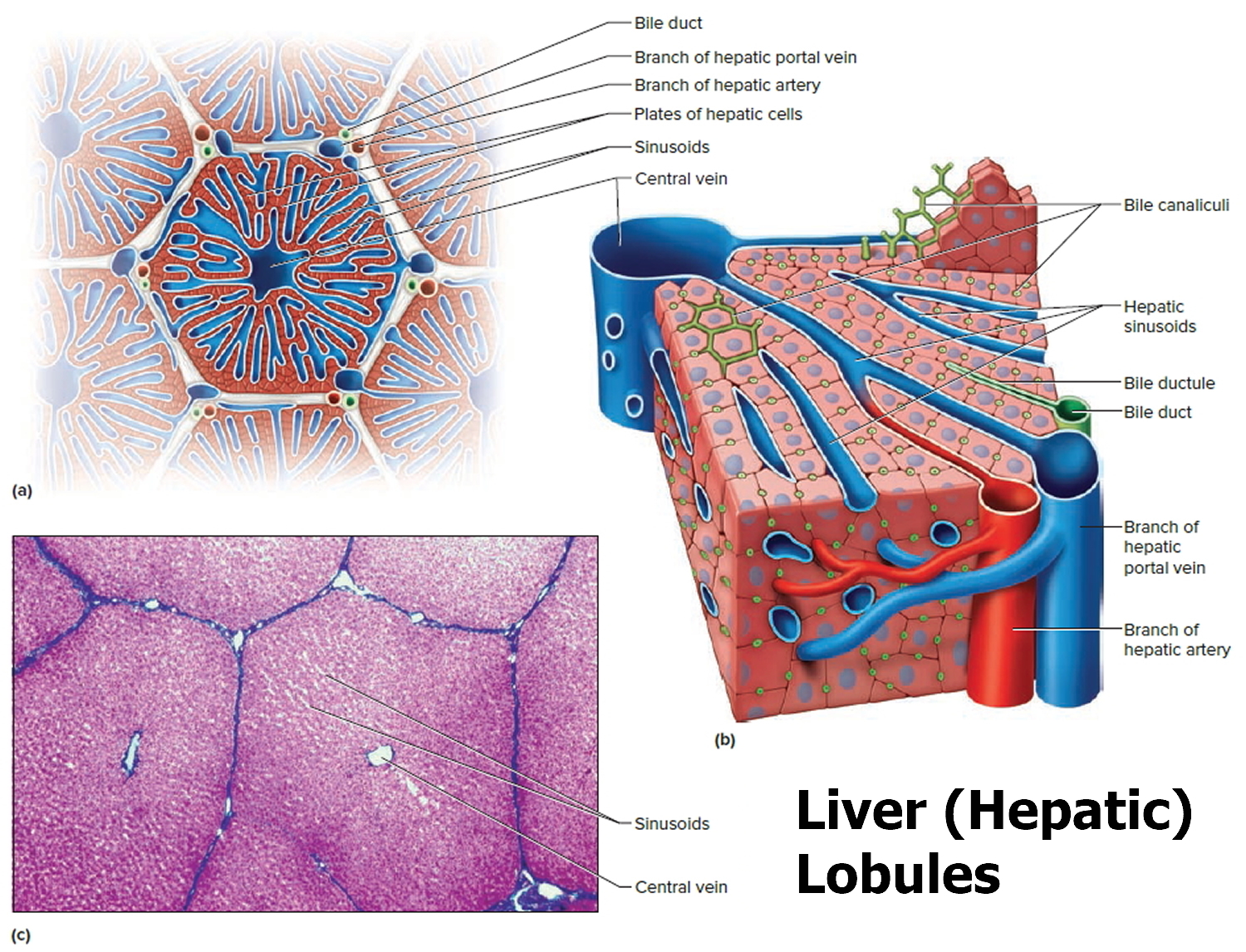
Footnote: (a) Cross section of a hepatic lobule. (b) Enlarged longitudinal section of a hepatic lobule. (c) Light micrograph of hepatic lobules in cross section.
Liver functions
Amazingly versatile, your liver performs over 500 functions. Its digestive function is to produce bile, a green alkaline liquid that is stored in the gallbladder and secreted into the duodenum. Bile salts emulsify fats in the small intestine; that is, they break up fatty nutrients into tiny particles, just as dish detergent breaks up a pool of fat drippings in a roasting pan. These smaller particles are more accessible to digestive enzymes from the pancreas. The liver also performs many metabolic functions and you cannot live without your liver:
- Picks up glucose from nutrient-rich blood returning from the alimentary canal and stores this carbohydrate as glycogen for subsequent use by the body.
- Processes fats and amino acids and stores certain vitamins.
- Detoxifies many poisons and drugs in the blood.
- Makes the blood proteins.
- It breaks down and stores many of the nutrients absorbed from the intestine that your body needs to function. Some nutrients must be changed (metabolized) in the liver before they can be used for energy or to build and repair body tissues.
- It makes most of the clotting factors that keep you from bleeding too much when you are cut or injured.
- It secretes bile into the intestines to help absorb nutrients (especially fats).
- It breaks down alcohol, drugs, and toxic wastes in the blood, which then pass from the body through urine and stool.
Almost all of these functions are carried out by a type of cell called a hepatocyte or simply a liver cell.
The liver carries on many important metabolic activities. The liver plays a key role in carbohydrate metabolism by helping maintain concentration of blood glucose within the normal range. Liver cells responding to the hormone insulin lower the blood glucose level by polymerizing glucose to glycogen. Liver cells responding to the hormone glucagon raise the blood glucose level by breaking down glycogen to glucose or by converting noncarbohydrates into glucose.
The liver’s effects on lipid metabolism include oxidizing (breaking down) fatty acids at an especially high rate; synthesizing lipoproteins, phospholipids, and cholesterol; and converting excess portions of carbohydrate molecules into fat molecules. The blood transports fats synthesized in the liver to adipose tissue for storage.
Other liver functions concern protein metabolism. They include deaminating amino acids; forming urea; synthesizing plasma proteins such as clotting factors; and converting certain amino acids into other amino acids.
The liver also stores many substances, including glycogen, iron, and vitamins A, D, and B12. In addition, macrophages in the liver help destroy damaged red blood cells and phagocytize foreign antigens. The liver also removes toxic substances such as alcohol and certain drugs from blood (detoxification).
Table 1. Major Functions of the Liver
| General Function | Specific Function |
| Carbohydrate metabolism | Polymerizes glucose to glycogen; breaks down glycogen to glucose; converts noncarbohydrates to glucose |
| Lipid metabolism | Oxidizes fatty acids; synthesizes lipoproteins, phospholipids, and cholesterol; converts excess portions of carbohydrate molecules into fats |
| Protein metabolism | Deaminates amino acids; forms urea; synthesizes plasma proteins; converts certain amino acids into other amino acids |
| Storage | Stores glycogen, iron, and vitamin A, vitamin D and vitamin B12 |
| Blood filtering | Removes damaged red blood cells and foreign substances by phagocytosis |
| Detoxification | Removes toxins from blood |
| Secretion | Produces and secretes bile |
The Bile
Bile is a yellowish-green liquid continuously secreted from hepatic cells. In addition to water, bile contains bile salts, bile pigments (bilirubin and biliverdin), cholesterol, and electrolytes. Of these, bile salts are the most abundant and are the only bile components that have a digestive function.
Bile pigments are breakdown products of hemoglobin from red blood cells and are normally secreted in the bile.
Jaundice, a yellowing of the skin and mucous membranes due to accumulation of bile pigment, has several causes. In obstructive jaundice bile ducts are blocked, perhaps by gallstones or tumors. In hepatocellular jaundice the liver is diseased, as in cirrhosis or hepatitis. In hemolytic jaundice red blood cells are destroyed too rapidly, as happens with an incompatible blood transfusion or a blood infection.
Regulation of Bile Release
Normally bile does not enter the duodenum until cholecystokinin stimulates the gallbladder to contract. The intestinal mucosa releases this hormone in response to proteins and fats in the small intestine. The hepatopancreatic sphincter usually remains contracted until a peristaltic wave in the duodenal wall approaches it. Then the sphincter relaxes, and bile is squirted into the duodenum.
Functions of Bile Salts
Bile salts aid digestive enzymes. Bile salts affect fat globules (clumped molecules of fats) much like a soap or detergent would affect them. That is, bile salts break fat globules into smaller droplets that are more soluble in water. This action, called emulsification, greatly increases the total surface area of the fatty substance. The resulting fat droplets disperse in water. Fat-splitting enzymes (lipases) can then digest the fat molecules more effectively. Bile salts also enhance absorption of fatty acids, cholesterol, and the fat-soluble vitamins A, D, E, and K.
Low levels of bile salts result in poor lipid absorption and vitamin deficiencies.
What does ALT mean in a blood test
The alanine aminotransferase (ALT) test is typically used to detect liver injury. It is often ordered in conjunction with aspartate aminotransferase (AST) as part of a liver panel or comprehensive metabolic panel (CMP) to screen for and/or help diagnose liver disease.
ALT is an enzyme found mostly in the cells of the liver and kidney. When the liver is damaged, ALT is released into the blood. This makes ALT a useful test for early detection of liver damage.
AST and ALT are considered to be two of the most important tests to detect liver injury, although ALT is more specific to the liver than is AST. Sometimes AST is compared directly to ALT and an AST/ALT ratio is calculated. This ratio may be used to distinguish between different causes of liver damage and to help recognize heart or muscle injury.
ALT values are often compared to the results of other tests such as alkaline phosphatase (ALP), total protein, and bilirubin to help determine which form of liver disease is present.
ALT is often used to monitor the treatment of persons who have liver disease, to see if the treatment is working, and may be ordered either by itself or along with other tests for this purpose.
When is ALT test ordered?
ALT may be ordered as part of a comprehensive metabolic panel when a person has a routine health examination.
A healthcare practitioner usually orders an ALT test (and several others) to evaluate a person who has signs and symptoms of a liver disorder. Some of these signs and symptoms may include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
ALT may also be ordered, either by itself or with other tests, for people who are at an increased risk for liver disease since many people with mild liver damage will have no signs or symptoms. Even without other symptoms, ALT will be increased with mild liver damage. Some examples include:
- Persons who have a history of known or possible exposure to hepatitis viruses
- Those who are heavy drinkers
- Individuals whose families have a history of liver disease
- Persons who take drugs that might damage the liver
- Persons who are overweight and/or have diabetes
When ALT is used to monitor the treatment of people who have liver disease, it may be ordered on a regular basis during the course of treatment to determine whether the therapy is effective.
Alt test range
ALT blood test normal range: Normal ALT are less than 36U/L [7 to 55 units per liter (U/L)]. This result is typical for adult men. Normal results vary from laboratory to laboratory and might be slightly different for women and children (neonate < 50 U/L).
A low level of ALT in the blood is expected and is normal.
ALT blood test high
Liver disease is the most common reason for higher than normal levels of ALT.
A shot or injection of medicine into the muscle tissue, or strenuous exercise, may increase ALT levels. And many drugs may raise ALT levels by causing liver damage in a very small percentage of patients taking the drug. This is true of both prescription drugs and some “natural” health products. Be sure to tell your healthcare provider about all of the drugs and/or health supplements you are taking.
Very high levels of ALT (more than 10 times normal) are usually due to acute hepatitis, sometimes due to a viral infection. In acute hepatitis, ALT levels usually stay high for about 1-2 months but can take as long as 3-6 months to return to normal. Levels of ALT may also be markedly elevated (sometimes over 100 times normal) as a result of exposure to drugs or other substances that are toxic to the liver or in conditions that cause decreased blood flow (ischemia) to the liver.
ALT levels are usually not as high in chronic hepatitis, often less than 4 times normal. In this case, ALT levels often vary between normal and slightly increased, so the test may be ordered frequently to see if there is a pattern. Other causes of moderate increases in ALT include obstruction of bile ducts, cirrhosis (usually the result of chronic hepatitis or bile duct obstruction), heart damage, alcohol abuse, and with tumors in the liver.
ALT is often performed together with a test for AST or as part of a liver panel. For more about ALT results in relation to other liver tests, see the Liver Panel article.
In most types of liver diseases, the ALT level is higher than AST and the AST/ALT ratio will be low (less than 1). There are a few exceptions; the AST/ALT ratio is usually greater than 1 in alcoholic hepatitis, cirrhosis, and with heart or muscle injury and may be greater than 1 for a day or two after onset of acute hepatitis.
What conditions other than liver problems can cause increased ALT?
ALT is more specific for the liver than AST and so is much less affected by conditions affecting other parts of the body. Nevertheless, injury to organs other than the liver, such as the heart and skeletal muscle, can cause elevations of ALT. For example, small increases may be seen with skeletal muscle damage or heart attacks.
What other tests may be performed to help determine the cause of liver damage?
After a thorough physical exam and evaluation of a person’s medical history, there are several other tests that may be performed as follow up depending on what is suspected to be the cause of liver damage. Some of these include:
- Tests for hepatitis A, hepatitis B, and hepatitis C
- Testing for exposure to drugs and other substances toxic to the liver (see Drug Abuse Testing and Emergency and Overdose Drug Testing)
- Ethanol level
- Copper and ceruloplasmin for Wilson disease
- Iron tests and genetic tests for hereditary hemochromatosis
A liver biopsy may be performed to help determine the cause of liver injury and to evaluate the extent of liver damage.
How is the sample collected for testing?
A blood sample is drawn from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Viral hepatitis (mainly hepatitis B virus [HBV] and hepatitis C virus [HCV] infections)
Viral hepatitis infection is the leading or secondary cause of ALT elevation in populations worldwide 1. ALT activity is an indicator of liver injury in patients with acute and chronic viral hepatitis 2.
With respect to hepatitis B virus (HBV) infection, ALT elevation is often observed in the process of the cytolytic immune response (acute phase) and the following ineffective HBV clearance (chronic phase) 3. Liaw et al 3 have described a fluctuation in ALT activity during the process of HBV infection. ALT activity is a crucial reference indicator in treatment selection and the evaluation of prognosis in patients infected with HBV 3. Nevertheless, controversy exists and Lai et al 45 reported significant fibrosis and inflammation in 37% of patients infected with HBV and persistently normal ALT levels 4. Unlike hepatitis B virus (HBV) infections, the ALT level is less meaningful for diagnosis and prognosis of hepatitis C virus (HCV) treatment. More patients infected with hepatitis C virus (HCV) progress to chronic hepatitis with persistent hepatocyte injury 2. Greater than 6 in 10 of common hepatitis C virus (HCV) carriers have normal ALT levels or mildly elevated ALT levels (< 2 times the upper limit of normal) with rare hepatic histologic lesions confirmed by liver biopsy 5. Recently, Ruhl et al 6 suggested that lowering the upper limit of normal of the ALT level (29 IU/L for men and 22 IU/L for women) was the best cut-off value to identify hepatitis C virus (HCV) infectors in the US population with a high prevalence of hepatitis C virus (HCV) infection. Otherwise, the HCV RNA titer is closely linked to the ALT elevation. Cathy et al 7 reported that approximately 68% of patients with positive HCV-RNA levels have ALT elevations in asymptomatic blood donors who tested positive for antibodies to the HCV (anti-HCV).
Alcohol intake
Excessive alcohol intake is another cause of ALT elevation in the general population. In an Italian population, 45.6% of altered liver tests have been attributed to excessive alcohol intake (≥28 g/day) 35, while in a US national population survey, excessive alcohol (>1 time/day) is a crucial cause of ALT elevation, second only to hepatitis C virus (HCV) infection 1, however, alcohol intake might be a time-and dose-dependent covariate that influences ALT activity. Short-term and light alcohol consumption was not shown to induce significant ALT elevation in adults 8, however, ethnicity differences exist regarding the biological consequences of alcohol abuse 9. In a UK study based on alcohol abusers from different areas worldwide, adults from South Asia were shown to be more susceptible to alcohol-related liver damage and the ALT levels were higher than in European alcohol abusers 10. Indeed, the effect of mild alcohol intake on ALT activity can be distinguished from binge drinking. Moderate alcohol intake does not contribute to significant ALT elevation, especially in a normal weight population, due to its potential effect on improvement of insulin sensitivity 11.
Some medications
Pratt et al 12 listed the medications that might cause ALT elevations. A randomized controlled trial indicated that the estimated odds ratios of ALT elevation in active treatment groups (including acetaminophen, paracetamol, hydromorphone+acetaminophen, morphine+acetaminophen, and oxycodone+acetaminophen) were 2.57-3.08 compared to the placebo group involving 343 healthy participants, even at the recommended dose 13. Another commonly used medication, statins, also causes mild ALT elevation 14. The mechanism underlying statin-associated ALT elevation is still unclear. Some scholars have suggested that the ALT elevation in statin users is attributed to cholesterol reduction in hepatocytes and co-morbid conditions, rather than liver damage or dysfunction 15. Therefore, the long-term medications should be carefully considered when faced with an unexplained ALT elevation. Pratt et al 16 also indicated that cessation of drug treatment is the best way to confirm the relationship between a drug and ALT elevation.
Coffee consumption
Of note, coffee intake might be a protective factor against ALT elevation. In NHANES III, there was a 50% and 70% decrease in ALT elevation amongst participants who consumed >2 cups of coffee/day or ≥373 mg of caffeine, respectively, compared to participants who did not consume coffee 17. Lee et al 18 attributed the protective effects of caffeine to antioxidant activity.
Non-alcoholic fatty liver disease (NAFLD)
NAFLD is a spectrum of clinical and pathologic changes, from fatty liver alone to steatohepatitis 19. Non-alcoholic fatty liver disease (NAFLD) is common in asymptomatic patients, and the prevalence ranges from 10 to 24% worldwide 20. Considered as a manifestation of the metabolic syndrome in liver 21, NAFLD has been strongly associated with ALT activity in previous studies 22. Non-alcoholic fatty liver disease (NAFLD) is the common cause of unexplained mild ALT elevation 23. NAFLD in asymptomatic patients is often serendipitously detected by liver biochemistry testing during routine health check-ups 24. Similar to the increasing prevalence of obesity 25, NAFLD is increasing and becoming a major health burden 26. In spite of the non-linear correlation between the degree of ALT elevation and the histologic severity of NAFLD 27, a mild ALT elevation is largely attributed to NAFLD. When faced with an unexplained ALT elevation (without viral hepatitis or a history of excessive alcohol intake), NAFLD should be considered in the differential diagnosis.
Autoimmune hepatitis
Autoimmune hepatitis is a less common liver disease than NAFLD 28, and the mechanism underlying autoimmune hepatitis is still unknown 29. ALT elevation is an available auxiliary measurement in the diagnosis of autoimmune hepatitis 30.
Moreover, ALT activity is a crucial indicator in detecting the effect of immunosuppressive treatment, prognosis, and long-term survival in patients with autoimmune hepatitis. In a study based on 84 Japanese autoimmune hepatitis patients, a persistently low ALT level (≤40 U/l) was the threshold value that was associated with improved prognosis 31. Another study also showed an association between persistent ALT elevation and poor survival in 69 autoimmune hepatitis patients 32. ALT is considered to be a crucial non-invasive marker of inflammation in patients with autoimmune hepatitis 33.
Non-hepatic cause of high ALT
Metabolic covariates
Except for apparent causes, such as viral hepatitis, alcohol intake, and some medications, the so-called unexplained causes of ALT elevation in some previous studies have mainly been attributed to metabolic syndrome 34. Similar to the pandemic of obesity 35, metabolic syndrome presents as a series of metabolic disorders, including glucose intolerance, central obesity, dyslipidaemia, and hypertension, has caused worldwide concern in the most recent decades.
Compared to the obvious cause of ALT elevation referred above, ALT elevation caused by metabolic syndrome is mild and neglected. In a cross-sectional study, the ALT level in metabolic syndrome patients, as defined by the National Cholesterol Education Programme Adult Treatment Panel III (NCEP-ATP-III) criteria, was approximately 30% higher than participants without metabolic syndrome in a male population from south China 36. This impact of metabolic syndrome on ALT elevation, however, is progressive and cumulative with a linear trend 37. Even within upper limit of normal values, which did not consider the impact of metabolic syndrome and are higher than the updated values, the increasing prevalence of metabolic syndrome is still correlated with the increasing ALT level in the general population. In a community-based Korean population, the odds ratios for metabolic syndrome in the highest quintiles of ALT were 7.1-fold higher than the reference quintile in men and 2.1-fold higher in women 38. All of the enrolled participants were selected within the upper limit of normal values (the upper limit of normal value is 30 U/l for males and 19 U/l for females) 38. Another Korean national health survey also showed a significantly increased prevalence of metabolic syndrome components, as defined by NCEP-ATP-III criteria, in the subgroup with high-normal ALT levels 39. With respect to the lipoproteins, ALT was shown to be stably and significantly associated with intermediate-density lipoprotein (IDL) and apolipoprotein B (ApoB) after adjusting various covariates in different models 40. These associations were commonly attributed to the stable and independent effects of insulin resistance and fatty liver disease in subjects with ALT elevations 41.
In addition, the impact of metabolic syndrome components on ALT activities varies to some extent. These distinguishing effects emerged after logistic regression using all of the metabolic syndrome components as covariates. The impact of the individual metabolic syndrome components on ALT elevation was disproportionate 42. The body mass index (BMI) and waist circumstance, representing the central obesity component of metabolic syndrome, were more closely linked to the ALT elevation 43, although, the underlying mechanism has not been elucidated. The possible explanation is that obesity, especially abdominal fat, is potentially involved in the visceral adipose deposition that causes hepatotoxic fatty acids 44. In a US national population-based study 45, BMI lost significance when evaluating the association between obesity and ALT abnormities after adjusting for leptin, insulin, and triglyceride concentrations, rather than the waist circumstance, which was representative of the visceral adipose deposition, indicating that BMI might be an intrinsic association between obesity and ALT abnormalities. Another viewpoint was that the obesity-ALT elevation association was modulated by insulin resistance. In a national health survey from a Korean adolescent population, the prevalence of insulin resistance status was positively correlated with the degree of obesity 46. The odds ratio of obesity-induced ALT elevation was significantly decreased after adjusting the homeostasis model as an index of insulin resistance status 47. Despite the ill-defined intrinsic mechanism, central obesity is the crucial metabolic syndrome component that most influences the ALT level in general population.
Celiac disease and muscle injury
Chronic ALT elevation is also found in several non-hepatic disorders, such as celiac disease and muscle injury 48. The intrinsic mechanism between celiac disease is not known. Approximately 40-57% of patients with celiac disease have abnormal liver tests 49. Celiac disease patients with elevated ALT levels should be treated with gluten-free diet; doing so will restore ALT levels to normal in 75-95% of patients within 6 months 49. It is well known that ALT elevation is often observed in patients with muscle necrosis 50 and the ALT elevation without evidence of liver disease should be considered due to muscle injury 48. Otherwise, the increased creatine kinaseand lactate dehydrogenase activities that occurred following muscle injury should be assayed to identify the cause of ALT elevation 51.
Hemochromatosis
As an ethnic specific disease mainly occurring in individuals of Nordic descent, hemochromatosis is a less common cause of ALT elevation. HFE gene mutations are the major cause of hereditary hemochromatosis, and iron overload is the main cause of hepatic injury. Measurements of serum ferritin, total iron-binding capacity, and the HEF mutation test can help diagnose hemochromatosis 52. Liver biopsy might be necessary if the aforementioned tests are negative in patients highly suspected to have hemochromatosis to evaluate the status of liver injury from iron overload.
- Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. The American journal of gastroenterology. 2003;98(5):960–967 https://www.ncbi.nlm.nih.gov/pubmed/12809815[↩][↩]
- Rehermann B, Nascimbeni M. Immunology of hepatitis B virus and hepatitis C virus infection. Nature Reviews Immunology. 2005;5(3):215–229 https://www.ncbi.nlm.nih.gov/pubmed/15738952[↩][↩]
- Liaw Y-F, Chu C-M. Hepatitis B virus infection. The Lancet. 2009;373(9663):582–592. https://www.ncbi.nlm.nih.gov/pubmed/19217993[↩][↩][↩]
- Lai M, Hyatt BJ, Nasser I, Curry M, Afdhal NH. The clinical significance of persistently normal ALT in chronic hepatitis B infection. Journal of hepatology. 2007;47(6):760–767 https://www.ncbi.nlm.nih.gov/pubmed/17928090[↩]
- Alter HJ, Conry-Cantilena C, Melpolder J, Tan D, Van Raden M, Herion D, Lau D, Hoofnagle JH. Hepatitis C in asymptomatic blood donors. Hepatology. 1997;26(S3):29S–33S[↩]
- Ruhl CE, Everhart JE. Upper limits of normal for alanine aminotransferase activity in the United States population. Hepatology. 2012;55(2):447–454. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3268908/[↩]
- Conry-Cantilena C, VanRaden M, Gibble J, Melpolder J, Shakil AO, Viladomiu L, Cheung L, DiBisceglie A, Hoofnagle J, Shih JW. Routes of infection, viremia, and liver disease in blood donors found to have hepatitis C virus infection. New England Journal of Medicine. 1996;334(26):1691–1696 https://www.nejm.org/doi/10.1056/NEJM199606273342602[↩]
- Gunji T, Matsuhashi N, Sato H, Iijima K, Fujibayashi K, Okumura M, Sasabe N, Urabe A. Risk factors for serum alanine aminotransferase elevation: A cross-sectional study of healthy adult males in Tokyo, Japan. Digestive and Liver Disease. 2010;42(12):882–887. https://www.ncbi.nlm.nih.gov/pubmed/20457548[↩]
- Stewart SH. Racial and Ethnic Differences in Alcohol-Associated Aspartate Aminotransferase and {gamma}-Glutamyltransferase Elevation. Archives of internal medicine. 2002;162(19):2236 https://www.ncbi.nlm.nih.gov/pubmed/12390068[↩]
- Wickramasinghe S, Corridan B, Izaguirre J, Hasan R, Marjot D. Ethnic differences in the biological consequences of alcohol abuse: a comparison between south Asian and European males. Alcohol and alcoholism. 1995;30(5):675–680 https://www.ncbi.nlm.nih.gov/pubmed/8554653[↩]
- Alatalo PI, Koivisto HM, Hietala JP, Puukka KS, Bloigu R, Niemelä OJ. Effect of moderate alcohol consumption on liver enzymes increases with increasing body mass index. The American journal of clinical nutrition. 2008;88(4):1097–1103 https://www.ncbi.nlm.nih.gov/pubmed/18842799[↩]
- Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. New England Journal of Medicine. 2000;342(17):1266–1271 https://www.nejm.org/doi/full/10.1056/NEJM200004273421707[↩]
- Watkins PB, Kaplowitz N, Slattery JT, Colonese CR, Colucci SV, Stewart PW, Harris SC. Aminotransferase elevations in healthy adults receiving 4 grams of acetaminophen daily. JAMA: the journal of the American Medical Association. 2006;296(1):87–93. https://jamanetwork.com/journals/jama/fullarticle/211014[↩]
- Ford I, Mooijaart SP, Lloyd S, Murray HM, Westendorp RG, de Craen AJ, Packard CJ, Buckley B, Barlow C, Preiss D. The inverse relationship between alanine aminotransferase in the normal range and adverse cardiovascular and non-cardiovascular outcomes. International journal of epidemiology. 2011;40(6):1530–1538[↩]
- Cohen DE, Anania FA, Chalasani N. An assessment of statin safety by hepatologists. The American journal of cardiology. 2006;97(8):S77–S81.[↩]
- Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. New England Journal of Medicine. 2000;342(17):1266–1271[↩]
- Ruhl CE, Everhart JE. Coffee and caffeine consumption reduce the risk of elevated serum alanine aminotransferase activity in the United States. Gastroenterology. 2005;128(1):24–32 https://www.ncbi.nlm.nih.gov/pubmed/15633120[↩]
- Lee K-G, Mitchell A, Shibamoto T. Antioxidative activities of aroma extracts isolated from natural plants. Biofactors. 2000;13(1):173–178. https://www.ncbi.nlm.nih.gov/pubmed/11237179[↩]
- Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, McCullough AJ. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology. 1999;116(6):1413–1419. https://www.ncbi.nlm.nih.gov/pubmed/10348825[↩]
- Angulo P. Nonalcoholic fatty liver disease. New England Journal of Medicine. 2002;346(16):1221–1231 https://www.nejm.org/doi/full/10.1056/NEJMra011775[↩]
- Marchesini G, Brizi M, Bianchi G, Tomassetti S, Bugianesi E, Lenzi M, McCullough AJ, Natale S, Forlani G, Melchionda N. Nonalcoholic fatty liver disease a feature of the metabolic syndrome. Diabetes. 2001;50(8):1844–1850. http://diabetes.diabetesjournals.org/content/50/8/1844.long[↩]
- Liu C-M, Tung T-H, Liu J-H, Chen V, Lin C-H, Hsu C-T, Chou P. A community-based epidemiological study of elevated serum alanine aminotransferase levels in Kinmen, Taiwan. World J Gastroenterol. 2005;11(11):1616–1622. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4305941/[↩]
- Liangpunsakul S, Chalasani N. Unexplained elevations in alanine aminotransferase in individuals with the metabolic syndrome: results from the third National Health and Nutrition Survey (NHANES III) The American journal of the medical sciences. 2005;329(3):111–116. https://www.ncbi.nlm.nih.gov/pubmed/15767815[↩]
- Sass DA, Chang P, Chopra KB. Nonalcoholic fatty liver disease: a clinical review. Digestive diseases and sciences. 2005;50(1):171–180 https://www.ncbi.nlm.nih.gov/pubmed/15712657[↩]
- James PT. Obesity: the worldwide epidemic. Clinics in dermatology. 2004;22(4):276–280. https://www.ncbi.nlm.nih.gov/pubmed/15475226[↩]
- Neuschwander-Tetri BA, Caldwell SH. Nonalcoholic steatohepatitis: summary of an AASLD Single Topic Conference. Hepatology. 2003;37(5):1202–1219.[↩]
- Sonsuz A, Basaranoglu M, Ozbay G. Relationship between aminotransferase levels and histopathological findings in patients with nonalcoholic steatohepatitis. The American journal of gastroenterology. 2000;95(5):1370–1371[↩]
- Muri Boberg K. Prevalence and epidemiology of autoimmune hepatitis. Clinics in liver disease. 2002;6(3):635–647. https://www.ncbi.nlm.nih.gov/pubmed/12362572[↩]
- Krawitt EL. Autoimmune hepatitis. New England Journal of Medicine. 2006;354(1):54–66. https://www.ncbi.nlm.nih.gov/pubmed/16394302[↩]
- Manns MP, Czaja AJ, Gorham JD, Krawitt EL, Mieli-Vergani G, Vergani D, Vierling JM. Diagnosis and management of autoimmune hepatitis. Hepatology. 2010;51(6):2193–2213. https://www.ncbi.nlm.nih.gov/pubmed/20513004[↩]
- Miyake Y, Iwasaki Y, Terada R, Takagi S, Okamaoto R, Ikeda H, Sakai N, Makino Y, Kobashi H, Takaguchi K. Persistent normalization of serum alanine aminotransferase levels improves the prognosis of type 1 autoimmune hepatitis. Journal of hepatology. 2005;43(6):951–957[↩]
- Miyake Y, Iwasaki Y, Terada R, Okamaoto R, Ikeda H, Makino Y, Kobashi H, Takaguchi K, Sakaguchi K, Shiratori Y. Persistent elevation of serum alanine aminotransferase levels leads to poor survival and hepatocellular carcinoma development in type 1 autoimmune hepatitis. Alimentary pharmacology & therapeutics. 2006;24(8):1197–1205[↩]
- Fabbri A, Lenzi M. Non-invasive markers of inflammation in autoimmune hepatitis. Liver International. 2013;33(9):1295–1297.[↩]
- Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. The American journal of gastroenterology. 2003;98(5):960–967. https://www.ncbi.nlm.nih.gov/pubmed/12809815[↩]
- James PT. Obesity: the worldwide epidemic. Clinics in dermatology. 2004;22(4):276–280.[↩]
- Liu Z, Hu Y, Yang X, Tan A, Gao Y, Qin X, Liang Y, Mo Z, Peng T. Combinative analysis of factors influence serum alanine aminotransferase activity in adult male population from southern China. Clinical biochemistry. 2012;45(18):1683–1688 https://www.ncbi.nlm.nih.gov/pubmed/22975640[↩]
- Yun JE, Kim SY, Kang H-C, Lee SJ, Kimm H, Jee SH. Alanine aminotransferase is associated with metabolic syndrome independently of insulin resistance. Circulation journal: official journal of the Japanese Circulation Society. 2010;75(4):964–969. https://www.jstage.jst.go.jp/article/circj/75/4/75_CJ-10-0465/_pdf/-char/en[↩]
- Jeong S, Nam H, Rhee J, Shin J, Kim J, Cho K. Metabolic syndrome and ALT: a community study in adult Koreans. International journal of obesity. 2004;28(8):1033–1038.[↩][↩]
- Suh S-Y, Choi S-E, Ahn H-Y, Yang H-M, Kim Y-I, Sung N-J. The association between normal alanine aminotransferase levels and the metabolic syndrome: 2005 Korean National Health and Nutrition Examination Survey. Metabolism. 2009;58(12):1731–1736.[↩]
- Lorenzo C, Hanley A, Rewers M, Haffner S. The association of alanine aminotransferase within the normal and mildly elevated range with lipoproteins and apolipoproteins: the Insulin Resistance Atherosclerosis Study. Diabetologia. 2013;56(4):746–757 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3615715/[↩]
- Yun JE, Kim SY, Kang H-C, Lee SJ, Kimm H, Jee SH. Alanine aminotransferase is associated with metabolic syndrome independently of insulin resistance. Circulation journal: official journal of the Japanese Circulation Society. 2010;75(4):964–969.[↩]
- Liu Z, Hu Y, Yang X, Tan A, Gao Y, Qin X, Liang Y, Mo Z, Peng T. Combinative analysis of factors influence serum alanine aminotransferase activity in adult male population from southern China. Clinical biochemistry. 2012;45(18):1683–1688[↩]
- Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. The American journal of gastroenterology. 2003;98(5):960–967.[↩]
- Falck-Ytter Y, Younossi ZM, Marchesini G, McCullough AJ. Clinical features and natural history of nonalcoholic steatosis syndromes. In: Seminars in liver disease: 2001; 2001. pp. 15–22.[↩]
- Ruhl CE, Everhart JE. Determinants of the association of overweight with elevated serum alanine aminotransferase activity in the United States. GASTROENTEROLOGY-BALTIMORE THEN PHILADELPHIA- 2003;124(1):71–79.[↩]
- Park SH, Heo NY, Park JH, Kim TO, Yang SY, Moon YS, Kim CH, Suk KT, Kim DJ, Lee HY. Obesity, insulin resistance, and the risk of an elevated alanine aminotransferase activity in the Korean adolescent population. Journal of Pediatric Endocrinology and Metabolism. 2012;25(9-10):945–949.[↩]
- Matthews D, Hosker J, Rudenski A, Naylor B, Treacher D, Turner R. Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28(7):412–419.[↩]
- Nathwani RA, Pais S, Reynolds TB, Kaplowitz N. Serum alanine aminotransferase in skeletal muscle diseases. Hepatology. 2005;41(2):380–382.[↩][↩]
- Novacek G, Miehsler W, Wrba F, Ferenci P, Penner E, Vogelsang H. Prevalence and clinical importance of hypertransaminasaemia in coeliac disease. European journal of gastroenterology & hepatology. 1999;11(3):283–288.[↩][↩]
- Janssen G, Kuipers H, Willems G, Does R, Janssen M, Geurten P. Plasma activity of muscle enzymes: quantification of skeletal muscle damage and relationship with metabolic variables. International journal of sports medicine. 1989;10(S 3):S160–S168.[↩]
- Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. New England Journal of Medicine. 2000;342(17):1266–1271.[↩]
- Powell LW, George DK, McDonnell SM, Kowdley KV. Diagnosis of hemochromatosis. Annals of Internal Medicine. 1998;129(11_Part_2):925–931.[↩]





{kind=link}