Contents
Pancreatic agenesis
Pancreatic agenesis is a very rare developmental disorder of the pancreas in which patients present with neonatal diabetes and pancreatic exocrine (pancreatic enzymes) insufficiency 1, 2, 3, 4. Total agenesis of the pancreas is extremely rare and is incompatible with life. On the other hand, partial pancreatic agenesis also known as pancreatic hypoplasia results from the absence of the ventral or dorsal pancreatic anlage (rudimentary pancreas), with partial agenesis of the dorsal pancreas is thought to be more common than ventral pancreatic agenesis 5. In complete dorsal agenesis of pancreas, the anterior head, neck, body and tail of the pancreas, the duct of Santorini and the minor papilla are absent 6. In partial dorsal agenesis of pancreas, a variable amount of pancreatic tissue is absent but a remnant of the duct of Santorini and the minor papilla are present.
Agenesis of the dorsal pancreas is characterized by the absence of the pancreatic body and tail; if only the pancreatic tail is missing, it is called partial agenesis of the dorsal pancreas. If the pancreatic body is also lacking and only the pancreatic head is present, it is known as complete agenesis of the dorsal pancreas 7.
Many patients with dorsal pancreatic agenesis are asymptomatic, but some patients may present with abdominal pain or bloating and have an increased risk of diabetes mellitus because most of the islet cells are located in the distal pancreas 8, 9, 10, 11.
A diagnosis of a pancreatic agenesis is made based upon identification of characteristic symptoms (if present), a detailed patient history, a thorough clinical evaluation and a variety of specialized tests including advanced imaging techniques (CT, MRI, ERCP and MRCP), blood tests and biochemical tests.
Pancreatic agenesis diagnosis is made by imaging studies revealing the partial absence of the pancreas.
There is no special treatment for agenesis of the dorsal pancreas itself, but sometimes it is necessary to treat the accompanying disease. Pancreatic agenesis management usually involves treatment of the diabetes and exocrine pancreatic insufficiency (EPI), when present.
Figure 1. Normal embryologic development of the pancreas and biliary tree

Footnotes: Drawings showing the normal embryologic development of the pancreas and biliary tree. The ventral pancreatic bud (arrow in A and B) and biliary system arise from the hepatic diverticulum, and the dorsal pancreatic bud (arrowhead in A and B) arises from the dorsal mesogastrium. (C) After clockwise rotation of the ventral bud around the caudal part of the foregut, there is fusion of the dorsal pancreas (located anterior) and ventral pancreas (located posterior). (D) Finally, the ventral and dorsal pancreatic ducts fuse, and the pancreas is predominantly drained through the ventral duct, which joins the common bile duct (CBD) at the level of the major papilla. The dorsal duct empties at the level of the minor papilla.
[Source 5 ]Figure 2. Normal pancreas anatomy
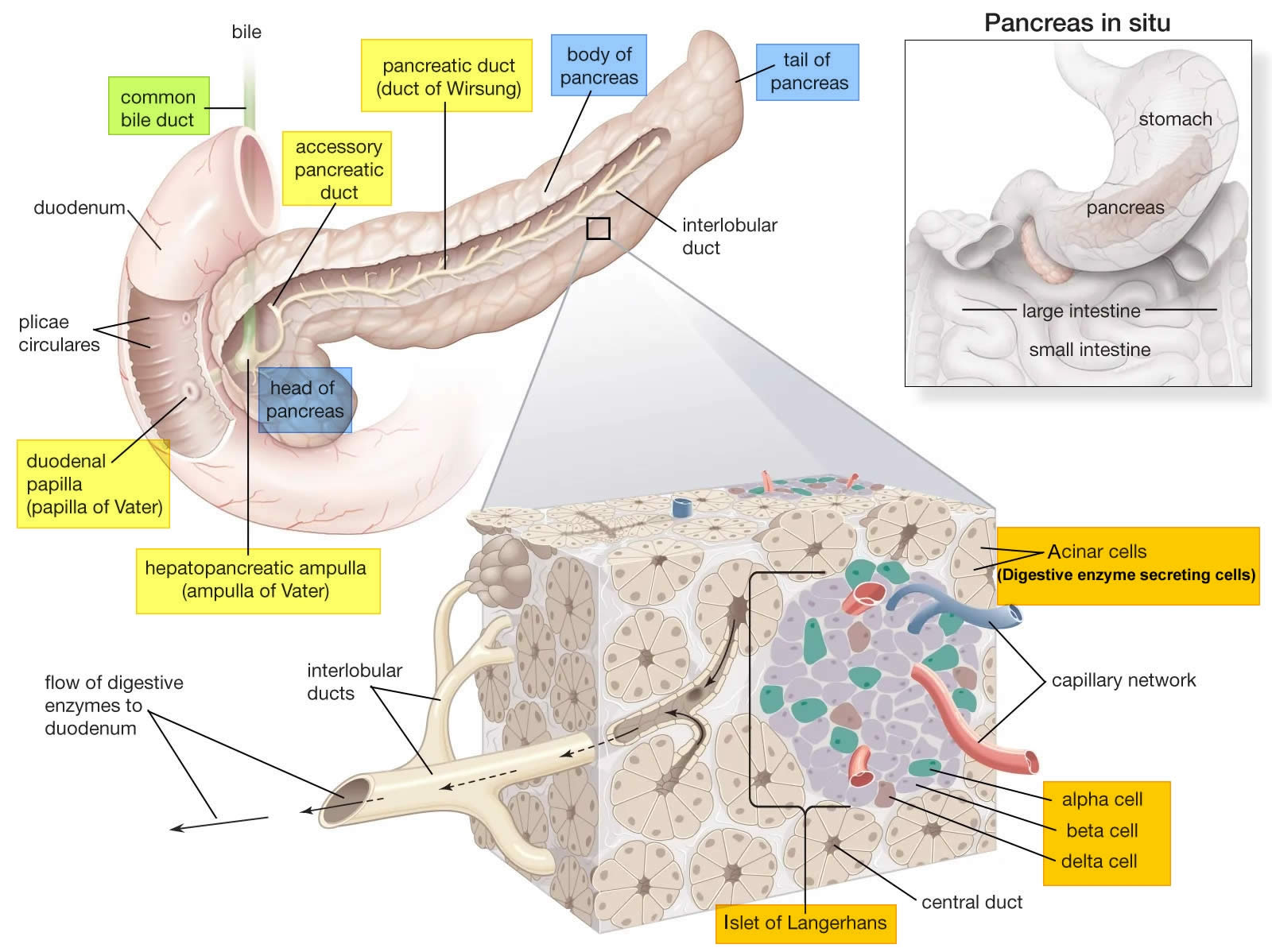
Figure 3. Dorsal agenesis of the pancreas
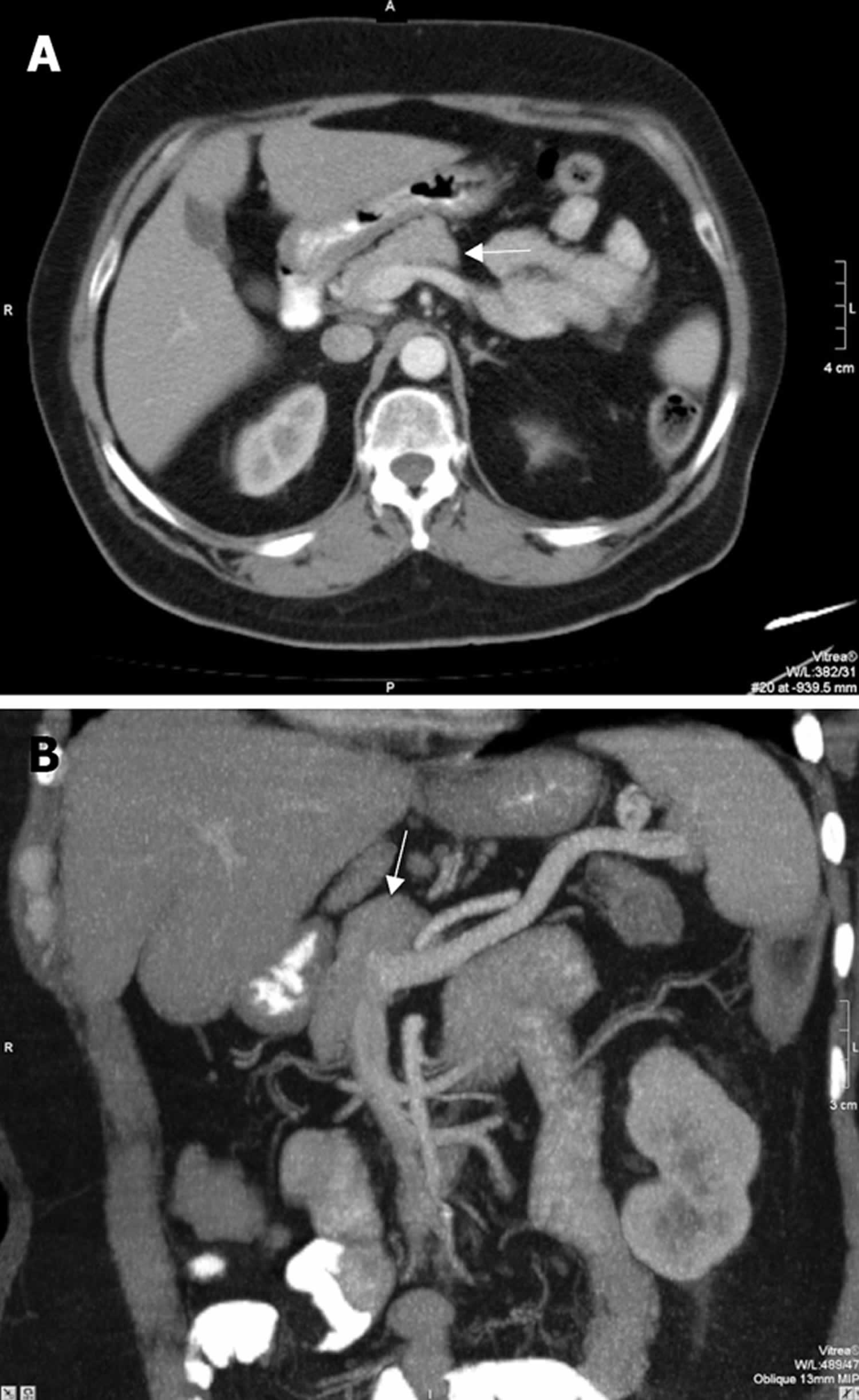
Footnotes: Axial CT (A) and thick-slice coronal oblique Maximum Intensity Projection (MIP) CT (B) images show the pancreatic head (arrow) and the absence of the body and tail of the pancreas. Upper abdominal Magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) were carried out with the suspicion of dorsal pancreatic agenesis. At MRCP, the major pancreatic duct was short and the dorsal pancreatic duct was not visualized.
[Source 10 ]Figure 4. Agenesis of the dorsal pancreas
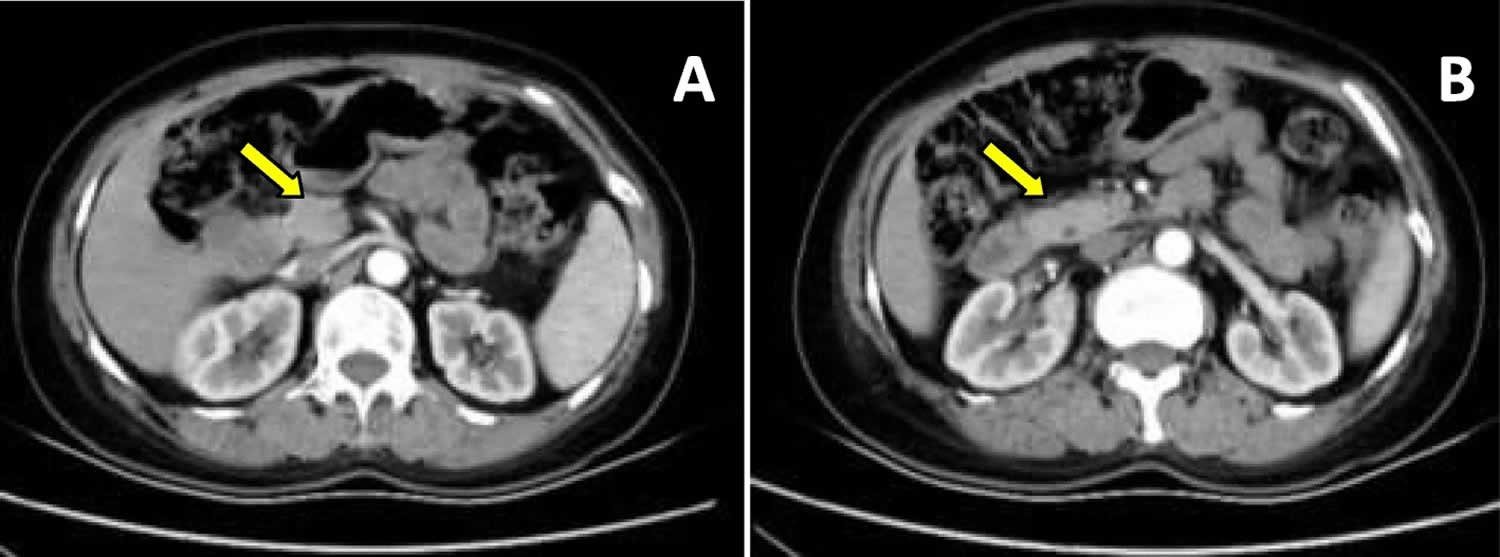
Footnotes: (A) and (B) Axial arterial phase CT image showing the absence of the pancreatic body and tail, without pancreatitis and pancreatic duct dilatation. The arrow show the pancreatic head.
[Source 1 ]Pancreatic agenesis causes
The exact cause of pancreatic agenesis is unknown. Most pancreatic agenesis occur randomly for no apparent reason (sporadically). Rare mutations in the GATA6, HNF1B, PDX1 (IPF1) or PTF1A gene can cause pancreatic agenesis; however, in most cases of pancreatic agenesis the cause is unknown 12, 13, 14, 15, 16, 17, 18, 19. The genetic basis for most instances of pancreatic agenesis is unknown 19, 20, 21, 22, 23. Some individuals may have a genetic predisposition to developing agenesis of pancreas. A person who is genetically predisposed to a disorder carries a gene (or genes) for the disease, but the disorder may not be expressed unless it is triggered or activated under certain circumstances, such as due to certain environmental factors. The genetic or environmental factors associated with pancreatic agenesis are unknown. More research is necessary to determine what specific factors may play a role in the development of pancreatic agenesis.
The pancreas develops by ventral and dorsal endodermal buds. The dorsal bud forms the upper part of the head, body and tail of the pancreas which drains through the Santorini duct. The ventral bud gives rise to the major part of the head and uncinate process which drains through Wirsung duct 24. Pancreatic agenesis results from an embryological failure of the dorsal pancreatic bud to form the body and tail of the pancreas. Partial dorsal pancreatic agenesis may be appreciated as a short, rounded pancreatic head adjacent to the duodenum with absence of the pancreatic neck, body, and tail. With complete agenesis of the dorsal pancreas, the neck, body, and tail of the pancreas, the duct of Santorini, and the minor duodenal papilla are all absent. With partial agenesis of the dorsal pancreas, the size of the body of the pancreas varies, there is a remnant of the duct of Santorini, and the minor duodenal papilla is present. Agenesis of the ventral pancreas and complete agenesis of the pancreas are lethal conditions 25. Dorsal pancreatic agenesis is an extremely rare congenital anomaly.
Failure of the ventral and dorsal pancreatic ducts to fuse is called pancreas divisum. In pancreas divisum, the ventral duct drains into major papilla, while the dorsal duct drains into separate minor papilla 24. Atrophy of the body and the tail of the pancreas secondary to chronic pancreatitis and sparing of the pancreatic head is called pseudo-agenesis 26. Pseudo-agenesis of the pancreas may mimic dorsal pancreatic agenesis. In the differential diagnosis of pseudo-agenesis of the pancreas, histories of previous abdominal pain, pancreatitis, CT scanning and the serum amylase level may be helpful 10. The complete absence of the dorsal duct and demonstration of short ventral duct is important in the diagnosis of the dorsal agenesis of pancreas 10.
Pancreatic agenesis symptoms
Total agenesis of the pancreas is extremely rare and is incompatible with life. Many patients with dorsal pancreatic agenesis are asymptomatic, but some patients may present with abdominal pain and have an increased risk of diabetes mellitus because most of the islet cells are located in the distal pancreas 8, 9, 10, 11.
Dorsal pancreatic agenesis may be associated with other conditions 27, 8, 28, 29, 9:
- Hyperglycemia (high blood sugar level) may be present in a significant proportion of cases (up to 50%)
- Solid pseudopapillary tumor of the pancreas: possible association
- Polysplenia syndrome (the presence of two or more spleens associated to various chest or abdominal congenital abnormalities)
- Pancreatitis
- Intestinal malrotation
In addition, agenesis of the dorsal pancreas associated with other organ malformations has also been reported, including polycystic kidney disease, Kartagener syndrome, multiple splenic deformities, congenital choledochal cysts and biliary atresia 30, 31.
Pancreatic agenesis is commonly associated with other malformations, in particular pancreaticobiliary duct anomalies, leading to acute or chronic pancreatitis, hyperglycemia (50% of cases), or, more rarely, polysplenia. In the majority of cases, patients are diagnosed after reporting abdominal pain. Agenesis of the dorsal pancreas usually manifests as diabetes.
Pancreatic agenesis diagnosis
A diagnosis of a pancreatic agenesis is made based upon identification of characteristic symptoms (if present), a detailed patient history, a thorough clinical evaluation and a variety of specialized tests including advanced imaging techniques (CT, MRI, ERCP and MRCP), blood tests and biochemical tests.
The diagnosis of agenesis of the dorsal pancreas mainly relies on imaging examinations. The complete absence of the dorsal duct and demonstration of short ventral duct is important in the diagnosis of the dorsal bud agenesis. Schnedl supported that the loss of the accessory pancreatic duct and the absence of the tail of the pancreas are conditions for the diagnosis of complete dorsal pancreatic hypoplasia 7. As most agenesis of the dorsal pancreas patients are accidentally discovered because of abdominal pain, they mainly first undergo ultrasound and CT. Ultrasound is affected by the gas in the intestine so it is difficult for this modality to identify the part of pancreas near the splenic vessels; therefore, it is easy for ultrasound to miss the disease. CT and MRI can show the complete or partial disappearance of the pancreatic body and tail 32. The splenic vessels are only visible in that area, and the pancreatic head could be compensated and slightly full. Abdominal CT may not evaluate the pancreatic duct in a detailed fashion. Therefore ERCP or MRCP is necessary for revealing the major and the accessory duct systems and has high value for identifying the complete or incomplete types of agenesis of the dorsal pancreas 33, 32. ERCP is an invasive technique. There is also radiation risk to the patient. MRCP can help the diagnosis of the dorsal pancreatic agenesis noninvasively with no radiation risk 26, 34, 35, 36.
Pancreatic agenesis needs to be differentiated from pancreatic fat infiltration, chronic pancreatitis and pancreatic body and tail atrophy. According to previous literature, agenesis of the dorsal pancreas mostly manifests as the absence of the pancreatic body and tail, the density and morphology of the remaining pancreatic head should be normal, except with compensatory enlargement of pancreatic head. Pancreatic fat infiltration have unique echo characteristics in ultrasound examination and fat signal fraction (FSF) is increased in MRI image, it shows more severe signal suppression than pancreatic tissue on fat suppression imaging; while chronic pancreatitis mostly has pancreatic duct dilatation, pancreas calcification and a lower apparent diffusion coefficient (ADC) values in MRI image, which means an increase in fibrosis 1. The full pancreatic head needs to be differentiated from pancreatic head tumor and pancreatitis. By observing the peripancreatic fat gap, the presence of calcifications and enlarged lymph nodes can help to confirm the diagnosis 1.
Pancreatic agenesis treatment
The severity of pancreatic agenesis depends on the amount of functional pancreatic tissue present. Because pancreatic agenesis may be associated with other malformations, the therapeutic management of individuals with agenesis of the pancreas may require the coordinated efforts of a team of medical professionals, such as physicians who specialize in the diagnosis and treatment of diabetes and pancreatic exocrine insufficiency (endocrinologists), specialists in diagnosis and treatment of gastrointestinal disorder (gastroenterologists), dietitians, surgeons, and other healthcare specialists. Pancreatic agenesis management involves treatment of the diabetes and exocrine deficiency, when present. Dorsal pancreatic agenesis can be started on insulin and a pancreatic enzyme replacement.
Dorsal pancreatic agenesis may be associated with other conditions 27, 8, 28, 29, 9:
- Hyperglycemia (high blood sugar level) may be present in a significant proportion of cases (up to 50%)
- Solid pseudopapillary tumor of the pancreas: possible association
- Polysplenia syndrome (the presence of two or more spleens associated to various chest or abdominal congenital abnormalities)
- Pancreatitis
- Intestinal malrotation
In addition, agenesis of the dorsal pancreas associated with other organ malformations has also been reported, including polycystic kidney disease, Kartagener syndrome, multiple splenic deformities, congenital choledochal cysts and biliary atresia 30, 31.
Approximately half of these patients need insulin therapy. A young woman with agenesis of the dorsal pancreas was reported to have asymptomatic insulin-dependent diabetes mellitus and already had severe retinal lesions at the time of presentation 37. Other studies reported agenesis of the dorsal pancreas combined with ampullary tumors, and the pathological types included cystic adenocarcinoma, solid pseudopapillary tumors, intraductal papillary mucinous neoplasms, pancreatic neuroendocrine tumors (PNETs) and cholangiocarcinoma 38, 39. Some patients with pancreatic pseudocysts were also found 40.The surgical treatment of these types of patients is no different from that for patients with normal pancreatic development, but after pancreatic head resection, due to the lack of the tail of the pancreas, postoperative pancreatic exocrine insufficiency and exogenous insulin dependence will be needed. The association between tumorigenesis and agenesis of the dorsal pancreas is unclear, but chronic pancreatitis caused by the latter is indeed one of the risk factors for cancer 1.
Pancreatic agenesis prognosis
Pancreatic agenesis prognosis is variable and it depends on the quality of treatment received and its associated with other malformations.
Nicolino et al. 41 reported a boy and girl, first cousins born of consanguineous parents, who had permanent neonatal diabetes treated by insulin pump with excellent linear growth thereafter: both patients’ weight, length, and bone age were within normal ranges at 4 years of age. Although there were no clinical signs of exocrine pancreas deficiency, biochemical investigation revealed low or undetectable serum lipase levels, and stool examination showed slightly increased fecal fat excretion, low chymotrypsin, and low elastase levels. In addition, IGF1 levels were very low, and vitamins A, D, E, and K levels were at the lower limits of normal, consistent with some degree of malabsorption 41. Abdominal ultrasound revealed a normal-sized pancreas in the boy, whereas the girl had a well-individualized and homogeneous head of the pancreas, but the body and tail of the pancreas could not be identified 41.
- Mei W, Cao F, Li F. Two cases of agenesis of the dorsal pancreas and a review of the literature. BMC Gastroenterol. 2020 Apr 6;20(1):94. doi: 10.1186/s12876-020-01245-8[↩][↩][↩][↩][↩]
- Wright NM, Metzger DL, Borowitz SM, Clarke WL. Permanent neonatal diabetes mellitus and pancreatic exocrine insufficiency resulting from congenital pancreatic agenesis. Am J Dis Child. 1993 Jun;147(6):607-9. doi: 10.1001/archpedi.1993.02160300013005[↩]
- Doxey BW, Jackson WD, Adler DG. A unique presentation: dorsal agenesis of the pancreas manifesting as pancreatic exocrine insufficiency in the absence of diabetes mellitus in an 8-year-old boy. Dig Dis Sci. 2008 Jul;53(7):2005-6. doi: 10.1007/s10620-007-0094-9[↩]
- Chen R, Hussain K, Al-Ali M, Dattani MT, Hindmarsh P, Jones PM, Marsh P. Neonatal and late-onset diabetes mellitus caused by failure of pancreatic development: report of 4 more cases and a review of the literature. Pediatrics. 2008 Jun;121(6):e1541-7. doi: 10.1542/peds.2007-3543[↩]
- Mortelé KJ, Rocha TC, Streeter JL, Taylor AJ. Multimodality imaging of pancreatic and biliary congenital anomalies. Radiographics. 2006 May-Jun;26(3):715-31. https://doi.org/10.1148/rg.263055164[↩][↩]
- Türkvatan A, Erden A, Türkoğlu MA, Yener Ö. Congenital variants and anomalies of the pancreas and pancreatic duct: imaging by magnetic resonance cholangiopancreaticography and multidetector computed tomography. Korean J Radiol. 2013 Nov-Dec;14(6):905-13. doi: 10.3348/kjr.2013.14.6.905[↩]
- Schnedl WJ, Reisinger EC, Schreiber F, Pieber TR, Lipp RW, Krejs GJ. Complete and partial agenesis of the dorsal pancreas within one family. Gastrointest Endosc. 1995;42(5):485–487. doi: 10.1016/S0016-5107(95)70055-2[↩][↩]
- Schnedl WJ, Piswanger-soelkner C, Wallner SJ et-al. Agenesis of the dorsal pancreas and associated diseases. Dig. Dis. Sci. 2009;54 (3): 481-7. doi:10.1007/s10620-008-0370-3[↩][↩][↩][↩]
- Ulusan S, Bal N, Kizilkilic O et-al. Case report: solid-pseudopapillary tumour of the pancreas associated with dorsal agenesis. Br J Radiol. 2005;78 (929): 441-3. doi:10.1259/bjr/91312352[↩][↩][↩][↩]
- Pasaoglu L, Vural M, Hatipoglu HG, Tereklioglu G, Koparal S. Agenesis of the dorsal pancreas. World J Gastroenterol. 2008 May 14;14(18):2915-6. doi: 10.3748/wjg.14.2915[↩][↩][↩][↩][↩]
- Lång K, Lasson A, Müller MF, Thorlacius H, Toth E, Olsson R. Dorsal agenesis of the pancreas – a rare cause of abdominal pain and insulin-dependent diabetes. Acta Radiol. 2012 Feb 1;53(1):2-4. doi: 10.1258/ar.2011.110480[↩][↩]
- Sellick GS, Barker KT, Stolte-Dijkstra I, Fleischmann C, Coleman RJ, Garrett C, Gloyn AL, Edghill EL, Hattersley AT, Wellauer PK, Goodwin G, Houlston RS. Mutations in PTF1A cause pancreatic and cerebellar agenesis. Nat Genet. 2004 Dec;36(12):1301-5. doi: 10.1038/ng1475[↩]
- Stoffers DA, Zinkin NT, Stanojevic V, Clarke WL, Habener JF. Pancreatic agenesis attributable to a single nucleotide deletion in the human IPF1 gene coding sequence. Nat Genet. 1997 Jan;15(1):106-10. doi: 10.1038/ng0197-106[↩]
- Schwitzgebel VM, Mamin A, Brun T, Ritz-Laser B, Zaiko M, Maret A, Jornayvaz FR, Theintz GE, Michielin O, Melloul D, Philippe J. Agenesis of human pancreas due to decreased half-life of insulin promoter factor 1. J Clin Endocrinol Metab. 2003 Sep;88(9):4398-406. doi: 10.1210/jc.2003-030046[↩]
- Stanescu DE, Hughes N, Patel P, De Leon DD. A novel mutation in GATA6 causes pancreatic agenesis. Pediatr Diabetes. 2015;16(1):67–70. doi: 10.1111/pedi.12111[↩]
- Chao CS, McKnight KD, Cox KL, Chang AL, Kim SK, Feldman BJ. Novel GATA6 mutations in patients with pancreatic agenesis and congenital heart malformations. PLoS One. 2015;10(2):e118449. doi: 10.1371/journal.pone.0118449[↩]
- Haldorsen IS, Vesterhus M, Raeder H, Jensen DK, Sovik O, Molven A, Njolstad PR. Lack of pancreatic body and tail in HNF1B mutation carriers. Diabet Med. 2008;25(7):782–787. doi: 10.1111/j.1464-5491.2008.02460.x[↩]
- Thomas IH, Saini NK, Adhikari A, Lee JM, Kasa-Vubu JZ, Vazquez DM, Menon RK, Chen M, Fajans SS. Neonatal diabetes mellitus with pancreatic agenesis in an infant with homozygous IPF-1 Pro63fsX60 mutation. Pediatr Diabetes. 2009 Nov;10(7):492-6. doi: 10.1111/j.1399-5448.2009.00526.x[↩]
- Allen HL, Flanagan SE, Shaw-Smith C, De Franco E, Akerman I, Caswell R; International Pancreatic Agenesis Consortium; Ferrer J, Hattersley AT, Ellard S. GATA6 haploinsufficiency causes pancreatic agenesis in humans. Nat Genet. 2011 Dec 11;44(1):20-22. doi: 10.1038/ng.1035[↩][↩]
- Nagano T, Mitchell JA, Sanz LA, Pauler FM, Ferguson-Smith AC, Feil R, Fraser P. The Air noncoding RNA epigenetically silences transcription by targeting G9a to chromatin. Science. 2008 Dec 12;322(5908):1717-20. doi: 10.1126/science.1163802[↩]
- Yau D, De Franco E, Flanagan SE, Ellard S, Blumenkrantz M, Mitchell JJ. Case report: maternal mosaicism resulting in inheritance of a novel GATA6 mutation causing pancreatic agenesis and neonatal diabetes mellitus. Diagn Pathol. 2017 Jan 3;12(1):1. doi: 10.1186/s13000-016-0592-1[↩]
- Kishore S, De Franco E, Cardenas-Diaz FL, Letourneau-Freiberg LR, Sanyoura M, Osorio-Quintero C, French DL, Greeley SAW, Hattersley AT, Gadue P. A Non-Coding Disease Modifier of Pancreatic Agenesis Identified by Genetic Correction in a Patient-Derived iPSC Line. Cell Stem Cell. 2020 Jul 2;27(1):137-146.e6. doi: 10.1016/j.stem.2020.05.001[↩]
- Xuan S, Borok MJ, Decker KJ, Battle MA, Duncan SA, Hale MA, Macdonald RJ, Sussel L. Pancreas-specific deletion of mouse Gata4 and Gata6 causes pancreatic agenesis. J Clin Invest. 2012 Oct;122(10):3516-28. doi: 10.1172/JCI63352[↩]
- Fukuoka K, Ajiki T, Yamamoto M, Fujiwara H, Onoyama H, Fujita T, Katayama N, Mizuguchi K, Ikuta H, Kuroda Y, Hanioka K. Complete agenesis of the dorsal pancreas. J Hepatobiliary Pancreat Surg. 1999;6(1):94-7. doi: 10.1007/s005340050090[↩][↩]
- Voldsgaard P, Kryger-Baggesen N, Lisse I. Agenesis of pancreas. Acta Paediatr. 1994 Jul;83(7):791-3. doi: 10.1111/j.1651-2227.1994.tb13144.x[↩]
- Gold RP. Agenesis and pseudo-agenesis of the dorsal pancreas. Abdom Imaging. 1993;18(2):141-4. doi: 10.1007/BF00198051[↩][↩]
- Dorsal pancreatic agenesis. https://radiopaedia.org/articles/dorsal-pancreatic-agenesis?lang=us[↩][↩]
- Maier M, Wiesner W, Mengiardi B. Annular pancreas and agenesis of the dorsal pancreas in a patient with polysplenia syndrome. AJR Am J Roentgenol. 2007;188 (2): W150-3. doi:10.2214/AJR.05.1859[↩][↩]
- Low JP, Williams D, Chaganti JR. Polysplenia syndrome with agenesis of the dorsal pancreas and preduodenal portal vein presenting with obstructive jaundice–a case report and literature review. Br J Radiol. 2011;84 (1007): e217-20. doi:10.1259/bjr/27680217[↩][↩]
- Demir MK, Furuncuoglu Y. Coincidence of Polysplenia, Kartagener syndrome, dorsal pancreas agenesis, and polycystic kidney disease in an adult. Eurasian J Med. 2017;49(2):152–154. doi: 10.5152/eurasianjmed.2017.17067[↩][↩]
- Jeong JH, Kim GH, Song GA, Lee DG, Moon JY, Cheong JH, Kim S. Polysplenia syndrome with congenital agenesis of dorsal pancreas presenting as acute pancreatitis and the role of endoscopic ultrasonography in its diagnosis. Korean J Gastroenterol. 2012;60(1):47–51. doi: 10.4166/kjg.2012.60.1.47[↩][↩]
- Macari M, Giovanniello G, Blair L, Krinsky G. Diagnosis of agenesis of the dorsal pancreas with MR pancreatography. AJR Am J Roentgenol. 1998;170(1):144–146. doi: 10.2214/ajr.170.1.9423620[↩][↩]
- Pasaoglu L, Vural M, Hatipoglu HG, Tereklioglu G, Koparal S. Agenesis of the dorsal pancreas. World J Gastroenterol. 2008;14(18):2915–2916. doi: 10.3748/wjg.14.2915[↩]
- Balakrishnan V, Narayanan VA, Siyad I, Radhakrishnan L, Nair P. Agenesis of the dorsal pancreas with chronic calcific pancreatitis. case report, review of the literature and genetic basis. JOP. 2006 Nov 10;7(6):651-9.[↩]
- Uygur-Bayramiçli O, Dabak R, Kiliçoglu G, Dolapçioglu C, Oztas D. Dorsal pancreatic agenesis. JOP. 2007 Jul 9;8(4):450-2.[↩]
- DU J, Xu GQ, Xu P, Jin EY, Liu Q, Li YM. Congenital short pancreas. Chin Med J (Engl). 2007 Feb 5;120(3):259-62.[↩]
- Liang K, Ou X, Huang X, Lan Q. Agenesis of the dorsal pancreas: a rare cause of insulin-dependent diabetes without abdominal pain: case report. Medicine (Baltimore) 2018;97(9):e46. doi: 10.1097/MD.0000000000010046[↩]
- Nassif S, Ponchiardi C, Sachs T. Pancreatic Neuroendocrine Tumor in the Setting of Dorsal Agenesis of the Pancreas. Case Rep Gastrointest Med. 2016;2016:3801962. doi: 10.1155/2016/3801962[↩]
- Erotokritou A, Gerharz CD, Sagir A. Agenesis of dorsal pancreas associated with pancreatic neuroendocrine tumor: a case report and review of the literature. J Med Case Rep. 2018 Jun 30;12(1):185. doi: 10.1186/s13256-018-1733-9[↩]
- Suh PS, Lee JH, Yu JS, Hee KJ, Kim B, Kim HJ, Huh J, Kim JK, Lee D. Three cases of pancreatic pseudocysts associated with dorsal pancreatic agenesis. Radiol Case Rep. 2019;14(1):79–82. doi: 10.1016/j.radcr.2018.09.023[↩]
- Nicolino M, Claiborn KC, Senée V, Boland A, Stoffers DA, Julier C. A novel hypomorphic PDX1 mutation responsible for permanent neonatal diabetes with subclinical exocrine deficiency. Diabetes. 2010 Mar;59(3):733-40. doi: 10.2337/db09-1284[↩][↩][↩]





{kind=link}