Contents
- Mesenteric venous thrombosis
- Mesenteric vein anatomy
- Mesenteric venous thrombosis causes
- Mesenteric venous thrombosis pathophysiology
- Mesenteric venous thrombosis symptoms
- Mesenteric venous thrombosis complications
- Mesenteric venous thrombosis diagnosis
- Mesenteric venous thrombosis differential diagnosis
- Mesenteric venous thrombosis treatment
- Mesenteric venous thrombosis prognosis
Mesenteric venous thrombosis
Mesenteric venous thrombosis is a rare life-threatening gastrointestinal and vascular emergency where a blood clot formed within the superior or inferior mesenteric vein or its branches, accounting for 5% to 15% of mesenteric ischemic events 1, 2, 3, 4, 5, 6, 7, 8, 9. Because the superior mesenteric vein (SMV) is involved in more than 90% of cases of mesenteric vein thrombosis, whereas the inferior mesenteric vein is only implicated in up to 11% of cases, people often use the terms “mesenteric venous thrombosis” and “superior mesenteric vein thrombosis” interchangeably.
Doctors classify mesenteric venous thrombosis according to how the symptoms appear.
- Acute mesenteric venous thrombosis: Symptoms begin suddenly, within 24 to 72 hours of blood clot formation. About 60% to 80% of all cases of mesenteric venous thrombosis are acute. Acute thrombosis can quickly damage your intestines since your blood has no way to reach them. The blood clot blocks its path.
- Subacute mesenteric venous thrombosis: Symptoms appear over a period of many days and may not be as severe as with acute thrombosis. In this case, some blood can still reach your intestines, but not enough. People often experience symptoms for up to two weeks before seeking medical care.
- Chronic mesenteric venous thrombosis: There may be no symptoms. That’s because enough blood can still reach your intestines through collateral vessels. These are small veins that gradually form to help transport your blood. Doctors usually find chronic mesenteric venous thrombosis when doing imaging tests for other reasons. About 20% to 40% of all cases of mesenteric venous thrombosis are chronic.
Patients with mesenteric venous thrombosis may present with a range of signs and symptoms, from mild abdominal pain to hemodynamic instability secondary to septic shock. Mesenteric venous thrombosis may occur due to a primary coagulopathy or an underlying infectious, traumatic, or inflammatory condition.
The location, type (i.e., acute, subacute or chronic onset) and extent of the thrombus affect mesenteric venous thrombosis prognosis. Patients with chronic mesenteric venous thrombosis may have complications stemming from venous hypertension, including malnutrition and esophageal or gastric varices. Chronic thrombi promote the formation of collaterals that protect your intestines from ischemic changes, but when a thrombus arises acutely, mesenteric ischemia may develop quickly; acute ischemia disrupts the intestinal mucosal barrier, promoting bacterial translocation and resulting in sepsis, multisystem organ failure, and death 1. Although mesenteric venous thrombosis is a relatively rare condition, mortality remains high due to nonspecific symptoms and delayed diagnosis 10, 11.
Venous thrombosis accounts for 5% to 15% of cases of acute mesenteric ischemia and are responsible for 1 in 5,000 to 15,000 inpatient admissions and 1 in 1,000 emergency department visits 1. Chronic mesenteric venous thrombosis accounts for 20% to 40% of all cases and is often an incidental finding on imaging scans for other reasons 1. Computed tomography (CT) has increased the number of cases diagnosed during evaluation for other reasons, and CT scans can identify approximately 90% of mesenteric venous thromboses 1. The incidence of mesenteric venous thrombosis is estimated to be 2.7 per 100,000 persons. Although mortality remains between 19% and 23%, there has been a trend toward earlier diagnosis and improved outcomes. Mesenteric venous thrombosis is slightly more common in men and most frequently presents in persons between the ages of 40 and 60 12, 13.
Mesenteric venous thrombosis can happen at any age, but it usually affects people in their 40s or 50s. The mesenteric vein thrombosis may be secondary to an inherited or acquired thrombophilia or as a consequence of or in conjunction with a proinflammatory state. Factors contributing to mesenteric venous thrombus formation include injury, stasis, malignancy, infection, trauma, and systemic inflammation. While greater than 25% of cases of mesenteric venous thrombosis may initially appear idiopathic, with thorough evaluation, many are shown to have an identifiable etiology. The thrombosis can originate in the vena rectae or a major vein and may involve the hepatic portal vein.
The acuity and extent of the thrombus will dictate the course of the disease and the recommended intervention.
Treatment of mesenteric venous thrombosis ranges from temporary anticoagulation with blood thinners when there is no associated bleeding disorder to management of the underlying proinflammatory disorder to prolonged intensive care unit admission and urgent surgical intervention 1. In some cases, medicine can be delivered directly into the clot to dissolve it. This procedure is called thrombolysis. The goal of treatment is to protect tissue, prevent the extension of the thrombosis, and minimize the chances of recurrence 1. Anticoagulation is often a mainstay of therapy. Anticoagulation is recommended even for those patients with varices, but patients with symptomatic varices may require decompression of their venous hypertension before they are anticoagulated.
Less often, the clot is removed with a type of surgery called thrombectomy.
If there are signs and symptoms of a severe infection called peritonitis, surgery to remove the injured part of the intestine is done. After surgery, an ileostomy (opening from the small intestine into a bag on the skin) or colostomy (an opening from the colon into the skin) may be needed.
Figure 1. Acute superior mesenteric venous thrombosis
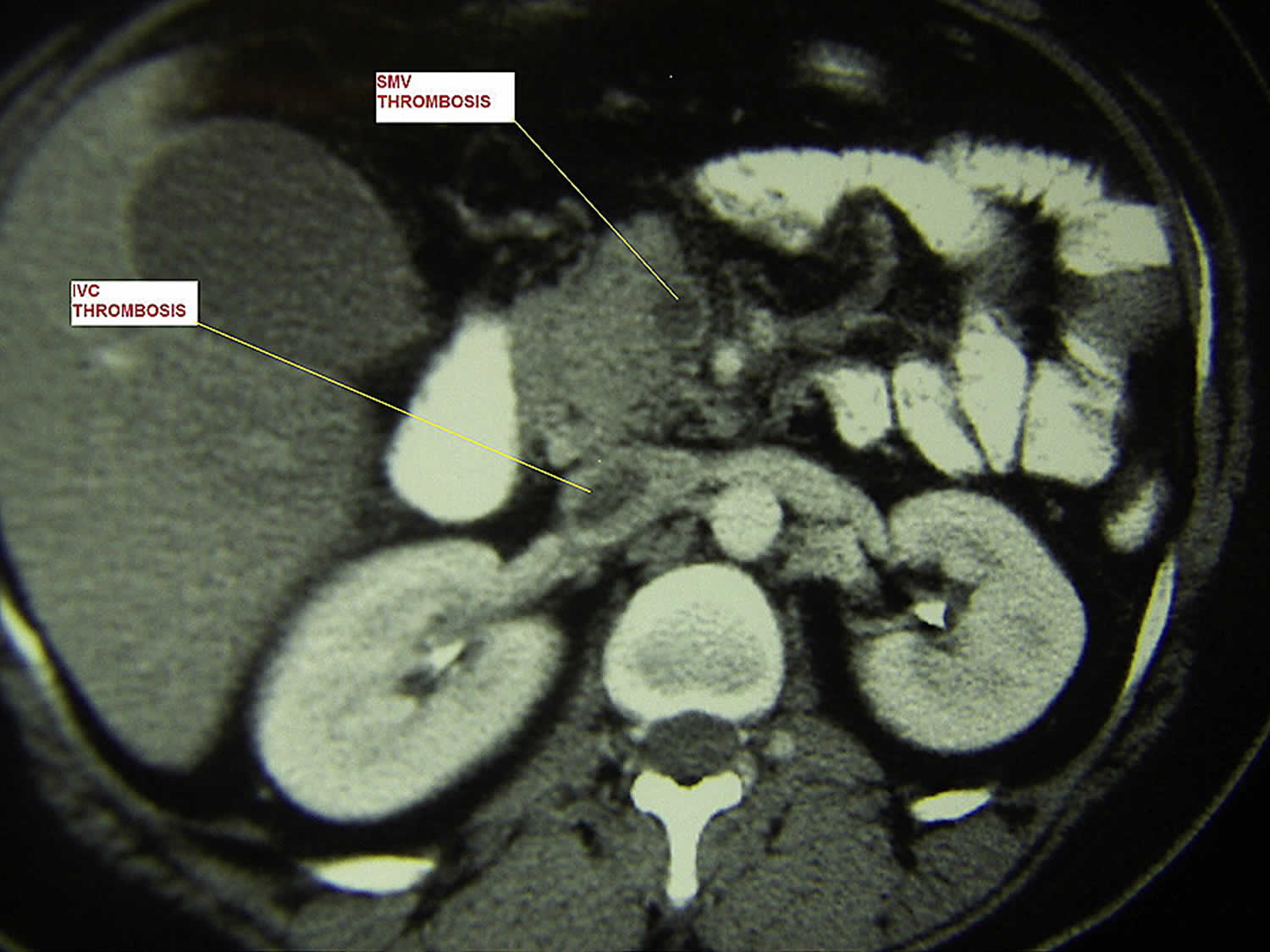
Footnote: Double contrast-enhanced computed tomography (CT) scan shows thrombosis of portal vein and inferior vena cava (IVC).
[Source 5 ]Mesenteric vein anatomy
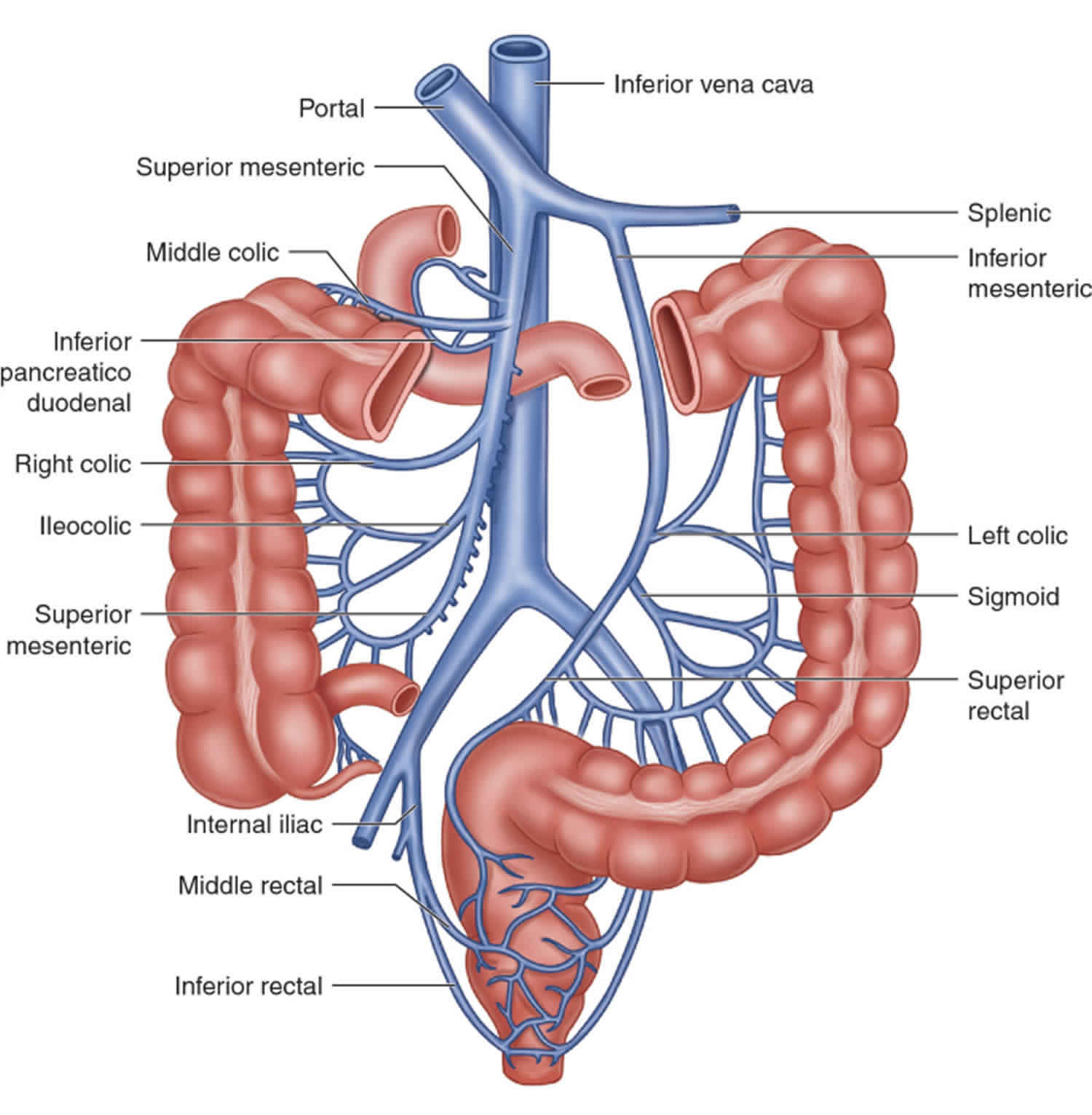
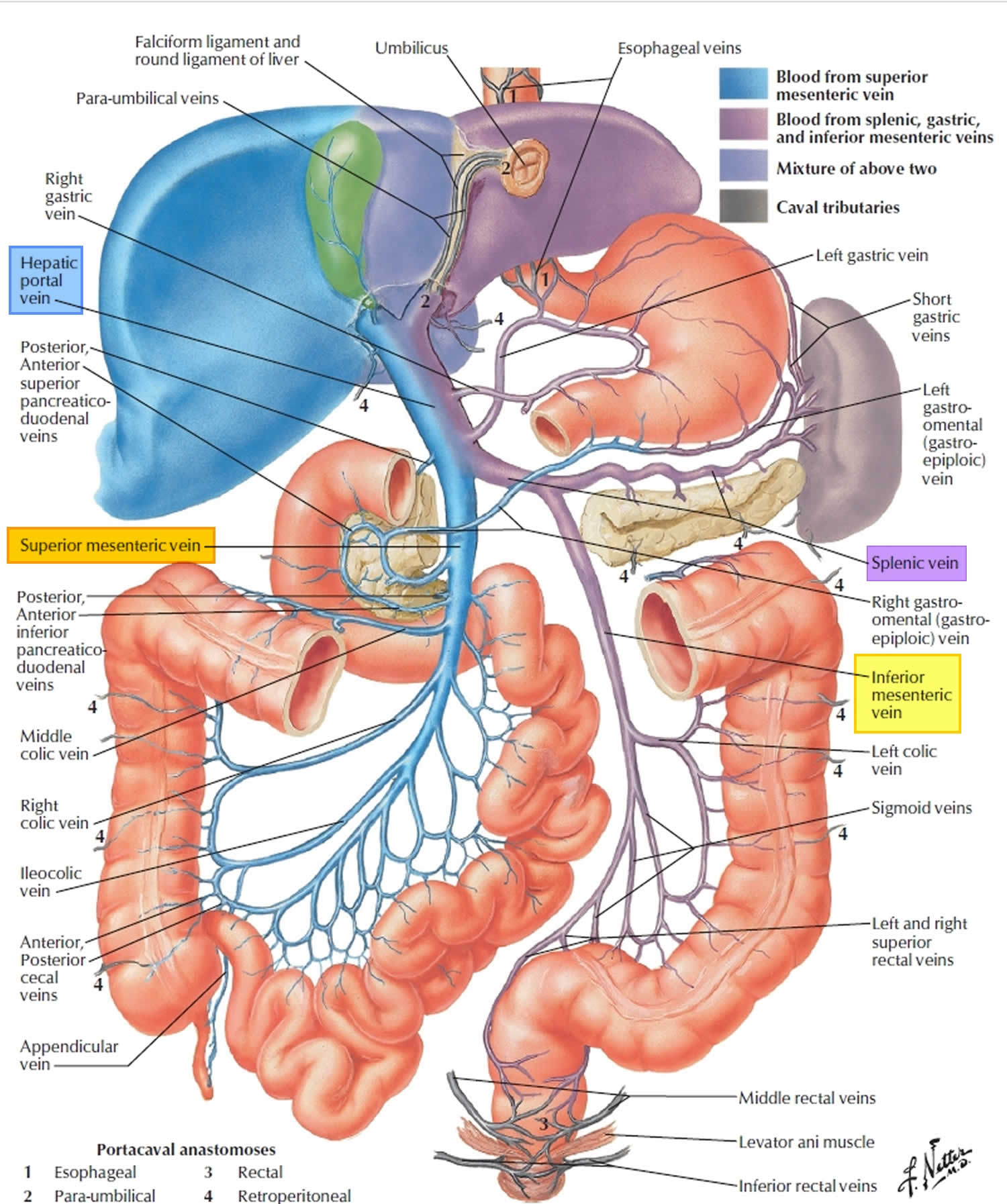
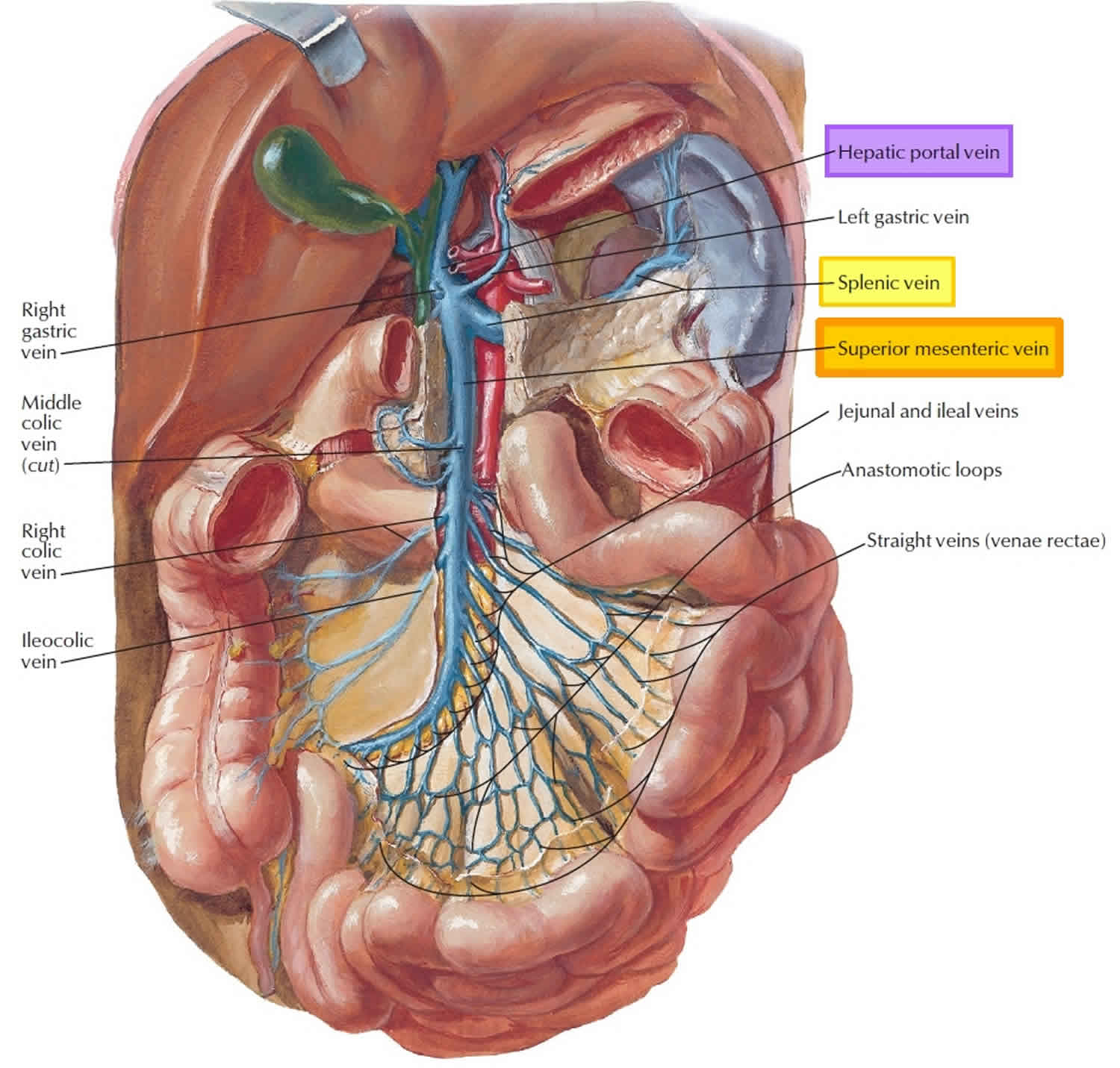
The venous drainage of the intestine follows the same pattern as the arterial circulation (Figures 2 to 5). The superior mesenteric vein (SMV) drains the entire small intestine from the second portion of the duodenum to approximately the right two-thirds of the transverse colon. The superior mesenteric vein (SMV) joins the splenic vein posterior to the neck of the pancreas to form the portal vein. The left gastric vein draining the lower part of the esophagus and upper half of the lesser curve of the stomach enters at the point of formation of the portal vein. Short gastric veins draining the fundus of the stomach enter into the splenic vein. The inferior mesenteric vein (IMV) drains the left colon and enters into the splenic vein.
- Superior mesenteric vein (SMV) ascends just to the right of the superior mesenteric artery. Superior mesenteric vein receives blood from the entire small intestine, the first half of the large intestine (ascending and transverse colon), and some of the stomach. Its superior part lies posterior to the stomach and pancreas. The superior mesenteric vein, too, exhibits a fanlike arrangement in the mesentery and then joins the splenic vein to form the hepatic portal vein.
- Inferior mesenteric vein (IMV) ascends along the posterior abdominal wall, well to the left of the inferior mesenteric artery. Inferior mesenteric vein (IMV) tributaries drain the organs that are supplied by that artery—namely, the distal part of the colon and the superior rectum. The inferior mesenteric vein converges in a fanlike array in the mesentery and empties into the splenic vein posterior to the stomach and pancreas.
- Splenic vein drains the spleen and travels across the abdominal cavity toward the liver. Splenic vein runs horizontally, posterior to the stomach and pancreas, and joins the superior mesenteric vein (SMV) to form the hepatic portal vein. Its tributaries correspond to the branches of the splenic artery. Along the way, splenic vein picks up pancreatic veins from the pancreas, then the inferior mesenteric vein, then ends where it meets the superior mesenteric vein. Even though the spleen is not a digestive organ, venous blood leaving the spleen drains through the hepatic portal system. As a result, any microbes that escape the spleen’s infection-fighting activities are carried to the liver for destruction.
- Hepatic portal vein is a short, vertical blood vessel that lies directly inferior to the liver and anterior to the inferior vena cava (IVC). Inferiorly, hepatic portal vein begins posterior to the pancreas as the union of the superior mesenteric vein (SMV) and splenic vein. Superiorly, hepatic portal vein travels about 8 cm upward and to the right, receives the cystic vein from the gallbladder, then enters the inferior surface of the liver and divides into right and left branches, whose smaller branches reach the liver sinusoids. Blood from the sinusoids empties into the hepatic veins and they empty into the inferior vena cava (IVC), thereby reentering the general systemic circulation. On its way to the liver, the hepatic portal vein receives the right and left gastric veins from the stomach.
- Left and right gastric veins form an arc along the lesser curvature of the stomach and empty into the hepatic portal vein.
Figure 2. Mesenteric vein anatomy
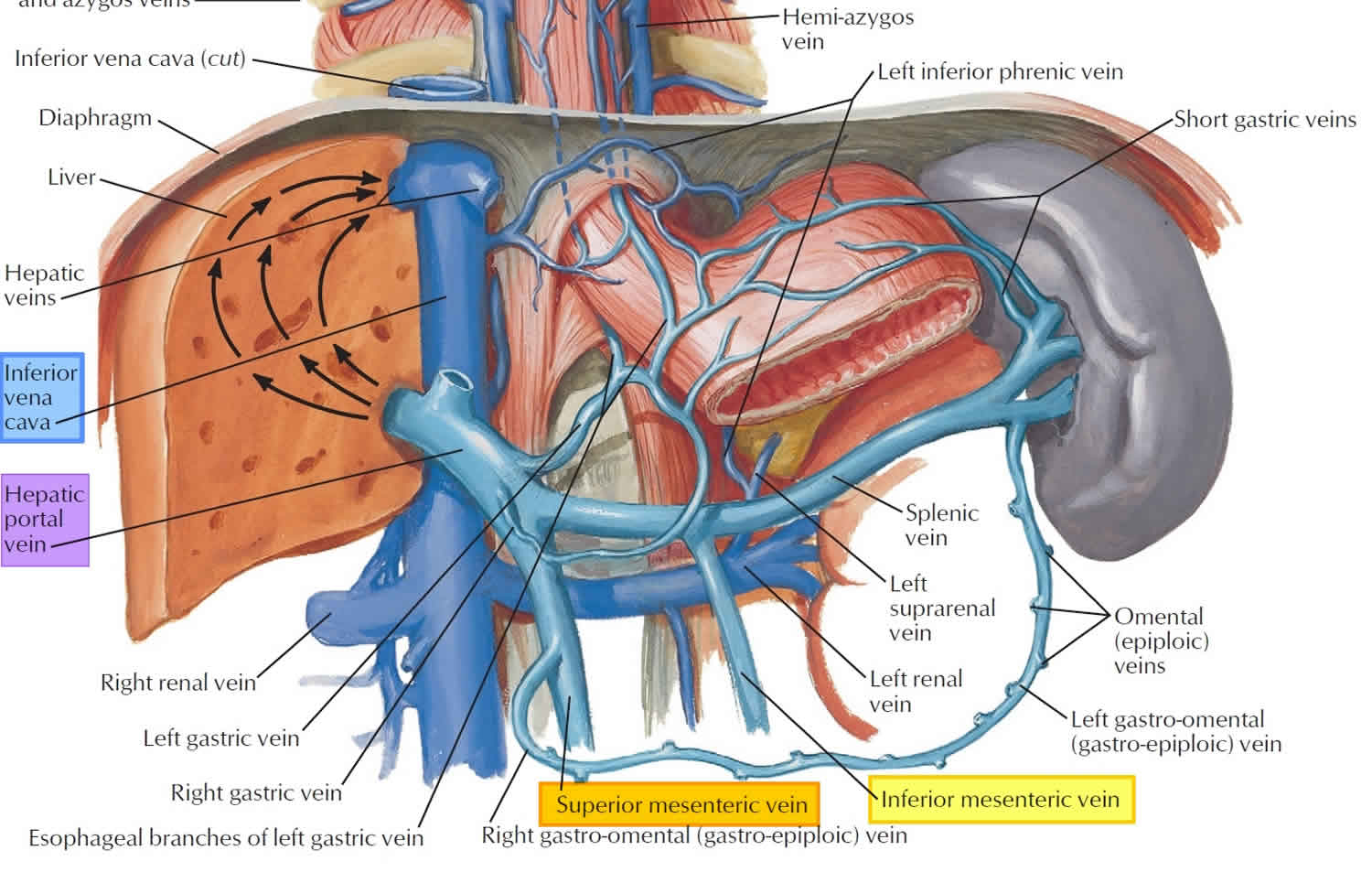
Figure 3. Mesenteric vein branches
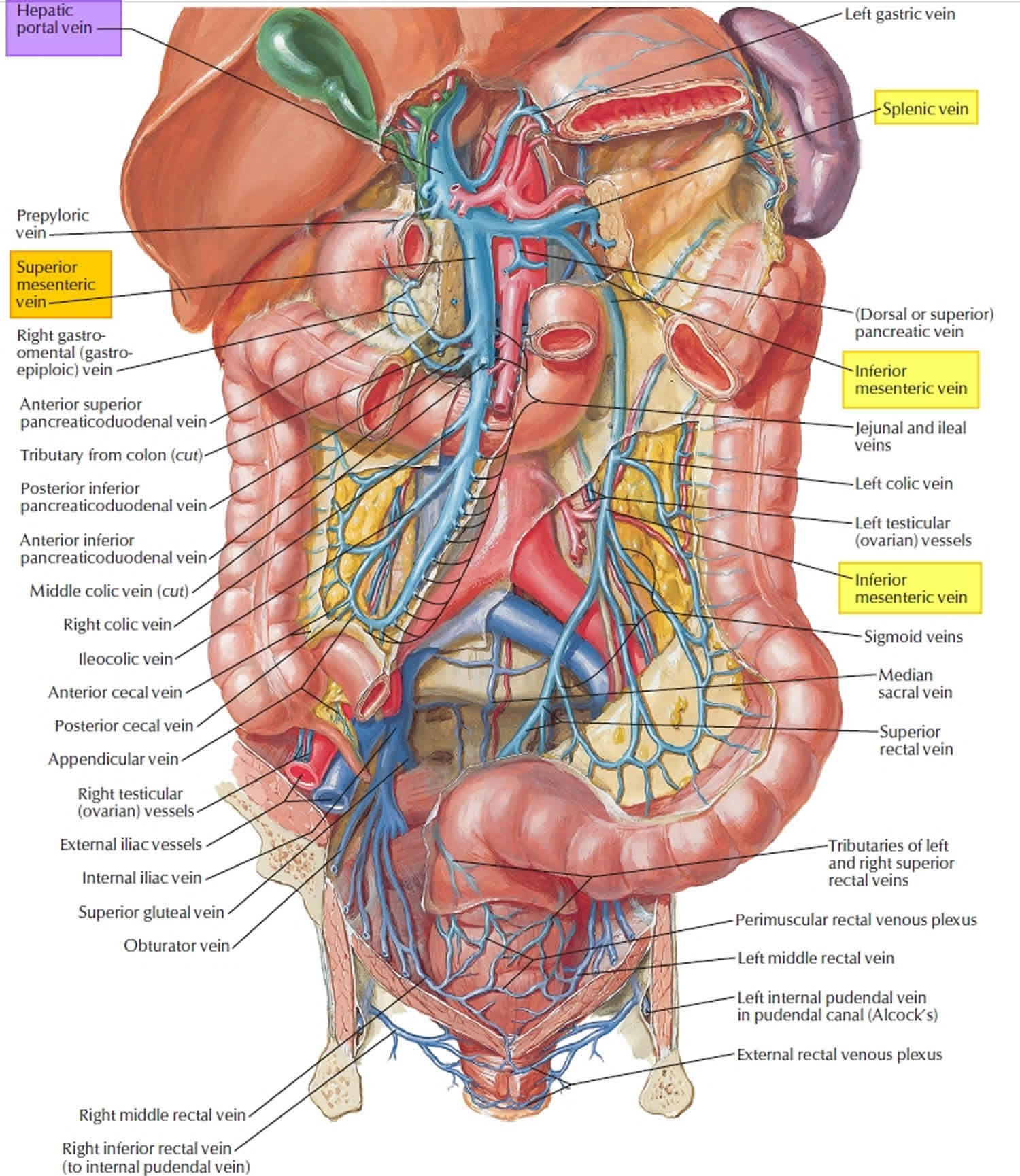
Figure 4. Hepatic portal vein tributaries (portacaval anastomoses)
Superior mesenteric vein
Your superior mesenteric vein (SMV) is a blood vessel that helps carry blood from your intestines to your liver. The superior mesenteric vein (SMV) plays an important role in the distribution of blood in your abdomen (belly) and ultimately your entire circulatory system.
Your superior mesenteric vein supports the work of your hepatic portal system (portal venous system). This is a network of veins that drains blood from organs in your belly and sends it to your liver. Your superior mesenteric vein (SMV) is one of the most important veins in this network because it collects blood from many other veins.
Your superior mesenteric vein (SMV) is a bit like a tree branch containing many twigs (smaller branches). The twigs are smaller veins that serve as tributaries, carrying blood from nearby organs into your superior mesenteric vein (SMV). Together with its tributaries, your superior mesenteric vein drains blood from your:
- Small intestine
- Large intestine
- Stomach
- Pancreas
- Appendix
Your superior mesenteric vein then supplies all this blood to your hepatic portal vein.
If you imagine your superior mesenteric vein (SMV) as a tree branch, then you can think of your hepatic portal vein as the tree trunk. This trunk is “planted” in your liver through an opening called your liver hilum. Blood in your portal vein drains into your liver. Your liver then filters and processes the blood before sending it into veins that lead to your heart. Then, the blood flows through your heart and lungs and back out to the rest of your body.
Figure 5. Superior mesenteric vein
Tributaries of the superior mesenteric vein
The table below lists tributaries of your superior mesenteric vein and what each one drains.
Table 1. Superior mesenteric vein tributary
| Superior mesenteric vein tributary | What it drains |
|---|---|
| Jejunal vein | Small intestine |
| Ileal vein | Small intestine |
| Ileocolic vein | Appendix |
| Right colic vein | Large intestine |
| Middle colic vein | Large intestine |
| Right gastroepiploic vein | Stomach |
| Inferior pancreaticoduodenal vein | Pancreas |
Superior mesenteric vein thrombosis
Superior mesenteric vein thrombosis is when a blood clot forms in your superior mesenteric vein. The blood clot can cut off the blood supply to your intestines, leading to intestinal damage and complications. Pain in your abdomen (belly) is the most common symptom. Superior mesenteric vein thrombosis can be fatal without timely diagnosis and treatment.
Sudden, severe pain in your belly is the most common symptom of acute superior mesenteric vein thrombosis. But some people with subacute or chronic superior mesenteric vein thrombosis have pain that comes and goes over days or weeks, or no symptoms at all. The sooner you receive care, the better your chances of a good outcome.
Figure 6. Superior mesenteric vein thrombosis

Footnotes: A 21-year-old female presented to the emergency room with two days of acute, sharp, right lower quadrant pain (RLQ). Her pain had started as periumbilical pain, which migrated to the right lower quadrant. She has had one week of nausea and vomiting without anorexia and did not relate pain to meals. She denied any traumatic events. Her past medical history was significant for a gonadal vein thrombosis after the birth of her first child and chronic pelvic pain for the previous seven months. One week prior to her emergency room presentation, she had completed a six-month course of warfarin for the gonadal vein thrombosis. At the time of presentation, she was on no medications and had no known drug allergies. There was no family history of bleeding or clotting disorders. Her physical exam was significant for right lower quadrant pain (RLQ) abdominal tenderness without guarding, rigidity or peritoneal signs. Computed tomography (CT) with contrast of her abdomen/pelvis showed a non-occlusive thrombosis of the superior mesenteric vein (red arrow).
[Source 14 ]Superior mesenteric vein thrombosis cause
Doctors divide the causes of superior mesenteric vein thrombosis into 3 main categories:
- Blood clotting disorders that make you more likely to develop a blood clot anywhere in your body. A blood clotting disorder makes your blood form clots too easily. This is also called a hypercoagulable state or thrombophilia. Hypercoagulable states are present in 60% to 75% of patients with mesenteric venous thrombosis. Often, an inherited or acquired thrombophilia coexists with trauma, infection, inflammation, or surgery to give rise to a thrombotic process. Thrombosis may also arise from stasis, such as heart failure or cirrhosis. Hypercoagulable conditions include malignancies, heparin-induced thrombocytopenia, essential thrombocythemia, polycythemia vera, antiphospholipid antibodies, oral contraceptive use, and pregnancy. Heritable hypercoagulable conditions include sickle cell disease, Factor V Leiden, excess prothrombotic factors, and deficiencies in antithrombin III or proteins C or S 13, 15, 14.
- Direct injury to your vein from inflammation or surgery.
- Slow or congested blood flow in your mesenteric vein and surrounding veins, due to conditions like cirrhosis, heart failure or compression from a mass or tumor.
Other causes of superior mesenteric vein thrombosis include:
- Appendicitis
- Cancer of the abdomen
- Diverticulitis
- Liver disease with cirrhosis
- High blood pressure in the blood vessels of the liver
- Abdominal surgery or trauma
- Pancreatitis
- Inflammatory bowel disorders
- Heart failure
- Protein C or S deficiencies
- Polycythemia vera
- Essential thrombocythemia
People who have disorders that make the blood more likely to stick together (clot) have a higher risk for superior mesenteric vein thrombosis. Birth control pills and estrogen medicines also increase risk.
Superior mesenteric vein thrombosis is more common in men than women. It mainly affects middle aged or older adults.
Superior mesenteric vein thrombosis symptoms
Superior mesenteric vein thrombosis symptoms may include any of the following:
- Abdominal pain, which may get worse after eating and over time
- Bloating
- Constipation
- Bloody diarrhea
- Fever
- Septic shock
- Lower gastrointestinal bleeding
- Vomiting and nausea
Superior mesenteric vein thrombosis diagnosis
A CT scan is the main test used to diagnose superior mesenteric vein thrombosis.
Other tests may include:
- Angiogram (studying the blood flow to the intestine)
- MRI of the abdomen
- Ultrasound of the abdomen and mesenteric veins
Superior mesenteric vein thrombosis treatment
It’s important to keep in mind that superior mesenteric vein thrombosis is fatal without treatment.
Your doctor will tailor treatment to your needs with the larger goals of:
- Restoring blood flow to your intestines so they can function normally.
- Preventing or limiting damage to your intestines.
- Preventing new blood clots from forming and determining the underlying cause.
Your doctor will use one or more of the following treatment methods depending on the onset (acute vs. chronic) and severity of your mesenteric vein thrombosis.
- Anticoagulation with blood thinners or anticoagulants: This is often the first treatment method doctors use. Anticoagulation involves giving you medication (blood thinners or anticoagulants) to get rid of the blood clot and prevent new ones from forming. Many doctors start with a heparin infusion and follow that up with warfarin. Some people need anticoagulant medication for six months or so, while others need it for longer. If you have a blood clotting disorder, or if the blood clot formed without a clear cause, you may need lifelong anticoagulation. People who take a blood thinner called warfarin (Jantoven) need regular blood tests to monitor levels of the drug in the body. Certain blood-thinning medications are not safe to take during pregnancy.
- Thrombolysis also called fibrinolytic therapy. Thrombolytic therapy is the use of drugs to break up or dissolve blood clots. With thrombolysis, your doctor uses an x-ray imaging and a catheter to guide special medication into your veins and destroy the blood clot. They usually deliver the medication over a period of 24 to 72 hours. Thrombolysis can cause serious bleeding, so they’re usually only used for people with severe blood clots.
- Thrombectomy: This is the surgical removal of the blood clot. Doctors limit this treatment to specific cases, such as people who aren’t candidates for thrombolysis. Doctors can use open surgery as well as minimally invasive methods for thrombectomy.
- Bowel resection: This is the medical term for surgery to remove part of your intestines. You may need a small bowel resection or colectomy if the blood clot stops blood flow to your intestines, causing permanent damage. If you start anticoagulation in the hospital, your provider will monitor your symptoms to determine if you need surgery and to identify complications.
Chronic mesenteric venous thrombosis
Chronic mesenteric venous thrombosis accounts for about 20% to 40% of all cases of mesenteric venous thrombosis, may be detected incidentally on abdominal imaging, and is differentiated from acute mesenteric venous thrombosis by the presence of an extensive collateral circulation 16, 17. The diagnosis of chronic mesenteric venous thrombosis is usually made on CT scan. Patients with portal venous thrombosis present with features of portal hypertension such as splenomegaly, variceal hemorrhage, and thrombocytopenia. If the thrombosis is distal to the junction of the left gastric vein and portal vein, both esophageal and gastric varices occur. However, if the thrombosis is proximal to this junction, gastric varices are predominant. Extensive thrombosis involving the portal vein, superior mesenteric vein, splenic vein, and inferior mesenteric vein results in extensive bowel edema, with sequelae being persistent abdominal pain, small-bowel strictures, and inability to meet nutritional needs via the gastrointestinal tract. Some patients may require long-term home parenteral nutrition. Chronic mesenteric venous thrombosis may also be associated with edema and extensive collateral vessels around the bile ducts, giving rise to portal hypertensive cholangiopathy mimicking primary sclerosing cholangitis on cholangiography. This entity presents with biochemical cholestasis, biliary strictures, biliary stones, and cholangitis.
Chronic mesenteric venous thrombosis diagnosis
Chronic mesenteric venous thrombosis is usually diagnosed on CT. However, magnetic resonance cholangiopancreatography is preferred whenever this diagnosis is suspected 18, 19. Endoscopic retrograde cholangiopancreatography (ERCP) may also be used but may be complicated by hemorrhage from puncture of the biliary varices by the biliary catheter used to inject radiologic contrast medium for delineation of the bile ducts.
Chronic mesenteric venous thrombosis treatment
Anticoagulation should be considered for patients with chronic portal venous thrombosis, especially those with prothrombotic states. However, data are limited on the use of anticoagulants in patients with chronic mesenteric venous thrombosis. In one retrospective study, 18 of 60 patients with chronic portal venous thrombosis underwent long-term anticoagulation. Five patients who had bleeding before anticoagulation had eradication of varices before starting anticoagulation. Of the other patients, 4 had bleeding on follow-up; good control of bleeding was achieved in 3, and the fourth patient died 20. These data suggest that varices should be adequately treated and obliterated before initiating anticoagulation.
Esophageal and/or gastric varices are managed as in patients with cirrhosis. Management includes prevention of a first variceal bleed for patients with varices but no history of bleeding, control of variceal hemorrhage, and prevention of recurrent bleeding. If feasible, transjugular intrahepatic portosystemic shunt (TIPS) may be recommended for patients who continue to experience bleeding despite combined endoscopic and pharmacological therapy 18. Patients without cirrhosis, especially in the pediatric age group, are managed by creation of a surgical shunt between the left portal vein and superior mesenteric vein (Rex bypass) 18. Patients with isolated gastric varices due to splenic venous thrombosis are amenable to cure by splenectomy 21.
Portal hypertensive cholangiopathy requires treatment if patients are symptomatic from cholangitis or biliary obstruction. Stones within the common duct are removed at endoscopic retrograde cholangiopancreatography. Caution is required during the procedure because the presence of portal hypertension makes bleeding more likely. Strictures in the bile ducts are treated with endoscopic stenting and in selected patients by portosystemic shunt surgery. Rarely, hepaticojejunostomy may be required 18.
Mesenteric venous thrombosis causes
Doctors divide the causes of mesenteric venous thrombosis into 3 main categories 9:
- Blood clotting disorders also called a hypercoagulable state or thrombophilia that make you more likely to develop a blood clot anywhere in your body. A blood clotting disorder makes your blood form clots too easily. Hypercoagulable states are present in 60% to 75% of patients with mesenteric venous thrombosis. Often, an inherited or acquired thrombophilia coexists with trauma, infection, inflammation, or surgery to give rise to a thrombotic process. Thrombosis may also arise from stasis, such as heart failure or cirrhosis.
- Hypercoagulable conditions include 13, 15, 14:
- Cancers
- Heparin-induced thrombocytopenia
- Essential thrombocythemia
- Polycythemia vera
- Antiphospholipid antibodies
- Oral contraceptive use, and pregnancy.
- Acquired hypercoagulable conditions include:
- Hematologic conditions
- Polycythemia vera
- Myelofibrosis
- Thrombocythemiaa
- JAK2 gene sequence variation
- Antiphospholipid antibodies
- Paroxysmal nocturnal hemoglobinuria
- Nonhematologic conditions
- Cancer
- Oral contraceptive pills
- Pregnancy
- Nephrotic syndrome
- Hyperhomocysteinemia
- Hematologic conditions
- Heritable hypercoagulable conditions include:
- Sickle cell disease
- Factor V Leiden deficiency
- Excess prothrombotic factors
- Antithrombin deficiency
- Protein C or S deficiency
- Prothrombin gene sequence variation (G20210A)
- Methylene tetrahydrofolate reductase gene sequence variation
- Hypercoagulable conditions include 13, 15, 14:
- Direct injury to your vein from inflammation or surgery.
- Inflammatory conditions
- Pancreatitis
- Inflammatory bowel disease
- Diverticulitis
- Peritonitis
- Appendicits
- Intra-abdominal surgery e.g., splenectomy.
- Abdominal trauma
- Inflammatory conditions
- Slow or congested blood flow in your mesenteric vein and surrounding veins, due to conditions like cirrhosis, congestive splenomegaly, congestive heart failure or compression from a mass or tumor.
- When the underlying etiology cannot be identified, the term primary or idiopathic mesenteric venous thrombosis is used.
People who have disorders that make the blood more likely to stick together (clot) have a higher risk for superior mesenteric vein thrombosis. Birth control pills and estrogen medicines also increase risk.
Mesenteric vein thrombosis is more common in men than women. It mainly affects middle aged or older adults.
Patients with a thrombus in a major mesenteric vein often have concurrent hepatic portal vein thrombosis; such persons are more likely to have an underlying localized condition such as inflammatory bowel disease (IBD), pancreatitis, diverticulitis, myeloproliferative neoplasms, and cancers 1. Portal vein involvement is also higher in persons with cirrhosis and has been reported in 15% of people awaiting liver transplantation. Patients with smaller vessel thrombosis in the vena rectae are more likely to have systemic thrombophilia 22.
Sometimes, doctors can’t identify a cause (idiopathic). While up to 25% of cases of mesenteric vein thrombosis may initially be construed as idiopathic, thorough evaluation often reveals the causative factor. For example, the gain-of-function JAK2V617F mutation results in a blood cell line proliferation; an assay for JAK2V617F mutation helps diagnose those with subclinical myeloproliferative disorders also called myeloproliferative neoplasms and can distinguish an inherited prothrombotic state from a reactive condition. The JAK2V617F mutation is detected in most cases of polycythemia vera and 50% of cases of essential thrombocythemia and myelofibrosis. In addition, the JAK2V617F mutation is reported in up to 46% of cases without overt myeloproliferative neoplasms 22, 23, 24. Myeloproliferative neoplasms are a rare group of diseases in which abnormal stem cells in the bone marrow produce excess numbers of one or more types of blood cells (red blood cells, white blood cells and/or platelets). These abnormal blood cells cannot function properly and can cause serious health problems unless properly treated and controlled. Myeloproliferative disorders (myeloproliferative neoplasms) are chronic diseases that, in most cases, remain stable for many years and progress gradually over time. Main types of myeloproliferative disorder (myeloproliferative neoplasm) are chronic myeloid leukemia (CML), polycythemia vera (PV), essential thrombocythemia (ET) and primary myelofibrosis (PMF) 25.
Risk factors for mesenteric venous thrombosis
You face a higher risk of mesenteric venous thrombosis if you have any of the following medical conditions:
- Inherited or acquired blood clotting disorders, including those caused by some medications.
- Inflammatory bowel disease (IBD).
- Cirrhosis (liver disease).
- Pancreatitis.
- Pancreatic cancer.
- Heart failure.
- Enlarged spleen.
- Large abdominal tumor or mass.
- Some viral infections.
Certain surgeries on your belly, like a splenectomy, can damage the inner lining of your blood vessels (endothelium). This damage leads to inflammation that can raise your risk of a blood clot.
Mesenteric venous thrombosis pathophysiology
The pathophysiology of mesenteric venous thrombosis depends on the onset, location, and causative factor of the thrombus. Systemic thrombophilia causes thrombi within the venae rectae. In contrast, local factors, such as intraabdominal cancer, pancreatitis, and diverticulitis, produce thrombi in the superior mesenteric vein, often with extension into the portal vein.
Thrombi within the small, more distal venous branches pose a risk for bowel infarction. Blood return from the bowel is impeded, resulting in venous engorgement and subsequent ischemia. Arterial spasms can also contribute to irreversible ischemia. The bowel mucosa becomes permeable at sites of infarction, permitting the translocation of bacteria and leading to sepsis 13, 15.
In chronic mesenteric venous thrombosis, collateral circulation develops in the form of extensive cavernoma around the chronically thrombosed area. Often, portal hypertension, varices, and thrombocytopenia coexist with chronic venous thrombosis, and those with portal venous thrombosis have splenomegaly secondary to tissue fibrosis. If the thrombosis is distal to the junction of the left gastric and portal vein, both esophageal and gastric varices are seen. However, if the thrombosis is proximal to this point, gastric varices predominate 26, 27.
Mesenteric venous thrombosis symptoms
Mesenteric venous thrombosis symptoms vary widely. Some people have no symptoms. This is often the case with chronic mesenteric venous thrombosis. However, acute mesenteric vein thrombosis can cause sudden and severe cramping in your belly. With the subacute mesenteric vein thrombosis, vague belly pain may come and go over several days or weeks.
Some people with mesenteric venous thrombosis develop portal hypertension. In that case, you may experience:
- Blood in your poop.
- Nausea and vomiting, with blood in your vomit.
- Bloated stomach.
- Swelling (edema) in your legs and feet.
- Mental confusion.
Mesenteric venous thrombosis usual presentation is acute abdominal pain located in the mid abdomen that is out of proportion to physical signs. Nausea, vomiting, diarrhea, or gastrointestinal bleeding may also occur. Other reported symptoms are constipation, anorexia, and fever. Fever at the onset of symptoms suggests pylephlebitis or an infected portal venous thrombosis seen with intestinal infections, usually acute diverticulitis or appendicitis.
In its severe form, it may present clinical symptoms suggestive of perforation and peritonitis. A new onset of ascites may also raise a suspicion of mesenteric venous thrombosis. In rare cases where ischemia continues, it may lead to bowel stricture and intestinal obstruction. Intestinal obstruction in superior mesenteric vein thrombosis is a consequence of persistent ischemia, and its clinical manifestations appear rather later in disease evolution 28. Most of the cases reporting intestinal obstruction as a result of superior mesenteric vein thrombosis had a two-stage presentation. First, there was a bowel ischemia, with patients describing abdominal pain, and second, they developed a bowel stricture and/or an intestinal obstruction 29.
About 75% of patients are symptomatic for more than 48 hours before presentation, with the mean duration of symptoms reported to vary from 6 to 14 days 11, 16, 30, 31, 32.Abdominal signs such as abdominal tenderness 11, 16, abdominal distention 33, 31, 11 and ascites 33, 34, 35 may occur with increasing ischemia. Patients may be dehydrated from volume loss or third-space compartmentalization of fluid.
In severe cases, peritoneal signs such as rebound tenderness, guarding, and/or rigidity may be noted because of transmural infarction and bowel gangrene. About 6% to 29% of patients, especially those with severe disease, may be hemodynamically unstable 33, 11, 35.
Peritoneal signs, hemodynamic instability, and fever suggest severe disease with bowel infarction and poor outcome 9.
If you develop new or worsening pain in your belly, it’s important to see a doctor right away so they can determine the reason. Because any delays in diagnosis and treatment can cause significant increases in morbidity and death.
Mesenteric venous thrombosis complications
Mesenteric venous thrombosis complications arise from the thrombosis, the treatments, and the underlying condition. A blood clot in your mesenteric veins causes tissue swelling in your intestine and can lead to mesenteric ischemia. This is reduced blood flow to parts of your digestive system. When your digestive organs don’t receive enough oxygen-rich blood, they can’t work properly. Also, their tissues can start to die. In some cases, this can result in holes developing in your intestine and the contents of your intestine leaking into the surrounding space. Other times, the helpful bacteria that normally live in your digestive system can spread elsewhere in your body, to areas where they don’t belong. This can lead to sepsis and life-threatening organ failure. As a result, mesenteric venous thrombosis can be fatal without prompt treatment.
Patients with chronic mesenteric venous thrombosis are at risk for many impairments of the gastrointestinal system such as biliary strictures, gallstones, and recurrent cholangitis; major reconstructive surgery is required occasionally. Significant bowel swelling (edema) arises in the setting of extensive chronic thrombosis within the portal, superior mesenteric, and splenic veins. Over time, a patient with considerable chronic thrombosis may develop clinically significant small bowel and biliary strictures that can cause malnutrition and cholangitis 36. Patients with chronic mesenteric venous thrombosis also suffer from chronic fatigue, bone pain, pruritis, weight loss, and bleeding from platelet dysfunction 36.
Thrombosis recurrence usually occurs within the first 30 days and may be as low as 0% to 3% in those who receive anticoagulation. Recurrence or extension of thrombosis may give rise to bowel infarction, sepsis, and death. Short bowel syndrome may be a consequence of bowel resection, and some patients require lifelong total parenteral nutrition 37.
Complications from catheter-directed thrombolysis include major and minor bleeding, fever, hematoma formation, pain, and infection. Transhepatic access for thrombolytic therapy carries an increased risk of bleeding, and the transileocolic approach may require surgical access. The bleeding risk from anticoagulation is less than 10%, and bleeding is usually within the gastrointestinal system. Patients with varices have a higher bleeding risk and should be pretreated with beta blockers or undergo definitive management of varices 38, 39.
The myeloproliferative neoplasms that predispose some patients to thrombosis can convert to leukemia and myelodysplasia.
Mesenteric venous thrombosis diagnosis
Doctor may suspect you have mesenteric venous thrombosis due to your symptoms. However, the diagnosis can be challenging because mesenteric venous thrombosis symptoms vary widely and some people have no symptoms. That means your symptoms could point to many different potential problems. A blood clot in your mesenteric vein isn’t always the first or most obvious explanation for pain in your belly or other symptoms.
If your doctor suspects you may have a blood clot, they’ll run imaging tests.
Imaging studies
The gold standard for diagnosing mesenteric venous thrombosis is CT angiography (CT with intravenous contrast). This imaging test uses intravenous contrast dye to view blood flow through your blood vessels. This can show how well blood is flowing through the arteries and veins in your belly and reveal if you have a blood clot. An abdominopelvic CT with intravenous contrast can diagnose mesenteric venous thrombosis in 90% of cases. The test results guide your treatment plan.
Sometimes, doctors use MRI angiography as an alternative, or to confirm unclear findings from CT angiography. Doctors may also use these studies to monitor how well you respond to treatment.
Magnetic resonance imaging (MRI), angiography, and abdominal Doppler ultrasonography are less commonly employed imaging modalities when evaluating patients with suspected mesenteric venous thrombosis. Abdominal Doppler ultrasonography can detect thrombosis in larger veins but has only 73% to 80% sensitivity and cannot visualize smaller vena recta 40, 2.
When a mesenteric venous thrombosis is identified on CT, magnetic resonance cholangiopancreatography (MRCP) or endoscopic retrograde cholangiopancreatography (ERCP) permits further assessment of the biliary system and degree of portal hypertension; ERCP carries a risk of bleeding from catheter injury. Esophagogastroduodenoscopy (EGD) is recommended to evaluate for esophageal and gastric varices 41.
Plain abdominal radiographs reveal abnormalities in 50% to 75% of cases but demonstrate nonspecific findings such as dilated bowel, thumbprinting, and, in cases of perforation, free air.
Laboratory testing
Routine laboratory testing is not specific for mesenteric venous thrombosis but provides general clinical information. Recommended laboratory studies include a complete blood count with a differential, comprehensive metabolic panel, coagulation tests, and a thrombophilia screen. An elevated lactate level is a late marker of ischemia, and amylase levels can also be elevated with bowel ischemia; amylase levels greater than 1000 U/L suggest pancreatitis. Blood cultures should be obtained from patients with fevers and hemodynamic instability. Patients with portal vein involvement or sepsis will have elevated liver enzymes 13, 42, 43.
Recommended testing after diagnosis of mesenteric venous thrombosis
Acute mesenteric venous thrombosis
- Detailed history and physical examination
- Abdominal computed tomography to confirm the diagnosis of mesenteric venous thrombosis and the extent of thrombosis, to differentiate acute from chronic mesenteric venous thrombosis, and to identify local causes of thrombosis and complications such as bowel gangrene or perforation
- Surgical consultation for infarction or perforation of bowel
- Coagulation profile
- Complete blood cell counts, basic panel, and liver function panel
- Thrombophilia screen
- JAK2 sequence variation screen
- Bone marrow examination
Chronic mesenteric venous thrombosis
- All tests for acute mesenteric venous thrombosis plus
- Upper gastrointestinal endoscopy for detection of varices
- Cholangiography for evaluation of portal hypertensive cholangiopathy
Mesenteric venous thrombosis differential diagnosis
The key to early diagnosis is a high level of clinical suspicion. Severe abdominal pain out of proportion to physical examination findings should be assumed to be acute mesenteric ischemia until disproven 36. Acute mesenteric ischemia is defined as an abrupt stopping of the mesenteric blood supply to the intestine with the development of symptoms that may vary with the time of onset, from minutes (in embolism) to hours (in atherothrombosis), leading to cellular damage, intestinal necrosis, and commonly patient death, if untreated.
It is also essential to distinguish mesenteric venous thrombosis from mesenteric arterial thrombosis, as the cause and approach to treatment are different 36.
Superior mesenteric artery (SMA) embolism (50% of severe abdominal pain cases) and atherosclerotic superior mesenteric artery occlusion (thrombosis) (15–25% of severe abdominal pain cases) are often referred to as an arterial acute mesenteric ischemia or an occlusive acute mesenteric ischemia 36. The overall incidence is low (0.09–0.2% of all acute admissions to emergency departments), representing an infrequent cause of abdominal pain but a common cause of emergent intestinal resection. Prompt diagnosis and intervention are essential to reduce the mortality rates, which exceed 50% 28.
Non-occlusive mesenteric ischemia (NOMI) (20% of severe abdominal pain cases), and mesenteric venous thrombosis (5–15% of severe abdominal pain cases).
Mesenteric venous thrombosis treatment
Prompt treatment is key to survival. The sooner you receive the correct diagnosis and treatment, the better your chances of a good outcome. Your doctor will tailor treatment to your needs with the larger goals of:
- Restoring blood flow to your intestines so they can function normally.
- Preventing or limiting damage to your intestines.
- Preventing new blood clots from forming and determining the underlying cause.
Your doctor will use one or more of the following treatment methods depending on the onset (acute vs. chronic) and severity of your mesenteric vein thrombosis.
- Anticoagulation with blood thinners or anticoagulants: This is often the first treatment method doctors use. Anticoagulation involves giving you medication (blood thinners or anticoagulants) to get rid of the blood clot and prevent new ones from forming. Many doctors start with a heparin infusion and follow that up with warfarin. Some people need anticoagulant medication for six months or so, while others need it for longer. If you have a blood clotting disorder, or if the blood clot formed without a clear cause, you may need lifelong anticoagulation. People who take a blood thinner called warfarin (Jantoven) need regular blood tests to monitor levels of the drug in the body. Certain blood-thinning medications are not safe to take during pregnancy.
- Thrombolysis also called fibrinolytic therapy. Thrombolytic therapy is the use of drugs to break up or dissolve blood clots. With thrombolysis, your doctor uses an x-ray imaging and a catheter to guide special medication into your veins and destroy the blood clot. They usually deliver the medication over a period of 24 to 72 hours. Thrombolysis can cause serious bleeding, so they’re usually only used for people with severe blood clots.
- Thrombectomy: This is the surgical removal of the blood clot. Doctors limit this treatment to specific cases, such as people who aren’t candidates for thrombolysis. Doctors can use open surgery as well as minimally invasive methods for thrombectomy.
- Bowel resection: This is the medical term for surgery to remove part of your intestines. You may need a small bowel resection or colectomy if the blood clot stops blood flow to your intestines, causing permanent damage. If you start anticoagulation in the hospital, your provider will monitor your symptoms to determine if you need surgery and to identify complications.
Figure 7. Acute mesenteric venous thrombosis treatment algorithm
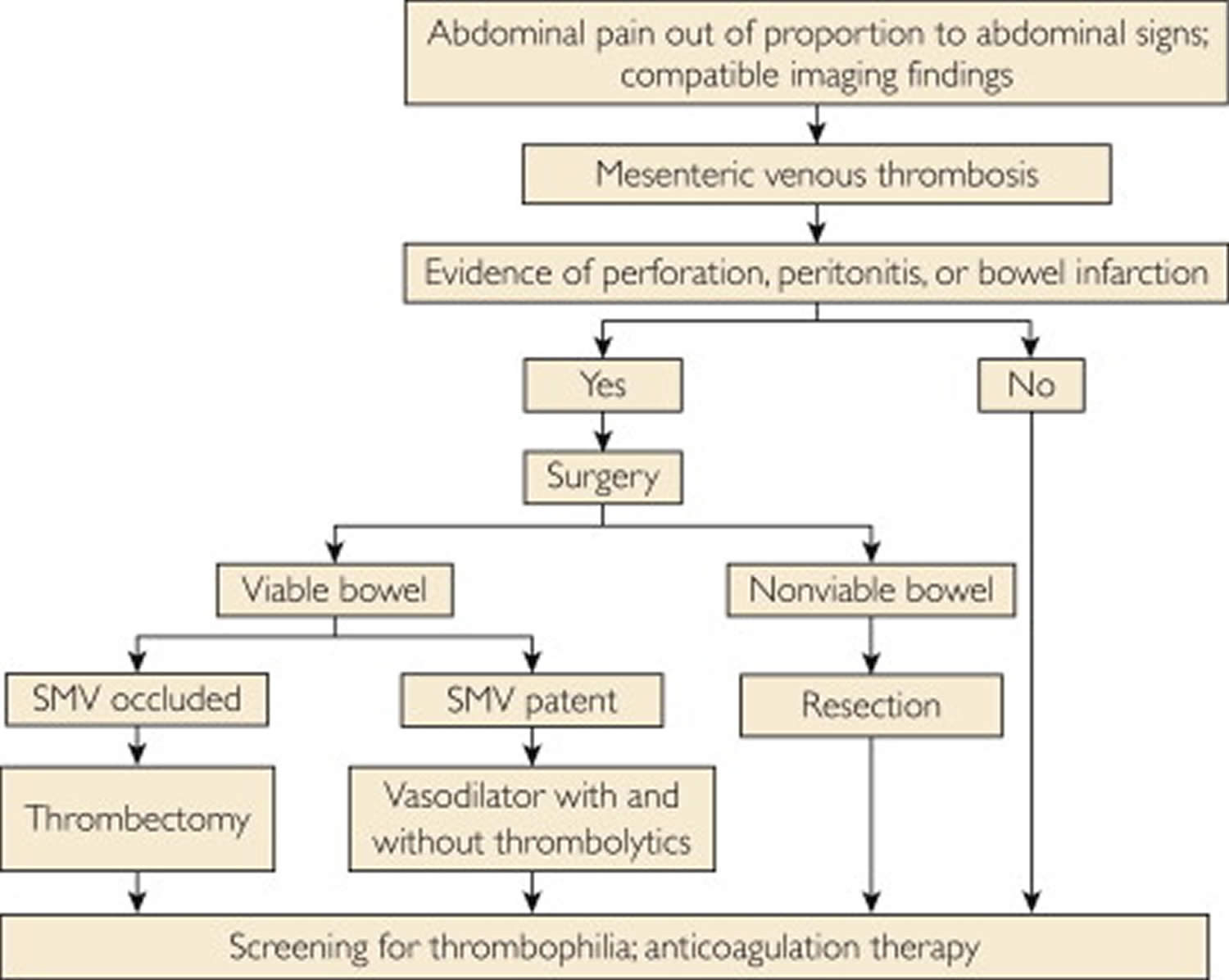
Footnote: Algorithm for management of acute mesenteric venous thrombosis
Abbreviation: SMV = superior mesenteric vein.
[Source 9 ]Treatment for acute and subacute mesenteric venous thromboses can range from bowel rest, resuscitation, and anticoagulation to extensive surgery with bowel resection 1. Treatment goals are to prevent bowel infarction, mitigate blot extension, and minimize recurrence risk. Initial treatment depends on clinical presentation, the acuity of the thrombosis, and the underlying cause. Stable patients may be treated nonoperatively with bowel rest, electrolyte replacement, and anticoagulation. Nasogastric decompression is often necessary, and total parenteral nutrition may be indicated. Patients with fever may benefit from broad-spectrum antibiotics to treat thrombophlebitis or enteric bacterial translocation 38.
Anticoagulation is the cornerstone of mesenteric venous thrombosis treatment. While there remains a possibility of invasive intervention, or for patients with kidney failure, the initial anticoagulant of choice is unfractionated heparin. Once the patient is stable, the anticoagulant is changed to an oral medication such as warfarin or a direct oral anticoagulant (DOAC). Warfarin has the disadvantages of required regular monitoring of the international normalized ratio, drug-drug interactions, and interaction with food due to its metabolism via the cytochrome P450 enzyme pathway 9. In this respect, newer oral anticoagulants such as direct thrombin inhibitors (ximelagatran, dabigatran, and AZD0837) and direct inhibitors of factor Xa (rivaroxaban, apixaban, edoxaban, otamixaban, LY517717, TAK-442, and fondaparinux) have fewer problems 9. However, because the dose is fixed on the basis of the patient’s body weight, lower doses of these newer agents may be required in the presence of extensive liver and kidney disease. Furthermore, in case of overdosing, the action cannot be reversed because of the unavailability of an antidote 44.
Patients with reversible causes of thrombosis should complete a 6-month course of anticoagulation therapy, while those with heritable or acquired thrombotic states continue lifelong anticoagulation.
Despite the risks, anticoagulation remains the mainstay of management, even in those patients with portal venous thrombosis who have cirrhosis and portal hypertension. Anticoagulation helps recanalize the vein. Patients with mesenteric venous thrombosis awaiting liver transplantation who receive anticoagulation experience recanalization in 50% of cases, while those not taking anticoagulation do not experience recanalization of the portal vein. Factors associated with failure of recanalization include splenic vein involvement, ascites, and significant clot burden 13.
Significant clot burden and clinical deterioration warrant invasive intervention 1. Historically, the only option for urgent intervention was open surgery. Interventional radiology can offer precise therapy such as catheter-directed thrombolysis, thrombectomy, and focal administration of pharmacologic agents, including papaverine for vasodilation, or tissue-type plasminogen activator (tPA) or streptokinase for clot lysis. These interventional radiology measures often result in symptomatic improvement and lower bowel resection rates, even with persistent radiographic thrombus 13.
During an interventional radiology procedure, access is obtained percutaneously via a transjugular or transhepatic approach 45, 46. A 4F or 5F angiographic catheter over a 0.035-inch hydrophilic guidewire is used to cross the thrombus. The angiographic catheter is exchanged with a multi-sidehole perfusion catheter, and the tip is placed in the mesenteric vein. If using tissue-type plasminogen activator (tPA), an initial dose of 5 mg is given, followed by continuous tissue-type plasminogen activator (tPA) infusion at 0.5 mg/h. Heparin sodium 40 mg every 12 hours and 80,0000 U/day of urokinase can also be used. A post-procedural venogram is performed. Contraindications for catheter-directed fibrinolysis include intracranial hemorrhage, a history of stroke, primary or metastatic central nervous system disease, recent surgery, trauma, and mesenteric infarction 38, 45, 46.
Open surgery is indicated if a patient becomes septic from ischemic bowel or a perforated viscus. The area of thrombosis is identified, and the affected bowel segment is resected. The goal of surgery is bowel conservation while resecting necrotic segments, and the average length of resection is 50 to 60 cm. Intraoperative Doppler ultrasonography may be used to assess the mesenteric blood supply. The surgeon may return in 24 hours for a second look before completing the anastomosis if there are concerns for ongoing ischemia 10, 43, 47, 48.
Patients with portal hypertension may require intervention such as a transjugular intrahepatic portosystemic shunt (TIPS) to minimize bleeding risks before anticoagulation. The goal of a transjugular intrahepatic portosystemic shunt (TIPS) is mechanical recanalization of the portal vein to maintain flow across the occluded segment. In patients with cirrhosis, a shunt can be created between the left portal vein and the superior mesenteric vein, and splenectomy is effective in those patients with isolated gastric varices from splenic vein thrombosis. Stenting may be required for biliary strictures formed as a consequence of chronic portal vein thrombosis. Rarely a hepaticojejunostomy is required to overcome the stenotic bile ducts 49, 50.
Mesenteric venous thrombosis prognosis
Mesenteric venous thrombosis prognosis depends on the cause of your thrombosis and any damage to your intestine. Getting treatment for the cause before the intestine has died can result in a good recovery.
While overall mortality has decreased due to earlier diagnosis and treatment, mesenteric venous thrombosis remains a life-threatening condition, and a delay in diagnosis directly correlates with worse outcomes. The most common causes of death in patients with mesenteric venous thrombosis are sepsis with multiorgan failure. Other causes of death in patients with mesenteric venous thrombosis include recurrent thrombosis, short bowel syndrome, and pulmonary embolism. Patient age, comorbidities, time to diagnosis, and successful revascularization impact outcomes 38.
The most important factor predicting the short-term (within 30 days) outcome is the presence of bowel infarction. Other factors that have been reported in various series are age, the lack of use of anticoagulation, treatment on a nonsurgical ward, and the presence of colonic ischemia 10, 34, 30, 17, 32.
Acute mesenteric venous thrombosis has a 30-day mortality of up to 32% 36. Timely diagnosis reduces mortality to less than 10%; the mortality rate approaches 60% when diagnosis is delayed 51, 38. If treatment is delayed longer than 24 hours from symptom onset, mortality ranges between 80% and 100% 52. For patients with chronic mesenteric venous thrombosis, 5-year survival rates are 78% to 83%, with outcome usually related to the severity and nature of the underlying condition 33, 20.
The long-term outcome of patients depends on the following factors 9:
- Underlying prothrombotic state. Patients with myeloproliferative neoplasms have the potential for clonal evolution to acute leukemia and myelodysplasia. This risk can be reduced considerably with the use of cytoreductive therapy and hydroxyurea 53. These patients also have poor quality of life including fatigue, bone pain, pruritus, and weight loss 54. Bleeding, usually mild, can occur because of thrombocytopenia or platelet dysfunction.
- Short Bowel Syndrome. Short bowel syndrome occurs in patients with extensive resection and should be avoided by preserving as much of the bowel as possible at laparotomy.
- Recurrent thrombosis. Recurrent thrombosis at any site has been reported in 3% to 40% of patients and within the mesenteric circulation in 0% to 25%. Most recurrences occur within the first 30 days after presentation. Recurrence rates may be as low as 0% to 3% in patients who continue to receive anticoagulation treatment 17, 55. Underlying thrombophilia and oral contraceptive therapy predict recurrent disease 17, 34.
- Bleeding from anticoagulation. Bleeding rates among patients treated with anticoagulation is low at less than 10%, with gastrointestinal bleeding being the most common 17, 34, 16, 56. Varices predict bleeding and if present should be managed as in patients with cirrhosis 34. Such management includes the use of pharmacological therapy with betaβ-blockers or endoscopic ligation of varices. Pharmacological therapy is preferred because variceal ligation may be associated with ligation ulcers and risk of bleeding in patients who are receiving anticoagulants. Unless associated with intracranial bleeding, hemorrhage is rarely the cause of death in patients treated with anticoagulation.
- Sulger E, Dhaliwal HS, Oropallo A, et al. Mesenteric Venous Thrombosis. [Updated 2024 Mar 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459184[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Reintam Blaser A, Mändul M, Björck M, et al. AMESI Investigators (Collaborators). Incidence, diagnosis, management and outcome of acute mesenteric ischaemia: a prospective, multicentre observational study (AMESI Study). Crit Care. 2024 Jan 23;28(1):32. doi: 10.1186/s13054-024-04807-4[↩][↩]
- Wang Y, Zhao R, Xia L, Cui YP, Zhou Y, Wu XT. Predictive Risk Factors of Intestinal Necrosis in Patients with Mesenteric Venous Thrombosis: Retrospective Study from a Single Center. Can J Gastroenterol Hepatol. 2019 May 7;2019:8906803. doi: 10.1155/2019/8906803[↩]
- Brunaud L, Antunes L, Collinet-Adler S, Marchal F, Ayav A, Bresler L, Boissel P. Acute mesenteric venous thrombosis: case for nonoperative management. J Vasc Surg. 2001 Oct;34(4):673-9. https://doi.org/10.1067/mva.2001.117331[↩]
- Alvi AR, Khan S, Niazi SK, Ghulam M, Bibi S. Acute mesenteric venous thrombosis: improved outcome with early diagnosis and prompt anticoagulation therapy. Int J Surg. 2009 Jun;7(3):210-3. https://doi.org/10.1016/j.ijsu.2009.03.002[↩][↩]
- Morasch MD, Ebaugh JL, Chiou AC, Matsumura JS, Pearce WH, Yao JS. Mesenteric venous thrombosis: a changing clinical entity. J Vasc Surg. 2001 Oct;34(4):680-4. https://doi.org/10.1067/mva.2001.116965[↩]
- Wang JS, Yao C, Wang SM, Lv WM, Lin YJ, Li XX. [Clinical analysis of mesenteric venous thrombosis:a report of 23 cases]. Zhonghua Wei Chang Wai Ke Za Zhi. 2005 Nov;8(6):493-5. Chinese.[↩]
- Hotoleanu C, Andercou O, Andercou A. Mesenteric venous thrombosis: clinical and therapeutical approach. Int Angiol. 2008 Dec;27(6):462-5.[↩]
- Singal AK, Kamath PS, Tefferi A. Mesenteric venous thrombosis. Mayo Clin Proc. 2013 Mar;88(3):285-94. https://doi.org/10.1016/j.mayocp.2013.01.012[↩][↩][↩][↩][↩][↩][↩]
- Acosta S, Alhadad A, Svensson P, Ekberg O. Epidemiology, risk and prognostic factors in mesenteric venous thrombosis. Br J Surg. 2008 Oct;95(10):1245-51. doi: 10.1002/bjs.6319[↩][↩][↩]
- Brunaud L, Antunes L, Collinet-Adler S, Marchal F, Ayav A, Bresler L, Boissel P. Acute mesenteric venous thrombosis: case for nonoperative management. J Vasc Surg. 2001 Oct;34(4):673-9. doi: 10.1067/mva.2001.117331[↩][↩][↩][↩][↩]
- Salim S, Zarrouk M, Elf J, Gottsäter A, Sveinsdottir S, Svensson P, Acosta S. Clinical implications of different risk factor profiles in patients with mesenteric venous thrombosis and systemic venous thromboembolism: a population-based study. J Thromb Thrombolysis. 2019 May;47(4):572-577. doi: 10.1007/s11239-019-01816-x[↩]
- Singal AK, Kamath PS, Tefferi A. Mesenteric venous thrombosis. Mayo Clin Proc. 2013 Mar;88(3):285-94. doi: 10.1016/j.mayocp.2013.01.012[↩][↩][↩][↩][↩][↩][↩]
- Gaspary MJ, Auten J, Durkovich D, Gable P. Superior mesenteric vein thrombosis mimicking acute appendicitis. West J Emerg Med. 2011 May;12(2):262-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3099621[↩][↩][↩]
- Duran R, Denys AL, Letovanec I, Meuli RA, Schmidt S. Multidetector CT features of mesenteric vein thrombosis. Radiographics. 2012 Sep-Oct;32(5):1503-22. doi: 10.1148/rg.325115100[↩][↩][↩]
- Kumar S, Kamath PS. Acute superior mesenteric venous thrombosis: one disease or two? Am J Gastroenterol. 2003 Jun;98(6):1299-304. doi: 10.1111/j.1572-0241.2003.07338.x[↩][↩][↩][↩]
- Amitrano L, Guardascione MA, Scaglione M, Pezzullo L, Sangiuliano N, Armellino MF, Manguso F, Margaglione M, Ames PR, Iannaccone L, Grandone E, Romano L, Balzano A. Prognostic factors in noncirrhotic patients with splanchnic vein thromboses. Am J Gastroenterol. 2007 Nov;102(11):2464-70. doi: 10.1111/j.1572-0241.2007.01477.x[↩][↩][↩][↩][↩]
- de Franchis R; Baveno V Faculty. Revising consensus in portal hypertension: report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol. 2010 Oct;53(4):762-8. doi: 10.1016/j.jhep.2010.06.004[↩][↩][↩][↩]
- Dhiman RK, Behera A, Chawla YK, Dilawari JB, Suri S. Portal hypertensive biliopathy. Gut. 2007 Jul;56(7):1001-8. doi: 10.1136/gut.2006.103606[↩]
- Orr DW, Harrison PM, Devlin J, Karani JB, Kane PA, Heaton ND, O’Grady JG, Heneghan MA. Chronic mesenteric venous thrombosis: evaluation and determinants of survival during long-term follow-up. Clin Gastroenterol Hepatol. 2007 Jan;5(1):80-6. doi: 10.1016/j.cgh.2006.09.030[↩][↩]
- Madsen MS, Petersen TH, Sommer H. Segmental portal hypertension. Ann Surg. 1986 Jul;204(1):72-7. doi: 10.1097/00000658-198607000-00010[↩]
- Holl K, Chatain N, Krapp S, Baumeister J, Maié T, Schmitz S, Scheufen A, Brock N, Koschmieder S, Moreno-Andrés D. Calreticulin and JAK2V617F driver mutations induce distinct mitotic defects in myeloproliferative neoplasms. Sci Rep. 2024 Feb 2;14(1):2810. doi: 10.1038/s41598-024-53240-8[↩][↩]
- Marconato R, Nezi G, Capovilla G, Moletta L, Baldan N, Canton SA, Spirch S, Salvador R, Merigliano S. Primary mesenteric vein thrombosis: a case series. J Surg Case Rep. 2020 Mar 24;2020(3):rjaa016. doi: 10.1093/jscr/rjaa016[↩]
- Nielsen C, Birgens HS, Nordestgaard BG, Kjaer L, Bojesen SE. The JAK2 V617F somatic mutation, mortality and cancer risk in the general population. Haematologica. 2011 Mar;96(3):450-3. doi: 10.3324/haematol.2010.033191[↩]
- Thapa B, Fazal S, Parsi M, et al. Myeloproliferative Neoplasms. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK531464[↩]
- Yoshida H, Shimizu T, Yoshioka M, Matsushita A, Kawano Y, Ueda J, Kawashima M, Taniai N, Mamada Y. The Role of the Spleen in Portal Hypertension. J Nippon Med Sch. 2023;90(1):20-25. doi: 10.1272/jnms.JNMS.2023_90-104[↩]
- Mayer P, Venkatasamy A, Baumert TF, Habersetzer F, Pessaux P, Saviano A, Felli E. Left-sided portal hypertension: Update and proposition of management algorithm. J Visc Surg. 2024 Feb;161(1):21-32. doi: 10.1016/j.jviscsurg.2023.11.005[↩]
- Acosta S., Ogren M., Sternby N.H., Bergqvist D., Bjorck M. Clinical implications for the management of acute thromboembolic occlusion of the superior mesenteric artery: Autopsy findings in 213 patients. Ann. Surg. 2005;241:516–522. doi: 10.1097/01.sla.0000154269.52294.57[↩][↩]
- De Stefano V., Martinelli I. Splanchnic vein thrombosis: Clinical presentation, risk factors and treatment. Intern. Emerg. Med. 2010;5:487–494. doi: 10.1007/s11739-010-0413-6[↩]
- Abu-Daff S, Abu-Daff N, Al-Shahed M. Mesenteric venous thrombosis and factors associated with mortality: a statistical analysis with five-year follow-up. J Gastrointest Surg. 2009 Jul;13(7):1245-50. doi: 10.1007/s11605-009-0833-7[↩][↩]
- Zhang J, Duan ZQ, Song QB, Luo YW, Xin SJ, Zhang Q. Acute mesenteric venous thrombosis: a better outcome achieved through improved imaging techniques and a changed policy of clinical management. Eur J Vasc Endovasc Surg. 2004 Sep;28(3):329-34. doi: 10.1016/j.ejvs.2004.06.001[↩][↩]
- Condat B, Pessione F, Helene Denninger M, Hillaire S, Valla D. Recent portal or mesenteric venous thrombosis: increased recognition and frequent recanalization on anticoagulant therapy. Hepatology. 2000 Sep;32(3):466-70. doi: 10.1053/jhep.2000.16597[↩][↩]
- Rhee RY, Gloviczki P. Mesenteric venous thrombosis. Surg Clin North Am. 1997 Apr;77(2):327-38. doi: 10.1016/s0039-6109(05)70552-1[↩][↩][↩][↩]
- Thatipelli MR, McBane RD, Hodge DO, Wysokinski WE. Survival and recurrence in patients with splanchnic vein thromboses. Clin Gastroenterol Hepatol. 2010 Feb;8(2):200-5. doi: 10.1016/j.cgh.2009.09.019[↩][↩][↩][↩][↩]
- Amarapurkar DN, Patel ND, Jatania J. Primary mesenteric venous thrombosis: a study from western India. Indian J Gastroenterol. 2007 May-Jun;26(3):113-7.[↩][↩]
- Stancu B, Chira A, Coman HF, Mihaileanu FV, Ciocan R, Gherman CD, Andercou OA. Intestinal Obstruction as Initial Presentation of Idiopathic Portal and Mesenteric Venous Thrombosis: Diagnosis, Management, and Literature Review. Diagnostics (Basel). 2024 Jan 30;14(3):304. doi: 10.3390/diagnostics14030304[↩][↩][↩][↩][↩][↩]
- Bagley K, Schuller JG. Mesenteric ischemia in the acute care setting. Nursing. 2024 Feb 1;54(2):48-55. doi: 10.1097/01.NURSE.0000998028.77929.e0[↩]
- Russell CE, Wadhera RK, Piazza G. Mesenteric venous thrombosis. Circulation. 2015 May 5;131(18):1599-603. doi: 10.1161/CIRCULATIONAHA.114.012871[↩][↩][↩][↩][↩]
- Kim HS, Patra A, Khan J, Arepally A, Streiff MB. Transhepatic catheter-directed thrombectomy and thrombolysis of acute superior mesenteric venous thrombosis. J Vasc Interv Radiol. 2005 Dec;16(12):1685-91. doi: 10.1097/01.RVI.0000182156.71059.B7[↩]
- Kunychka M, Váňa J, Žáček M, Chromčiková M. Acute mesenteric ischemia – a persistent problem. Rozhl Chir. 2023;102(6):228-235. English. doi: 10.33699/PIS.2023.102.6.228-235[↩]
- Bayraktar Y, Harmanci O. Etiology and consequences of thrombosis in abdominal vessels. World J Gastroenterol. 2006 Feb 28;12(8):1165-74. doi: 10.3748/wjg.v12.i8.1165[↩]
- Nielsen C, Lindholt JS, Erlandsen EJ, Mortensen FV. d-lactate as a marker of venous-induced intestinal ischemia: an experimental study in pigs. Int J Surg. 2011;9(5):428-32. doi: 10.1016/j.ijsu.2011.04.004[↩]
- Morasch MD, Ebaugh JL, Chiou AC, Matsumura JS, Pearce WH, Yao JS. Mesenteric venous thrombosis: a changing clinical entity. J Vasc Surg. 2001 Oct;34(4):680-4. doi: 10.1067/mva.2001.116965[↩][↩]
- Maan A, Padmanabhan R, Shaikh AY, Mansour M, Ruskin JN, Heist EK. Newer anticoagulants in cardiovascular disease: a systematic review of the literature. Cardiol Rev. 2012 Sep-Oct;20(5):209-21. doi: 10.1097/CRD.0b013e3182503e2d[↩]
- Barah A, Al-Hashimi I, Kassamali R, Aldebyani Q, Almokdad O, Elmagdoub A, Khader M, Rehman SU, Omar A. Catheter-Directed Thrombolysis in the treatment of acute Portomesenteric Vein Thrombosis after Laparoscopic Sleeve Gastrectomy. Thromb J. 2022 Sep 29;20(1):57. doi: 10.1186/s12959-022-00415-w[↩][↩]
- Gao Z, Yin L, Pan Y, Chen B. Treatment of Superior Mesenteric Vein Thrombus by Catheter-Directed Thrombolysis. Ann Vasc Surg. 2020 May;65:286.e9-286.e13. doi: 10.1016/j.avsg.2019.11.021[↩][↩]
- Kaplan JL, Weintraub SL, Hunt JP, Gonzalez A, Lopera J, Brazzini A. Treatment of superior mesenteric and portal vein thrombosis with direct thrombolytic infusion via an operatively placed mesenteric catheter. Am Surg. 2004 Jul;70(7):600-4.[↩]
- Kozuch PL, Brandt LJ. Review article: diagnosis and management of mesenteric ischaemia with an emphasis on pharmacotherapy. Aliment Pharmacol Ther. 2005 Feb 1;21(3):201-15. doi: 10.1111/j.1365-2036.2005.02269.x[↩]
- Liu X, Wang Y, Zheng L, Zhu J. Risk factors analysis of endoscopy and TIPS in the treatment of secondary esophagogastric varicose bleeding with cirrhosis. Afr Health Sci. 2023 Sep;23(3):655-663. doi: 10.4314/ahs.v23i3.76[↩]
- Shalvoy MR, Ahmed M, Weinstein JL, Ramalingam V, Malik MS, Ali A, Shenoy-Bhangle AS, Curry MP, Sarwar A. Transjugular Intrahepatic Portosystemic Shunt and Thrombectomy (TIPS-Thrombectomy) for Symptomatic Acute Noncirrhotic Portal Vein Thrombosis. J Vasc Interv Radiol. 2023 Aug;34(8):1373-1381.e3. doi: 10.1016/j.jvir.2023.05.009[↩]
- Schoots IG, Koffeman GI, Legemate DA, Levi M, van Gulik TM. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. 2004 Jan;91(1):17-27. doi: 10.1002/bjs.4459[↩]
- Klar E, Rahmanian PB, Bücker A, Hauenstein K, Jauch KW, Luther B. Acute mesenteric ischemia: a vascular emergency. Dtsch Arztebl Int. 2012 Apr;109(14):249-56. doi: 10.3238/arztebl.2012.0249[↩]
- Björkholm M, Derolf AR, Hultcrantz M, Kristinsson SY, Ekstrand C, Goldin LR, Andreasson B, Birgegård G, Linder O, Malm C, Markevärn B, Nilsson L, Samuelsson J, Granath F, Landgren O. Treatment-related risk factors for transformation to acute myeloid leukemia and myelodysplastic syndromes in myeloproliferative neoplasms. J Clin Oncol. 2011 Jun 10;29(17):2410-5. doi: 10.1200/JCO.2011.34.7542[↩]
- Mesa RA, Niblack J, Wadleigh M, Verstovsek S, Camoriano J, Barnes S, Tan AD, Atherton PJ, Sloan JA, Tefferi A. The burden of fatigue and quality of life in myeloproliferative disorders (MPDs): an international Internet-based survey of 1179 MPD patients. Cancer. 2007 Jan 1;109(1):68-76. doi: 10.1002/cncr.22365[↩]
- Dentali F, Ageno W, Witt D, Malato A, Clark N, Garcia D, McCool K, Siragusa S, Dyke S, Crowther M; WARPED consortium. Natural history of mesenteric venous thrombosis in patients treated with vitamin K antagonists: a multi-centre, retrospective cohort study. Thromb Haemost. 2009 Sep;102(3):501-4. doi: 10.1160/TH08-12-0842[↩]
- Plessier A, Darwish-Murad S, Hernandez-Guerra M, Consigny Y, Fabris F, Trebicka J, Heller J, Morard I, Lasser L, Langlet P, Denninger MH, Vidaud D, Condat B, Hadengue A, Primignani M, Garcia-Pagan JC, Janssen HL, Valla D; European Network for Vascular Disorders of the Liver (EN-Vie). Acute portal vein thrombosis unrelated to cirrhosis: a prospective multicenter follow-up study. Hepatology. 2010 Jan;51(1):210-8. doi: 10.1002/hep.23259[↩]





{kind=link}