Contents
Trichoepithelioma
Trichoepitheliomas are rare, noncancerous (benign) skin tumors that grow from hair follicles on your face or scalp, but can also appear on your body, arms, legs, or vulva 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14. Trichoepithelioma is classified as a benign adnexal tumor from hair follicles and most commonly appears as either a solitary lesion or multiple nodules 15. Trichoepitheliomas are usually skin-colored, translucent, and appear as smooth, round bumps or nodules measuring less than 1 cm in diameter. Trichoepitheliomas may also be blue, brown, flesh-colored, pink or yellow. Trichoepitheliomas are generally benign, but can rarely develop into basal cell carcinoma (BCC).
Trichoepitheliomas are usually asymptomatic and don’t itch or ulcerate are generally considered harmless. Trichoepitheliomas can appear as a single lesion or multiple nodules. Inherited forms of trichoepithelioma in Brooke-Spiegler syndrome appear as multiple lesions. Multiple trichoepitheliomas typically start to develop in your early childhood or around puberty while solitary trichoepitheliomas often present in the second or third decades of your of life. Brooke-Spiegler syndrome predominantly affects young women (male-to-female ratio of 1:6-9.6). Overall, trichoepitheliomas are most often diagnosed in adult women 15.
Trichoepitheliomas can be inherited due to mutations in the CYLD gene. The CYLD gene provides instructions for making CYLD enzyme called CYLD lysine 63 deubiquitinase that helps regulate numerous signaling pathways, many of which are involved in cell growth 16. These pathways include nuclear factor-kappa-B (NF-KB), Wnt, c-Jun N-terminal kinase (JNK), transforming growth factor beta-1 (TGFB1), and Notch signaling pathways 16. By regulating these signaling pathways, the CYLD lysine 63 deubiquitinase enzyme helps cells respond properly to signals that promote cell growth and division (proliferation) or self-destruction (apoptosis), as necessary. By regulating signals that control cell growth, the CYLD lysine 63 deubiquitinase (CYLD) enzyme acts as a tumor suppressor, which means that it helps prevent cells from growing and dividing too fast or in an uncontrolled way.
Trichoepithelioma can also occur sporadically and the exact cause of sporadic forms of trichoepithelioma is unknown. Most sporadic trichoepithelioma present in adults aged 40 or older 13.
The exact incidence and prevalence of trichoepithelioma in the general population as well as familial genetic syndromes are not known, but cases are rare 13. However, one dermatopathology lab in the United States reported 2.14–2.75 cases of trichoepithelioma per year 15.
Trichoepitheliomas can be safely removed surgically. Other treatments include dermal abrasion, laser surgery, and curettage. Topical 5% imiquimod cream or retinoic acid may also be used.
Figure 1. Hair follicle and skin anatomy
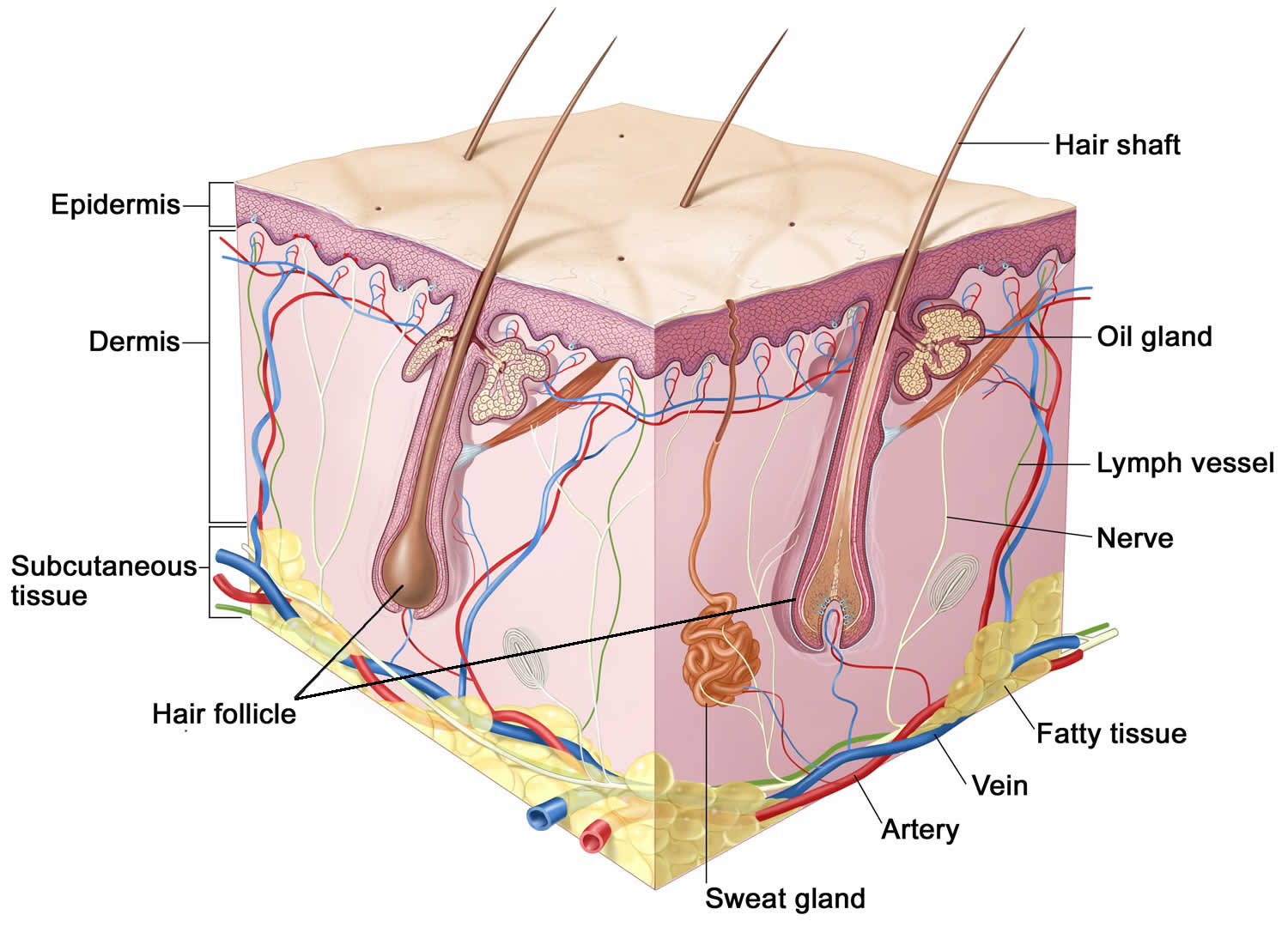
Figure 2. Trichoepithelioma

Footnotes: A 28-year-old female patient presented to her doctor with multiple skin-colored papules on her face that had been present for 15 years prior to visiting the clinic. The patient reported that her mother, maternal uncles, and maternal cousins had similar lesions on their face, scalp, and body. Right and left sides of her face has multiple trichoepitheliomas on the bilateral nasolabial fold, upper lip, and alar rim (side of the nose near the nostril).
[Source 17 ]Figure 3. Solitary trichoepithelioma

Figure 4. Multiple familial trichoepithelioma

Figure 5. Desmoplastic trichoepithelioma

Figure 6. Ttrichoepithelioma pathology
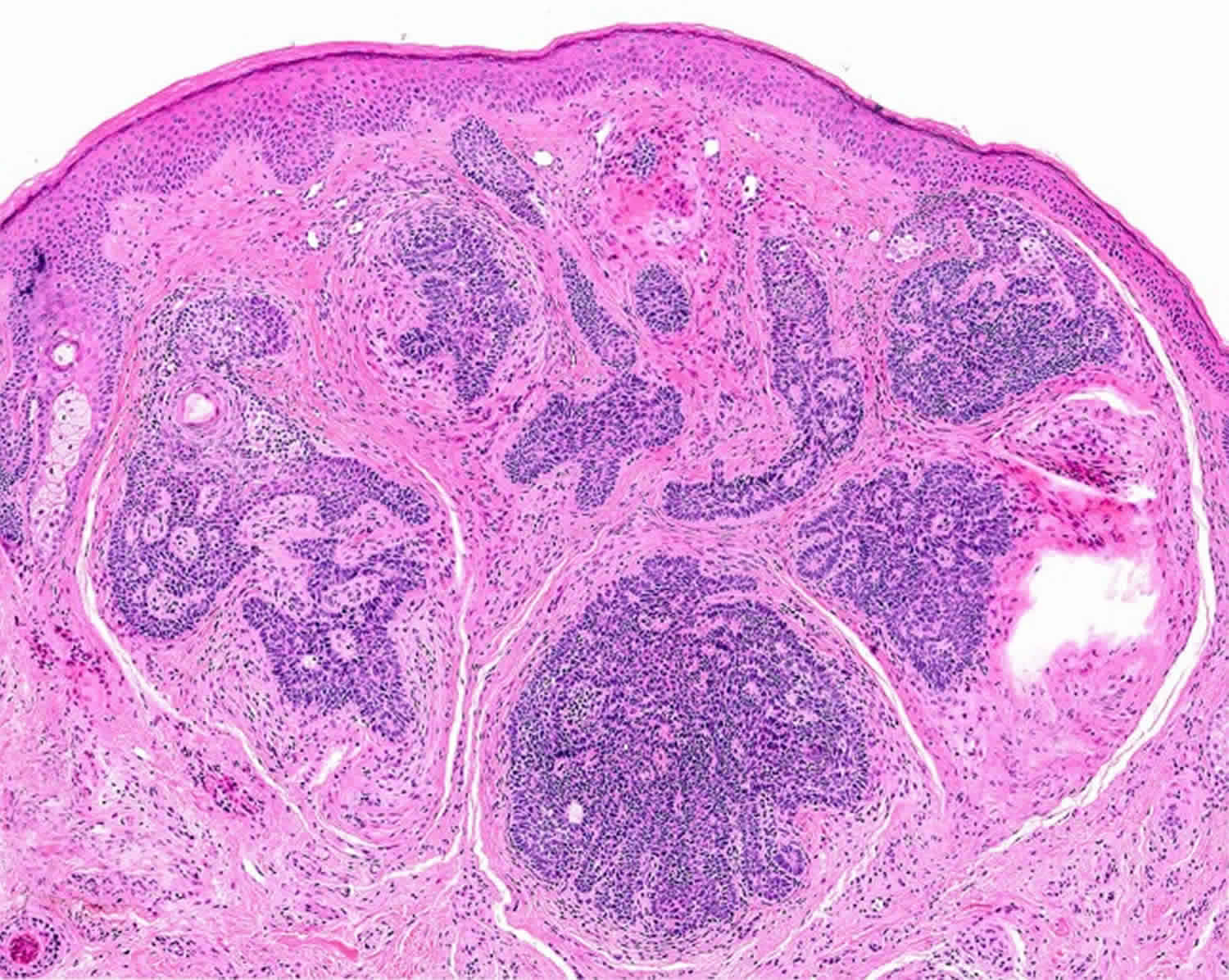
Footnotes: Trichoepithelioma has two components, namely the follicular germinative epithelium and the specific follicular stroma. The epithelial component is composed of bland basaloid cells arranged in a cribriform pattern, whereas the stroma resembles follicular papillae and the perifollicular sheath.
[Source 12 ]Who gets a trichoepithelioma?
Poeple with Brooke-Spiegler syndrome developed multiple trichoepitheliomas, and cylindromas on their skin. Brooke-Spiegler syndrome (BRSS or BSS), also known as CYLD cutaneous syndrome, Ancell-Spiegler cylindromas or Spiegler-Brooke syndrome, is a rare genetic skin condition that causes tumors derived from skin appendages (hair follicle tumors and sweat gland tumors) often on your face, neck and scalp 18, 19, 20, 21, 12, 22, 23, 24, 17, 25, 26, 27. The hair follicle tumors and sweat gland tumors may also grow on other parts of your body. Brooke–Spiegler syndrome (BSS) is characterized by the growth of cylindromas, spiradenomas, trichoepitheliomas, or their combination. Brooke-Spiegler syndrome (BSS) includes familial cylindromatosis and multiple familial trichoepitheliomas (MFT). The tumors often appear in your teens and early 20s. Brooke-Spiegler syndrome tumors are usually noncancerous (benign), though they sometimes become cancerous (malignant) over time 28. Although malignant transformation is rare, it should be considered in cases of rapid enlargement and bleeding 21. Large, noncancerous tumors may become open wounds and at risk of infection.
Brooke-Spiegler syndrome is an autosomal dominant disorder. This means that one of your parents is a carrier of Brooke-Spiegler syndrome and will have symptoms of the condition. You usually inherit Brooke-Spiegler syndrome from your biological parents (a genetic condition). As their child, there’s a 50% chance that you’ll also have Brooke-Spiegler syndrome. But sometimes, people with Brooke-Spiegler syndrome have no family history of the condition.
In order to diagnose Brooke-Spiegler syndrome, your doctor will first ask about your symptoms, medical history and family medical history. He/she will also do a physical exam. Brooke-Spiegler syndrome may be suspected if you have a family history of multiple benign skin tumors. Other skin tumor such as cylindromas, trichoepitheliomas and spiradenomas are difficult to distinguish clinically. Therefore skin biopsy is required to confirm the diagnosis. During a skin biopsy your doctor will remove a sample of cells within a tumor. Then, they send the sample to a laboratory for examination under a microscope. Your doctor may also suggest genetic testing. This test can find changes in your genes that cause Brooke-Spiegler syndrome.
Unfortunately, there’s no cure for Brooke-Spiegler syndrome. Although Brooke-Spiegler syndrome doesn’t go away, surgery and other treatments can help. With proper treatment, most people with Brooke-Spiegler syndrome can continue to lead full and active lives.
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://findageneticcounselor.nsgc.org) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://abgc.learningbuilder.com/Search/Public/MemberRole/Verification) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (https://www.acmg.net/ACMG/Directories.aspx) has a searchable database of medical genetics clinic services in the United States.
How common is Brooke-Spiegler syndrome?
Brooke-Spiegler syndrome is a rare condition. Researchers estimate that Brooke-Spiegler syndrome affects roughly 1 out of every 100,000 people. The estimated incidence of Brooke–Spiegler syndrome (BSS) is approximately 1 in 100,000 in the UK 29.
Who might have Brooke-Spiegler syndrome?
People of every age, race and sex can have Brooke-Spiegler syndrome. But you’re more at risk of Brooke-Spiegler syndrome if one of your parents carries the genetic mutation for Brooke-Spiegler syndrome.
Brooke-Spiegler syndrome is an autosomal dominant disorder. This means that one of your parents is a carrier of Brooke-Spiegler syndrome and will have symptoms of the condition. You usually inherit Brooke-Spiegler syndrome from your biological parents (a genetic condition). As their child, there’s a 50% chance that you’ll also have Brooke-Spiegler syndrome. But sometimes, people with Brooke-Spiegler syndrome have no family history of the condition.
Most people first show Brooke-Spiegler syndrome symptoms as teenagers or young adults. The number of tumors often starts to increase when you’re in your 30s or 40s 21. Females often have more tumors than males.
How can I reduce my risk of Brooke-Spiegler syndrome?
Unfortunately, you can’t reduce your risk of Brooke-Spiegler syndrome. But treatment can help reduce the number and size of tumors you have.
How does Brooke-Spiegler syndrome differ from neurofibromatosis?
Both Brooke-Spiegler syndrome and neurofibromatosis are genetic conditions that cause primarily benign tumors. But Brooke-Spiegler syndrome causes tumors mainly on your skin, while neurofibromatosis causes tumors both on and under your skin and along your nerves.
There are 3 types of neurofibromatosis:
- Neurofibromatosis type 1 (NF1), where tumors (neurofibromas) form on or under your skin.
- Neurofibromatosis type 2 (NF2), where tumors (schwannomas) form on the nerves of your brain and spinal cord (peripheral nervous system). These tumors often affect the nerves that control hearing (auditory nerves).
- Schwannomatosis, where schwannomas form on nerves in your peripheral nervous system. These tumors usually don’t affect your auditory nerves.
Trichoepithelioma causes
Trichoepithelioma is caused by the benign (non-cancerous) growth of epithelial-mesenchymal cells (basal cells) of the hair follicles 30, 15. There are 3 variants: solitary, multiple, and desmoplastic trichoepithelioma 15.
- Solitary trichoepithelioma nodules are the least common and usually spare the eyelids. Solitary trichoepithelioma nodules do not follow an inheritance pattern and occur due to mutation in the PTCH tumor suppressor gene 31, 32, 15.
- Multiple nodular trichoepitheliomas are the most common type, and can occur as part of Multiple Familial Trichoepithelioma (MFT), an uncommon autosomal dominant disorder 33, 34, 35, 36, 37. Initial reports linked Multiple Familial Trichoepithelioma (MFT) to chromosome 9p21, but recent reports have found mutations in cylandromatosis tumor suppressor gene (CYLD), which maps to chromosome 16q12-q13 in most of the cases. Mutation in the CYLD gene gives rise to Multiple Familial Trichoepithelioma (MFT) indistinguishable from phenotype assigned to 9p21 38. For example, Brooke-Spiegler syndrome is caused by a mutation in the CYLD oncogene and present with hair follicle tumors and sweat gland tumors (trichoepitheliomas, spiradenomas and cylindromas) 39.
- Desmoplastic trichoepitheliomas arise from cells lining the hair follicle. Desmoplastic trichoepitheliomas usually present as a single lesion and most commonly affect the face. Desmoplastic trichoepitheliomas often present as a single discrete white papule with a central indentation on the cheek 1. Typically, desmoplastic trichoepitheliomas lack ulceration and are superficial in nature, developing slowly on the face or cheeks of middle-aged females 40. Desmoplastic trichoepitheliomas are caused by a mutation in the 9p21 and 16q12-q13 chromosome 15. Their most common driver mutations are due to either congenital or acquired loss-of-function mutations in the CYLD (CYLD lysine 63 deubiquitinase) gene 40.
Trichoepitheliomas may be associated with a familial genetic condition called multiple familial trichoepithelioma (MFT). Multiple familial trichoepithelioma (MFT) is a disorder linked to two autosomal dominant mutations affecting tumor suppressor genes. The first gene is on the long arm of chromosome 9q21 13.
The second is the cylindromatous tumor suppressor gene (CYLD) on chromosome 16q12-q13, which is also the gene implicated in Brooke-Spiegler syndrome 13. This leads to a loss of function of the deubiquitinating enzyme CYLD, which results in elevated NFκB signaling. These patients present with multiple trichoepitheliomas beginning in adolescence/early adulthood 13.
Desmoplastic trichoepithelioma
Desmoplastic trichoepithelioma is a harmless facial skin lesion. It is an uncommon form of trichoepithelioma, with a reported incidence of 1 in 5000 skin biopsies in a cohort of British adults. It has also been called ‘sclerosing epithelial hamartoma’.
Desmoplastic trichoepithelioma grows from cells lining the hair follicle. It is classified as a benign adnexal or hair follicle tumor.
Desmoplastic trichoepithelioma is most often identified in middle-aged females, although it may also occur at other ages and in males. A lesion may have been present for many years before being brought to medical attention.
Desmoplastic trichoepithelioma typically present as a firm skin-colored to red, annular (ring-shaped) plaque with a central dimple. It is usually found on the upper cheek. Desmoplastic trichoepithelioma is stable or may slowly grow up to 1 cm in diameter. Multiple lesions are quite rare.
Desmoplastic trichoepithelioma treatment
True desmoplastic trichoepithelioma is a benign tumor with no malignant potential, so there is no need to remove them. However, it is best to keep the lesion under observation in case the diagnosis is incorrect, as basal cell carcinoma may look very similar.
Treatment options include:
- Curettage and electrodesiccation
- Surgical excision
- Mohs micrographic surgery, which ensures clear margins.
Multiple familial trichoepithelioma
Multiple familial trichoepithelioma is a genetic disorder characterized by multiple smooth, round, firm, skin-colored tumors (trichoepitheliomas) that usually occur on the face, but may also occur on the scalp, neck, and trunk 41. The tumors are from immature hair follicles 42. They usually first develop during childhood or adolescence and may grow larger and increase in number over time 43. The genetic disorder can be caused by mutations in the CYLD gene or by mutations in other genes which are still unknown. The condition may be divided in two subtypes, multiple familial trichoepithelioma type 1 and multiple familial trichoepithelioma type 2. Susceptibility to multiple familial trichoepithelioma is inherited in an autosomal dominant fashion, which means one copy of the mutated gene in each cell increases the risk of developing this disorder. However, a second, non-inherited (acquired) mutation is required for the tumors to develop in this disorder.
People with multiple familial trichoepithelioma typically develop large numbers of smooth, round, firm skin-colored tumors called trichoepitheliomas, which arise from hair follicles 42. These benign (noncancerous) tumors may occasionally transform into a type of skin cancer called basal cell carcinoma 44. Occasionally, other types of tumors, including growths called spiradenomas (which originate in sweat glands) and cylindromas (which likely originate in hair follicles) also develop. Affected people are also at risk of developing tumors in other tissues, particularly benign tumors of the salivary glands 41.
The tumors in multiple familial trichoepithelioma typically first appear during childhood or adolescence. They appear most often around the nose, forehead, and upper lip. Occasionally they occur on the scalp, neck, and upper trunk. They may grow larger and increase in number over time 41. In rare cases, the tumors may get in the way of the eyes, ears, nose, or mouth and affect vision or hearing. The growths can be disfiguring and may cause depression or other psychological problems. For reasons that remain unknown, females are often more severely affected than males 41.
Treatment often involves surgery to remove a single lesion and cryosurgery or laser surgery for multiple ones 45.
Multiple familial trichoepithelioma cause
Multiple familial trichoepithelioma can be caused by mutations in the CYLD gene which is found on chromosome 16 46. It is thought to be inherited in an autosomal dominant fashion with reduced penetrance. Autosomal dominant means that a single mutation in one copy of a gene is sufficient to cause the condition. Reduced penetrance means that not everyone with the gene mutation will develop symptoms of the condition 43.
Susceptibility to multiple familial trichoepithelioma has an autosomal dominant pattern of inheritance. This means that one mutated copy of the CYLD gene in each cell increases the risk that a person will develop the multiple familial trichoepithelioma. However, a second, non-inherited (acquired) mutation is needed for development of the skin tumors characteristic of this condition 41.
Do people with multiple familial trichoepithelioma always have affected family members?
Multiple familial trichoepithelioma is thought to be due to a single mutation in the CYLD gene or in another gene which has yet to be identified. A number of case reports of families with multiple familial trichoepithelioma demonstrating an autosomal dominant pattern of inheritance have been reported in the medical literature. Still, as with other autosomal dominant conditions, it is possible for a new mutation to occur for the first time in a family in an affected individual. For example a CYLD gene mutation may occur spontaneously for the first time in an egg or sperm or in the fertilized egg sometime after conception. This phenomenon is called a de novo or “new” mutation. A person with a new mutation would not be expected to have other affected family members.
In addition, some literature suggests that mutations that cause multiple familial trichoepithelioma may have reduced penetrance. This means that a person may inherit the disease causing mutation, yet never develop symptoms of the condition. As a result it is possible for a person with multiple familial trichoepithelioma to have a parent or other relative with the disease causing mutation, but with no symptoms of the condition.
If you have concerns about if and how multiple familial trichoepithelioma may be running in your family, we recommend that you speak with a genetics professional.
To find a medical professional who specializes in genetics, you can ask your doctor for a referral or you can search for one yourself. Online directories are provided by the American College of Medical Genetics (https://www.acmg.net/) and the National Society of Genetic Counselors (https://www.findageneticcounselor.com/).
Multiple familial trichoepithelioma diagnosis
A diagnosis of multiple familial trichoepithelioma is made based on the symptoms in the patient, the patient’s family history, and the appearance of the trichoepithelioma cells under a microscope (histology) 42. Multiple familial trichoepithelioma must be distinguished from basal cell carcinoma (cancerous tumor) and other rare genetic syndromes such as Cowden syndrome.
Multiple familial trichoepithelioma treatment
Several therapies have been used to treat multiple trichoepitheliomas, with variable to poor results. A single trichoepithelioma may be treated with surgery. Cryosurgery or laser surgery may be used to remove multiple trichoepitheliomas 43. Imiquimod cream has also been used as a treatment for trichoepitheliomas, with some improvement in symptoms 47. Other treatments have included dermabrasion, photodynamic therapy, and other medications 48. However, in most cases, multiple trichoepitheliomas eventually regrow following treatment 49.
Trichoepithelioma signs and symptoms
Trichoepitheliomas are rare, noncancerous (benign) skin tumors that grow from hair follicles on your face or scalp, but can also appear on your body, arms, legs, or vulva 12. Trichoepitheliomas are typically seen on your face, particularly your upper lip, nasolabial folds, nose, eyelids, and forehead. They are sometimes also seen on the scalp, neck, upper torso, or elsewhere on the body, and can be pink-blue in color with a symmetrical distribution.
Trichoepitheliomas are usually skin-colored, translucent, and appear as smooth, round bumps or nodules measuring less than 1 cm in diameter. Trichoepitheliomas may also be blue, brown, flesh-colored, pink or yellow.
The desmoplastic trichoepithelioma is a solitary ring-shaped lesion which can mimic the appearance of a basal cell carcinoma (BCC).
Since basal cell carcinoma (BCC) and trichoepithelioma share a wide range of clinical and histopathological features, misdiagnosing trichoepithelioma as BCC is not uncommon 2.
Trichoepithelioma complications
Trichoepitheliomas are generally benign, but can rarely develop into basal cell carcinoma (BCC) 5. Trichoepitheliomas can undergo transformation to basal cell carcinoma (BCC) and usually occurs in the setting of multiple trichoepitheliomas, but there are reported cases of sporadic trichoepithelioma in association with BCC 50, 51.
Other complications of a trichoepithelioma may include:
- Recurrence (rare) after surgical removal. As trichoepitheliomas are benign entities, surgical excision is curative with a minimal likelihood of disease recurrence or metastasis.
- Psychosocial implications. Sometimes, the skin tumors may grow larger and be disfiguring. These symptoms can lead to depression.
- Surgical complications (scarring and hypopigmentation)
Trichoepithelioma diagnosis
In order to diagnose trichoepithelioma, your doctor will first ask about your symptoms, medical history and family medical history. He/she will also do a physical exam. Brooke-Spiegler syndrome may be suspected if you have a family history of multiple benign skin tumors. Other skin tumor such as cylindromas and spiradenomas are difficult to distinguish clinically. Therefore skin biopsy or surgical excision is required to confirm the diagnosis. Full-thickness skin biopsy via shave, punch, incisional, or excisional biopsy is advised 52. During a skin biopsy your doctor will remove a sample of cells within a tumor. Then, they send the sample to a laboratory for examination under a microscope. In challenging cases, cytokeratin 20 (CK20) can distinguish trichoepithelioma from basal cell carcinoma (BCC), as this marker routinely stains Merkel cells in benign, hair-germ tumors 13. The cytokeratin 20 (CK20) stain may be used alongside androgen receptor staining when evaluating trichoepithelioma versus BCC, as androgen receptor positivity (with CK20 negativity) suggests basal cell carcinoma (BCC). However, androgen receptor positivity may be focal or completely absent in some cases of BCC.
Your doctor may also suggest genetic testing. This test can find changes in your genes that cause Brooke-Spiegler syndrome.
Trichoepithelioma treatment
Trichoepithelioma treatment options include:
- Excision or shave biopsy / surgical removal clear margins. Excision biopsy refers to the removal of a skin lesion by completely cutting it out 53.
- Cryotherapy, where extreme cold freezes tumor tissue.
- Dermabrasion, where a rotating instrument removes the top layer of your skin.
- Curettage. Curettage is a type of electrosurgery in which a skin lesion is scraped off and heat is applied to the skin surface.
- Radiofrequency ablation. Radiofrequency ablation (RFA) is a minimally invasive procedure that uses radio waves to create heat and destroy tissue.
- Laser therapy. Erbium:yttrium-aluminum-garnet (Er:YAG) laser or CO2 laser ablation.
Other treatment modalities may involve using CO2 laser treatment and topical 1% sirolimus cream as suppressive therapy to treat patients with multiple trichoepitheliomas 54. A study compared neodymiumdoped:YAG, Er:YAG, and CO2 laser treatment and saw significant improvements in skin rejuvenation using the neodymium-doped:YAG laser 55.
Trichoepithelioma prognosis
Most people with solitary trichoepithelioma have an excellent prognosis 13. After excision of solitary nodules, recurrence is very rare. However, as trichoepithelioma has a similar histology to basal cells, there is a small risk of malignant transformation into basal cell carcinoma (BCC). Furthermore, the likelihood of lesion recurrence dramatically increases in patients with familial genetic syndromes such as Brooke-Spiegler syndrome 13.
- Khan H, Mpyisi L, Azzam MJ, Braudis K. Infiltrative Basal Cell Carcinoma (iBCC) Adjacent to a Desmoplastic Trichoepithelioma (DTE): A Case Report and Literature Review of iBCCs and DTEs. Cureus. 2024 Jun 7;16(6):e61893. doi: 10.7759/cureus.61893[↩][↩]
- Ahmad A, Salman FM, Jeragh F, Dashti Y. Enemy in disguise: A case report of solitary trichoepithelioma initially diagnosed as BCC. Int J Surg Case Rep. 2023 Feb;103:107897. doi: 10.1016/j.ijscr.2023.107897[↩][↩]
- Rahman J, Tahir M, Arekemase H, Murtazaliev S, Sonawane S. Desmoplastic Trichoepithelioma: Histopathologic and Immunohistochemical Criteria for Differentiation of a Rare Benign Hair Follicle Tumor From Other Cutaneous Adnexal Tumors. Cureus. 2020 Aug 12;12(8):e9703. doi: 10.7759/cureus.9703[↩]
- Kallam AR, Satyanarayana MA, Aryasomayajula S, Krishna BA. Basal Cell Carcinoma Developing from Trichoepithelioma: Review of Three Cases. J Clin Diagn Res. 2016 Mar;10(3):PD17-9. doi: 10.7860/JCDR/2016/15432.7464[↩]
- Sangwaiya A, Sharma J, Sharma S, Munghate A, Samal S, Sen R. Multiple Familial Trichoepithelioma with an Adjacent Basal Cell Carcinoma, Transformation or Collision – A Case Report and Review of Literature. Indian J Dermatol. 2015 May-Jun;60(3):280-3. doi: 10.4103/0019-5154.156380[↩][↩]
- Brinkhuizen T, Weijzen CA, Eben J, Thissen MR, van Marion AM, Lohman BG, Winnepenninckx VJ, Nelemans PJ, van Steensel MA. Immunohistochemical analysis of the mechanistic target of rapamycin and hypoxia signalling pathways in basal cell carcinoma and trichoepithelioma. PLoS One. 2014 Sep 2;9(9):e106427. doi: 10.1371/journal.pone.0106427[↩]
- Gupta A, Ali MJ, Mishra DK, Naik MN. Solitary Trichoepithelioma of the Eyelid: A Clinico-Pathological Correlation. Int J Trichology. 2015 Apr-Jun;7(2):80-1. doi: 10.4103/0974-7753.160119[↩]
- Navarrete-Dechent C, Bajaj S, Marghoob AA, González S, Muñoz D. Multiple familial trichoepithelioma: confirmation via dermoscopy. Dermatol Pract Concept. 2016 Jul 31;6(3):51-4. doi: 10.5826/dpc.0603a10[↩]
- Hihara M, Kouchi Y, Takao T, Fujita M, Kakudo N. Morpheaform basal cell carcinoma of the nasal ala associated with multiple familial trichoepithelioma reconstructed by anterolateral thigh flap: a case report. Case Reports Plast Surg Hand Surg. 2023 Aug 2;10(1):2242494. doi: 10.1080/23320885.2023.2242494[↩]
- Mohammadi AA, Seyed Jafari SM. Trichoepithelioma: a rare but crucial dermatologic issue. World J Plast Surg. 2014 Jul;3(2):142-5. https://pmc.ncbi.nlm.nih.gov/articles/PMC4236999[↩]
- Greywal T, Rubin AG, Jiang B. A Rare Presentation of Basal Cell Carcinoma Arising within Trichoepithelioma: A Diagnostic Challenge. Cureus. 2019 Aug 16;11(8):e5401. doi: 10.7759/cureus.5401[↩]
- Kazakov DV. Brooke-Spiegler Syndrome and Phenotypic Variants: An Update. Head Neck Pathol. 2016 Jun;10(2):125-30. doi: 10.1007/s12105-016-0705-x[↩][↩][↩][↩]
- Schukow C, Ahmed A. Trichoblastoma and Trichoepithelioma. [Updated 2023 Mar 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK589680[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Putnam AR, Thompson KS, Wallentine JC. Diagnostic Pathology: Pediatric Neoplasms. Elsevier; 2018. Trichoepithelioma; pp. 42–45.[↩]
- Trichoepithelioma. https://dermnetnz.org/topics/trichoepithelioma[↩][↩][↩][↩][↩][↩][↩]
- CYLD gene. https://medlineplus.gov/genetics/gene/cyld[↩][↩]
- Thomas LW, Pham CT, Coakley B, Lee P. Treatment of Brooke-Spiegler Syndrome Trichoepitheliomas with Erbium: Yttrium-Aluminum-Garnet Laser: A Case Report and Review of the Literature. J Clin Aesthet Dermatol. 2020 Jul;13(7):41-44. https://pmc.ncbi.nlm.nih.gov/articles/PMC7492015[↩][↩]
- Mohiuddin W, Laun J, Cruse W. Brooke-Spiegler Syndrome. Eplasty. 2018 Jul 23;18:ic14. https://pmc.ncbi.nlm.nih.gov/articles/PMC6062842[↩]
- Young AL, Kellermayer R, Szigeti R, Tészás A, Azmi S, Celebi JT. CYLD mutations underlie Brooke-Spiegler, familial cylindromatosis, and multiple familial trichoepithelioma syndromes. Clin Genet. 2006;70(3):246–9. doi: 10.1111/j.1399-0004.2006.00667.x[↩]
- Trufant J, Robinson M, Patel R. Brooke-Spiegler syndrome. Dermatol Online J. 2012 Dec 15;18(12):16. https://escholarship.org/uc/item/4b04h9p3[↩]
- Kim C, Kovich OI, Dosik J. Brooke-Spiegler syndrome. Dermatol Online J. 2007 Jan 27;13(1):10. https://escholarship.org/uc/item/4fj5p51c[↩][↩][↩]
- Brooke-Spiegler syndrome. https://dermnetnz.org/topics/brooke-spiegler-syndrome[↩]
- Brooke-Spiegler Syndrome. https://my.clevelandclinic.org/health/diseases/brooke-spiegler-syndrome[↩]
- Manchanda K, Bansal M, Bhayana AA, Pandey S. Brooke-spiegler syndrome: a rare entity. Int J Trichology. 2012 Jan;4(1):29-31. doi: 10.4103/0974-7753.96084[↩]
- Rathi M, Awasthi S, Budania SK, Ahmad F, Dutta S, Kumar A. Brooke-spiegler syndrome: a rare entity. Case Rep Pathol. 2014;2014:231895. doi: 10.1155/2014/231895[↩]
- Sicinska J, Rakowska A, Czuwara-Ladykowska J, Mroz A, Lipinski M, Nasierowska-Guttmejer A, Sikorska J, Sklinda K, Slowinska M, Kowalska-Oledzka E, Walecka I, Walecki J, Rudnicka L. Cylindroma transforming into basal cell carcinoma in a patient with Brooke-Spiegler syndrome. J Dermatol Case Rep. 2007 Dec 29;1(1):4-9. doi: 10.3315/jdcr.2007.1.1002[↩]
- Brambullo T, De Lazzari A, Franchi A, Trevisson E, Garau ML, Scarmozzino F, Vindigni V, Bassetto F. A Misdiagnosed Familiar Brooke-Spiegler Syndrome: Case Report and Review of the Literature. J Clin Med. 2024 Apr 12;13(8):2240. doi: 10.3390/jcm13082240[↩]
- De Francesco V, Frattasio A, Pillon B, Stinco G, Scott CA, Trotter D, et al. Carcinosarcoma arising in a patient with multiple cylindromas. Am J Dermatopathol. 2005;27:21–6. doi: 10.1097/01.dad.0000141548.69423.c7[↩]
- Cranston A, Stocken DD, Stamp E, Roblin D, Hamlin J, Langtry J, Plummer R, Ashworth A, Burn J, Rajan N. Tropomyosin Receptor Antagonism in Cylindromatosis (TRAC), an early phase trial of a topical tropomyosin kinase inhibitor as a treatment for inherited CYLD defective skin tumours: study protocol for a randomised controlled trial. Trials. 2017 Mar 7;18(1):111. doi: 10.1186/s13063-017-1812-z[↩]
- Calonje E. Rook’s Textbook of Dermatology. Chichester: Wiley-Blackwell; 2010. Tumours of the skin appendages. In: Burns T, Breathnach S, Cox N, Griffiths C, editors.[↩]
- Matt D., Xin H., Vortmeyer A.O., Zhuang Z., Burg G., Böni R. Sporadic trichoepithelioma demonstrates deletions at 9q22. 3. Arch. Dermatol. 2000;136(5):657–660. doi: 10.1001/archderm.136.5.657[↩]
- Martinez CA, Priolli DG, Piovesan H, Waisberg J. Nonsolitary giant perianal trichoepithelioma with malignant transformation into basal cell carcinoma: Report of a case and review of the literature. Dis Colon Rectum. 2004;47:773–7. doi: 10.1007/s10350-003-0104-8[↩]
- A case of multiple desmoplastic trichoepithelioma. Moon SH, Choi HS, Kwon HI, Ko JY, Kim JE. Ann Dermatol. 2016;28:411–413. doi: 10.5021/ad.2016.28.3.411[↩]
- Mosby SP, Naidu MN, Ranpise SG, Magar S. Trichoepithelioma. J Indian Acad Oral Med Radiol. 2011;23:448–50.[↩]
- Yiltok SJ, Echejoh GO, Mohammad AM, Ituen AM, Igoche MI, Dades OT. Multiple familial trichoepithelioma: a case report and review of literature. Niger J Clin Pract. 2010 Jun;13(2):230-2.[↩]
- Desmoplastic trichoepithelioma. Brownstein MH, Shapiro L. Cancer. 1977;40:6–2979. doi: 10.1002/1097-0142(197712)40:6<2979::aid-cncr2820400633>3.0.co;2-8[↩]
- Adnexal skin tumors in Zaria, Nigeria. Samaila MO. Ann Afr Med. 2008;7:6–10. doi: 10.4103/1596-3519.55691[↩]
- Kaur T, Puri KJ, Chahal KS, Budhwar J. Multiple familial trichoepithelioma: A case report and review. EJOD. 2012;8:11.[↩]
- Kazakov DV. Brooke-Spiegler Syndrome and phenotypic variants: an update. Head Neck Pathol. 2016;10(2):125–130. doi: 10.1007/s12105-016-0705-x[↩]
- Desmoplastic trichoepithelioma. Moynihan GD, Skrokov RA, Huh J, Pardes JB, Septon R. J Am Acad Dermatol. 2011;64:438–439. doi: 10.1016/j.jaad.2010.04.053[↩][↩]
- Multiple familial trichoepithelioma. https://ghr.nlm.nih.gov/condition/multiple-familial-trichoepithelioma[↩][↩][↩][↩][↩]
- Morelli JG. Tumors of the Skin. In: Kliegman eds. Nelson Textbook of Pediatrics, 18th ed. Philadelphia, PA: Saunders; 2007[↩][↩][↩]
- Neff AG, Carter KD. Benign Eyelid Lesions. In: Yanoff & Duker. Ophthalmology, 3rd ed. Philadelphia, PA: Mosby; 2008[↩][↩][↩]
- Multiple Familial Trichoepitheliomas. https://www.orpha.net/data/patho/GB/uk-Trichoepithelioma.pdf[↩]
- Nagy N, Farkas K, Kemény L & Széll M. Phenotype-genotype correlations for clinical variants caused by CYLD mutations. Eur J Med Genet. 2015 May;. May, 2015; 58(5):271-8.[↩]
- TRICHOEPITHELIOMA, MULTIPLE FAMILIAL, 1 https://omim.org/entry/601606[↩]
- Alessi SS, Sanches JA, Oliveira WR, Messina MC, Pimentel ER, Festa Neto C. Treatment of cutaneous tumors with topical 5% imiquimod cream. Clinics. 2009; 64(10):961-966.[↩]
- Trichoepithelioma. https://www.dermnetnz.org/topics/trichoepithelioma[↩]
- Trichoepithelioma. https://emedicine.medscape.com/article/1060049-overview[↩]
- Mapar MA, Ranjbari N, Afshar N, Karimzadeh I, Karimzadeh A. Severely disfiguring multiple familial trichoepitheliomas with basal cell carcinoma. Indian J Dermatol Venereol Leprol. 2014;80:349–52. doi: 10.4103/0378-6323.136924[↩]
- Sangwaiya A, Sharma J, Sharma S, Munghate A, Samal S, Sen R. Multiple familial trichoepithelioma with an adjacent basal cell carcinoma, transformation or collision – A case report and review of literature. Indian J Dermatol. 2015;60:280–83. doi: 10.4103/0019-5154.156380[↩]
- Shehan JM, Huerter CJ. Desmoplastic trichoepithelioma: report of a case illustrating its natural history. Cutis. 2008 Mar;81(3):236-8. https://cdn.mdedge.com/files/s3fs-public/Document/September-2017/081030236.pdf[↩]
- Desmoplastic trichoepithelioma. Mamelak AJ, Goldberg LH, Katz TM, Graves JJ, Arnon O, Kimyai-Asadi A. J Am Acad Dermatol. 2010;62:102–106. doi: 10.1016/j.jaad.2009.06.066[↩]
- LoPiccolo MC, Sage RJ, Kouba DJ. Comparing ablative fractionated resurfacing, photodynamic therapy, and topical imiquimod in the treatment of trichoblastomas of Brooke-Spiegler Syndrome: a case study. Dermatol Surg. 2011;37(7):1047–1050. doi: 10.1111/j.1524-4725.2011.01907.x[↩]
- Alshami MA. New application of the long-pulsed Nd-YAG laser as an ablative resurfacing tool for skin rejuvenation: a 7-year study. J Cosmet Dermatol. 2013;12(3):170–178. doi: 10.1111/jocd.12052[↩]





{kind=link}