Contents
- Atrioventricular Septal Defect
- Atrioventricular septal defect types
- Atrioventricular septal defect causes
- Atrioventricular septal defect prevention
- Atrioventricular septal defect signs and symptoms
- Atrioventricular septal defect complications
- Atrioventricular septal defect diagnosis
- Atrioventricular septal defect treatment
- Atrioventricular septal defect prognosis
Atrioventricular Septal Defect
Atrioventricular septal defect (AVSD) also called atrioventricular canal defect (AV canal defect) or endocardial cushion defect is a heart defect in which there are holes between the chambers of the right and left sides of the heart, and the valves that control the flow of blood between these chambers may not be formed correctly 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12. In atrioventricular septal defect, blood flows where it normally should not go. The blood may also have a lower than normal amount of oxygen, and extra blood can flow to the lungs. This extra blood being pumped into the lungs forces the heart and lungs to work hard and may lead to congestive heart failure.
Atrioventricular septal defect may be classified as partial or complete. In a partial septal defect, either the upper (atrial) or lower (ventricular) part of the septum may be affected. A complete septal defect, which is more common, means that the hole is located where the upper (atrial) and lower (ventricular) parts of the septum meet.
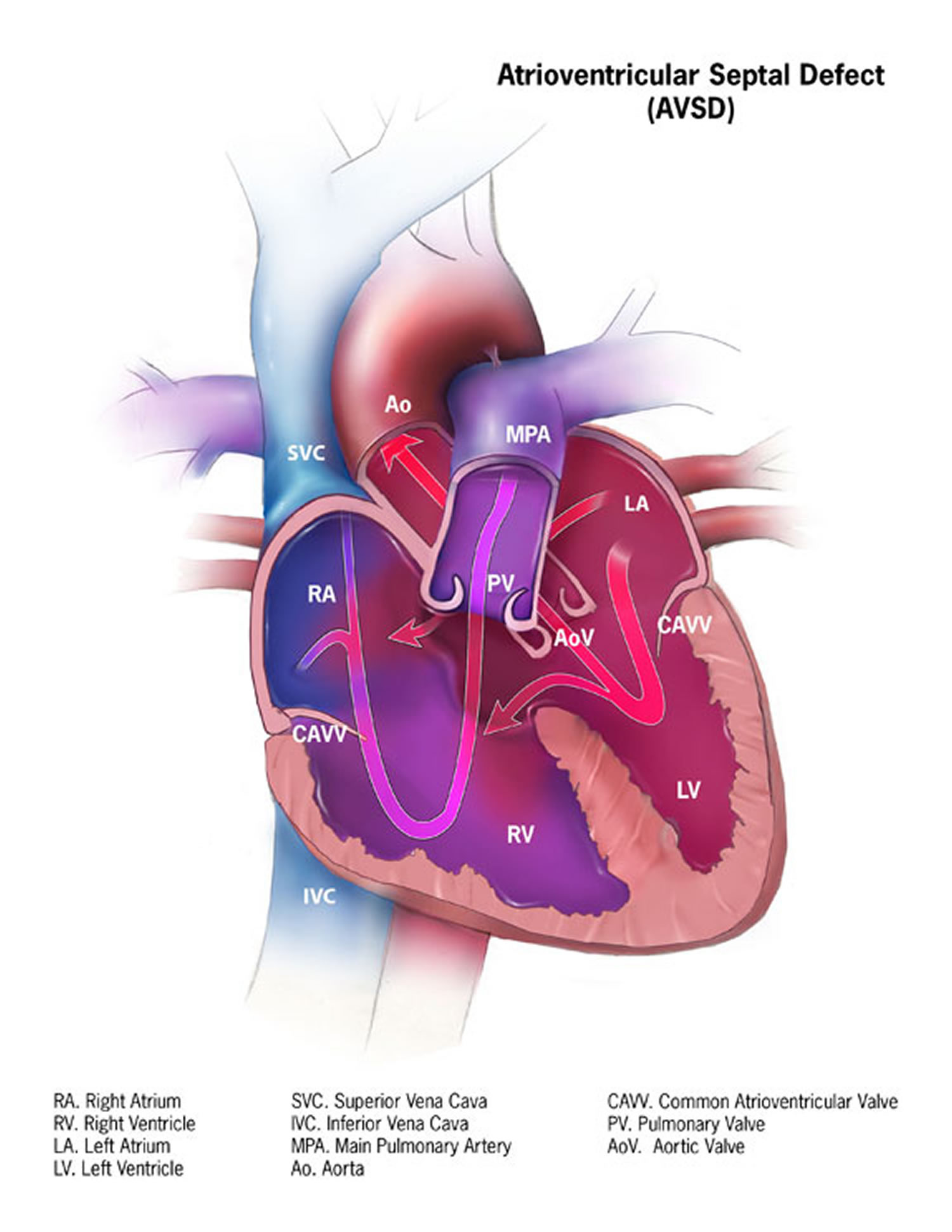
Normally, the tricuspid valve directs blood from the upper-right chamber (the right atrium) to the lower-right chamber (the right ventricle), and the mitral valve allows blood to move from the upper-left chamber (the left atrium) to the lower-left chamber (the left ventricle). But with complete atrioventricular septal defect, just one large hole and one valve are present, and the valve may not close all the way. This allows blood to flow in all directions inside the heart.
Atrioventricular septal defect:
- A hole in the wall dividing the heart’s upper chambers (atrial septal defect or ASD),
- A hole in the wall separating the heart’s lower chambers (ventricular septal defect or VSD) and
- Abnormalities of the tricuspid and mitral valves.
Some patients with atrioventricular septal defects have a small or no opening between the bottom chambers of the heart. They can present in adulthood with findings similar to patients with atrial septal defects (ASD); this can be referred to as an “ostium primum” atrial septal defect. Even less commonly, only the hole between the lower chambers is present.
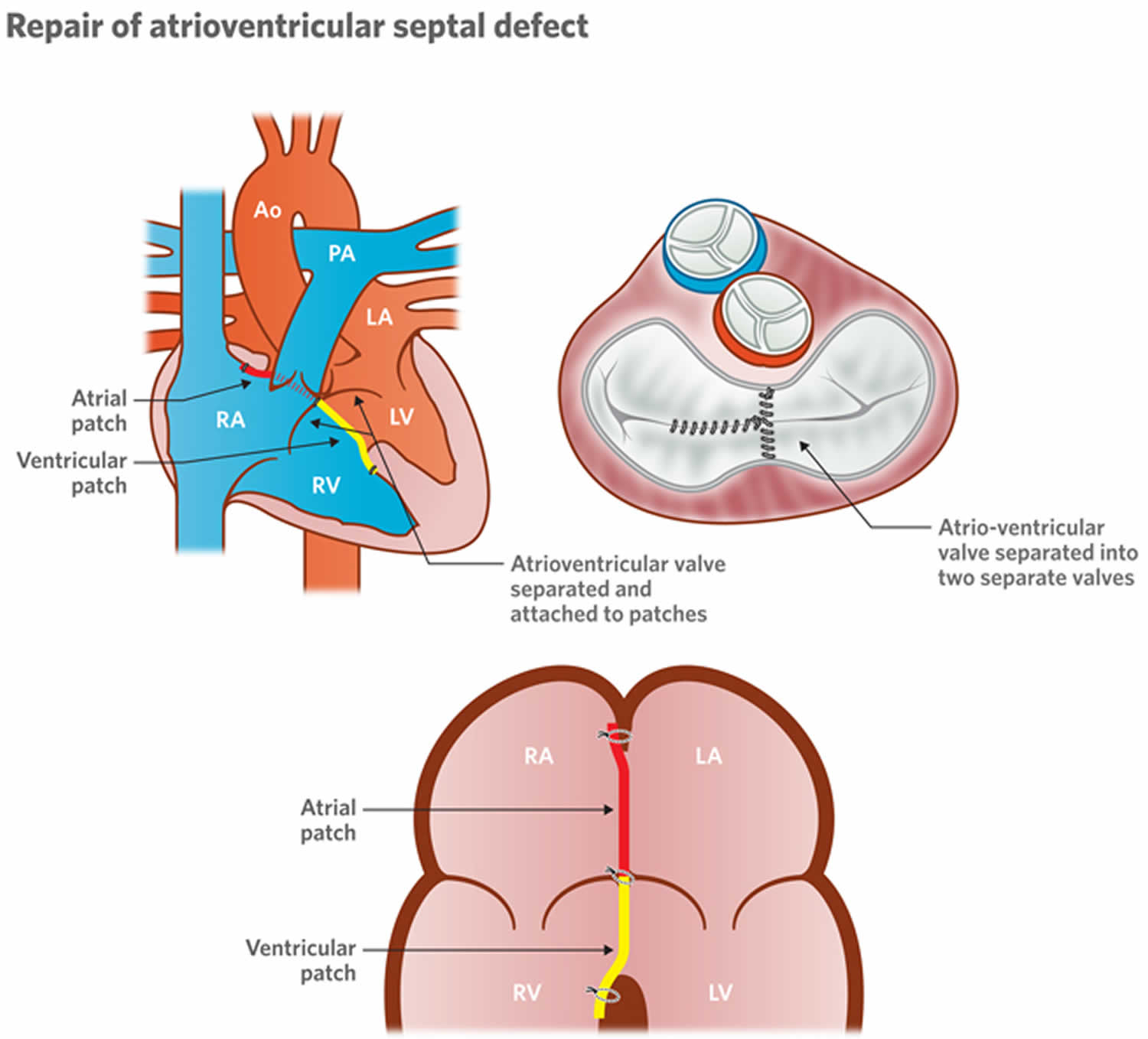
Surgery is needed to repair complete and partial atrioventricular septal defects. Surgery is usually done in the first few months after birth with most cases in the first four to six months to correct a complete atrioventricular septal defect. The procedure involves closing the hole in the wall (septum) between the heart chambers with one or two patches. The patches stay in the heart permanently, becoming part of the septum as the heart’s lining grows over them.
For a partial atrioventricular septal defect, surgery also involves repair of the mitral valve, so it will close tightly. If repair isn’t possible, the valve might need to be replaced.
For a complete atrioventricular septal defect, surgery also includes separation of the large single valve that separates the upper and lower chambers of the heart into two valves, on both the left and right sides of the repaired septum. If separating the single valve isn’t possible, heart valve replacement of both the tricuspid and mitral valves might be needed.
Normal heart
The heart is divided into four chambers, two on the right and two on the left.
The right side of your heart moves blood into vessels that lead to the lungs. There, oxygen enriches the blood. The oxygen-rich blood flows back to your heart’s left side and is pumped into a large vessel (aorta) that circulates blood to the rest of your body.
Valves control the flow of blood into and out of the chambers of your heart. These valves open to allow blood to move to the next chamber or to one of the arteries, and close to keep blood from flowing backward.
Figure 1. The anatomy of the heart chambers
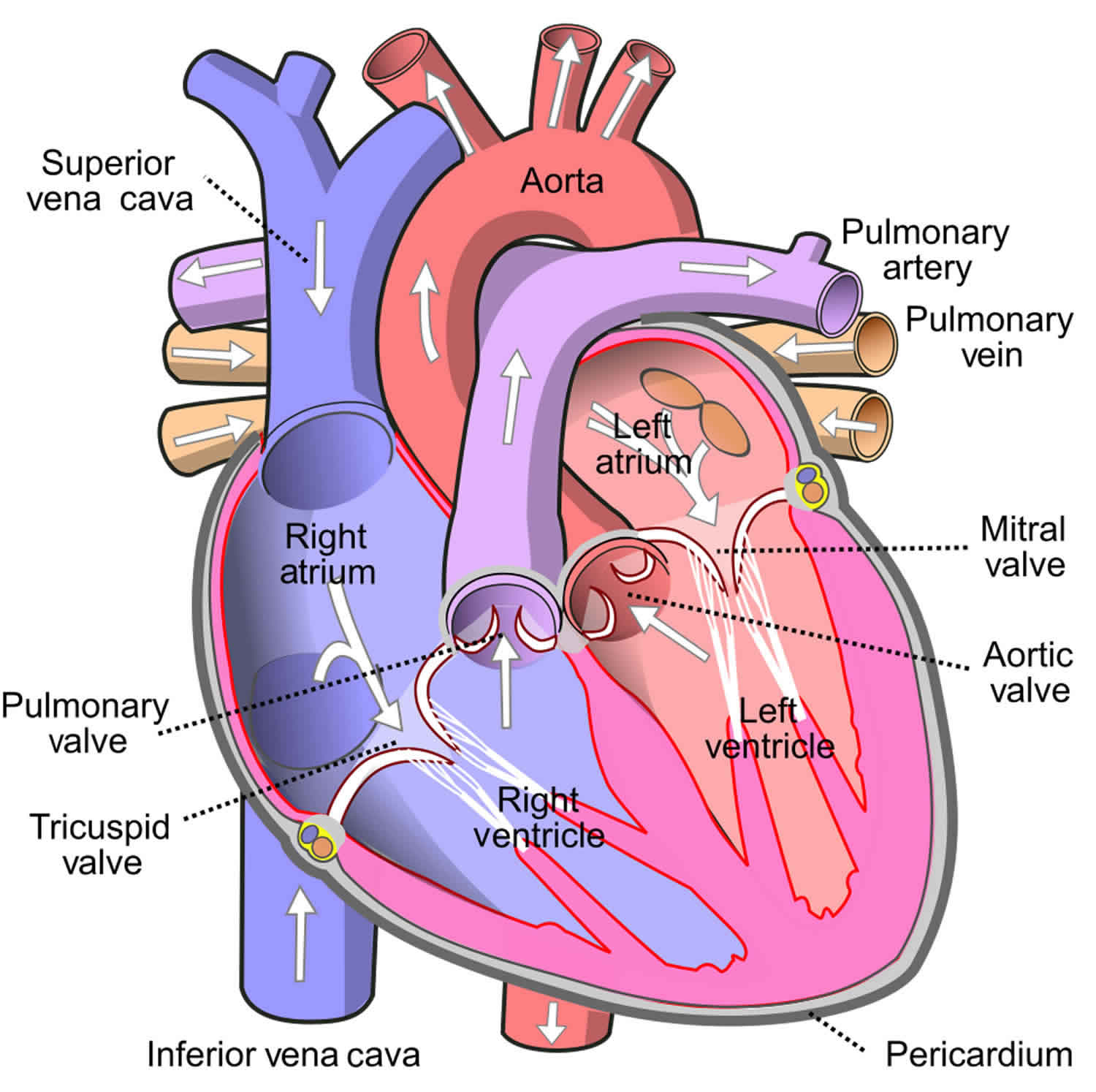
Figure 2. Normal heart blood flow

Figure 3. Atrioventricular canal defect

 [Source 1 ]
[Source 1 ]How common is atrioventricular septal defect?
The Centers for Disease Control and Prevention estimates that about 2,000 babies (1 in 2,120 babies) are born with atrioventricular septal defect every year in the United States 13.
Atrioventricular septal defect types
There are 3 general types of atrioventricular septal defect that can occur, depending on which structures are not formed correctly 14, 15, 16:
Complete Atrioventricular Septal Defect
A complete atrioventricular septal defect occurs when there is a large hole in the center of the heart which allows blood to flow between all four chambers of the heart. This hole occurs where the septa (walls) separating the two top chambers (atria) and two bottom chambers (ventricles) normally meet. There is also one common atrioventricular valve in the center of the heart instead of two separate valves – the tricuspid valve on the right side of the heart and the mitral valve on the left side of the heart. This common valve often has leaflets (flaps) that may not be formed correctly or do not close tightly. Sometimes there’s leakiness (regurgitation) of the abnormal single valve. This may add to the heart failure symptoms. A complete atrioventricular septal defect arises during pregnancy when the common valve fails to separate into the two distinct valves (tricuspid and mitral valves) and when the septa (walls) that split the upper and lower chambers of the heart do not grow all the way to meet in the center of the heart.
Normally, the left side of the heart only pumps blood to the body, and the heart’s right side only pumps blood to the lungs. In a child with atrioventricular septal defect, blood can travel across the holes from the left heart chambers to the right heart chambers and out into the lung arteries. The extra blood being pumped into the lung arteries makes the heart and lungs work harder and the lungs can become congested.
High pressure may occur in the blood vessels in the lungs that can lead to permanent damage with pulmonary hypertension that persists into adulthood.
Many adults who have not had previous repair have pulmonary hypertension (see Eisenmenger’s syndrome). Eisenmenger syndrome is a severe, long-term complication of a congenital heart defect, like a hole in the heart wall (ventricular septal defect or atrial septal defect), resulting in pulmonary hypertension and right-to-left shunt (oxygen-poor blood from the right side of the heart flows into the left side), leading to cyanosis and other symptoms such as shortness of breath, fatigue (feeling tired), dizziness and syncope (fainting), heart failure, arrhythmias (irregular heartbeats), clubbing (enlargement of the fingertips and toes), increased risk of blood clots and stroke.
Eisenmenger syndrome is more common than in patients with an atrial septal defect or a ventricular septal defect. Even in adults without Eisenmenger’s syndrome, symptoms including shortness of breath, intolerance to exercise and palpitations are common. On physical examinations, murmurs due to the blood flow across the defects and due to the valve leak are common.
Partial or Incomplete Atrioventricular Septal Defect
A partial or incomplete atrioventricular septal defect occurs when the heart has some, but not all of the defects of a complete atrioventricular septal defect. There is usually a hole in the atrial wall or in the ventricular wall near the center of the heart. A partial atrioventricular septal defect usually has both mitral and tricuspid valves, but one of the valves (usually mitral) may not close completely, allowing blood to leak backward from the left ventricle into the left atrium.
Surgical intervention for uncomplicated incomplete atrioventricular septal defect is generally characterized by its simplicity and overall positive outcomes 3. The mortality after 30 days following the repair of incomplete atrioventricular septal defect is rare, ranging from 0% to 4% of patients 17, 18, 19. However, as with complete atrioventricular septal defect, left atrioventricular valve regurgitation emerges as a primary cause of late morbidity following incomplete atrioventricular septal defect repair. Despite low early mortality and excellent long-term survival, prior investigations have demonstrated that reoperation for significant postoperative left atrioventricular valve regurgitation is required in 3% to 13% of patients who undergo repair for partial and transitional atrioventricular septal defect 20, 21.
Transitional atrioventricular septal defect
Transitional atrioventricular septal defect extends beyond the features of partial or incomplete atrioventricular septal defect and encompasses the presence of a small and restrictive ventricular septal defect 22, 23.
Children with partial and transitional atrioventricular septal defect are largely asymptomatic, which leads to the deferral of surgical treatment until the preschool or older age stage 24, 25, 26.
Atrioventricular septal defect causes
The causes of congenital heart defects, such as atrioventricular septal defect, among most babies are unknown 1. Some babies have heart defects because of changes in their genes or chromosomes. In particular, atrioventricular septal defect is common in babies with Down syndrome, a genetic condition that involves an extra chromosome 21 (also called trisomy 21) 1. Congenital heart defects are also thought to be caused by the combination of genes and other factors that might increase the risk of having a baby with a congenital heart defect, such as things the mother comes in contact with in her environment, what she eats or drinks, or certain medications she uses during pregnancy 1.
Risk factors for atrioventricular septal defect
Factors that might increase a baby’s risk of developing atrioventricular septal defect before birth include:
- Down syndrome also called trisomy 21
- German measles (rubella) or another viral illness during a mother’s early pregnancy
- Alcohol consumption during pregnancy
- Poorly controlled diabetes during pregnancy
- Smoking during pregnancy
- Certain medications taken during pregnancy — talk to your doctor before taking any drugs while you’re pregnant or trying to become pregnant
- Having a parent who had a congenital heart defect.
Atrioventricular septal defect prevention
Atrioventricular septal defect generally can’t be prevented.
Heredity may play a role in some heart defects. If you have a family history of heart defects or if you already have a child with a congenital heart defect, talk with a genetic counselor and a cardiologist before getting pregnant again.
Immunization with rubella vaccine has been one of the most effective preventive strategies against congenital heart defects.
Atrioventricular septal defect signs and symptoms
Atrioventricular septal defect can involve only the two upper chambers of the heart (partial) or all four chambers (complete). In either type, extra blood circulates in the lungs.
Atrioventricular septal defect is often associated with Down syndrome. A child with atrioventricular septal defect may breathe faster and harder than normal. Infants may have trouble feeding and growing at a normal rate. Symptoms may not occur until several weeks after birth. High pressure may occur in the blood vessels in the lungs because more blood than normal is being pumped there. Over time this causes permanent damage to the lung blood vessels.
In some infants, the common valve between the upper and lower chambers doesn’t close properly. This lets blood leak backward from the heart’s lower chambers to the upper ones. This leak, called regurgitation or insufficiency, can make the heart work harder and the heart becomes enlarged from working too hard.
Complete atrioventricular septal defect symptoms
Complete atrioventricular septal defect signs and symptoms usually develop in the first several weeks of life. These signs and symptoms are generally similar to those associated with heart failure and might include:
- Difficulty breathing or rapid breathing
- Wheezing
- Fatigue
- Lack of appetite
- Poor weight gain
- Pale skin color
- Bluish discoloration of the lips and skin
- Excessive sweating
- Irregular or rapid heartbeat
- Swelling in the legs, ankles and feet (edema)
Partial atrioventricular septal defect symptoms
Partial atrioventricular septal defect signs and symptoms might not appear until early adulthood and might be related to complications that develop as a result of the defect. These signs and symptoms can include:
- Abnormal heartbeat (arrhythmia)
- Shortness of breath
- High blood pressure in the lungs (pulmonary hypertension)
- Heart valve problems
- Heart failure.
Atrioventricular septal defect complications
Complications of atrioventricular septal defect can include:
- Enlargement of the heart. Increased blood flow through the heart forces it to work harder than normal, causing it to enlarge.
- Pulmonary hypertension. When there is a hole (defect) that allows mixing of oxygenated (red) and deoxygenated (blue) blood, the amount of blood that goes to the lungs is increased. This results in pressure buildup in the lungs, causing high blood pressure in the lungs.
- Respiratory tract infections. Atrioventricular canal defect can cause recurrent bouts of lung infections.
- Heart failure. Untreated, atrioventricular canal defect usually results in the heart’s inability to pump enough blood to meet the body’s needs.
Most of the complications of atrioventricular septal defect are related to intracardiac shunts (an abnormal pathway for blood flow within the heart where blood bypasses the normal circulation, potentially leading to mixing of oxygenated and deoxygenated blood) or atrioventricular valve regurgitation. In complete atrioventricular septal defect, shunting of blood from left to right leads to right-sided heart overload and signs of heart failure and pulmonary congestion at a very early age, which contributes to significant mortality during infancy. If the shunt is not corrected, it causes an irreversible pulmonary vascular disease that leads to pulmonary hypertension and Eisenmenger syndrome.
Regurgitation of blood from the ventricle to atria through the atrioventricular valve leads to pulmonary congestion and enlargement of the atrium. Enlargement of the atrium can lead to supraventricular arrhythmias (heart rhythm disorders originating above the ventricles, usually in the atria, and can cause the heart to beat too fast, too slow, or irregularly). Other complications are related to poor feeding, which may include malnutrition and failure to thrive.
Complications later in life
Treatment greatly improves the outlook (prognosis) for children with atrioventricular septal defect. However, some children who have corrective surgery may still be at risk later in life of:
- Leaky heart valves
- Narrowing of the heart valves
- Abnormal heart rhythm
- Breathing difficulties associated with lung damage
Common signs and symptoms of these complications include:
- Shortness of breath
- Fatigue
- Rapid, fluttering heartbeat
Additional surgery might be needed to correct complications of atrioventricular septal defect.
Atrioventricular septal defect diagnosis
Atrioventricular septal defect may be diagnosed during pregnancy through ultrasound or soon after the baby is born with special heart imaging.
When listening to your baby’s heart, your baby’s doctor might hear an abnormal whooshing sound (heart murmur) caused by turbulent blood flow.
If your baby is experiencing the signs and symptoms of atrioventricular septal defect, your baby’s doctor might recommend:
- Electrocardiogram (ECG or EKG). Electrical signals are recorded as they travel through the heart. Your doctor can look for patterns that indicate abnormal heart function.
- Echocardiogram. Sound waves produce live-action images of the heart. Echocardiogram can reveal a hole in the heart and abnormal heart valves, as well as abnormal blood flow through the heart.
- Chest X-ray. The image can show evidence of an enlarged heart.
- Cardiac catheterization. A thin, flexible tube (catheter) is inserted into a blood vessel in the groin and up to the heart. A dye injected through the catheter makes the heart structures visible on
- X-ray pictures. The catheter also allows the doctor to measure pressure in the chambers of the heart and in the blood vessels.
During Pregnancy
During pregnancy, there are screening tests also called prenatal tests to check for birth defects and other conditions. Atrioventricular Septal Defect may be diagnosed during pregnancy with an ultrasound test (which creates pictures of the baby using sound waves), but whether or not the defect can be seen with the ultrasound test depends on the size or type (partial or complete) of the Atrioventricular Septal Defect. The healthcare provider can request a fetal echocardiogram to confirm the diagnosis if Atrioventricular Septal Defect is suspected. A fetal echocardiogram is an ultrasound of the baby’s heart which shows more detail than the routine prenatal ultrasound test. The fetal echocardiogram can show problems with the structure of the heart and how well the heart is working.
After the Baby is Born
During a physical exam of an infant, a complete Atrioventricular Septal Defect may be suspected. Using a stethoscope, a doctor will often hear a heart murmur (an abnormal “whooshing” sound caused by blood flowing through the abnormal hole). However, not all heart murmurs are present at birth. Babies with a complete Atrioventricular Septal Defect usually do show signs of problems within the first few weeks after birth. When symptoms do occur, they may include
- Breathing problems
- Pounding heart
- Weak pulse
- Ashen or bluish skin color
- Poor feeding, slow weight gain
- Tiring easily
- Swelling of the legs or belly
For partial Atrioventricular Septal Defects, if the holes between the chambers of the heart are not large, the signs and symptoms may not occur in the newborn or infancy periods. In these cases, people with a partial Atrioventricular Septal Defect might not be diagnosed for years.
Symptoms which might indicate that a child’s complete Atrioventricular Septal Defect or partial Atrioventricular Septal Defect is getting worse include
- Arrhythmia, an abnormal heart rhythm. An arrhythmia can cause the heart to beat too fast, too slow, or erratically. When the heart does not beat properly, it can’t pump blood effectively.
- Congestive heart failure, when the heart cannot pump enough blood and oxygen to meet the needs of the body.
- Pulmonary hypertension, a type of high blood pressure that affects the arteries in the lungs and the right side of the heart.
The healthcare provider can request one or more tests to confirm the diagnosis of Atrioventricular Septal Defect. The most common test is an echocardiogram. This is an ultrasound of the heart that can show problems with the structure of the heart, like holes between the chambers of the right and left side of the heart, and any irregular blood flow. An electrocardiogram (EKG), which measures the electrical activity of the heart, chest x-rays, and other medical tests may also be used to make the diagnosis. Because many babies with Down syndrome have an Atrioventricular Septal Defect, all infants with Down syndrome should have an echocardiogram to look for an Atrioventricular Septal Defect or other heart defects.
Atrioventricular septal defect treatment
All atrioventricular septal defects, both partial and complete types, usually require surgery 27, 28. During surgery, any holes in the chambers are closed using patches. If the mitral valve does not close completely, it is repaired or replaced. For a complete atrioventricular septal defect, the common valve is separated into two distinct valves – one on the right side and one on the left side. However, left atrioventricular valve regurgitation may develop as a major event after surgery in 8% to 10% of patients, sometimes requiring re-operation 29, 30. The presence of mild to moderate or even more severe left atrioventricular valve regurgitation postoperatively, the width of left atrioventricular valve cleft ≥1 cm, and younger age at first repair are independently associated with increased risk of recurrent left atrioventricular valve regurgitation after partial and transitional atrioventricular septal defect (AVSD) repair 3.
The age at which surgery is done depends on your child’s health and the specific structure of the atrioventricular septal defect. If possible, surgery should be done before there is permanent damage to the lungs from too much blood being pumped to the lungs. Medication may be used to treat congestive heart failure, but it is only a short term measure until the infant is strong enough for surgery.
Deciding how to manage this complex group of patients requires assessment of pre-operative imaging and hemodynamic data, which are essential for the optimal selection of surgical procedures to reduce the requirement of recurrent surgery and postoperative complications 31. Ventricular volumes determined by three dimensional echocardiography and magnetic resonance imaging scans may guide therapy with the ability to recruit ventricles with volume as low as 15–30 ml/m² 32. In previous studies, the requirement of the recurrent procedure is reported as high as 18.2% at 15 years after surgical correction and left atrioventricular valve dysplasia, absence of cleft closure and associated cardiac malformations are found to increase the rate of recurrent procedures 33.
Atrioventricular septal repair is a complex surgical procedure and carries operative mortality of more than 3% even in the present time with advanced surgical techniques 34. Atrioventricular septal repair also carries significant postoperative mortality and morbidity due to residual intracardiac shunts, atrioventricular valve regurgitation, left ventricular outflow tract obstruction, and arrhythmias 35.
The first successful surgical repair of a complete atrioventricular septal defect was done by Lillehei et al. in 1955 15, 36. Using the technique of controlled cross circulation 15, 36. Long-term results from earlier studies had demonstrated a 15 years survival of 86%–89% 37, 33, however despite improved survival, several single-center studies have reported that up to 10% of patients after complete atrioventricular septal defect repair will require a reoperation within 10 to 15 years, for left atrioventricular valve regurgitation and left ventricular outflow tract obstruction 35. Ginde, et al. 38 operated on 198 children with complete atrioventricular septal defect between 1974 and 2000. Their overall perioperative mortality was 10.1% with a significant decrease to 2.9% in the late surgical era 1991–2000 38. The estimated overall survival for the entire group was 85% at 10 years, 82% at 20 years and 71% at 30 years 35.
In complete atrioventricular septal defect, surgical closure should be performed in early infancy to reduce the pulmonary vascular disease 39. On the other hand, incomplete atrioventricular septal defect, a repair can be slightly delayed if the patient is not symptomatic 39.
For partial atrioventricular septal defect, the primary repair is preferred with patch closure and atrioventricular valvuloplasty.
For balanced complete atrioventricular septal defect, early primary repair with two patch closure techniques is preferred over one patch closure, as one patch closure is associated with an increased rate of recurrent procedures due to patch dehiscence and residual shunt 39.
Pulmonary artery banding is no longer used in the elective routine repair of complete atrioventricular septal defect in favor of a 1 stage repair 35, 40. However, 5% to 10% of patients coming for atrioventricular septal defect surgery will require pulmonary artery debanding 41.
Unbalanced atrioventricular septal defect is defined as a atrioventricular septal defect with an atrioventricular valve override of more than 60% over either ventricle or the presence of hypoplastic nonapex forming ventricles or in case of a right dominant atrioventricular septal defect a left ventricle with indexed volumes at least 2 standard deviation smaller than normal, represent 10%–15% of all atrioventricular septal defect 35. This defect is characterized by underdevelopment of one of the ventricles and varying degrees of malalignment of the common atrioventricular valve, over the hypoplastic ventricle and associated hypoplasia of the outflow valve related to decreased flow 42. For unbalanced atrioventricular septal defect, repair technique may include single ventricle palliation with the staged biventricular repair or primary biventricular repair 35. More recently, biventricular conversion from single ventricle palliation has been advocated, particularly in patients with trisomy 21 and heterotaxy, who tolerate single ventricle palliation poorly. Staged biventricular recruitment has also been advocated for complete biventricular repair.
In an infant with severe symptoms or high blood pressure in the lungs (pulmonary hypertension), particularly those with complete atrioventricular septal defect, surgery must usually be done in infancy at 1–3 months of age to prevent the development of left atrioventricular valve dysplasia and annular dilatation 35. Routine left atrioventricular valve cleft closure and commissural and/or annular plication should be routinely performed at primary repair 43. The surgery to fix these defects involves patching the atrial septal defect and the ventricular septal defect and repairing the heart valve. During the operation, the surgeon closes the large hole with one or two patches. Later the patch will become a permanent part of the heart as the heart’s lining grows over it. To repair the single valve, the surgeon divides the single valve between the heart’s upper and lower chambers and makes two separate valves. These will be made as close to normal valves as possible.
Left atrioventricular valvuloplasty is superior to left atrioventricular valve replacement because of preserved somatic growth, and absence of hemorrhagic, thromboembolic, and infectious complications, however durability of repair is it’s weakest link, especially in children with complex left atrioventricular valve pathology such as left atrioventricular valve dysplasia, double outlet left atrioventricular valve, and pseudoparachute left atrioventricular valve 35.
Left ventricular outflow tract obstruction is frequently due to an acquired discrete subaortic membrane. In addition, the classic 1 patch technique of surgical repair is a risk factor for reoperation, largely due to residual ventricular septal defects, and patch dehiscence 35, 44. The classic 1 patch technique involves dividing the common atrioventricular valve leaflets and suspending them from a single patch resulting in more distortion of the valve tissue and atrioventricular valve regurgitation. The risk appears lower with the two patch repair technique.
If an infant is very ill, or has a defect that may be too complex to repair in infancy, a temporary operation to relieve symptoms and high pressure in the lungs may be needed before the definitive operation. This procedure (pulmonary artery banding) narrows the pulmonary artery to reduce the blood flow to the lungs. When the child is older, an operation is done to remove the band and fix the atrioventricular septal defect with open-heart surgery.
Surgical repair of an atrioventricular septal defect usually restores blood circulation to normal. For many patients, the long-term outlook is good, and no medicines or additional surgery are needed. Because this is a more complicated congenital heart defect, late problems in adults are more common than after an atrial septal defect or ventricular septal defect is closed. As the child grows, the repair may partially break down leading to patch leaks, valve leakage and narrowing of the blood flow channel to the body. These problems may increase the workload of the heart and cause symptoms.
Infants who have surgical repairs for atrioventricular septal defect are not cured; they might have lifelong complications. The most common of these complications is a leaky mitral valve. This is when the mitral valve does not close all the way so that it allows blood to flow backwards through the valve. A leaky mitral valve can cause the heart to work harder to get enough blood to the rest of the body; a leaky mitral valve might have to be surgically repaired. A child or adult with an atrioventricular septal defect will need regular follow-up visits with a cardiologist (a heart doctor) to monitor his or her progress, avoid complications, and check for other health conditions that might develop as the child gets older. With proper treatment, most babies with atrioventricular septal defect grow up to lead healthy, productive lives.
Figure 4. Repair of atrioventricular septal defect
After surgery
If the heart defect is repaired successfully, your child will likely lead a normal life, often with no activity restrictions.
However, you or your child will need lifelong follow-up care with a cardiologist trained in congenital heart disease. Your cardiologist will likely recommend a follow-up exam once a year or more frequently if problems, such as a leaky heart valve, remain. Adults whose congenital heart defects were treated as children may need care from a cardiologist trained in adult congenital heart disease (adult congenital cardiologist) throughout life. Special attention and care may be needed around the time of procedures, such as an operation which does not involve the heart.
You or your child might also need to take preventive antibiotics before certain dental and other surgical procedures if he or she:
- Has remaining heart defects after surgery
- Received an artificial heart valve
- Received artificial (prosthetic) material during heart repair
The antibiotics are used to prevent a bacterial infection of the lining of the heart (endocarditis).
Many people who have corrective surgery for atrioventricular canal defect don’t need additional surgery. However, some complications, such as heart valve leaks, may require treatment.
What if the atrioventricular septal defect is still present? Should it be repaired in adulthood?
The decision to repair an atrioventricular septal defect in adulthood is complicated. It depends on the pressures in the lung and the heart’s pumping function. However, when the pressures aren’t too high and the pump function is good, these defects can be repaired and adult patients are likely to improve. A heart catheterization is almost always required to know whether the atrioventricular septal defect should be closed. These defects can’t be closed or repaired in the catheterization laboratory, however, because of their location and the need to fix the heart valves.
Problems you may have
Problems in patients with repaired atrioventricular septal defect depend on whether there are patch leaks and whether there’s a lot of valve regurgitation. Shortness of breath, inability to exercise and swelling in the legs are all signs of heart failure. Abnormal heart rhythms may cause palpitations (skipped or rapid heartbeats) and, rarely, fainting. Some patients may need a pacemaker after the repair if the electrical system has been damaged.
Patients with unrepaired atrioventricular septal defect are often blue (see Eisenmenger’s syndrome). Because of valve leaks on the heart’s left side, they’re more likely to have heart failure than other patients with Eisenmenger’s syndrome due to atrial septal defect and ventricular septal defect.
What activities can my child do?
If the atrioventricular septal defect has been closed with surgery, your child may not need any special precautions regarding physical activities and may be able to participate in normal activities without increased risk. Being physically active is healthy for the cardiovascular system, but some children may need to limit their activity. However, patients with heart failure and pulmonary hypertension may need some restrictions. Discuss this with your child’s pediatric cardiologist.
What will my child need in the future?
After surgery your child must be examined regularly by a pediatric cardiologist. More medical or surgical treatment is sometimes needed.
Surgical repair of atrioventricular septal defect usually restores the blood circulation to normal. However, the reconstructed valve may not work normally. The valve structures can leak or narrow. But, for many children, the long-term outlook is good, and usually no medicines or additional surgery are needed.
Ongoing care
An adult with a repaired or unrepaired atrioventricular septal defect must be examined regularly by a cardiologist with experience in adult congenital heart disease. The frequency of the visits depends on the extent of problems with the repair, the presence of abnormal heart rhythms (arrhythmias) and pulmonary hypertension. In general, you should visit the cardiologist at least once a year. You should also consult a cardiologist with expertise in care of adult congenital heart disease if you’re undergoing any type of non-heart surgery or invasive procedure or thinking about heart surgery.
Medical therapy
Heart failure medications may be needed, especially in patients with valve regurgitation, to help their heart pump better and/or lower blood pressure. Patients with pulmonary hypertension may also require medications. Your cardiologist can monitor you with noninvasive tests if needed. These include electrocardiograms, Holter monitors, exercise stress tests and echocardiograms. When further surgery is contemplated, a heart catheterization is almost always needed.
What about preventing endocarditis?
Children with atrioventricular septal defect may risk endocarditis both before and after repair. Lifelong endocarditis prophylaxis is recommended. Ask about your child’s risk of endocarditis and about your child’s need to take antibiotics before certain dental procedures.
Infective endocarditis
Dental procedures and infective endocarditis
In the past, patients with nearly every type of congenital heart defect needed to receive antibiotics one hour before dental procedures or operations on the mouth, throat, gastrointestinal genital, or urinary tract. However, in 2007 the American Heart Association simplified its recommendations. Today, antibiotics before dental procedures are only recommended for patients with the highest risk of infective endocarditis, those who have 45:
- A prosthetic heart valve or who have had a heart valve repaired with prosthetic material.
- A history of endocarditis.
- A heart transplant with abnormal heart valve function
- Certain congenital heart defects including:
- Cyanotic congenital heart disease (birth defects with oxygen levels lower than normal), that has not been fully repaired, including children who have had a surgical shunts and conduits.
- A congenital heart defect that’s been completely repaired with prosthetic material or a device for the first six months after the repair procedure. Prophylaxis is reasonable because endothelialization of prosthetic material occurs within six months after the procedure.
- Repaired congenital heart disease with residual defects, such as persisting leaks or abnormal flow at or adjacent to a prosthetic patch or prosthetic device.
Key changes for patients with congenital heart defects
Preventive antibiotics are no longer recommended for any other congenital heart disease than these:
- Cyanotic congenital heart disease (birth defects with oxygen levels lower than normal), that has not been fully repaired, including children who have had a surgical shunts and conduits.
- A congenital heart defect that’s been completely repaired with prosthetic material or a device for the first six months after the repair procedure. Prophylaxis is reasonable because endothelialization of prosthetic material occurs within six months after the procedure.
- Repaired congenital heart disease with residual defects, such as persisting leaks or abnormal flow at or adjacent to a prosthetic patch or prosthetic device.
Additionally, taking antibiotics just to prevent endocarditis is not recommended for patients who have procedures involving the reproductive, urinary or gastrointestinal tracts.
If you still require antibiotic prophylaxis for dental treatment or oral surgery, your cardiologist may give you an American Heart Association wallet card (see Figure 5 below).
Show this card to your dentist, pediatrician, family doctor or other physician. It advises them to give you the proper antibiotic and dose. For smaller children, the dose will vary according to the child’s weight. Always remind the dentist or doctor if you (or your child) are allergic to any antibiotics or other medications. Brushing, flossing, and visiting your dentist regularly helps keep your smile bright and prevents tooth and gum infections that could lead to endocarditis.
Your cardiologist can provide you more information and can answer your questions about preventing endocarditis.
Figure 5. American Heart Association prevention of infective endocarditis


Pregnancy
Women who had an atrioventricular canal defect that was surgically corrected before any permanent lung damage occurred can generally expect to have normal pregnancies. If there are problems like a leaking valve or irregular heart rhythms, you may be at increased risk for complications of pregnancy. If you have heart failure or pulmonary hypertension, pregnancy isn’t recommended. Women with unrepaired AV canal defects or who have leftover problems should talk to their cardiologist before deciding to get pregnant. See the sections on Pregnancy and on Genetic Counseling for more information. Pregnant women with repaired AV canal defects who are free of significant problems may not require high risk obstetrical care. In contrast those unrepaired AV canal defects, significant valve leaks or pulmonary hypertension.
Evaluation by a cardiologist trained in congenital heart disease (adult congenital cardiologist) is recommended for women with repaired or unrepaired atrioventricular canal defect before they attempt pregnancy.
Will I need more surgery?
The function of the repaired valves is a long-term concern. Some patients will need their valve replaced with a mechanical one when they get older. It’s rare that the valve can be further repaired. Other patients may need more surgery to close patch leaks.
Atrioventricular septal defect prognosis
The prognosis of untreated atrioventricular septal defect is poor 39. Around 50% of the infants with complete atrioventricular septal defect die during infancy, either due to congestive heart failure, pulmonary arterial hypertension or lung infections 35, 44. Those who survive beyond one year, they develop the irreversible pulmonary vascular disease (pulmonary hypertension) and later on Eisenmenger’s syndrome 39. Early repair minimizes the risk of premature death or pulmonary arterial hypertension 35. Repair of atrioventricular septal defect in early infancy conventionally carried greater morbidity and mortality than repair performed later in life, however, improved surgical techniques, heart protection, and postoperative care has led to a progressive reduction in operative mortality to <3% 35.
The historical reason for avoiding early repair was linked to the difficulties in the repair of flimsy atrioventricular valve leaflets in small children, however, due to large left to right shunting (after 4–6 weeks of life), such infants experience heart symptoms which are not always controlled with anti-congestive treatment 35. When associated with Down’s syndrome they have repeated chest infections, which further worsens abnormal pulmonary vascular resistance 35. Variables associated with increased hospital mortality include longer cardiopulmonary bypass and aortic cross-clamp time, the presence of left atrioventricular valve dysplasia is linked to worse preoperative function; more often needing additional measures for repair of left atrioventricular valve and a higher incidence of later reoperation for left atrioventricular valve dysfunction 35.
Patients with atrioventricular septal defect undergoing surgical repair have 15 years of survival of around 90%, and 9% to 10% of those require reoperation within 15 years 37. Surgery for left atrioventricular valve regurgitation is the most common indication for reoperation occurring very early at a median period of 1.1 years after the first surgery 35, 44. Reoperation can be better achieved with valve repair rather than valve replacement 35, 44. Repair during infancy 46 and unsutured clefts 47, 48 are reported to be risk factors influencing late left atrioventricular valve regurgitation.
Abbruzzese and his colleague 49 have elucidated that preoperative left atrioventricular valve insufficiency and associated valvular malformations are major determinants of late left atrioventricular valve insufficiency in partial atrioventricular septal defect. Furthermore, the study conducted by Kobayashi et al. 24 demonstrated left atrioventricular valve regurgitation as a major cause of late morbidity. Specifically, the postoperative grade of left atrioventricular valve regurgitation is the only independent risk factor for late left atrioventricular valve regurgitation. Consequently, it is imperative to emphasize the optimization of left atrioventricular valve repair to minimize residual regurgitation, even mild regurgitation. The surgical repair for left atrioventricular valve remains a challenge in patients younger than 3 months, less than four kilograms, or with other genetic disorders.
In a study by St. Louis et al 34, using the Society Thoracic Surgeons congenital heart surgery database analyzing the results of surgical correction of 2399 children from 101 centers from 2008 to 2011. Of these children, 78% had Down’s syndrome. Median age at surgery was 4.6 months with 11.8% aged <2.5 months. Pulmonary artery band removal was performed in 4.6% of patients at surgical repair 34.
Major complications occurred in 9.8% including permanent pacemaker implantation in 2.7% 34. Overall mortality was 3% 34. Weight <3.5 kg and age <2.5 months were associated with higher mortality, longer postoperative length of stay in the Intensive Care Unit (ICU) and higher incidence of major complications 34. Surprisingly, children with Down’s syndrome had lower morbidity and mortality than other children, and their duration of ICU stay was similar 34.
Xie et al 50 from the Royal children’s Hospital Melbourne presented data from 2000 to 2011 including 138 patients with common atrioventricular septal defect using the 2 patch technique in 92% and one patch in 2.2% their operative mortality was 1.4% and overall mortality was 5.8%. Freedom from reoperation was 84.3% at 8 years 50. Age >6 months at repair was associated with higher rates of reoperation, however, operating at age <6 months was associated with longer ICU stay. Moderate atrioventricular valve regurgitation at discharge was a risk factor for reoperation. Down’s syndrome present in 75% of patients was not a risk of a factor for higher mortality, morbidity, reoperations, ICU stay or duration of ventilation.
Pilchard et al 51 review on the perioperative and intensive care management of children with complete atrioventricular septal defect have highlighted some key topics.
- Down’s syndrome: up to 50% to 70% of children with atrioventricular septal defect may have Down’s syndrome, also having a high incidence of extracardiac anomalies including abnormalities of the central nervous system, hypotonia, seizures, gut abnormalities, thyroid disorders, and airway abnormalities such as tracheal stenosis and laryngotracheomalacia, also there may be sedation issues, pulmonary arterial hypertension, and vascular access concerns, higher right-sided cardiac pressures and pulmonary vascular resistance.
- Arrhythmias: There is a 72% incidence of postoperative arrhythmias most commonly junctional ectopic tachycardia, followed by complete AV block, ventricular tachycardia and reentrant supraventricular tachycardia (SVT) and nonsustained supraventricular tachycardia (SVT). At present, intravenous amiodarone is the recommended pharmacological treatment for most postoperative tachyarrhythmias to control the rate and restore AV synchrony.
- Pulmonary arterial hypertension: Pulmonary arterial hypertension occurring in approximately 2% of children with hypertensive crisis occurring in 0.75%. This results in prolonged mechanical ventilation and increased the length of ICU stay and mortality of 20%. The incidence has reduced after the introduction of nitric oxide and earlier age at surgery. Pulmonary artery catheters may be required in children with pulmonary artery pressures 60% of systemic or if inhaled nitric oxide was required for separation from the bypass. Management would include pulmonary vasodilators (inhaled nitric oxide), sedation and analgesia, judicious use of Positive End-Expiratory Pressure (PEEP) to prevent lung atelectasis, and sodium bicarbonate to buffer acidosis. Rebound pulmonary hypertension after stopping nitric oxide requires sildenafil.
- Thyroid hormone: Hypothyroidism is common in children with congenital heart disease and in Down’s is as common as 7% to 50% requiring routine screening. Cardiopulmonary bypass also suppresses thyroid hormone production, causing decreased myocardial contractility and cardiac output.
- Sedation and analgesia: especially in Down’s syndrome due to abnormal opioid receptor concentration in cerebral cortex along with differences in nociception, anxiety levels, and neurotransmission. Dexmedetomidine and caudal analgesia offer promising therapy, with dexmedetomidine infusion, having additional antiarrhythmic effects.
Janai et al 52 retrospectively studied 157 children with complete atrioventricular septal defect who underwent surgical correction from 1999 to 2013 with atrioventricular septal defect repair. Mean age at surgery was 125 ± 56.9 days. Nearly 63.6% of these children had Down’s syndrome 52. Although the authors have followed routine anesthetic, cardiopulmonary bypass and postoperative management principles as would be followed today across the world in most pediatric cardiac centers, their series is astonishing because of the 0% mortality reported by them compared to the 3%–5% reported in most of the other series 38, 43, 41, 53, the main reasons probably are the early age at surgery, overall team experience, protocolized management, use of transesophageal echocardiography both intra- and postoperatively for management.
- Centers for Disease Control and Prevention. Division of Birth Defects and Developmental Disabilities. Facts about Atrioventricular Septal Defect (AVSD). https://www.cdc.gov/ncbddd/heartdefects/avsd.html[↩][↩][↩][↩][↩]
- Cai Y, Chen R, Chen G, Shi Q, Mi Y, Zhang H, Jia B. Middle to long-term outcomes of surgical repair for atrioventricular septal defect: a single-center study. J Thorac Dis. 2022 Oct;14(10):3706-3718. doi: 10.21037/jtd-22-790[↩]
- Li J, Liu T, Xie Y, Zhang X, Liu J, Zhang R, Yang Y, Zhu S, Yang Y, Wang J, Zhang L, Lv Q, He L, Fang L, Wu W, Li H, Li Y, Xie M. Risk factors for the recurrence of left atrioventricular valvular regurgitation after surgical repair of partial and transitional atrioventricular septal defect. J Thorac Dis. 2024 May 31;16(5):3117-3128. doi: 10.21037/jtd-23-1694[↩][↩][↩]
- Fong LS, Youssef D, Ayer J, Nicholson IA, Winlaw DS, Orr Y. Correlation of ventricular septal defect height and outcomes after complete atrioventricular septal defect repair. Interact Cardiovasc Thorac Surg. 2022 Feb 21;34(3):431-437. doi: 10.1093/icvts/ivab263[↩]
- Zhou X, Yang T, Ruan Y, Zhang Y, Liu X, Zhao Y, Gu X, Xu X, Han J, He Y. Application of neural networks in prenatal diagnosis of atrioventricular septal defect. Transl Pediatr. 2024 Jan 29;13(1):26-37. doi: 10.21037/tp-23-394[↩]
- Olariu IC, Popoiu A, Ardelean AM, Isac R, Steflea RM, Olariu T, Chirita-Emandi A, Stroescu R, Gafencu M, Doros G. Challenges in the Surgical Treatment of Atrioventricular Septal Defect in Children With and Without Down Syndrome in Romania-A Developing Country. Front Pediatr. 2021 Jul 7;9:612644. doi: 10.3389/fped.2021.612644[↩]
- Bamberg M, Simon M, Bandini A, Hahn JK, Schlensak C, Icheva V, Hofbeck M, Rosenberger P, Magunia H, Keller M. Left Atrioventricular Transvalvular Pressure Gradients Derived from Intraoperative and Postoperative Echocardiograms following Atrioventricular Septal Defect Repair. Diagnostics (Basel). 2023 Mar 2;13(5):957. doi: 10.3390/diagnostics13050957[↩]
- Reynen S, Hövels-Gürich HH, Vazquez-Jimenez JF, Messmer BJ, Sachweh JS. Long-Term Outcome Up To 40 Years after Single Patch Repair of Complete Atrioventricular Septal Defect in Infancy or Childhood. Thorac Cardiovasc Surg. 2021 Dec;69(S 03):e68-e75. doi: 10.1055/s-0041-1740070[↩]
- Waldmann V, Bessière F, Gardey K, Hascoët S, Henaine R, Iserin L, Ladouceur M, Bonnet D, Marijon E, Maltret A, Combes N, de Groot N. Catheter ablation of atrial tachyarrhythmias in patients with atrioventricular septal defect. Europace. 2023 Aug 2;25(9):euad275. doi: 10.1093/europace/euad275[↩]
- Hu H, Geng Z, Zhang S, Xu Y, Wang Q, Chen S, Zhang B, Sun K, Lu Y. Rare copy number variation analysis identifies disease-related variants in atrioventricular septal defect patients. Front Genet. 2023 Feb 3;14:1075349. doi: 10.3389/fgene.2023.1075349[↩]
- Kadowaki S, Saprungruang A, Okumura M, Dragulescu A, Honjo O. Unexpected Growth of Small Right Ventricle After Failed Repair of Atrioventricular Septal Defect. Ann Thorac Surg Short Rep. 2023 Aug 23;2(1):63-65. doi: 10.1016/j.atssr.2023.08.002[↩]
- Chandiramani A, Bader V, Finlay E, Lilley S, Young D, Peng E. The impact of surgical repair on left ventricular outflow tract in atrioventricular septal defect with common atrioventricular valve orifice. JTCVS Open. 2023 Jan 19;14:385-395. doi: 10.1016/j.xjon.2022.11.023[↩]
- Parker SE, Mai CT, Canfield MA, Rickard R, Wang Y, Meyer RE, Anderson P, Mason CA, Collins JS, Kirby RS, & Correa A, for the National Birth Defects Prevention Network. Updated national birth prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol 2010;88:1008-1016.[↩]
- Jacobs JP, Burke RP, Quintessenza JA, Mavroudis C. Congenital heart surgery nomenclature and database project: Atrioventricular canal defect. Ann Thorac Surg. 2000;69:S36–43. doi: 10.1016/s0003-4975(99)01235-7[↩]
- LILLEHEI CW, COHEN M, WARDEN HE, VARCO RL. The direct-vision intracardiac correction of congenital anomalies by controlled cross circulation; results in thirty-two patients with ventricular septal defects, tetralogy of Fallot, and atrioventricularis communis defects. Surgery. 1955 Jul;38(1):11-29.[↩][↩][↩]
- Rastelli G, Kirklin JW, Titus JL. Anatomic observations on complete form of persistent common atrioventricular canal with special reference to atrioventricular valves. Mayo Clin Proc. 1966 May;41(5):296-308.[↩]
- McGrath LB, Gonzalez-Lavin L. Actuarial survival, freedom from reoperation, and other events after repair of atrioventricular septal defects. J Thorac Cardiovasc Surg 1987;94:582-90. 10.1016/S0022-5223(19)36222-1[↩]
- Pan-Chih , Chen-Chun. Surgical treatment of atrioventricular canal malformations. Ann Thorac Surg 1987;43:150-4. 10.1016/S0003-4975(10)60384-0[↩]
- Ceithaml EL, Midgley FM, Perry LW. Long-term results after surgical repair of incomplete endocardial cushion defects. Ann Thorac Surg 1989;48:413-6. 10.1016/S0003-4975(10)62868-8[↩]
- Baufreton C, Journois D, Leca F, et al. Ten-year experience with surgical treatment of partial atrioventricular septal defect: risk factors in the early postoperative period. J Thorac Cardiovasc Surg 1996;112:14-20. 10.1016/S0022-5223(96)70172-1[↩]
- Najm HK, Williams WG, Chuaratanaphong S, et al. Primum atrial septal defect in children: early results, risk factors, and freedom from reoperation. Ann Thorac Surg 1998;66:829-35. 10.1016/S0003-4975(98)00607-9[↩]
- Jacobs JP, Burke RP, Quintessenza JA, et al. Congenital Heart Surgery Nomenclature and Database Project: atrioventricular canal defect. Ann Thorac Surg 2000;69:S36-43. 10.1016/S0003-4975(99)01235-7[↩]
- Beaton AZ, Pike JI, Stallings C, et al. Predictors of repair and outcome in prenatally diagnosed atrioventricular septal defects. J Am Soc Echocardiogr 2013;26:208-16. 10.1016/j.echo.2012.11.007[↩]
- Kobayashi Y, Kasahara S, Sano S, et al. Staged repair for complete atrioventricular septal defect in patients weighing less than 4.0 kg. J Thorac Cardiovasc Surg 2024;167:1136-44. 10.1016/j.jtcvs.2023.07.003[↩][↩]
- Gellis L, McGeoghegan P, Lu M, et al. Left atrioventricular valve repair after primary atrioventricular canal surgery: Predictors of durability. J Thorac Cardiovasc Surg 2023;166:1168-77. 10.1016/j.jtcvs.2023.04.004[↩]
- Chowdhury UK, Airan B, Malhotra A, et al. Specific issues after surgical repair of partial atrioventricular septal defect: actuarial survival, freedom from reoperation, fate of the left atrioventricular valve, prevalence of left ventricular outflow tract obstruction, and other events. J Thorac Cardiovasc Surg 2009;137:548-555.e2. 10.1016/j.jtcvs.2008.04.035[↩]
- Schleiger A, Miera O, Peters B, et al. Long-term results after surgical repair of atrioventricular septal defect. Interact Cardiovasc Thorac Surg 2019;28:789-96. 10.1093/icvts/ivy334[↩]
- Goutallier CS, Buratto E, Schulz A, et al. Repair of complete atrioventricular septal defect between 2 and 3.5 kilograms: Defining the limits of safe repair. J Thorac Cardiovasc Surg 2022;164:1167-75. 10.1016/j.jtcvs.2022.02.031[↩]
- Mery CM, Zea-Vera R, Chacon-Portillo MA, et al. Contemporary Outcomes After Repair of Isolated and Complex Complete Atrioventricular Septal Defect. Ann Thorac Surg 2018;106:1429-37. 10.1016/j.athoracsur.2018.06.006[↩]
- Airaksinen R, Mattila I, Jokinen E, et al. Complete Atrioventricular Septal Defect: Evolution of Results in a Single Center During 50 Years. Ann Thorac Surg 2019;107:1824-30. 10.1016/j.athoracsur.2019.01.020[↩]
- Overman DM, Baffa JM, Cohen MS, Mertens L, Gremmels DB, Jegatheeswaram A, et al. Unbalanced atrioventricular septal defect: Definition and decision making. World J Pediatr Congenit Heart Surg. 2010;1:91–6. doi: 10.1177/2150135110363024[↩]
- Jegatheeswaran A, Pizarro C, Caldarone CA, Cohen MS, Baffa JM, Gremmels DB, et al. Echocardiographic definition and surgical decision-making in unbalanced atrioventricular septal defect: A congenital heart surgeons’ society multiinstitutional study. Circulation. 2010;122:S209–15. doi: 10.1161/CIRCULATIONAHA.109.925636[↩]
- Hoohenkerk GJ, Bruggemans EF, Rijlaarsdam M, Schoof PH, Koolbergen DR, Hazekamp MG. More than 30 years’ experience with surgical correction of atrioventricular septal defects. Ann Thorac Surg. 2010 Nov;90(5):1554-61. doi: 10.1016/j.athoracsur.2010.06.008[↩][↩]
- St Louis JD, Jodhka U, Jacobs JP, He X, Hill KD, Pasquali SK, Jacobs ML. Contemporary outcomes of complete atrioventricular septal defect repair: analysis of the Society of Thoracic Surgeons Congenital Heart Surgery Database. J Thorac Cardiovasc Surg. 2014 Dec;148(6):2526-31. doi: 10.1016/j.jtcvs.2014.05.095[↩][↩][↩][↩][↩][↩][↩]
- Chauhan S. Atrioventricular septal defects. Ann Card Anaesth. 2018 Jan-Mar;21(1):1-3. doi: 10.4103/aca.ACA_219_17[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- LILLEHEI CW. Controlled cross circulation for direct-vision intracardiac surgery; correction of ventricular septal defects, atrioventricularis communis, and tetralogy of Fallot. Postgrad Med. 1955 May;17(5):388-96. doi: 10.1080/00325481.1955.11708211[↩][↩]
- Crawford FA Jr, Stroud MR. Surgical repair of complete atrioventricular septal defect. Ann Thorac Surg. 2001 Nov;72(5):1621-8; discussion 1628-9. doi: 10.1016/s0003-4975(01)03170-8[↩][↩]
- Ginde S, Lam J, Garic KD, Cohen S. Long term outcomes after surgical repair of complete atrio ventricular septal defect. J Thorac Cardio Vasc Surg. 2015;150:369–74. doi: 10.1016/j.jtcvs.2015.05.011[↩][↩][↩]
- Ahmed I, Anjum F. Atrioventricular Septal Defect. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562194[↩][↩][↩][↩][↩]
- Vida VL, Tessari C, Castaldi B, Padalino MA, Milanesi O, Gregori D, Stellin G. Early Correction of Common Atrioventricular Septal Defects: A Single-Center 20-Year Experience. Ann Thorac Surg. 2016 Dec;102(6):2044-2051. doi: 10.1016/j.athoracsur.2016.09.020[↩]
- Vida VL, Tessari C, Castaldi B, Padalino MA, Milanesi O, Gregori D, et al. Early correction of common atrioventricular septal defects: A single-center 20-year experience. Ann Thorac Surg. 2016;102:2044–51. doi: 10.1016/j.athoracsur.2016.09.020[↩][↩]
- Cohen MS, Jacobs ML, Weinberg PM, Rychik J. Morphometric analysis of unbalanced common atrioventricular canal using two-dimensional echocardiography. J Am Coll Cardiol. 1996;28:1017–23. doi: 10.1016/s0735-1097(96)00262-8[↩]
- Sojak V, Kooij M, Yazdanbakhsh A, Koolbergen DR, Bruggemans EF, Hazekamp MG, et al. A single-centre 37-year experience with reoperation after primary repair of atrioventricular septal defect. Eur J Cardiothorac Surg. 2016;49:538–44. doi: 10.1093/ejcts/ezv115[↩][↩]
- Calabrò R, Limongelli G. Complete atrioventricular canal. Orphanet J Rare Dis. 2006 Apr 5;1:8. doi: 10.1186/1750-1172-1-8[↩][↩][↩][↩]
- Infective Endocarditis. https://www.heart.org/en/health-topics/infective-endocarditis[↩]
- Giamberti A, Marino B, di Carlo D, et al. Partial atrioventricular canal with congestive heart failure in the first year of life: surgical options. Ann Thorac Surg 1996;62:151-4. 10.1016/0003-4975(96)00262-7[↩]
- Pozzi M, Remig J, Fimmers R, et al. Atrioventricular septal defects. Analysis of short- and medium-term results. J Thorac Cardiovasc Surg 1991;101:138-42. 10.1016/S0022-5223(19)36803-5[↩]
- Aharon AS, Laks H, Drinkwater DC, et al. Early and late results of mitral valve repair in children. J Thorac Cardiovasc Surg 1994;107:1262-70; discussion 1270-1. 10.1016/S0022-5223(94)70047-8[↩]
- Abbruzzese PA, Napoleone A, Bini RM, et al. Late left atrioventricular valve insufficiency after repair of partial atrioventricular septal defects: anatomical and surgical determinants. Ann Thorac Surg 1990;49:111-4. 10.1016/0003-4975(90)90366-E[↩]
- Xie O, Brizard CP, d’Udekem Y, Galati JC, Kelly A, Yong MS, et al. Outcomes of repair of complete atrioventricular septal defect in the current era. Eur J Cardiothorac Surg. 2014;45:610–7. doi: 10.1093/ejcts/ezt444[↩][↩]
- Pilchard J, Dadlani G, Andropoulos D, Jacobs JP, Cooper DS. Intensive care and perioperative management of patients with complete atrioventricular septal defect. World J Pediatr Congenit Heart Surg. 2010;1:105–11. doi: 10.1177/2150135109360815[↩]
- Janai AR, Bellinghausen W, Turton E, Bevilacqua C, Zakhary W, Kostelka M, et al. Retrospective study of complete atrioventricular canal defects: Anesthetic and perioperative challenges. Ann Card Anaesth. 2018;21:15–21. doi: 10.4103/aca.ACA_110_17[↩][↩]
- St. Louis JD, Jodkka U, Jacobs JP, Xia H. Contemporary outcomes of complete AVSD repair: Analysis of the STS congenital heart surgery database. J Thorac Cardio Vasc Surg. 2014;148:2526–31. doi: 10.1016/j.jtcvs.2014.05.095[↩]




{kind=link}