
Contents
What is abdominoplasty
Abdominoplasty is an abdominal wall surgery, which is a procedure that improves the appearance of flabby, stretched-out abdominal (belly) muscles and skin. Abdominoplasty surgery is also called a tummy tuck. Abdominoplasty surgery can range from a simple mini-abdominoplasty to more extensive surgery. Abdominoplasty is able to eliminate excess skin and stubborn excess deposits of fat in the midsection. Abdominoplasty surgery can also repair abdominal muscle separation, known as diastasis recti. Abdominoplasty surgery can help you achieve a tighter, flatter, more fit appearance of the abdomen and flanks (love handles).
The abdominoplasty is one of the most commonly performed aesthetic surgical procedures across the world. It is estimated that more than 800,000 people undergo this operation each year, making it the sixth most common cosmetic procedure 1. The main objective of an abdominoplasty is to reshape the body contour by means of excising redundant skin and fat tissue to remodel the abdominal wall. Since its initial conception more than a century ago, various surgical alternatives have been proposed 2. However, it was during the 1960s and 1970s that the contributions of Vernon 3, Pitanguy 4 and Grazer 5 established the founding pillars of modern abdominoplasty. Abdominoplasty is also the second most popular body cosmetic surgery nationwide and is performed over 100,000 times per year in the United States.
Abdominoplasty surgery is not the same as liposuction, which is another way to remove fat. But, abdominoplasty is sometimes combined with liposuction. Abdominoplasty in combination with liposuction of the abdomen and flanks can remove stubborn pads of fat that may be resistant to diet and exercise.
An abdominoplasty is not a substitute for weight loss and patients should reach their goal weight prior to undergoing abdominoplasty surgery. However, if you have subcutaneous fat around your abdomen that persists despite your best weight loss efforts, your American Board of Plastic Surgery certified plastic surgeon can include liposuction in your abdominoplasty procedure to better contour the midsection.
The best candidates for an abdominoplasty have loose skin around their abdomen, as well as loose abdominal muscles (diastasis recti) or excess fatty deposits. Most frequently, abdominoplasty patients are women who have been pregnant, but the procedure can also benefit men or women who have lost a significant amount of weight that left them with baggy skin and an unflattering midsection. A consultation with a board certified plastic surgeon (American Board of Plastic Surgery) will help you better understand the results you can expect to see from an abdominoplasty surgery and whether you might be a good candidate
During an abdominoplasty surgery, the surgeon will make a cut in the fold under the belly. This is the “bikini line.” Skin is also cut around the belly button. A large area of fat and skin are then pulled away from the muscle.
Reasons for abdominoplasty
Most of the time, abdominoplasty surgery is an elective or cosmetic procedure because it is an operation you choose to have. Abdominoplasty surgery is not usually needed for health reasons. Cosmetic abdomen repair can help improve appearance, particularly after a lot of weight gain or loss. Abdominoplasty surgery helps flatten the lower abdomen and tighten stretched skin.
A flabby abdomen is caused not only by the accumulation of fat, but also by the poor elasticity of the skin, excess skin, and the stretching of the inner girdle of connective tissue (abdominal fascia) and abdominal muscles that extends from the ribs to the pubic bone. This inner girdle, which holds the internal organs in place, is responsible for the tone and appearance of the abdomen.
Your abdomen is more likely to protrude after your abdominal fascia has been stretched during pregnancy or after significant changes in your weight. A tummy tuck can remove loose, excess skin and fat, and tighten weak fascia. A tummy tuck can also remove stretch marks and excess skin in the lower abdomen below the bellybutton. However, a tummy tuck won’t correct stretch marks outside of this area.
Abdominoplasty surgery may also help relieve skin rashes or infections that develop under large flaps of skin.
Abdominoplasty can be helpful when:
- Diet and exercise have not helped improve muscle tone, such as in women who have had more than one pregnancy.
- Skin and muscle cannot regain its normal tone. This can be a problem for very overweight people who lost a lot of weight.
You might consider a abdominoplasty if:
- You have excess skin that’s accumulated around the area of your bellybutton
- You have a weak lower abdominal wall
- Liposuction didn’t adequately improve the appearance of your abdomen
- You previously had a C-section and have retracted scarring
If you’ve previously had a Caesarean section, your plastic surgeon might be able to incorporate your existing C-section scar into your abdominoplasty scar.
An abdominoplasty can also be done in combination with other body contouring cosmetic procedures, such as breast surgery.
An abdominoplasty isn’t for everyone. Your doctor might caution against an abdominoplasty if you:
- Plan to lose a significant amount of weight
- Might consider future pregnancy
- Have a severe chronic condition, such as heart disease, diabetes or irritable bowel syndrome
- Have a body mass index (BMI) that’s greater than 30
Abdominoplasty procedure is a major surgery. Be sure you understand the risks and benefits before having it.
Abdominoplasty is not used as an alternative to weight loss.
Abdominoplasty risks
Risks for anesthesia and surgery in general are:
- Reactions to medicines
- Breathing problems
- Bleeding, blood clots, or infection
Risks for abdominoplasty surgery are:
- Loss of skin
- Nerve damage that can cause pain or numbness in part of your belly
- Poor healing
- Fluid accumulation beneath the skin (seroma). Drainage tubes left in place after surgery can help reduce the risk of seroma. Your doctor might also remove fluid after surgery using a needle and syringe.
- Poor wound healing. Sometimes areas along the incision line heal poorly or begin to separate. You might be given antibiotics during and after surgery to prevent a resulting infection.
- Excessive scarring. The incision scar from a abdominoplasty is permanent, but is placed along the easily hidden bikini line. The length and visibility of the scar will vary from person to person.
- Tissue necrosis. During a abdominoplasty, fatty tissue deep within your skin in the abdominal area might get damaged or die. Smoking increases the risk of tissue necrosis. Depending on the size of the area, tissue might heal on its own within weeks or require a surgical touch-up procedure.
- Changes in skin sensation. During a abdominoplasty, the repositioning of your abdominal tissues can affect superficial sensory nerves in the abdominal area, and infrequently, in the upper thighs. You’ll likely feel some reduced sensation or numbness. This usually diminishes in the months after the procedure.
Like any other type of major surgery, a abdominoplasty poses a risk of bleeding, infection and an adverse reaction to anesthesia.
According to the published case series, local complications are considerably more common than complications with systemic repercussions 6. Approximately 10% to 20% of patients suffer a local complication following abdominoplasty, while fewer than 1% suffer a systemic complication. Complications including seroma, hematoma, infection, skin necrosis, suture extrusions, hypertrophic scars, neurological symptoms, umbilical anomalies, deep venous thrombosis and pulmonary thromboembolism, respiratory distress, and death 6.
The combination of abdominoplasty with abdominal liposuction remains a controversial subject. This controversy reached its zenith in February of 2004 when, after several patient deaths, the state of Florida placed a temporary moratorium preventing the simultaneous combination of abdominoplasty with liposuction in the office setting, mandating a minimum 14-day interval between the two operations 7. This has led to the evolution of a different operation entirely, sometimes called lipoabdominoplasty 8. Lipoabdominoplasty differs from the combination of abdominoplasty and liposuction in that the liposuction is performed first in lipoabdominoplasty, and there is limited undermining of the abdominal flap in the area above the umbilicus, thus sparing multiple perforator vessels. This new operation slowly evolved out of many surgeons’ efforts. This operation differs from traditional abdominoplasty in several ways. First, the liposuction is performed first and the flap is elevated with hydrodissection and liposuction. Second, there is typically limited undermining of the flap above the umbilicus. Third, there is usually no closure, or only segmental closure of the rectus diastasis 9. The results shown in the article by Brauman and Capocci are impressive, and this is a useful technique for body contouring 9. Avelar’s technique involves even less undermining of the superior abdominal flap, and the umbilicus is not transposed 10. His technique does involve the addition of skin excision in the inframammary area in selected cases.
Despite all the complications mentioned, abdominoplasties and lipoabdominoplasties are reproducible and very gratifying operations for both patients and surgeons.
Seroma
The accumulation of serous fluid underneath the abdominal flap is the most frequent complication following an abdominoplasty. In the series of 1,008 cases published by Neaman et al. 11 in 2013, the reported seroma rate was 15.4%. In this study, the authors identified an association between adjuvant liposuction and a higher risk of suffering a seroma, particularly in male patients.
The possibility of a higher incidence of seroma in lipoabdominoplasties than in abdominoplasties without liposuction remains controversial. Najera et al. 12 published a series of 200 patients, showing that the seroma rates in the abdominoplasty and lipoabdominoplasty groups were 16% and 31.2%, respectively. These percentages are far greater than the 0.04% seroma rate reported by Hurvitz et al. 13. Unfortunately, no consensus exists regarding the definition of a clinically significant seroma or an objective method of assessing this outcome.
Fortunately, most seromas usually resolve after puncture and repeated aspiration. Injection of steroids after draining a seroma to accelerate the process is not backed by supporting evidence. Alkylating agents, such as bleomycin, doxycycline, and talcum powder 14, have been used for recurrent seromas, inspired by their use for persistent pleural effusion. Surgery is a last resort, with the objective of obliterating the space occupied by the seroma by approximating its walls 15.
Infection
Infections are the second most common complication following abdominoplasty, with an estimated incidence between 1% and 3.8% 16, including operative site infections and infected seromas. There is often inflammation of a delimitated area that typically presents erythema, edema, tenderness, and an elevated local temperature. Exudate and systemic symptoms might also be present in more severe infections.
Immunosuppressed states, malnutrition, and diabetes are known risk factors for any kind of infectious process. Particularly, for abdominoplasties, obese and overweight patients seem to have an elevated infection risk 17.
Tobacco consumption also increases the risk of infection, raising the infection rate to 12.7%, compared with 5% in nonsmokers, according to the case series published by Manassa et al. 18. This is explained by the vasoconstriction that follows smoking, which impairs cellular immunity 19. Other complications, such as flap necrosis due to insufficient irrigation and seromas, also increase the risk of infection.
Skin necrosis
Flap compromise due to insufficient perfusion can cause different complications depending on its severity. Epidermolysis is a mild variant, and its natural course is towards spontaneous reepithelization. However, when necrosis occurs in the skin and subdermal tissue, healing can be a tortuous process. Initially, necrosis may manifest with signs of insufficient irrigation, such as delayed capillary fill and diminished local temperature.
The incidence of skin necrosis varies between 3% and 4.4% if a limited dissection technique is used, preserving an adequate number of perforating vessels 20. The rate of reoperations to achieve an acceptable aesthetic result associated with this complication is less than 1%.
The most important risk factor for this complication is tobacco consumption, which triples the risk 21. Cessation of this habit lowers the risk and should be encouraged in every patient before surgery. Performing abdominoplasties along with other aesthetic operations at the same time also increases the risk of skin necrosis.
Hematoma
Hematomas are less frequent than seromas or skin necrosis, with a reported incidence of 2% 20. Neither Samra et al. 22 nor Hensel et al. 23 encountered any differences in the rate of this complication between patients who underwent abdominoplasties and those who underwent lipoabdominoplasties 22.
The clinical presentation of a hematoma depends on its volume. If it is small enough, it can be completely asymptomatic, but if larger it manifests with swelling, localized pain, and ecchymosis, usually during the first 24 hours. Large hematomas with active bleeding can consequently result in hemodynamic instability and hypovolemic shock, which is a reason why they need to be carefully monitored in order to decide promptly whether exploration is indicated 24.
The risk factors for hematoma as a complication of abdominoplasty, as for any other surgical procedure involving the abdominal wall, are hypertension, unsuccessful hemostasis during the operation, and congenital and acquired coagulopathies. Moreover, a higher incidence of hematoma has been demonstrated in patients with a higher body mass index 25.
Other local complications
Suture extrusion is another local complication that, according to the published literature, occurs in at least 5% of cases 26. The consequent inflammation and swelling usually cause great concern, especially when associated with exudate. Fortunately, resolution is fast once the offending suture is removed. The use of slow-reabsorption barbed sutures is associated with higher rates of suture extrusion, while their fast-absorption variants (V-Loc 90, Covidien) are less closely associated with this side effect 27.
Necrosis of the umbilicus due to insufficient irrigation through its pedicle occurs in about 0.2% of cases 26. Special care while performing the plication must be taken to avoid strangulation of the umbilicus.
Approximately 1.9% of patients suffer some degree of neurological symptoms following abdominoplasty, with the lateral femoral cutaneous nerve the most commonly involved, followed by the iliohypogastric nerve 28. A careful dissection around the anterior superior iliac spine allows preservation of the lateral femoral cutaneous nerve. Neurological lesions can cause neuropathic pain, hypoesthesia, paraesthesia, hyperesthesia, or allodynia. Meralgia paresthetica is the most common presentation following a lateral cutaneous nerve injury. Once diagnosed, conservative treatment includes massages and analgesia. The use of anticonvulsants, tricyclic antidepressants, nerve blocks, and steroid injections can also be indicated, depending on the clinical presentation. If after 6 months there is no resolution and symptoms are severe, referral to a pain specialist is recommended. Surgical exploration of the nerve trajectory may be useful to free an entrapment or to excise a neuroma 29.
Rupture of the vertical plication of the rectus abdominis sheath has been reported. It can occur years after the abdominoplasty and present as fast-growing abdominal pseudo-tumors 30. Clinically, these are difficult to differentiate from malignant tumours or hernias, and for this reason, imaging studies are usually required to confirm the diagnosis.
Systemic complications
Systemic complications are the most feared and severe complications and, fortunately, the least frequent ones after an abdominoplasty. The incidence of thromboembolism ranges between 0.3% and 1.1%, depending on the series 20. These reports contain cases diagnosed using Doppler ultrasound imaging, without consideration of subclinical deep venous thromboses that resolve spontaneously without causing symptoms. Apart from the classically described risk factors for this complication, patients undergoing abdominoplasty are at an even higher risk if their body mass index is 30 kg/m2 or more 31. Combining this surgery with other intraabdominal operations at the same time increases the risk of deep venous thrombosis to 2.17%, contrasting with an incidence of 0.76% when it is associated with another aesthetic procedure 31. Reports of fat embolism following an abdominoplasty are scarce 32.
The indication for thromboembolism prophylaxis in abdominoplasties is still a controversial issue. Newall et al. 33 and Hatef et al. 34 have reported that using low-molecular-weight heparin in high-risk patients reduced the rate of deep venous thrombosis. These studies also showed a consequent increase in the incidence of haematomas when chemoprophylaxis was used. Other authors prefer prevention protocols that avoid the use of low-molecular-weight heparin by using intermittent pneumatic compression intraoperatively and until the patient is discharged, in combination with early assisted walking in the first postoperative hours. These precautions, along with ensuring tobacco cessation for at least a month before surgery, allowed Somogyi et al. 35 to report only 1 case of deep venous thrombosis among the 404 patients in their case series.
Death following an abdominoplasty has rarely been reported in the literature 36, with an incidence ranging from 0.04% to 0.16% in series published around 25 years ago 37 and mortality has not been mentioned in more recent series. Most cases of mortality were attributed to massive pulmonary embolism. However, these statistics do not consider abdominoplasties performed by uncertified plastic surgeons working under limited safety conditions.
Before the abdominoplasty procedure
Initially, you’ll talk to a plastic surgeon about a tummy tuck. During your first visit, your plastic surgeon will likely:
- Review your medical history. Be prepared to answer questions about current and past medical conditions. Talk about any medications you’re taking or you have taken recently, as well as any surgeries you’ve had. Tell your doctor if you are allergic to any medications. If your desire for a tummy tuck is related to weight loss, your doctor will likely ask detailed questions about your weight gain and loss.
- Do a physical exam. To determine your treatment options, the doctor will examine your abdomen. The doctor might also take pictures of your abdomen for your medical record.
- Discuss your expectations. Explain why you want a tummy tuck, and what you’re hoping for in terms of appearance after the procedure. Make sure you understand the benefits and risks, including scarring. Keep in mind that previous abdominal surgery might limit your results.
Tell your surgeon or nurse:
- If you could be pregnant
- What medicines you are taking, even drugs, supplements, or herbs you bought without a prescription
Before abdominoplasty surgery:
- Several days before surgery, you may be asked to stop taking blood thinning drugs. These include aspirin, ibuprofen (Advil, Motrin), warfarin (Coumadin), and herbal supplements, which can increase bleeding.
- Ask your surgeon which drugs you should still take on the day of your surgery.
- If you smoke, try to stop. Smoking decreases blood flow in the skin and can slow the healing process. In addition, smoking increases the risk of tissue damage. If you smoke, your doctor will recommend that you stop smoking before surgery and during recovery.
- Maintain a stable weight. Ideally, you’ll maintain a stable weight for at least 12 months before having a abdominoplasty. If you’re severely overweight, your doctor will recommend that you lose weight before the procedure. Significant weight loss after the procedure can diminish your results.
- Take medication to prevent complications. Shortly before your abdominoplasty, you’ll need to begin taking an anticoagulant to prevent blood clotting.
- Arrange for help during recovery. Make plans for someone to drive you home after you leave the hospital and stay with you for at least the first night of your recovery at home.
On the day of abdominoplasty surgery:
- Follow instructions about when to stop eating and drinking.
- Take the drugs your surgeon told you to take with a small sip of water.
- Arrive at the hospital on time.
Abdominoplasty procedure
Your abdominoplasty surgery will be done in an operating room in a hospital or an outpatient surgical facility. You will receive general anesthesia. This will keep you asleep and pain-free during the procedure. The abdominoplasty surgery takes 2 to 6 hours. You can expect to stay in the hospital for 1 to 3 days after abdominoplasty surgery.
After you receive anesthesia, your surgeon will make a cut (incision) across your abdomen to open up the area. This cut will be just above your pubic area (see Figure 1). Your plastic surgeon will make incisions to remove most of the skin and fat between your bellybutton and pubic hair in a horizontal oval or elliptical shape. The fascia, which overlies the abdominal muscles, will be tightened with permanent sutures.
Your surgeon will remove fatty tissue and loose skin from the middle and lower sections of your abdomen to make it firmer and flatter. In extended full abdominoplasty surgeries, the surgeon also removes excess fat and skin (love handles) from the sides of the abdomen. Your abdominal muscles may be tightened also.
Your plastic surgeon will then reposition the skin around your bellybutton. Your bellybutton will be brought out through a small incision and sutured in its normal position. The incision from hip to hip above the pubic hair will be stitched together and will leave a scar that falls along the natural crease within the bikini line.
Mini abdominoplasty is performed when there are areas of fat pockets (love handles). It can be done with much smaller cuts.
Your surgeon will close your cut with stitches. Small tubes called drains may be inserted to allow fluid to drain out of your cut. These will be removed later.
A firm elastic dressing (bandage) will be placed over your abdomen.
During the procedure you might be given an antibiotic to prevent infection.
The abdominoplasty procedure typically takes about three hours.
For less complicated abdominoplasty surgery, your surgeon may use a medical device called an endoscope. Endoscopes are tiny cameras that are inserted into the skin through very small cuts. They are connected to a video monitor in the operating room that allows the surgeon to see the area being worked on. Your surgeon will remove excess fat with other small tools that are inserted through other small cuts. This surgery is called endoscopic surgery.
Figure 1. Abdominoplasty surgery
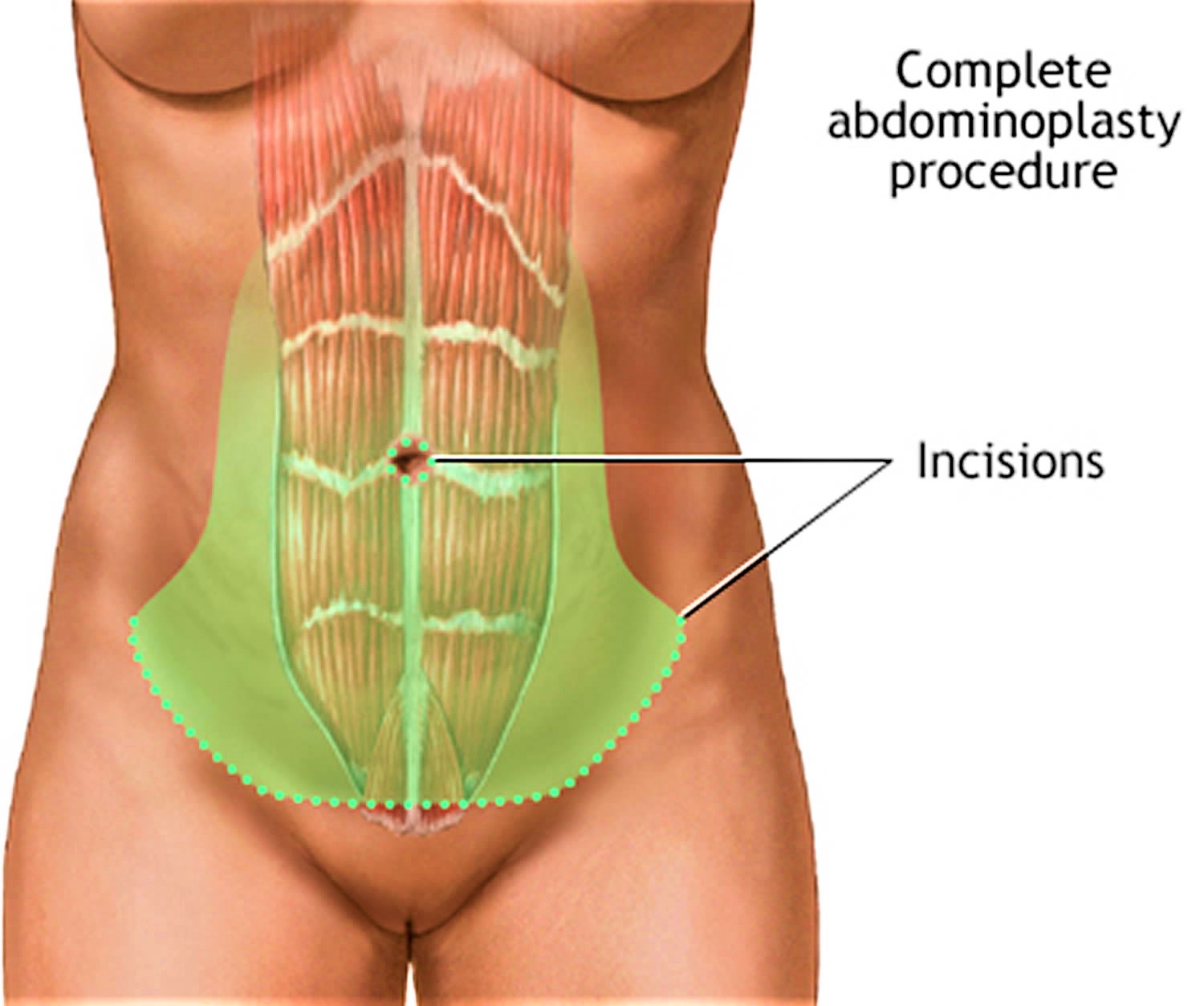
Figure 2. Abdominoplasty surgery – the surgeon tightens the abdominal muscles in the belly
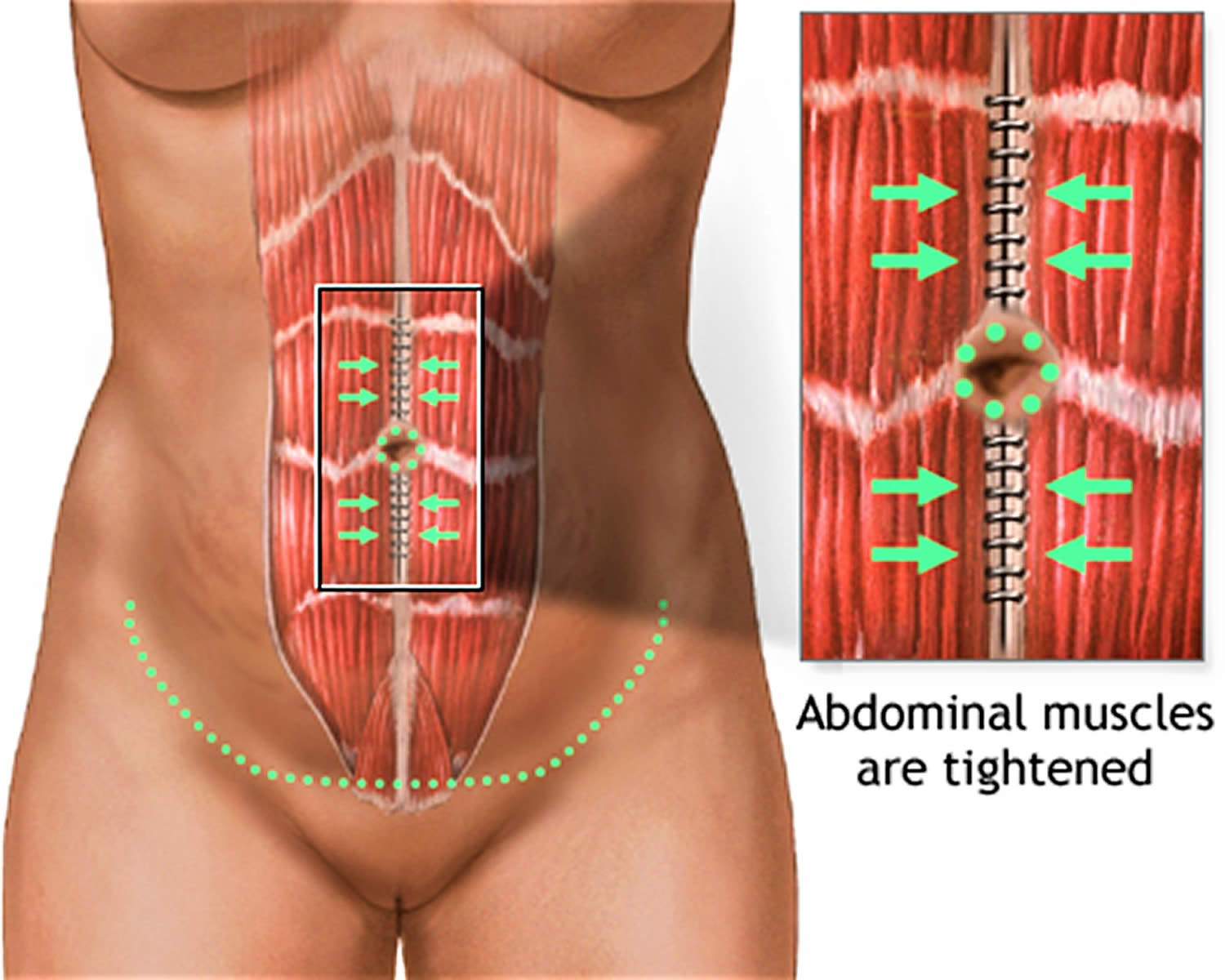
Figure 3. Abdominoplasty surgery – the skin is then stretched downward. Extra skin and fat are trimmed away. A new hole will be cut for the belly button. The opening will then be closed with stitches.
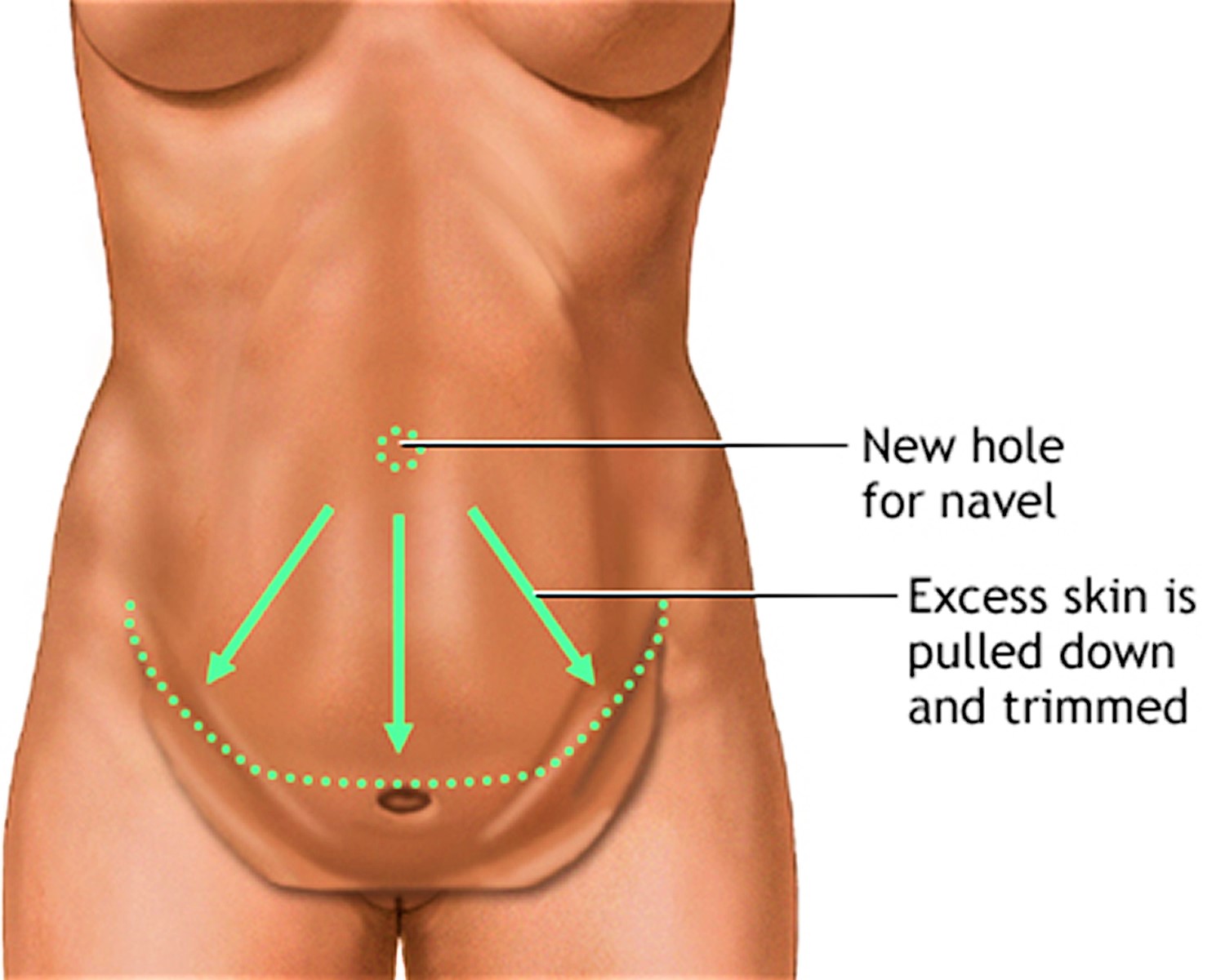
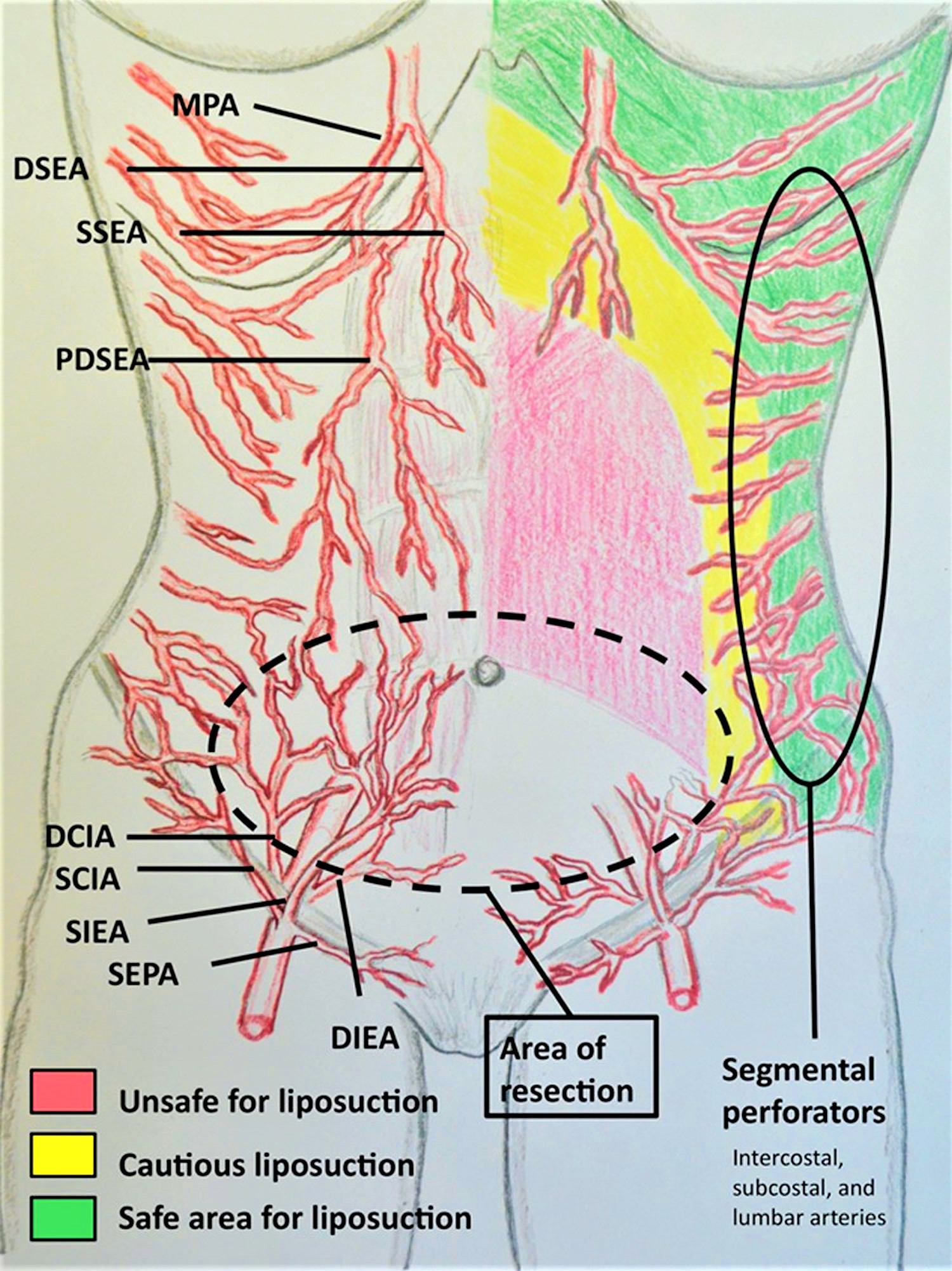
Figure 4. Abdominoplasty surgery with abdominal liposuction safe areas and unsafe areas
How long does the abdominoplasty surgery take?
Because an abdominoplasty is such a personalized procedure, the exact duration of your abdominoplasty surgery depends on the approach that your surgeon uses for you. In some patients whose needs are minimal, an abdominoplasty can take less than an hour. For others, the abdominoplasty procedure can last 4 hours or more. The best way to gain a better understanding of how long your particular abdominoplasty will last is to come in for a consultation with a board certified plastic surgeon so that she/he can assess your needs.
Abdominoplasty cost
The cost of an abdominoplasty will vary depending on your location and what cosmetic surgeon you see. If you are after good results and outcome from any surgery, then price shouldn’t be your deciding factor. Just because a doctor offers this procedure does not mean he is qualified or board certified in abdominoplasty surgery.
The average cost of an abdominoplasty is $5,992, according to 2017 statistics from the American Society of Plastic Surgeons.
The average fee referenced above does not include anesthesia, operating room facilities or other related expenses.
A surgeon’s fee will be based on his or her experience, the type of procedure used and the geographic office location.
Most health insurance does not cover an abdominoplasty surgery or its complications, but many plastic surgeons offer patient financing plans, so be sure to ask.
- Full Abdominoplasty with rectus muscle repair – from $9,995 all inclusive (approx.)
- Abdominoplasty with liposuction – from $14,995 all inclusive (approx.)
Will I have an obvious abdominoplasty scar?
As with all surgeries, the scarring from an abdominoplasty is permanent. However, your board certified plastic surgeon will take special care to place the scar below your bikini line, meaning your scar shouldn’t be visible even if you’re only wearing a bathing suit. Typically, a full abdominoplasty scar will stretch from one hip to the other, although a mini abdominoplasty scar will be slightly shorter. The abdominoplasty scar will fade with time.
Male patients tend to present less pleasing scars than women following abdominoplasty 6. The inguinal skin in men is thinner and more pigmented than the rest of the skin in the abdominal region. Differences in skin color between both sides of the scar, along with a disparity in skin thickness, result in a suboptimal aesthetic outcome.
Even with these precautions, the reported incidence of keloid and hypertrophic scars ranges between 1% and 3.7% 6. In these cases, compression with silicone strips has proven to be useful 38, leaving intralesional treatments and scar revision as second- and third-line treatments.
The term “dog ear” is frequently used to describe the conic deformity produced by skin excess after a circular or asymmetrical wound is closed. This defect is always iatrogenic (caused by the surgeon) and in the case of a considerably sized dog ear, it is advisable to correct the defect during the operation, mainly because its postoperative improvement is often unpredictable 39. A simple alternative for correcting a dog ear is to extend the skin excision in the same direction. It is preferable to perform a 90° incision at the end of the initial incision and to resect the excess skin or to de-epithelialize the redundant skin, avoiding extending the wound 40.
How long will I have to wait before seeing my final results?
Your abdominoplasty results will be noticeable immediately after your abdominoplasty surgery, although you can expect swelling and bruising to obscure your final outcome. While post-operative swelling should decrease significantly over the first several weeks, your final results may not be apparent until 6 months after surgery.
What is liposuction?
Liposuction is a type of cosmetic surgery. Liposuction removes unwanted excess body fat by suction using special surgical equipment to improve body appearance and to smooth irregular body shapes. The procedure is sometimes called body contouring.
Liposuction may be useful for contouring under the chin, neck, cheeks, upper arms, breasts, abdomen, buttocks, hips, thighs, knees, calves, and ankle areas.
Liposuction is a surgical procedure with risks, and it may involve a painful recovery. Liposuction can have serious or rare fatal complications. So, you should carefully think about your decision to have this surgery.
Mini abdominoplasty
If your skin laxity is primarily focused in the lower abdomen, bellow the belly button, and any abdominal separation (diastasis recti) is minimal, you may be a good candidate for a mini abdominoplasty, which uses a less aggressive approach to address only the lower abdomen.
On the other hand, if you have skin laxity throughout your upper and lower abdomen or more pronounced abdominal separation (diastasis recti), a full abdominoplasty might be the best option for you.
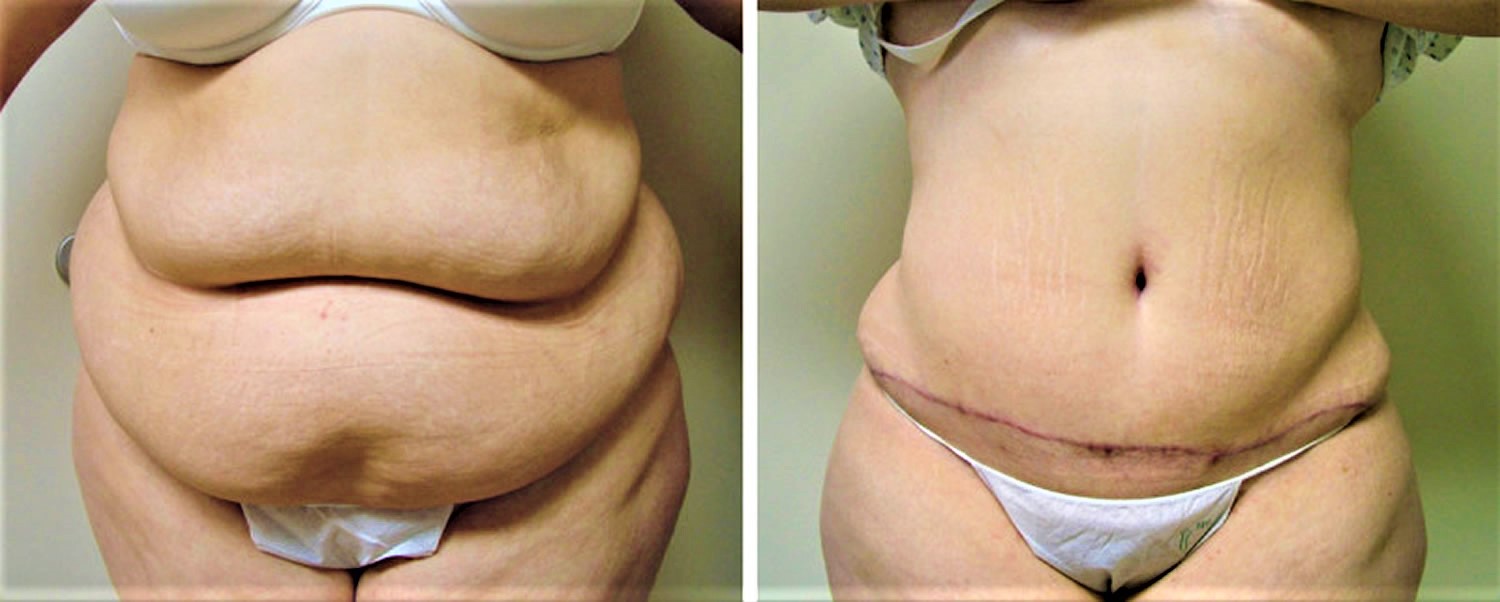
Abdominoplasty before and after
Figure 5. Abdominoplasty before and after

Footnotes: This patient presented with protuberant belly with an unsightly vertical Caesarean section scar. Her abdominal area was reconstructed with low-tension abdominoplasty with rectus muscle repair and natural umbilicoplasty.
Figure 6. Abdominoplasty before and after

Footnotes: This patient presented with significant abdominal skin laxity, as well as excess fat, and muscle diastasis resulting a protruding abdomen. She had restorative abdominoplasty with rectus muscle repair and umbilicoplasty in order to reconstruct her abdominal area. The patient is seen here with dramatic improvement of her body contour 8 months post-op.
Figure 7. Abdominoplasty before and after

Footnotes: A 45-year-old patient with a preoperative body mass index of 28, shown (left) before surgery and (right) 7 months after abdominoplasty combined with concurrent abdomen, flank, and mid-back liposuction.
Figure 8. Abdominoplasty before and after
Footnotes: A 29-year-old patient with a preoperative body mass index of 35, shown (left) before surgery and (right) approximately 4 weeks after abdominoplasty with concurrent abdomen, flank, and back liposuction. The purpose of showing this early result is to confirm that the changes present are attributable solely to the surgery and not to patient weight loss after surgery. Note that the incisions are still erythematous and the patient is still slightly swollen after surgery.
Abdominoplasty recovery
After a abdominoplasty, your abdominal incision and your bellybutton will likely be covered with surgical dressing. Small tubes might be placed along the incision site to drain any excess blood or fluid.
Your bed will be positioned to keep your upper body slightly raised and your knees at an angle for the first few days after surgery. Members of your health care team will also help you walk as early as the first day after a abdominoplasty to help prevent the formation of blood clots.
You will have some pain and discomfort for several days after abdominoplasty surgery. Your surgeon will prescribe pain medicine to help you manage your pain or you can manage discomfort with over-the-counter pain medications. It may help to rest with your legs and hips bent during recovery to reduce pressure on your abdomen. Resting with the legs and hips bent will put less stress on your belly.
Your surgeon may also give you a compression garment to wear, which can help speed up the abdominoplasty recovery process by promoting blood flow and reducing swelling. Wearing an elastic support similar to a girdle for 2 to 3 weeks will provide extra support while you heal.
Your scars will become flatter and lighter in color over the next year. DO NOT expose the area to sun, because it can worsen the scar and darken the color. Keep it covered when you are out in the sun.
Most people are happy with the results of abdominoplasty. Many feel a new sense of self-confidence.
Abdominoplasty recovery time
While everyone’s recovery experience is different and your recovery will vary depending on the type of abdominoplasty you get, you can expect to feel some soreness around the site of your incision accompanied by some degree of discomfort in the abdominal area.
After abdominoplasty surgery, there may be some pain and discomfort. This may last for several days.
You should take time away from work and other responsibilities to rest for at least 1 to 2 weeks. You should avoid strenuous activity and anything that makes you strain for 4 to 6 weeks. You will probably be able to return to work in 2 to 4 weeks.
Abdominoplasty results
By removing excess skin and fat and restoring your abdominal wall, a abdominoplasty can give your abdomen a more toned appearance.
Abdominoplasty results are usually long lasting. Keep in mind that maintaining a stable weight is crucial for retaining your results.
- International Society of Aesthetic Plastic Surgery . International study on aesthetic/cosmetic procedures performed in 2013. Hanover: International Society of Aesthetic Plastic Surgery; 2014.[↩]
- Kelly HA. Excision of the fat of the abdominal wall lipectomy. Surg Gynecol Obstet. 1910;10:229–31.[↩]
- Umbilical transplantation upward and abdominal contouring in lipectomy. VERNON S. Am J Surg. 1957 Sep; 94(3):490-2. https://www.ncbi.nlm.nih.gov/pubmed/13458618/[↩]
- Pitanguy I. Abdominal lipectomy: an approach to it through an analysis of 300 consecutive cases. Plast Reconstr Surg. 1967;40:384–91.[↩]
- Abdominoplasty. Grazer FM. Plast Reconstr Surg. 1973 Jun; 51(6):617-23. https://www.ncbi.nlm.nih.gov/pubmed/4705318/[↩]
- Vidal P, Berner JE, Will PA. Managing Complications in Abdominoplasty: A Literature Review. Archives of Plastic Surgery. 2017;44(5):457-468. doi:10.5999/aps.2017.44.5.457. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5621815/[↩][↩][↩][↩]
- Florida Board of Medicine. Emergency Rule 64b8er04-2: Moratorium on combined liposuction/abdominoplasty procedures in office surgery settings Florida Administrative Weekly. 2004;30:808.[↩]
- Samra S, Sawh-Martinez R, Barry O, Persing JA. Complication rates of lipoabdominoplasty versus traditional abdominoplasty in high-risk patients. Plast Reconstr Surg. 2010;125:683–690. https://www.ncbi.nlm.nih.gov/pubmed/20124853[↩]
- Brauman D, Capocci J. Liposuction abdominoplasty: An advanced body contouring technique. Plast Reconstr Surg. 2009;124:1685–1695. https://www.ncbi.nlm.nih.gov/pubmed/20009857[↩][↩]
- Avelar JM. Abdominoplasty without panniculus undermining and resection: Analysis and 3-year follow-up of 97 consecutive cases. Aesthet Surg J. 2002;22:16–25. https://www.ncbi.nlm.nih.gov/pubmed/19331948[↩]
- Neaman KC, Armstrong SD, Baca ME, et al. Outcomes of traditional cosmetic abdominoplasty in a community setting: a retrospective analysis of 1008 patients. Plast Reconstr Surg. 2013;131:403e–410e. https://www.ncbi.nlm.nih.gov/pubmed/23446591[↩]
- Najera RM, Asheld W, Sayeed SM, et al. Comparison of seroma formation following abdominoplasty with or without liposuction. Plast Reconstr Surg. 2011;127:417–22. https://www.ncbi.nlm.nih.gov/pubmed/21200239[↩]
- Hurvitz KA, Olaya WA, Nguyen A, et al. Evidence-based medicine: abdominoplasty. Plast Reconstr Surg. 2014;133:1214–21. https://www.ncbi.nlm.nih.gov/pubmed/24776552[↩]
- Throckmorton AD, Askegard-Giesmann J, Hoskin TL, et al. Sclerotherapy for the treatment of postmastectomy seroma. Am J Surg. 2008;196:541–4. https://www.ncbi.nlm.nih.gov/pubmed/18809059[↩]
- Nayak N, Narayan D. Buried dermal flap for the treatment of chronic postoperative seroma. BMJ Case Rep. 2010;2010:bcr0120102668 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3029351/[↩]
- Matarasso A, Swift RW, Rankin M. Abdominoplasty and abdominal contour surgery: a national plastic surgery survey. Plast Reconstr Surg. 2006;117:1797–808[↩]
- Rogliani M, Silvi E, Labardi L, et al. Obese and nonobese patients: complications of abdominoplasty. Ann Plast Surg. 2006;57:336–8 https://www.ncbi.nlm.nih.gov/pubmed/16929206[↩]
- Manassa EH, Hertl CH, Olbrisch RR. Wound healing problems in smokers and nonsmokers after 132 abdominoplasties. Plast Reconstr Surg. 2003;111:2082–7. https://www.ncbi.nlm.nih.gov/pubmed/12711974[↩]
- Hopf HW, Rollins MD. Wounds: an overview of the role of oxygen. Antioxid Redox Signal. 2007;9:1183–92.[↩]
- Matarasso A, Swift RW, Rankin M. Abdominoplasty and abdominal contour surgery: a national plastic surgery survey. Plast Reconstr Surg. 2006;117:1797–808.[↩][↩][↩]
- Manassa EH, Hertl CH, Olbrisch RR. Wound healing problems in smokers and nonsmokers after 132 abdominoplasties. Plast Reconstr Surg. 2003;111:2082–7.[↩]
- Samra S, Sawh-Martinez R, Barry O, et al. Complication rates of lipoabdominoplasty versus traditional abdominoplasty in high-risk patients. Plast Reconstr Surg. 2010;125:683–90. https://www.ncbi.nlm.nih.gov/pubmed/20124853[↩][↩]
- Hensel JM, Lehman JA, Jr, Tantri MP, et al. An outcomes analysis and satisfaction survey of 199 consecutive abdominoplasties. Ann Plast Surg. 2001;46:357–63. https://www.ncbi.nlm.nih.gov/pubmed/11324875[↩]
- David JS, Spann C, Marcotte G, et al. Haemorrhagic shock, therapeutic management. Ann Fr Anesth Reanim. 2013;32:497–503[↩]
- Rogliani M, Silvi E, Labardi L, et al. Obese and nonobese patients: complications of abdominoplasty. Ann Plast Surg. 2006;57:336–8.[↩]
- Neaman KC, Armstrong SD, Baca ME, et al. Outcomes of traditional cosmetic abdominoplasty in a community setting: a retrospective analysis of 1008 patients. Plast Reconstr Surg. 2013;131:403e–410e.[↩][↩]
- Rubin JP, Hunstad JP, Polynice A, et al. A multicenter randomized controlled trial comparing absorbable barbed sutures versus conventional absorbable sutures for dermal closure in open surgical procedures. Aesthet Surg J. 2014;34:272–83. https://www.ncbi.nlm.nih.gov/pubmed/24421408[↩]
- Ducic I, Zakaria HM, Felder JM 3rd, et al. Abdominoplasty-related nerve injuries: systematic review and treatment options. Aesthet Surg J. 2014;34:284–97. https://www.ncbi.nlm.nih.gov/pubmed/24436448[↩]
- Madura JA, Madura JA, 2nd, Copper CM, et al. Inguinal neurectomy for inguinal nerve entrapment: an experience with 100 patients. Am J Surg. 2005;189:283–7. https://www.ncbi.nlm.nih.gov/pubmed/15792751[↩]
- Dragu A, Bach AD, Polykandriotis E, et al. Pseudotumors after primary abdominal lipectomy as a new sequela in patients with abdominal apron. Obes Surg. 2009;19:1599–604[↩]
- Hatef DA, Kenkel JM, Nguyen MQ, et al. Thromboembolic risk assessment and the efficacy of enoxaparin prophylaxis in excisional body contouring surgery. Plast Reconstr Surg. 2008;122:269–79.[↩][↩]
- Shaikh N, Hanssens Y, Kettern MA, et al. Cerebral fat embolism as a rare complication of liposuction with abdominoplasty. Rev Neurol. 2008;47:277–8.[↩]
- Newall G, Ruiz-Razura A, Mentz HA, et al. A retrospective study on the use of a low-molecular-weight heparin for thromboembolism prophylaxis in large-volume liposuction and body contouring procedures. Aesthetic Plast Surg. 2006;30:86–95.[↩]
- Hatef DA, Trussler AP, Kenkel JM. Procedural risk for venous thromboembolism in abdominal contouring surgery: a systematic review of the literature. Plast Reconstr Surg. 2010;125:352–62.[↩]
- Somogyi RB, Ahmad J, Shih JG, et al. Venous thromboembolism in abdominoplasty: a comprehensive approach to lower procedural risk. Aesthet Surg J. 2012;32:322–9.[↩]
- Christman KD. Death following suction lipectomy and abdominoplasty. Plast Reconstr Surg. 1986;78:428.[↩]
- Teimourian B, Rogers WB., 3rd A national survey of complications associated with suction lipectomy: a comparative study. Plast Reconstr Surg. 1989;84:628–31[↩]
- O’Brien L, Jones DJ. Silicone gel sheeting for preventing and treating hypertrophic and keloid scars. Cochrane Database of Systematic Reviews 2013, Issue 9. Art. No.: CD003826. DOI: 10.1002/14651858.CD003826.pub3. http://cochranelibrary-wiley.com/doi/10.1002/14651858.CD003826.pub3/full[↩]
- Jaibaji M, Morton JD, Green AR. Dog ear: an overview of causes and treatment. Ann R Coll Surg Engl. 2001;83:136–8 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2503349/pdf/annrcse01630-0070.pdf[↩]
- Grassetti L, Lazzeri D, Torresetti M, et al. Aesthetic refinement of the dog ear correction: the 90 degrees incision technique and review of the literature. Arch Plast Surg. 2013;40:268–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665876/[↩]





{kind=link}