Contents
- Actinomycosis
- Actinomycosis causes
- Actinomycosis pathophysiology
- Actinomycosis prevention
- Actinomycosis signs and symptoms
- Orocervicofacial Actinomycosis
- Thoracic Actinomycosis
- Abdominal and Pelvic Actinomycosis
- Cutaneous actinomycosis
- Musculoskeletal actinomycosis
- Cerebral actinomycosis
- Disseminated actinomycosis
- Bisphosphonate-related osteonecrosis of the jaw
- Osteoradionecrosis
- Anti-tumor necrosis factor alpha drugs
- Hereditary hemorrhagic telangiectasia
- Chronic granulomatous disease
- Eye Infections
- Ear, Nose, and Throat Infections
- Dental caries
- Endodontic infections
- Oral infections in tissues surrounding teeth/implants.
- The upper body infections
- The lower body infections
- Genital tract infections
- Urinary tract infections
- Bone and Joint Infections
- Foreign-Body Infections
- Infective Endocarditis
- Bacteremia and Sepsis
- Actinomycosis complications
- Actinomycosis diagnosis
- Actinomycosis differential diagnosis
- Actinomycosis treatment
- Actinomycosis prognosis
Actinomycosis
Actinomycosis is a rare chronic bacterial infection typically caused by Gram-positive filamentous non-acid fast anaerobic Actinomyces bacteria most commonly or about 70% of infections are caused by Actinomyces israelii and Actinomyces gerencseriae bacteria, commonly found in the mouth on the gums, tonsils, and teeth, the intestines, and urogenital tract 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12. Actinomycosis infection causes pus-filled wounds, usually around your face and mouth, which slowly spread to nearby tissue. Actinomycosis often presents as multiple sulfur-containing abscesses (pus-filled areas) with draining sinus tracts (tunnels that can extend to the skin allowing drainage of pus) and may also involve other parts of the body. The most common locations affected are the face and neck (cervicofacial area), followed by the abdomen and pelvic region 1, 2, 13, 14. Sulfur granules, which are rounded or spherical and yellowish or whitish in color, and ≤ 1 mm in diameter do not contain sulfur, but are so named because of their yellow appearance. The sulfur-containing granules consist of a tangled mass of the branching filaments of Actinomyces bacteria.
Actinomyces bacteria are commensal bacteria that normally colonize the human mouth, urogenital tract, and gastrointestinal tract without harming human health 15, 16, 17, 18, 19, 20, 21, 22. Because Actinomyces bacteria are commensal bacteria that live naturally in your body without harming you, it is very difficult to determine normal flora colonization versus infection 23, 24, 25. However, surgery, injury, weakened immune system or disease can cause Actinomyces bacteria to grow in places they don’t belong. For example, Actinomyces lung infection may occur in patients with alcohol use disorder and seizure disorders (epilepsy) 1. Actinomyces lung infection usually occurs as a complication of aspiration when food, liquid, or other material enters a person’s airway and eventually the lungs by accident. Rarely actinomycosis can result from a human bite 1. Actinomyces infection in the face and neck areas typically occurs following oral cavity surgery in patients with poor oral hygiene 1. Pelvic actinomycosis has been associated with the use of intrauterine devices (IUDs) 1. Abdominal actinomycosis has been reported after any abdominal surgery but is most commonly seen after an appendectomy (a surgical procedure to remove the appendix) 1.
Actinomyces israelii (A. israelii) bacteria are the most common cause of actinomycosis 1. But many other types of Actinomyces bacteria can also cause it, including Actinomyces naeslundii, Actinomyces odontolyticus, Actinomyces viscosus, Actinomyces graevenitzii, Actinomyces gerencseriae, Actinomyces meyeri, Actinomyces neuii, Actinomyces turicensis, Actinomyces odontolyticus, Actinomyces viscosus and many others 26, 27, 28, 29, 30, 31.
Around 60% of Actinomyces infections are in the face and neck regions and described as “lumpy jaw syndrome” 1. The predisposing risk factors for face and neck Actinomyces infection include infection in erupting teeth, dental caries, gingivitis, and dental extraction, diabetes, alcohol use disorder, malnutrition, and cancer.
Actinomycosis most often occurs in adult males and takes several forms 32, 33, 34, 14:
- Face and Neck actinomycosis (cervicofacial with lumpy jaw syndrome): The most common portal of entry is periodontal disease with swelling, hard lumps sometimes called “lumpy jaw syndrome”and draining sores.
- Lungs and Chest actinomycosis: Pulmonary disease results from aspiration of oral secretions. Chest and lung symptoms may include cough, chest pain, difficulty breathing, potentially mimicking tuberculosis or cancer.
- Abdominal actinomycosis: Disease presumably results from a break in the mucosa of a diverticulum or the appendix or from trauma. Symptoms may include abdominal pain, fever, potentially mimicking other abdominal conditions.
- Uterine actinomycosis: This localized pelvic form is a complication of certain types of intrauterine device (IUD).
- Generalized actinomycosis: Rarely, the actinomyces infection spreads from primary infection sites, presumably by blood seeding to affect the skin, bones, and other areas.
The characteristic lesion of actinomycosis is a region of skin or tissue that feels firmer or thicker than the surrounding area with multiple, small, communicating abscesses surrounded by granulation tissue. Lesions tend to form sinus tracts that communicate to the skin and drain a purulent discharge containing “sulfur” granules. Infection spreads to contiguous tissues but only rarely carried by the blood.
Actinomycosis is usually caused by dental disease or surgery, but abdominal surgeries, aspiration and intrauterine device (IUDs) can also cause it.
Actinomyces infection diagnosis can be difficult as isolation of the organism requires prolonged bacterial culture under anaerobic conditions 1. Actinomyces infection is usually polymicrobial and very rarely spreads via bloodstream. The other organisms which are usually associated with Actinomyces infection are Aggregatibacter actinomycetemcomitans, Prevotella, Streptococcus, Enterobacteriaceae, Peptostreptococcus, and Staphylococcus 35, 36, 37. Actinomyces bacteria infects by inhibiting host defenses and/or reducing partial pressures of oxygen.
Actinomycosis is treated with long-term high doses antibiotic therapy typically penicillin or other beta-lactam antibiotics (e.g., cephalosporins, carbapenems, monobactams, beta-lactamase inhibitors) over several months 1, 38. Surgery may be necessary in some cases. The response to treatment can be monitored with imaging.
Antibiotics commonly used to treat actinomyces infection includes 1:
- Penicillin G
- Beta-lactams with a long course of oral amoxicillin
- Cephalosporin
If the patient is allergic to penicillin, alternatives include:
- Clindamycin
- Macrolides (erythromycin, clarithromycin or azithromycin)
- Doxycycline
A combination of metronidazole and a beta-lactamase inhibitor may be tried in polymicrobial infections 1.
Antimicrobial susceptibility testing is not indicated due to predictable antibiogram (a summary table showing the susceptibility of different microorganisms to various antimicrobials) 1.
The duration of therapy is usually 6 to 12 months but can be shortened if surgical resection of the infected site has been performed 1. Type of surgery will depend upon the site and extent of the disease, but it usually involves incision and drainage of abscesses, decompression of closed space, and excision of sinus tracts 1.
Cervicofacial actinomycosis has tendency to recur. Recurrent infections were seen mainly in patients who either had insufficient duration or incomplete treatment with antibiotics 35.
Figure 1. Actinomyces israelii
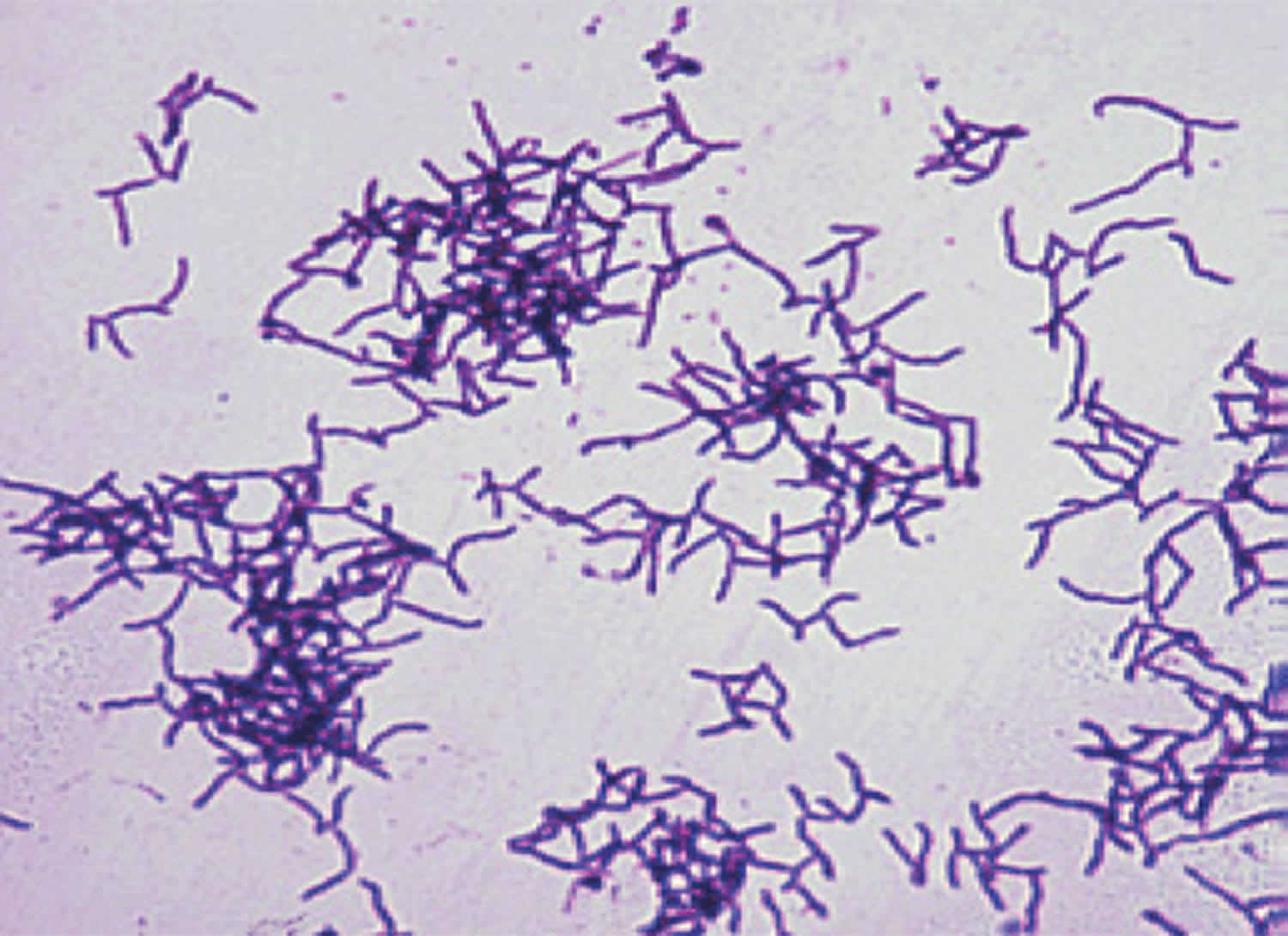
Footnote: Actinomyces israelii Gram stain from culture.
[Source 39 ]Figure 2. Human Actinomyces species natural habitats
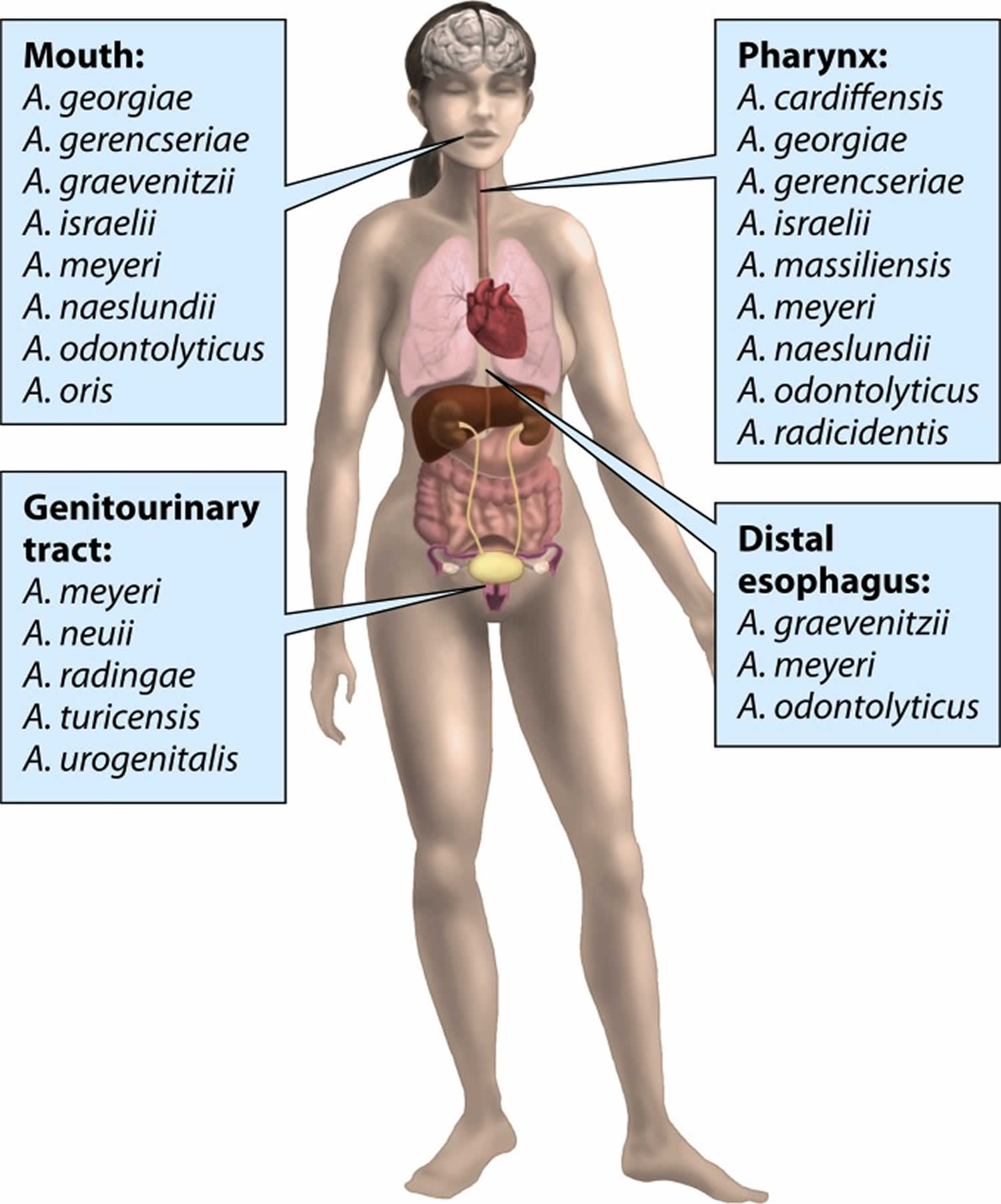
Figure 3. Actinomyces human infections
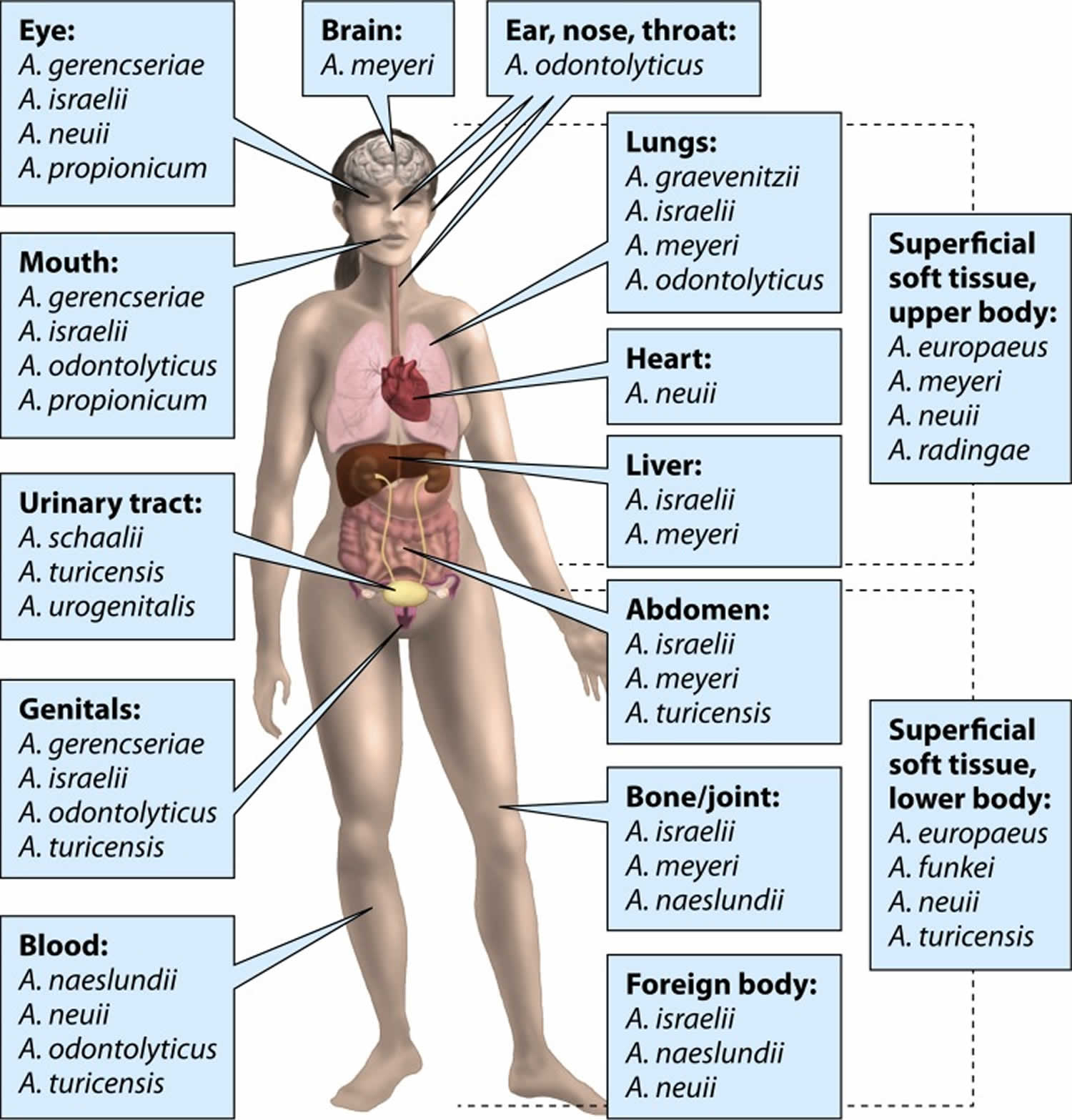
Figure 4. Actinomycosis of jaw (lumpy jaw syndrome)

Footnotes: 22-year-old Indian farmer from Jalgaon (India) presented with asymptomatic spongy red raised lesions on the right side of his chin since 3 months. It started as a single red raised lesion resembling an insect bite which gradually increased in size and firmness. On reaching the size of a one rupee coin, numerous solid and fluid filled small lesions started developing on the plaque in close proximity to each other. They would rupture spontaneously to release scanty, viscid, odorless, clear fluid, and occasionally blood. There was no discharge of grains or bony particles. There was no history of preceding congenital anomaly, trauma, dental infection, use of dentures, or plant twig for brushing teeth. One and half month later, he noticed similar lesions on the mucosal aspect of the chin corresponding to the external lesions discharging similar clear, odorless, and salty fluid. He was a chronic gutkha chewer since 7–8 years. Examination revealed an ill defined, nontender, indurated dusky red plaque measuring 4 × 5 cm² on the right side of the chin extending vertically from the angle of the mouth to the lower border of the mandible and horizontally from the mentum to 6 cm laterally. Overlying the indurated area were multiple spongy papulovesicles and sessile nodules of variable size, closely grouped giving a “frogspawn appearance” and on rupturing discharged clear, viscid, odorless fluid without granules, pus or bony particles. These lesions extended to the corresponding buccal mucosa as smaller white papules with difficulty to insinuate a finger between the mucosa and mandible. There were enlarged, nontender, matted cervical lymph nodes.
Skin biopsy revealed a hyperkeratotic and acanthotic epidermis with the deep dermis showing slender-beaded Gram-positive filaments crowded at the center and radiating parallely along the border suggestive of actinomycotic granule. They were surrounded by dense mixed inflammatory infiltrate and demonstrated the “Splendore Hoeppli” phenomenon. However, repeated cultures did not grow any organism. On the basis of histopathological demonstration of grain, a final diagnosis of cervicofacial actinomycosis was made, with the clinical presentation masquerading as lymphangioma circumscriptum. The patient was treated with injection crystalline penicillin 4 million units intravenously thrice daily for 6 weeks with tablet cotrimoxazole 960 mg twice daily. After 6 weeks, the intravenous route was to oral Penicillin G 400 mg twice daily with continuation of cotrimoxazole. There was significant reduction in the size of the entire plaque and individual lesions within the first month of therapy and complete clinical resolution by 4 months.
[Source 40 ]Figure 5. Cervicofacial actinomycosis

Footnotes: Cervicofacial actinomycosis. Seen from the left lateral perspective, this female patient displayed a fistula that had formed on the region of her left cheek, which had been brought on by an infection known as actinomycosis, or mycetoma, caused by the Gram-positive, fungus-like aerobic bacteria of the order Actinomycetales. Mycetoma is a slowly progressive, destructive infection of the cutaneous and subcutaneous tissues, fascia, and can progress to a point where it can affect bone as well.
[Source 1 ]Figure 6. Cervicofacial actinomycosis

Footnote: Cervicofacial actinomycosis. Drainage from a preaural lesion originating from sinus tract is shown.
[Source 14 ]Figure 7. Actinomycosis Foot Infection

Footnotes: Actinomycosis Foot Infection With Multiple Sinuses. A 42-year-old construction worker from Mexico was first seen in the wound center with a chief complaint of a left swollen foot slowly progressing over multiple years. He complains of multiple small wounds with purulent drainage on the plantar aspect of the left foot. The patient was in his usual state of health until approximately 3 years ago, when he noted some discoloration of the left plantar area. The swelling got progressively worse over approximately 2 years and had been unchanged during the past year. On examination, the patient was afebrile, and his systemic examination was negative. Local examination showed a massively swollen left foot from the metatarsal area to the toes. The skin was thick, hyperpigmented, and with a few dry fistulous tracts. The plantar area of foot had multiple small sinus lesions with some nodules, no foul odor, no areas of drainage, and no subcutaneous crepitus. Two fistulous tracts in the medial aspect of the heel were noted. There were no lymphatic streaks or palpable inguinal adenopathy. Peripheral pulses were present. A biopsy of the left foot was stained with hematoxylin and eosin showing epidermal and soft tissue abscess formation, with many of the abscesses containing purple filamentous sulfur granules. The biopsy also showed sinus tract formation throughout the soft tissue and hemosiderin deposition within the dermis. No fungal organisms were identified on the Gomori’s methenamine silver stain. Identification of the organism as Actinomyces israelii was made on the morphologic and biochemical characteristics. A culture of the biopsy with antibiotic sensitivity was found to be sensitive to penicillin.
[Source 13 ]How do you get actinomycosis?
Actinomyces bacteria are commensal bacteria that normally colonize the human mouth, urogenital tract, and gastrointestinal tract without harming human health. Because Actinomyces bacteria are commensal bacteria that live naturally in your body without harming you, it is very difficult to determine normal flora colonization versus infection 23, 24, 25. You get actinomycosis when Actinomyces bacteria get into parts of your body where they don’t belong. For instance, surgery, injury or certain diseases can cause a break in a mucous membrane that allows the bacteria to infect part of your body where they don’t normally live. Foreign objects in mucous membranes can also allow bacteria to grow.
The most common way to get actinomycosis is as a result of gum disease due to poor dental hygiene or dental procedures. Other causes include:
- Intrauterine devices (IUD).
- Getting food, liquids or a foreign object into your lungs (aspiration).
- Abdominal diseases like appendicitis, diverticulitis or peptic ulcer disease.
- Gallbladder removal (cholecystectomy), colectomy or another surgery in your abdominal cavity.
Is actinomycosis contagious?
No, actinomycosis isn’t contagious. You can’t get it from someone who’s infected.
Can actinomycosis be deadly?
Yes, actinomycosis can be deadly. While most people with actinomycosis recover with treatment, the infection can spread if left untreated or if you stop treatment too soon. Nasal infections are particularly dangerous because they can spread to your brain.
Actinomycosis causes
Actinomyces bacteria are commensal bacteria that normally colonize the human mouth, urogenital tract, and gastrointestinal tract without harming human health 15, 16, 17, 18, 19, 20, 21, 22. Because Actinomyces bacteria are commensal bacteria that live naturally in your body without harming you, it is very difficult to determine normal flora colonization versus infection 23, 24, 25. However, surgery, injury, weakened immune system or disease can cause Actinomyces bacteria to grow in places they don’t belong. For example, Actinomyces lung infection may occur in patients with alcohol use disorder and seizure disorders (epilepsy) 1. Actinomyces lung infection usually occurs as a complication of aspiration when food, liquid, or other material enters a person’s airway and eventually the lungs by accident. Rarely actinomycosis can result from a human bite 1. Actinomyces infection in the face and neck areas typically occurs following oral cavity surgery in patients with poor oral hygiene 1. Pelvic actinomycosis has been associated with the use of intrauterine devices (IUDs) 1. Abdominal actinomycosis has been reported after any abdominal surgery but is most commonly seen after an appendectomy (a surgical procedure to remove the appendix) 1.
Actinomyces israelii (A. israelii) bacteria are the most common cause of actinomycosis 1. But many other types of Actinomyces bacteria can also cause it, including Actinomyces naeslundii, Actinomyces odontolyticus, Actinomyces viscosus, Actinomyces graevenitzii, Actinomyces gerencseriae, Actinomyces meyeri, Actinomyces neuii, Actinomyces turicensis, Actinomyces odontolyticus, Actinomyces viscosus and many others 26, 27, 28, 29, 30, 31.
Around 60% of Actinomyces infections are in the face and neck regions and described as “lumpy jaw syndrome” 1. The predisposing risk factors for face and neck Actinomyces infection include infection in erupting teeth, dental caries, gingivitis, and dental extraction, diabetes, alcohol use disorder, malnutrition, and cancer.
Human immunodeficiency virus (HIV), solid organ transplantation of lungs or kidneys, biologic agents like infliximab (a medication that reduces inflammation by blocking the action of a protein called tumor necrosis factor alpha [TNF-α]) and acute lymphoblastic leukemia treated with chemotherapy are other risk factors 1.
Actinomyces lung infections are primarily due to the aspiration of oral and gastrointestinal secretions. Risk factors include people with alcohol use disorder and seizure disorders (epilepsy), as well as any chronic lung disease that lead to tissue destruction and break in normal mucosal defenses such as chronic obstructive pulmonary disease (COPD), bronchiectasis, tuberculosis (TB), silicosis, among others 1. Actinomyces lung infections can also be a direct or indirect extension from a face and neck infection. From the lungs, Actinomyces can easily spread to mediastinum (the central compartment of the chest cavity located between the two lungs) and pleura (a serous membrane that surrounds the lungs and lines the chest cavity). Bronchial and laryngeal infections are rare. Vocal cord infection may mimic cancer.
The second most frequent site for Actinomyces infection is the genitourinary tract. The primary risk factor is the use of the intrauterine device (IUD).
Abdominal actinomycosis is most common in the appendix, cecum, and colon. Abdominal surgery is the most significant risk factor.
Skin and soft tissue actinomycosis is rare but can occur secondary to skin injury.
Bloodstream dissemination is extremely rare.
Actinomycosis spreads slowly into nearby tissues, usually causing a long-lasting, tunneling wound or an opening underneath your skin called a sinus. The wound is filled with yellowish pus and “sulfur granules”. Sulfur granules are clumps made up of immune cells and parts of the Actinomyces bacteria. They don’t actually contain sulfur — the name comes from the yellow color.
Actinomycosis can sometimes take weeks or months to cause symptoms after the infection starts.
The incidence of Actinomycosis is greater in males age 20 to 60 years with a peak incidence in 40 to 50 years 1. The male to female ratio for incidence is 3:1 1. The use of intrauterine device (IUD) contraceptive devices in females has increased the incidence. Actinomyces infection has a higher prevalence within areas with low socioeconomic status. There is no racial tendency 41.
Risk factors for actinomycosis
Anything that can injure tissue in your mouth, digestive tract or uterus can increase your risk for actinomycosis. This includes:
- Diseases or conditions that damage your tissues.
- Poor dental hygiene.
- Implanted devices, surgeries or procedures. For IUDs, the risk increases the longer you’ve had the device in.
Doctors aren’t sure why, but men are at a higher risk for actinomycosis than women. You’re also at a higher risk if you have a weakened immune system, since you can’t fight off infections as easily.
Actinomycosis pathophysiology
Actinomyces bacteria are commensal bacteria that normally colonize the human mouth, urogenital tract, and gastrointestinal tract without harming human health 15, 16, 17, 18, 19, 20, 21, 22. Because Actinomyces bacteria are commensal bacteria that live naturally in your body without harming you, it is very difficult to determine normal flora colonization versus infection 23, 24, 25.
Actinomyces bacteria is not virulent and only invades the body to cause deeper infections when there is tissue injury and a subsequent break in the normal mucosal barrier. Actinomyces infection is mostly induced by the presence of multiple microorganisms, with as many as 5 to 10 other bacterial species present. Actinomyces infection is established with the help of a companion bacteria by inhibiting host defenses, reducing oxygen tension, or by producing a toxin that facilitates the inoculation of actinomycoses 42, 43, 44.
Once mucosal barriers are breached, and infection is established, the human host responds by initiating an intense inflammatory response which is suppurative and granulomatous 1. Actinomyces infection does not respect tissue planes and spreads contiguously. This results in draining sinus tracts, tiny yellow clumps called sulfur granules, and the result may be intense fibrosis of tissue.
Actinomycosis prevention
You can reduce your risk of cervicofacial actinomycosis (the most common type) by taking care of your dental health. This includes:
- Avoiding smoking and other tobacco products.
- Brushing your teeth at least twice a day with fluoride toothpaste.
- Flossing your teeth at least twice a day.
- Visiting your dentist regularly. Your dentist can spot any potential issues with your teeth and gums early.
Other forms of actinomycosis are hard to prevent, but they’re also uncommon.
Actinomycosis signs and symptoms
Actinomyces most commonly infect areas around your mouth and face sometimes called “lumpy jaw syndrome”. But you can get actinomycosis in other parts of your body, as well. Doctors refer to the type of actinomycosis by the part of your body that’s infected 32, 33, 34:
- Cervicofacial (face and neck) actinomycosis usually begins as a small, flat, hard swelling, with or without pain, under the oral mucosa or the skin of the neck or as a subperiosteal swelling of the jaw. Subsequently, areas of softening appear and develop into sinuses and fistulas that discharge the characteristic sulfur granules. The cheek, tongue, pharynx, salivary glands, cranial bones, meninges, or brain may be affected, usually by direct extension.
- Abdominal actinomycosis, the intestines usually the cecum and appendix and the peritoneum are infected. Pain, fever, vomiting, diarrhea or constipation, and emaciation are characteristic. One or more abdominal masses develop and cause signs of partial intestinal obstruction. Draining sinuses and intestinal fistulas may develop and extend to the external abdominal wall.
- Pelvic or uterine actinomycosis, affects your pelvic area and reproductive organs. Women who use an IUD have vaginal discharge and pelvic or lower abdominal pain.
- Thoracic or pulmonary actinomycosis, lung involvement resembles tuberculosis (TB). Extensive invasion may occur before chest pain, fever, and productive cough appear. Perforation of the chest wall, with chronic draining sinuses, may result.
- Generalized actinomycosis, infection spreads hematogenously to multiple areas, including the skin, vertebral bodies, brain, liver, kidneys, ureters, and, in women, pelvic organs. Diverse symptoms (eg, back pain, headache, abdominal pain) related to these sites may occur.
Some actinomycosis cases have been linked to specific conditions such as osteoradionecrosis or bisphosphonate-related osteonecrosis of the jaws 45, 46, the use of anti-inflammatory drugs 47, 48 or some hereditary diseases 49, 50. Also, unusual presentations of human actinomycosis have been reported, which presents a diagnostic challenge 51.
Symptoms of actinomycosis depend on where you’re infected. Actinomycosis signs and symptoms can include:
- Fever.
- Weight loss.
- Bumpy, fluid-filled areas on your neck, jaw or face or in your mouth (cervicofacial infection).
- Pain when you chew or severe jaw tightness (infection in your mouth or jaw).
- Chest pain (lung infection).
- Abdominal pain (pelvic or abdominal infection).
- Vaginal bleeding or discharge (pelvic infection).
Since Actinomyces grow slowly, symptoms might not develop for months or years after the surgery or illness that started the infection.
Characteristic features of actinomycosis include chronic signs and symptoms, abscess formation with sinus tracts, and purulent discharge 32.
Orocervicofacial Actinomycosis
Orocervicofacial actinomycosis also known as mouth, neck and face actinomycosis is the most common form of actinomycosis, consisting of more than half of all actinomycosis cases 32, 34, 33. According to Schaal and Lee in Germany over a period of 25 years 29, cervicofacial actinomycosis cases were common, making up ∼25% of the odontogenic infections examined in their laboratory. This may not be surprising, since the mouth, particularly dental plaque, is the primary habitat of Actinomyces species. Poor oral hygiene is seen as an important predisposing factor for actinomycosis, as are smoking and heavy use of alcohol, reflecting the poor health behavior of the host. Actinomyces can easily gain access to oral tissues via invasive dental procedures such as tooth extraction 34.
Other locations for actinomycotic lesions categorized as cervicofacial actinomycosis include the nasal and sinus region 52, 53, 54; pharynx 55, 56; larynx and tonsils 57, 58, 59, 60; middle ear, mastoid, and/or temporal bone 61, 62, 63; and skull base with the craniovertebral junction 64. A more distant location is the esophagus, from where actinomycotic lesions have also been recovered in both immunocompetent and immunocompromised individuals 65, 66.
The most comprehensive data on the bacteriology of orocervicofacial actinomycosis come from a study conducted in two reference laboratories in Germany 28. Altogether, 12,253 specimens, collected between 1972 and 1999 from patients having cervicofacial inflammatory processes, were examined thoroughly by using culture-based techniques with a wide variety of growth media and incubation times of up to 14 days. Of these, 1,997 specimens yielded growth of filamentous bacteria, consisting primarily of Actinomyces israelii (42%) and Actinomyces gerencseriae (26.7%) 28. In addition, Actinomyces naeslundii or Actinomyces viscosus was found in ∼9% of the specimens, while Actinomyces odontolyticus, Actinomyces meyeri, Actinomyces georgiae, and Actinomyces neuii subsp. neuii were occasionally recovered 28. Those authors suggested, however, that the latter Actinomyces findings could be due to these species being part of a polymicrobial infection rather than indicating their potential to cause true actinomycotic lesions, and the absence of real causative organisms may be explained by missing them in culture 28. Furthermore, 20% of Actinomyces isolates could not be identified to the species level, which is not surprising if the number of recently described novel species and the number of known unnamed species are considered. Noteworthy is that ∼90% of the 1,997 specimens also contained other bacterial species 28. In a reference laboratory in the United Kingdom, 88 clinical strains from unspecified infections of the neck-face area were identified; Actinomyces israelii, Actinomyces naeslundii, Actinomyces odontolyticus, and Actinomyces gerencseriae proved to be the main Actinomyces species, with each of them having a prevalence of ∼10% 67. Among the strain collection, several Actinomyces graevenitzii, Actinomyces meyeri, and Actinomyces turicensis as well as sporadic Actinomyces europaeus, Actinomyces georgiae, Actinomyces neuii, Actinomyces cardiffensis, and Actinomyces funkei strains were also identified 67, 68.
A recent report 69 reviewed 17 cases of pediatric cervicofacial actinomycosis, defined as a culture positive for Actinomyces or a biopsy specimen with “sulfur granules”. Of the 13 cases with a culture positive for Actinomyces, five isolates were identified as Actinomyces israelii, and three isolates each were identified as Actinomyces odontolyticus, “Actinomyces viscosus,” or Actinomyces bovis. It is not uncommon, however, that there are uncertainties in identifications in sporadic case reports. For instance, as nonhuman species, Actinomyces bovis and “Actinomyces viscosus” have probably been misidentified. Bacterial masses similar to those seen in actinomycosis, and from which Actinomyces israelii has been isolated, have also been recognized in pediatric osteomyelitis, and in the majority of cases, their location is the mandible 70.
Within the mouth, the hard palate is an uncommon site for actinomycosis, since only four cases have been described in the literature; in one of these cases, Actinomyces naeslundii was isolated from a diabetic patient 71. Another report described an ulcer-type actinomycotic lesion with Actinomyces odontolyticus on the oral mucosa of a patient with diabetes 72. Except for actinomycotic cases with Actinomyces meyeri in the middle ear and mastoid 61 and Actinomyces israelii in the mastoid 63 and in the skull base 64, identified by molecular methods, as well as Actinomyces odontolyticus in the larynx 60, diagnoses were not based on microbiology but on clinical manifestations and histopathology with or without a presentation of sulfur granules. In some cases, culture was performed, resulting in “no growth,” or the species identification was not defined. Therefore, which specific Actinomyces species could have been involved in these actinomycotic lesions remains unclear.
Thoracic Actinomycosis
The main source of thoracic actinomycosis is considered to be the aspiration of oropharyngeal secretions, although hematogenous spread or direct spread from local infections can result in actinomycotic lesions at pulmonary sites 33, 34. Alternative causes to be considered in differential diagnoses include lung cancer, pneumonia, and tuberculosis 73. Since the spread of an actinomycotic lesion occurs despite anatomic barriers, invasion into the pleura or the chest wall can result in empyema or actinomycosis in the chest wall and surrounding bone structures 33, 32.
Actinomyces graevenitzii appears to have a predilection for respiratory sites 74, 67. Actinomyces graevenitzii has been reported to be a causative organism in thoracic actinomycosis 48, 75, 76, multiple lung abscesses mimicking coccidioidomycosis 77 and organizing pneumonia with microabscesses 78. These observations are credible due to the possibility of aspiration, since Actinomyces graevenitzii colonizes the oral cavity 15. Actinomyces meyeri 79, 80, Actinomyces israelii 81, 82, Actinomyces odontolyticus 83, 84, and Actinomyces cardiffensis 85 have been recovered from actinomycotic lesions at pulmonary sites. Actinomyces cardiffensis has also been isolated from the blood of a patient with multiple lung abscesses and septicemia 86. Sporadic findings of Actinomyces naeslundii and “Actinomyces viscosus” from pediatric actinomycosis cases have been reported (95). Interestingly, a variety of typical oral species were present as concomitant bacteria in most specimens. Rarely, a progressing thoracic lesion extends to extrathoracic tissues, with abscess formation on the thoracic wall and pus eroding through the chest wall, causing “empyema necessitatis”. This is a severe condition, where Actinomyces odontolyticus, Actinomyces israelii, Actinomyces gerencseriae, and unspecified Actinomyces species have been detected as causative organisms besides mycobacteria and staphylococci 87, 88, 89. There are reports of cases where thoracic actinomycosis was found together with tuberculosis 75. In most of these cases, actinomycosis was due to Actinomyces israelii, while in one case, Actinomyces graevenitzii was identified as the causative organism.
Other Actinomyces species isolated from thorax specimens, collected in routine clinical laboratories and identified in a reference laboratory, were mainly Actinomyces meyeri and Actinomyces odontolyticus, but one isolate each of Actinomyces turicensis, Actinomyces cardiffensis, and Actinomyces funkei were also detected 67. Since there was no further clinical or histopathological information, it is not possible to confirm their connection specifically to actinomycosis.
Abdominal and Pelvic Actinomycosis
Abdominal actinomycosis is mainly a consequence of invasive procedures or abdominal infection such as appendicitis 34. Laparoscopic cholecystectomy with a lost gallstone(s) has been reported to be a potential complication leading to actinomycosis; Actinomyces naeslundii and an unspecified Actinomyces species were detected in two cases of abdominal abscesses 90, while Actinomyces meyeri was found in a case of abdominal actinomycosis extending from the kidney up to the thorax 91 and in an actinomycotic subphrenic abscess 92. Actinomyces israelii and Actinomyces meyeri have been identified in pus specimens from periappendical abscesses 93. Actinomyces meyeri was also implicated in splenic abscesses in a young girl with autoimmune hepatitis 94. In some abdominal actinomycosis cases arising from an abdominal source or even from the mouth, Actinomyces can result in pericarditis or the involvement of the liver; several Actinomyces species, particularly Actinomyces israelii 95, 96, 97, 98 and Actinomyces meyeri 99, 100, 40, 101, but also Actinomyces funkei 102, Actinomyces odontolyticus 103, and Actinomyces turicensis 104, have been detected in liver abscesses. Actinomyces neuii has been detected in pericardial effusion samples of patients with chronic pericarditis 105. It is notable, however, that Actinomyces neuii is not considered to be involved in classical actinomycosis 106, 107.
Pelvic actinomycosis has usually been connected to Actinomyces present on an intrauterine contraceptive device (IUD) after its prolonged use 32, 34. In a study conducted in Singapore, cervical smears of 1,108 women with IUDs were screened for Actinomyces-like organisms by two cytologists 108. The prevalence of smears positive for target organisms was nearly 14%; however, no connection between positive smears and the duration of placement of the IUD was found, contrary to most reports 109. Moreover, nearly all women, despite the presence of Actinomyces-like organisms, were asymptomatic 108, 109. When considering the frequency of use of IUDs, the recovery of <100 actinomycotic specimens, most of those being tubo-ovarian abscesses, between 1926 and 1995 indicated that the risk of pelvic actinomycosis in relation to the use of IUDs is very low 110. Among 130 Actinomyces isolates from clinical material associated with IUDs sent to a reference laboratory for identification to the species level, one-third were identified as Actinomyces israelii, with its prevalence being double those of Actinomyces turicensis, Actinomyces naeslundii, Actinomyces odontolyticus, and Actinomyces gerencseriae, which were the next most common species 67. In an in vitro study, Actinomyces israelii grown in synthetic intrauterine medium was demonstrated to attach to and form spiderlike colonies and porous biofilm structures on copper plates, where the presence of sulfur was also confirmed 111. Actinomyces israelii has been found in IUD users with pelvic manifestations 112, 113. Furthermore, Actinomyces odontolyticus 114 and some of the more recently isolated Actinomyces species, including Actinomyces urogenitalis 115, 116, Actinomyces hongkongensis 117, 118, Actinomyces cardiffensis 68, and Actinomyces turicensis 119, 120, appear to play a role in IUD-associated pelvic actinomycosis. Certain gynecologic procedures may predispose an individual to complications with Actinomyces organisms; a case of bacteremia from a tubo-ovarian abscess caused by Actinomyces urogenitalis in a non-IUD user exposed to a transvaginal oocyte retrieval procedure was reported 116, while in IUD users, a similar procedure resulted in an infectious complication with Actinomyces israelii 112, and another gynecologic procedure, hysterectomy and salpingectomy, resulted in pelvic actinomycosis due to Actinomyces hongkongensis 117. The type strain of Actinomyces hongkongensis originates from a pus specimen from a pelvic actinomycosis case where ovarian tubes were described as being filled with pus 118.
The spread of causative organisms from pelvic sites to the abdominal region or vice versa can lead to abdominopelvic actinomycosis 33.
Cutaneous actinomycosis
Cutaneous actinomycosis is usually a secondary infectious process with an underlying focus at deeper tissues, or it appears as a result of hematogenous spread from actinomycotic lesion elsewhere in the body. Manifestations with a single or multiple draining sinuses can occur at various body sites, including the face, chest, midriff, hip, as well as upper and lower extremities. Primary cutaneous actinomycosis with multiple lesions has been described to be a first sign of a patient’s HIV infection 121. Actinomyces meyeri and “Actinomyces viscosus” have been reported to be causative organisms of cutaneous actinomycosis 122, 123, 101.
Musculoskeletal actinomycosis
Musculoskeletal actinomycotic disease has been associated mainly with Actinomyces israelii. Typically, the patients’ dentition and oral hygiene are poor, which are predisposing factors for the disease to occur. A recent report described an actinomycotic case with an involvement of the cervical spine, where Actinomyces meyeri was isolated from prevertebral pus samples and blood 124. Among 15 actinomycotic cases with an involvement of thoracic vertebral bone, however, Actinomyces israelii was detected in 9 of the cases, and Actinomyces meyeri was detected in 1 125. In one Actinomyces israelii case, no signs of osteomyelitis in the spinal column were observed; the organism was detected in cerebrospinal fluid, and the entire spinal cord was involved, leaving the patient with severe neurological symptoms 126. Furthermore, Actinomyces israelii has been isolated from actinomycotic tissue biopsy specimens taken from the spine, together with Fusobacterium nucleatum and Aggregatibacter actinomycetemcomitans 127; iliac bone 128; and bones of a hand with extensive deformities 129. The latter was a most unusual case, initiated during the invasion of Normandy Beach in 1944, due to the persistence of the lesion despite long-term therapeutic interventions.
Cerebral actinomycosis
Actinomycotic lesions in the central nervous system (brain and spinal cord) cause the most severe form of actinomycosis 33, 34. Actinomyces organisms usually gain access to the central nervous system (brain and spinal cord) either by hematogenous spread from remote sites or directly from local actinomycotic lesions of the head, and the disease usually appears as a single or multiple brain abscesses; among 70 cases of actinomycosis in the central nervous system (brain and spinal cord), two-thirds proved to be brain abscesses 130. Actinomyces species isolated from cerebrospinal fluid include Actinomyces israelii, from a patient with meningitis 93 and Actinomyces naeslundii (sensu stricto) 26. Clinicians should be aware of the possibility of actinomycosis in the central nervous system (brain and spinal cord), especially in patients with neurological symptoms who have a history of actinomycosis elsewhere in the body 131. Pediatric cerebral actinomycosis cases are very rare; Actinomyces israelii was detected in a 10-year-old boy with congenital heart disease 132 and “Actinomyces viscosus” together with Streptococcus constellatus were detected in an immunocompetent 7-year-old girl, who died due to subdural empyema 133. In the latter case, again, poor dental health was suspected to be a predisposing factor.
Disseminated actinomycosis
Disseminated actinomycosis exhibits multiorgan involvement 32 and usually also has a polymicrobial nature; Aggregatibacter (formerly Actinobacillus) actinomycetemcomitans is often among the coinfecting organisms 79, 134, 135. Actinomyces meyeri in particular has a tendency to be involved in disseminated infections 79, 134, 136. Despite the severity of disseminated Actinomyces infection, it can have clinically mild manifestations. For example, a patient with longstanding shoulder pain with gradual spread to the chest area was finally diagnosed with pericarditis and pneumonia, after many challenges. This infection was caused by Actinomyces and Actinobacillus (Aggregatibacter) actinomycetemcomitans, and 6 months later, the patient also developed a brain abscess 135. The patient’s poor dentition was seen as a predisposing factor.
Bisphosphonates are commonly used drugs in oncology. Bisphosphonate-related osteonecrosis of the jaws (BRONJ) is widely considered a specific disease entity where Actinomyces organisms may play an important role 137, 46. In three case series on bisphosphonate-related osteonecrosis of the jaws (BRONJ) including a total of 96 patients, the rate of detection of Actinomyces varied between 53% and 86% 46, 138, 139. As known for most actinomycosis cases, concomitant or coinfecting organisms are usually present; therefore, it is conceivable that multiple bacterial morphotypes, located on active sites of bone resorption, were seen in bisphosphonate-related osteonecrosis of the jaws (BRONJ) lesions examined by scanning electron microscopy 140.
Osteoradionecrosis
Another type of therapy used in oncology, namely, irradiation of the head and neck area, can lead to devitalization and necrosis of the jaw bone. Out of 50 patients examined, 12% were diagnosed as having an actinomycotic bone lesion 138. It is notable that, already in the early 1980s, Actinomyces israelii was suggested to be an associated organism on the basis of immunocytological findings 141, but this was ignored at that time. Later, the impact of Actinomyces as an infectious organism under irradiation of the head and neck area was reinforced when Actinomyces, identified as Actinomyces israelii, was found prominently colonizing necrotic bone in the majority of 31 patients with osteoradionecrosis 45. Furthermore, it was shown that patients with bone biopsy specimens positive for Actinomyces were more susceptible to treatment failures than those with Actinomyces-negative biopsy specimens 142. In a study using sequencing of the 16S rRNA gene, however, only one Actinomyces israelii-positive specimen from osteoradionecrotic bone was found among six specimens examined 143, whereas the use of a DNA-DNA checkerboard method with targeted probes revealed the presence of Actinomyces species in all 12 resected jaw bone specimens examined 144. Ten specimens consisting of deep medullar bone of the jaw were positive for Actinomyces israelii, six for were positive “Actinomyces viscosus” and five were positive for Actinomyces gerencseriae. These discrepancies in bacterial findings may be explained by different methodologies used in these studies.
Anti-tumor necrosis factor alpha drugs
Anti-tumor necrosis factor alpha (TNF-α) drugs, which are increasingly used in the treatment of inflammatory diseases such as rheumatoid arthritis and Crohn’s disease, have been linked to an increased susceptibility to bacterial infections. The most common infections resulting in hospitalization are pneumonia, skin/soft tissue infections, urinary tract infections, and bacteremia/sepsis 145. Sporadic actinomycosis cases have also been reported in this context, including thoracic actinomycosis due to Actinomyces graevenitzii 48, rapidly progressing pneumonia due to Actinomyces meyeri 146, as well as cutaneous actinomycosis, with one case due to Actinomyces neuii subsp. anitratus and another case due to coinfection with Actinomyces turicensis and Actinomyces urogenitalis 47.
Hereditary hemorrhagic telangiectasia
Hereditary hemorrhagic telangiectasia is a vascular dysplasia with multiple-organ involvement. Recently, a case of multiple brain abscesses caused by Actinomyces israelii in a patient with hereditary hemorrhagic telangiectasia was described, and a review of such cases was conducted 49. Individuals with hereditary hemorrhagic telangiectasia are especially predisposed to brain abscesses, which are found in 75% of these individuals. In the literature between 1953 and 2013, ∼10 actinomycosis cases in hereditary hemorrhagic telangiectasia patients are known, where Actinomyces israelii, Actinomyces meyeri, Actinomyces odontolyticus, and Actinomyces bovis were implicated 49, 147. Other bacteria were also present in half of the cases; for example, organisms isolated concomitantly with Actinomyces meyeri were Streptococcus intermedius, Fusobacterium nucleatum, Capnocytophaga spp., and Staphylococcus epidermidis 148 and in another case, organisms isolated concomitantly with Actinomyces odontolyticus included Haemophilus aphrophilus (now Aggregatibacter aphrophilus), peptostreptococci, and Bacteroides sp. 149. These findings suggest an oral source of these polymicrobial brain abscesses.
Chronic granulomatous disease
The rare hereditary condition chronic granulomatous disease, which affects the clearance of phagocytosed microorganisms, can lead to severe infections, especially in the lungs, skin, lymph nodes, gastrointestinal tract, and liver, caused by fungi (e.g., Aspergillus) or aerobic bacteria (e.g., Staphylococcus aureus) 150. Interestingly, Actinomyces was detected in two pulmonary specimens from a total of 684 infectious episodes in 284 patients. Indeed, it was recently reported that patients suffering from chronic granulomatous disease could be especially vulnerable to actinomycosis 50. This case series of 10 patients consisted mainly of abscess specimens collected from the upper part of the body (submandibular region, neck, liver, and lung). Typically, recurrent infections in these patients are connected to catalase-producing bacteria and fungi 151, but here mainly catalase-negative Actinomyces species, including Actinomyces naeslundii (n = 5), Actinomyces gerencseriae (n = 1), Actinomyces meyeri (n = 1), an unspecified Actinomyces sp. (n = 1), and two cases specified as “actinomycosis,” were suggested to be causative organisms of chronic granulomatous disease-related actinomycosis 50. However, whether the described cases represented typical actinomycosis or another type of Actinomyces-associated infection remained unclear.
Eye Infections
Actinomyces species have been isolated from cases of endophthalmitis, keratitis, and canaliculitis. Of these, the most common infection is postoperative endophthalmitis after an ocular procedure, where Actinomyces neuii 152, 153, 154, Actinomyces meyeri 155 and “Actinomyces viscosus” 156 have been detected, while in cases of endogenous endophthalmitis, which is far less common, Actinomyces neuii 157 and Actinomyces israelii 158 have been detected. Actinomyces israelii has also been isolated from cases of postoperative keratitis 159 and primary infections of the lacrimal duct, i.e., canaliculitis 160, 161, 162. In addition, Actinomyces meyeri and Actinomyces georgiae have been found in specimens from cases of canaliculitis 163, 160, while Actinomyces naeslundii was identified in a swab specimen taken from a cornea after trauma leading to keratitis 93. Of 59 eye secretions/tear fluid examined in a reference laboratory in Germany, 22% were positive for “Actinomyces viscosus,” 19% were positive for Actinomyces israelii, 14% were positive for Actinomyces naeslundii, and 10% were positive for Actinomyces gerencseriae and Actinomyces odontolyticus each; Actinomyces israelii and Actinomyces gerencseriae were isolated from canaliculitis cases, whereas “Actinomyces viscosus,” Actinomyces naeslundii, and Actinomyces odontolyticus were more common in cases of conjunctivitis 29. Among 15 clinical strains collected from eye infections (infection not specified) and sent to a reference laboratory in the United Kingdom for identification, Actinomyces gerencseriae, Actinomyces israelii, Actinomyces odontolyticus, Actinomyces naeslundii, and Actinomyces georgiae, in descending order, were detected 67.
Ear, Nose, and Throat Infections
Actinomyces has been detected at increased frequencies in the nasopharynx of children suffering from recurrent otitis media during their first 2 years of life 18. In nasopharyngeal aspirates collected during acute otitis media episodes, one-quarter were colonized by Actinomyces odontolyticus, but Actinomyces gerencseriae was also found 164. In a culture-based study of peritonsillar abscesses, Actinomyces odontolyticus was found in one-quarter of 124 pus aspirates collected from young adults 165. Actinomyces turicensis has been detected in chronic otitis media and mastoiditis cases 166, while one Actinomyces cardiffensis strain was found in pus collected from temporal, large, and small parietal and ear abscesses in a patient after mastoidectomy 68. Moreover, another Actinomyces cardiffensis strain was obtained from an antral washout specimen of a patient with sinusitis 68, and a novel Actinomyces nasicola strain was obtained from pus collected from the nasal antrum 167.
Dental caries
Actinomyces species are involved in infectious processes of the mouth, including a wide variety of diseases induced by polymicrobial living in biofilms. The role of Actinomyces in dental caries is well known; in this context, the most important species are Actinomyces gerencseriae and Actinomyces israelii 17, 168, 169. Actinomyces gerencseriae in particular is among the most active species in dental plaque of children suffering from severe early childhood caries, which is a chronic disease causing extensive destruction of the primary dentition 169. Elderly subjects with exposed root surfaces usually due to treated or untreated advanced periodontitis are susceptible to root caries, where certain Actinomyces species are considered important causative organisms, particularly Actinomyces israelii and Actinomyces gerencseriae, but Actinomyces naeslundii, Actinomyces odontolyticus, and Actinomyces georgiae have also been isolated 168. Both Actinomyces naeslundii genospecies 1 (Actinomyces naeslundii sensu stricto) and genospecies 2 (now Actinomyces oris) colonize active root caries lesions 170.
Endodontic infections
The primary cause of endodontic infection is dental caries, when untreated progresses into the pulp cavum and root canal, infecting the pulp and eventually causing necrosis of the pulpal tissue. Since the infectious process can be asymptomatic, if no root canal treatment is given, microorganisms may gain access to even periapical sites. Actinomyces species are rarely involved in early stages of endodontic infections but are typically found in persistent infections and extraradicular lesions 171, 172, 173, 174, 175. Rates of detection of Actinomyces in clinical endodontic samples varied from 9% among 53 specimens examined by DNA-DNA checkerboard analysis 176 to 56% among 129 specimens examined by PCR 175. There were also obvious differences in the species distribution: Actinomyces gerencseriae and Actinomyces israelii 176 on the one hand and “Actinomyces viscosus” and Actinomyces israelii 175 on the other hand were reported as major Actinomyces species in teeth with abscesses, whereas Actinomyces naeslundii was either absent 176 or present at low levels 175. In a culture-based study of refractory periapical infections, sulfur granules were found in 9 of 36 periapical lesions 174; five of the seven culture-positive granules grew Actinomyces, including Actinomyces israelii, “Actinomyces viscosus,” Actinomyces naeslundii, and Actinomyces meyeri. Also, Actinomyces radicidentis isolates have been recovered sporadically from endodontic specimens 172, 177. Most, if not all, endodontic infections are polymicrobial 175. Two novel Actinomyces species, Actinomyces oricola and Actinomyces dentalis, with one strain each, have been isolated from dental abscesses 178, 179.
Oral infections in tissues surrounding teeth/implants.
Actinomyces organisms, particularly Actinomyces naeslundii and Actinomyces oris, are common in dental plaque 26. Actinomyces naeslundii has been found in cases of dental plaque-induced gingivitis, although Actinomyces naeslundii and Actinomyces gerencseriae were also reported to be associated with periodontal health 180. Somewhat surprising was the detection of Actinomyces gerencseriae as one of the dominant species of the microbiota at the gingival margin in relation to a severe form of gingival disease, necrotizing ulcerative gingivitis 181. Typically, Gram-negative anaerobes, such as fusobacteria, Prevotella intermedia, and spirochetes, are considered the etiologic organisms of this acute and painful disease, which destroys soft tissues around affected teeth, especially interdental gingival papillae. Elevated levels of Actinomyces neuii in subgingival sites of women with gingivitis were reported in a study where the DNA-DNA checkerboard technique was used as a detection method 182. Otherwise, Actinomyces neuii is seldom detected in oral biofilms. The known cross-reactivity of the checkerboard method may explain this unusual finding. Furthermore, Actinomyces odontolyticus, Actinomyces israelii, Actinomyces naeslundii/“Actinomyces viscosus,” Actinomyces meyeri, and Actinomyces gerencseriae, in descending order, have been recovered from a case of pericoronitis of wisdom teeth 183, while Actinomyces odontolyticus, Actinomyces naeslundii, “Actinomyces viscosus,” Actinomyces israelii, Actinomyces georgiae, Actinomyces gerencseriae, and Actinomyces graevenitzii, in descending order, were recovered from 33 failed dental implant fixtures, which had been removed due to infection 184. When bone was harvested from jawbone(s) for augmentation procedures, which may occasionally be needed for successful implantation of dental implant fixtures, Actinomyces odontolyticus was found to be among the most frequent contaminants of bone debris 185.
The upper body infections
Many Actinomyces species have been identified in soft tissue abscesses of the body above the waistline. Breast tissue is a site commonly affected by actinomycosis, with Actinomyces neuii especially being identified as a causative organism 186, 187, 188. Also, Actinomyces europaeus 189, 190, Actinomyces radingae 191, Actinomyces meyeri 192 and Actinomyces turicensis 191, 193 have been recovered. In one breast abscess case, Actinomyces turicensis was isolated in pure culture 74. Nipple piercing was suggested to be a predisposing factor for Actinomyces infection of the breast in two patients, one due to Actinomyces radingae 191 and another due to Actinomyces turicensis together with a Gram-positive anaerobic coccus, Peptoniphilus harei 193. Other sites of the upper body with abscesses with an involvement of Actinomyces organisms include the face, neck, axilla, armpit, chest, and/or back, with Actinomyces europaeus, Actinomyces georgiae, Actinomyces meyeri, Actinomyces neuii (both subspecies), and Actinomyces radingae being the identified species 192. In addition, Actinomyces turicensis has been isolated from necrotic tissue associated with cervicofacial fasciitis 93, and Actinomyces neuii has been isolated from a mammary hematoma 194.
The lower body infections
The majority of skin-related infections caused by Actinomyces below the waistline are due to Actinomyces turicensis 195, 196. Abscesses are typically found in the groin, buttock, rectal area, and skin of the genitals. Other Actinomyces species commonly detected include Actinomyces europaeus, Actinomyces funkei, Actinomyces neuii (both subspecies), and Actinomyces radingae 196, 190. It has been suggested that lipid-rich areas are favorable for the growth of these Actinomyces species 166. Furthermore, Actinomyces europaeus, Actinomyces funkei, and Actinomyces turicensis have been isolated from decubitus ulcers 102, 190; Actinomyces neuii and Actinomyces radingae have been isolated from diabetic ulcers 163, 106; and Actinomyces europaeus, Actinomyces turicensis, and Actinomyces odontolyticus have been isolated from skin-related infections in lower extremities 190, 197. It was suggested that the latter species, isolated from an intravenous drug abuser, originated from the oral cavity due to licking of an injection needle 197. This is consistent with the results of a study comparing bacterial recoveries from soft tissue abscesses of intravenous drug abusers and nonusers 198. Oral-type bacteria, including Actinomyces odontolyticus, dominated in the majority of abscesses of drug abusers but not nonusers. In another case, Actinomyces odontolyticus together with Eikenella corrodens, both oral species, caused infection in a foot due to trauma by toothpick puncture 199. A coinfection by two Actinomyces species, Actinomyces europaeus and Actinomyces turicensis, resulting in subcutaneous fistulae in association with an irritative exoprosthesis of a leg was reported 200. Sporadic Actinomyces findings include Actinomyces neuii and Actinomyces europaeus in infected atheromas 190, 106 and an Actinomyces hominis strain in a wound specimen 201, but their location was not specified. A case with a large vulvar lesion was connected to Actinomyces israelii, present together with Propionibacterium acnes and Peptostreptococcus sp. 202. Recently, a polymicrobial case of Fournier’s gangrene affecting an immunocompetent elderly man was analyzed by using 16S rRNA gene sequencing, which revealed the presence of Actinomyces funkei together with Fusobacterium gonidiaformans and Clostridium hathewayi as etiologic organisms 203. Seven cases of Actinomyces funkei infection were also detected recently in Spain by using sequencing-based isolate identification. Positive specimens included specimens from three abscesses, three wounds, and one bronchial aspirate 203.
Genital tract infections
The most common infections due to Actinomyces species in the genital tract are associated with the use of an IUD. Among 130 isolates from IUD-related infections, Actinomyces israelii in particular as well as Actinomyces turicensis, the Actinomyces naeslundii-“Actinomyces viscosus” complex, Actinomyces odontolyticus, and Actinomyces gerencseriae were identified as the main species in a reference laboratory in the United Kingdom, but Actinomyces cardiffensis and Actinomyces funkei were also not uncommon 67, 68. According to data from a reference laboratory in Germany 29, Actinomyces israelii was the most frequently detected isolate from IUDs and cervical secretions. Also “Actinomyces viscosus” was frequently found, whereas Actinomyces gerencseriae, Actinomyces naeslundii, and Actinomyces odontolyticus were identified in only 5% of 82 specimens. In addition, Actinomyces urogenitalis and Actinomyces radingae have been isolated from IUDs and vaginal secretions 27, 204, 163. Actinomyces urogenitalis has also been detected in high numbers in vaginal samples from patients with bacterial vaginosis 204. Actinomyces turicensis can be detected in a variety of infections of the female genital tract, such as adnexitis, endometritis, cervicitis, vaginitis, and vulvitis 166. In pregnancy, Actinomyces neuii has been found in infected amniotic fluid 106 and in severe cases of chorioamnionitis, leading to sepsis of the neonate 205. Actinomyces meyeri has been found to cause chorioamnionitis, leading to necrotizing funisitis and preterm birth 206. In infections of the genital tract in males, Actinomyces neuii has been detected in prostatitis cases 106, and Actinomyces turicensis has been detected in balanitis, penile abscess, and prostatitis cases 163, 166.
Urinary tract infections
In both males and females, Actinomyces turicensis has been detected in connection with urethritis and cystitis 166, 74. Other Actinomyces organisms found in the urinary tract include Actinomyces urogenitalis from urethra and urine 204, Actinomyces neuii in urinary tract infection 106, and Actinomyces europaeus in patients with cystitis or purulent urethritis 166. There are often other bacteria present, and only slightly elevated levels of leukocytes are observed in urine 166.
Bone and Joint Infections
Actinomyces species have been recovered from infections affecting bone, including osteomyelitis with an involvement of Actinomyces meyeri in the jaw, symphysis pubis, leg (tibia), and foot 101; Actinomyces israelii in osteomyelitis of the sternum 207; Actinomyces naeslundii in chronic osteomyelitis with thickening of the periosteum in the lower leg 208; and Actinomyces graevenitzii in an osteitis lesion of the jaw 209. There are also reports where two causative organisms of chronic osteomyelitis have been described, including Actinomyces meyeri together with Fusobacterium nucleatum in the leg (fibula) 210 and Actinomyces neuii subsp. neuii together with Dermabacter hominis in the calcaneus 211. Spondylodiscitis can rarely be due to Actinomyces organisms, such as Actinomyces meyeri 101 and Actinomyces israelii 212. A strain representing the novel Actinomyces species Actinomyces timonensis was isolated from an osteoarticular specimen of a 13-year-old girl suffering from chronic sacroiliitis 213.
Foreign-Body Infections
Different types of devices and materials are increasingly used in modern medicine to support defective or lost functions of the human body. According to recent reports, Actinomyces neuii, especially Actinomyces neuii subsp. neuii, seems to be the most frequently detected Actinomyces species in infected tissues around different types of prostheses, including mammary prostheses 214, penile prostheses 215, prosthetic valves 216, and hip prostheses 217, but also in connection to medical devices such as ventriculoperitoneal shunts 218, 219 and peritoneal dialysis catheters 220. In addition, Actinomyces israelii and Actinomyces naeslundii have been identified as causative agents of periprosthetic infections of the hip or knee joints 221, 222, 223. Moreover, Actinomyces odontolyticus was isolated from a subcutaneous abscess connected to an exit site of a catheter in a patient treated with continuous ambulatory peritoneal dialysis 224. Recently, Actinomyces meyeri was found to be the cause of a disseminated infection resulting in fatal mediastinitis after an esophageal stent operation 225.
Infective Endocarditis
Although Actinomyces species are rarely considered causative organisms in cases of endocarditis, isolation of Actinomyces neuii 216, 226, 107, Actinomyces funkei 227, Actinomyces israelii 228, 229, “Actinomyces viscosus” 229, 230, 231, and Actinomyces meyeri 232 has been reported. One reason for the rarity of reports of Actinomyces in blood specimens could be due to considering the finding to be insignificant or, if an organism is isolated, to the difficulty of identification of members of this group. Methodological improvements in identification and the availability of these methods in clinical microbiology laboratories, e.g., matrix-assisted laser desorption ionization–time of flight (MALDI-TOF) mass spectrometry and 16S rRNA gene sequencing, may allow more definitive data to be collected.
Bacteremia and Sepsis
Several Actinomyces species have been detected in blood, including Actinomyces funkei 233, Actinomyces georgiae 163, Actinomyces graevenitzii 234, Actinomyces massiliensis 235, Actinomyces naeslundii 236, Actinomyces neuii 194, Actinomyces odontolyticus 93, Actinomyces turicensis 163, and “Actinomyces viscosus” 93. An important source of Actinomyces bacteremias is the mouth in particular. Since bacteremia is common after invasive dental procedures and after tooth brushing in subjects with gingivitis and periodontitis, who typically have inflamed bleeding gums, oral actinobacteria can easily gain access to the bloodstream; Actinomyces georgiae, Actinomyces meyeri, Actinomyces odontolyticus, Actinomyces cardiffensis, and a number of unnamed Actinomyces phylotypes were detected in blood samples particularly following the extraction of a tooth without antibiotic prophylaxis 237.
Actinomycosis complications
If you don’t treat Actinomyces infection or don’t complete your course of antibiotics, Actinomyces infection can spread and cause:
- Tissue death (necrosis).
- Bone infection (osteomyelitis) and destruction.
- Brain abscess.
- Organ failure.
Actinomycosis diagnosis
Early diagnosis of slowly progressing actinomycosis is difficult due to the nonspecific nature of the signs and symptoms of the disease, such as swelling, cough, low-grade fever, and weight loss, which leads to delays in patients seeking medical care.
Actinomycosis is suspected clinically based on your symptoms and confirmed by identification of Actinomyces israelii (A. israelii) or other Actinomyces species (e.g., Actinomyces naeslundii, Actinomyces odontolyticus, Actinomyces viscosus, Actinomyces gerencseriae and others) using microscopy and culture of sputum (ideally obtained endoscopically), pus, or a biopsy specimen. A pathologist uses a microscope to look for Actinomyces or the granules it causes in the sample.
Imaging tests (eg, chest x-ray, abdominal or thoracic CT) are often done depending on findings.
Hard macroscopic grains called “sulfur granules” in pus have been considered among the confirmatory characteristics of actinomycotic lesions; however, they are not always present in pus samples 28, 33. When available, “sulfur granules” are of diagnostic value; in a histopathological examination, the granules are crushed, Gram stained, and viewed under a microscope, revealing typical Gram-positive branching filaments forming segment-like structures and being surrounded by inflammatory cells, mainly polymorphonuclear neutrophils 32, 30. In pus or tissue, Actinomyces bacteria appear as the distinctive sulfur granules or as tangled masses of branched and unbranched wavy bacterial filaments, pus cells, and debris, surrounded by an outer zone of radiating, club-shaped, hyaline, and refractive filaments that take Hematoxylin-Eosin stain in tissue but are positive on Gram stain. The laboratory must be notified that actinomycosis is suspected because special procedures are required to isolate and identify these organisms.
Lesions in any location may simulate malignant growths. Lung lesions must be distinguished from those of tuberculosis (TB) and cancer. Most abdominal lesions occur in the ileocecal region and are difficult to diagnose, except during laparotomy or when draining sinuses appear in the abdominal wall.
Actinomycosis differential diagnosis
Actinomycosis differential diagnosis will depend upon the site of infection. Actinomyces is a slow-spreading infection that can mimic benign or malignant tumors, nocardiosis, and tuberculosis (TB).
The other important differential diagnosis to consider are the following:
- Aspiration pneumonia
- Appendicitis
- Diverticulosis
- Crohn’s disease
- Lung abscess
- Fungal pneumonia
- Pelvic inflammatory disease
- Brain abscess
- Dental abscess
Actinomycosis treatment
Doctors treat actinomycosis with high doses of antibiotics. A doctor usually gives you antibiotics through an IV in your arm for a few days or weeks, then you continue to take an antibiotic in pill form at home. Your doctor may also need to drain infected areas and remove dead tissue from them (debridement).
Antibiotics that treat actinomycosis may include:
- Penicillin.
- Amoxicillin.
- Erythromycin.
- Tetracycline.
- Doxycycline.
- Minocycline.
- Clindamycin.
You may need to take antibiotics for months or even a year for actinomycosis to completely go away. If you stop antibiotics too soon, the infection can come back or start spreading again.
Most patients with actinomycosis respond to antibiotics, but response is usually slow because of extensive tissue induration and the relatively avascular nature of the lesions. Therefore, treatment must be continued for at least 8 weeks and occasionally for ≥ 1 year, until symptoms and signs have resolved but can be shortened if surgical resection of the infected site has been performed 14, 1. Type of surgery will depend upon the site and extent of the disease, but it usually involves incision and drainage of abscesses, decompression of closed space, and excision of sinus tracts.
High doses of penicillin G (eg, 3 to 5 million units IV every 6 hours) are usually effective 14. Penicillin V 1 g orally 4 times a day may be substituted after about 2 to 6 weeks. Oral tetracycline 500 mg every 6 hours or doxycycline 100 mg every 12 hours may be given instead of penicillin 14. Minocycline, clindamycin, and erythromycin have also been successful. Antibiotic regimens may be broadened to cover other pathogens cultured from lesions 14.
Treatment of IUD-associated pelvic actinomycosis also involves removal of the IUD. Extensive pelvic disease may require drainage of intra-abdominal abscesses, sometimes with hysterectomy (surgical procedure where the uterus or womb is removed) and salpingo-oophorectomy (surgical removal of the fallopian tubes and ovaries) 14.
Anecdotal reports suggest that hyperbaric oxygen therapy might be helpful 14.
Extensive and repeated surgical procedures may be required. Sometimes small abscesses can be aspirated; large ones are drained, and fistulas are excised surgically.
Actinomycosis prognosis
If you have actinomycosis, you can expect to be on antibiotics for a long period of time from several months or longer to completely get rid of the infection. You’ll need regular follow-ups with your doctor to make sure the antibiotic is working. You’ll also need to pay close attention to your symptoms and let your doctor know right away if they’re getting worse. Huang et al. 238 reported actinomycotic brain abscess which developed 15 months after 6 weeks of successful treatment of nasopharyngeal actinomycosis. Long-term surveillance, therefore, is still necessary for patients suffered with actinomycosis in any particular area in cervicofacial region.
Prolonged antibiotic therapy is usually required, and the outlook (prognosis) for actinomycosis is usually good. You have the best chance of a full recovery if:
- You have the cervicofacial actinomycosis.
- Your actinomyces infection is treated early.
- You continue taking the entire course of antibiotics as directed by your doctor.
- You don’t have underlying immune system issues.
With better oral hygiene, availability of antibiotics, and advanced surgical techniques, Actinomycosis outcome, and mortality have improved. For extensive and complicated Actinomyces disease such as the thoracic, abdominal, and generalized actinomycosis, antibiotics and surgical treatment are required. In these cases, morbidity is high, and death may occur, especially if the central nervous system (brain and spinal cord) is involved 3 , 14, 1.
- Sharma S, Hashmi MF, Valentino III DJ. Actinomycosis. [Updated 2023 Aug 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482151[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Boot M, Archer J, Ali I. The diagnosis and management of pulmonary actinomycosis. J Infect Public Health. 2023 Apr;16(4):490-500. doi: 10.1016/j.jiph.2023.02.004[↩][↩]
- Meena DS, Kumar D, Sharma M, Malik M, Ravindra A, Santhanam N, Bohra GK, Garg MK. The epidemiology, clinical presentation and treatment outcomes in CNS actinomycosis: a systematic review of reported cases. Orphanet J Rare Dis. 2023 Jun 2;18(1):133. doi: 10.1186/s13023-023-02744-z[↩][↩]
- Wong VK, Turmezei TD, Weston VC. 2011. Actinomycosis. BMJ 343:d6099. doi: 10.1136/bmj.d6099[↩]
- Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015;28:419–442. doi: 10.1128/CMR.00100-14[↩]
- García-García A, Ramírez-Durán N, Sandoval-Trujillo H, Romero-Figueroa MDS. Pelvic Actinomycosis. Can J Infect Dis Med Microbiol. 2017;2017:9428650. doi: 10.1155/2017/9428650[↩]
- Steininger C, Willinger B. Resistance patterns in clinical isolates of pathogenic Actinomyces species. J Antimicrob Chemother. 2016 Feb;71(2):422-7. doi: 10.1093/jac/dkv347[↩]
- Egal A, Etienney I, Beate H, Fléjou JF, Cuenod CA, Atienza P, Bauer P. Diagnosis and Management of a Cryptoglandular Actinomycotic Fistula-in-Ano: An Update on 7 New Cases and a Review of the Literature. Ann Coloproctol. 2018 Jun;34(3):152-156. doi: 10.3393/ac.2017.07.23[↩]
- Demirhan S, Orner E, Szymczak W, Lee PJ, Aldrich M. Skin and Soft Tissue Actinomycosis in Children and Adolescents. Pediatr Infect Dis J. 2024 Aug 1;43(8):743-747. doi: 10.1097/INF.0000000000004345[↩]
- Bhat A, J M, Mascarenhas D. Bronchiectatic Actinomycosis with Osseous Metaplasia Masquerading as Lung Cancer. Turk Patoloji Derg. 2024;40(3):205. doi: 10.5146/tjpath.2024.13407err. Erratum for: doi: 10.5146/tjpath.2024.13407[↩]
- Hadgaonkar S, Rathi P, Vincent V, Shyam A, Sancheti P. Actinomycotic Infection of Spine – A Rare Disease with Diagnostic Challenge, an Update on Spinal Infection. J Orthop Case Rep. 2021;11(1):72-78. doi: 10.13107/jocr.2021.v11.i01.1970[↩]
- Wallace RJ Jr, Musher DM. Actinomycosis: an update. Int J Dermatol. 1977 Apr;16(3):185-7. https://doi.org/10.1111/j.1365-4362.1977.tb01849.x[↩]
- Bettesworth J, Gill K, Shah J. Primary actinomycosis of the foot: a case report and literature review. J Am Col Certif Wound Spec. 2009 Jul 3;1(3):95-100. doi: 10.1016/j.jcws.2009.06.004[↩][↩]
- Actinomycosis. https://www.msdmanuals.com/professional/infectious-diseases/anaerobic-bacteria/actinomycosis[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Sarkonen N, Könönen E, Summanen P, Kanervo A, Takala A, Jousimies-Somer H. 2000. Oral colonization with Actinomyces species in infants by two years of age. J Dent Res 79:864–867. doi: 10.1177/00220345000790031301[↩][↩][↩][↩]
- Zijnge V, van Leeuwen MBM, Degener JE, Abbas F, Thurnheer T, Gmür R, Harmsen HJM. 2010. Oral biofilm architecture on natural teeth. PLoS One 5:e9321. doi: 10.1371/journal.pone.0009321[↩][↩][↩]
- Tang G, Yip HK, Samaranayake LP, Luo G, Lo ECM, Teo CS. 2003. Actinomyces spp. in supragingival plaque of ethnic Chinese preschool children with and without active dental caries. Caries Res 37:381–390. doi: 10.1159/000072172[↩][↩][↩][↩]
- Könönen E, Syrjänen R, Takala A, Jousimies-Somer H. 2003. Nasopharyngeal carriage of anaerobes during health and acute otitis media by two years of age. Diagn Microbiol Infect Dis 46:167–172. doi: 10.1016/S0732-8893(03)00049-X[↩][↩][↩][↩]
- Jensen A, Fagö-Olsen H, Sørensen CH, Kilian M. 2013. Molecular mapping to species level of the tonsillar crypt microbiota associated with health and recurrent tonsillitis. PLoS One 8:e56418. doi: 10.1371/journal.pone.0056418[↩][↩][↩]
- Cho I, Blaser MJ. 2012. The human microbiome: at the interface of health and disease. Nat Rev Genet 13:260–270. doi: 10.1038/nrg3182[↩][↩][↩]
- Ou G, Hedberg M, Hörstedt P, Baranov V, Forsberg G, Drobni M, Sandström O, Wai SN, Johansson I, Hammarström M-L, Hernell O, Hammarström S. 2009. Proximal small intestinal microbiota and identification of rod-shaped bacteria associated with childhood celiac disease. Am J Gastroenterol 104:3058–3067. doi: 10.1038/ajg.2009.524[↩][↩][↩]
- Stearns JC, Lynch MDJ, Senadheera DB, Tenenbaum HC, Goldberg MB, Cvitkovitch DG, Croitoru K, Moreno-Hagelsieb G, Neufeld JD. 2011. Bacterial biogeography of the human digestive tract. Sci Rep 1:170. doi: 10.1038/srep00170[↩][↩][↩]
- McCann A, Alvi SA, Newman J, Kakarala K, Staecker H, Chiu A, Villwock JA. Atypical Form of Cervicofacial Actinomycosis Involving the Skull Base and Temporal Bone. Ann Otol Rhinol Laryngol. 2019 Feb;128(2):152-156. doi: 10.1177/0003489418808541[↩][↩][↩][↩]
- Valdés-Peregrina EN, Bonifaz A, Arteaga-Sarmiento JF, Hernández-González M. Actinomicosis primaria intestinal. Informe de un caso en íleon y colon. Revisión de la literatura [Primary intestinal actinomycosis in ilium and colon. A case report and review of the literature]. Rev Esp Patol. 2018 Oct-Dec;51(4):253-256. Spanish. doi: 10.1016/j.patol.2017.10.005[↩][↩][↩][↩]
- Sadeghi S, Azaïs M, Ghannoum J. Actinomycosis Presenting as Macroglossia: Case Report and Review of Literature. Head Neck Pathol. 2019 Sep;13(3):327-330. doi: 10.1007/s12105-018-0966-7[↩][↩][↩][↩]
- Henssge U, Do T, Radford DR, Gilbert SC, Clark D, Beighton D. 2009. Emended description of Actinomyces naeslundii and descriptions of Actinomyces oris sp. nov. and Actinomyces johnsonii sp. nov., previously identified as Actinomyces naeslundii genospecies 1, 2 and WVA 963. Int J Syst Evol Microbiol 59:509–516. doi: 10.1099/ijs.0.000950-0[↩][↩][↩][↩]
- Hall V. 2008. Actinomyces—gathering evidence of human colonization and infection. Anaerobe 14:1–7. doi: 10.1016/j.anaerobe.2007.12.001[↩][↩][↩]
- Pulverer G, Schutt-Gerowitt H, Schaal KP. 2003. Human cervicofacial actinomycoses: microbiological data for 1997 cases. Clin Infect Dis 37:490–497. doi: 10.1086/376621[↩][↩][↩][↩][↩][↩][↩][↩]
- Schaal KP, Lee HJ. 1992. Actinomycete infections in humans—a review. Gene 115:201–211. doi: 10.1016/0378-1119(92)90560-C[↩][↩][↩][↩][↩]
- Wade WG, Könönen E. 2011. Propionibacterium, Lactobacillus, Actinomyces, and other non-spore-forming anaerobic gram-positive rods, p 817–833. In Versalovic J, Carroll KC, Funke G, Jorgensen JH, Landry ML, Warnock DW (ed), Manual of clinical microbiology, 10th ed ASM Press, Washington, DC.[↩][↩][↩]
- Könönen E, Wade WG. Actinomyces and related organisms in human infections. Clin Microbiol Rev. 2015 Apr;28(2):419-42. doi: 10.1128/CMR.00100-14[↩][↩][↩][↩]
- Russo TA. 2009. Agents of actinomycosis, p 2864–2873. In Mandell GL, Bennett JE, Dolin R (ed), Principles and practice in infectious diseases, 7th ed Elsevier, Philadelphia, PA.[↩][↩][↩][↩][↩][↩][↩][↩]
- Smego RA Jr, Foglia G. Actinomycosis. Clin Infect Dis. 1998 Jun;26(6):1255-61; quiz 1262-3. doi: 10.1086/516337[↩][↩][↩][↩][↩][↩][↩][↩]
- Wong VK, Turmezei TD, Weston VC. Actinomycosis. BMJ. 2011 Oct 11;343:d6099. doi: 10.1136/bmj.d6099[↩][↩][↩][↩][↩][↩][↩][↩]
- Ahmed S, Ali M, Adegbite N, Vaidhyanath R, Avery C. Actinomycosis of tongue: Rare presentation mimicking malignancy with literature review and imaging features. Radiol Case Rep. 2018 Nov 8;14(2):190-194. doi: 10.1016/j.radcr.2018.10.022[↩][↩]
- Tippett E, Goyal N, Guy S, Wong J. Actinomyces spp. bloodstream and deep vein thrombus infections in people who inject drugs. Infection. 2019 Jun;47(3):479-482. doi: 10.1007/s15010-018-1246-x[↩]
- Mishra A, Prabhuraj AR, Bhat D, Nandeesh BN, Mhatre R. Intracranial Actinomycosis Manifesting as a Parenchymal Mass Lesion: A Case Report and Review of Literature. World Neurosurg. 2019 Feb;122:190-194. doi: 10.1016/j.wneu.2018.10.134[↩]
- Pandey N, Cascella M. Beta-Lactam Antibiotics. [Updated 2023 Jun 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545311[↩]
- Korsapati H, Babaei A, Bhargava V, Dohil R, Quin A, Mittal RK. Dysfunction of the longitudinal muscles of the oesophagus in eosinophilic oesophagitis. Gut. 2009 Aug;58(8):1056-62. doi: 10.1136/gut.2008.168146[↩]
- Kura MM, Rane VK. Cervicofacial actinomycosis mimicking lymphangioma circumscriptum. Indian J Dermatol. 2011 May;56(3):321-3. doi: 10.4103/0019-5154.82493[↩][↩]
- Rolfe R, Steed LL, Salgado C, Kilby JM. Actinomyces meyeri, a Common Agent of Actinomycosis. Am J Med Sci. 2016 Jul;352(1):53-62. doi: 10.1016/j.amjms.2016.03.003[↩]
- Gomes-Silva W, Pereira DL, Fregnani ER, Almeida OP, Armada L, Pires FR. Clinicopathological and ultrastructural characterization of periapical actinomycosis. Med Oral Patol Oral Cir Bucal. 2020 Jan 1;25(1):e131-e136. doi: 10.4317/medoral.23247[↩]
- Ge MJ, Fu YQ, Zhou H, Wang J, Zhou JY. [Clinical feature analysis of 30 cases with pulmonary actinomycosis]. Zhonghua Yi Xue Za Zhi. 2019 Dec 10;99(46):3617-3621. Chinese. doi: 10.3760/cma.j.issn.0376-2491.2019.46.005[↩]
- Palm A, Isaksson J, Brandén E, Hillerdal G. Torakal aktinomykos – allvarlig sjukdom och en diagnostisk svår utmaning – Men med rätt behandling är prognosen god [Thoracal actinomycosis – a diagnostic challenge]. Lakartidningen. 2019 Dec 3;116:FR6A. https://lakartidningen.se/klinik-och-vetenskap-1/artiklar-1/fallbeskrivning/2019/12/torakal-aktinomykos-allvarlig-sjukdom-och-en-diagnostisk-svar-utmaning/[↩]
- Hansen T, Kunkel M, Kirkpatrick CJ, Weber A. 2006. Actinomyces in infected osteoradionecrosis—underestimated? Hum Pathol 37:61–67. doi: 10.1016/j.humpath.2005.09.018[↩][↩]
- Schipmann S, Metzler P, Rössle M, Zemann W, von Jackowski J, Obwegeser JA, Grätz KW, Jacobsen C. 2013. Osteopathology associated with bone resorption inhibitors—which role does Actinomyces play? A presentation of 51 cases with systematic review of the literature. J Oral Pathol Med 42:587–593. doi: 10.1111/jop.12038[↩][↩][↩]
- Breton AL, Lamblin G, Pariset C, Jullien D. 2014. Cutaneous actinomycosis associated with anti-TNF-alpha therapy: report of two cases. Dermatology 228:112–114. doi: 10.1159/000357522[↩][↩]
- Cohen RD, Bowie WR, Enns R, Flint J, Fitzgerald JM. 2007. Pulmonary actinomycosis complicating infliximab therapy for Crohn’s disease. Thorax 62:1013–1014. doi: 10.1136/thx.2006.075150[↩][↩][↩]
- Koubaa M, Lahiani D, Mâaloul I, Fourati H, Chaari L, Marrakchi C, Mnif Z, Boudawara Z, Ben Jemâa M. 2013. Actinomycotic brain abscess as the first clinical manifestation of hereditary hemorrhagic telangiectasia—case report and review of the literature. Ann Hematol 92:1141–1143. doi: 10.1007/s00277-012-1666-0[↩][↩][↩]
- Reichenbach J, Lopatin U, Mahlaoui N, Beovic B, Siler U, Zbinden R, Seger RA, Galmiche L, Brousse N, Kayal S, Gungor T, Blanche S, Holland SM. 2009. Actinomyces in chronic granulomatous disease: an emerging and unanticipated pathogen. Clin Infect Dis 49:1703–1710. doi: 10.1086/647945[↩][↩][↩]
- Acevedo F, Baudrand R, Letelier LM, Gaete P. 2008. Actinomycosis: a great pretender. Case reports of unusual presentations and a review of the literature. Int J Infect Dis 12:358–362. doi: 10.1016/j.ijid.2007.10.006[↩]
- Özcan C, Talas D, Görur K, Aydin Ö, Yildiz A. 2005. Actinomycosis of the middle turbinate: an unusual cause of nasal obstruction. Eur Arch Otorhinolaryngol 262:412–415. doi: 10.1007/s00405-004-0832-y[↩]
- Vorasubin N, Wu AW, Day C, Suh JD. 2013. Invasive sinonasal actinomycosis: case report and literature review. Laryngoscope 123:334–338. doi: 10.1002/lary.23477[↩]
- Woo H-J, Bae CH, Song S-Y, Choi YS, Kim Y-D. 2008. Actinomycosis of the paranasal sinus. Otolaryngol Head Neck Surg 139:460–462. doi: 10.1016/j.otohns.2008.06.001[↩]
- Daamen N, Johnson JT. 2004. Nasopharyngeal actinomycosis: a rare cause of nasal airway obstruction. Laryngoscope 114:1403–1405. doi: 10.1097/00005537-200408000-00016[↩]
- Zheng Y, Tang J. 2013. Retropharyngeal abscess due to Actinomyces species in an immunocompromised patient: case report. J Oral Maxillofac Surg 71:e147–e150. doi: 10.1016/j.joms.2012.11.008[↩]
- Batur Calis A, Özbal AE, Basak T, Turgut S. 2006. Laryngeal actinomycosis accompanying laryngeal carcinoma: report of two cases. Eur Arch Otorhinolaryngol 263:783–785. doi: 10.1007/s00405-006-0057-3[↩]
- Cohen PR, Tschen JA. 2010. Tonsillar actinomycosis mimicking a tonsillolith: colonization of the palantine tonsil presenting as a foul-smelling, removable, unilateral, giant tonsillar concretion. Int J Dermatol 49:1165–1168. doi: 10.1111/j.1365-4632.2009.04432.x[↩]
- Takasaki K, Kitaoka K, Kaieda S, Hayashi T, Abe K, Takahashi H. 2006. A case of actinomycosis causing unilateral tonsillar hypertrophy. Acta Otolaryngol 126:1001–1004. doi: 10.1080/00016480600590604[↩]
- Lensing F, Abele T, Wiggins R 3rd, Quigley E. Laryngeal actinomycosis. Proc (Bayl Univ Med Cent). 2014 Jan;27(1):35-6. doi: 10.1080/08998280.2014.11929047[↩][↩]
- Kakuta R, Hidaka H, Yano H, Miyazaki H, Suzaki H, Nakamura Y, Kanamori H, Endo S, Hirakata Y, Kaku M, Kobayashi T. 2013. Identification of Actinomyces meyeri actinomycosis in middle ear and mastoid by 16S rRNA analysis. J Med Microbiol 62:1245–1248. doi: 10.1099/jmm.0.051698-0[↩][↩]
- Mehta D, Statham M, Choo D. 2007. Actinomycosis of the temporal bone with labyrinthine and facial nerve involvement. Laryngoscope 117:1999–2001. doi: 10.1097/MLG.0b013e318133a127[↩]
- Salipante SJ, Hoogestraat DR, Abbott AN, SenGupta DJ, Cummings LA, Butler-Wu SM, Stephens K, Cookson BT, Hoffman NG. 2014. Coinfection of Fusobacterium nucleatum and Actinomyces israelii in mastoiditis diagnosed by next-generation DNA sequencing. J Clin Microbiol 52:1789–1792. doi: 10.1128/JCM.03133-13[↩][↩]
- Nomura M, Shin M, Ohta M, Nukui Y, Ohkusu K, Saito N. 2011. Atypical osteomyelitis of the skull base and craniovertebral junction caused by Actinomyces infection—case report. Neurol Med Chir (Tokyo) 51:64–66. doi: 10.2176/nmc.51.64[↩][↩]
- Abdalla J, Myers J, Moorman J. 2005. Actinomycotic infection of the oesophagus. J Infect 51:E39–E43. doi: 10.1016/j.jinf.2004.08.011[↩]
- Murchan EM, Redelman-Sidi G, Patel M, Dimaio C, Seo SK. 2010. Esophageal actinomycosis in a fifty-three-year-old man with HIV: case report and review of the literature. AIDS Patient Care STDs 24:73–78. doi: 10.1089/apc.2009.0185[↩]
- Hall V, Talbot PR, Stubbs SL, Duerden BI. 2001. Identification of clinical isolates of Actinomyces species by amplified 16S ribosomal DNA restriction analysis. J Clin Microbiol 39:3555–3562. doi: 10.1128/JCM.39.10.3555-3562.2001[↩][↩][↩][↩][↩][↩][↩]
- Hall V, Collins MD, Hutson R, Falsen E, Duerden BI. 2002. Actinomyces cardiffensis sp. nov. from human clinical sources. J Clin Microbiol 40:3427–3431. doi: 10.1128/JCM.40.9.3427-3431.2002[↩][↩][↩][↩][↩]
- Thacker SA, Healy CM. 2014. Pediatric cervicofacial actinomycosis: an unusual cause of head and neck masses. J Pediatr Infect Dis 3:e15–e19. doi: 10.1093/jpids/pit016[↩]
- Robinson JL, Vaudry WL, Dobrovolsky W. 2005. Actinomycosis presenting as osteomyelitis in the pediatric population. Pediatr Infect Dis J 24:365–369. doi: 10.1097/01.inf.0000157215.15152.c2[↩]
- de Andrade AL, Novaes MM, Germano AR, Luz KG, de Almeida Freitas R, Galvao HC. 2014. Acute primary actinomycosis involving the hard palate of a diabetic patient. J Oral Maxillofac Surg 72:537–541. doi: 10.1016/j.joms.2013.08.006[↩]
- Alamillos-Granados FJ, Dean-Ferrer A, Garcia-Lopez A, Lopez-Rubio F. 2000. Actinomycotic ulcer of the oral mucosa: an unusual presentation of oral actinomycosis. Br J Oral Maxillofac Surg 38:121–123. doi: 10.1054/bjom.1997.0373[↩]
- Kim SR, Jung LY, Oh I-J, et al. 2013. Pulmonary actinomycosis during the first decade of 21st century: cases of 94 patients. BMC Infect Dis 13:216. doi: 10.1186/1471-2334-13-216[↩]
- Clarridge JE, Zhang Q. 2002. Genotypic diversity of clinical Actinomyces species: phenotype, source, and disease correlation among genospecies. J Clin Microbiol 40:3442–3448. doi: 10.1128/JCM.40.9.3442-3448.2002[↩][↩][↩]
- Tietz A, Aldridge KE, Figueroa JE. 2005. Disseminated coinfection with Actinomyces graevenitzii and Mycobacterium tuberculosis: case report and review of the literature. J Clin Microbiol 43:3017–3022. doi: 10.1128/JCM.43.6.3017-3022.2005[↩][↩]
- Gliga S, Devaux M, Gosset Woimant M, Mompoint D, Perronne C, Davido B. Actinomyces graevenitzii pulmonary abscess mimicking tuberculosis in a healthy young man. Can Respir J. 2014 November/December;21(6):e75-e77. doi: 10.1155/2014/841480[↩]
- Nagaoka K, Izumikawa K, Yamamoto Y, Yanagihara K, Ohkusu K, Kohno S. 2012. Multiple lung abscesses caused by Actinomyces graevenitzii mimicking acute pulmonary coccidioidomycosis. J Clin Microbiol 50:3125–3128. doi: 10.1128/JCM.00761-12[↩]
- Fujita Y, Iikura M, Horio Y, Ohkusu K, Kobayashi N. 2012. Pulmonary Actinomyces graevenitzii infection presenting as organizing pneumonia diagnosed by PCR analysis. J Med Microbiol 61:1156–1158. doi: 10.1099/jmm.0.040394-0[↩]
- Apothéloz C, Regamey C. 1996. Disseminated infection due to Actinomyces meyeri: case report and review. Clin Infect Dis 22:621–625. doi: 10.1093/clinids/22.4.621[↩][↩][↩]
- Vallet C, Pezzetta E, Nicolet-Chatelin G, El Lamaa Z, Martinet O, Ris H-B. 2004. Stage III empyema caused by Actinomyces meyeri: a plea for decortication. J Thorac Cardiovasc Surg 127:1511–1513. doi: 10.1016/j.jtcvs.2003.11.043[↩]
- Bartlett AH, Rivera AL, Krishnamurthy R, Baker CJ. 2008. Thoracic actinomycosis in children: case report and review of the literature. Pediatr Infect Dis J 27:165–169. doi: 10.1097/INF.0b013e3181598353[↩]
- Huits RM, Winter HL, Slebos DJ. 2006. A painful swelling on the chest. Thoracic actinomycosis. Clin Infect Dis 42:100–102, 148–150. doi: 10.1086/498513[↩]
- Cone LA, Leung MM, Hirschberg J. 2003. Actinomyces odontolyticus bacteremia. Emerg Infect Dis 9:1629–1632. doi: 10.3201/eid0912.020646[↩]
- Takiguchi Y, Terano T, Hirai A. 2003. Lung abscess caused by Actinomyces odontolyticus. Intern Med 42:723–725. doi: 10.2169/internalmedicine.42.723[↩]
- Wakabayashi K, Yano S, Kadowaki T, Tokushima T, Kanda H, Kobayashi K, Kimura M, Ishikawa S, Ikeda T. 2012. Pulmonary actinomycosis caused by Actinomyces cardiffensis. Intern Med 51:2929–2931. doi: 10.2169/internalmedicine.51.7997[↩]
- Seo JY, Yeom J-S, Ko KS. 2012. Actinomyces cardiffensis septicemia: a case report. Diagn Microbiol Infect Dis 73:86–88. doi: 10.1016/j.diagmicrobio.2012.02.012[↩]
- Gupta A, Lodato RF. 2012. Empyema necessitatis due to Actinomyces israelii. Am J Respir Crit Care Med 185:e16. doi: 10.1164/rccm.201108-1532CR[↩]
- Llamas-Velasco M, Domínguez I, Ovejero E, Pérez-Gala S, García-Diez A. 2010. Empyema necessitatis revisited. Eur J Dermatol 20:115–119. doi: 10.1684/ejd.2010.0809[↩]
- Pérez-Castrillón JL, Gonzalez-Castâneda C, del Campo-Matias F, Bellido-Casado J, Diaz G. Empyema necessitatis due to Actinomyces odontolyticus. Chest. 1997 Apr;111(4):1144. doi: 10.1378/chest.111.4.1144-a[↩]
- Vyas JM, Kasmar A, Chang HR, Holden J, Hohmann E. 2007. Abdominal abscesses due to actinomycosis after laparoscopic cholecystectomy: case reports and review. Clin Infect Dis 44:e1–e4. doi: 10.1086/510077[↩]
- Ladic A, Petrovic I, Augustin G, Puretic H, Skegro M, Gojevic A, Nikolic I. 2013. Hemoptysis as an early symptom of abdominal actinomycosis with thoracic extension ten years after cholecystectomy with retained gallstone. Surg Infect 14:408–411. doi: 10.1089/sur.2012.027[↩]
- Zbar AP, Ranasinghe W, Kennedy PJ. 2009. Subphrenic abscess secondary to Actinomycosis meyeri and Klebsiella ozaenae following laparoscopic cholecystectomy. South Med J 102:725–727. doi: 10.1097/SMJ.0b013e3181abddc5[↩]
- Hansen JM, Fjeldsøe-Nielsen H, Sulim S, Kemp M, Christensen JJ. 2009. Actinomyces species: a Danish survey on human infections and microbiological characteristics. Open Microbiol J 3:113–120. doi: 10.2174/1874285800903010113[↩][↩][↩][↩][↩][↩]
- Garduño E, Rebollo M, Asencio MA, Carro J, Pascasio JM, Blanco J. 2000. Splenic abscesses caused by Actinomyces meyeri in a patient with autoimmune hepatitis. Diagn Microbiol Infect Dis 37:213–214. doi: 10.1016/S0732-8893(00)00133-4[↩]
- Llenas-García J, Lalueza-Blanco A, Fernández-Ruiz M, Villar-Silva J, Ochoa M, Lozano F, Lizasoain M, Aguado JM. 2012. Primary hepatic actinomycosis presenting as purulent pericarditis with cardiac tamponade. Infection 40:339–341. doi: 10.1007/s15010-011-0200-y[↩]
- Makaryus AN, Latzman J, Yang R, Rosman D. 2005. A rare case of Actinomyces israelii presenting as pericarditis in a 75-year-old man. Cardiol Rev 13:125–127. doi: 10.1097/01.crd.0000148846.97618.aa[↩]
- Saad M, Moorman J. 2005. Images in clinical medicine. Actinomyces hepatic abscess with cutaneous fistula. N Engl J Med 353:e16. doi: 10.1056/NEJMicm050528[↩]
- Uehara Y, Takahashi T, Yagoshi M, Shimoguchi K, Yanai M, Kumasaka K, Kikuchi K. 2010. Liver abscess of Actinomyces israelii in a hemodialysis patient: case report and review of the literature. Intern Med 49:2017–2020. doi: 10.2169/internalmedicine.49.3700[↩]
- Gajdács M, Urbán E, Terhes G. Microbiological and Clinical Aspects of Cervicofacial Actinomyces Infections: An Overview. Dent J (Basel). 2019 Sep 1;7(3):85. doi: 10.3390/dj7030085[↩]
- Valour F, Chidiac C, Ferry T; Lyon Bone and Joint Infection Study Group. A 22-year-old woman with right lumpy jaw syndrome and fistulActinomyces BMJ Case Rep. 2015 Feb 5;2015:bcr2014206557. doi: 10.1136/bcr-2014-206557[↩]
- Fazili T, Blair D, Riddell S, Kiska D, Nagra S. 2012. Actinomyces meyeri infection: case report and review of the literature. J Infect 65:357–361. doi: 10.1016/j.jinf.2012.02.016[↩][↩][↩][↩]
- Hinić V, Straub C, Schultheiss E, Kaempfer P, Frei R, Goldenberger D. 2013. Identification of a novel 16S rRNA gene variant of Actinomyces funkei from six patients with purulent infections. Clin Microbiol Infect 19:E312–E314. doi: 10.1111/1469-0691.12201[↩][↩]
- Chao CT, Liao CH, Lai CC, Hsueh PR. 2011. Liver abscess due to Actinomyces odontolyticus in an immunocompetent patient. Infection 39:77–79. doi: 10.1007/s15010-010-0063-7[↩]
- Riegert-Johnson DL, Sandhu N, Rajkumar SV, Patel R. 2002. Thrombotic thrombocytopenic purpura associated with a hepatic abscess due to Actinomyces turicensis. Clin Infect Dis 35:636–637. doi: 10.1086/342327[↩]
- Levy P-Y, Fournier P-E, Charrel R, Metras D, Habib G, Raoult D. 2006. Molecular analysis of pericardial fluid: a 7-year experience. Eur Heart J 27:1942–1946. doi: 10.1093/eurheartj/ehl025[↩]
- Funke G, von Graevenitz A. 1995. Infections due to Actinomyces neuii (former “CDC coryneform group 1” bacteria). Infection 23:73–75. doi: 10.1007/BF01833868[↩][↩][↩][↩][↩][↩]
- von Graevenitz A. 2011. Actinomyces neuii: review of an unusual infectious agent. Infection 39:97–100. doi: 10.1007/s15010-011-0088-6[↩][↩]
- Kalaichelvan V, Maw AA, Singh K. 2006. Actinomyces in cervical smears of women using the intrauterine device in Singapore. Contraception 73:352–355. doi: 10.1016/j.contraception.2005.09.005[↩][↩]
- Westhoff C. 2007. IUDs and colonization or infection with Actinomyces. Contraception 75:S48–S50. doi: 10.1016/j.contraception.2007.01.006[↩][↩]
- Fiorino AS. 1996. Intrauterine contraceptive device-associated actinomycotic abscess and Actinomyces detection on cervical smear. Obstet Gynecol 87:142–149. doi: 10.1016/0029-7844(95)00350-9[↩]
- Carrillo M, Valdez B, Vargas L, Alvarez L, Schorr M, Zlatev R, Stoytcheva M. 2010. In vitro Actinomyces israelii biofilm development on IUD copper surfaces. Contraception 81:261–264. doi: 10.1016/j.contraception.2009.09.008[↩]
- Asemota OA, Girda E, Dueñas O, Neal-Perry G, Pollack SE. 2013. Actinomycosis pelvic abscess after in vitro fertilization. Fertil Steril 100:408–411. doi: 10.1016/j.fertnstert.2013.04.018[↩][↩]
- Elhag KM, Bahar AM, Mubarak AA. 1988. The effect of a copper intra-uterine contraceptive device on the microbial ecology of the female genital tract. J Med Microbiol 25:245–251. doi: 10.1099/00222615-25-4-245[↩]
- Woo PCY, Fung AMY, Lau SKP, Hon E, Yuen K. 2002. Diagnosis of pelvic actinomycosis by 16S ribosomal RNA gene sequencing and its clinical significance. Diagn Microbiol Infect Dis 43:113–118. doi: 10.1016/S0732-8893(02)00375-9[↩]
- Elsayed S, George A, Zhang K. 2006. Intrauterine contraceptive device-associated pelvic actinomycosis caused by Actinomyces urogenitalis. Anaerobe 12:67–70. doi: 10.1016/j.anaerobe.2005.12.004[↩]
- Van Hoecke F, Beuckelaers E, Lissens P, Boudewijns M. 2013. Actinomyces urogenitalis bacteremia and tubo-ovarian abscess after an in vitro fertilization (IVF) procedure. J Clin Microbiol 51:4252–4254. doi: 10.1128/JCM.02142-13[↩][↩]
- Flynn AN, Lyndon CA, Church DL. 2013. Identification by 16S rRNA gene sequencing of an Actinomyces hongkongensis isolate recovered from a patient with pelvic actinomycosis. J Clin Microbiol 51:2721–2723. doi: 10.1128/JCM.00509-13[↩][↩]
- Woo PC, Fung AM, Lau SK, Teng JL, Wong BH, Wong MK, Hon E, Tang GW, Yuen KY. 2003. Actinomyces hongkongensis sp. nov. a novel Actinomyces species isolated from a patient with pelvic actinomycosis. Syst Appl Microbiol 26:518–522. doi: 10.1078/072320203770865819[↩][↩]
- Matsuda K, Nakajima H, Khan KN, Tanigawa T, Hamaguchi D, Kitajima M, Hiraki K, Moriyama S, Masuzaki H. 2012. Preoperative diagnosis of pelvic actinomycosis by clinical cytology. Int J Womens Health 4:527–533. doi: 10.2147/IJWH.S35573[↩]
- Ong C, Barnes S, Senanayake S. Actinomyces turicensis infection mimicking ovarian tumour. Singapore Med J. 2012 Jan;53(1):e9-e11. https://smj.sma.org.sg/5301/5301cr4.pdf[↩]
- Gomes J, Pereira T, Carvalho A, Brito C. Primary cutaneous actinomycosis caused by Actinomyces meyeri as first manifestation of HIV infection. Dermatol Online J. 2011 Nov 15;17(11):5. https://escholarship.org/uc/item/0n05580m[↩]
- Capobianco G, Dessole S, Becchere MP, Profili S, Cosmi E, Cherchi PL, Meloni GB. 2005. A rare case of primary actinomycosis of the breast caused by Actinomyces viscosus: diagnosis by fine-needle aspiration cytology under ultrasound guidance. Breast J 11:57–59. doi: 10.1111/j.1075-122X.2005.21613.x[↩]
- Hermida MD, Della Giovanna P, Lapadula M, García S, Cabrera HN. 2009. Actinomyces meyeri cutaneous actinomycosis. Int J Dermatol 48:154–156. doi: 10.1111/j.1365-4632.2009.03798.x[↩]
- Duvignaud A, Ribeiro E, Moynet D, Longy-Boursier M, Malvy D. 2014. Cervical spondylitis and spinal abscess due to Actinomyces meyeri. Braz J Infect Dis 18:106–109. doi: 10.1016/j.bjid.2013.05.016[↩]
- Honda H, Bankowski MJ, Kajioka EHN, Chokrungvaranon N, Kim W, Gallacher ST. 2008. Thoracic vertebral actinomycosis: Actinomyces israelii and Fusobacterium nucleatum. J Clin Microbiol 46:2009–2014. doi: 10.1128/JCM.01706-07[↩]
- Gaïni S, Røge BT, Pedersen C, Pedersen SS, Brenøe A-S. 2006. Severe Actinomyces israelii infection involving the entire spinal cord. Scand J Infect Dis 38:211–213. doi: 10.1080/00365540500322312[↩]
- Ghafghaichi L, Troy S, Budvytiene I, Banaei N, Baron EJ. 2010. Mixed infection involving Actinomyces, Aggregatibacter, and Fusobacterium species presenting as perispinal tumor. Anaerobe 16:174–178. doi: 10.1016/j.anaerobe.2009.07.003[↩]
- Edwards TM, Demos TC, Lomasney LM. 2011. Radiologic case study. Musculoskeletal actinomycosis. Orthopedics 34:641, 730–733. doi: 10.3928/01477447-20110714-49[↩]
- Musher DM. 1998. Actinomycosis of 54 years’ duration. Clin Infect Dis 27:889. doi: 10.1086/514965[↩]
- Smego RA., Jr 1987. Actinomycosis of the central nervous system. Rev Infect Dis 9:855–865. doi: 10.1093/clinids/9.5.855[↩]
- Van Dellen JR. 2010. Actinomycosis: an ancient disease difficult to diagnose. World Neurosurg 74:263–264. doi: 10.1016/j.wneu.2010.06.012[↩]
- Olah E, Berger C, Boltshauser E, Nadal D. 2004. Cerebral actinomycosis before adolescence. Neuropediatrics 35:239–241. doi: 10.1055/s-2004-820895[↩]
- Bouziri A, Khaldi A, Smaoui H, Menif K, Ben Jaballah N. 2011. Fatal subdural empyema caused by Streptococcus constellatus and Actinomyces viscosus in a child—case report. J Microbiol Immunol Infect 44:394–396. doi: 10.1016/j.jmii.2010.03.002[↩]
- Kuijper EJ, Wiggerts HO, Jonker GJ, Schaal KP, de Gans J. 1992. Disseminated actinomycosis due to Actinomyces meyeri and Actinobacillus actinomycetemcomitans. Scand J Infect Dis 24:667–672. doi: 10.3109/00365549209054655[↩][↩]
- Zijlstra EE, Swart GR, Godfroy FJ, Degener JE. 1992. Pericarditis, pneumonia and brain abscess due to a combined Actinomyces-Actinobacillus actinomycetemcomitans infection. J Infect 25:83–87. doi: 10.1016/0163-4453(92)93633-2[↩][↩]
- Colmegna I, Rodriguez-Barradas M, Rauch R, Clarridge J, Young EJ. 2003. Disseminated Actinomyces meyeri infection resembling lung cancer with brain metastases. Am J Med Sci 326:152–155. doi: 10.1097/00000441-200309000-00010[↩]
- Naik NH, Russo TA. 2009. Bisphosphonate-related osteonecrosis of the jaw: the role of Actinomyces. Clin Infect Dis 49:1729–1732. doi: 10.1086/648075[↩]
- Curi MM, Dib LL, Kowalski LP, Landman G, Mangini C. 2000. Opportunistic actinomycosis in osteoradionecrosis of the jaws in patients affected by head and neck cancer: incidence and clinical significance. Oral Oncol 36:294–299. doi: 10.1016/S1368-8375(99)00080-9[↩][↩]
- Kos M, Kuebler JF, Luczak K, Engelke W. 2010. Bisphosphonate-related osteonecrosis of the jaws: a review of 34 cases and evaluation of risk. J Craniomaxillofac Surg 38:255–259. doi: 10.1016/j.jcms.2009.06.005[↩]
- Sedghizadeh PP, Kumar SKS, Gorur A, Schaudinn C, Shuler CF, Costerton JW. 2009. Microbial biofilms in osteomyelitis of the jaw and osteonecrosis of the jaw secondary to bisphosphonate therapy. J Am Dent Assoc 140:1259–1265. doi: 10.14219/jada.archive.2009.0049[↩]
- Happonen RP, Viander M, Pelliniemi L, Aitasalo K. 1983. Actinomyces israelii in osteoradionecrosis of the jaws. Histopathologic and immunocytochemical study of five cases. Oral Surg Oral Med Oral Pathol 55:580–588. doi: 10.1016/0030-4220(83)90374-2[↩]
- Hansen T, Wagner W, Kirkpatrick CJ, Kunkel M. 2006. Infected osteoradionecrosis of the mandible: follow-up study suggests deterioration in outcome for patients with Actinomyces-positive bone biopsies. Int J Oral Maxillofac Surg 35:1001–1004. doi: 10.1016/j.ijom.2006.08.006[↩]
- Aas JA, Reime L, Pedersen K, Eribe ERK, Abesha-Belay E, Støre G, Olsen I. 13 July 2010. Osteoradionecrosis contains a wide variety of cultivable and non-cultivable bacteria. J Oral Microbiol doi: 10.3402/jom.v2i0.5072[↩]
- Støre G, Eribe ERK, Olsen I. 2005. DNA-DNA hybridization demonstrates multiple bacteria in osteoradionecrosis. Int J Oral Maxillofac Surg 34:193–196. doi: 10.1016/j.ijom.2004.06.010[↩]
- Curtis JR, Yang S, Patkar NM, Chen L, Singh JA, Cannon GW, Mikuls TR, Delzell E, Saag KG, Safford MM, DuVall S, Alexander K, Napalkov P, Winthrop KL, Burton MJ, Kamauu A, Baddley JW. 2014. Risk of hospitalized bacterial infections associated with biologic treatment among US veterans with rheumatoid arthritis. Arthritis Care Res 66:990–997. doi: 10.1002/acr.22281[↩]
- Marie I, Lahaxe L, Levesque H, Heliot P. 2008. Pulmonary actinomycosis in a patient with diffuse systemic sclerosis treated with infliximab. QJM 101:419–421. doi: 10.1093/qjmed/hcn028[↩]
- Chen KH, Lin CH. 2013. Brain abscess as an initial presentation in a patient of hereditary haemorrhagic telangiectasia caused by a novel ENG mutation. BMJ Case Rep 2013:bcr2013008802. doi: 10.1136/bcr-2013-008802[↩]
- Hall WA. Hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber disease) presenting with polymicrobial brain abscess. Case report. J Neurosurg. 1994 Aug;81(2):294-6. doi: 10.3171/jns.1994.81.2.0294[↩]
- Woods ML. Photo quiz I. Hereditary hemorrhagic telangiectasia, pulmonary arteriovenous malformations, and brain abscess. Clin Infect Dis. 1998 May;26(5):1071, 1220-1. doi: 10.1086/520296[↩]
- van den Berg JM, van Koppen E, Ahlin A, Belohradsky BH, Bernatowska E, Corbeel L, Español T, Fischer A, Kurenko-Deptuch M, Mouy R, Petropoulou T, Roesler J, Seger R, Stasia M-J, Valerius NH, Weening RS, Wolach B, Roos D, Kuijpers TW. 2009. Chronic granulomatous disease: the European experience. PLoS One 4:e5234. doi: 10.1371/journal.pone.0005234[↩]
- Agger WA, Kowalski TJ. 2010. Chronic granulomatous disease, catalase, and Actinomyces. Clin Infect Dis 50:1325–1326. doi: 10.1086/651690[↩]
- Garelick JM, Khodabakhsh AJ, Josephberg RG. 2002. Acute postoperative endophthalmitis caused by Actinomyces neuii. Am J Ophthalmol 133:145–147. doi: 10.1016/S0002-9394(01)01206-5[↩]
- Raman VS, Evans N, Shreshta B, Cunningham R. 2004. Chronic postoperative endophthalmitis caused by Actinomyces neuii. J Cataract Refract Surg 30:2641–2643. doi: 10.1016/j.jcrs.2004.04.070[↩]
- Pérez-Santonja JJ, Campos-Mollo E, Fuentes-Campos E, Samper-Giménez J, Alió JL. Actinomyces neuii subspecies anitratus chronic endophthalmitis after cataract surgery. Eur J Ophthalmol. 2007 May-Jun;17(3):445-7. doi: 10.1177/112067210701700331[↩]
- Peponis VG, Chalkiadakis SE, Parikakis EA, Mitropoulos PG. 2011. Chronic postoperative endophthalmitis caused by Actinomyces meyeri. Case Rep Ophthalmol 2:95–98. doi: 10.1159/00032606[↩]
- Scarano FJ, Ruddat MS, Robinson A. 1999. Actinomyces viscosus postoperative endophthalmitis. Diagn Microbiol Infect Dis 34:115–117. doi: 10.1016/S0732-8893(99)00009-7[↩]
- Graffi S, Peretz A, Naftali M. 2012. Endogenous endophthalmitis with an unusual infective agent: Actinomyces neuii. Eur J Ophthalmol 22:834–835. doi: 10.5301/ejo.5000106[↩]
- Milman T, Mirani N, Gibler T, Van Gelder RN, Langer PD. 2008. Actinomyces israelii endogenous endophthalmitis. Br J Ophthalmol 92:427–428. doi: 10.1136/bjo.2007.123596[↩]
- Karimian F, Feizi S, Nazari R, Zarin-Bakhsh P. 2008. Delayed-onset Actinomyces keratitis after laser in situ keratomileusis. Cornea 27:843–846. doi: 10.1097/ICO.0b013e31816a624a[↩]
- Hussain I, Bonshek RE, Loudon K, Armstrong M, Tullo AB. 1993. Canalicular infection caused by Actinomyces. Eye 7:542–544. doi: 10.1038/eye.1993.118[↩][↩]
- Yuksel D, Hazirolan D, Sungur G, Duman S. 2012. Actinomyces canaliculitis and its surgical treatment. Int Ophthalmol 32:183–186. doi: 10.1007/s10792-012-9531-7[↩]
- Olender A, Matysik-Woźniak A, Rymgayłło-Jankowska B, Rejdak R. The cause of Actinomyces canalictulis–a case study. Ann Agric Environ Med. 2013;20(4):742-4. https://www.aaem.pl/The-cause-of-Actinomyces-canalictulis-a-case-study,72009,0,2.html[↩]
- Kerttula AM, Carlson P, Sarkonen N, Hall V, Könönen E. 2005. Enzymatic/biochemical analysis of Actinomyces with commercial test kits with an emphasis on newly described species. Anaerobe 11:99–108. doi: 10.1016/j.anaerobe.2004.11.002[↩][↩][↩][↩][↩][↩]
- Könönen E, Kanervo A, Bryk A, Aino T, Syrjänen R, Jousimies-Somer H. 1999. Anaerobes in the nasopharynx during acute otitis media episodes in infancy. Anaerobe 5:237–239. doi: 10.1006/anae.1999.0225[↩]
- Jousimies-Somer H, Savolainen S, Mäkitie A, Ylikoski J. 1993. Bacteriologic findings in peritonsillar abscesses in young adults. Clin Infect Dis 16(Suppl 4):S292–S298. doi: 10.1093/clinids/16.Supplement_4.S292[↩]
- Sabbe LJ, Van De Merwe D, Schouls L, Bergmans A, Vaneechoutte M, Vandamme P. Clinical spectrum of infections due to the newly described Actinomyces species A. turicensis, A. radingae, and A. europaeus. J Clin Microbiol. 1999 Jan;37(1):8-13. doi: 10.1128/JCM.37.1.8-13.1999[↩][↩][↩][↩][↩][↩][↩]
- Hall V, Collins MD, Lawson PA, Falsen E, Duerden BI. 2003. Actinomyces nasicola sp. nov., isolated from a human nose. Int J Syst Evol Microbiol 53:1445–1448. doi: 10.1099/ijs.0.02582-0[↩]
- Brailsford SR, Tregaskis RB, Leftwich HS, Beighton D. 1999. The predominant Actinomyces spp. isolated from infected dentin of active root caries lesions. J Dent Res 78:1525–1534. doi: 10.1177/00220345990780090701[↩][↩]
- Tanner ACR, Mathney JMJ, Kent RL, Chalmers NI, Hughes CV, Loo CY, Pradhan N, Kanasi E, Hwang J, Dahlan MA, Papadopolou E, Dewhirst FE. 2011. Cultivable anaerobic microbiota of severe early childhood caries. J Clin Microbiol 49:1464–1474. doi: 10.1128/JCM.02427-10[↩][↩]
- Bowden GH, Nolette N, Ryding H, Cleghorn BM. 1999. The diversity and distribution of the predominant ribotypes of Actinomyces naeslundii genospecies 1 and 2 in samples from enamel and from healthy and carious root surfaces of teeth. J Dent Res 78:1800–1809. doi: 10.1177/00220345990780120601[↩]
- Signoretti FGC, Endo MS, Gomes BPFA, Montagner F, Tosello FB, Jacinto RC. 2011. Persistent extraradicular infection in root-filled asymptomatic human tooth: scanning electron microscopic analysis and microbial investigation after apical microsurgery. J Endod 37:1696–1700. doi: 10.1016/j.joen.2011.09.018[↩]
- Siqueira JF, Rôças IN. 2003. Polymerase chain reaction detection of Propionibacterium propionicus and Actinomyces radicidentis in primary and persistent endodontic infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96:215–222. doi: 10.1016/S1079-2104(03)00158-6[↩][↩]
- Siqueira JF, Rôças IN, Souto R, de Uzeda M, Colombo AP. 2002. Actinomyces species, streptococci, and Enterococcus faecalis in primary root canal infections. J Endod 28:168–172. doi: 10.1097/00004770-200203000-00006[↩]
- Sunde PT, Olsen I, Debelian GJ, Tronstad L. 2002. Microbiota of periapical lesions refractory to endodontic therapy. J Endod 28:304–310. doi: 10.1097/00004770-200204000-00011[↩][↩]
- Xia T, Baumgartner JC. 2003. Occurrence of Actinomyces in infections of endodontic origin. J Endod 29:549–552. doi: 10.1097/00004770-200309000-00001[↩][↩][↩][↩][↩]
- Siqueira JF, Rôças IN, Souto R, de Uzeda M, Colombo AP. 2002. Actinomyces species, streptococci, and Enterococcus faecalis in primary root canal infections. J Endod 28:168–172. doi: 10.1097/00004770-200203000-0000[↩][↩][↩]
- Collins MD, Hoyles L, Kalfas S, Sundquist G, Monsen T, Nikolaitchouk N, Falsen E. Characterization of Actinomyces isolates from infected root canals of teeth: description of Actinomyces radicidentis sp. nov. J Clin Microbiol. 2000 Sep;38(9):3399-403. doi: 10.1128/JCM.38.9.3399-3403.2000[↩]
- Hall V, Collins MD, Hutson RA, Inganäs E, Falsen E, Duerden BI. 2003. Actinomyces oricola sp. nov., from a human dental abscess. Int J Syst Evol Microbiol 53:1515–1518. doi: 10.1099/ijs.0.02576-0[↩]
- Hall V, Collins MD, Lawson PA, Falsen E, Duerden BI. 2005. Actinomyces dentalis sp. nov., from a human dental abscess. Int J Syst Evol Microbiol 55:427–431. doi: 10.1099/ijs.0.63376-0[↩]
- Tanner A, Maiden MF, Macuch PJ, Murray LL, Kent RL. 1998. Microbiota of health, gingivitis, and initial periodontitis. J Clin Periodontol 25:85–98. doi: 10.1111/j.1600-051X.1998.tb02414.x[↩]
- Gmür R, Wyss C, Xue Y, Thurnheer T, Guggenheim B. 2004. Gingival crevice microbiota from Chinese patients with gingivitis or necrotizing ulcerative gingivitis. Eur J Oral Sci 112:33–41. doi: 10.1111/j.0909-8836.2004.00103.x[↩]
- Persson GR, Hitti J, Paul K, Hirschi R, Weibel M, Rothen M, Persson RE. 2008. Tannerella forsythia and Pseudomonas aeruginosa in subgingival bacterial samples from parous women. J Periodontol 79:508–516. doi: 10.1902/jop.2008.070350[↩]
- Sixou J-L, Magaud C, Jolivet-Gougeon A, Cormier M, Bonnaure-Mallet M. 2003. Evaluation of the mandibular third molar pericoronitis flora and its susceptibility to different antibiotics prescribed in France. J Clin Microbiol 41:5794–5797. doi: 10.1128/JCM.41.12.5794-5797.2003[↩]
- Sarkonen N, Könönen E, Eerola E, Könönen M, Jousimies-Somer H, Laine P. 2005. Characterization of Actinomyces species isolated from failed dental implant fixtures. Anaerobe 11:231–237. doi: 10.1016/j.anaerobe.2005.01.002[↩]
- Young MP, Carter DH, Worthington H, Korachi M, Drucker DB. 2001. Microbial analysis of bone collected during implant surgery: a clinical and laboratory study. Clin Oral Implants Res 12:95–103. doi: 10.1034/j.1600-0501.2001.012002095.x[↩]
- Gómez-Garcés JL, Burillo A, Gil Y, Sáez-Nieto JA. 2010. Soft tissue infections caused by Actinomyces neuii, a rare pathogen. J Clin Microbiol 48:1508–1509. doi: 10.1128/JCM.02139-09[↩]
- Lacoste C, Escande M-C, Jammet P, Nos C. 2009. Breast Actinomyces neuii abscess simulating primary malignancy: a case diagnosed by fine-needle aspiration. Diagn Cytopathol 37:311–312. doi: 10.1002/dc.21044[↩]
- Olson JM, Vary JC Jr. Primary cutaneous Actinomyces neuii infection of the breast successfully treated with doxycycline. Cutis. 2013 Dec;92(6):E3-4. https://www.mdedge.com/dermatology/article/79309/primary-cutaneous-actinomyces-neuii-infection-breast-successfully-treated[↩]
- Silva WA, Pinheiro AM, Jahns B, Bögli-Stuber K, Droz S, Zimmerli S. 2011. Breast abscess due to Actinomyces europaeus. Infection 39:255–258. doi: 10.1007/s15010-011-0119-3[↩]
- Funke G, Alvarez N, Pascual C, Falsen E, Akervall E, Sabbe L, Schouls L, Weiss N, Collins MD. 1997. Actinomyces europaeus sp. nov., isolated from human clinical specimens. Int J Syst Bacteriol 47:687–692. doi: 10.1099/00207713-47-3-687[↩][↩][↩][↩][↩]
- Attar KH, Waghorn D, Lyons M, Cunnick G. 2007. Rare species of Actinomyces as causative pathogens in breast abscess. Breast J 13:501–505. doi: 10.1111/j.1524-4741.2007.00472.x[↩][↩][↩]
- Cato EP, Moore WEC, Nygaard G, Holdeman LV. 1984. Actinomyces meyeri sp. nov., specific epithet rev. Int J Syst Bacteriol 34:487–489. doi: 10.1099/00207713-34-4-487[↩][↩]
- Abdulrahman GO Jr, Gateley CA. 2015. Primary actinomycosis of the breast caused by Actinomyces turicensis with associated Peptoniphilus harei. Breast Dis 35:45–47. doi: 10.3233/BD-140381[↩][↩]
- Funke G, Stubbs S, von Graevenitz A, Collins MD. Assignment of human-derived CDC group 1 coryneform bacteria and CDC group 1-like coryneform bacteria to the genus Actinomyces as Actinomyces neuii subsp. neuii sp. nov., subsp. nov., and Actinomyces neuii subsp. anitratus subsp. nov. Int J Syst Bacteriol. 1994 Jan;44(1):167-71. doi: 10.1099/00207713-44-1-167[↩][↩]
- Chudackova E, Geigerova L, Hrabak J, Bergerova T, Liska V, Scharfen J Jr. 2010. Seven isolates of Actinomyces turicensis from patients with surgical infections of the anogenital area in a Czech hospital. J Clin Microbiol 48:2660–2661. doi: 10.1128/JCM.00548-10[↩]
- Ng LS, Sim JH, Eng LC, Menon S, Tan TY. 2012. Comparison of phenotypic methods and matrix-assisted laser desorption ionisation time-of-flight mass spectrometry for the identification of aero-tolerant Actinomyces spp. isolated from soft-tissue infections. Eur J Clin Microbiol Infect Dis 31:1749–1752. doi: 10.1007/s10096-011-1496-3[↩][↩]
- Sofianou D, Avgoustinakis E, Dilopoulou A, Pournaras S, Tsirakidis G, Tsakris A. 2004. Soft-tissue abscess involving Actinomyces odontolyticus and two Prevotella species in an intravenous drug abuser. Comp Immunol Microbiol Infect Dis 27:75–79. doi: 10.1016/S0147-9571(03)00052-3[↩][↩]
- Summanen PH, Talan DA, Strong C, McTeague M, Bennion R, Thompson JE, Väisänen ML, Moran G, Winer M, Finegold SM. 1995. Bacteriology of skin and soft-tissue infections: comparison of infections in intravenous drug users and individuals with no history of intravenous drug use. Clin Infect Dis 20(Suppl 2):S279–S282. doi: 10.1093/clinids/20.Supplement_2.S279[↩]
- Davanos E, Rahman SM, Nogid B. 2008. Treatment of Eikenella corrodens and Actinomyces odontolyticus foot abscess in a penicillin-allergic patient. Ann Pharmacother 42:1706–1710. doi: 10.1345/aph.1L257[↩]
- Zautner AE, Schmitz S, Aepinus C, Schmialek A, Podbielski A. 2009. Subcutaneous fistulae in a patient with femoral hypoplasia due to Actinomyces europaeus and Actinomyces turicensis. Infection 37:289–291. doi: 10.1007/s15010-008-7392-9[↩]
- Funke G, Englert R, Frodl R, Bernard KA, Stenger S. 2010. Actinomyces hominis sp. nov., isolated from a wound swab. Int J Syst Evol Microbiol 60:1678–1681. doi: 10.1099/ijs.0.015818-0[↩]
- McElroy JY, Gorens ME, Jackson LN, Stigger D, Becker T, Sheiner E. 2006. Actinomyces israelii may produce vulvar lesions suspicious for malignancy. Infect Dis Obstet Gynecol 2006:48269. doi: 10.1155/IDOG/2006/48269[↩]
- Tena D, Losa C, Medina-Pascual MJ, Saez-Nieto JA. 2014. Fournier’s gangrene caused by Actinomyces funkei, Fusobacterium gonidiaformans and Clostridium hathewayi. Anaerobe 27:14–16. doi: 10.1016/j.anaerobe.2014.02.004[↩][↩]
- Nikolaitchouk N, Hoyles L, Falsen E, Grainger JM, Collins MD. 2000. Characterization of Actinomyces isolates from samples from the human urogenital tract: description of Actinomyces urogenitalis sp. nov. Int J Syst Evol Microbiol 50:1649–1654. doi: 10.1099/00207713-50-4-1649[↩][↩][↩]
- Mann C, Dertinger S, Hartmann G, Schurz R, Simma B. 2002. Actinomyces neuii and neonatal sepsis. Infection 30:178–180. doi: 10.1007/s15010-002-2165-3[↩]
- Wright JR, Stinson D, Wade A, Haldane D, Heifetz SA. 1994. Necrotizing funisitis associated with Actinomyces meyeri infection: a case report. Pediatr Pathol 14:927–934. doi: 10.3109/15513819409037689[↩]
- Pinilla I, Martín-Hervás C, Gil-Garay E. 2006. Primary sternal osteomyelitis caused by Actinomyces israelii. South Med J 99:96–97. doi: 10.1097/01.smj.0000197512.82441.41[↩]
- Vandevelde AG, Jenkins SG, Hardy PR. 1995. Sclerosing osteomyelitis and Actinomyces naeslundii infection of surrounding tissues. Clin Infect Dis 20:1037–1039. doi: 10.1093/clinids/20.4.1037[↩]
- Ramos CP, Falsen E, Alvarez N, Akervall E, Sjödén B, Collins MD. 1997. Actinomyces graevenitzii sp. nov., isolated from human clinical specimens. Int J Syst Bacteriol 47:885–888. doi: 10.1099/00207713-47-3-885[↩]
- Lee MJ, Ha YE, Park HY, Lee JH, Lee YJ, Sung KS, Kang C-I, Chung DR, Song J-H, Peck KR. 2012. Osteomyelitis of a long bone due to Fusobacterium nucleatum and Actinomyces meyeri in an immunocompetent adult: a case report and literature review. BMC Infect Dis 12:161. doi: 10.1186/1471-2334-12-161[↩]
- Van Bosterhaut B, Boucquey P, Janssens M, Wauters G, Delmée M. 2002. Chronic osteomyelitis due to Actinomyces neuii subspecies neuii and Dermabacter hominis. Eur J Clin Microbiol Infect Dis 21:486–487. doi: 10.1007/s10096-002-0747-8[↩]
- Lecouvet F, Irenge L, Vandercam B, Nzeusseu A, Hamels S, Gala J-L. 2004. The etiologic diagnosis of infectious discitis is improved by amplification-based DNA analysis. Arthritis Rheum 50:2985–2994. doi: 10.1002/art.20462[↩]
- Renvoise A, Raoult D, Roux V. 2010. Actinomyces timonensis sp. nov., isolated from a human clinical osteo-articular sample. Int J Syst Evol Microbiol 60:1516–1521. doi: 10.1099/ijs.0.012914-0[↩]
- Brunner S, Graf S, Riegel P, Altwegg M. 2000. Catalase-negative Actinomyces neuii subsp. neuii isolated from an infected mammary prosthesis. Int J Med Microbiol 290:285–287. doi: 10.1016/S1438-4221(00)80128-9[↩]
- Hsi RS, Hotaling JM, Spencer ES, Bollyky PL, Walsh TJ. 2011. Isolated infection of a decommissioned penile prosthesis reservoir with Actinomyces neuii. J Sex Med 8:923–926. doi: 10.1111/j.1743-6109.2010.02144.x[↩]
- Grundmann S, Huebner J, Stuplich J, Koch A, Wu K, Geibel-Zehender A, Bode C, Brunner M. 2010. Prosthetic valve endocarditis due to Actinomyces neuii successfully treated with antibiotic therapy. J Clin Microbiol 48:1008–1011. doi: 10.1128/JCM.01106-09[↩][↩]
- Rieber H, Schwarz R, Krämer O, Cordier W, Frommelt L. 2009. Actinomyces neuii subsp. neuii associated with periprosthetic infection in total hip arthroplasty as causative agent. J Clin Microbiol 47:4183–4184. doi: 10.1128/JCM.01249-09[↩]
- Anderson IA, Jarral F, Sethi K, Chumas PD. 2014. Paediatric ventriculoperitoneal shunt infection caused by Actinomyces neuii. BMJ Case Rep 2014:bcr2014204576. doi: 10.1136/bcr-2014-204576[↩]
- Watkins RR, Anthony K, Schroder S, Hall GS. 2008. Ventriculoperitoneal shunt infection caused by Actinomyces neuii subsp. neuii. J Clin Microbiol 46:1888–1889. doi: 10.1128/JCM.02141-07[↩]
- Varughese S, Bargman J. 2014. Actinomyces neuii PD peritonitis—resolution of infection without catheter removal. Perit Dial Int 34:815–816. doi: 10.3747/pdi.2013.00146[↩]
- Hedke J, Skripitz R, Ellenrieder M, Frickmann H, Köller T, Podbielski A, Mittelmeier W. 2012. Low-grade infection after a total knee arthroplasty caused by Actinomyces naeslundii. J Med Microbiol 61:1162–1164. doi: 10.1099/jmm.0.030395-0[↩]
- Zaman R, Abbas M, Burd E. 2002. Late prosthetic hip joint infection with Actinomyces israelii in an intravenous drug user: case report and literature review. J Clin Microbiol 40:4391–4392. doi: 10.1128/JCM.40.11.4391-4392.2002[↩]
- Wüst J, Steiger U, Vuong H, Zbinden R. Infection of a hip prosthesis by Actinomyces naeslundii. J Clin Microbiol. 2000 Feb;38(2):929-30. doi: 10.1128/JCM.38.2.929-930.2000[↩]
- Siu YP, Tong MK, Lee MK, Leung KT, Kwan TH. Exit-site infection caused by Actinomyces odontolyticus in a CAPD patient. Perit Dial Int. 2004 Nov-Dec;24(6):602-3.[↩]
- Branquinho DF, Andrade DR, Almeida N, Sofia C. 2014. Mediastinitis by Actinomyces meyeri after oesophageal stent placement. BMJ Case Rep 2014:bcr2014204499. doi: 10.1136/bcr-2014-204499[↩]
- Cohen E, Bishara J, Medalion B, Sagie A, Garty M. 2007. Infective endocarditis due to Actinomyces neuii. Scand J Infect Dis 39:180–183. doi: 10.1080/00365540600802007[↩]
- Westling K, Lidman C, Thalme A. 2002. Tricuspid valve endocarditis caused by a new species of actinomyces: Actinomyces funkei. Scand J Infect Dis 34:206–207. doi: 10.1080/00365540110077425[↩]
- Adalja AA, Vergis EN. 2010. Actinomyces israelii endocarditis misidentified as “diptheroids.” Anaerobe 16:472–473. doi: 10.1016/j.anaerobe.2010.05.003[↩]
- Lam S, Samraj J, Rahman S, Hilton E. 1993. Primary actinomycotic endocarditis: case report and review. Clin Infect Dis 16:481–485. doi: 10.1093/clind/16.4.481[↩][↩]
- Julian KG, de Flesco L, Clarke LE, Parent LJ. 2005. Actinomyces viscosus endocarditis requiring aortic valve replacement. J Infect 50:359–362. doi: 10.1016/j.jinf.2004.04.006[↩]
- Mardis JS, Many WJ Jr. Endocarditis due to Actinomyces viscosus. South Med J. 2001 Feb;94(2):240-3.[↩]
- Moffatt S, Ahmen AR, Forward K. First reported case of bacterial endocarditis attributable to Actinomyces meyeri. Can J Infect Dis. 1996 Jan;7(1):71-3. doi: 10.1155/1996/761841[↩]
- Lawson PA, Nikolaitchouk N, Falsen E, Westling K, Collins MD. 2001. Actinomyces funkei sp. nov., isolated from human clinical specimens. Int J Syst Evol Microbiol 51:853–855. doi: 10.1099/00207713-51-3-853[↩]
- Hwang SS, Park SD, Jang IH, Uh Y, Yoon KJ, Kim HY. 2011. Actinomyces graevenitzii bacteremia in a patient with alcoholic liver cirrhosis. Anaerobe 17:87–89. doi: 10.1016/j.anaerobe.2011.03.002[↩]
- Renvoise A, Raoult D, Roux V. 2009. Actinomyces massiliensis sp. nov., isolated from a patient blood culture. Int J Syst Evol Microbiol 59:540–544. doi: 10.1099/ijs.0.001503-0[↩]
- Topic MB, Desnica B, Vickovic N, Skuhala T, Bayer K, Bukovski S. 2014. The polymicrobial Actinomyces naeslundii and Pseudomonas aeruginosa sepsis in a patient with ulcerative colitis 2 months after colonoscopy. Wien Klin Wochenschr 126:130–132. doi: 10.1007/s00508-013-0471-7[↩]
- Bahrani-Mougeot FK, Paster BJ, Coleman S, Ashar J, Barbuto S, Lockhart PB. 2008. Diverse and novel oral bacterial species in blood following dental procedures. J Clin Microbiol 46:2129–2132. doi: 10.1128/JCM.02004-07[↩]
- Hwang CS, Lee H, Hong MP, Kim JH, Kim KS. Brain abscess caused by chronic invasive actinomycosis in the nasopharynx: a case report and literature review. Medicine. Apr 2018;97(16) doi: 10.1097/MD.0000000000010406[↩]



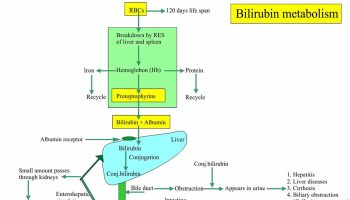

{kind=link}