Contents
What is an arachnoid cyst
Arachnoid cyst is cerebrospinal fluid (CSF) filled sac, not tumors (not cancer), that is located on the arachnoid membrane that covers the brain (intracranial) and the spinal cord (spinal), one of the three membranes that cover the brain and spinal cord 1. Arachnoid cysts are benign, and the vast majority remain asymptomatic throughout life 2. The exact cause of arachnoid cysts is unknown. Arachnoid cysts account for ~1% of all intracranial masses 1. Although the vast majority are sporadic, they are seen with increased frequency in mucopolysaccharidoses 1.
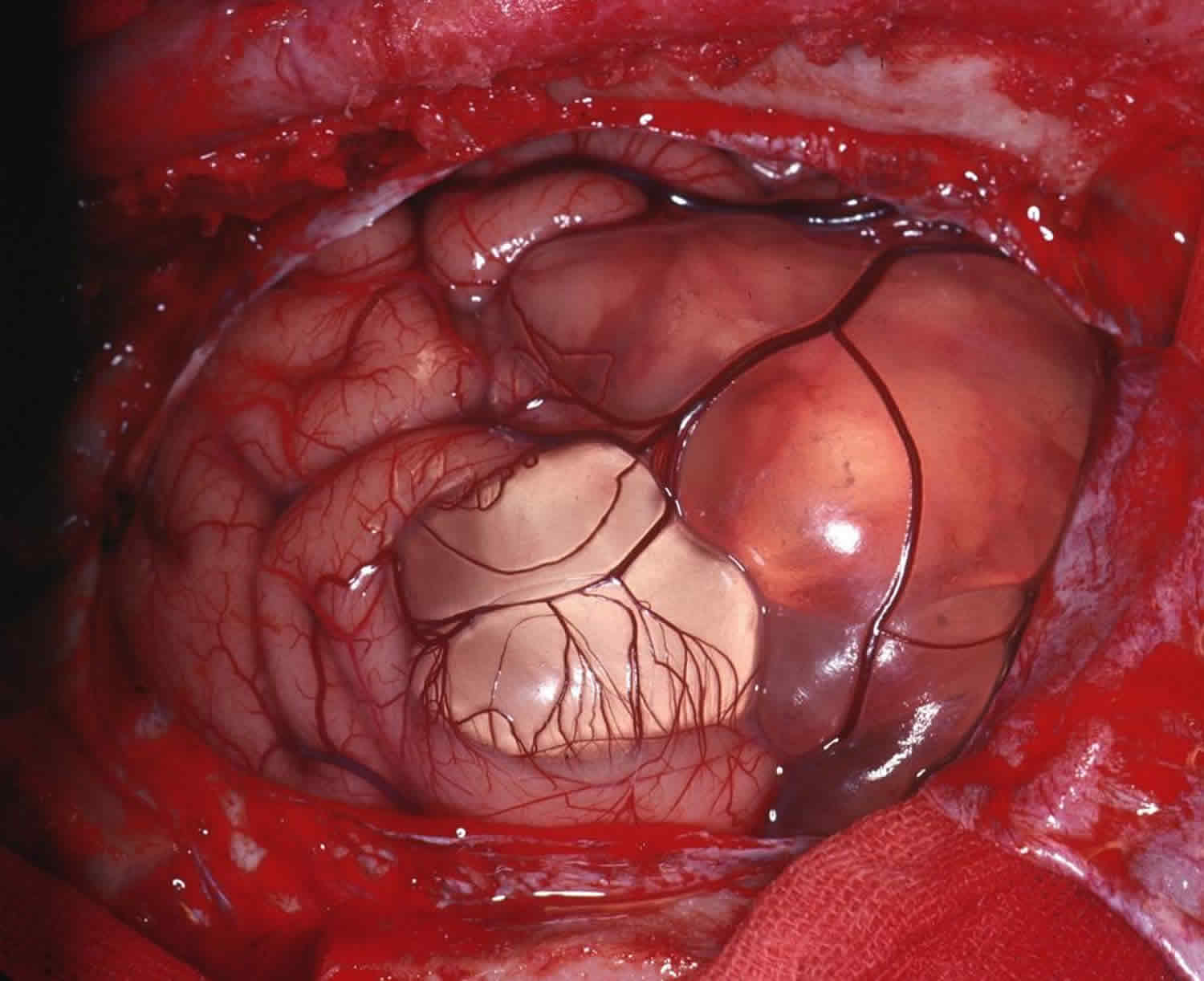
There are three connective tissue membranes called meninges, which are protective, connective tissue coverings that lie just external to the brain and spinal cord (the central nervous system): the dura mater (outermost layer), arachnoid (middle layer) and pia mater (deepest layer). Their functions are to cover and protect the central nervous system (the spinal cord and brain); enclose and protect the blood vessels that supply the central nervous system (CNS); contain the cerebrospinal fluid (CSF). The arachnoid membrane (arachnoid mater) lies just deep to the dura mater (outermost layer). Deep to the arachnoid membrane is the wide subarachnoid space, which is spanned by weblike threads that hold the arachnoid mater to the underlying pia mater. This web is the basis of the name arachnoid, which means “spiderlike.” The subarachnoid space is filled with cerebrospinal fluid (CSF) and it also contains the largest blood vessels that supply the brain. Because the arachnoid is fine and elastic, these vessels are rather poorly protected.
Arachnoid cysts appear on the arachnoid membrane, and they may also expand into the space between the pia mater and arachnoid membranes (subarachnoid space).
Cerebrospinal fluid (CSF) is a watery broth that fills the subarachnoid space and the central hollow cavities of the brain and spinal cord. Cerebrospinal fluid (CSF) aids in protecting and nourishing the neural tissue.
- Cerebrospinal fluid (CSF) a liquid medium that surrounds and gives buoyancy to the central nervous system. The brain and spinal cord actually float in the cerebrospinal fluid (CSF), which prevents these delicate organs from being crushed under their own weight.
- The layer of cerebrospinal fluid (CSF) surrounding the central nervous system resists compressive forces and cushions the brain and spinal cord from blows and jolts.
- Cerebrospinal fluid (CSF) helps to nourish the brain, to remove wastes produced by neurons, and to carry chemical signals such as hormones between different parts of the central nervous system. Although similar in composition to the blood plasma from which it arises, cerebrospinal fluid (CSF) contains more sodium and chloride ions and less protein.
Amazingly, very little CSF is needed to perform these functions: only 100–160 ml, about half a cup, is present at any time. Cerebrospinal fluid (CSF) is produced in the ventricles of the brain, circulates through the hollow central cavities of the central nervous system (the spinal cord and brain) and the subarachnoid space, and is reabsorbed back into the blood in the dural venous sinuses (see Figure 5).
- Primary arachnoid cysts are present at birth (congenital) and are the result of developmental abnormalities in the brain and spinal cord that arise during the early weeks of gestation. Primary arachnoid cysts are the most common type of brain cyst. They are congenital lesions that occur as a result of the splitting of the arachnoid membrane.
- Secondary arachnoid cysts are not as common as primary cysts and develop as a result of head injury, meningitis, or tumors or as a complication of brain surgery.
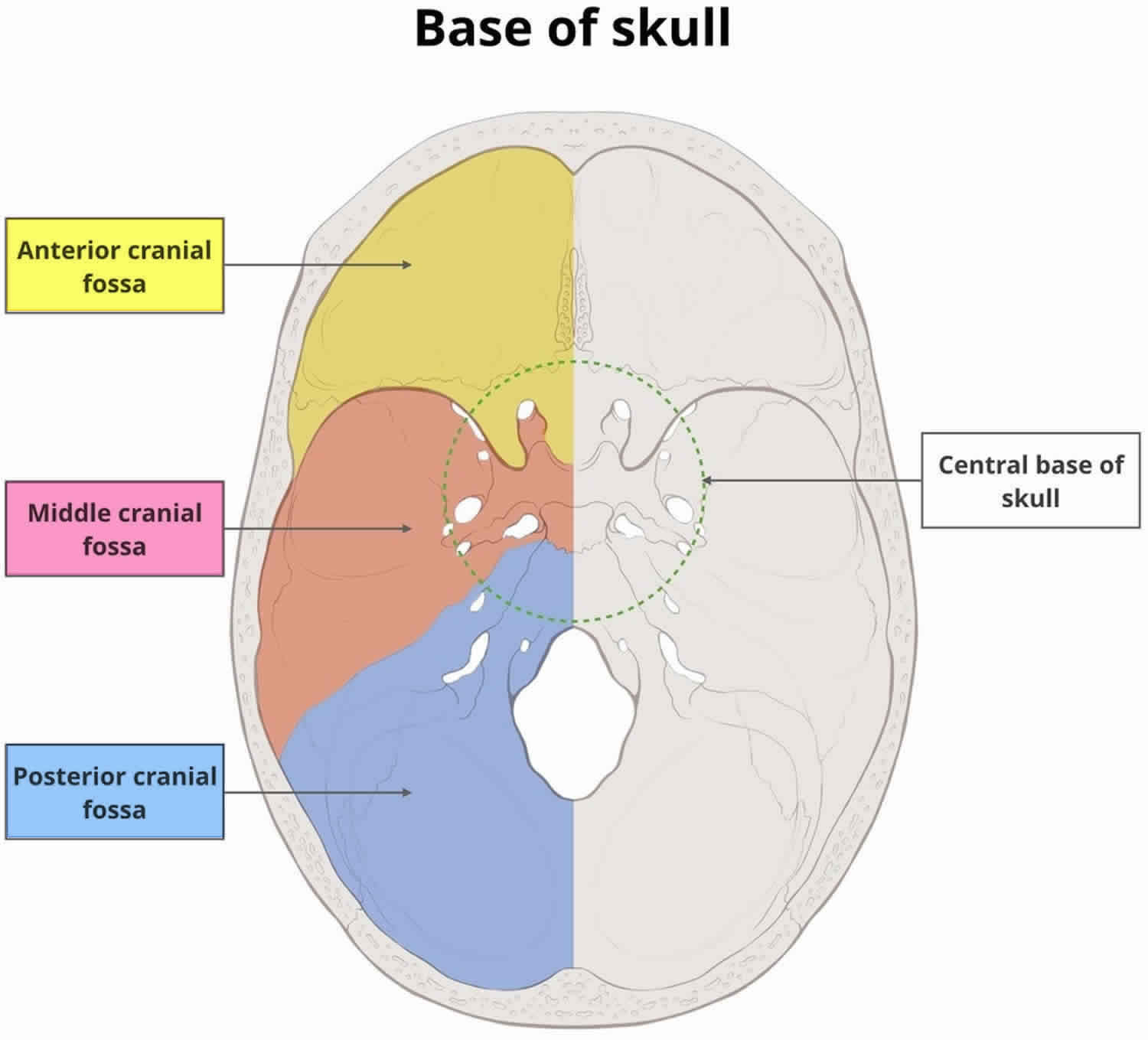
Arachnoid cysts are classified according to their specific location. The most common locations for intracranial arachnoid cysts are the middle cranial fossa (near the temporal lobe) (50-60%), the suprasellar region (near the third ventricle) and the posterior fossa, which contains the cerebellum, pons, and medulla oblongata. Arachnoid cysts involving the spinal cord are rarer. In many cases, arachnoid cysts do not cause symptoms (asymptomatic). In cases in which symptoms occur, headaches, seizures and abnormal accumulation of excessive cerebrospinal fluid in the brain (hydrocephalus) are common.
The location and size of the cyst determine the symptoms and when those symptoms begin. Most individuals with arachnoid cysts develop symptoms before the age of 20, and especially during the first year of life, but some people with arachnoid cysts don’t develop symptoms. Males are four times more likely to have arachnoid cysts than females.
Typical symptoms of an arachnoid cyst around the brain include headache, nausea and vomiting, seizures, hearing and visual disturbances, vertigo, and difficulties with balance and walking. Arachnoid cysts around the spinal cord compress the spinal cord or nerve roots and cause symptoms such as progressive back and leg pain and tingling or numbness in the legs or arms. Diagnosis usually involves a brain scan or spine scan using diffusion-weighted MRI (magnetic resonance imaging) which helps distinguish fluid-filled arachnoid cysts from other types of cysts.
There has been active debate about how to treat arachnoid cysts. The need for treatment depends mostly upon the location and size of the cyst. If the cyst is small, not disturbing surrounding tissue, and not causing symptoms, some doctors will refrain from treatment. In the past, doctors placed shunts in the cyst to drain its fluid. Now with microneurosurgical techniques and endoscopic tools that allow for minimally invasive surgery, more doctors are opting to surgically remove the membranes of the cyst or open the cyst so its fluid can drain into the cerebrospinal fluid and be absorbed.
Untreated, arachnoid cysts may cause permanent severe neurological damage when progressive expansion of the cyst(s) or bleeding into the cyst injures the brain or spinal cord. Symptoms usually resolve or improve with treatment.
Figure 1. Meninges of the brain
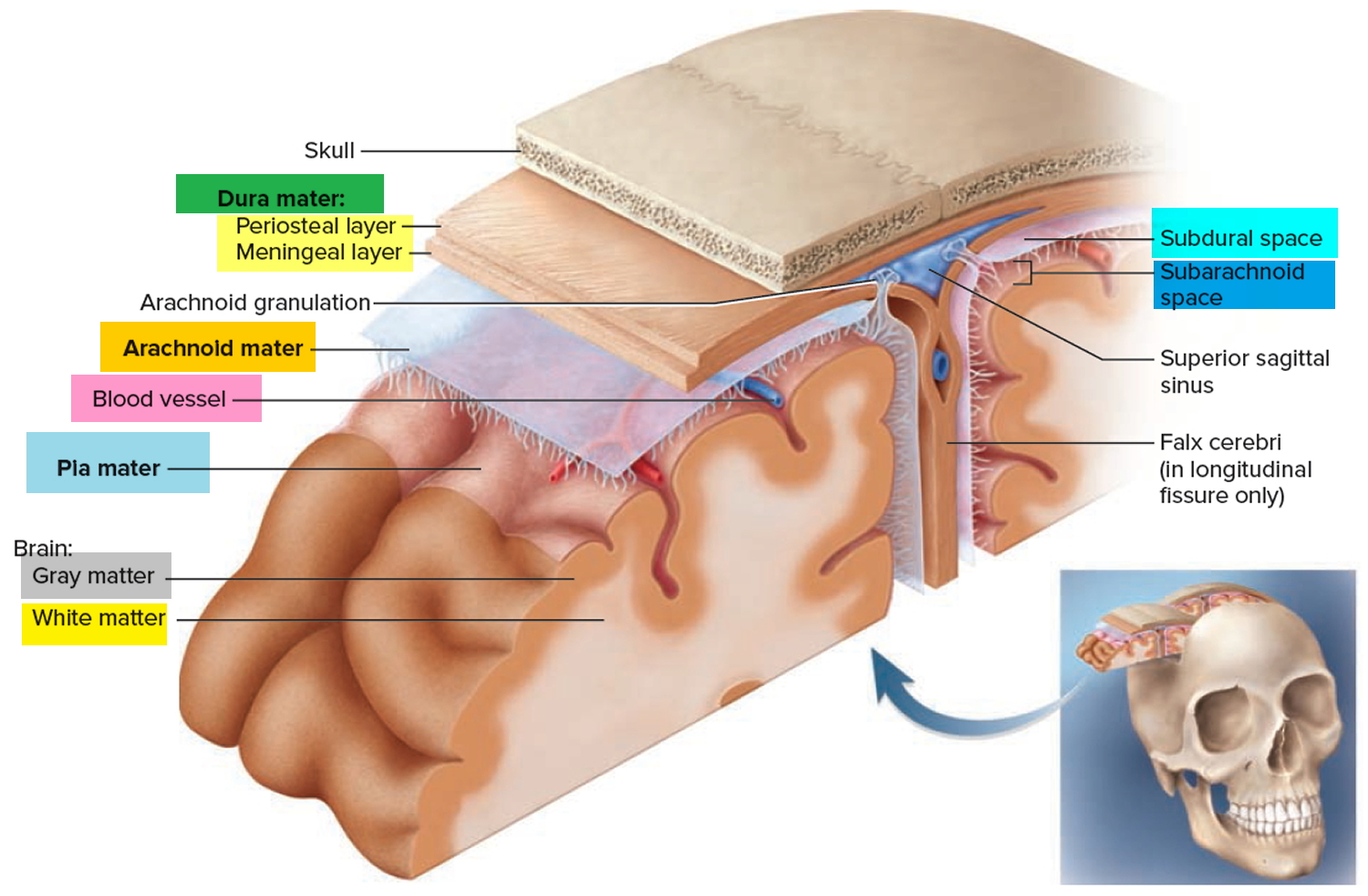
Figure 2. Meninges of the spinal cord
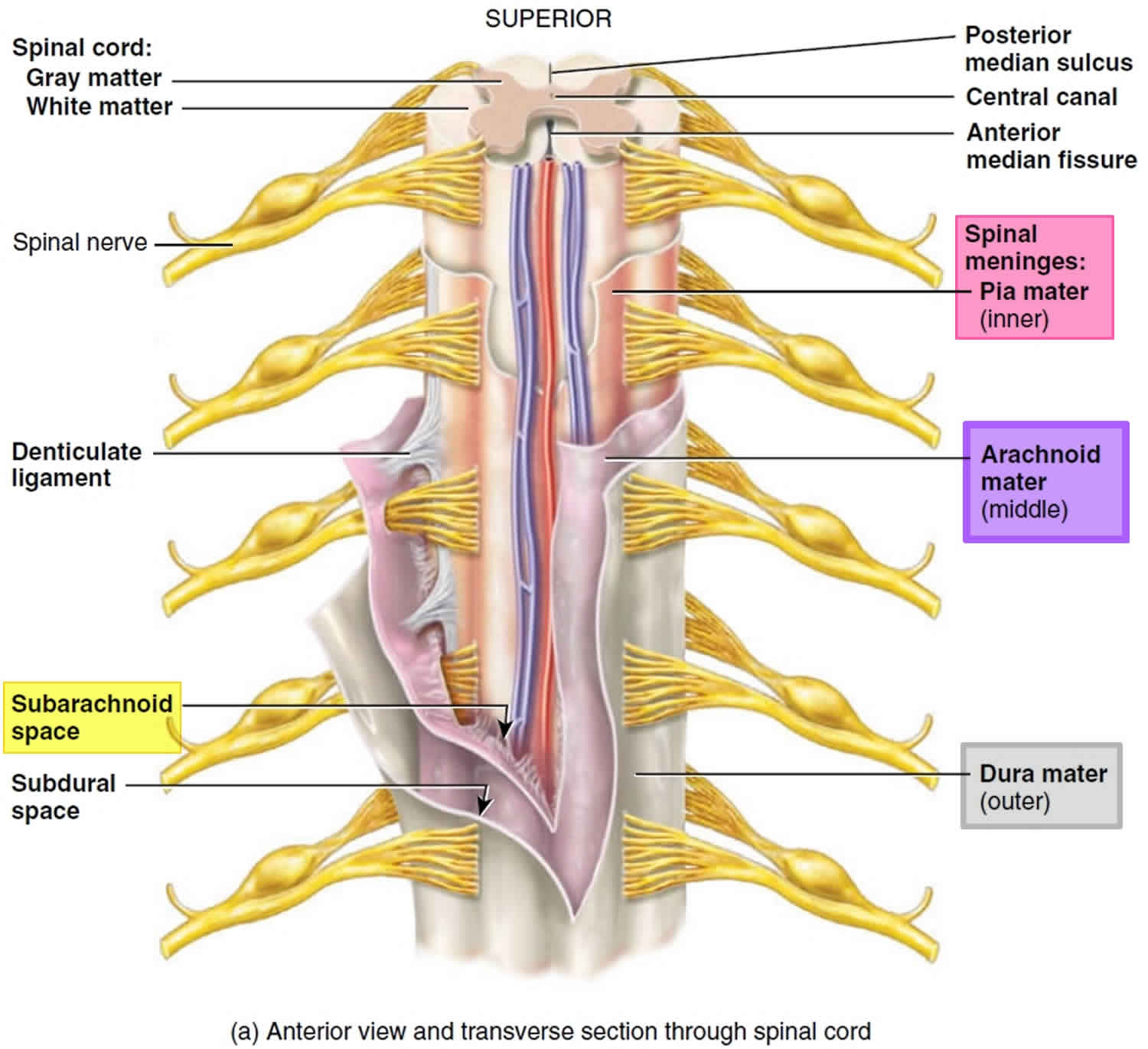
Figure 3. Human brain
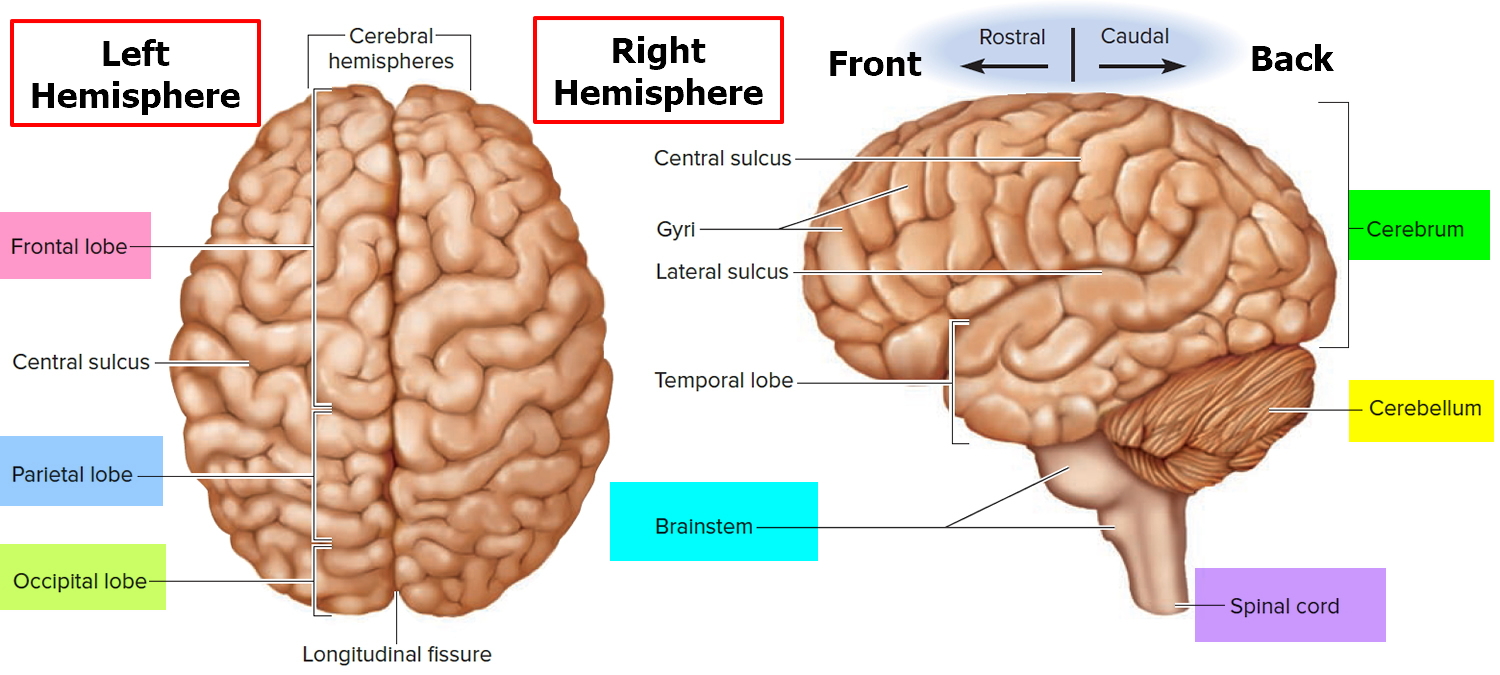
Figure 4. Spinal cord
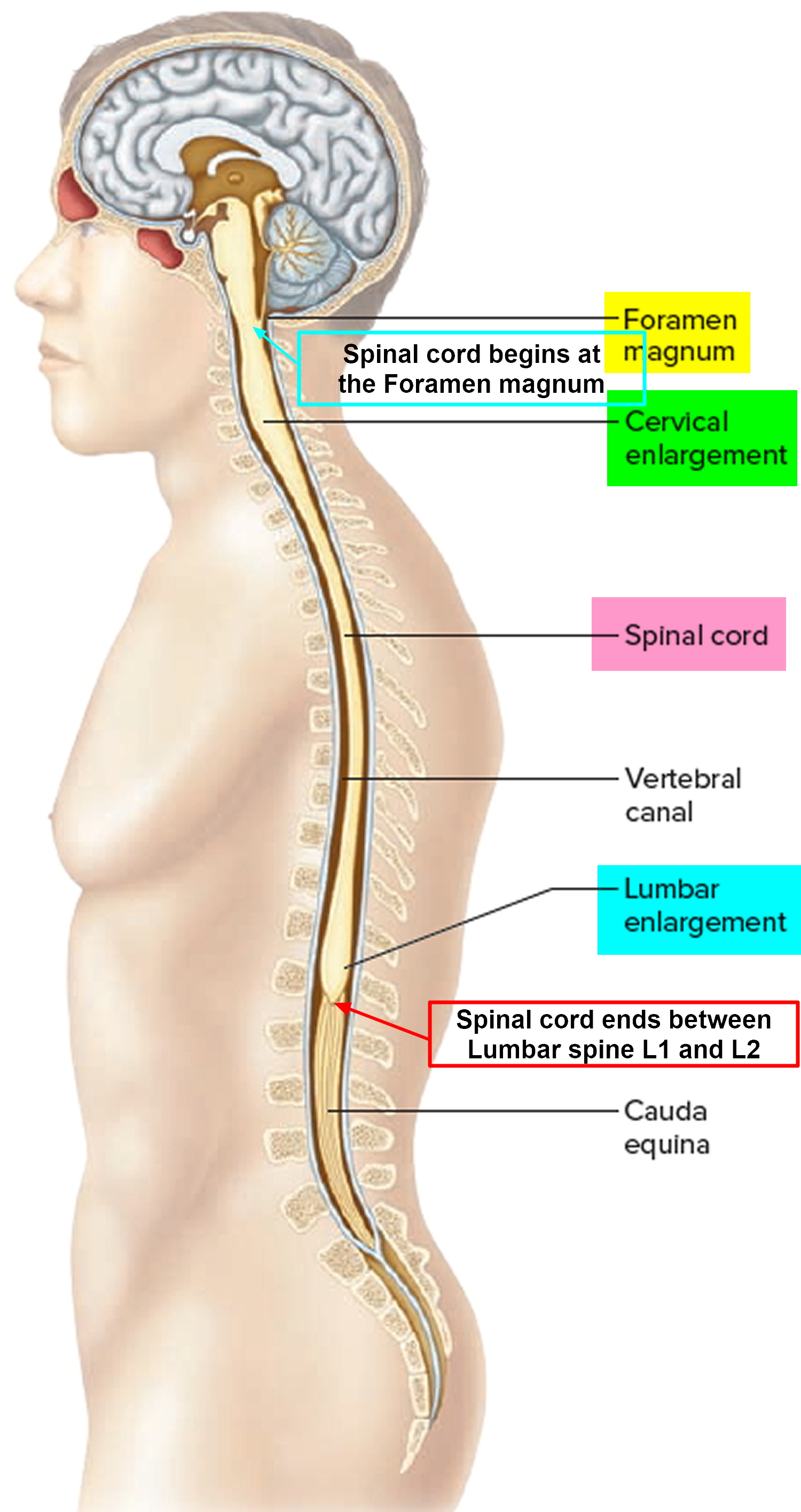
Figure 5. Cerebrospinal fluid formation, absorption and circulation around and within the brain
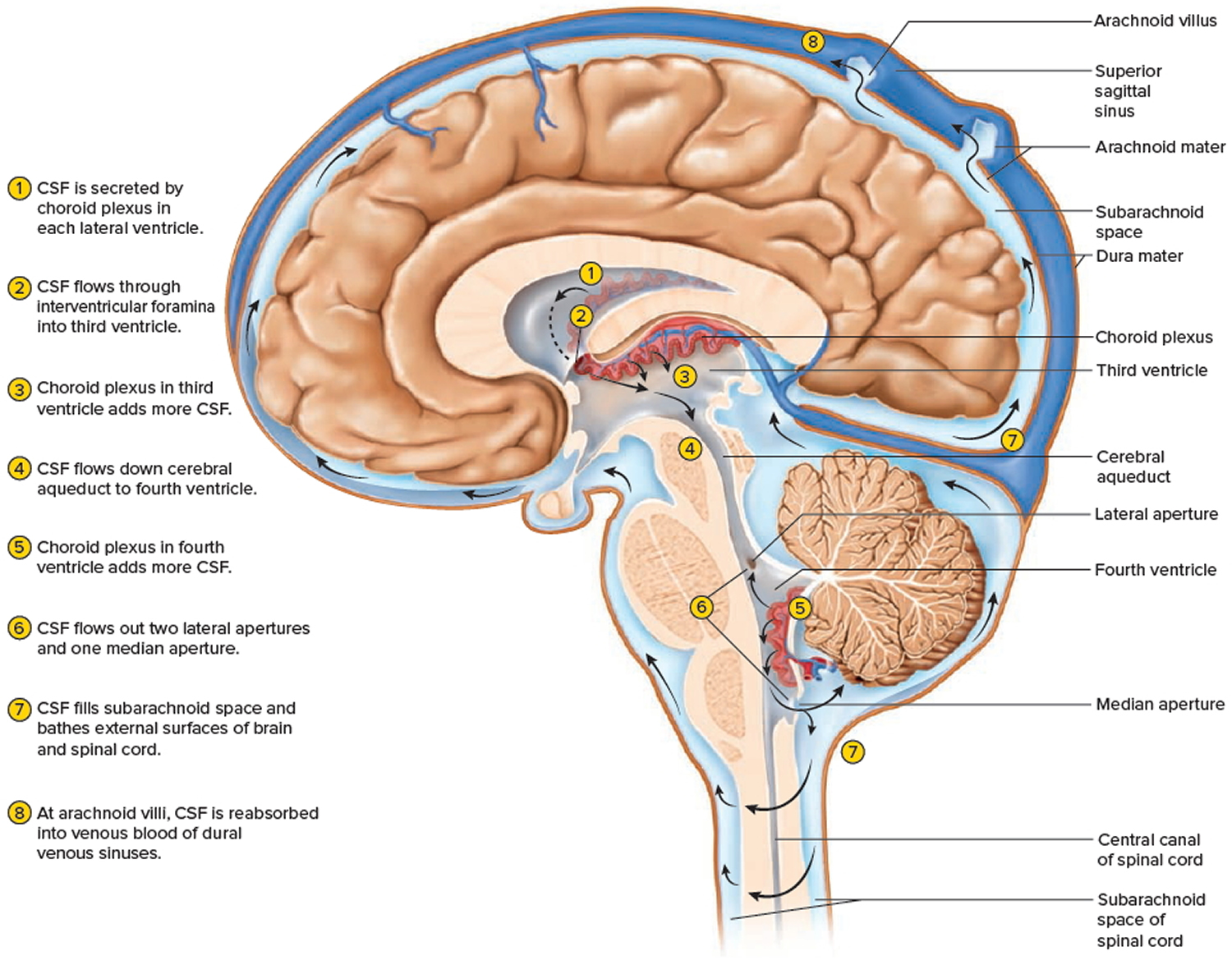 Figure 6. Middle cranial fossa
Figure 6. Middle cranial fossa
What is known about the long-term outlook associated with arachnoid cysts diagnosed prenatally?
Factors that reportedly seem to influence the prognosis for a fetus with an arachnoid cyst include the size (and whether it is growing), gestational age at the diagnosis, and the location of the cyst. Small cysts are usually asymptomatic. Interhemispheric cysts (those that extend between the 2 hemispheres) are often associated with complete or partial agenesis of the corpus callosum and carry a risk of causing intellectual disability. Brain compression by a large cyst may lead to hydrocephalus and may cause seizures, headache, and neurological signs after birth. The neurological prognosis often depends on the possibility of surgical treatment 3.
In a study of 54 fetuses with arachnoid cysts diagnosed in the second and third trimesters of pregnancy, a good prognosis was reported in 88% of the cases in terms of behavior, neurological development, and intelligence at 4 years of age. Several pregnancies were terminated because they were associated with other brain abnormalities. Some reports describe complete resolution of the cysts and that cysts rarely progress after birth 3.
A fetal MRI can help physicians to see and monitor compression of the aqueduct, communication between the cyst and the ventricles, and corpus callosum abnormalities 4. Because arachnoid cysts have a somewhat uncertain prognosis, knowing what to do when learning about an arachnoid cyst during pregnancy can be difficult. Some individuals may consider termination of pregnancy due to the uncertainty of the prognosis 3.
Individuals who have learned that an arachnoid cyst has been diagnosed during the pregnancy should consider meeting with a genetic counselor. A genetic counselor can interpret information about the condition, review available options, and provide supportive counseling to individuals and their family members.
Arachnoid cyst symptoms
In most cases, arachnoid cysts are present at birth (congenital), but usually do not cause any symptoms (asymptomatic) throughout an individual’s life. Less often, arachnoid cysts may develop because of head injury, the presence of a tumor, infection or surgery on the brain
Whether symptoms develop depends upon the size and the specific location of the cyst within the brain. Small arachnoid cysts usually do not cause symptoms. However, arachnoid cysts can increase in size causing symptoms to appear, especially if they press against a cranial nerve, the brain, or the spinal cord.
Most cases of arachnoid cysts that are associated with symptoms occur in childhood. The specific symptoms present vary from case to case. It is important to note that affected individuals will not have all of the symptoms listed below.
The most common symptoms associated with arachnoid cysts are usually nonspecific and include headaches, nausea, vomiting, dizziness and the accumulation of excessive cerebrospinal fluid in the brain (hydrocephalus), resulting in increased intracranial pressure In rare cases, in some children, an arachnoid cyst can cause malformation of certain cranial bones, resulting in an abnormally enlarged head (macrocephaly).
A variety of additional symptoms occur in some individuals with arachnoid cysts depending upon the size and location of the cyst. Most arachnoid cysts occur near the middle cranial fossa region of the brain. Such symptoms include lethargy, seizures, vision abnormalities and hearing abnormalities. Neurological signs may be present because arachnoid cysts may cause increased pressure on structures of the brain. Such neurological findings may include developmental delays, behavioral changes, an inability to control voluntary movements (ataxia), difficulties with balance and walking and cognitive impairment. Weakness or paralysis on one side of the body (hemiparesis) has also been reported.
In addition to hydrocephalus, cysts located in the suprasellar region may be associated with vision disturbances, continuous bobbing of the head, and abnormalities affecting certain hormone-producing glands that help to regulate the rate of growth, sexual development, and certain metabolic functions (endocrine system).
Other symptoms and physical findings have been reported to be associated with arachnoid cysts including migraine headaches, attention-deficit disorder and difficulties understanding or expressing language (aphasia). The exact cause and effect relationship between these findings and arachnoid cysts is not clear.
Specific symptoms depend on the location of arachnoid cyst, but can include:
- headache
- memory loss
- hearing loss or impairment
- nausea/vomiting
- ataxia (lack of muscle control)
- hemiparesis (weakness or paralysis on one side of the body)
- mass protrusion in the skull
- lethargy
- seizures
- behavioral changes
- increased intracrainal pressure
- educational problems due to location of the cyst
- developmental delay
- hydrocephalus due to obstruction of normal cerebrospinal fluid (CSF)
- early onset of puberty
- visual impairment
- vertigo
- difficulties with balance and walking
- dizziness
- sensitivity to heat and light
- emotional symptoms may include depression and anxiety
Although they occur much less often than those found within the skull (intracranial), arachnoid cysts may also arise near the spine (spinal arachnoid cysts). Spinal arachnoid cysts may compress the spinal cord or nerve roots and cause symptoms such as progressive weakness of the legs, tingling or numbness in the hands or feet, abnormal side-to-side curvature of the spine (scoliosis), back pain, and involuntary muscle spasms (spasticity) that result in slow, stiff movements of the legs. In rare cases, these cysts may cause paralysis of the legs (paraplegia). Urinary tract infections may also occur in individuals with spinal arachnoid cysts.
Some locations deserve special mention and separate discussion:
- suprasellar cistern (see suprasellar arachnoid cyst)
- within the ventricles (see intraventricular arachnoid cyst)
- posterior cranial fossa
- cisterna magna
- cerebellopontine angle
- spinal canal (see spinal arachnoid cysts)
Suprasellar arachnoid cyst
Suprasellar arachnoid cysts can be challenging to diagnose and, unlike many other arachnoid cysts, are usually symptomatic.
As can be expected from its location, suprasellar arachnoid cysts manifest clinically in the same way as other suprasellar masses, with visual symptoms due to compression and distortion of the optic pathways. Often these lesions extend superiorly, invaginating into the third ventricle and obstruct the outflow of the lateral ventricles, resulting in obstructive hydrocephalus 5.
Distortion of the pituitary infundibulum can also cause endocrine dysfunction 6.
Current treatment of choice is to perform an endoscopic third ventriculostomy and creation of a communication between the third ventricle, cyst and basal cisterns, simultaneously treating the obstructive hydrocephalus and resolving the mass effect of the cyst itself 7.
Intraventricular arachnoid cyst
Intraventricular simple cysts, frequently referred to as intraventricular arachnoid cysts, are rare and usually asymptomatic. They represent an uncommon cause of an intraventricular cystic lesion.
It is important to realize (although this is of little clinical importance) that the term intraventricular arachnoid cyst is used as a blanket term for a number of cysts which share identical imaging and operative features but are histologically distinct. Some are indeed a type of arachnoid cyst whereas others are lined other tissue and are in fact ependymal cysts, neuroepithelial cysts or very large choroid plexus cysts 8.
Like arachnoid cysts elsewhere, they may be asymptomatic and discovered incidentally. When a cyst becomes symptomatic, the patient may present with headache, signs and symptoms of obstructive hydrocephalus, focal neurology or seizures 9.
Intraventricular arachnoid cysts are non-neoplastic, benign and usually asymptomatic. If large and/or thought to be symptomatic, these cysts can be fenestrated endoscopically 10.
Posterior fossa arachnoid cyst
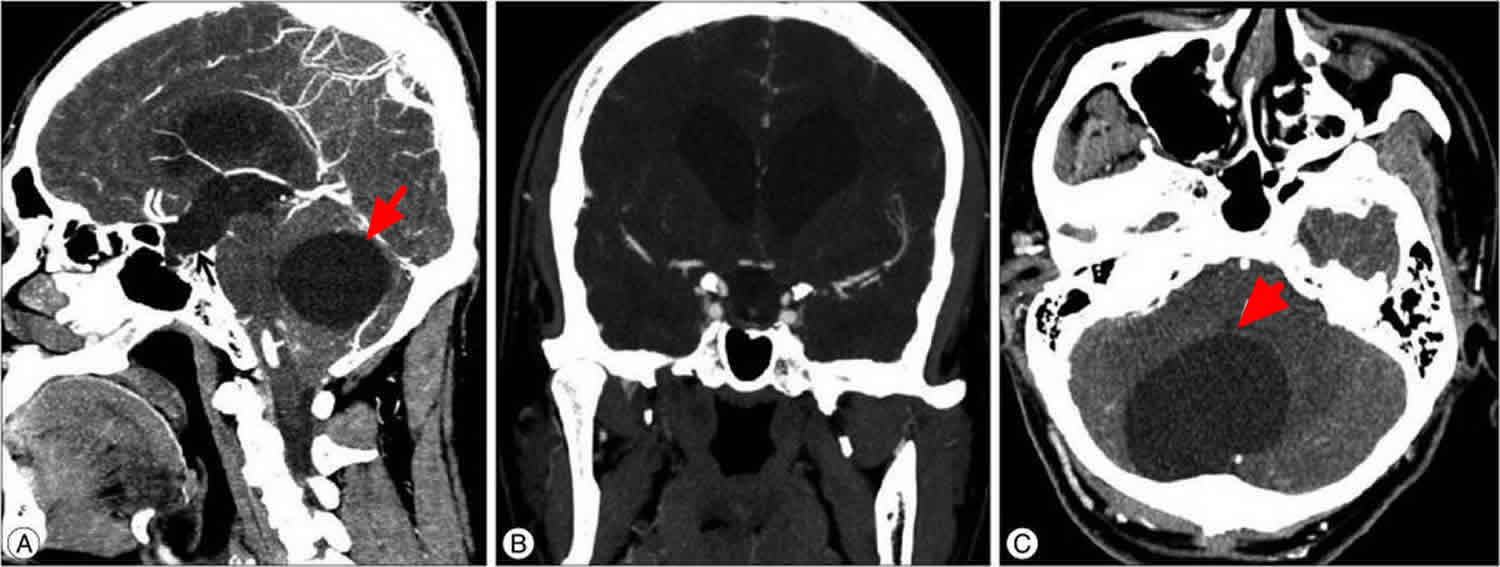
Posterior fossa is a site next to the middle fossa where arachnoid cyst frequently occurs (see Figures 6 and 7). Generally, most arachnoid cysts are asymptomatic and are found incidentally in most cases. Although arachnoid cysts are benign and asymptomatic lesions, patients with posterior fossa arachnoid cysts often complain of headaches, gait disturbance, and ataxia due to the local mass effects on the cerebellum. Common features of posterior fossa arachnoid cysts are secondary cerebellar tonsillar herniation with syringomyelia due to mass effect, and the lesions cross most areas of the foramen magnum. It is very rare that a foramen magnum arachnoid cyst directly compresses the spinal cord and develops syringomyelia 11. Posterior fossa arachnoid cyst usually occupies the cerebellopontine angle, a condition from which most experience in its treatment has been obtained. For example, Samii et al. 12 in 1999 reported 12 cases of posterior fossa arachnoid cyst which extended into the cerebellopontine angle. Prognosis in most cases was good after excision of the cysts.
The patients with posterior fossa arachnoid cysts usually do not complain of visual symptoms, as the cyst is not adjacent to the optic nerves. However, a posterior fossa arachnoid cyst can indirectly disrupt the CSF flows and, in turn, the disruption increases the whole ventricle size and the increased intracranial pressure.
Arachnoid cysts can be managed with a variety of procedures including foramen magnum decompression, with or without cyst removal, cysto-peritoneal shunting or endoscopic cyst fenestration 13. As in the present case, posterior fossa decompression and cyst excision result in a good outcome 11.
Figure 7. Posterior fossa arachnoid cyst
Spinal arachnoid cyst
Spinal arachnoid cysts are relatively uncommon and may be either intradural (type III meningeal cyst) or extradural (type IA meningeal cyst) 14. Spinal arachnoid cysts may present at any age. There is no gender predilection.
Most spinal arachnoid cysts are asymptomatic and are discovered incidentally. Clinical symptoms, if present, may include pain, weakness, numbness, and/or bladder/bowel incontinence. Symptoms may be exacerbated by postural changes and the Valsalva maneuver.
As with any arachnoid cyst, spinal arachnoid cysts are CSF-filled sacs contained by the arachnoid mater. The degree of communication with the surrounding CSF space is variable with some cysts freely communicating and others not at all 15.
Spinal arachnoid cysts may be congenital or acquired. Secondary arachnoid cysts are usually due to trauma, hemorrhage, inflammation, surgery or lumbar puncture 16.
Spinal arachnoid cysts associations
Location
Most primary intradural spinal arachnoid cysts are dorsal to the cord 18. They occur at the following locations:
- thoracic: 80%
- cervical: 15%
- lumbar: 5%
Secondary spinal arachnoid cysts can be located anywhere, depending on where the insult has occurred.
Incidental asymptomatic cysts are managed conservatively. Symptomatic cysts can be treated with surgical excision. An important component of surgical treatment of epidural cysts includes closure of the arachnoid defect, if any, which could become a source of CSF leak.
Figure 8. Spinal arachnoid cyst

Footnote: Sagittal image shows that the spinal arachnoid cyst extends from T1 to T5 vertebrae and compresses the spinal cord of a 9-year-old Chinese boy who presented with a two-week history of progressive paraparesis and gait ataxia.
[Source 19 ]Arachnoid cyst causes
The exact cause of arachnoid cysts is not known. Researchers believe that most cases of arachnoid cysts are developmental malformations that arise from the unexplained splitting or tearing of the arachnoid membrane. According to the medical literature, cases of arachnoid cysts have run in families (familial cases) suggesting that a genetic predisposition may play a role in the development of arachnoid cysts in some individuals.
In some cases, arachnoid cysts occurring in the middle fossa are accompanied by underdevelopment (hypoplasia) or compression of the temporal lobe. The exact role that temporal lobe abnormalities play in the development of middle fossa arachnoid cysts is unknown.
Some complications of arachnoid cysts can occur when a cyst is damaged because of minor head trauma. Trauma can cause the fluid within a cyst to leak into other areas (e.g., subarachnoid space). Blood vessels on the surface of a cyst may tear and bleed into the cyst (intracystic hemorrhage), increasing its size. If a blood vessel bleeds on the outside of a cyst, a collection of blood (hematoma) may result. In the cases of intracystic hemorrhage and hematoma, the individual may have symptoms of increased pressure within the cranium and signs of compression of nearby nerve (neural) tissue.
In some cases, arachnoid cysts are part of a genetic syndrome such as Chudley-McCullough syndrome, mucopolysaccharidosis, arachnoiditis, agenesis of the corpus callosum or Marfan syndrome, where there are many other associated signs and symptoms 20.
Affected populations
Arachnoid cysts affect males more often than females. These cysts may occur at any age and have been found in all races and geographic locations. They are the most common type of intracranial arachnoid cyst. Because many cases of arachnoid cysts have no symptoms, it is difficult to determine the true frequency of this disorder in the general population.
Arachnoid cyst diagnosis
A diagnosis of arachnoid cysts is often made incidentally, often during examination of an individual with seizures. A diagnosis may be suspected based upon a detailed patient history, a thorough clinical examination, and a variety of specialized tests, especially advanced imaging studies such as computed tomography (CT scan) and magnetic resonance imaging (MRI). CT scans and MRIs can reveal or confirm the presence of arachnoid cysts. During CT scanning, a computer and x-rays are used to create a film showing cross-sectional images of the brain’s tissue structure. During MRI, a magnetic field and radio waves are used to create cross-sectional images of the brain.
Arachnoid cyst treatment
Most arachnoid cysts are found incidentally and remain constant in size, leading many physicians to recommend conservative treatment. When no symptoms are present, no treatment may be necessary and affected individuals may be periodically monitored. If symptoms arise, a cyst can be reevaluated.
When treatment is necessary the specific therapy used depends upon whether symptoms are present, the size of the cyst and the specific location of the cyst within the skull.
In cases where treatment is recommended, therapy traditionally consists of one of two procedures – an open craniotomy fenestration or ventriculoperitoneal shunting.
During a craniotomy fenestration, a portion of the skull is removed to give a surgeon access to the cyst, where multiple openings are made in the cyst wall, (fenestrations), to allow cerebrospinal fluid to drain into the subarachnoid space where the fluid is reabsorbed into the surrounding tissue. Alternatively, some cases may be treated by surgically inserting a device (shunt) into the cyst to provide drainage either into the ventricular system of the brain or into the abdominal cavity. This will drain the cyst and provide an adequate passageway for cerebrospinal fluid to circulate.
More recently, advancements in minimally invasive brain and skull base surgery have evolved these traditional procedures into fully endoscopic techniques, distinguished by shorter operating times, fewer complications, excellent outcomes with faster recovery and overall decreased patient morbidity. While the approach varies depending on the size and location of the arachnoid cyst, fully endoscopic surgical management has provided the surgeon with superior access for either fenestration, or in other cases, resection of the cyst without the complications and risks associated with brain manipulation or retraction. Few facilities provide minimally invasive, endoscope assisted fenestrations, endoscopic shunt placement and endscope assisted or fully endoscopic resection of arachnoid cysts as treatment when indicated.
Spinal arachnoid cysts may be treated by the complete surgical removal (resection) of the cyst, if possible. Surgery generally leads to a resolution of symptoms. In some cases, complete surgical removal of a spinal cyst is not possible. In such cases, fenestration or shunting of the cyst to drain the fluid may be necessary.
Other treatment is symptomatic and supportive.
- Arachnoid Cysts. https://rarediseases.org/rare-diseases/arachnoid-cysts/[↩][↩][↩]
- Arachnoid cyst. https://radiopaedia.org/articles/arachnoid-cyst[↩]
- Bretelle, F, Senat MV, Bernard JP, Hillion Y, & Ville Y. First-trimester diagnosis of fetal arachnoid cyst: prenatal implication. Ultrasound Obstet Gynecol. 2002 Oct;20(4):400-2. https://obgyn.onlinelibrary.wiley.com/doi/pdf/10.1046/j.1469-0705.2002.00813.x[↩][↩][↩]
- Chen CP, Su YN, Weng SL, Tsai FJ, Chen CY, Liu YP, Chern SR, Chen WL, Wu PC, & Wang W.. Rapid aneuploidy diagnosis of trisomy 18 by array comparative genomic hybridization using uncultured amniocytes in a pregnancy with fetal arachnoid cyst detected in late second trimester. Taiwan J Obstet Gynecol. September 2012; 51(3):481-484. https://ac.els-cdn.com/S1028455912001507/1-s2.0-S1028455912001507-main.pdf?_tid=2546b7c4-65ee-47b1-85ca-7ce92a2f03ad&acdnat=1541419018_7ef9e82811d7f100d49d9cd4e1e57b84[↩]
- Kornienko VN, Pronin IN. Diagnostic Neuroradiology. Springer Verlag. (2008) ISBN:3540756523.[↩]
- Sansregret A, Ledoux R, Duplantis F et-al. Suprasellar subarachnoid cysts. Radioclinical features. Am J Roentgenol Radium Ther Nucl Med. 1969;105 (2): 291-7. Am J Roentgenol Radium Ther Nucl Med. 1969 Feb;105(2):291-7. https://www.ncbi.nlm.nih.gov/pubmed/5304736[↩]
- Mattox A, Choi JD, Leith-gray L et-al. Guidelines for the management of obstructive hydrocephalus from suprasellar-prepontine arachnoid cysts using endoscopic third ventriculocystocisternostomy. Surg Innov. 2010;17 (3): 206-16. doi:10.1177/1553350610377212 https://www.ncbi.nlm.nih.gov/pubmed/20688773[↩]
- Kaufman HH. Cerebrospinal Fluid Collections. Thieme. (1998) ISBN:1879284480.[↩]
- Okamura K, Watanabe M, Inoue N et-al. [Intraventricular arachnoid cyst–on the origin of intraventricular arachnoid cysts]. No To Shinkei. 1996;48 (11): 1015-21 https://www.ncbi.nlm.nih.gov/pubmed/8951893[↩]
- Xi-an Z, Songtao Q, Yuping P. Endoscopic treatment of intraventricular cerebrospinal fluid cysts: 10 consecutive cases. Minim Invasive Neurosurg. 2009;52 (4): 158-62. doi:10.1055/s-0029-1239587 https://www.ncbi.nlm.nih.gov/pubmed/19838968[↩]
- Huang H, Li Y, Xu K, Li Y, Qu L, Yu J. Foramen magnum arachnoid cyst induces compression of the spinal cord and syringomyelia: case report and literature review. Int J Med Sci. 2011;8(4):345-50. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3107467/[↩][↩]
- Arachnoid cysts of the posterior fossa. Samii M, Carvalho GA, Schuhmann MU, Matthies C. Surg Neurol. 1999 Apr; 51(4):376-82.[↩]
- Jain R, Sawlani V, Phadke R, Kumar R. Retrocerebellar arachnoid cyst with syringomyelia: A case report. Neurol India. 2000;48:81–3.[↩]
- Nabors MW, Pait TG, Byrd EB et-al. Updated assessment and current classification of spinal meningeal cysts. J. Neurosurg. 1988;68 (3): 366-77. doi:10.3171/jns.1988.68.3.0366 https://www.ncbi.nlm.nih.gov/pubmed/3343608[↩]
- Silbergleit R, Brunberg JA, Patel SC et-al. Imaging of spinal intradural arachnoid cysts: MRI, myelography and CT. Neuroradiology. 1998;40 (10): 664-8. Neuroradiology. 1998 Oct;40(10):664-8. https://www.ncbi.nlm.nih.gov/pubmed/9833898[↩]
- Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Lippincott Williams & Wilkins. (2007) ISBN:0781761352[↩]
- Rao ZX, Li J, Hang SQ, You C. Congenital spinal intradural arachnoid cyst associated with intrathoracic meningocele in a child. J Zhejiang Univ Sci B. 2010;11(6):429-32. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2880355[↩][↩]
- Intradural extramedullary cysts of the spinal canal: clinical presentation, radiographic diagnosis, and surgical management. Osenbach RK, Godersky JC, Traynelis VC, Schelper RD. Neurosurgery. 1992 Jan; 30(1):35-42.[↩]
- Rao ZX, Li J, Hang SQ, You C. Congenital spinal intradural arachnoid cyst associated with intrathoracic meningocele in a child. J Zhejiang Univ Sci B. 2010;11(6):429-32. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2880355/[↩]
- Khan AN. Arachnoid Cyst Imaging. https://emedicine.medscape.com/article/336489-overview[↩]





{kind=link}