
Contents
Are canned vegetables healthy
Canned foods are a core component of the diets of many Americans 1. A 2013 survey of more than 1000 Americans showed that greater than 60% of the respondents reported eating canned foods at least once or twice each week 2. Of those 80% of Americans who consumed canned foods, the average individual partook in approximately five canned food eating occasions in those two weeks, or, roughly one canned food every three days. Many Americans use canned foods for their cost and/or convenience; and not for their nutritional properties 2. Results from the National Health and Nutrition Examination Survey 2001-2010 3 suggest canned fruit and canned vegetables consumption was associated with higher intake of select nutrients, a higher-quality diet, and comparable adiposity (obesity) measures and blood pressure. However, in general, fresh fruits and vegetables are recommended as the primary nutrient-dense dietary options, because fresh produce picked at peak maturity offers the highest amount of vitamins and minerals and tastes the best, but soon after harvest these nutrients degrade. It can take 1-2 weeks for produce to be transported from farms to supermarkets and then purchased by the consumer. Several more days may pass before you actually eat it. Part of the nutrient losses occur with moisture loss if water-rich produce sits at room temperature. Estimates show that at room temperature, fresh peas lose about 50% of vitamin C in one week, and fresh spinach can lose 100% of the vitamin in less than 4 days 4. Asparagus loses about 30% of vitamin C during canning but only 10% after blanching and freezing. The takeaway message is, unless fruits and vegetables are eaten immediately after harvesting, there is going to be nutrient loss to some degree. Regardless of losses, fruits and vegetables remain a valuable source of a variety of nutrients. In certain cases, frozen or canned produce may contain higher levels of nutrients than fresh produce that has been stored for too long. To obtain the most nutrients, consume fresh produce within a few days, or frozen varieties within a few weeks. When choosing canned or frozen produce, select options that do not include extra sodium, sugar, or other additives. Refrigeration can slow degradation, but even so, certain highly perishable fruits like berries only last about a week before visible changes in color, texture, and flavor set in. Apples, pears, and squashes are less sensitive and can last for 1-2 months with refrigeration. Generally, the freezing process averages about 50% loss of vitamin C (range 10-90%), and canning treatment causes average losses greater than 60% (range 8-90%) 4. The ranges are wide depending on the exact processing treatment, storage conditions, and type of produce. But regardless of losses during processing, some or many of the nutrients are retained, which upon storage are further preserved through protection from oxygen, heat, and light. Broccoli retains almost 100% of vitamin C after freezing.
For longer storage, canning and freezing can preserve nutrients more effectively than refrigeration. Initially some nutrients are lost during processing. For example, canning uses heat treatment or other methods to destroy bacteria, followed by storage in a liquid medium in an airtight container; freezing entails a prior step of blanching the produce quickly to deactivate enzymes that speed ripening. In both cases, some water-soluble vitamins like C and B may be destroyed or leached into the cooking or storage liquid. Home cooking of fresh or processed produce will also cause additional losses due to nutrients destroyed by heat or seeping into the cooking water. Microwave cooking and steaming as opposed to boiling and deep-frying preserves the most nutrients due to quicker cooking times and reduced contact with water.
However, fresh foods are not always available to all Americans due to seasonal, economic and geographic factors. Recent research has shown that canned options contain comparable nutrient profiles to fresh foods 5, 6, 7, 8, therefore nutrient-dense canned foods should be considered as healthy options alongside fresh foods, or as nutritious alternatives to fresh foods. Additionally, a study by Kapica et al. 6, provided evidence that canned foods are some of the most cost-effective and accessible nutrient options available to Americans. Furthermore, the 2015 Dietary Guidelines for Americans 9 promotes nutrient-dense canned foods such as vegetables, fruits, legumes and seafood (especially those which are low in salt and sugar) along with fresh and frozen options to meet the recommended dietary intakes for food groups and nutrient levels.
In 2012, Durst and Weaver 10 provided evidence that the canning and storage process can increase the content of certain nutrients and antioxidant function in peaches after 3 months. This phenomenon likely occurs during processing in which the inactivation of degradation enzymes inhibits the breakdown of ascorbic acid and other antioxidants. The researchers 10 showed that vitamin C, folate and antioxidant levels as measured by ferric reducing antioxidant power assay were all higher when compared to fresh peaches. Importantly, the measurements showed that folate, vitamin C, and antioxidants levels were stable over the three months storage period in the canned peaches, and most alterations in nutrient content occurred during processing and not over the storage period. So, while the thermal treatment used in the canning process can result in the breakdown or transformation of some water-soluble vitamins, the remaining nutrients are much more stable over time compared to those in fresh or frozen products since there is less exposure to oxidation and microbial threats 11. Recent research has even shown that the thermal processing techniques used in the canning process may actually preserve or enhance some nutritional qualities in nutrient-dense foods such as canned beans, vegetables and fruits when compared to fresh foods 12.
Generally, fresh and canned foods contain similar quantities of most fat-soluble vitamins, minerals and fiber. Although, there is evidence that some nutrient and bioactive losses occur during the canning process, there is also evidence to the contrary, therefore it is important to recognize that the consumption of nutrient-dense canned foods are a viable and cost effective way to contribute to the overall nutritional quality of the diet 8. The canning process may even increase the bioavailable levels of certain carotenoids with the best known example being the increase in lycopene in processed tomato products 5. Additionally, processed tomatoes have higher β-carotene levels compared to fresh tomatoes, as do a variety of other fruits and vegetables which can range up to 50% higher than their fresh counterparts 13. Furthermore, the canning process has also been shown to improve the protein (>7%) and fiber (>5%) content of multiple bean varieties, while also reducing the quantity of lectins 14. While the canning process can improve the nutrient and bioactive levels of certain foods, it is also been shown to reduce the levels of certain nutrients in some foods as well 14. Therefore, the canning process likely affects all foods differently, and the changes in overall nutrient and bioactive profile cannot be fully extrapolated from the currently available body of science. Further research is needed on different canning processes, storage times, and the resultant nutrient and bioactive profiles of canned foods in order to better understand how these foods affect the overall nutritional intake of their consumers.
A 2012 study by Kapica et al. 6, provided evidence that canned foods, including vegetables, fruits, fish and beans actually provided nutrients at a lower or comparable cost compared to fresh, frozen or dried options, showing that cost-effective, accessible, and nutrient-dense food options can be available in some of the lowest income and highest food insecure areas in the US. While fresh produce and seafood are often perceived as some of the healthiest dietary options 2, the 2015 Dietary Guidelines for Americans 15 repetitively suggests that fresh, frozen and canned vegetables and fruits all count towards the Dietary Guidelines for Americans recommendations. Additionally, canned or tinned seafood such as albacore tuna, anchovies, sardines, and salmon are all rich sources of the omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), which are recommended by Dietary Guidelines for Americans, especially for pregnant and breastfeeding mothers 15. Canned seafood is also a source of three of the four Dietary Guidelines for Americans “nutrients of concern”: with canned sardines being a good source of calcium; canned salmon, sardines and tuna being good sources of vitamin D; and canned clams containing 542 mg of potassium per serving 15.
While potassium is designated as a “nutrient of concern” by the Dietary Guidelines for Americans because it is a shortfall nutrient in the US diet, sodium is considered a “nutrient of concern” of because it is generally over consumed in the US diet. The Dietary Guidelines for Americans aims to reduce dietary sodium intake in the US diet since excess amounts can negatively affect several chronic diseases such as hypertension, diabetes and kidney disease 15. Canned foods are often associated with sodium intake, but according to the Centers for Disease Control and Prevention (CDC), canned foods such as fruits and vegetables are not one of the top ten sources of sodium in the US diet 16. Additionally, nutrient-dense canned foods such as fruits, vegetables and legumes come in many low-sodium and sodium-free options. Moreover, studies have shown that simply rinsing off sodium-containing canned foods such as vegetables and beans can reduce sodium content by up to 41% 17.
Although canned foods are featured in grocery stores, and used in restaurant meals and government assistance programs, the frequency of canned food consumption in the US has been on a steady decline over the last 10 years with Annual Eatings per Capita rates decreasing by 7.5% from 2003 to 2013 18. The “eat rate” (i.e., the average number of times an individual consumes a product during a two-week period) for canned foods has also declined by 4% over the same time course 19. The misconceptions about the nutritional impact and healthfulness of canned foods, and their decreasing usage rate may both be contributing factors to the nutritional inadequacy of the American diet.
In a study of its kind, Comerford 18 compared the nutrition status frequent canned food users (FCU) and infrequent canned food users (ICU) over 2 years involving 4000 American households or 9761 individuals (> 400,000 eating occasions total). The final sample consisted of 5316 survey respondents—1165 children and adolescents between the ages of 2–17 years and 4151 adults (64% female, 36% male) over the age of 18 years. Depending on their consumption habits, canned food consumers were placed into three groups: Frequent Canned Food Users (FCU), Average Canned Food Users (ACU) and Infrequent Canned Food Users (ICU). Frequent Canned Food Users (FCU) were defined as those individuals who consumed canned foods six or more times in the two weeks study period, while Infrequent Canned Food Users (ICU) consumed canned foods 1–2 times over the two-week study period. Average Canned Food Users (ACU) consumed canned goods between three to five times during the two-week study period, and were not included in the final analysis. Two groups were singled out and dichotomized for further investigation and comparison of canned food consumption—infrequent users relative to frequent users. Additional analysis was performed to determine the overall and subcomponent diet quality on selected days. Specifically, to compare essential nutrient intake on days when canned foods were eaten versus days when canned foods were not eaten. The results of that study 18 indicated that more frequent canned food consumption is associated with healthier eating patterns, such as greater intake of several Dietary Guidelines for Americans recommended food groups and higher daily nutrient intakes. That study 18 provided evidence that frequent canned food consumers took in more nutrient-dense foods such as fruits, vegetables and legumes, when compared to infrequent canned food consumers (see Figure 4 below). The frequent canned food users (FCU) group also ingested significantly higher amounts of fiber and protein, and 17 different essential micronutrients over the two-week study period (see Table 2). These results are promising for consumers and parents who have often been hesitant to recognize canned foods as nutritionally robust options for meeting dietary requirements. However, the overall results regarding nutrient intakes for both the infrequent canned food users (ICU) and frequent canned food users (FCU) study groups—and for Americans in general—are still far from the ideal amounts recommended by the Dietary Guidelines for Americans 20.
The results from that study showed that the frequent canned food users (FCU) group consumed more sodium than the infrequent canned food users (ICU) group (see Table 2), however the frequent canned food users (FCU) group also consumed more potassium as well; and the difference in potassium intake between groups was greater than for sodium intake (~19% vs. ~12%, respectively). The sodium/potassium ratio was also 7% lower in the group which consumed canned foods more frequently [1.49 for infrequent canned food users (ICU) vs. 1.39 for frequent canned food users (FCU)]. The sodium/potassium ratio has been shown to be a more representative indicator of cardiovascular disease and hypertension risk than sodium intake levels alone 21, with increased potassium levels being shown to be able to diminish the negative effects of sodium on hypertension 22. Although high sodium intakes are epidemic in the US, they are not really an issue specific to canned foods, rather they are a ubiquitous part of the US food supply and American eating patterns as a whole.
Table 1. Demographics of frequent canned food users (FCU) and infrequent canned food users (ICU)
| Demographics | % Infrequent Can Users (ICU) | % Frequent Can Users (FCU) |
| Age (years) | ||
| 2–17 | 20.5 | 23.4 |
| 18–65 | 65.6 | 59.6 |
| 65 | 13.9 | 17 |
| BMI | ||
| Underweight | 4.2 | 3.8 |
| Optimal | 38.2 | 36.6 |
| Overweight | 28.7 | 32.1 |
| Obese | 28.8 | 27.4 |
| Household Income | ||
| Under $10,000 | 6.1 | 10 |
| $10,000–$19,999 | 7.8 | 11.8 |
| $20,000–$29,999 | 11.8 | 17.3 |
| $30,000–$39,999 | 13.9 | 14.3 |
| $40,000–$49,999 | 10.5 | 12.2 |
| $50,000–$59,999 | 9 | 5.7 |
| $60,000–$69,999 | 9.6 | 5.5 |
| $70,000 and Over | 31.2 | 23.2 |
Notes: Body Mass Index = BMI. Percentage of infrequent (n = 2732) and frequent (n = 2584) canned food users socio-demographic and anthropometric information. Data from the NPD Group’s National Eating Trends intake diary panel 2011–2013 and Nutrient Intake databases.
[Source 18]Figure 1. Average number of Fresh Foods eaten over a two-week period between Frequent and Infrequent Canned Food Users (FCU and ICU)
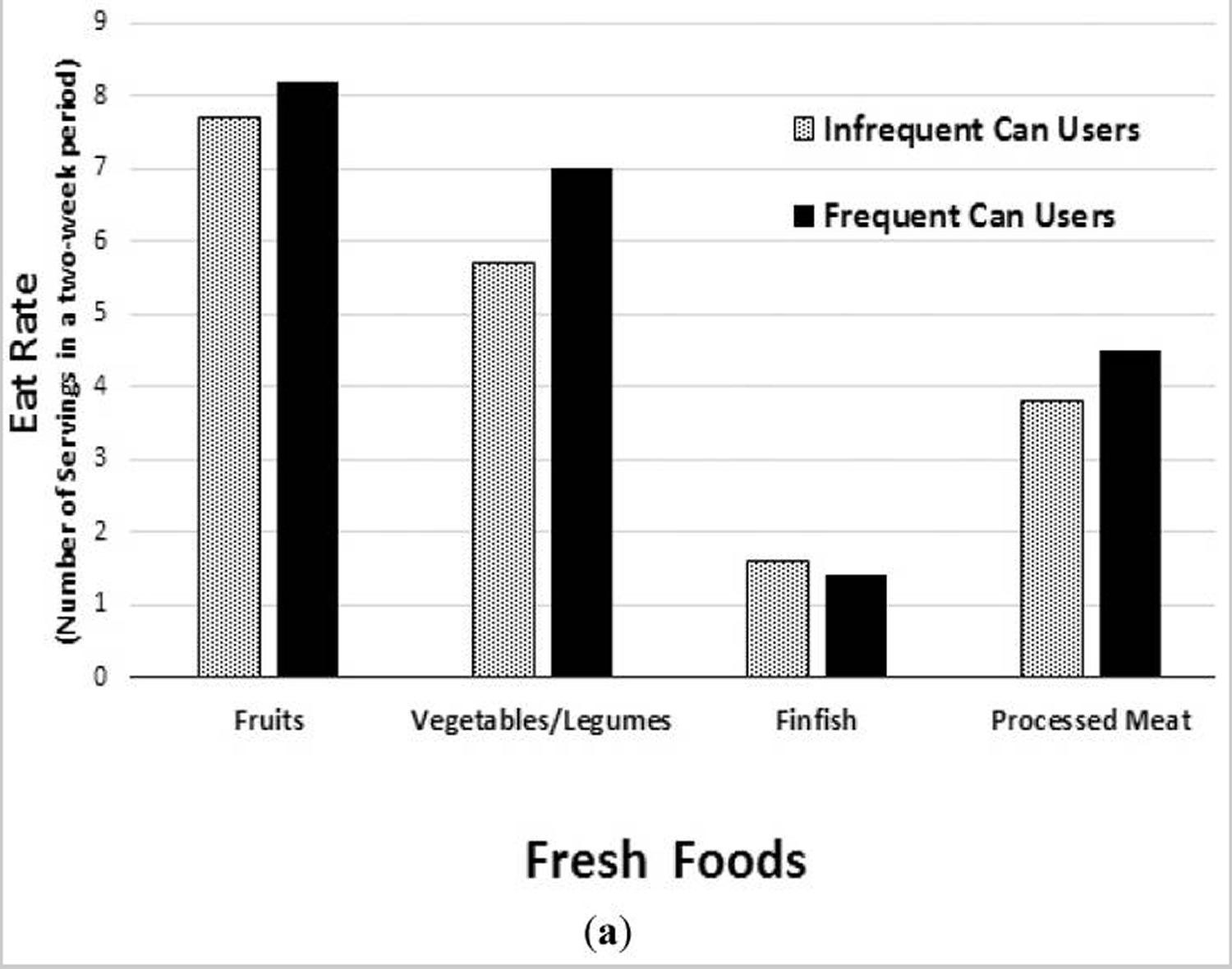
Notes: (a) Fresh Foods Eat Rate (i.e., average number of food category eating occasions over a two-week period) among Frequent and Infrequent Canned Food Users (FCU and ICU). Proportion of infrequent (n = 2732) and frequent (n = 2584) canned food users Eat Rate. Data from the NPD Group’s National Eating Trends® intake diary panel 2011–2013 and Nutrient Intake databases. Statistical confidence level set at 95% for two-tailed t test. p-Value < 0.025% considered significant. The FCU group had a significantly higher Eat Rate for all food groups listed, except for fresh fin fish, which was significantly higher in the ICU group
[Source 18]Table 2. Average number and types of Canned Foods eaten over a two-week period between Frequent and Infrequent Canned Food Users (FCU and ICU)
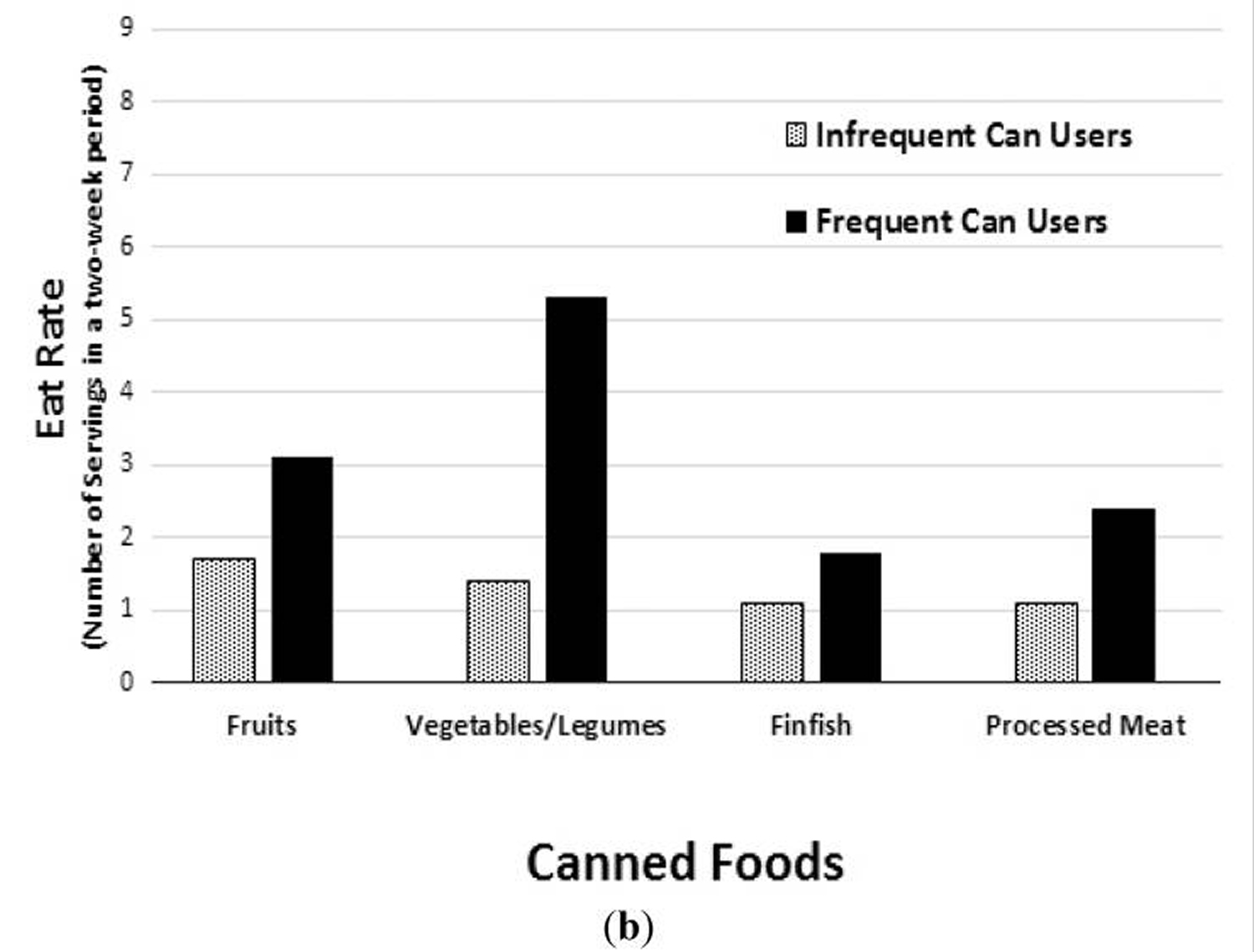
Notes: (b) Types of canned foods Eat Rate (i.e., average number of food category eating occasions over a two-week period) among Frequent and Infrequent Canned Food Users (FCU and ICU). Proportion of infrequent (n = 2732) and frequent (n = 2584) canned food users Eat Rate. Data from the NPD Group’s National Eating Trends® intake diary panel 2011–2013 and Nutrient Intake databases. Statistical confidence level set at 95% for two-tailed t test. p-Value < 0.025% considered significant. The FCU group had a significantly higher Eat Rate for all food groups listed, except for fresh fin fish, which was significantly higher in the ICU group
[Source 18]Nutrient Intake
The frequent canned food users (FCU) group took in significantly higher amounts of 18 essential nutrients and fibers as well, when compared to the infrequent canned food users (ICU) group (Table 2) 18. On average, the frequent canned food users (FCU) group took in approximately 3 g more fiber (~20% more), 154 mg more calcium (~16% more), 38 mg more magnesium (~16% more), 24 mg more vitamin C (~31% more), 147 µg more vitamin A (~22% more), and 49 µg more folate (~12% more) each day (Table 2). The frequent canned food users (FCU) group also took in an average of 454 mg more potassium (~19% more), and 420 mg more sodium (~12% more) per day than the infrequent canned food users (ICU) group (Table 2). As shown in Figure 3, the frequent canned food users (FCU) group met or exceeded the Recommended Dietary Allowance (RDA) for 16 different nutrients and fibers on significantly more days during the two-week study than the infrequent canned food users (ICU) group. Compared with the infrequent canned food users (ICU) group, the frequent canned food users (FCU) group had a significantly higher percentage of days meeting or exceeding the RDA for protein (85.8% vs. 90.5%, respectively), and fiber (3.1% vs. 7.7%, respectively). Compared to the infrequent canned food users (ICU) group, the frequent canned food users (FCU) group also had a higher percentage of days meeting or exceeding the RDA for the fat-soluble vitamins, vitamin A (31.8% vs. 45.7%, respectively), and vitamin E (4.1% vs. 7.6%, respectively). The frequent canned food users (FCU) group met or exceeded the RDA for seven water-soluble vitamins (vitamin C, thiamin, riboflavin, niacin, vitamin B6, folate, and vitamin B12). The RDA for three of the water-soluble vitamins (vitamin C, vitamin B6, and folate) was met or exceeded by an average of over 10% more often during the two-week study period by the frequent canned food users (FCU) group, when compared to the infrequent canned food users (ICU) group. Furthermore, the frequent canned food users (FCU) group met or exceeded the RDA for six minerals (calcium, magnesium, phosphorus, iron, zinc, and selenium), with the Recommended Dietary Allowance (RDA) for calcium, magnesium and zinc being met or exceeded by an average of over 9% more often during the two-week study period, compared to the infrequent canned food users (ICU) group.
Table 2. Average daily nutrient intake between frequent (FCU) and infrequent canned foods users (ICU)
| Nutrient | ICU | FCU |
| Fiber (g) | 13.1 ± 6.2 | 16.0 ± 7.4 |
| Protein (g) | 69.7 ± 26.7 | 76.3 ± 29.9 |
| Vitamin A (RAE) (µg) | 585 ± 417 | 732 ± 417 |
| Vitamin E (mg) | 6.1 ± 3.5 | 7.1 ± 4.0 |
| Vitamin C (mg) | 65.9 ± 64.6 | 89.7 ± 68.9 |
| Thiamin (mg) | 1.6 ± 0.7 | 1.8 ± 0.8 |
| Riboflavin (mg) | 1.9 ± 0.8 | 2.2 ± 0.9 |
| Niacin (mg) | 20.9 ± 8.9 | 23.2 ± 9.7 |
| Vitamin B6 (mg) | 1.6 ± 0.8 | 1.9 ± 0.9 |
| Folate/Folic Acid (µg) | 370 ± 188 | 419 ± 200 |
| Vitamin B12 (µg) | 4.8 ± 4.2 | 5.7 ± 5.2 |
| Calcium (mg) | 873 ± 417 | 1027 ± 493 |
| Magnesium (mg) | 219 ± 87 | 257 ± 101 |
| Phosphorus (mg) | 1178 ± 437 | 1331 ± 522 |
| Iron (mg) | 14.3 ± 7.1 | 16.4 ± 7.8 |
| Zinc (mg) | 10.4 ± 5.4 | 11.6 ± 5.8 |
| Selenium (µg) | 101 ± 44 | 108 ± 47 |
| Sodium (mg) | 3168 ± 1283 | 3588 ± 1482 |
| Potassium (mg) | 2132 ± 827 | 2586 ± 988 |
Notes: RAE = Retinol Activity Equivalents. Average nutrient intake (mean and standard deviation) of infrequent (n = 2732) and frequent (n = 2584) canned food users. Data from the NPD Group’s National Eating Trends® intake diary panel 2011–2013 and Nutrient Intake databases.
[Source 18]Figure 3. Percentage of days in which participants met or exceeded the Recommended Dietary Allowance (RDA) for different nutrients among Frequent and Infrequent Canned Food Users (FCU and ICU)
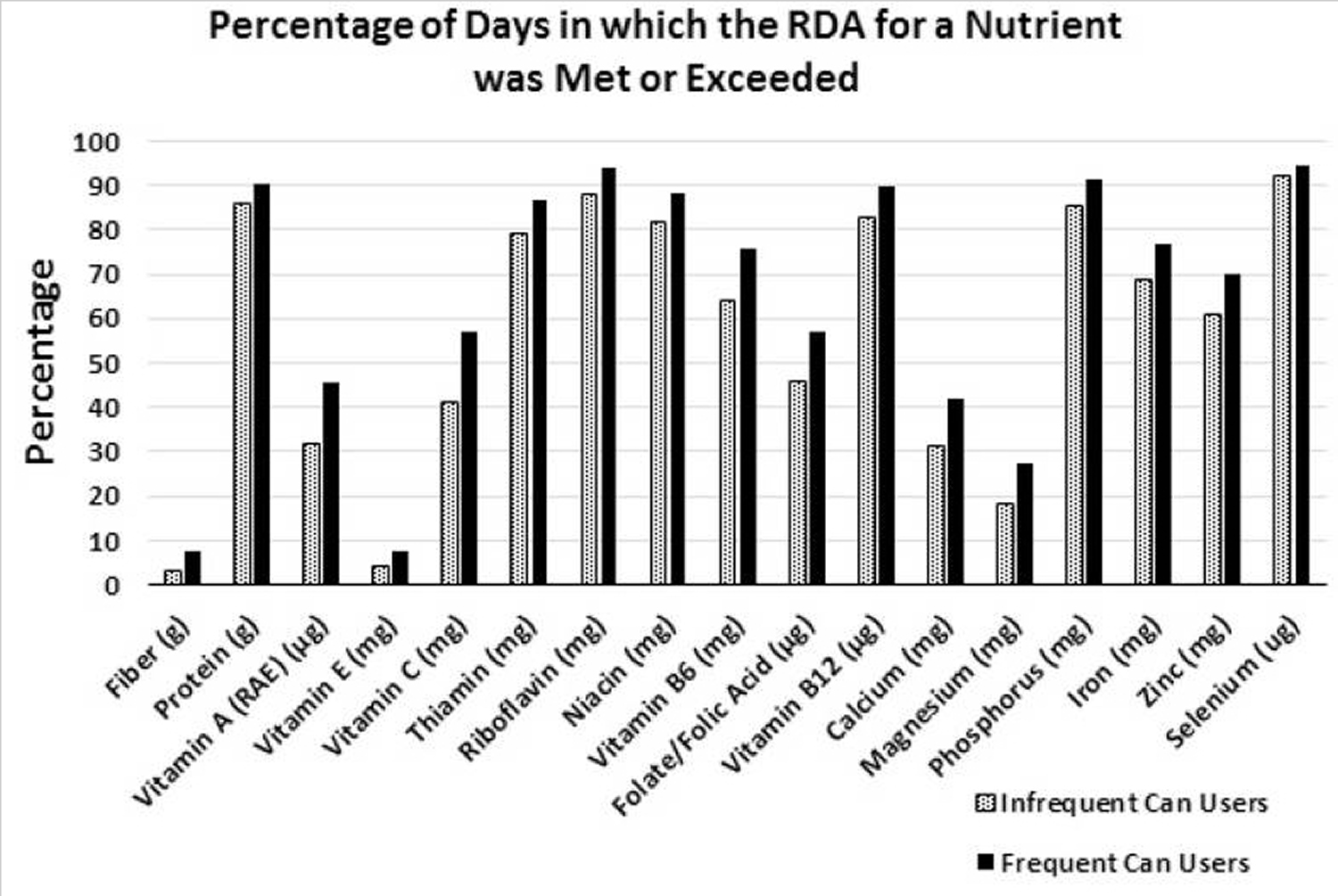
Notes: Percentage of days in which participants met or exceeded the Recommended Dietary Allowance (RDA) for different nutrients among Frequent and Infrequent Canned Food Users (FCU and ICU). Percentage of infrequent (n = 2732) and frequent (n = 2584) canned food users survey days in which the RDA was met or exceeded for a nutrient. Data from the NPD Group’s National Eating Trends® intake diary panel 2011–2013 and Nutrient Intake databases.
[Source 18]Canned Food Days vs. Non-Canned Food Days
Further analysis was performed to determine the differences in nutrient intake between the infrequent canned food users (ICU) and frequent canned food users (FCU) groups on days when canned foods were or were not consumed. The results showed that on days when canned foods were consumed, a significantly higher percentage of people in frequent canned food users (FCU) group met or exceeded the RDA for 15 different nutrients, compared to the infrequent canned food users (ICU) group (Table 3). Additionally, when compared to the infrequent canned food users (ICU) group, a significantly higher percentage of the frequent canned food users (FCU) group also met or exceeded the RDA for the same 15 nutrients on days when canned foods were not consumed. Some of the largest differences in nutrient intake between the frequent canned food users (FCU) and infrequent canned food users (ICU) groups were for vitamin A (17% higher on canned food days; 10% higher on non-canned food days); vitamin C (17% higher on canned food days; 15% higher on non-canned food days); folate (15.4% higher on canned food days; 9.9% higher on non-canned food days); vitamin B6 (13.8% higher on canned food days; 8.8% higher on non-canned food days); and calcium (12.8% higher on canned food days; 8.5% higher on non-canned food days). Although the percentage of people meeting or exceeding the RDA for dietary fiber intake did not significantly differ between the infrequent canned food users (ICU) and frequent canned food users (FCU) groups on either canned or non-canned days, there were nearly three times as many people in the frequent canned food users (FCU) group who met or exceeded the requirement on days in which canned foods were consumed, compared to the infrequent canned food users (ICU) group (9.4% vs. 3.9%, respectively).
Table 3. Percentage of Canned vs. Non-Canned consumption days in which participants met or exceeded the Recommended Dietary Allowance (RDA) for a nutrient among Frequent and Infrequent Canned Food Users.
| Variable | % Canned Days that the RDA Was Met or Exceeded | % Non-Canned Days that the RDA Was Met or Exceeded | ||
| IFU | FCU | IFU | FCU | |
| Fiber | 3.9 | 9.4 | 3 | 5.5 |
| Protein | 86.1 | 91.6 | 85.8 | 89.1 |
| Vitamin A | 31.7 | 48.7 | 31.9 | 41.9 |
| Vitamin E | 3.5 | 7.5 | 4.2 | 7.7 |
| Vitamin C | 41 | 58 | 41 | 56 |
| Thiamin | 76.3 | 87.2 | 79.3 | 86.5 |
| Riboflavin | 87.5 | 94.1 | 88.2 | 93.4 |
| Niacin | 80.5 | 89.5 | 82 | 87.1 |
| Vitamin B6 | 64.2 | 78 | 63.7 | 72.5 |
| Folate | 42.1 | 57.5 | 46.3 | 56.2 |
| Vitamin B12 | 82.5 | 90.2 | 82.7 | 89.1 |
| Calcium | 30.3 | 43.1 | 31.7 | 40.2 |
| Magnesium | 17.6 | 29.3 | 18.2 | 25.4 |
| Phosphorus | 85.7 | 92 | 85.5 | 90.1 |
| Iron | 71 | 78.4 | 68.5 | 74.7 |
| Zinc | 64.2 | 72.4 | 60.3 | 66.6 |
| Selenium | 91.7 | 94.5 | 92.2 | 94.7 |
Notes: Percentage of infrequent (n = 2732) and frequent (n = 2584) canned food users (ICU and FCU, respectively) survey days in which the Recommended Dietary Allowance (RDA) was met or exceeded for a nutrient. Data divided by days in which canned foods were consumed and days in which no canned foods were consumed. Data sourced from the NPD Group’s National Eating Trends® intake diary panel 2011–2013 and Nutrient Intake databases.
[Source 18]Food Group Intake and Eat Rate
A comparison of food group intake between infrequent and frequent canned food consumers showed that the frequent canned food users (FCU) group had significantly higher average daily intake of the four primary nutrient-dense food groups; fruits, vegetables, dairy and protein foods (Figure 4). Compared to the infrequent canned food users (ICU) group, the frequent canned food users (FCU) consumed 30.3% more servings of fruit, 21.4% more servings of vegetables, 18.2% more servings of milk, yogurt and cheese, and 8.5% more servings of protein-rich foods such as meat, fish, poultry, beans, eggs, and nuts (Figure 4). Over the course of two week study period, the average Eat Rate was also recorded for fruits, vegetables/legumes, fin-fish, processed meat and combination dishes (Figure 1 above). Eat Rate is defined as the average number of times a canned eating individual consumes a product during a two-week period. When compared to the infrequent canned food users (ICU) group, the frequent canned food users (FCU) group had a 116% higher Eat Rate of canned vegetables/legumes, and a 58% higher Eat Rate of canned fruits. Interestingly, when compared to the infrequent canned food users (ICU) group, the frequent canned food users (FCU) group also had a 20% higher Eat Rate of fresh vegetables/legumes, and 6% higher Eat Rate of fresh fruits. The only category of food in which the infrequent canned food users (ICU) group had a significantly higher Eat Rate compared to the frequent canned food users (FCU) group was fresh fin-fish (13% higher for the infrequent canned food users (ICU) group), while the infrequent canned food users (ICU) group had a 48% lower Eat Rate of canned fin-fish.
Figure 4. Mean number of nutrient-dense food group servings per day among frequent and infrequent canned food users (FCU and ICU)
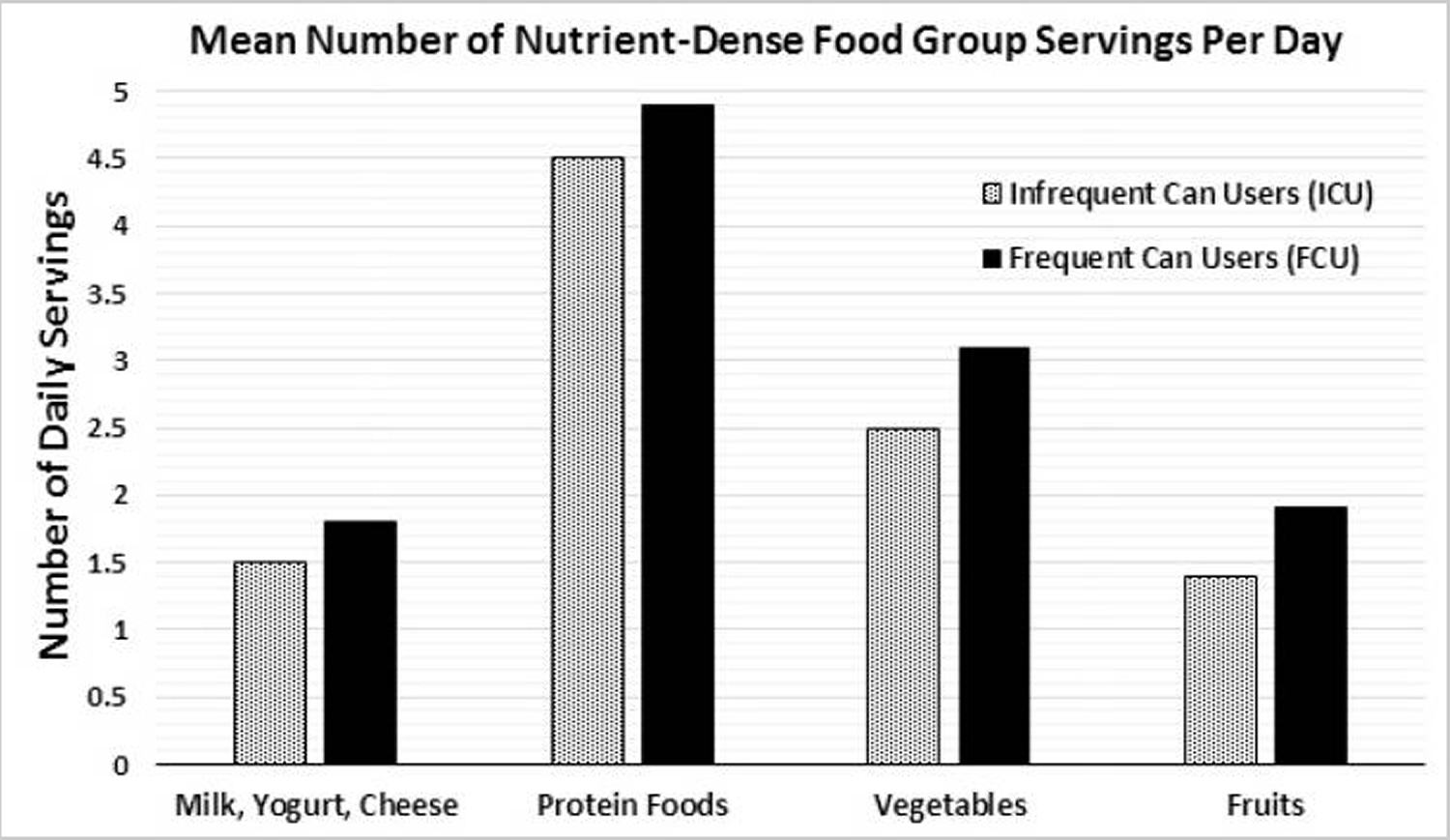
Notes: Mean number of nutrient-dense food group servings per day among frequent and infrequent canned food users (FCU and ICU). Proportion of infrequent (n = 2732) and frequent (n = 2584) canned food users average daily intake of nutrient-dense food groups. Data from The NPD Group’s National Eating Trends® intake diary panel 2011–2013 and Nutrient Intake databases.
[Source 18]In summary, children and adults in the US who frequently consume canned foods, have higher nutrient intakes and healthier eating habits compared to those who infrequently consume canned foods. In this study 18, frequent canned food consumption was associated with higher intakes of 17 essential nutrients including calcium, potassium and fiber—three shortfall nutrients according to the 2015-2020 Dietary Guidelines for Americans. Frequent canned food consumption was also associated with a greater likelihood of consuming nutrient-dense food groups recommended by the Dietary Guidelines for Americans such as: fruits, vegetables, dairy products and protein foods. Therefore, in addition to fresh foods, nutrient-dense canned foods should be promoted by health and nutrition professionals for their ability to improve nutrient intakes and the diet quality of Americans.
The Dietary Guidelines for Americans recommendations to consume more nutrient-dense foods and less calorie-dense/nutrient-poor foods pose a challenge to a substantial number of Americans who do not have the means to do so (i.e., for reasons having to do with cost and/or accessibility). For example, over 14% Americans receive assistance from the Supplemental Nutrition Assistance Program (SNAP program) 23, but, even with this assistance, they still tend to have lower diet quality scores than non-Supplemental Nutrition Assistance Program (SNAP program) participants with similar incomes 24. Furthermore, 7% of Americans, or roughly 23.5 million people live in urban or rural areas known as “food deserts,” which have limited access to fresh, healthy and affordable food 25. Therefore, several Dietary Guidelines for Americans recommended items such as fresh produce or fresh seafood are not always available options for many Americans. However, canned foods are a way to get many of these recommended foods and their unique array of nutrients at affordable prices, even in underserved areas such as food deserts.
Relative to the infrequent canned food users (ICU) group, the frequent canned food users (FCU) group were twice as likely to be participants in the government assistance programs—Supplemental Nutrition Assistance Program (SNAP program) (11.9% vs. 23.5%, respectively) and Women, Infants and Children Program (6.3% vs. 11.8%, respectively) —highlighting the important role canned foods play for individuals facing economic hardships and who have less access to fresh and frozen food varieties. In fact, canned fruits, vegetables, fish and beans are all Women, Infants and Children-eligible foods 26 and Women, Infants and Children recommends low-salt and low-sugar canned and jarred foods as part of a healthy infant and toddler feeding program 27.
Bisphenol A (BPA) in Canned Foods
Bisphenol A (BPA, 2,2-bis(4-hydroxyphenyl)propane), a synthetic chemical used as a starting substance to make resins, plastics, polycarbonate bottles and internal lining of cans 28 with endocrine disrupting properties approved for use in food packaging in the 1960’s 29. BPA, a well-known endocrine disruptor, interacts with female hormone receptors and activates the female hormones, showing weak estrogenic effects 30. Such effects have been confirmed in animal testing as well, with signs of lower sperm counts, uterotrophic effects, precocious puberty effects on female animals, and effects on male reproductive organ development observed 31. In human, it is associated with behavior disorder, such as aggression and hyperactivity, drug addiction, recurrent miscarriages, diabetes, coronary heart diseases, and liver toxicity 32. Despite a growing body of research into the safety of BPA, no single study conclusively proves that BPA is harmful to humans. There is a lack of human data in this area, which is a problem. This is mainly due to the difficulty in finding people who have not been exposed to BPA. There are also ethical constraints. For example, it is not possible to test potentially harmful chemicals on pregnant women to see the effects on their children. This means that researchers depend on animal studies, which have only limited application to humans. Animal research has connected BPA exposure to a range of health problems in mice or rats, including metabolic disorders and obesity, male fertility problems, asthma and intestinal inflammation.
Metal food and drink cans are commonly coated with epoxy films made from phenolic polymers produced from bisphenol A (BPA) 33. Exposure occurs primarily through the diet 34. Bisphenol A has been quantified in many canned goods 33, 35, where it is present as a by-product of interior epoxy coatings used to prevent corrosion. Detectable BPA concentrations across all foods ranged from 2.6 to 730 ng/g 33. Large variations in BPA concentrations were found between different products of the same food type and between different lots of the same product. Given the large concentration ranges, the only distinguishable trend was that canned fruits and canned tuna showed the lowest BPA concentrations 33. Experiments with fortified frozen vegetables and brine solutions, as well as higher BPA concentrations in canned food solids over liquid portions, clearly indicated that BPA partitions into the solid portion of foods. In adults, urinary BPA concentrations are positively associated with cardiovascular disease and diabetes 36, 37.
Bisphenol A (BPA) is commonly utilized as a monomer base for polycarbonate plastic and as a linkage in epoxy resins. Polycarbonate plastic is a hard, clear plastic used in a wide range of consumer products including food storage containers 38. Enamel coatings made of epoxy resins are used to line the inside of many food and beverage containers 29. Additional BPA uses include as a color developer in thermal receipts 30, in medical devices 30 and as a component of some dental composites 39.
The widespread use of polycarbonate plastics and epoxy resins in consumer products 40 has contributed to the ubiquitous BPA exposure in the human population, with BPA being detected in the urine of 92.6 % of the American population 41. Although BPA exposure has been measured in household dust and air 42 and in water contaminated by landfill leachate 43, diet is considered the main contributor of BPA exposure 44.
BPA in food packaging is a concern due to its propensity to leach into the product. BPA molecules migrating into the food from its incomplete polymerization in the manufacturing of epoxy resins of cans was recognized in 1995 45. Polymeric coatings on light metal packaging, used for foods and beverages, are one of the previously identified major sources of exposure to via the diet 46. Migration from coatings of canned products and from lids of glass jars and bottles may occur due to the presence of BPA monomer from incompletely polymerised epoxy resin coatings and of BPA present as a residual impurity of the epoxy substance bisphenol A diglycidyl ether (BADGE). Subsequent studies have shown that BPA can leach into food from polycarbonate plastic bottles, plastic storage containers, and polyvinyl chloride (PVC) stretch film 47. Intervention studies have shown an ability to decrease or increase urinary BPA concentration by controlling the consumption of known sources of BPA from the food system 48. Studies closely following dietary intake and collecting multiple biomarker samples validated with pharmacokinetics data have shown that about two-thirds of BPA exposure can be attributed to diet, and one third is unaccounted for 44. Analysis of fasting data have also shown that when dietary intake stops, BPA is still present in the body indicating non-food pathways or possible storage of BPA in fat 49.
When BPA is ingested by humans, it is transformed by the liver into bisphenol A-glucuronide, a highly water soluble compound 50. In pharmacokinetics studies, BPA’s half-life in the body is less than six hours, and BPA is completely eliminated from the body in 24 hours 50. Because of BPA rapid clearance from the body through urine, total urinary BPA compounds, comprised of free plus conjugated BPA, are the most appropriate BPA exposure assessment marker 37. The best urinary collection method including single samples vs. 24-hour sampling, and the timing of sampling have been investigated 51. The conclusions of those studies vary depending on a researcher’s intent to determine individual or population level BPA exposures and short-term vs. long term exposure profiles. Spot urine samples collected by large cross-sectional population level surveys, such as the National Health and Nutrition Examination Survey (NHANES), can characterize average population exposures 52.
Several expert bodies and regulatory authorities have issued risk assessments of consumer exposure to BPA over recent years. European Food Safety Authority (EFSA) started work in 2012 on a new risk assessment of BPA 53. It completed a full risk assessment of BPA in 2006 and established a Tolerable Daily Intake (TDI) of 5 μg/kg body weight per day for the substance, as have other recognized bodies. The Tolerable Daily Intake (TDI) is an estimate of the amount of a substance, expressed on a body weight basis, that can be ingested daily over a lifetime without appreciable risk. EFSA also evaluated intakes of BPA through food and drink for adults, infants and children and found that intakes were all well below the TDI. European Food Safety Authority (EFSA) has updated its scientific advice on BPA several times since 2006, most recently in 2018 46. In its latest BPA risk assessment published in 2015 54, the Panel on Food Contact Materials, Enzymes, Flavourings and Processing Aids 46 reduced and set the Tolerable Daily Intake (TDI) for BPA on a temporary basis to Tolerable Daily Intake (TDI) for BPA of 4 μg/kg body weight per day to account for uncertainties related to possible BPA effects at low doses on mammary gland, reproductive, neurological, immune and/or metabolic systems, thus committing to a re-evaluation of the TDI in light of the new data available. Notwithstanding this, the European Commission and member states decided to prohibit the use of BPA in polycarbonate articles that were considered to be one of the major contributors of exposure, particularly for babies, so the use of BPA to make plastic infant feeding bottles was banned in the European Union from 2011 55.
In July 2012 the U.S. Food and Drug Administration (FDA) 29 amended its Food Additive Regulations to no longer provide for the use of BPA-based polycarbonate resins in baby bottles and sippy cups. The FDA took this action in response to a food additive petition filed by the American Chemistry Council (ACC). The American Chemistry Council (ACC) petition demonstrated, from publicly available information and information collected from industry sources, that the use of polycarbonate resins in baby bottles and sippy cups had been abandoned.
In July, 2013 the FDA also amended its regulations to no longer provide for the use of BPA-based epoxy resins as coatings in packaging for infant formula. The FDA took this action in response to a food additive petition filed by Congressman Edward Markey of Massachusetts. This petition demonstrated, from publicly available information and information collected from industry sources, that the use of BPA-based epoxy resins as coatings in packaging for infant formula had been abandoned.
According to the FDA 29 an amendment of the food additive regulations based on abandonment is not based on safety, but is based on the fact that the regulatory authorization is no longer necessary for the specific use of the food additive because that use has been permanently and completely abandoned. The safety of a food additive is not relevant to FDA’s determination regarding whether a certain use of that food additive has been abandoned.
In a UK a study 56 involving 19–64 year olds, it was found the levels of exposure to BPA emanating from light metal packaging using conservative assumptions are well below the TDI of 4 μg/kg body weight per day. The ‘drivers’ of exposure to BPA from light metal packaging using the 97.5th percentile consumer, the main ‘drivers’ of exposure are (mg/person/day): Beer (0.049), Soup and Cider (both 0.023), Carbonates (0.02), Preserved pasta and Preserved ready meals (both 0.018), Canned fruit (0.012), Canned vegetables (0.011) and Canned tomatoes (0.010). All others are below 0.010 with many < 0.0001. Other percentiles or total population can be treated in a similar manner to determine the relevant ‘drivers’.
Table 4. Refined deterministic assessment of exposure for the total population to BPA from light metal packaging for those metal packs with significant market shares
| FACET food groups | Pack type a | Area (cm²/g) | Percentage metal | BPA levels (mg/ dm²) | Food consumed (g/person/day) for the total population | |
|---|---|---|---|---|---|---|
| Minimum | Maximum | Mean | ||||
| Condensed/evaporated milk | PT20/21 | 0.84 | 100 | 0.00005 | 0.02 | 0.5 |
| Jams and fruit preserves | PT41 | 0.16 | 100 | 0.002 | 0.016 | 3.6 |
| Canned/preserved fruit | PT20/21 | 0.85 | 83 | 0.00005 | 0.02 | 4.3 |
| Preserved vegetables without sauces | PT20/21 | 0.97 | 94 | 0.00005 | 0.02 | 7.2 |
| Canned/preserved tomatoes | PT20/21 | 1.08 | 100 | 0.00005 | 0.02 | 2.2 |
| Canned beans and pulses | PT20/21 | 1.19 | 100 | 0.00005 | 0.02 | 0.7 |
| Pasta sauces (tomato based) | PT41 | 0.16 | 65 | 0.002 | 0.016 | 3.4 |
| Pickled vegetables | PT41 | 0.16 | 90 | 0.002 | 0.016 | 2 |
| Preserved meat and meat products | PT20/21 | 0.96 | 100 | 0.00005 | 0.02 | 1.3 |
| Preserved fish/seafood without sauce | PT20/21 | 1.13 | 99 | 0.00005 | 0.02 | 5.7 |
| Vinaigrettes | PT35 | 0.03 | 91 | 0.002 | 0.016 | 0.5 |
| Table sauces | PT35 | 0.05 | 85 | 0.002 | 0.016 | 2.3 |
| Wet sauces PT21/PT41 10.3/80.7 | PT20/21 | 0.85 | 10 | 0.00005 | 0.02 | 14 |
| PT41 | 0.2 | 81 | 0.002 | 0.016 | 14 | |
| PT20 and 21/PT41 average ratio of 10.3/80.7 c | 14 | |||||
| Canned/preserved soup | PT20/21 | 0.96 | 100 | 0.00005 | 0.02 | 10 |
| Beer | PT8 | 0.91 | 74 | 0.001 | 0.004 | 217 |
| Cider | PT8 | 0.9 | 61 | 0.001 | 0.004 | 20 |
| Canned/preserved pasta | PT20/21 | 1.09 | 100 | 0.00005 | 0.02 | 2.8 |
| Canned/preserved ready meals | PT20/21 | 1.09 | 99 | 0.00005 | 0.02 | 18 |
| Preserved fish/seafood with sauce | PT20/21 | 1.2 | 99 | 0.00005 | 0.02 | 0.3 |
Notes: 0 = 0.0000.
FACET = The European Flavours, Additives, and food Contact materials Exposure Task
aPT 8 beverage cans, PT 20/21 food cans with either classic or easy open ends, PT 35 glass bottle metal closure (small area), PT 41 metal closure for glass jars (larger area).
bMinimum and maximum calculated exposures relate to the minimum and maximum levels of extractable BPA
cFor 12.1.10 Wet sauces the contribution from coated metal packaging comes from either food cans (PT20 or PT21) or metal closures on jars (PT41). The exposure has been calculated using the ratio of market shares for cans and closures of 10.3/80.7.
In the US using the National Health and Nutrition Examination Survey (NHANES) data: 2003–2004, 2005–2006, and 2007–2008 US population 57, it was found canned food consumption in the last 24 hours was associated with higher urinary BPA concentrations in both children and adults. The associations between canned food and urinary BPA concentrations were stronger among children compared to adults. Canned beverages were not associated with higher urinary BPA concentrations. Among specific canned foods, canned vegetable and fruit, canned pasta, and canned soup were associated with higher BPA concentrations while canned dairy and canned meat and fish were not. The association was strong for canned soup for the overall population, however, the strong association of urinary BPA concentration and soup consumption did not hold for the youth population. These findings need to be interpreted cautiously as the number of participants consuming canned soup was small (n=23 overall, n=8 for youth) with soup only representing 3% of the canned food eaten. This study is the first known analysis of NHANES data for dietary contributions of BPA exposure using USDA Food Codes. A major strength of the study includes the use of a nationally representative sample to evaluate associations between sources of exposure and biomarkers of internal dose.
Highlights of the US study 57:
- 9% participants consumed one canned food and 2% two or more on the previous day.
- One canned food vs. none was associated with 24% higher urinary BPA concentrations.
- ≥ 2 canned foods vs. none was associated with 54% higher urinary BPA concentrations.
- Some canned foods (vegetables, fruit, pasta, soup) were associated with higher BPA.
- Canned beverages were not associated with urinary BPA concentrations.
Table 5. Ratios of Urinary Bisphenol A Concentrations and Self-Reported Canned Food Type Intake in the past 24-hours- Canned Food Sub-categories
| Whole Population (n=6372) | Youth Pop. (6–19 yrs) (n=2279) | Adult Pop. (20–83 yrs) (n=4093) | ||||
| Canned Food Sub-Categories.: | n | Ratio (95% CI) | n | Ratio (95% CI) | n | Ratio (95% CI) |
| Veg and Fruit – 0 | 6021 | 1.00 (ref.) | 2176 | 1.00 (ref.) | 3845 | 1.00 (ref.) |
| Veg and Fruit – 1 or more | 351 | 1.41 (1.23, 1.63) | 103 | 1.57 (1.21, 2.02) | 248 | 1.37 (1.17, 1.60) |
| Pasta- 0 | 6306 | 1.0 (ref.) | 2246 | 1.00 (ref.) | 4060 | 1.00 (ref.) |
| Pasta- 1 or more | 66 | 1.70 (1.18, 2.44) | 33 | 1.62 (1.36, 1.93) | 33 | 1.68 (1.00, 2.81) |
| Soup- 0 | 6349 | 1.00 (ref.) | 2271 | 1.00 (ref.) | 4078 | 1.00 (ref.) |
| Soup- 1 or more | 23 | 2.29 (1.22, 4.30) | 8 | 1.41 (0.66, 3.03) | 15 | 2.65 (1.23, 5.70) |
| Dairy- 0 | 6327 | 1.00 (ref.) | 2259 | 1.00 (ref.) | 4068 | 1.00 (ref.) |
| Dairy- 1 or more | 45 | 1.14 (0.72, 1.80) | 20 | 1.00 (0.64, 1.55) | 25 | 1.19 (0.64, 2.22) |
| Meat and Fish- 0 | 6125 | 1.00 (ref.) | 2217 | 1.00 (ref.) | 3908 | 1.00 (ref.) |
| Meat and Fish- 1 or more | 247 | 1.02 (0.86, 1.20) | 62 | 1.02 (0.71, 1.46) | 185 | 1.02 (0.87, 1.19) |
Notes: GM= geometric mean, CI = confidence interval, Veg = Vegetable, ref.= reference
Whole, Youth, and Adult Population models shown as adjusted ratio of geometric means (95% CI), adjusted for sex, age, race, income, education, smoking, and creatinine.
[Source 57]A new study from researchers at the Harvard School of Public Health 58 has found that a group of volunteers who consumed a serving of canned soup each day for five days had a more than 1,000% increase in urinary bisphenol A (BPA) concentrations compared with when the same individuals consumed fresh soup daily for five days. The researchers, set out to quantify whether canned-soup consumption would increase urinary BPA concentrations relative to eating fresh soup. They recruited student and staff volunteers from Harvard School of Public Health. One group consumed a 12-ounce serving of vegetarian canned soup each day for five days; another group consumed 12 ounces of vegetarian fresh soup (prepared without canned ingredients) daily for five days. After a two-day “washout” period, the groups reversed their assignments. Urine samples of the 75 volunteers taken during the testing showed that consumption of a serving of canned soup daily was associated with a 1,221% increase in BPA compared to levels in urine collected after consumption of fresh soup 58. The researchers note that the elevation in urinary BPA concentrations may be temporary and that further research is needed to quantify its duration. The magnitude of the rise in urinary BPA we observed after just one serving of soup was unexpected and may be of concern among individuals who regularly consume foods from cans or drink several canned beverages daily. Moreover, the generalizability of that study result is limited due to selection of participants from 1 schooland testing of a single soup brand; however, generalizability to canned goods with similar BPA content is expected. The effect of such intermittent elevations in urinary BPA concentration is unknown. The absolute urinary BPA concentrations observed following canned soup consumption are among the most extreme reported in a nonoccupational setting. For comparison, the 95th percentile unadjusted urinary BPA in the 2007–2008 National Health and Examination Survey was 13.0 μg/L 59. The observed increase in urinary BPA concentrations following canned soup consumption, even if not sustained, may be important, especially in light of available or proposed alternatives to epoxy resins linings for most canned goods. It may be advisable for manufacturers to consider eliminating BPA from can linings, said the senior author of the study 58. That study is one of the first to quantify BPA levels in humans after ingestion of canned foods.
Previous studies have linked elevated urinary BPA concentrations are positively associated with cardiovascular disease and diabetes 36. Scientists have known for a while that drinking beverages that have been stored in certain hard plastics can increase the amount of BPA in your body. That study 58 suggested that canned foods may be an even greater concern, especially given their wide use. Exposure to the endocrine-disrupting chemical BPA, used in the lining of metal food and beverage cans, has been shown to interfere with reproductive development in animals and has been linked with cardiovascular disease, diabetes, and obesity in humans. In addition to the lining of food and beverage cans, BPA is also found in polycarbonate bottles (identified by the recycling number 7) and dentistry composites and sealants.
Figure 5. Adjusted Urinary Bisphenol A Concentration After a Week of Canned Soup Consumption
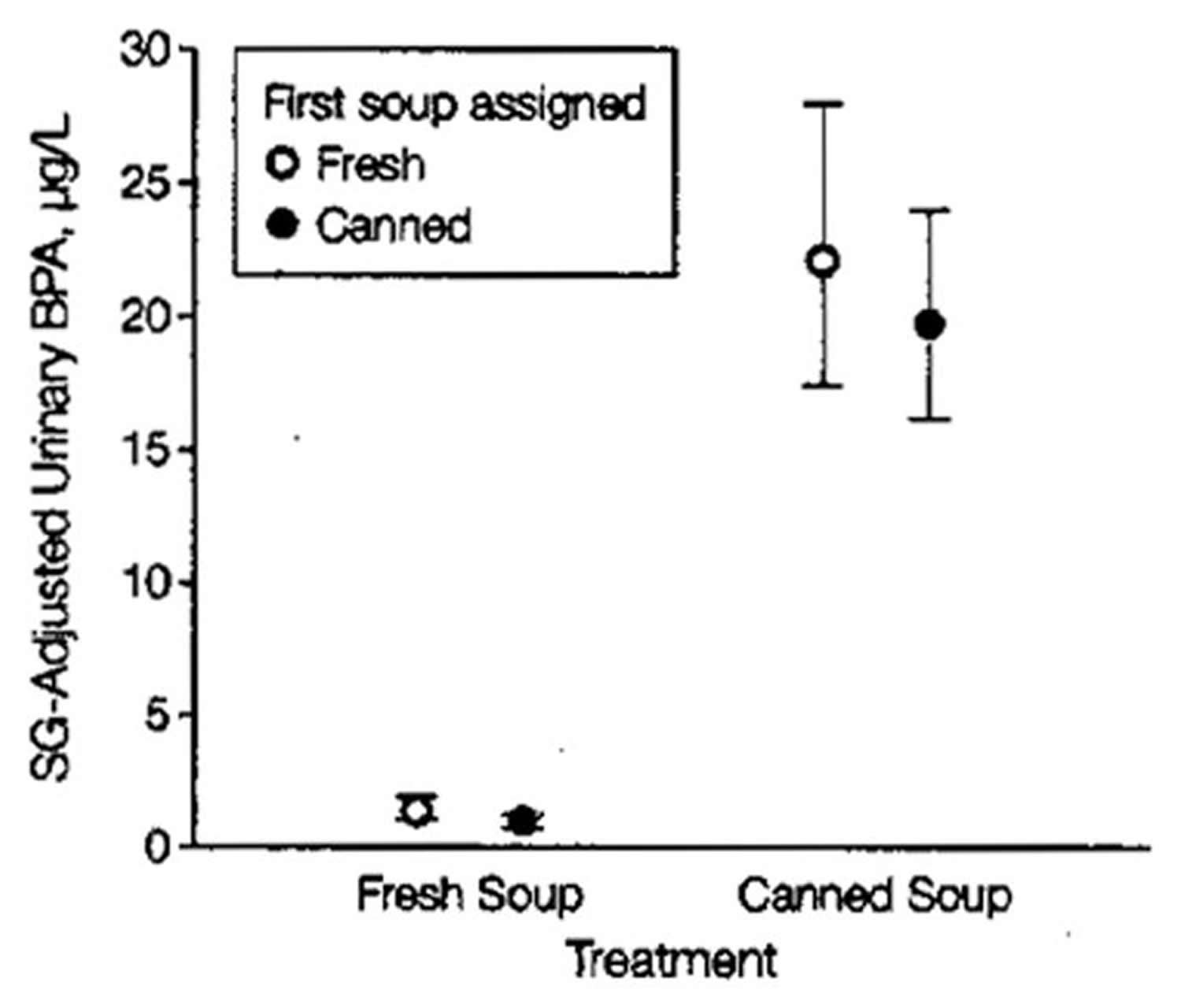 Notes: Geometric mean specific gravity (SG)–adjusted urinary bisphenol A (BPA) concentration following a week of daily consumption of fresh or canned soup. For reference, the unadjusted geometric mean for the 2007–2008 National Health and Examination Survey (NHANES) was 2.08 μg/L (95% CI, 1.92–2.26 μg/L), and the 95th percentile was 13.0 μg/L (95% CI, 10.0–15.4 μg/L). Error bars indicate 95% CIs.
Notes: Geometric mean specific gravity (SG)–adjusted urinary bisphenol A (BPA) concentration following a week of daily consumption of fresh or canned soup. For reference, the unadjusted geometric mean for the 2007–2008 National Health and Examination Survey (NHANES) was 2.08 μg/L (95% CI, 1.92–2.26 μg/L), and the 95th percentile was 13.0 μg/L (95% CI, 10.0–15.4 μg/L). Error bars indicate 95% CIs.
The Centers for Disease Control and Prevention (CDC) in its Fourth National Report on Human Exposure to Environmental Chemicals Report, measured BPA in the urine of 2,517 participants aged six years and older who took part in CDC’s National Health and Nutrition Examination Survey (NHANES) during 2003–2004. CDC scientists found detectable levels of BPA in 93% of 2,517 urine samples from people six years and older 60, 61. The Centers for Disease Control and Prevention (CDC) NHANES data are considered representative of exposures in the United States. Another reason for concern, especially for parents, may be because some animal studies report effects in fetuses and newborns exposed to BPA.
In the fall of 2014, FDA experts from across the agency, specializing in toxicology, analytical chemistry, endocrinology, epidemiology, and other fields, completed a four-year review of more than 300 scientific studies. The FDA review has not found any information in the evaluated studies to prompt a revision of FDA’s safety assessment of BPA in food packaging at this time 62. Based on FDA’s ongoing safety review of scientific evidence, the available information continues to support the safety of BPA for the currently approved uses in food containers and packaging 62. The FDA will also continue to consult with other expert agencies in the federal government, including the National Institutes of Health (and the National Toxicology Program), the Environmental Protection Agency, the Consumer Product Safety Commission, and the Centers for Disease Control and Prevention. The FDA will continue to participate in discussions with our international regulatory and public health counterparts who are also engaged in assessing the safety of BPA.
What about frozen vegetables and BPA?
Frozen food intake and BPA exposure can be associated with packaging material for frozen food, cooking method and food container 63. Plastic wraps used in food packaging can cause BPA leakage and urinary BPA concentrations decreased when consumption of plastic packaged food were limited for 3 days compared to when on a general diet 64, 65. It can be presumed through these studies 64, 65 that the use of plastic packaging for most frozen foods is one of the causes of increased BPA exposure. Also, BPA migration can occur from plastic containers used for microwave oven, and BPA exposure could increase when using vinyl wrapping in a microwave oven to defrost frozen food 66. This Korean study 63 showed that the geometrical mean of urinary BPA levels was significant in female group using zip-top or plastic bags as refrigerator storage containers. Therefore, use of these containers for frozen food storage can also increase BPA exposure as a result of frozen food consumption.
Summary
Bisphenol A (BPA) is an industrial chemical that has been used to make certain plastics and resins since the 1960s. Bisphenol A (BPA) is found in polycarbonate plastics and epoxy resins. Polycarbonate plastics are often used in containers that store food and beverages, such as water bottles and canned foods. They may also be used in other consumer goods. Epoxy resins are used to coat the inside of metal products, such as food cans, bottle tops and water supply lines. Some dental sealants and composites also may contain BPA. BPA can also be found in breast milk 61.
Some research has shown that BPA can seep into food or beverages from containers that are made with BPA. The degree to which BPA leaches from polycarbonate bottles into liquid may depend more on the temperature of the liquid or bottle, than the age of the container 61. Exposure to BPA is a concern because of possible health effects of BPA on the brain, behavior and prostate gland of fetuses, infants and children. Additional research suggests a possible link between BPA and increased blood pressure and heart disease. However, the Food and Drug Administration (FDA) has said that BPA is safe at the very low levels that occur in some foods. This assessment is based on review of hundreds of studies 62. Therefore more research is needed to fully understand the health effects of BPA exposure.
Due to the potential harm of Bisphenol A (BPA) and the fact that Bisphenol A is found in canned foods, with higher BPA concentrations being found canned vegetables and canned fruit, canned pasta and canned soup and in lower concentration canned dairy and canned meat and fish. If you’re concerned about BPA, it’s best you reduce your use of canned foods since most cans are lined with BPA-containing resin. Use glass, porcelain or stainless steel containers for hot foods and liquids instead of plastic containers. The National Institute of Environmental Health Sciences, part of the National Institutes of Health, advises against microwaving polycarbonate plastics or putting them in the dishwasher, because the plastic may break down over time and allow BPA to leach into foods.
Use BPA-free products. Manufacturers are creating more and more BPA-free products. Look for products labeled as BPA-free. If a product isn’t labeled, keep in mind that some, but not all, plastics marked with recycle codes 3 or 7 may be made with BPA.
Parents and caregivers, can make the personal choice to reduce exposures of their infants and children to BPA:
- Don’t microwave polycarbonate plastic food containers. Polycarbonate is strong and durable, but over time it may break down from over use at high temperatures.
- Plastic containers have recycle codes on the bottom. Some, but not all, plastics that are marked with recycle codes 3 or 7 may be made with BPA.
- Reduce your use of canned foods and packed foods.
- When possible, opt for glass, porcelain or stainless steel containers, particularly for hot food or liquids.
- Use baby bottles that are BPA free.
- Comerford KB. Frequent Canned Food Use is Positively Associated with Nutrient-Dense Food Group Consumption and Higher Nutrient Intakes in US Children and Adults. Nutrients. 2015;7(7):5586-5600. doi:10.3390/nu7075240.[↩]
- Canned Food Alliance . Telephone Survey (Landline and Mobile Numbers) of 1007 American Adults by Caravan(r) Survey, April 4–7 2013. Margin of Error +/− 3.1%. Canned Food Alliance; Pittsburgh, PA, USA: 2013.[↩][↩][↩]
- Canned Vegetable and Fruit Consumption Is Associated with Changes in Nutrient Intake and Higher Diet Quality in Children and Adults: National Health and Nutrition Examination Survey 2001-2010. J Acad Nutr Diet. 2016 Jun;116(6):940-8. doi: 10.1016/j.jand.2015.10.013. Epub 2015 Nov 24. https://jandonline.org/article/S2212-2672(15)01587-7/fulltext[↩]
- Rickman, J.C., Barrett, D.M., Bruhn, C.M. Nutritional comparison of fresh, frozen and canned fruits and vegetables. Part 1. Vitamins C and B and phenolic compounds. J Sci Food Agric. 2007; 87:930–944.[↩][↩]
- Miller S.R., Knudson W.A. Nutrition and cost comparisons of select canned, frozen, and fresh fruits and vegetables. Am. J. Lifestyle Med. 2014 doi: 10.1177/1559827614522942.[↩][↩]
- Kapica C., Weiss W. Canned fruits, vegetables, beans and fish provide nutrients at a lower cost compared to fresh, frozen or dried. J. Nutr. Food Sci. 2012;26 doi: 10.4172/2155-9600.1000131.[↩][↩][↩]
- Rickman J.C., Bruhn C.M., Barrett D.M. Nutritional comparison of fresh, frozen, and canned fruits and vegetables—II. Vitamin A and carotenoids, vitamin E, minerals and fiber. J. Sci. Food Agric. 2007;87:1185–1196. doi: 10.1002/jsfa.2824.[↩]
- Rickman J.C., Barrett D.M., Bruhn C.M. Nutritional comparison of fresh, frozen and canned fruits and vegetables. Part 1. Vitamins C and B and phenolic compounds. J. Sci. Food Agric. 2007;87:930–944. doi: 10.1002/jsfa.2825.[↩][↩]
- Food and Nutrition. https://health.gov/dietaryguidelines/[↩]
- Durst R.W., Weaver G.W. Nutritional content of fresh and canned peaches. J. Sci. Food Agric. 2013;93:593–603. doi: 10.1002/jsfa.5849. https://www.ncbi.nlm.nih.gov/pubmed/22968977[↩][↩]
- Rickman J.C., Bruhn C.M., Barrett D.M. Nutritional comparison of fresh, frozen, and canned fruits and vegetables—II. Vitamin A and carotenoids, vitamin E, minerals and fiber. J. Sci. Food Agric. 2007;87:1185–1196. doi: 10.1002/jsfa.2824[↩]
- Pedrosa M.M., Cuadrado C., Burbano C., Muzquiz M., Cabellos B., Olmedilla-Alonso B., Asensio-Vegas C. Effects of industrial canning on the proximate composition, bioactive compounds contents and nutritional profile of two Spanish common dry beans (phaseolus vulgaris L.) Food Chem. 2015;166:68–75. doi: 10.1016/j.foodchem.2014.05.158. https://www.ncbi.nlm.nih.gov/pubmed/25053030[↩]
- Lessin W.J., Catigani G.L., Schwartz S.J. Quantification of cis-trans isomers of provitamin A carotenoids in fresh and processed fruits and vegetables. J. Agric. Food Chem. 1997;45:3728–3732. doi: 10.1021/jf960803z.[↩]
- Pedrosa M.M., Cuadrado C., Burbano C., Muzquiz M., Cabellos B., Olmedilla-Alonso B., Asensio-Vegas C. Effects of industrial canning on the proximate composition, bioactive compounds contents and nutritional profile of two Spanish common dry beans (phaseolus vulgaris L.) Food Chem. 2015;166:68–75. doi: 10.1016/j.foodchem.2014.05.158 https://www.ncbi.nlm.nih.gov/pubmed/25053030[↩][↩]
- Dietary Guidelines for Americans. https://health.gov/dietaryguidelines/[↩][↩][↩][↩]
- Center of Disease Control and Prevention (CDC) Top 10 Sources of Sodium. https://www.cdc.gov/salt/sources.htm[↩]
- Duyff R.L., Mout J.R., Jones J.B. Sodium reduction in canned beans after draining, rinsing. J. Culin. Sci. Technol. 2011;9:106–112. doi: 10.1080/15428052.2011.582405.[↩]
- Comerford KB. Frequent Canned Food Use is Positively Associated with Nutrient-Dense Food Group Consumption and Higher Nutrient Intakes in US Children and Adults. Nutrients. 2015;7(7):5586-5600. doi:10.3390/nu7075240. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4517017/[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- The NPD Group National Eating Trends® (NET®) Database, in-Home Individual Database. https://tools.nccor.org/css/system/69/[↩]
- Dietary Guidelines for Americans. https://health.gov/dietaryguidelines[↩]
- Zhang Z., Cogswell M.E., Gillespie C., Fang J., Loustalot F., Dai S., Carriquiry A.L., Kuklina E.V., Hong Y., Merritt R., et al. Association between usual sodium and potassium intake and blood pressure and hypertension among U.S. adults: NHANES 2005–2010. PLoS ONE. 2013;8:e75289. doi: 10.1371/journal.pone.0075289 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3794974/[↩]
- Rodrigues S.L., Baldo M.P., Machado R.C., Forechi L., Molina Mdel C., Mill J.G. High potassium intake blunts the effect of elevated sodium intake on blood pressure levels. J. Am. Soc. Hypertens. JASH. 2014;8:232–238. doi: 10.1016/j.jash.2014.01.001 https://www.ncbi.nlm.nih.gov/pubmed/24524886[↩]
- U.S. Department of Agriculture (USDA) Food and Nutrition Service, Office of Research and Analysis . Building a Healthy America: A Profile of the Supplemental Nutrition Assistance Program. U.S. Department of Agriculture; Washington, DC, USA: 2014.[↩]
- Nguyen B.T., Shuval K., Njike V.Y., Katz D.L. The supplemental nutrition assistance program and dietary quality among us adults: Findings from a nationally representative survey. Mayo Clin. Proc. 2014;89:1211–1219. doi: 10.1016/j.mayocp.2014.05.010. https://www.ncbi.nlm.nih.gov/pubmed/25107469[↩]
- USDA Agricultural marketing service: Food deserts. https://www.ers.usda.gov/data/fooddesert[↩]
- USDA Women, infants and children (WIC) WIC food packages—Regulatory requirements for WIC-eligible foods. https://www.fns.usda.gov/wic/wic-food-packages-regulatory-requirements-wic-eligible-foods[↩]
- Wolfe D., Pipes D., Lucas B. I’m ready! Feeding family foods to your baby. https://wicworks.fns.usda.gov/[↩]
- EFSA. Call for data relevant to the hazard assessment of Bisphenol A (BPA) 2018. http://www.efsa.europa.eu/en/consultations/call/180309-0[↩]
- U.S. Food and Drug Administration. Bisphenol A (BPA): Use in Food Contact Application. https://www.fda.gov/NewsEvents/PublicHealthFocus/ucm064437.htm[↩][↩][↩][↩]
- A review of dietary and non-dietary exposure to bisphenol-A. Geens T, Aerts D, Berthot C, Bourguignon JP, Goeyens L, Lecomte P, Maghuin-Rogister G, Pironnet AM, Pussemier L, Scippo ML, Van Loco J, Covaci A. Food Chem Toxicol. 2012 Oct; 50(10):3725-40. https://www.ncbi.nlm.nih.gov/pubmed/22889897/[↩][↩][↩]
- Human health risk on environmental exposure to Bisphenol-A: a review. Tsai WT. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2006; 24(2):225-55. https://www.ncbi.nlm.nih.gov/pubmed/17114111/[↩]
- Urinary, circulating, and tissue biomonitoring studies indicate widespread exposure to bisphenol A. Vandenberg LN, Chahoud I, Heindel JJ, Padmanabhan V, Paumgartten FJ, Schoenfelder G. Environ Health Perspect. 2010 Aug; 118(8):1055-70. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2920080/[↩]
- Concentration of bisphenol A in highly consumed canned foods on the U.S. market. Noonan GO, Ackerman LK, Begley TH. J Agric Food Chem. 2011 Jul 13; 59(13):7178-85. https://www.ncbi.nlm.nih.gov/pubmed/21598963/[↩][↩][↩][↩]
- An observational study of the potential exposures of preschool children to pentachlorophenol, bisphenol-A, and nonylphenol at home and daycare. Wilson NK, Chuang JC, Morgan MK, Lordo RA, Sheldon LS. Environ Res. 2007 Jan; 103(1):9-20. https://www.ncbi.nlm.nih.gov/pubmed/16750524/[↩]
- Concern over canned foods. Our tests find wide range of bisphenol A in soups, juice, and more. Consum Rep. 2009 Dec; 74(12):54-5. https://www.ncbi.nlm.nih.gov/pubmed/20358654[↩]
- Association of urinary bisphenol A concentration with medical disorders and laboratory abnormalities in adults. Lang IA, Galloway TS, Scarlett A, Henley WE, Depledge M, Wallace RB, Melzer D. JAMA. 2008 Sep 17; 300(11):1303-10. https://www.ncbi.nlm.nih.gov/pubmed/18799442/[↩][↩]
- Melzer D, Rice NE, Lewis C, Henley WE, Galloway TS. Association of urinary bisphenol A concentration with heart disease: Evidence from NHANES 2003/06. PLoS One. 2010;5:e8673. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2800195/[↩][↩]
- Bisphenol-A: an estrogenic substance is released from polycarbonate flasks during autoclaving. Krishnan AV, Stathis P, Permuth SF, Tokes L, Feldman D. Endocrinology. 1993 Jun; 132(6):2279-86. https://academic.oup.com/endo/article-abstract/132/6/2279/3034917[↩]
- Exposure to bisphenol A from bis-glycidyl dimethacrylate-based dental sealants. Joskow R, Barr DB, Barr JR, Calafat AM, Needham LL, Rubin C. J Am Dent Assoc. 2006 Mar; 137(3):353-62. https://www.ncbi.nlm.nih.gov/pubmed/16570469/[↩]
- Association of urinary bisphenol a concentration with heart disease: evidence from NHANES 2003/06. Melzer D, Rice NE, Lewis C, Henley WE, Galloway TS. PLoS One. 2010 Jan 13; 5(1):e8673. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2800195/[↩]
- Exposure of the U.S. population to bisphenol A and 4-tertiary-octylphenol: 2003-2004. Calafat AM, Ye X, Wong LY, Reidy JA, Needham LL. Environ Health Perspect. 2008 Jan; 116(1):39-44. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2199288/[↩]
- Occurrence of bisphenol A in indoor dust from two locations in the eastern United States and implications for human exposures. Loganathan SN, Kannan K. Arch Environ Contam Toxicol. 2011 Jul; 61(1):68-73. https://www.ncbi.nlm.nih.gov/pubmed/21221962/[↩]
- Human exposure to bisphenol A (BPA). Vandenberg LN, Hauser R, Marcus M, Olea N, Welshons WV. Reprod Toxicol. 2007 Aug-Sep; 24(2):139-77. https://www.ncbi.nlm.nih.gov/pubmed/17825522/[↩]
- Reconstruction of bisphenol A intake using a simple pharmacokinetic model. Christensen KL, Lorber M, Ye X, Calafat AM. J Expo Sci Environ Epidemiol. 2015 May; 25(3):240-8. https://www.ncbi.nlm.nih.gov/pubmed/24252884/[↩][↩]
- Xenoestrogens released from lacquer coatings in food cans. Brotons JA, Olea-Serrano MF, Villalobos M, Pedraza V, Olea N. Environ Health Perspect. 1995 Jun; 103(6):608-12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1519121/pdf/envhper00355-0084.pdf[↩]
- European Food Safety Authority (EFSA). Call for data relevant to the hazard assessment of Bisphenol A (BPA) 2018. http://www.efsa.europa.eu/en/consultations/call/180309-0[↩][↩][↩]
- Most plastic products release estrogenic chemicals: a potential health problem that can be solved. Yang CZ, Yaniger SI, Jordan VC, Klein DJ, Bittner GD. Environ Health Perspect. 2011 Jul; 119(7):989-96. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3222987/[↩]
- Canned soup consumption and urinary bisphenol A: a randomized crossover trial. Carwile JL, Ye X, Zhou X, Calafat AM, Michels KB. JAMA. 2011 Nov 23; 306(20):2218-20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3367259/[↩]
- Bisphenol A data in NHANES suggest longer than expected half-life, substantial nonfood exposure, or both. Stahlhut RW, Welshons WV, Swan SH. Environ Health Perspect. 2009 May; 117(5):784-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2685842/[↩]
- Volkel W, Colnot T, Csanady GA, Filser JG, Dekant W. Metabolism and kinetics of bisphenol A in humans at low doses following oral administration. Chem Res Toxicol. 2002;15:1281.[↩][↩]
- LaKind JS, Naiman DQ. Temporal trends in bisphenol A exposure in the United States from 2003–2012 and factors associated with bpa exposure: Spot samples and urine dilution complicate data interpretation. Environ Res. 2015;142:84–95 https://www.sciencedirect.com/science/article/pii/S0013935115001887[↩]
- Lakind JS, Naiman DQ. Bisphenol A (BPA) daily intakes in the United States: Estimates from the 2003–2004 NHANES urinary BPA data. J Expo Sci Environ Epidemiol. 2008;18:608 https://www.ncbi.nlm.nih.gov/pubmed/18414515[↩]
- EFSA. Bisphenol A: EFSA launches full re-evaluation focussing on exposure and possible low dose effects. 2012. http://www.efsa.europa.eu/en/press/news/120424[↩]
- https://efsa.onlinelibrary.wiley.com/doi/pdf/10.2903/sp.efsa.2017.EN-1354[↩]
- EC 2011[↩]
- Oldring PKT, Castle L, O’Mahony C, Dixon J. Estimates of Dietary Exposure to Bisphenol A (BPA) from Light Metal Packaging using Food Consumption and Packaging usage Data: A Refined Deterministic Approach and a Fully Probabilistic (FACET) Approach. Food Additives & Contaminants Part A, Chemistry, Analysis, Control, Exposure & Risk Assessment. 2014;31(3):466-489. doi:10.1080/19440049.2013.860240. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3998095/[↩][↩]
- Hartle JC, Navas-Acien, Lawrence RS. The consumption of canned food and beverages and urinary Bisphenol A concentrations in NHANES 2003–2008. Environmental research. 2016;150:375-382. doi:10.1016/j.envres.2016.06.008. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5003675[↩][↩][↩]
- Carwile JL, Ye X, Zhou X, Calafat AM, Michels KB. Canned Soup Consumption and Urinary Bisphenol A: A Randomized Crossover Trial. Jama. 2011;306(20):2218-2220. doi:10.1001/jama.2011.1721. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3367259/[↩][↩][↩][↩][↩]
- Fourth National Report on Human Exposure to Environmental Chemicals. Centers for Disease Control and Prevention, National Center for Environmental Health; https://www.cdc.gov/exposurereport/[↩]
- Bisphenol A (BPA) Factsheet. https://www.cdc.gov/biomonitoring/BisphenolA_FactSheet.html[↩]
- Bisphenol A (BPA). https://www.niehs.nih.gov/health/topics/agents/sya-bpa/index.cfm[↩][↩][↩]
- Bisphenol A (BPA): Use in Food Contact Application. https://www.fda.gov/NewsEvents/PublicHealthFocus/ucm064437.htm[↩][↩][↩]
- Park J-S, Kim S, Park M, et al. Relationship between dietary factors and bisphenol a exposure: the second Korean National Environmental Health Survey (KoNEHS 2012–2014). Annals of Occupational and Environmental Medicine. 2017;29:42. doi:10.1186/s40557-017-0200-1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5646104/[↩][↩]
- Rudel RA, Gray JM, Engel CL, Rawsthorne TW, Dodson RE, Ackerman JM, et al. Food packaging and bisphenol a and bis(2-ethyhexyl) phthalate exposure: findings from a dietary intervention. Environ Health Perspect. 2011;119(7):914–920. doi: 10.1289/ehp.1003170 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3223004/[↩][↩]
- López-Cervantes J, Paseiro-Losada P. Determination of bisphenol a in, and its migration from, PVC stretch film used for food packaging. Food Addit Contam. 2003;20(6):596–606. doi: 10.1080/0265203031000109495 https://www.ncbi.nlm.nih.gov/pubmed/12881134[↩][↩]
- Yang M, Kim SY, Lee SM, Chang SS, Kawamoto T, Jang JY, et al. Biological monitoring of bisphenol a in a Korean population. Arch Environ Contam Toxicol. 2003;44(4):546–551. doi: 10.1007/s00244-002-2124-0 https://www.ncbi.nlm.nih.gov/pubmed/12712285[↩]





{kind=link}