Contents
What is artificial insemination
Artificial insemination also called intrauterine insemination, is a procedure for treating infertility using the process of injecting sperm directly into a woman’s uterus using a catheter, to assist conception in an infertile couple. Artificial insemination is used to treat women who have normal and healthy fallopian tubes, but for unknown reasons cannot conceive. This may be due to mechanical difficulties with intercourse – for example a man is not able to achieve an erection or has structural problems of the penis after trauma or surgery. Artificial insemination might also be used when semen has been frozen due to a male partner’s absence or prior to cancer treatment.
Sperm is retrieved from the male partner or a sperm donor and a solution with a high concentration of sperm is prepared. These sperm washing procedures are necessary to remove prostaglandins, infectious agents and antigenic proteins 1. Another substantial advantage of these techniques is the removal of nonmotile spermatozoa, either leucocytes or immature germ cells. This may be an important factor in enhancing sperm quality by a decreased release of lymphokines and/or cytokines and a reduction in the formation of free oxygen radicals after sperm preparation. Sperm preparation techniques should isolate and select sperm cells with intact functional and genetic properties, including normal morphology, minimal DNA damage, and intact cell membranes with functional binding properties. The final result is a better sperm fertilizing ability and an increasing number of motile sperm that are morphologically normal at the site of fertilization.
The solution is then injected directly into the uterus of the female partner while she is ovulating. Artificial insemination may be timed to coincide with a woman’s natural ovulation cycle however it is also commonly used in conjunction with pharmaceutically stimulated ovulation. The process of injecting sperm directly into the uterus bypasses the process through which the sperm travel from the vagina, through the cervix and cervical mucus and into a woman’s uterus and fallopian tubes, which occurs when sperm is ejaculated into a woman’s vagina during intercourse.
Artificial insemination increases the chances of conception in cases where fertility is underpinned by immotile or morphologically abnormal sperm, as it places the sperm closer to the vicinity of the egg and reduces the distance which sperm need to travel to come into contact with an egg.
Artificial insemination can also be used in cases of female factor infertility, for example in cases where a woman’s cervical mucus is thought to be ‘hostile’ to sperm (i.e. rather than aiding the entry of sperm into the cervix, the cervical mucus is thought to inhibit its entry).
Artificial insemination is also commonly used when the causes underpinning a couple’s infertility cannot be diagnosed.
Artificial insemination is a simple and cost effective alternative to more complex, costly and invasive assisted reproductive techniques (ART). While artificial insemination was easier, it was not as successful as the current procedure. Another procedure, fallopian tube sperm perfusion (FSP), uses a similar technique, but instead injects sperm directly into the fallopian tubes during ovulation, and therefore even closer to the vicinity of the egg than traditional artificial insemination (which injects sperm into the uterus). Fallopian tube sperm perfusion (FSP) is a similarly non-invasive and cost effective technique.
Artificial insemination is the oldest assisted reproductive technique and remains the most widely used worldwide. Artificial insemination techniques were first investigated in the 17th century, as a treatment for infertility related to male sexual dysfunction (e.g. the inability to ejaculate). Dutch scientists first reported conception following artificial insemination in 1742, when they successfully fertilized the eggs of fish, by artificially inseminating female fish with fish sperm. Successful conception following the artificial insemination of a mammal was first documented later that century (1780) by an Italian scientist, when a dog was successfully impregnated 1.
Why is artificial insemination done?
A couple’s ability to become pregnant depends on many different factors. Artificial insemination is used most often in couples who have:
- Donor sperm. For women who need to use donor sperm to get pregnant, artificial insemination is most commonly used to achieve pregnancy. Frozen donor sperm specimens are obtained from certified labs and thawed before the artificial insemination procedure.
- Unexplained infertility. The most common use for artificial insemination is when no cause for the infertility is found. Artificial insemination is often performed as a first treatment for unexplained infertility along with ovulation-inducing medications. Infertile women sometimes take medications (by mouth or as an injection) that cause their ovaries to mature several eggs at once. The goal is to increase the chance of pregnancy by putting more sperm in contact with more eggs.
- Endometriosis-related infertility. For infertility related to endometriosis, using medications to obtain a good quality egg along with performing artificial insemination is often the first treatment approach.
- Problems with sperm delivery. Artificial insemination can also be used for couples in which the male partner cannot become or stay erect or is not able to ejaculate effectively, or at all. For example, retrograde ejaculation is when the sperm are released backward into the bladder, instead of through the penis, at the time of male orgasm. Prior surgeries or medical conditions, such as diabetes, can cause retrograde ejaculation. Also, artificial insemination may help if the man has an abnormal urethral opening (opening of the penis).
- Mild male factor infertility (subfertility). Your partner’s semen analysis, one of the first steps in the medical assessment of infertility, may show below-average sperm concentration, weak movement (motility) of sperm, or abnormalities in sperm size and shape (morphology). artificial insemination can overcome some of these problems because preparing sperm for the procedure helps separate highly motile, normal sperm from those of lower quality.
- Cervical factor infertility. Your cervix, at the lower end of the uterus, provides the opening between your vagina and uterus. Mucus produced by the cervix around the time of ovulation provides an ideal environment for sperm to travel from your vagina to the fallopian tubes. But, if your cervical mucus is too thick, it may impede the sperm’s journey. Artificial insemination bypasses the cervix, depositing sperm directly into your uterus and increasing the number of sperm available to meet the awaiting egg.
- Cervical stenosis or abnormalities. Artificial insemination is helpful when a woman’s cervix has scarring that prevents the sperm from entering the uterus from the vagina. This may be seen in women who have had surgery on their cervix (cryosurgery, cone biopsy, Loop Electrosurgical Excision Procedure [LEEP], etc.). artificial insemination can also assist when a woman has a cervix that is shaped abnormally in a way that prevents the passage of sperm.
- Semen allergy. Rarely, a woman could have an allergy to proteins in her partner’s semen. Ejaculation into the vagina causes redness, burning and swelling where the semen contacts the skin. A condom can protect you from the symptoms, but it also prevents pregnancy. If your sensitivity is severe, artificial insemination can be effective, since many of the semen proteins are removed before the sperm is inserted.
- Lack of ovulation (anovulation). Most of the time women who do not release an egg regularly (ovulate) can become pregnant through intercourse. Sometimes, artificial insemination may be helpful.
- Fertility preservation. Men may collect and freeze (cryopreserve) their sperm for future use before having a vasectomy, testicular surgery, or radiation/chemotherapy treatment for cancer. The sperm may be thawed later and used for artificial insemination.
- Third-party reproduction. Artificial insemination is used when couples use sperm from a man who is not the woman’s partner to have a baby. This is called donor insemination (DI). Donor insemination is done when the male partner has no sperm or when the sperm quality is so low that his sperm cannot be used for conception, and in vitro fertilization (IVF) is not an option. Donor insemination can also be used if the man has certain genetic diseases that he does not want to pass on to his children. Single women or lesbian couples who want to have a baby may also consider donor insemination.
You may be offered artificial insemination if:
- you’re unable to have vaginal sex – for example, because of a physical disability or psychosexual problem
- you have a condition that means you need specific help to conceive, for example, if one of you has HIV and it’s not safe to have unprotected sex
- you’re in a same-sex relationship and haven’t got pregnant after up to six cycles of artificial insemination using donor sperm from a licensed fertility unit
Artificial insemination risks
Artificial insemination is a relatively simple and safe procedure, and the risk of serious complications is low. Risks include:
- Infection. There’s a slight risk of developing an infection as a result of the procedure.
- Spotting. Sometimes the process of placing the catheter in the uterus causes a small amount of vaginal bleeding. This doesn’t usually have an effect on the chance of pregnancy.
- Multiple pregnancy. Artificial insemination itself isn’t associated with an increased risk of a multiple pregnancy — twins, triplets or more. But, when coordinated with ovulation-inducing medications, the risk of a multiple pregnancy increases significantly. A multiple pregnancy has higher risks than a single pregnancy does, including early labor and low birth weight.
Some women have mild cramps similar to period pains, but otherwise the risks involved with artificial insemination are minimal.
If you take a fertility medicine to stimulate ovulation, there is a small risk of developing a condition called ovarian hyperstimulation syndrome. There’s also a chance that you will have more than one baby, which carries additional risks for both you and your babies.
If a woman is taking fertility medications to increase the number of eggs when she has an artificial insemination, her chance of getting pregnant with twins, triplets, or more is greater than if she were not taking fertility medications. Having an artificial insemination does not increase the risk of birth defects. The chance of birth defects in all children is 2% to 4% whether conceived naturally or from artificial insemination. The risk of developing an infection after an artificial insemination is small.
Types of artificial insemination
Artificial insemination also called intrauterine insemination, is a procedure for treating infertility using the process of injecting sperm directly into a woman’s uterus using a catheter, to assist conception in an infertile couple.
Another procedure, fallopian tube sperm perfusion (FSP), uses a similar technique, but instead injects sperm directly into the fallopian tubes during ovulation, and therefore even closer to the vicinity of the egg than traditional artificial insemination (which injects sperm into the uterus). Fallopian tube sperm perfusion (FSP) is a similarly non-invasive and cost effective technique.
Types of assisted reproductive treatment (ART)
Assisted reproductive treatment (ART), also known as assisted reproductive technology, refers to treatments used to assist people in achieving a pregnancy. ART covers a wide spectrum of treatments. Depending on the cause of infertility, the following types of treatment may be suggested.
Ovulation induction
Ovulation induction may be used by women who are not ovulating or are not ovulating regularly. Ovulation induction involves taking a hormone medication (tablet or injection), which stimulates the production of follicle-stimulating hormone. This encourages the development of one or more follicles. When the follicles are large enough, another hormone is administered which releases the egg from the follicle. If the couple has intercourse around this time, the chances of conception are greatly increased.
Donor conception
There are several ways that donor sperm, eggs or embryos can be used in ART treatments.
Donor sperm insemination
Donor sperm insemination may be used when:
- a male partner does not produce sperm,
- a male partner does not produce normal sperm, or
- there is a high risk of a man passing on a genetic disease or abnormality to a child.
Donor insemination may also be used by single women and women in same-sex relationships. The process of donor insemination is the same as artificial insemination.
Donor eggs
Treatment with donor eggs is possible if:
- a woman cannot produce eggs or her eggs are of low quality. This may occur due to age or premature ovarian failure (where the woman no longer produces mature eggs for ovulation).
- a woman has experienced several miscarriages, or
- there is a high risk of the woman passing on a genetic disease or abnormality to a child.
In these cases, the egg donor undergoes hormone stimulation to produce multiple eggs. When the eggs are mature they are retrieved and sperm from the recipient’s partner or a donor is added to the eggs. Two to five days later, when embryos are formed, an embryo is inserted into the recipient woman’s uterus. The recipient woman may take hormones in preparation for the embryo transfer, and for approximately 10 weeks after the embryos have been transferred.
Donor embryos
Donor embryos can be used if a person or couple requires donor sperm and donor eggs to achieve a pregnancy. Although rare, some people choose to donate frozen embryos that they no longer need (after in-vitro fertilization (IVF) procedures, for example) for use by others undergoing in-vitro fertilization (IVF). When the recipient woman is ready, embryos are thawed and transferred to her uterus.
In-vitro fertilization (IVF)
IVF is used in a range of circumstances to assist with conception but is often the only means of achieving pregnancy for women whose fallopian tubes are blocked. In IVF, the woman’s eggs are collected, along with sperm from the male partner or donor. The egg and sperm are left in a culture dish in the laboratory to allow the egg to be fertilized. If fertilization occurs and an embryo develops, the embryo is then placed into the woman’s uterus in a procedure called an embryo transfer. Sometimes multiple embryos may develop, and they can be frozen for use in later transfer procedures.
Gamete intrafallopian transfer (GIFT)
Gamete intrafallopian transfer (GIFT) was launched as a more ‘natural’ version of IVF. Instead of fertilization occurring in a culture dish in a laboratory, the woman’s eggs are retrieved from her ovaries and inserted between two layers of sperm in fine tubing. This tubing is then fed into one of the woman’s fallopian tubes, where the egg and sperm are left to fertilize naturally. GIFT is no longer commonly used. However, it is sometimes used as an option for couples who don’t want to use IVF for religious reasons, providing that the woman’s fallopian tubes are functioning.
Intracytoplasmic sperm injection (ICSI)
Intracytoplasmic sperm injection (ICSI) is used for the same reasons as IVF, but especially to overcome sperm problems. Essentially, ICSI follows the same process as IVF, except ICSI involves the direct injection of a single sperm into each egg to achieve fertilization.
Preimplantation genetic diagnosis
Preimplantation genetic diagnosis is used to reduce the risk or avoid transmission of a genetic disease or chromosomal abnormality. Preimplantation genetic diagnosis can be used by couples who have, or have a family history of, a genetic disease or chromosomal abnormality that they risk passing on to their children. Preimplantation genetic diagnosis is also used for couples who have had repeated miscarriages or repeated IVF failure and also for women of advanced maternal age (generally over 36-38 years of age).
In preimplantation genetic diagnosis , embryos are generated through the process of IVF or ICSI and then one or two cells are removed from the embryo and are screened for a genetic condition. Embryos unaffected by a particular genetic condition may then be selected for transfer to the woman’s uterus.
Surrogacy
Surrogacy is a form of ART in which a woman (the surrogate) carries a child for another person or couple with the intention of giving the child to that person or couple after birth.
How does artificial insemination work?
The process of artificial insemination involves insertion of a male partner’s semen through the female’s cervix and into the uterus at or just before the time of ovulation. Artificial insemination can be performed during a natural menstrual cycle or in combination with ovulation induction if the woman has irregular menstrual cycles. Only doctors can perform artificial insemination, although a person is not prevented from performing self insemination or artificial insemination at home. If a pregnancy is not achieved after a few artificial insemination attempts, the use of in-vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI) may be discussed.
Artificial insemination process
Fertility tests before artificial insemination
Before artificial insemination is carried out, you and your partner’s fertility will need to be assessed to find out why you are having difficulty conceiving and to see whether artificial insemination is suitable for you.
For a woman to have artificial insemination, her fallopian tubes (the tubes connecting the ovaries to the womb) must be open and healthy.
You and your partner won’t usually be offered artificial insemination if you have:
- unexplained infertility
- a low sperm count or poor‑quality sperm
- mild endometriosis
This is because there is some evidence to suggest that it won’t increase your chances of getting pregnant in these circumstances compared with natural attempts.
Sperm collection
If a couple decides to have artificial insemination using their own sperm, the man will be asked to provide a sperm sample at the fertility clinic by masturbating into a specimen cup. This usually happens on the same day that artificial insemination treatment takes place.
The sperm needed for artificial insemination can be collected in several ways. Most commonly, the man masturbates into a sterile glass or plastic cup that is provided by the doctor’s office or andrology laboratory, a laboratory that specializes in dealing with male health issues. Sperm can also be collected during sex in a special condom that the doctor provides. If a man has retrograde ejaculation, the sperm can be retrieved in the laboratory from urine he has collected.
Men who have a difficult time with erection or ejaculation despite using medications, as well as men with a spinal cord injury, may be able to produce a sperm sample with the help of vibratory stimulation or electroejaculation. Vibratory stimulation commonly takes place in an office and uses a handheld vibratory device. Electroejaculation uses electrical stimulation in order to produce a sperm specimen. For men with a complete spinal cord injury, electroejaculation is commonly performed in the office, while patients with an incomplete spinal cord injury may have an electroejaculation procedure performed under anesthesia in the operating room.
Once collected, the semen sample is then “washed” in the laboratory to concentrate the sperm and remove the seminal fluid (seminal fluid can cause severe cramping in the woman). This process can take up to 2 hours to complete.
Artificial insemination using donor sperm
Frozen sperm from a donor can also be used for artificial insemination, regardless of whether you are single or in a partnership, gay or straight.
All licensed fertility clinics in the US are required to screen donor sperm for infections and inherited diseases.
Some infections take a while to show, so the sperm will be frozen for six months to allow time for infections, such as HIV, to be detected.
The sperm is frozen whether it’s from someone you know or from a registered, licensed sperm bank.
Choosing to use donated sperm can be a difficult decision, and you should be offered counseling before you go ahead.
Timing your artificial insemination treatment
You may be offered artificial insemination in a natural (unstimulated) cycle or in a stimulated cycle.
To increase your chances of success, a cycle of artificial insemination should be carried out just after ovulation. Ovulation usually happens between 12 and 16 days after a woman has had their period, if you have a regular menstrual cycle. This can vary if you have an irregular menstrual cycle.
You may be given an ovulation prediction kit to help you work out the date of ovulation. An ovulation prediction kit device detects hormones released during ovulation in urine or saliva.
Otherwise, blood tests may be used to find out when you are about to ovulate.
Stimulated artificial insemination
Sometimes, fertility medicines are used to stimulate ovulation before artificial insemination. In this case, vaginal ultrasound scans are used to track the development of your eggs. As soon as an egg is mature, you’ll be given a hormone injection to stimulate its release.
Artificial insemination preparation
Intrauterine insemination involves careful coordination before the actual procedure:
- Preparing the semen sample. Your partner provides a semen sample at the doctor’s office, or a vial of frozen donor sperm can be thawed and prepared. Because nonsperm elements in semen can cause reactions in the woman’s body that interfere with fertilization, the sample will be washed in a way that separates the highly active, normal sperm from lower quality sperm and other elements. The likelihood of achieving pregnancy increases by using a small, highly concentrated sample of healthy sperm.
- Monitoring for ovulation. Because the timing of artificial insemination is crucial, monitoring for signs of impending ovulation is critical. To do this, you might use an at-home urine ovulation predictor kit that detects when your body produces a surge or release of luteinizing hormone (LH). Or, an imaging method that lets your doctor visualize your ovaries and egg growth (transvaginal ultrasound) can be done. You also may be given an injection of human chorionic gonadotropin (hCG) to make you ovulate one or more eggs at the right time.
- Determining optimal timing. Most artificial inseminations are done a day or two after detecting ovulation. Your doctor should have a plan spelled out for the timing of your artificial insemination.
During the artificial insemination procedure
The visit for intrauterine insemination takes about 15 to 20 minutes and is usually done in a doctor’s office or clinic. The artificial insemination procedure itself takes just a minute or two and requires no medications or pain relievers. Your doctor or a specially trained nurse performs the procedure.
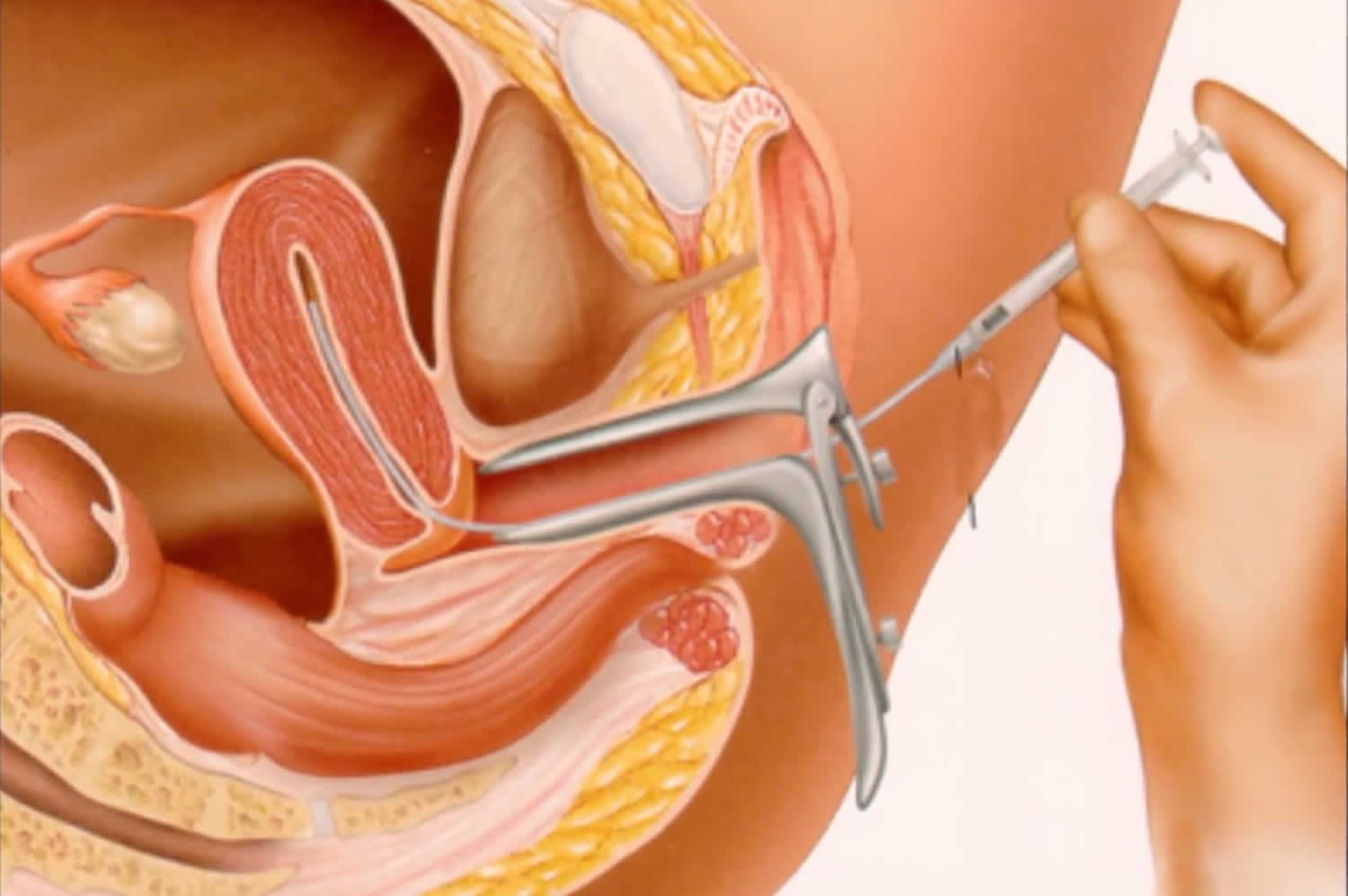
While lying on an exam table, you’ll put your legs into stirrups and a speculum will be inserted into your vagina — similar to what you experience during a Pap test. During the procedure, the doctor or nurse:
- Attaches a vial containing a sample of healthy sperm to the end of a long, thin, flexible tube (catheter)
- Inserts the catheter into your vagina, through your cervical opening and into your uterus
- Pushes the sperm sample through the tube into your uterus
- Removes the catheter, followed by the speculum
After the artificial insemination procedure
After insemination, you’ll be asked to lie on your back for a brief period. Once the procedure is over, you can get dressed and go about your normal daily activities. You may experience some light spotting for a day or two after the procedure.
Results
Wait two weeks before taking an at-home pregnancy test. Testing too soon could produce a result that is:
- False-negative. If pregnancy hormones aren’t yet at measurable levels, the test result may be negative when, in fact, you really are pregnant.
- False-positive. If you’re using ovulation-inducing medication such as HCG, the medication that’s still circulating in your body could indicate a pregnancy when you really aren’t pregnant.
Your doctor may instruct you to return about two weeks after your home kit results for a blood test, which is more sensitive in detecting pregnancy hormones after fertilization.
If you don’t become pregnant, you might try artificial insemination again before moving on to other fertility treatments. Often, the same therapy is used for three to six months to maximize chances of pregnancy.
Artificial insemination success rate
Artificial insemination success rate depends on lots of different things, including:
- the cause of infertility
- the woman’s age
- the man’s sperm count and sperm quality (using fresh sperm leads to higher conception rates than using frozen sperm)
- whether or not fertility medicines are used to stimulate ovulation (this can increase your chances of success)
There are many different factors involved, so it’s best to talk to your fertility team about your individual chances of success.
Artificial insemination works best in patients with unexplained infertility, women with a cervix that limits the passage of sperm, and men who are unable to ejaculate effectively. For example, for unexplained infertilty, the pregnancy rate with artificial insemination is double that over no treatment.
Artificial insemination does not work as well for men who produce few sperm or have slight abnormalities with their sperm and does not help women who have severe fallopian tube disease, moderate to severe endometriosis, or a history of pelvic (lower belly) infections. Other fertility treatments are better for these patients.
Overall, if artificial inseminations are performed every month with fresh or frozen sperm, success rates can be better. The success rates depend on whether fertility medications are used, age of the woman, and infertility diagnosis, as well as other factors.
How much is it for artificial insemination?
Costs range from about $800 to $1,300 for each cycle of artificial insemination treatment.





{kind=link}