
Contents
Ataxia with Vitamin E Deficiency
Ataxia with vitamin E deficiency (AVED), also known as Familial Isolated Vitamin E deficiency, Isolated Vitamin E deficiency or Friedreich-like ataxia with vitamin E deficiency, is a rare progressive neurodegenerative disorder of autosomal recessive cerebellar ataxia (ARCA) 1, 2, 3, 4, 5, 6. The most prominent symptoms of ataxia with vitamin E deficiency (AVED) include progressive cerebellar ataxia (difficulty coordinating movements), slurred speech (dysarthria), numbness in the hands and feet (peripheral neuropathy), absence of neurologic reflexes (areflexia), and progressive leg weakness 4. Ataxia with vitamin E deficiency (AVED) patients may also have retinitis pigmentosa (a group of rare eye diseases that affect the retina that causes severe vision impairment such as decreased vision at night or in low light and loss of side vision (tunnel vision)), a disease of the heart muscle (cardiomyopathy) and scoliosis (a sideways curvature of the spine) 7, 8. Ataxia with vitamin E deficiency (AVED) symptoms typically begin during childhood or adolescence and worsen with age, resulting in the need for a wheelchair by early adulthood 9. Vitamin E supplementation may prevent the worsening of the condition of patients with ataxia with vitamin E deficiency (AVED).
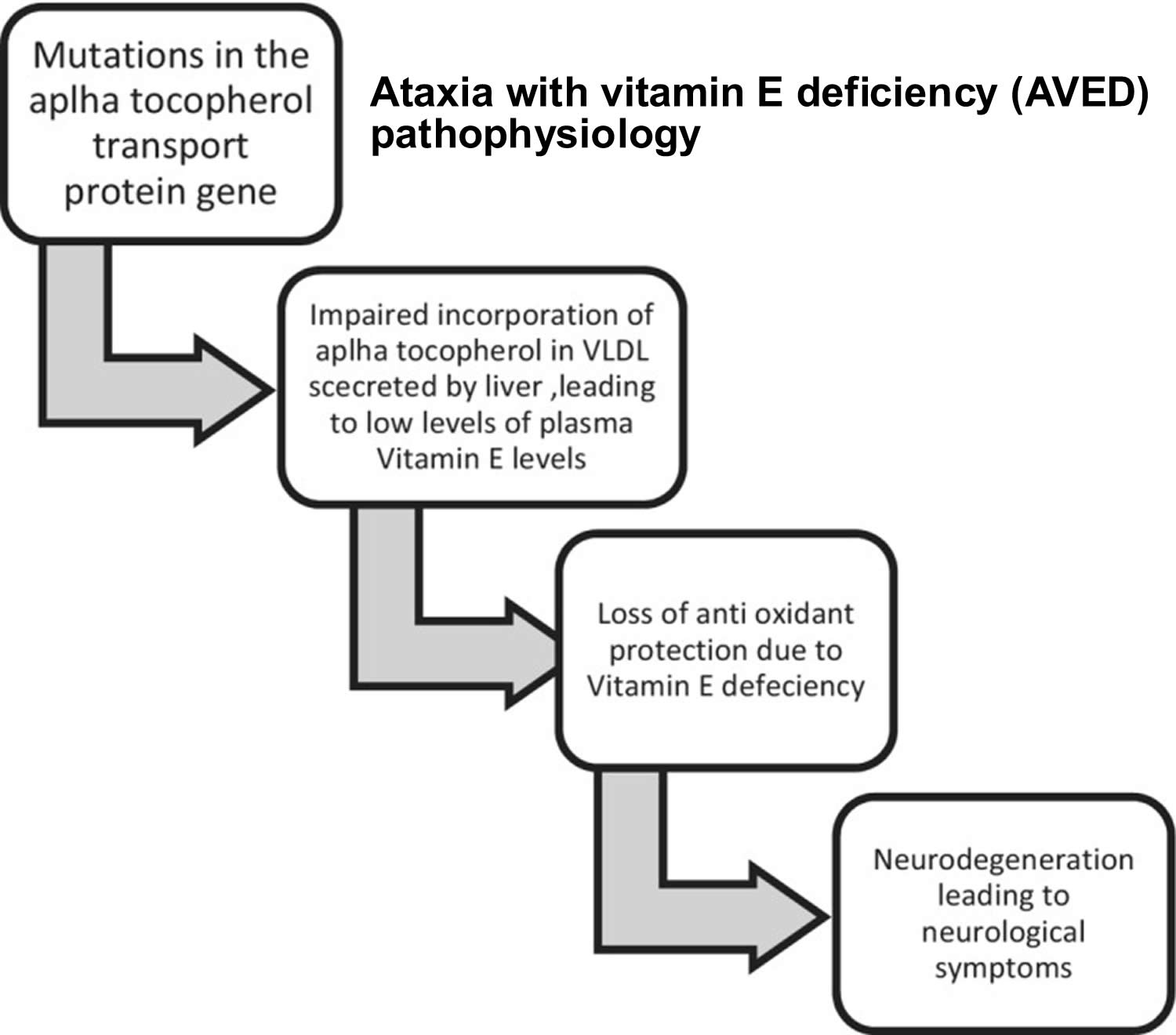
Ataxia with vitamin E deficiency (AVED) is caused by mutations in the alpha-tocopherol transfer protein (TTPA) gene, which encodes the alpha-tocopherol transfer protein (α-TTP), which in turn binds alpha-tocopherol and transports vitamin E from liver cells to circulating lipoproteins 10. More than 20 mutations in the TTPA gene have been found to cause ataxia with vitamin E deficiency 11. Some of these TTPA mutations cause no functional protein to be made, while others change a single protein building block (amino acid) in the alpha-tocopherol transfer protein (α-TTP), reducing its function 11. As a result, the body cannot retain or use dietary vitamin E, which leads to reduced levels of vitamin E in your blood and the accumulation of free radicals. Mutations in the TTPA gene that cause no functional alpha-tocopherol transfer protein (α-TTP) to be made are associated with a severe form of ataxia that begins at a young age 11. Mutations that reduce but do not eliminate the alpha-tocopherol transfer protein (α-TTP) function are associated with milder ataxia that occurs at a later age and progresses more slowly. One TTPA gene mutation that is found in the Japanese population changes the amino acid histidine to the amino acid glutamine at position 101 in the αTTP protein (written as His101Glu or H101Q). This mutation is associated with the development of an eye disorder called retinitis pigmentosa that causes vision loss in people with ataxia with vitamin E deficiency 11.
Ataxia with vitamin E deficiency (AVED) affects both males and females equally. Ataxia with vitamin E deficiency (AVED) is estimated to occur in fewer than 1 in 1,000,000 people 12. North African populations are most affected with AVED. Other cases have been reported in the Mediterranean region and Northern European countries. There have been cases in Asian countries such as Japan, China and the Philippines. The onset of AVED can occur during childhood or adulthood with cases reported ranging in children as young as 2 and adults as old as 52. Typically, the disease presents in individuals between ages 5 and 20 years. The disorder was first described in the medical literature in 1981.
Untreated ataxia with vitamin E deficiency (AVED) generally manifests between ages 5 and 15 years 3. The first signs and symptoms include progressive ataxia, clumsiness of the hands, loss of proprioception, and absence of neurologic reflexes (areflexia). Other features often observed are dysdiadochokinesia, dysarthria, positive Romberg sign, head titubation, decreased visual acuity, and positive Babinski sign 3. Although age of onset and disease course are more uniform within a given family, disease manifestations and their severity can vary even among siblings.
Ataxia with vitamin E deficiency (AVED) is caused by alpha-tocopherol transfer protein (TTPA) gene mutations on chromosome 8q13 (long arm of chromosome 8), which encodes the alpha-tocopherol transfer protein (α-TTP), which in turn binds alpha-tocopherol and transports vitamin E from liver cells to circulating lipoproteins 13, 14, 15, 16, 17, 18, 19, 20, 21. When the alpha-tocopherol transfer protein (TTPA) gene is damaged, vitamin E cannot be distributed throughout the body. Vitamin E is important because it protects the cells of the neurological system (neurons) from damaging molecules called free radicals. Ataxia with vitamin E deficiency (AVED) is inherited in an autosomal recessive manner 10.
Marriotti et al. 22 reported cerebellar atrophy in some individuals with AVED. Spinal sensory demyelination with neuronal atrophy and axonal spheroids and neuronal lipofuscin accumulation in the third cortical layer of the cerebral cortex, thalamus, lateral geniculate body, spinal horns, and posterior root ganglia are the commonest histopathology findings 23. The following criteria should be met to diagnose ataxia with vitamin E deficiency (AVED) 24:
- Friedreich ataxia‐like neurologic phenotype
- Markedly reduced plasma vitamin E
- Normal lipoprotein profile
- Exclusion of disease that cause fat malabsorption.
Individuals with AVED are treated with high doses of vitamin E supplements, but recovery is slow and incomplete 25. Early diagnosis and treatment can slow down or stop the progression of the disorder and in some people, even improve existing symptoms. Lifelong treatment with vitamin E will be needed. Genetic counseling is recommended for affected individuals and their families.
Vitamin E supplementation should be started as soon as possible, but the optimal dosage is still variable 24. The doses and the route of vitamin E supplementation depend on the causes of vitamin E deficiency. The treatment of choice for AVED is lifelong high‐dose oral vitamin E supplementation. The early use of vitamin E supplementation in the disease process helps to reverse some neurological symptoms like ataxia and intellectual deterioration 26.
Figure 1. Ataxia with vitamin E deficiency (AVED) pathophysiology
Ataxia with Vitamin E Deficiency causes
Ataxia with vitamin E deficiency (AVED) is caused by changes (mutations or pathogenic variants) in the TTPA gene, which provides instructions to synthesize the alpha-tocopherol transfer protein (αTTP) 27. Alpha-tocopherol transfer protein (αTTP) controls the distribution and transportation of vitamin E from the liver to other cells and tissues throughout the body, including the brain. Individuals with AVED have non-working genes for TTPA and therefore, vitamin E cannot be properly distributed throughout the body especially to the brain where it is necessary for proper function. AVED is characterized by very low levels of vitamin E in the blood and tissues in the brain. Without normal levels of vitamin E in the tissues, an individual with AVED experiences damage to the body from lack of protection from damaging free radicals.
The mechanism of neurologic dysfunction in AVED is unknown, but neuronal oxidative injury has been hypothesized 1. Brain imaging demonstrates cerebellar atrophy in up to 50% of cases 14, 28. Other brain regions are also affected. Animal models of AVED and post-mortem studies of humans with secondary vitamin E deficiency have shown evidence of degenerative changes in the substantia nigra, posterior column, nerve roots, and peripheral nervous system 29, 30, 31, 32, 33, 34, 35:915–936. doi: 10.4049/jimmunol.0903008)). Post-mortem studies of patients with AVED demonstrate loss of cerebellar Purkinje cells, dying back-type posterior column degeneration with spheroids and corpora amylacea, and lipofuscin accumulation 36, 37. Ataxia in AVED is likely caused by a combination of cerebellar and posterior column degeneration 1.
Ataxia with vitamin E deficiency (AVED) is inherited, or passed down from parent to child, in an autosomal recessive manner. Recessive genetic disorders occur when an individual inherits a non-working gene from each parent. If an individual receives one working gene and one non-working gene for the disease, the person will be a carrier for the disease, but usually will not show symptoms. The risk for two carrier parents to both pass the non-working gene and, therefore, have a child with AVED is 25% with each pregnancy. The risk of having a child who is a carrier, like the parents, is 50% with each pregnancy. The chance for a child to receive working genes from both parents is 25%. The risk is the same for males and females.
Ataxia with vitamin E deficiency inheritance pattern
Ataxia with vitamin E deficiency (AVED) is inherited in an autosomal recessive pattern, which means both copies of the TTPA gene in each cell have mutations. The parents of an individual with ataxia with vitamin E deficiency (AVED) each carry one copy of the mutated gene, but they typically do not have any health problems associated with the condition.
It is rare to see any history of autosomal recessive conditions within a family because if someone is a carrier for one of these conditions, they would have to have a child with someone who is also a carrier for the same condition. Autosomal recessive conditions are individually pretty rare, so the chance that you and your partner are carriers for the same recessive genetic condition are likely low. Even if both partners are a carrier for the same condition, there is only a 25% chance that they will both pass down the non-working copy of the gene to the baby, thus causing a genetic condition. This chance is the same with each pregnancy, no matter how many children they have with or without the condition.
- If both partners are carriers of the same abnormal gene, they may pass on either their normal gene or their abnormal gene to their child. This occurs randomly.
- Each child of parents who both carry the same abnormal gene therefore has a 25% (1 in 4) chance of inheriting a abnormal gene from both parents and being affected by the condition.
- This also means that there is a 75% ( 3 in 4) chance that a child will not be affected by the condition. This chance remains the same in every pregnancy and is the same for boys or girls.
- There is also a 50% (2 in 4) chance that the child will inherit just one copy of the abnormal gene from a parent. If this happens, then they will be healthy carriers like their parents.
- Lastly, there is a 25% (1 in 4) chance that the child will inherit both normal copies of the gene. In this case the child will not have the condition, and will not be a carrier.
These possible outcomes occur randomly. The chance remains the same in every pregnancy and is the same for boys and girls.
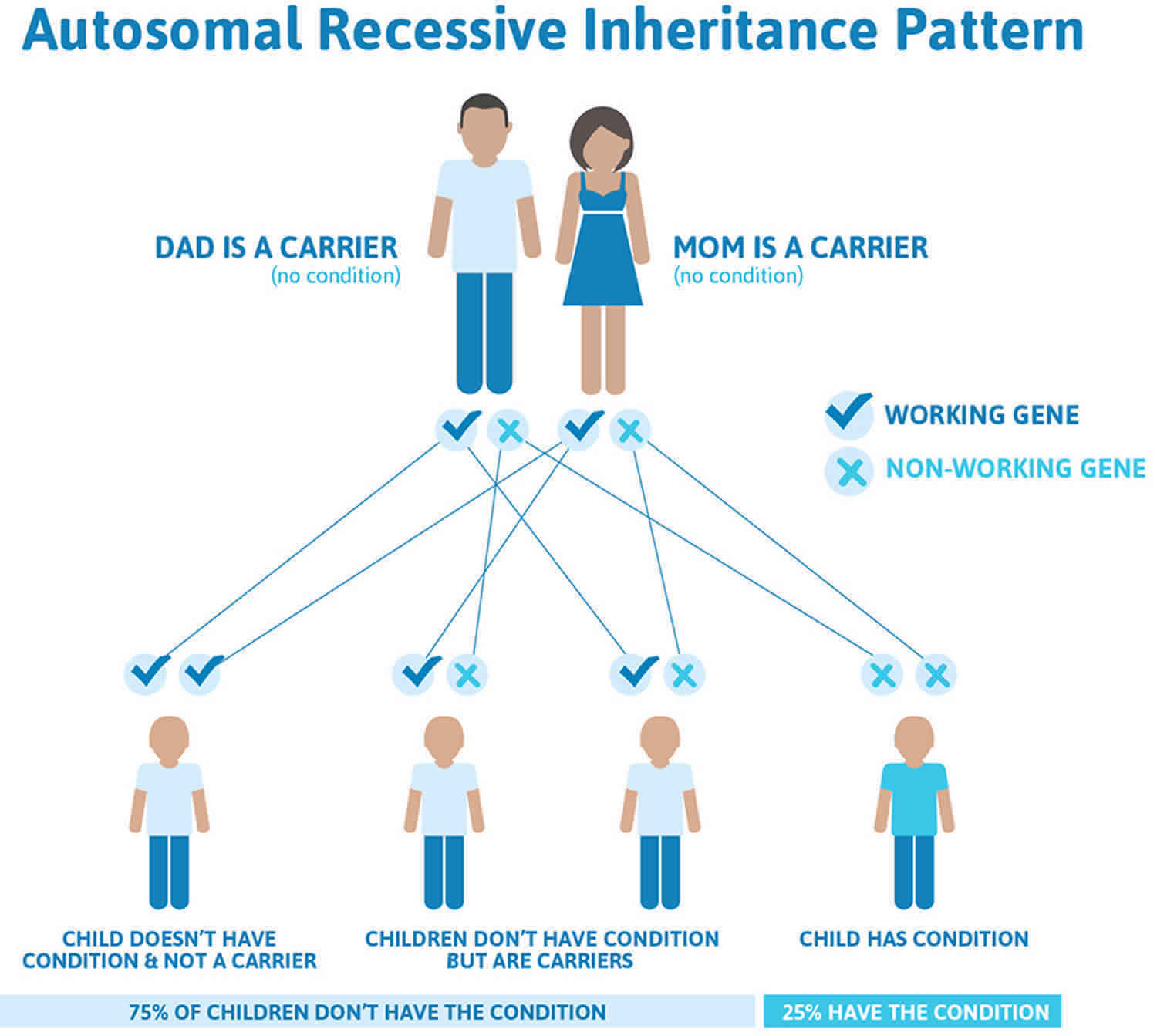
Figure 2 illustrates autosomal recessive inheritance. The example below shows what happens when both dad and mum is a carrier of the abnormal gene, there is only a 25% chance that they will both pass down the abnormal gene to the baby, thus causing a genetic condition.
Figure 2. Ataxia with vitamin E deficiency autosomal recessive inheritance pattern
People with specific questions about genetic risks or genetic testing for themselves or family members should speak with a genetics professional.
Resources for locating a genetics professional in your community are available online:
- The National Society of Genetic Counselors (https://www.findageneticcounselor.com/) offers a searchable directory of genetic counselors in the United States and Canada. You can search by location, name, area of practice/specialization, and/or ZIP Code.
- The American Board of Genetic Counseling (https://www.abgc.net/about-genetic-counseling/find-a-certified-counselor/) provides a searchable directory of certified genetic counselors worldwide. You can search by practice area, name, organization, or location.
- The Canadian Association of Genetic Counselors (https://www.cagc-accg.ca/index.php?page=225) has a searchable directory of genetic counselors in Canada. You can search by name, distance from an address, province, or services.
- The American College of Medical Genetics and Genomics (http://www.acmg.net/ACMG/Genetic_Services_Directory_Search.aspx) has a searchable database of medical genetics clinic services in the United States.
Ataxia with Vitamin E Deficiency signs and symptoms
Individuals usually show symptoms between 5 and 20 years of age. Symptoms and the severity of ataxia with vitamin E deficiency (AVED) may be different from person to person. Without treatment, symptoms may get worse as the person grows older.
Table 1. Untreated individuals with Ataxia with Vitamin E Deficiency
| Signs and symptoms | % of Persons with signs and symptoms | ||
|---|---|---|---|
| Cerebellar involvement | Gait impairment | 93.4% | |
| Dysarthria Dysarthria occurs when the muscles you use for speech are weak or you have difficulty controlling them. Dysarthria often causes slurred or slow speech that can be difficult to understand. | 61.8% | ||
| Head titubation (involuntary tremor or uncontrollable rhythmic shaking that occurs in the head) | 33% | ||
| Nystagmus | 5.3% | ||
| Lower motor neuron involvement | Areflexia | 94.7% | |
| Deep sensory disturbances | 67.1% | ||
| Upper motor neuron involvement | Babinski sign | 85.5% | |
| Urinary urgency | 22.4% | ||
| Pigmentary retinopathy | 2.3% | ||
| Cardiomyopathy | 1.5% | ||
Footnote: Frequency of signs and symptoms associated with untreated individuals with ataxia with vitamin E deficiency (AVED) based on findings in 132 individuals of North African heritage.
[Source 5 ]AVED affects the brain and spinal cord (central nervous system or CNS) as well as the motor and sensory nerves that connect the central nervous system (CNS) to the rest of the body (peripheral nervous system) 12. This results in ataxia, which is difficulty controlling body movements and numbness of the hands and feet (peripheral neuropathy). Individuals with AVED develop increasing weakness of the legs, which may appear as an unsteady or staggering way of walking (gait) or trembling when standing still 12. If symptoms become very severe, an individual with AVED may require a wheelchair if they cannot walk 12. Clinical symptoms like progressive ataxia with decreased reflex remain the prominent symptoms of AVED. According to the study done in North Africa, most of the individuals with AVED had mild neuropathy and were mostly combined types of neuropathies (both sensory and motor) 38.
Additional symptoms related to the central nervous system (CNS) include loss of proprioception, which is an awareness of joint position in relation to other parts of the body 12. With time, reflexes in the legs may slow down or be absent (areflexia). Involvement of the throat muscles may lead to impaired swallowing or choking and may cause difficulty in eating. Slurred speech or difficulty speaking (dysarthria) may also be present. Some affected individuals may develop a tremor or shaking of the head (titubation). Intellect and emotions are rarely affected.
In some people with AVED, psychotic episodes and intellectual decline have been described 3. In rare individuals, school performance declines secondary to loss of intellectual capacities 3.
In addition to neurological symptoms, individuals with AVED may develop symptoms affecting other systems of the body including the eyes 12. Retinitis pigmentosa (RP) is a large group of rare eye diseases that cause progressive degeneration of the membrane lining the eyes (retina). This results in visual impairment or decreased vision. A high percentage of affected individuals (e.g., 8/11 individuals in one series) experience decreased visual acuity 8. Some affected individuals may have yellow “fatty” deposits (xanthelasma) in the retina.
Affected individuals may also develop sideways curvature of the spine (scoliosis), degenerative changes of the heart muscle (cardiomyopathy) or “fatty” deposits (xanthomas) affecting the Achilles tendon around the ankle 12.
Some individuals with ataxia with vitamin E deficiency (AVED) may experience a form of dystonia 39, 1. Dystonia is the name for a group of movement disorders generally characterized by involuntary muscle contractions that force the body into abnormal, sometimes painful, movements and positions (postures). These contractions result in twisting and repetitive movements. Dystonia can affect just one muscle, a group of muscles or all of your muscles. Symptoms can include tremors, voice problems or a dragging foot. Symptoms often start in childhood. They can also start in the late teens or early adulthood. Some cases worsen over time. Others are mild.
Ataxia with Vitamin E Deficiency diagnosis
A diagnosis of ataxia with vitamin E deficiency (AVED) is made upon a thorough clinical evaluation, a detailed patient history, and a variety of tests and characteristic findings (e.g., low levels of vitamin E with normal levels of lipoproteins and lipids with no evidence of fat malabsorption and abnormalities in the TTPA gene).
AVED should be suspected in an individual with the following clinical and laboratory findings and family history 3:
- Family history
- Family history is consistent with autosomal recessive inheritance (e.g., affected sibs and/or parental consanguinity). Absence of a known family history does not preclude the diagnosis.
- Clinical features
- Onset between ages 5 and 15 years
- Progressive cerebellar findings including the following:
- Gait ataxia
- Clumsiness of the hands
- Loss of proprioception (especially distal joint position and vibration sense)
- Dysdiadochokinesia
- Positive Romberg sign
- Head titubation
- Lower motor neuron involvement. Areflexia
- Upper motor neuron involvement. Positive Babinski sign
- Ophthalmologic involvement. Decreased visual acuity due to macular degeneration, pigmentary retinopathy
- Supportive laboratory findings
- Normal lipid and lipoprotein profile
- Very low plasma vitamin E (alpha-tocopherol, or α-tocopherol) concentration
- Note: There is no universal normal range of plasma vitamin E concentration, as it depends on the test method and varies among laboratories.
- In Finckh et al 40, the plasma vitamin E (alpha-tocopherol, or α-tocopherol) concentration normal range lies between 9.0 and 29.8 µmol/L. In El Euch-Fayache et al 5, the normal range is given as 16.3-34.9 µmol/L, while individuals with AVED had vitamin E levels between 0.00 and 3.76 µmol/L (mean 0.95 µmol/L). In individuals with AVED, the plasma vitamin E concentration is generally lower than 4.0 µmol/L (<1.7 mg/L) 16, 14.
- Because oxidation of alpha-tocopherol (α-tocopherol) by air may invalidate test results, the following precautions with a blood sample should be taken:
- Centrifugation of the EDTA blood soon after venipuncture
- Quick separation of plasma from blood cells after centrifugation and subsequent flash freezing of the plasma in liquid nitrogen
- Filling the space above the plasma with an inert gas (e.g., argon or nitrogen)
- Protecting the sample from light by wrapping the container in aluminum foil, or using a black or light-shielded Eppendorf tube
- Shipment of the sample to the test laboratory in dry ice
- Electrophysiologic findings
- No electrophysiologic findings (motor nerve conduction velocities, compound muscle action potentials, or nerve sensory action potentials) are specific to or diagnostic of AVED; even the presence of a severe neuropathy does not exclude the diagnosis of AVED.
- Somatosensory evoked potentials show increased central conduction time between the segment C1 (N13b) and the sensorimotor cortex (N20) and increased latencies of the N20 (median nerve) and P40 (tibial nerve) waves. The P40 wave may be missing completely 26.
- Neuroimaging
The diagnosis of ataxia with vitamin E deficiency (AVED) is established by molecular genetic testing with the identification of abnormalities in the TTPA gene 3.
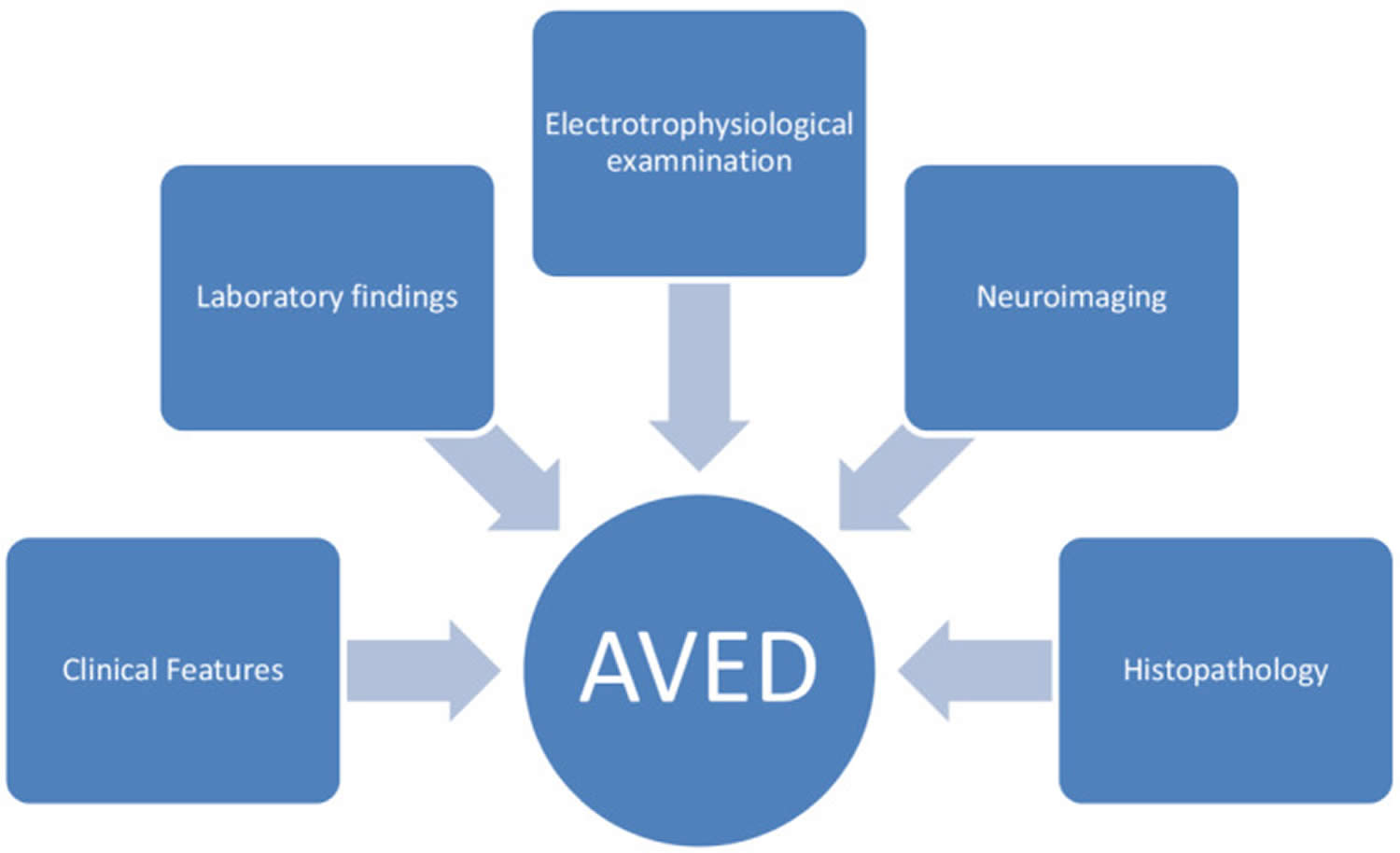
Figure 3. Ataxia with vitamin E deficiency (AVED) diagnosis
Ataxia with Vitamin E Deficiency (AVED) treatment
Individuals with ataxia with vitamin E deficiency (AVED) are treated with high doses of vitamin E supplements. Early diagnosis and treatment can slow down or stop the progression of the disorder and in some people, even improve existing symptoms. The treatment of choice for ataxia with vitamin E deficiency (AVED) is lifelong high-dose oral vitamin E supplementation. With treatment, plasma vitamin E concentrations can become normal. Genetic counseling is recommended for affected individuals and their families.
One of the following vitamin E preparations is used 3:
- The chemically manufactured racemic form, all-rac-alpha-tocopherol acetate
- The naturally occurring form, RRR-alpha-tocopherol
- It is currently unknown whether affected individuals should be treated with all-rac-alpha-tocopherol acetate or with RRR-alpha-tocopherol. It is known that alpha-tocopherol transfer protein (α-TTP) stereoselectively binds and transports 2R-alpha-tocopherols 42, 43, 44. For some TTPA pathogenic variants, this stereoselective binding capacity is lost and affected individuals cannot discriminate between RRR- and SRR-alpha-tocopherol 18, 16. In this instance, affected individuals would also be able to incorporate non-2R-alpha-tocopherol stereoisomers into their bodies if they were supplemented with all-rac-alpha-tocopherol. Since potential side effects of the synthetic stereoisomers have not been studied in detail, it seems appropriate to treat with RRR-alpha-tocopherol, despite the higher cost.
When vitamin E treatment is initiated in presymptomatic individuals (e.g., younger age), manifestations of ataxia with vitamin E deficiency (AVED) do not develop 45, 5.
No large-scale therapeutic studies have been performed to determine optimal vitamin E dosage and to evaluate outcomes 3. The reported vitamin E dose ranges from 800 mg to 1,500 mg (or 40 mg/kg body weight in children) 46, 47, 45, 16, 26, 48, 28, 14. The ideal dose of vitamin E ranges from 800 mg to 1500 mg (40 mg/kg/day) in children 22, 25.
Periodic follow‐up is required during vitamin E therapy. The plasma concentration of vitamin E should be measured in regular intervals, usually, every 6 months to maintain the level of vitamin E in the high normal range especially in children. Ideally the plasma vitamin E concentration should be maintained in the high-normal range 3.
Individuals with AVED should avoid smoking and occupations requiring quick responses or good balance. Smoking reduces the total radical trapping antioxidant parameter of plasma (TRAP), which is regarded as the best prognostic marker during the supplementation of vitamin E, leading to the reduction in plasma vitamin level 49.
Symptomatic individuals
Some clinical signs and symptoms (e.g., ataxia and intellectual deterioration) can be reversed in symptomatic individuals if treatment is initiated early in the disease process 26.
In older individuals, disease progression can be stopped, but deficits in proprioception and gait unsteadiness generally remain 28, 14, 5.
Supportive Care
The goals of supportive care in those with clinical signs and symptoms of AVED are to maximize function and reduce complications. Depending on the clinical signs and symptoms, it is recommended that each individual be managed by a multidisciplinary team of relevant specialists such as neurologists, occupational therapists, physical therapists, physiatrists, orthopedists, nutritionists, speech-language pathologists, pulmonologists, and mental health specialists 3.
Pregnancy Management
Because reduced vitamin E levels are associated with low fertility and embryo resorption in mice 50 and α-tocopherol transfer protein is highly expressed in the human placenta 51, it is advisable for women with AVED to maintain vitamin E levels in the high-normal range during pregnancy 3.
Ataxia with Vitamin E Deficiency prognosis
Ataxia with Vitamin E Deficiency (AVED) prognosis despite the supplementation of vitamin E depends on the timing of the supplementation and the age of the onset of vitamin E deficiency. Vitamin E treatment in pre‐symptomatic individuals with a history of family cases of AVED can help to prevent the individual from primary manifestations. The symptoms do not develop in the individuals with the initiation of vitamin E earlier in pre‐symptomatic individuals who are at risk 52, 14, 28. Older individuals usually remain deficient in proprioception and gait unsteadiness although the progression of the disease can be stopped with vitamin E supplementation 38.
Without treatment, most patients with ataxia with vitamin E deficiency (AVED) disease onset during childhood (age <18 years) become wheelchair-bound within 5–20 years of disease onset 1.
The specific response of dystonia in AVED to vitamin E treatment is variable 1. Dystonia has been reported to improve in two patients 14, 39 and most patients with dystonia as a feature of their disease had stabilization or improvement of their other symptoms on high dose vitamin E 1. One patient, however, experienced progressive dystonia despite escalating doses of vitamin E supplementation 53. There are anecdotal reports of dystonia improvement in response to symptomatic treatment with botulinum toxin, trihexyphenidyl and clonazepam 53, 39.
- Becker AE, Vargas W, Pearson TS. Ataxia with Vitamin E Deficiency May Present with Cervical Dystonia. Tremor Other Hyperkinet Mov (N Y). 2016 May 17;6:374. doi: 10.7916/D8B85820[↩][↩][↩][↩][↩][↩][↩]
- Elkamil A, Johansen KK, Aasly J. Ataxia with vitamin e deficiency in norway. J Mov Disord. 2015 Jan;8(1):33-6. doi: 10.14802/jmd.14030[↩]
- Schuelke M. Ataxia with Vitamin E Deficiency. 2005 May 20 [Updated 2023 Mar 16]. In: Adam MP, Mirzaa GM, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1241[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Zhang LW, Liu B, Peng DT. Clinical and genetic study of ataxia with vitamin E deficiency: A case report. World J Clin Cases. 2022 Aug 16;10(23):8271-8276. doi: 10.12998/wjcc.v10.i23.8271[↩][↩]
- El Euch-Fayache G, Bouhlal Y, Amouri R, Feki M, Hentati F. Molecular, clinical and peripheral neuropathy study of Tunisian patients with ataxia with vitamin E deficiency. Brain. 2014 Feb;137(Pt 2):402-10. doi: 10.1093/brain/awt339[↩][↩][↩][↩][↩]
- Hamza W, Ali Pacha L, Hamadouche T, Muller J, Drouot N, Ferrat F, Makri S, Chaouch M, Tazir M, Koenig M, Benhassine T. Molecular and clinical study of a cohort of 110 Algerian patients with autosomal recessive ataxia. BMC Med Genet. 2015 Jun 12;16:36. doi: 10.1186/s12881-015-0180-3[↩]
- Esmer C, Salazar MA, Rentería PE, Bravo OA. Clinical and molecular findings in a patient with ataxia with vitamin E deficiency, homozygous for the c.205-1G>C mutation in the TTPA gene. Bol Med Hos Infant Mex. 2013;70:313–317.[↩]
- Benomar A, Yahyaoui M, Meggouh F, Bouhouche A, Boutchich M, Bouslam N, Zaim A, Schmitt M, Belaidi H, Ouazzani R, Chkili T, Koenig M. Clinical comparison between AVED patients with 744 del A mutation and Friedreich ataxia with GAA expansion in 15 Moroccan families. J Neurol Sci. 2002 Jun 15;198(1-2):25-9. doi: 10.1016/s0022-510x(02)00057-6[↩][↩]
- Ataxia with vitamin E deficiency. https://rarediseases.info.nih.gov/diseases/8595/ataxia-with-vitamin-e-deficiency[↩]
- Chung S, Ghelfi M, Atkinson J, Parker R, Qian J, Carlin C, Manor D. Vitamin E and Phosphoinositides Regulate the Intracellular Localization of the Hepatic α-Tocopherol Transfer Protein. J Biol Chem. 2016 Aug 12;291(33):17028-39. doi: 10.1074/jbc.M116.734210[↩][↩]
- TTPA gene. https://medlineplus.gov/genetics/gene/ttpa[↩][↩][↩][↩]
- Ataxia with Vitamin E Deficiency. https://rarediseases.org/rare-diseases/ataxia-with-vitamin-e-deficiency[↩][↩][↩][↩][↩][↩][↩]
- Ouahchi K, Arita M, Kayden H, Hentati F, Ben Hamida M, Sokol R, Arai H, Inoue K, Mandel JL, Koenig M. Ataxia with isolated vitamin E deficiency is caused by mutations in the alpha-tocopherol transfer protein. Nat Genet. 1995 Feb;9(2):141-5. doi: 10.1038/ng0295-141[↩]
- Mariotti C, Gellera C, Rimoldi M, Mineri R, Uziel G, Zorzi G, Pareyson D, Piccolo G, Gambi D, Piacentini S, Squitieri F, Capra R, Castellotti B, Di Donato S. Ataxia with isolated vitamin E deficiency: neurological phenotype, clinical follow-up and novel mutations in TTPA gene in Italian families. Neurol Sci. 2004 Jul;25(3):130-7. doi: 10.1007/s10072-004-0246-z[↩][↩][↩][↩][↩][↩][↩][↩]
- Gotoda T, Arita M, Arai H, Inoue K, Yokota T, Fukuo Y, Yazaki Y, Yamada N. Adult-onset spinocerebellar dysfunction caused by a mutation in the gene for the alpha-tocopherol-transfer protein. N Engl J Med. 1995 Nov 16;333(20):1313-8. doi: 10.1056/NEJM199511163332003[↩]
- Cavalier L, Ouahchi K, Kayden HJ, Di Donato S, Reutenauer L, Mandel JL, Koenig M. Ataxia with isolated vitamin E deficiency: heterogeneity of mutations and phenotypic variability in a large number of families. Am J Hum Genet. 1998 Feb;62(2):301-10. doi: 10.1086/301699[↩][↩][↩][↩]
- Sokol RJ. Vitamin E deficiency and neurologic disease. Annu Rev Nutr. 1988;8:351-73. doi: 10.1146/annurev.nu.08.070188.002031[↩]
- Traber MG, Sokol RJ, Kohlschütter A, Yokota T, Muller DP, Dufour R, Kayden HJ. Impaired discrimination between stereoisomers of alpha-tocopherol in patients with familial isolated vitamin E deficiency. J Lipid Res. 1993 Feb;34(2):201-10.[↩][↩]
- Yokota T, Shiojiri T, Gotoda T, Arai H. Retinitis pigmentosa and ataxia caused by a mutation in the gene for the alpha-tocopherol-transfer protein. N Engl J Med. 1996 Dec 5;335(23):1770-1. doi: 10.1056/NEJM199612053352315[↩]
- Yokota T, Shiojiri T, Gotoda T, Arita M, Arai H, Ohga T, Kanda T, Suzuki J, Imai T, Matsumoto H, Harino S, Kiyosawa M, Mizusawa H, Inoue K. Friedreich-like ataxia with retinitis pigmentosa caused by the His101Gln mutation of the alpha-tocopherol transfer protein gene. Ann Neurol. 1997 Jun;41(6):826-32. doi: 10.1002/ana.410410621[↩]
- Yokota T, Uchihara T, Kumagai J, Shiojiri T, Pang JJ, Arita M, Arai H, Hayashi M, Kiyosawa M, Okeda R, Mizusawa H. Postmortem study of ataxia with retinitis pigmentosa by mutation of the alpha-tocopherol transfer protein gene. J Neurol Neurosurg Psychiatry. 2000 Apr;68(4):521-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1736898/pdf/v068p00521.pdf[↩]
- Mariotti C, Gellera C, Rimoldi M, et al. Ataxia with isolated vitamin E deficiency: neurological phenotype, clinical follow‐up and novel mutations in TTPA gene in Italian families. Neurol Sci. 2004;25(3):130‐137. doi: 10.1007/s10072-004-0246-z[↩][↩]
- Ulatowski L, Parker R, Warrier G, Sultana R, Butterfield DA, Manor D. Vitamin E is essential for Purkinje neuron integrity. Neuroscience. 2014;260:120‐129. doi: 10.1016/j.neuroscience.2013.12.001[↩]
- Thapa S, Shah S, Chand S, Sah SK, Gyawali P, Paudel S, Khanal P. Ataxia due to vitamin E deficiency: A case report and updated review. Clin Case Rep. 2022 Sep 6;10(9):e6303. doi: 10.1002/ccr3.6303[↩][↩][↩][↩]
- Gabsi S, Gouider‐Khouja N, Belal S, et al. Effect of vitamin E supplementation in patients with ataxia with vitamin E deficiency. Eur J Neurol. 2001;8(5):477‐481. doi: 10.1046/j.1468-1331.2001.00273.x[↩][↩]
- Schuelke M, Mayatepek E, Inter M, Becker M, Pfeiffer E, Speer A, Hübner C, Finckh B. Treatment of ataxia in isolated vitamin E deficiency caused by alpha-tocopherol transfer protein deficiency. J Pediatr. 1999 Feb;134(2):240-4. doi: 10.1016/s0022-3476(99)70424-5[↩][↩][↩][↩]
- Di Donato I, Bianchi S, Federico A. Ataxia with vitamin E deficiency: update of molecular diagnosis. Neurol Sci. 2010 Aug;31(4):511-5. doi: 10.1007/s10072-010-0261-1[↩]
- Gabsi S, Gouider-Khouja N, Belal S, Fki M, Kefi M, Turki I, Ben Hamida M, Kayden H, Mebazaa R, Hentati F. Effect of vitamin E supplementation in patients with ataxia with vitamin E deficiency. Eur J Neurol. 2001 Sep;8(5):477-81. doi: 10.1046/j.1468-1331.2001.00273.x[↩][↩][↩][↩]
- Dexter DT, Nanayakkara I, Goss-Sampson MA, et al. Nigral dopaminergic cell loss in vitamin E deficient rats. Neuroreport. 1994;5:1773–1776. doi: 10.1097/00001756-199409080-00022[↩]
- Geller A, Gilles F, Shwachman H. Degeneration of fasciculus gracilis in cystic fibrosis. Neurology. 1977;27:185–187. doi: 10.1212/WNL.27.2.185[↩]
- Nelson JS, Fitch CD, Fischer VW, Broun GO, Chou AC. Progressive neuropathologic lesions in vitamin E-deficient rhesus monkeys. J Neuropathol Exp Neurol. 1981;40:166–186. doi: 10.1097/00005072-198103000-00008[↩]
- Rosenblum JL, Keating JP, Prensky AL, Nelson JS. A progressive neurologic syndrome in children with chronic liver disease. N Engl J Med. 1981;304:503–508. doi: 10.1056/NEJM198102263040902[↩]
- Sung JH, Park SH, Mastri AR, Warwick WJ. Axonal dystrophy in the gracile nucleus in congenital biliary atresia and cystic fibrosis (mucoviscidosis): beneficial effect of vitamin E therapy. J Neuropathol Exp Neurol. 1980;39:584–597. doi: 10.1097/00005072-198009000-00007[↩]
- Weder B, Meienberg O, Wildi E, Meier C. Neurologic disorder of vitamin E deficiency in acquired intestinal malabsorption. Neurology. 1984;34:1561–1565. doi: 10.1212/WNL.34.12.1561[↩]
- Southam E, Thomas PK, King RHM, Goss-Sampson MA, Muller DPR. Experimental vitamin E deficiency in rats. Morphological and functional evidence of abnormal axonal transport secondary to free radical damage. Brain. 1991;114((Pt 2[↩]
- Larnaout A, Belal S, Zouari M, et al. Friedreich’s ataxia with isolated vitamin E deficiency: a neuropathological study of a Tunisian patient. Acta Neuropathol. 1997;93:633–637. doi: 10.1007/s004010050662[↩]
- Yokota T, Uchihara T, Kumagai J, et al. Postmortem study of ataxia with retinitis pigmentosa by mutation of the alpha-tocopherol transfer protein gene. J Neurol Neurosurg Psychiatry. 2000;68:521–525. doi: 10.1136/jnnp.68.4.521[↩]
- El Euch‐Fayache G, Bouhlal Y, Amouri R, Feki M, Hentati F. Molecular, clinical and peripheral neuropathy study of Tunisian patients with ataxia with vitamin E deficiency. Brain. 2014;137(Pt 2):402‐410. doi: 10.1093/brain/awt339[↩][↩]
- Angelini L, Erba A, Mariotti C, Gellera C, Ciano C, Nardocci N. Myoclonic dystonia as unique presentation of isolated vitamin E deficiency in a young patient. Mov Disord. 2002 May;17(3):612-4. doi: 10.1002/mds.10026[↩][↩][↩]
- Finckh B, Kontush A, Commentz J, Hübner C, Burdelski M, Kohlschütter A. Monitoring of ubiquinol-10, ubiquinone-10, carotenoids, and tocopherols in neonatal plasma microsamples using high-performance liquid chromatography with coulometric electrochemical detection. Anal Biochem. 1995 Dec 10;232(2):210-6. doi: 10.1006/abio.1995.0009[↩]
- Usuki F, Maruyama K. Ataxia caused by mutations in the alpha-tocopherol transfer protein gene. J Neurol Neurosurg Psychiatry. 2000 Aug;69(2):254-6. doi: 10.1136/jnnp.69.2.254[↩]
- Weiser H, Riss G, Kormann AW. Biodiscrimination of the eight alpha-tocopherol stereoisomers results in preferential accumulation of the four 2R forms in tissues and plasma of rats. J Nutr. 1996 Oct;126(10):2539-49. doi: 10.1093/jn/126.10.2539[↩]
- Hosomi A, Arita M, Sato Y, Kiyose C, Ueda T, Igarashi O, Arai H, Inoue K. Affinity for alpha-tocopherol transfer protein as a determinant of the biological activities of vitamin E analogs. FEBS Lett. 1997 Jun 2;409(1):105-8. doi: 10.1016/s0014-5793(97)00499-7[↩]
- Leonard SW, Terasawa Y, Farese RV Jr, Traber MG. Incorporation of deuterated RRR- or all-rac-alpha-tocopherol in plasma and tissues of alpha-tocopherol transfer protein–null mice. Am J Clin Nutr. 2002 Mar;75(3):555-60. doi: 10.1093/ajcn/75.3.555[↩]
- Amiel J, Maziere JC, Beucler I, Koenig M, Reutenauer L, Loux N, Bonnefont D, Féo C, Landrieu P. Familial isolated vitamin E deficiency. Extensive study of a large family with a 5-year therapeutic follow-up. J Inherit Metab Dis. 1995;18(3):333-40. doi: 10.1007/BF00710425[↩][↩]
- Burck U, Goebel HH, Kuhlendahl HD, Meier C, Goebel KM. Neuromyopathy and vitamin E deficiency in man. Neuropediatrics. 1981 Aug;12(3):267-78. doi: 10.1055/s-2008-1059657[↩]
- Harding AE, Matthews S, Jones S, Ellis CJ, Booth IW, Muller DP. Spinocerebellar degeneration associated with a selective defect of vitamin E absorption. N Engl J Med. 1985 Jul 4;313(1):32-5. doi: 10.1056/NEJM198507043130107[↩]
- Schuelke M, Finckh B, Sistermans EA, Ausems MG, Hübner C, von Moers A. Ataxia with vitamin E deficiency: biochemical effects of malcompliance with vitamin E therapy. Neurology. 2000 Nov 28;55(10):1584-6. doi: 10.1212/wnl.55.10.1584[↩]
- Bruno RS, Traber MG. Vitamin E biokinetics, oxidative stress and cigarette smoking. Pathophysiology. 2006;13(3):143‐149. doi: 10.1016/j.pathophys.2006.05.003[↩]
- Traber MG, Manor D. Vitamin E. Adv Nutr. 2012 May 1;3(3):330-1. doi: 10.3945/an.112.002139[↩]
- Müller-Schmehl K, Beninde J, Finckh B, Florian S, Dudenhausen JW, Brigelius-Flohé R, Schuelke M. Localization of alpha-tocopherol transfer protein in trophoblast, fetal capillaries’ endothelium and amnion epithelium of human term placenta. Free Radic Res. 2004 Apr;38(4):413-20. doi: 10.1080/10715760310001659611[↩]
- Amiel J, Maziere JC, Beucler I, et al. Familial isolated vitamin E deficiency. Extensive study of a large family with a 5‐year therapeutic follow‐up. J Inherit Metab Dis. 1995;18(3):333‐340. doi: 10.1007/BF00710425[↩]
- Roubertie A, Biolsi B, Rivier F, Humbertclaude V, Cheminal R, Echenne B. Ataxia with vitamin E deficiency and severe dystonia: report of a case. Brain Dev. 2003 Sep;25(6):442-5. doi: 10.1016/s0387-7604(03)00054-8[↩][↩]





{kind=link}