
Contents
- Why does birth control make you gain weight
- What causes weight gain when using birth control ?
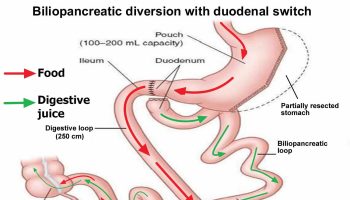
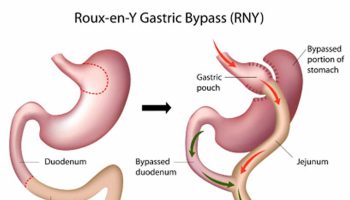
- What are the treatments for obesity and overweight ?
Why does birth control make you gain weight
Weight gain is often considered a side effect of using combination contraceptives (that is, an estrogen plus a progestin) 1 and many women and clinicians believe that an association exists. Birth control pills also called oral contraceptives or just “the pill” contain man-made forms of 2 hormones called estrogen and progestin 2. These hormones are made naturally in a woman’s ovaries. Birth control pills can contain both of these hormones or have progestin only. Both estrogen and progestin hormones in the birth control pills prevent a woman’s ovary from releasing an egg during her menstrual cycle (called ovulation). They do this by changing the levels of the natural hormones the body makes. Progestins also make the mucus around a woman’s cervix thick and sticky. This helps prevent sperm from entering the uterus.
- The most common type of birth control pill combines the hormones estrogen and progestin. There are many different forms of this type of pill.
- The “mini-pill” is a type of birth control pill that contains only progestin, no estrogen. These pills are an option for women who do not like the side effects of estrogen or who cannot take estrogen for medical reasons.
- They can also be used after delivery in women who are breastfeeding.
Weight gain is thought to be a side effect of birth control methods. Many women and healthcare providers believe that pills and patches cause weight gain. However, there are no significant differences among combined oral contraceptives in terms of weight gain 3. Furthermore, a causal relationship between combination contraceptives and weight gain has not been established 4. Many women consider weight gain a side effect of using hormonal contraceptives 5, 6. This perception may be based on self-report of side effects rather than actual weight changes 7, 8, 9.
Concern about weight gain can deter the initiation of contraceptives and cause early discontinuation among users. In a United States study of bone mineral density, weight gain was reported more often by women using depot medroxyprogesterone acetate (DMPA) than those using a low-dose oral contraceptive 8. Weight gain was the most common side effect reported with DMPA use, after menstrual disturbances, in a New Zealand study 7, and was the most common self-reported side effect in a study from Iran 10. Reported weight gain has been a major reason for discontinuing DMPA use in the US 11. Some evidence suggests that DMPA is a concern for adolescents who are already obese 12. From a survey of Latin American women across four countries, more women believed levonorgestrel-releasing intrauterine contraception (LNG-IUC) led to weight gain, mood swings, and infertility compared with copper IUC 13. In a US study, more women reported weight gain as a side effect for the etonogestrel implant than for LNG-IUC 14. Weight gain was also reported for levonorgestrel implants 15. The gain may have been greater among women in the US than among those in China, and may be partly attributable to differences in dietary habits.
- For most women, birth control pills, vaginal rings and contraceptive skin patches are very unlikely to affect their weight much. Many women slowly gain weight over the years, whether or not they use hormonal contraception 16.
A systematic review of randomized controlled trials did not find a causal connection between combined hormonal contraceptives and weight gain 17, whereas a Cochrane review found the evidence to be insufficient 18. Extended-cycle combined oral contraceptives do not cause more weight gain than standard regimens 19. A randomized prospective trial of two combined oral contraceptive regimens and the ethinyl estradiol/etonogestrel vaginal ring (Nuvaring) did not find significant weight gain in any group 20.
Effects birth control and weight gain are the subject of debate
Women who stop taking the pill often do so because they think it has been causing them to gain weight. Clinical studies in this area are contradictory: Some women said that they gained weight, while others reported losing weight. This is why both weight gain and weight loss are listed as possible side effects on the product information of hormonal contraceptives.
If people put on weight it is usually due to one of the following changes:
- Fluid retention
- An increase in muscle tissue (because muscle is heavier than other tissue)
- An increase in body fat
Theoretically, hormonal contraceptives could contribute to weight gain if they led to fluid retention 21 and increased body fat 1. Also, combined contraceptives are sometimes believed to increase appetite. But it’s not that easy to say whether that’s true because women who don’t use hormonal contraceptives also gain weight as they age.
The research results are uncertain
In order to find out whether the birth control pill actually influences body weight, doctors would need studies with one group of women who use hormonal contraceptives over a long period of time and another group who do not. Then the groups could be compared to see if there are any differences in their weight.
In 2014 researchers from the Cochrane Collaboration 4 looked for such good-quality studies on hormonal contraceptives in which weight was recorded. They were only able to find a few studies that compared hormonal contraceptives with “fake” hormonal contraceptives (placebos) and measured the impact on weight. This is not that surprising, though. Because hormonal contraceptives are so reliable, not many women are willing to use contraceptives that could be less effective or may even be placebos and not work at all.
None of the studies found by the researchers show a clear link between hormonal contraception and weight gain 4. But these studies did not have enough participants and were not well-designed to be able to provide a definite answer. In addition, most of the studies didn’t record the participants’ weight very carefully. At most, only the number of women who reported that they stopped taking the pill because of weight gain was recorded. So it’s not possible to say for sure whether the participants who used hormonal contraceptives gained more weight than the women in the other group.
A major effect on weight is unlikely
Because of this, one group of researchers also looked for studies where different combined contraceptives were compared with one another and weight was carefully recorded. They found 45 studies in which many different types of hormonal contraceptives were compared. So it’s difficult to tell how the individual types affect weight.
What’s more, no link was found between hormone dosage and weight gain. If hormones really did influence weight gain, then you would expect higher doses to lead to more weight gain. Such a link was not established.
On the whole, the researchers concluded that it seems very unlikely that hormonal contraceptives cause major weight gain. If there were a strong effect, it would have been noticed in the studies. But this doesn’t rule out the possibility that individual women could in fact gain weight.
Birth control shot may make you gain weight
Many clinicians and women also believe that progestin-only contraceptives cause weight gain 22. Progestin-only contraceptives are appropriate for many women who cannot or should not take estrogen. Progestin-only contraceptives do not contain estrogen, unlike combined hormonal contraceptives that have both progestin and estrogen. Therefore, progestin-only contraceptives are appropriate for women who cannot or should not take estrogen 23. Progestin-only contraceptives include injectables, intrauterine contraception, implants, and oral contraceptives. Many progestin-only contraceptives are long-acting, cost-effective methods of preventing pregnancy. However, concern about weight gain can deter the initiation of contraceptives and cause early discontinuation among users.
In Medical Eligibility Criteria, progestin-only contraceptives are category 1 for women who are obese (body mass index (BMI) ≥ 30 kg/m2) 24, 25, 26. Category 1 is a condition with no restriction for use of the contraceptive method. For obese adolescents, long-acting injectable depot medroxyprogesterone acetate (DMPA sometimes called Depo-Provera, the Depo shot) is category 2 due to possible effects on bone mineral density. For category 2, method advantages generally outweigh the theoretical or proven risks. Progestin-only contraceptives are also category 1 for breastfeeding women who are at least six weeks postpartum. Combined hormonal contraceptives (containing both estrogen and progestin) are category 3 for such women until six months postpartum 26. In the US, combined hormonal contraceptives are considered category 2 by one month postpartum 25.
Worldwide, intrauterine contraception (IUC) is the most commonly used reversible method among women married or in union 27. In the US in 2012, IUC use was low compared with oral contraceptive use 28. However, use of long-acting reversible methods (LARC) increased to 11.6% from 8.5% in 2009 29. Nearly three-fourths of IUC users were using hormonal IUC. Worldwide, the method used most frequently after IUC is oral contraceptives, which include combined oral contraceptives (COCs) and progestin-only pills (POPs). In the least developed countries, injectables are most commonly used, followed by oral contraceptives 27. Some injectable contraceptives contain both estrogen and progestin, while others like DMPA are progestin-only.
The birth control shot (sometimes called Depo-Provera, the Depo shot, or DMPA) contains the hormone progestin. Progestin stops you from getting pregnant by preventing ovulation. When there’s no egg in the tube, pregnancy can’t happen. It also works by making cervical mucus thicker. When the mucus on the cervix is thicker, the sperm can’t get through. And when the sperm and the egg can’t get together, pregnancy can’t happen.
The long-acting injectable depot medroxyprogesterone acetate (Depo-Provera) is the only hormonal contraceptive that is consistently associated with weight gain. A prospective study found that women who used Depo-Provera gained an average of 11.2 lb (5.1 kg) over 36 months, whereas women who used combined oral contraceptives did not gain any weight 30, 31. However, in a 2016 Cochrane review 32 that included 22 clinical studies involving a total of 11,450 women. By contraceptive method, the review has 16 studies of depot medroxyprogesterone acetate (DMPA), 4 of levonorgestrel-releasing intrauterine contraception (LNG-IUC), 5 for implants, and 2 for progestin-only pills. More than half of the studies had low quality evidence. Overall these 22 studies showed limited evidence of change in weight or body composition with use of progestin-only contraceptives 32. Mean weight gain at 6 or 12 months was less than 2 kg (4.4 lb) for most studies. Those with multiyear data showed mean weight change was approximately twice as much at two to four years than at one year, but generally the study groups did not differ significantly. Therefore, appropriate counseling about typical weight gain may help reduce discontinuation of contraceptives due to perceptions of weight gain.
What causes weight gain when using birth control ?
A number of factors can play a role in weight gain. Weight gain and obesity results from a combination of causes and contributing factors, including individual factors such as behavior, stress, lack of sleep and genetics. Behaviors can include dietary patterns, physical activity, inactivity, medication use and other exposures. Additional contributing factors in our society include the food and physical activity environment, education and skills, and food marketing and promotion. Some of these factors are discussed briefly below.
Energy imbalances cause the body to store fat
Energy imbalances can cause overweight and obesity. An energy imbalance means that your energy IN does not equal your energy OUT. This energy is measured in calories. Energy IN is the amount of calories you get from food and drinks. Energy OUT is the amount of calories that your body uses for things such as breathing, digesting, being physically active, and regulating body temperature.
Overweight and obesity develop over time when you take in more calories than you use, or when energy IN is more than your energy OUT. This type of energy imbalance causes your body to store fat.
Your body uses certain nutrients such as carbohydrates or sugars, proteins, and fats from the foods you eat to:
- make energy for immediate use to power routine daily body functions and physical activity.
- store energy for future use by your body. Sugars are stored as glycogen in the liver and muscles. Fats are stored mainly as triglycerides in fat tissue.
The amount of energy that your body gets from the food you eat depends on the type of foods you eat, how the food is prepared, and how long it has been since you last ate.
Risk Factors
There are many risk factors for overweight and obesity. Some risk factors can be changed, such as unhealthy lifestyle habits and environments. Other risk factors, such as age, family history and genetics, race and ethnicity, and sex, cannot be changed. Heathy lifestyle changes can decrease your risk for developing overweight and obesity.
Unhealthy lifestyle habits
- Lack of physical activity, unhealthy eating patterns, not enough sleep, and high amounts of stress can increase your risk for overweight and obesity.
- Lack of physical activity
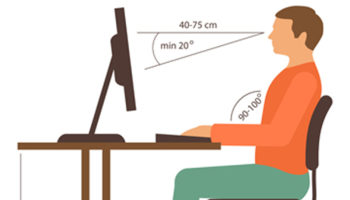
Lack of physical activity due to high amounts of TV, computer, videogame or other screen usage has been associated with a high body mass index. Healthy lifestyle changes, such as being physically active and reducing screen time, can help you aim for a healthy weight.
Unhealthy eating behaviors
Some unhealthy eating behaviors can increase your risk for overweight and obesity.
- Eating more calories than you use. The amount of calories you need will vary based on your sex, age, and physical activity level. Find out your daily calorie needs or goals with the Body Weight Planner 33.
- Eating too much saturated and trans fats
- Eating foods high in added sugars
Not enough sleep
Many studies have seen a high BMI in people who do not get enough sleep. Some studies have seen a relationship between sleep and the way our bodies use nutrients for energy and how lack of sleep can affect hormones that control hunger urges. Visit our Sleep Deprivation and Deficiency Health Topic for more information about lack of sleep.
High amounts of stress
Acute stress and chronic stress affect the brain and trigger the production of hormones, such as cortisol, that control our energy balances and hunger urges. Acute stress can trigger hormone changes that make you not want to eat. If the stress becomes chronic, hormone changes can make you eat more and store more fat.
Food and Activity
People gain weight when they eat more calories than they burn through activity. This imbalance is the greatest contributor to weight gain.
The world around you influences your ability to maintain a healthy weight. For example:
- Not having area parks, sidewalks, and affordable gyms makes it hard for people to be physically active.
- Oversized food portions increase Americans’ calorie intake, making even more physical activity necessary to maintain a healthy weight.
- Some people don’t have access to supermarkets that sell affordable healthy foods, such as fresh fruits and vegetables.
- Food advertising encourages people to buy unhealthy foods, such as high-fat snacks and sugary drinks 34.
Behavior
Healthy behaviors include a healthy diet pattern and regular physical activity. Energy balance of the number of calories consumed from foods and beverages with the number of calories the body uses for activity plays a role in preventing excess weight gain. A healthy diet pattern follows the Dietary Guidelines for Americans which emphasizes eating whole grains, fruits, vegetables, lean protein, low-fat and fat-free dairy products and drinking water. The Physical Activity Guidelines for Americans recommends adults do at least 150 minutes of moderate intensity activity or 75 minutes of vigorous intensity activity, or a combination of both, along with 2 days of strength training per week.
- Having a healthy diet pattern and regular physical activity is also important for long term health benefits and prevention of chronic diseases such as Type 2 diabetes and heart disease.
The key to achieving and maintaining a healthy weight isn’t short-term dietary changes; it’s about a lifestyle that includes healthy eating and regular physical activity.
- Body Weight Planner. https://www.supertracker.usda.gov/bwp/index.html
To find out about how many calories you should eat to lose weight according to your weight, age, sex, height and physical activity, you can use a FREE online app Body Weight Planner 33
- ChooseMyPlate. https://www.choosemyplate.gov/
To find out about the 5 Food Groups you should have on your plate for a meal, you can use a FREE online app ChooseMyPlate 35
- SuperTracker website: https://supertracker.usda.gov
To find out What and How Much To Eat, you can use a FREE, award-winning, state-of-the-art, online diet and activity tracking tool called SuperTracker 36 from the United States Department of Agriculture Center for Nutrition Policy and Promotion 36. This free application empowers you to build a healthier diet, manage weight, and reduce your risk of chronic diet-related diseases. You can use SuperTracker 36 to determine what and how much to eat; track foods, physical activities, and weight; and personalize with goal setting, virtual coaching, and journaling.
- BMI Calculator Adults. https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html
- BMI Calculator Children. https://nccd.cdc.gov/dnpabmi/Calculator.aspx
To find out about your body mass index (BMI), you can use a FREE online BMI calculators from the Centers for Disease Control and Prevention (CDC) – for Adults 37 and for Children 38
Community Environment
People and families may make decisions based on their environment or community. For example, a person may choose not to walk or bike to the store or to work because of a lack of sidewalks or safe bike trails. Community, home, child care, school, health care, and workplace settings can all influence people’s daily behaviors. Therefore, it is important to create environments in these locations that make it easier to engage in physical activity and eat a healthy diet.
Many environmental factors can increase your risk for overweight and obesity:
- social factors such as having a low socioeconomic status or an unhealthy social or unsafe environment in the neighborhood
- built environment factors such as easy access to unhealthy fast foods, limited access to recreational facilities or parks, and few safe or easy ways to walk in your neighborhood
- exposure to chemicals known as obesogens that can change hormones and increase fatty tissue in our bodies.
Exposure to chemicals known as obesogens
Scientists are exploring the role that chemicals may play in weight gain and obesity. Some of these chemicals are toxic to animals and humans, and some interfere with how the body’s hormones function. The ones that impact hormones are called endocrine disrupting chemicals, or endocrine disruptors, and are linked to a variety of diseases 39. Some endocrine disruptors have been shown to be obesogens, or involved in weight gain, and may be contributing to the obesity problem in this country.
The term obesogens was coined around 2006, based on the knowledge that exposures during early development to specific chemicals were found to disrupt normal metabolic processes and increase susceptibility to weight gain across the lifespan. Poor nutrition and lack of exercise are known contributors to obesity, but these chemicals may also be contributing.
How obesogens work in the body
Unhealthy diet and lack of exercise are the main factors that contribute to weight gain and obesity, but studies have found that obesogens may also be playing a role. Obesogens do not directly cause obesity, but they may increase the sensitivity, or susceptibility, to gaining weight, especially when the exposures occur during development.
Obesogens are believed to work in several ways.
They may change how a person’s fat cells develop, meaning they may increase fat storage capacity or the number of fat cells.
Also, obesogens may make it more difficult to maintain a healthy weight, by changing how the body regulates feelings of hunger and fullness, or increasing the effects of high fat and high sugar diets.
Examples of chemicals that may be obesogens
- Cigarette smoke
- Air pollution
- Tributyltin, a chemical that is widely used as a fungicide and heat stabilizer in polyvinyl chloride (PVC) piping
- Flame retardants
- Phthalates, a broad class of chemicals that are added to many consumer products to make them softer
- Bisphenol A
- Some pesticides
- Polychlorinated biphenyls (PCBs), industrial chemicals that were used widely in the past in products such as paints, cements, fluorescent light ballasts, sealants, and adhesives.
Cigarette Smoke
Cigarette smoke contains a number of toxic chemicals and irritants. People with allergies may be more sensitive to cigarette smoke than others and research studies indicate that smoking may aggravate allergies.
Smoking does not just harm smokers but also those around them. Research has shown that children and spouses of smokers tend to have more respiratory infections and asthma than those of non-smokers. In addition, exposure to secondhand smoke can increase the risk of allergic complications such as sinusitis and bronchitis .
Common symptoms of smoke irritation are burning or watery eyes, nasal congestion, coughing, hoarseness and shortness of breath presenting as a wheeze.
More than 58 million nonsmokers in the United States are still exposed to secondhand smoke, even though cigarette smoking rates are dropping and many states prohibit smoking in public places such as worksites, restaurants, and bars. In all, about 1 of every 4 nonsmokers is exposed to the dangerous chemicals in secondhand smoke.
Secondhand smoke exposure occurs when nonsmokers breathe in tobacco smoke exhaled by smokers or when they breathe the smoke from burning tobacco products. The Environmental Protection Agency has classified secondhand smoke as a Group A carcinogen—an agent that is known to cause cancer in humans—and the Surgeon General has concluded that there is no safe level of exposure to secondhand smoke.
Secondhand smoke contains dangerous chemicals that can damage the lungs and heart. It is known to cause heart disease and cancer in adult nonsmokers, and even brief exposure can trigger a heart attack or stroke. Secondhand smoke can also cause sudden infant death syndrome (SIDS), respiratory infections, ear infections, and asthma attacks in infants and children. Every year, exposure to secondhand smoke causes:
- 41,000 adult nonsmokers to die from heart disease or lung cancer
- 400 infants to die from SIDS
Preventive Strategies
- Don’t smoke and if you do, seek support to quit smoking.
- Seek smoke-free environments in restaurants, theaters and hotel rooms.
- Avoid smoking in closed areas like homes or cars where others may be exposed to second-hand smoke.
Air Pollution
Air pollution is a mixture of natural and man-made substances in the air we breathe. It is typically separated into two categories: outdoor air pollution and indoor air pollution.
Outdoor air pollution involves exposures that take place outside of the built environment. Examples include:
- Fine particles produced by the burning of fossil fuels (i.e. the coal and petroleum used in traffic and energy production)
- Noxious gases (sulfur dioxide, nitrogen oxides, carbon monoxide, chemical vapors, etc.)
- Ground-level ozone (a reactive form of oxygen and a primary component of urban smog)
- Tabacco Smoke
Indoor air pollution involves exposures to particulates, carbon oxides, and other pollutants carried by indoor air or dust. Examples include:
- Gases (carbon monoxide, radon, etc.)
- Household products and chemicals
- Building materials (asbestos, formaldehyde, lead, etc.)
- Outdoor indoor allergens (cockroach and mouse dropping, etc.)
- Tobacco smoke
- Mold and pollen
In some instances, outdoor air pollution can make its way indoors by way of open windows, doors, ventilation, etc.
What health effects are linked to air pollution ?
Over the past 30 years, researchers have unearthed a wide array of health effects which are believed to be associated with air pollution exposure. Among them are respiratory diseases (including asthma and changes in lung function), cardiovascular diseases, adverse pregnancy outcomes (such as preterm birth), and even death.
In 2013, the World Health Organization concluded that outdoor air pollution is carcinogen to humans 40.
How can I reduce my risk for air pollution exposure ?
Indoor air pollution can be reduced by making sure that a building is well-ventilated and cleaned regularly to prevent the buildup of agents like dust and mold. Occupants would also be wise to remove any known pollutants and or irritants (aerosols, stringent cleaning supplies, etc.) whenever possible.
Outdoor air pollution exposures can be reduced by checking one’s Air Quality Index (AQI), avoiding heavy traffic when possible, and avoiding secondhand tobacco smoke.
Flame Retardants
Flame retardants are chemicals that are added or applied to materials in order to slow or prevent the start/growth of fire 41. They have been used in many consumer and industrial products since the 1970s, to decrease the ability of materials to ignite.
Flame retardants are often added or applied to the following products:
- Furnishings, such as foam, upholstery, mattresses, carpets, curtains, and fabric blinds.
- Electronics and electrical devices, such as computers, laptops, phones, televisions, and household appliances, plus wires and cables.
- Building and construction materials, including electrical wires and cables, and insulation materials, such as polystyrene and polyurethane insulation foams.
- Transportation products, such as seats, seat covers and fillings, bumpers, overhead compartments, and other parts of automobiles, airplanes, and trains.
Many flame retardants have been removed from the market or are no longer produced. However, because they do not easily break down, they can remain persistent in the environment for years. They can also bioaccumulate, or build up in people and animals over time.
How are people exposed to flame retardants ?
People can be exposed to flame retardants through a variety of ways, including diet; consumer products in the home, car, airplane, and workplace; and house dust 42.
- These chemicals can get into the air, water, and soil during manufacture.
- Chemicals can leak from products into dust and into the air.
- Dust can get on hands and food and then into the mouth when food is eaten.
- Through e-waste or the uncontrolled burning and dismantling of electronic and electric waste.
What are some of the potential health effects associated with flame retardants ?
Although flame retardants can offer benefits when they are added to some products, a growing body of evidence shows that many of these chemicals are associated with adverse health effects in animals and humans. These include:
- Endocrine and thyroid disruption
- Impacts to the immune system
- Reproductive toxicity
- Cancer
- Adverse effects on fetal and child development
- Neurologic function
Who is most vulnerable ?
Children may be particularly vulnerable to the toxic effects of these chemicals, because their brain and other organs are still developing. Hand-to-mouth behavior and proximity to the floor increases the potential of children to be exposed to flame retardants. Researchers have found that children have higher concentrations of flame retardants in their bodies than adults.
Are there different types of flame retardants ?
There are hundreds of different flame retardants. They are often broken into categories based on chemical structure and properties. In general, flame retardants are grouped based on whether they contain bromine, chlorine, phosphorus, nitrogen, metals, or boron.
Brominated flame retardants — Contain bromine and are the most abundantly used flame retardants. Used in many consumer goods, including electronics, furniture, building materials, etc. and have been linked to endocrine disruption among other effects.
Polybrominated diphenyl ethers (PBDE’s) —PBDEs do not chemically bind with the products to which they are added (furniture, electronics, etc.) so they easily release from these products and enter air and dust. PBDEs can lower birth weight/length of children, and impair neurological development.
Tetrabromobisphenol A (TBBPA) — Widely used to make computer circuit boards and electronics. Also used in some textiles and paper, or as an additive in other flame retardants.
Hexabromocyclododecane (HBCD) — An additive primarily used in polystyrene foam building materials. The primary risk to humans is from leaching out of products and getting into indoor dust. Low levels of HBCD have also been found in some food products.
Organophosphate flame retardants (OPFRs) — With the phasing out of PBDEs, some OPFRs have been identified as replacements.
What is Bisphenol A (BPA)
Bisphenol A (BPA) is a chemical produced in large quantities for use primarily in the production of polycarbonate plastics and epoxy resins 43.
Where is BPA found ?
Polycarbonate plastics have many applications including use in some food and drink packaging, e.g., water and infant bottles, compact discs, impact-resistant safety equipment, and medical devices. Epoxy resins are used as lacquers to coat metal products such as food cans, bottle tops, and water supply pipes. Some dental sealants and composites may also contribute to BPA exposure.
How does BPA get into the body ?
The primary source of exposure to BPA for most people is through the diet. While air, dust, and water are other possible sources of exposure, BPA in food and beverages accounts for the majority of daily human exposure.
Bisphenol A can leach into food from the protective internal epoxy resin coatings of canned foods and from consumer products such as polycarbonate tableware, food storage containers, water bottles, and baby bottles. The degree to which BPA leaches from polycarbonate bottles into liquid may depend more on the temperature of the liquid or bottle, than the age of the container. BPA can also be found in breast milk.
Why are people concerned about BPA ?
One reason people may be concerned about BPA is because human exposure to BPA is widespread. The 2003-2004 National Health and Nutrition Examination Survey (NHANES III) conducted by the Centers for Disease Control and Prevention (CDC) found detectable levels of BPA in 93% of 2517 urine samples from people six years and older. The CDC NHANES data are considered representative of exposures in the United States. Another reason for concern, especially for parents, may be because some animal studies report effects in fetuses and newborns exposed to BPA.
If I am concerned, what can I do to prevent exposure to BPA ?
Some animal studies suggest that infants and children may be the most vulnerable to the effects of BPA. Parents and caregivers, can make the personal choice to reduce exposures of their infants and children to BPA:
- Don’t microwave polycarbonate plastic food containers. Polycarbonate is strong and durable, but over time it may break down from over use at high temperatures.
- Plastic containers have recycle codes on the bottom. Some, but not all, plastics that are marked with recycle codes 3 or 7 may be made with BPA.
- Reduce your use of canned foods.
- When possible, opt for glass, porcelain or stainless steel containers, particularly for hot food or liquids.
- Use baby bottles that are BPA free.
Pesticides
A pesticide is any substance used to kill, repel, or control certain forms of plant or animal life that are considered to be pests. Pesticides include herbicides for destroying weeds and other unwanted vegetation, insecticides for controlling a wide variety of insects, fungicides used to prevent the growth of molds and mildew, disinfectants for preventing the spread of bacteria, and compounds used to control mice and rats. Because of the widespread use of agricultural chemicals in food production, people are exposed to low levels of pesticide residues through their diets. Scientists do not yet have a clear understanding of the health effects of these pesticide residues. Results from the Agricultural Health Study, an ongoing study of pesticide exposures in farm families, may be found at 44. Other evidence suggests that children are particularly susceptible to adverse effects from exposure to pesticides, including neurodevelopmental effects. People may also be exposed to pesticides used in a variety of settings including homes, schools, hospitals, and workplaces.
Health consequences
The most sensitive time for exposure to obesogens is during early development — as a fetus or during the first years of life — when the body’s weight control mechanisms are being developed.
Obesity is a disease itself, but other diseases or disorders that develop as a result of, or in combination with obesity, such as cardiovascular disease, liver disease, diabetes, arthritis, and others, also can contribute to health problems associated with weight gain.
Prevention
Try to minimize exposures to environmental chemicals. This is often challenging, since it is hard to know where and what products contain these chemicals.
Some general advice is to:
- Eat fresh fruit and vegetables
- Reduce use of plastics
- Do not use plastics in the microwave (unless it’s microwave safe)
- Purchase furniture that has not been treated with flame retardants
- Choose fragrance-free products.
Genetics
Research shows that genetics plays a role in obesity. Genes can directly cause obesity in such disorders as Prader-Willi syndrome, Bardet-Biedl syndrome
Alström syndrome and Cohen syndrome.
Genes also may contribute to a person’s susceptibility to weight gain. Scientists believe that genes may increase a person’s likelihood of becoming obese but that outside factors, such as an abundant food supply or little physical activity, also may be required for a person to put on excess weight 45.
Health Conditions
Some hormone problems may cause overweight and obesity, such as underactive thyroid (hypothyroidism), Cushing syndrome and polycystic ovary syndrome (PCOS).
Polycystic ovary syndrome (PCOS) is a condition that can cause infertility, enlarged ovaries, irregular menstrual cycles, excessive body or facial hair, acne, and obesity. Also called PCOS. POCS increases the risk for diabetes, heart disease, high blood pressure and endometrial cancer.
Hypothyroidism. People with this condition have low levels of thyroid hormones. These low levels are associated with decreased metabolism and weight gain, even when food intake is reduced. People with hypothyroidism also produce less body heat, have a lower body temperature, and do not efficiently use stored fat for energy.
Cushing’s syndrome. People with this condition have high levels of glucocorticoids, such as cortisol, in the blood. High cortisol levels make the body feel like it is under chronic stress. As a result, people have an increase in appetite and the body will store more fat. Cushing’s syndrome may develop after taking certain medicines or because the body naturally makes too much cortisol.
Tumors. Some tumors, such as craneopharingioma, can cause severe obesity because the tumors develop near parts of the brain that control hunger.
Medications
Medicines such as corticosteroids, antipsychotics, antidepressants, antiepileptics, and antihyperglycemics can cause weight gain and lead to overweight and obesity.
Talk to your doctor if you notice weight gain while you are using one of these medicines. Ask if there are other forms of the same medicine or other medicines that can treat your medical condition, but have less of an effect on your weight. Do not stop taking the medicine without talking to your doctor.
Stress, Emotional Factors, and Poor Sleep
Some people eat more than usual when they are bored, angry, upset, or stressed.
Studies also have found that the less people sleep, the more likely they are to be overweight or obese. This is partly because hormones that are released during sleep control appetite and the body’s use of energy.
What are the treatments for obesity and overweight ?
To maintain a healthy weight, it is important to create a balance between the calories eaten and the calories burned through physical activity and bodily functions. To lose weight, a person usually needs to reduce calories and increase physical activity.
If lifestyle changes are not enough, medicines and weight-loss surgery also are options for some people who need to lose weight.
What are some tips for healthy eating ?
- Emphasize fruits, vegetables, whole grains, and fat-free or low-fat milk and dairy products.
- Include lean meats, poultry, fish, beans, eggs, and nuts.
- Eat a diet low in saturated fats, trans fats, cholesterol, salt (sodium), and added sugars.
- Drink more water instead of sugary drinks.
How much physical activity does an adult need ?
Getting enough physical activity is an important way to help prevent or reduce overweight and obesity and related health problems.
- Adults age 18 and older need at least 30 minutes of physical activity on 5 or more days of the week to be healthy.
- Children and teens need at least 60 minutes of activity a day for their health.
- Nelson AL. Combined oral contraceptives. In: Hatcher RA, Trussell J, Nelson AL, Cates W, Stewart FH, Kowal D, et al. editor(s). Contraceptive Technology. 19th Edition. New York: Ardent Media, Inc., 2007:193-270.[↩][↩]
- Birth control pills – overview. https://medlineplus.gov/ency/article/007460.htm[↩]
- Moreau C, Trussell J, Gilbert F, Bajos N, Bouyer J. Oral contraceptive tolerance: does the type of pill matter? Obstet Gynecol. 2007;109(6):1277–1285.[↩]
- Gallo MF, Lopez LM, Grimes DA, Carayon F, Schulz KF, Helmerhorst FM. Combination contraceptives: effects on weight. Cochrane Database of Systematic Reviews 2014, Issue 1. Art. No.: CD003987. DOI: 10.1002/14651858.CD003987.pub5. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD003987.pub5/full[↩][↩][↩]
- Bartz D, Goldberg AB. Injectable contraceptives. In: Hatcher RA, Trussell J, Nelson AL, Cates W, Kowal D, Policar MS editor(s). Contraceptive Technology. 20th Edition. New York: Ardent Media, Inc., 2011:209-36.[↩]
- Raymond EG. Progestin-only pills. In: Hatcher RA, Trussell J, Nelson AL, Cates W Jr, Kowal D, Policar MS editor(s). Contraceptive technology. 20th Edition. New York: Ardent Media, Inc., 2011:237-47.[↩]
- Paul C, Skegg DC, Williams S. Depot medroxyprogesterone acetate. Patterns of use and reasons for discontinuation. Contraception. 1997/12/31 1997; Vol. 56, issue 4:209-14.[↩][↩]
- Berenson AB, Odom SD, Breitkopf CR, Rahman M. Physiologic and psychologic symptoms associated with use of injectable contraception and 20 µg oral contraceptive pills. American Journal of Obstetrics and Gynecology. 2008/07/05 2008; Vol. 199, issue 4:351e1-12.[↩][↩]
- Nault AM, Peipert JF, Zhao Q, Madden T, Secura GM. Validity of perceived weight gain in women using long-acting reversible contraception and depot medroxyprogesterone acetate. American Journal of Obstetrics and Gynecology 2013;208(1):48 e1-8.[↩]
- Veisi F, Zangeneh M. Comparison of two different injectable contraceptive methods: depo-medroxy progesterone acetate (DMPA) and Cyclofem. Journal of Family and Reproductive Health 2013;7(3):109-13.[↩]
- Bonny AE, Britto MT, Huang B, Succop P, Slap GB. Weight gain, adiposity, and eating behaviors among adolescent females on depot medroxyprogesterone acetate (DMPA). Journal of Pediatric and Adolescent Gynecology 2004;17(2):109-15.[↩]
- Curtis KM, Ravi A, Gaffield ML. Progestogen-only contraceptive use in obese women. Contraception. 2009/09/16 2009; Vol. 80, issue 4:346-54.[↩]
- Silva-Filho AL, Lira J, Rocha AL, Ferreira MC, Lamaita RM, Candido EB, et al. Non-hormonal and hormonal intrauterine contraception: survey of patients’ perceptions in four Latin American countries. European Journal of Contraception and Reproductive Health Care 2016 Feb 5 [Epub ahead of print]:1-7.[↩]
- Dickerson LM, Diaz VA, Jordon J, Davis E, Chirina S, Goddard JA, et al. Satisfaction, early removal, and side effects associated with long-acting reversible contraception. Family Medicine 2013;45(10):701-7.[↩]
- Sivin I. Risks and benefits, advantages and disadvantages of levonorgestrel-releasing contraceptive implants. Drug Safety. 2003/03/26 2003; Vol. 26, issue 5:303-35.[↩]
- Contraception: Do hormonal contraceptives cause weight gain ? https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0093796/[↩]
- Gallo MF, Grimes DA, Schulz KF, Helmerhorst FM. Combination estrogen- progestin contraceptives and body weight: systematic review of randomized controlled trials. Obstet Gynecol. 2004;103(2):359–373.[↩]
- Gallo MF, Lopez LM, Grimes DA, Schulz KF, Helmerhorst FM. Combination contraceptives: effects on weight. Cochrane Database Syst Rev. 2008;(4):CD003987.[↩]
- Miller L, Hughes JP. Continuous combination oral contraceptive pills to eliminate withdrawal bleeding: a randomized trial. Obstet Gynecol. 2003;101(4):653–661.[↩]
- Sabatini R, Cagiano R. Comparison profiles of cycle control, side effects and sexual satisfaction of three hormonal contraceptives. Contraception. 2006;74(3):220–223.[↩]
- Corvol P, Elkik F, Feneant M, Oblin ME, Michaud A, Claire M, et al. Effect of progesterone and progestins on water and salt metabolism. In: CW Bardin, E Milgrom, P Mauvais-Jarvis editor(s). Progesterone and Progestins. New York: Raven Press, 1983.[↩]
- Albright M, Rani S, Gavagan T. HelpDesk answers: do hormonal contraceptives lead to weight gain?. Journal of Family Practice 2015;64(6):371-2.[↩]
- American College of Obstetricians and Gynecologists. ACOG technical bulletin. Use of hormonal contraception in women with coexisting medical conditions. Washington, D.C.: American College of Obstetricians and Gynecologists, 2006.[↩]
- World Health Organization, Department of Reproductive Healh. Medical eligibility criteria for contraceptive use. Fifth edition – Executive Summary, 2015. http://www.who.int/reproductivehealth/publications/family_planning/Ex-Summ-MEC-5/en/[↩]
- Centers for Disease Control and Prevention. Summary Chart of U.S. Medical Eligibility Criteria for Contraceptive Use. https://www.cdc.gov/reproductivehealth/contraception/mmwr/mec/summary.html[↩][↩]
- World Health Organization, Department of Reproductive Health. Medical eligibility criteria wheel for contraceptive use. 2015. http://www.who.int/reproductivehealth/publications/family_planning/Ex-Summ-MEC-5/en/[↩][↩]
- United Nations, Department of Economic and Social Affairs. World Contraceptive Patterns 2015. www.un.org/en/development/desa/population/publications[↩][↩]
- Guttmacher Institute. Contraceptive Use in the United States. October 2015. www.guttmacher.org/pubs/fb_contr_use.html[↩]
- Kavanaugh ML, Jerman J, Finer LB. Changes in use of long-acting reversible contraceptive methods among U.S. women, 2009-2012. Obstetrics and Gynecology 2015;126(5):917-27.[↩]
- Berenson AB, Odom SD, Breitkopf CR, Rahman M. Physiologic and psychologic symptoms associated with use of injectable contraception and 20 microg oral contraceptive pills. Am J Obstet Gynecol. 2008;199(4):351.e1–351.e12.[↩]
- Berenson AB, Rahman M. Changes in weight, total fat, percent body fat, and central-to-peripheral fat ratio associated with injectable and oral contraceptive use. Am J Obstet Gynecol. 2009;200(3):329. e1–329. e8.[↩]
- Lopez LM, Ramesh S, Chen M, Edelman A, Otterness C, Trussell J, Helmerhorst FM. Progestin-only contraceptives: effects on weight. Cochrane Database of Systematic Reviews 2016, Issue 8. Art. No.: CD008815. DOI: 10.1002/14651858.CD008815.pub4. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD008815.pub4/full[↩][↩]
- Body Weight Planner. https://www.supertracker.usda.gov/bwp/index.html[↩][↩]
- National Heart, Lung, and Blood Institute. (2012). What causes overweight and obesity? https://www.nhlbi.nih.gov/health/health-topics/topics/obe/causes[↩]
- ChooseMyPlate. https://www.choosemyplate.gov/[↩]
- https://supertracker.usda.gov/[↩][↩][↩]
- BMI Calculator Adults. https://www.cdc.gov/healthyweight/assessing/bmi/adult_BMI/english_bmi_calculator/bmi_calculator.html[↩]
- BMI Calculator Children. https://nccd.cdc.gov/dnpabmi/Calculator.aspx[↩]
- Obesogens. https://www.niehs.nih.gov/health/topics/conditions/obesity/obesogens/index.cfm[↩]
- Ambient (outdoor) air quality and health. http://www.who.int/mediacentre/factsheets/fs313/en/[↩]
- Flame retardants. https://www.niehs.nih.gov/health/topics/agents/flame_retardants/index.cfm[↩]
- https://www.epa.gov/saferchoice/consumer-fact-sheet-flame-retardants[↩]
- Bisphenol A (BPA). https://www.niehs.nih.gov/health/topics/agents/sya-bpa/index.cfm[↩]
- http://aghealth.nih.gov[↩]
- Centers for Disease Control and Prevention. (2012). Overweight and obesity: Causes and consequences. https://www.cdc.gov/obesity/adult/causes.html[↩]


{kind=link}