
Contents
How to do a self breast exam
Women of all ages should become familiar with their breasts. But it becomes more important as you get older as the risk of breast cancer increases with age.
Everyone’s breasts are different. It is important that you get to know what your breasts look and feel like, so you know what is normal for you. There is no right or wrong way to do this, however the following suggestions can be used as a guide.
Begin with a visual examination of your breasts
Sit or stand shirtless and braless in front of a mirror with your arms at your sides. If you have a vision impairment that makes it difficult for you to visually inspect your breasts, ask a trusted friend or a family member to help you. To inspect your breasts visually, do the following:
- Look in the mirror and feel your breasts from time to time.
- Face forward and look for puckering, dimpling, or changes in size, shape or symmetry.
- Check to see if your nipples are turned in (inverted).
- Inspect your breasts with your hands pressed down on your hips.
- Inspect your breasts with your arms raised overhead and the palms of your hands pressed together.
- Lift your breasts to see if ridges along the bottom are symmetrical.
Next, use your hands to examine your breasts
- Feel them while you are in the shower or bath, lying in bed or getting dressed. It should only take a few minutes.
- Remember to feel all the breast tissue, from the collarbone to below the bra line and under the arms.
- Use the flat part of your fingers and the finger pads to feel near the surface and deeper into the breasts.
Common ways to perform the manual part of the breast exam include:
- Lying down. Choose a bed or other flat surface to lie down on your back. When lying down, breast tissue spreads out, making it thinner and easier to feel.
- In the shower. Lather your fingers and breasts with soap to help your fingers glide more smoothly over your skin.
When examining your breasts, some general tips to keep in mind include:
- Use the pads of your fingers. Use the pads, not the very tips, of your three middle fingers for the exam. If you have difficulty feeling with your finger pads, use another part of your hand that is more sensitive, such as your palm or the backs of your fingers.
- Use different pressure levels. Your goal is to feel different depths of the breast by using different levels of pressure to feel all the breast tissue. Use light pressure to feel the tissue closest to the skin, medium pressure to feel a little deeper, and firm pressure to feel the tissue closest to the chest and ribs. Be sure to use each pressure level before moving on to the next spot. If you’re not sure how hard to press, talk with your doctor or nurse.
- Take your time. Don’t rush. It may take several minutes to carefully examine your breasts.
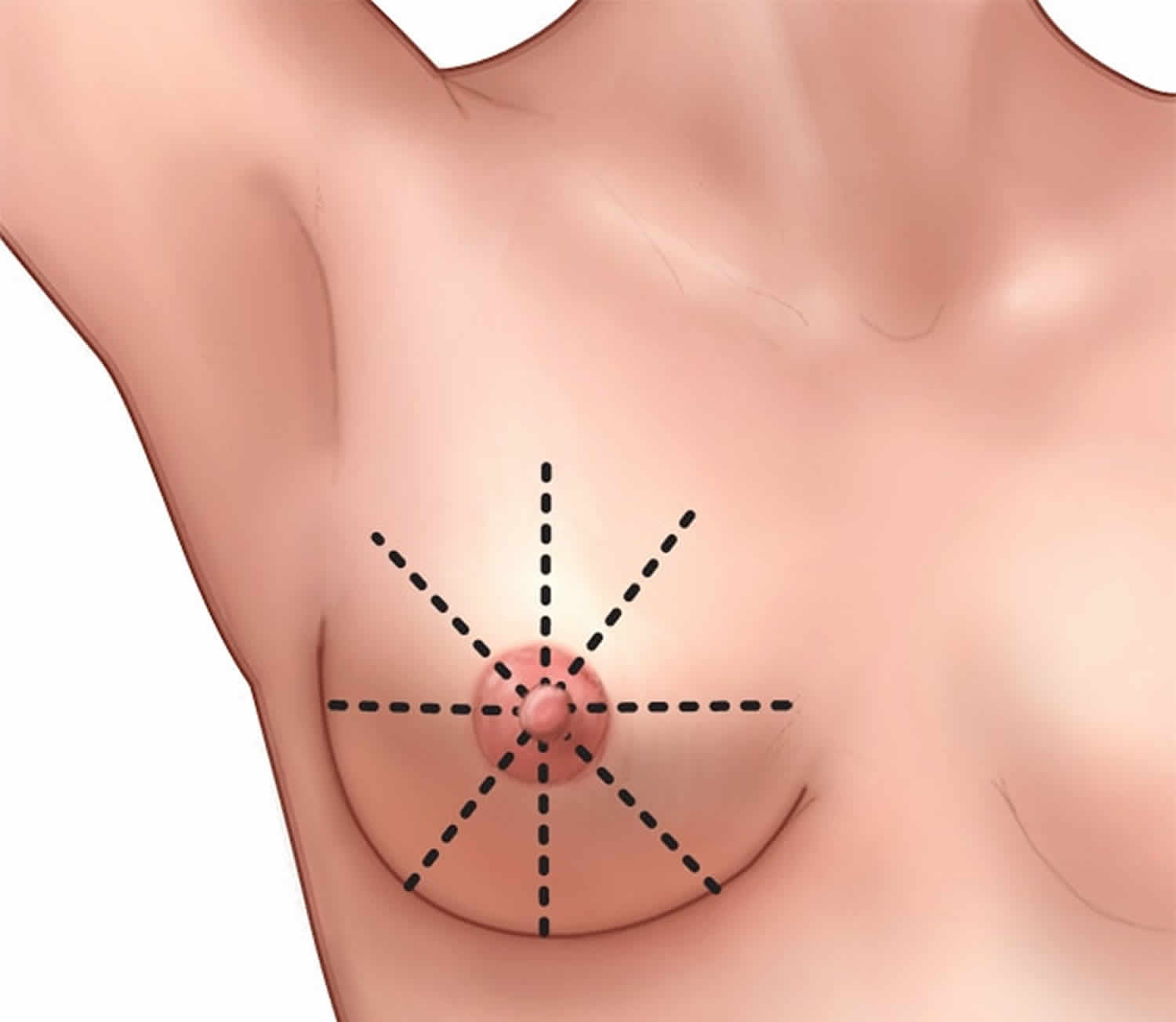
- Follow a pattern. Use a methodical technique to ensure you examine your entire breast. For instance, imagine the face of a clock over your breast or the slices of a pie. Begin near your collarbone and examine that section, moving your fingers toward your nipple. Then move your fingers to the next section.
If you have a disability that makes it difficult to examine your breasts using this technique, you likely can still conduct a breast self-exam. Ask your doctor to show you ways you can examine your breasts.
If you are still having your periods, expect your breasts to feel different at different times of the month. For example, some women get painful, lumpy or swollen breasts just before their period starts and softer breasts after their period has finished.
See your doctor if you notice any unusual changes. If you find any unusual changes, it is important that you see your doctor straight away. Unusual breast changes include:
- a lump, lumpiness or thickening in the breast or under the arm
- changes in the skin on or around the breast, such as dimpling, puckering or redness
- changes in the nipple, such as inversion, new nipple discharge, or itchy or ulcerated skin
- an area of the breast that feels different from the rest
- new pain that doesn’t go away.
Your doctor will examine your breasts and ask about your medical history. Your doctor may send you for tests to find out what caused the changes.
Most changes are not breast cancer. However, it is always important to have any changes checked out straight away by your doctor.
Figure 1. Self breast exam pattern
Make an appointment with your doctor if you notice:
- A hard lump or knot near your underarm
- Changes in the way your breasts look or feel, including thickening or prominent fullness that is different from the surrounding tissue
- Dimples, puckers, bulges or ridges on the skin of your breast
- A recent change in a nipple to become pushed in (inverted) instead of sticking out
- Redness, warmth, swelling or pain
- Itching, scales, sores or rashes
- Bloody nipple discharge
Your doctor may recommend additional tests and procedures to investigate breast changes, including a clinical breast exam, mammogram and ultrasound.
Follow-up tests to diagnose breast changes
The procedures and tests listed below may be recommended by your health care provider to help diagnose a breast change that was found on a mammogram or that you or your health care provider felt.
- Diagnostic mammography: A type of mammography in which more x-ray pictures of the breast are taken from different angles to allow a possible abnormality to be examined more closely.
- Ultrasound: A procedure that makes a picture (called a sonogram) of breast tissue in order to find out if a lump is solid or is filled with fluid (that is, a cyst). Pictures are made using sound waves.
- MRI (also called Magnetic Resonance Imaging): A procedure that uses a powerful magnet, radio waves, and a computer to take detailed pictures of areas inside the breast. An MRI can be used to learn more about breast lumps or large lymph nodes that were found during a clinical breast exam or breast self-exam but were not seen on a mammogram or ultrasound.
- Ductography (also called a galactography): A procedure that takes pictures of the breast ducts, so that doctors can learn more about certain kinds of abnormal nipple discharge or masses such as intraductal papillomas (wart-like tumors that are benign). Pictures of the breast ducts are taken using a contrast material that is given through an injection to help breast ducts show up clearly.
- Biopsy: A procedure that removes a sample of breast tissue or an entire lump so that it can be checked for signs of disease. Imaging procedures (such as ultrasound, MRIs, or x-rays) are often used during a biopsy to guide the surgeon. A pathologist then examines the sample under a microscope or performs other tests on it. Common types of breast biopsies include:
- Core needle biopsy: The use of a wide needle to remove small tissue sample(s) that are about the size of a grain of rice. It may cause a temporary bruise. Also called core biopsy.
- Fine-needle aspiration biopsy: The use of a thin needle to drain fluid and/or to remove cells.
- Surgical biopsy: The removal of part, or all, of a lump so it can be checked for signs of cancer. An incisional biopsy removes a sample of breast tissue. An excisional biopsy removes an entire lump or suspicious area. Wire localization (also called needle localization and needle (wire) localization) may be used to mark the area of abnormal tissue before the biopsy.
- Vacuum-assisted biopsy: The removal of a small sample of breast tissue using a probe that is connected to a vacuum device. The small cut made in the breast is much smaller than with surgical biopsy. This procedure causes little scarring, and no stitches are needed. It may also be called vacuum-assisted core biopsy.
Biopsies are usually done in a doctor’s office or a clinic on an outpatient basis. This means you will go home the same day as the procedure. Local anesthesia is used for many biopsies, so you’ll be awake but won’t feel pain during the procedure. General anesthesia is commonly used for surgical biopsies, which means you’ll be asleep during the procedure.
Breast conditions and treatment
The following alphabetical list of breast conditions includes follow-up steps and treatments that may be recommended by your health care provider. Some of these breast conditions are associated with an increased risk of breast cancer, although most are benign.
- Adenosis: A benign condition of glandular tissue in the breast that may result in small round lumps, lumpiness, or lumps that are too small to be felt. If there is scar-like fibrous tissue, the condition is called sclerosing adenosis.
- Atypical ductal hyperplasia: A condition in which there are more cells than normal in the breast ducts and the cells look abnormal under a microscope. Women with atypical ductal hyperplasia have an increased risk of breast cancer.
- If atypical ductal hyperplasia is found after a core needle biopsy, then a surgical biopsy is often recommended as the next step.
- If atypical ductal hyperplasia is found and diagnosed after a surgical biopsy that takes out the entire area of atypical ductal hyperplasia, follow-up care includes more frequent mammograms. Sometimes, your doctor may advise more frequent clinical breast exams and breast self-exams.
- Drugs such as tamoxifen (for all women) or raloxifene or an aromatase inhibitor (for postmenopausal women) may also be prescribed.
- Atypical lobular hyperplasia: A condition in which there are more cells than normal in the breast lobules and the cells may look abnormal. Women with atypical lobular hyperplasia have an increased risk of breast cancer.
- If atypical lobular hyperplasia is found after a core needle biopsy, as is often the case, your doctor will talk with you about whether a surgical biopsy or more frequent mammograms are recommended.
- If atypical lobular hyperplasia is found during a surgical biopsy that takes out the entire area of ALH, follow-up care generally includes only more frequent mammograms.
- Drugs such as tamoxifen (for all women) or raloxifene or an aromatase inhibitor (for postmenopausal women) may also be prescribed.
- Cysts: Fluid-filled lumps that are often found in both breasts. They may be painful just before your menstrual period begins. Some cysts may be felt, while others are too small to be felt. Cysts are most common in premenopausal women and in women taking menopausal hormone therapy. Cysts are diagnosed with ultrasound and/or fine needle aspiration and usually don’t require additional treatment.
- Ductal carcinoma in situ (DCIS): A condition in which abnormal cells are found in the lining of a breast duct. DCIS may also be referred to as intraductal carcinoma. In some cases, DCIS will become invasive breast cancer. Treatment is based on how much and what part of the breast is affected and how abnormal the cells look (grade). Most women with DCIS are cured with proper treatment. Treatment may include:
- Lumpectomy. This is a type of breast-conserving surgery (also called breast-sparing surgery). This may be followed by radiation therapy.
- Mastectomy. This is surgery to remove the breast or as much of the breast tissue as possible.
- Tamoxifen. This drug may also be taken to lower the chance that DCIS will come back after treatment or to prevent invasive breast cancer.
- Duct ectasia (also called mammary duct ectasia): A breast condition in which the ducts in the breast thicken and become blocked with fluid, causing nipple discharge, tender or red nipples, and inverted nipples. If the blocked duct becomes infected, you may feel a lump under the nipple. Most often this condition goes away on its own and doesn’t need treatment. Your health care provider may suggest you take pain medicine; apply a warm, wet cloth to your breast; use breast pads for nipple discharge; and/or take antibiotics.
- Fat necrosis: A breast condition that may cause round, firm, usually painless lumps. It may appear after an injury to the breast, surgery, or radiation therapy. Skin around the lump may look red, bruised, or dimpled. A biopsy may be used to both diagnose and remove fat necrosis.
- Fibroadenoma: A benign tumor that feels like a hard, round lump in the breast. These lumps move easily and usually don’t hurt. Fibroadenomas are the most common benign breast tumor in women under 30 years old. Complex fibroadenomas may slightly increase your risk of breast cancer. These lumps may go away, or your doctor may advise that they be removed.
- Fibrocystic breast changes (also called fibrosis or fibrocystic breast disease): A common breast condition that causes painful, lumpy breasts. Symptoms often start before or during your menstrual period. Other changes may include sensitive nipples and itching. Fibrosis is most common among women under the age of 45 and among women taking hormone replacement therapy. As many as half of all women may have fibrocystic breast changes at some point in their lives. Although these changes are not usually treated, your health care provider may recommend that you take pain medicine, apply heat or ice compresses, and/or wear a tighter fitting bra.
- Granular cell tumors: These rare tumors are almost always benign. Symptoms may include a firm lump in the breast. Surgery may be needed to remove these tumors.
- Intraductal papilloma: A wart-like growth that is usually close to the nipple. It may cause pain, a lump, and clear, sticky, or bloody discharge. Single papillomas don’t increase a woman’s risk of breast cancer. However, women with multiple papillomas have an increased risk of breast cancer. A biopsy is often used to both diagnose and remove these growths.
- Lobular carcinoma in situ (LCIS): A condition in which abnormal cells are found in the breast lobules. There are more abnormal cells in the lobules with LCIS than with atypical lobular hyperplasia. Women with lobular carcinoma in situ have an increased risk of developing cancer in either breast.
- If lobular carcinoma in situ is found after a core needle biopsy, an excisional biopsy will be done.
- If lobular carcinoma in situ is diagnosed and removed during an excisional biopsy, follow-up includes more frequent mammograms. Your doctor may also advise more frequent clinical breast exams and breast self-exams.
- Drugs such as tamoxifen (for all women) or raloxifene or an aromatase inhibitor (for postmenopausal women) may also be prescribed by your doctor.
- Mastitis: A breast condition in which the breast looks red and feels lumpy, warm, and tender. It is most common among women who are breastfeeding and is caused when a milk duct becomes blocked and infected. Mastitis is commonly treated with antibiotics and can be prevented with a change in breastfeeding techniques that your doctor, nurse, or a breastfeeding consultant can help with.
- Phyllodes tumor (also called CSP and cystosarcoma phyllodes): A rare type of breast tumor that is usually benign but may be cancer. In rare cases, it may spread to other parts of the body. These tumors are usually removed surgically.
- Sclerosing Adenosis: A type of adenosis in which scar-like fibrous tissue is found in the glands of the breast. It may cause pain and slightly increase a woman’s risk of breast cancer. Although treatment is not usually needed, your doctor may advise taking pain medicine, making dietary changes, or wearing a bra with extra support.
What to look for in self breast exam
A self breast exam for breast awareness is an inspection of your breasts that you do on your own. To help increase your breast awareness, you use your eyes and hands to determine if there are any changes to the look and feel of your breasts.
If you notice new breast changes, discuss these with your doctor. Though most breast changes detected during a self-exam for breast awareness have benign causes, some changes may signal something serious, such as breast cancer.
A self breast exam that you do for breast awareness helps you understand the normal look and feel of your breasts. If you notice a change in your breasts that seems abnormal or if you notice one breast is different when compared with the other, you can report it to your doctor.
There are many conditions that can cause changes in your breasts, including breast cancer.
Although the self breast exam technique isn’t always a reliable way to detect breast cancer, a significant number of women report that the first sign of their breast cancer was a new breast lump they discovered on their own. For this reason, doctors recommend being familiar with the normal consistency of your breasts.
To prepare for your self-breast exam for breast awareness:
- Ask your doctor for a demonstration. Before you begin breast self-exams for breast awareness, you may find it helpful to discuss the instructions and technique with your doctor.
- If you menstruate, choose a time in your cycle when your breasts are least tender. Your hormone levels fluctuate each month during your menstrual cycle, which causes changes in breast tissue. Swelling begins to decrease when your period starts. The best time to perform a self-exam for breast awareness is usually the week after your period ends.
Breast changes of concern
Some breast changes can be felt by a woman or her health care provider, but most can be detected only during an imaging procedure such as a mammogram, MRI, or ultrasound. Whether a breast change was found by your doctor or you noticed a change, it’s important to follow up with your doctor to have the change checked and properly diagnosed.
Check with your health care provider if your breast looks or feels different, or if you notice one of these symptoms:
- Lump or firm feeling in your breast or under your arm. Lumps come in different shapes and sizes. Normal breast tissue can sometimes feel lumpy. Doing breast self-exams can help you learn how your breasts normally feel and make it easier to notice and find any changes, but breast self-exams are not a substitute for mammograms.
- Nipple changes or discharge. Nipple discharge may be different colors or textures. It can be caused by birth control pills, some medicines, and infections. But because it can also be a sign of cancer, it should always be checked.
- Skin that is itchy, red, scaled, dimpled or puckered
Breast changes during your lifetime that are not cancer
Most women have changes in the breasts at different times during their lifetime 1.
- Before or during your menstrual periods, your breasts may feel swollen, tender, or painful. You may also feel one or more lumps during this time because of extra fluid in your breasts. Your health care provider may have you come back for a return visit at a different time in your menstrual cycle to see if the lump has changed.
- During pregnancy, your breasts may feel lumpy. This is usually because the glands that produce milk are increasing in number and getting larger. While breastfeeding, you may get a condition called mastitis. This happens when a milk duct becomes blocked. Mastitis causes the breast to look red and feel lumpy, warm, and tender. It may be caused by an infection and it is often treated with antibiotics. Sometimes the duct may need to be drained.
- As you approach menopause, your hormone levels change. This can make your breasts feel tender, even when you are not having your menstrual period. Your breasts may also feel more lumpy than they did before.
- If you are taking hormones (such as menopausal hormone therapy, birth control pills, or injections) your breasts may become more dense. This can make a mammogram harder to interpret. Be sure to let your health care provider know if you are taking hormones.
- After menopause, your hormone levels drop. You may stop having any lumps, pain, or nipple discharge that you used to have.
Self breast exam limitations
A self breast exam for breast awareness is a safe way to become familiar with the normal look and feel of your breasts.
However, there are some limitations and risks, including:
- Anxiety caused by finding a lump. Most of the changes or lumps women find in their breasts aren’t cancerous. Still, finding something suspicious in your breast can make you anxious about what it may mean. You may endure several days of worry until you can see your doctor.
- Additional tests and procedures may be necessary to check out lumps or changes. If you discover a suspicious lump, you may end up having imaging test such as a diagnostic mammogram or a breast ultrasound, or a procedure to remove breast tissue for examination (biopsy). If it turns out the lump was noncancerous (benign), you might feel that you’ve undergone an invasive procedure unnecessarily.
- Overestimating the benefits of self breast exam. A self breast exam isn’t a substitute for a breast exam by your doctor (clinical breast exam) or a screening mammogram. Becoming familiar with the normal look and feel of your breasts can supplement breast cancer screening, but can’t replace it.
Discuss the benefits and limitations of being familiar with the consistency of your breasts with your doctor.
Most medical organizations don’t recommend routine breast self-exams as a part of breast cancer screening. That’s because breast self-exams haven’t been shown to be effective in detecting cancer or improving survival for women who have breast cancer.
There is no direct high-quality evidence from clinical trials that population-based screening using self breast exam is effective in reducing the number of deaths from breast cancer 2, 3. Randomized controlled trials of screening at a population level using clinical breast examination compared to no screening have been undertaken, two in India 4, 5 and one in Egypt 6, but have not reported results on breast cancer mortality.
In 2015 the International Agency for Research on Cancer (IARC) Working Group concluded that there was inadequate evidence that clinical breast examination reduces breast cancer mortality, and noted that in three clinical trials of clinical breast examination compared to no screening, breast cancers detected at baseline and in the early years of the trials tended to be of a smaller size and less advanced stage in the group of women that had clinical breast examination 7.
For women who are not participating in regular mammographic screening, regular clinical breast examination may offer some benefit.
Still, doctors believe there is value in women being familiar with their own breasts, so they understand what’s normal and promptly report changes.
How is breast cancer diagnosed?
Doctors often use additional tests to find or diagnose breast cancer. They may refer women to a breast specialist or a surgeon. This does not mean that she has cancer or that she needs surgery. These doctors are experts in diagnosing breast problems.
- Breast ultrasound. A machine that uses sound waves to make detailed pictures, called sonograms, of areas inside the breast.
- Diagnostic mammogram. If you have a problem in your breast, such as lumps, or if an area of the breast looks abnormal on a screening mammogram, doctors may have you get a diagnostic mammogram. This is a more detailed X-ray of the breast.
- Magnetic resonance imaging (MRI). A kind of body scan that uses a magnet linked to a computer. The MRI scan will make detailed pictures of areas inside the breast.
- Biopsy. This is a test that removes tissue or fluid from the breast to be looked at under a microscope and do more testing. There are different kinds of biopsies (for example, fine-needle aspiration, core biopsy, or open biopsy).
- Breast Changes and Conditions. https://www.cancer.gov/types/breast/breast-changes[↩]
- Humphrey LL, Helfand M, Chan BKS and Woolf SH. Breast Cancer Screening: A Summary of the Evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137 (5 Part 1):347-360[↩]
- Kösters J GP. Regular self-examination or clinical examination for early detection of breast cancer. Cochrane Database of Systematic Reviews. Issue 2. 2003;(Art. No.: CD003373 ):DOI: 10.1002/14651858.CD003373[↩]
- Mittra I, Mishra GA, Singh S, et al. A cluster randomized, controlled trial of breast and cervix cancer screening in Mumbai, India: methodology and interim results after 3 rounds of screening. Int J Cancer. 2010;126 976-984.[↩]
- Sankaranarayanan R, Ramadas K, Thara S, et al. Clinical Breast Examination: Preliminary Results from a Cluster Randomized Controlled Trial in India. J Natl Cancer Inst. 2011;103 1-5[↩]
- Boulos S, Gadallah M, Neguib S, et al. Breast screening in the emerging world: high prevalence of breast cancer in Cairo. Breast. 2005;14 (5):340-6[↩]
- Lauby-Secretan B, Scoccianti C, Loomis D, et al. Breast-cancer screening–viewpoint of the IARC Working Group. N Engl J Med. 2015;372 (24):2353-8[↩]





{kind=link}